Consumer willingness to pay for a hypothetical Chagas disease vaccine in Brazil: a cross-sectional study and the implications
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Chagas disease is a serious public health problem, endemic in 21 countries in Latin America. A future vaccine can contribute to decreasing the number of cases and its complications. Methods: A cross-sectional study was conducted with residents of the northern region of Brazil, on the willingness to pay for a hypothetical vaccine against Chagas disease (effective protection of 80%). Results: We interviewed 619 individuals and seven were excluded from the analysis and the value of willingness to pay was US$23.77 (100.00 BRL). Conclusion: The Northern region of Brazil is one of the largest markets for this vaccine, due to its epidemiological relevance, so economic studies with this vaccine will be important to assist in the assessment of technologies.
The disorderly growth of urbanization in Brazil, coupled with environmental conditions such as accelerated deforestation and the climate, have contributed to the emergence and high prevalence of tropical infections including Chagas disease. Tropical diseases occur in 149 countries [1], representing 11.4% of the global burden of disease [2] and affecting one billion people globally [1]. These infections are responsible for causing between 500,000 to 1 million deaths annually [2]. As a result, billions of dollars are typically spent each year on preventive measures and treatment in many developing economies [1,3]. In Brazil, the most prevalent tropical diseases include malaria, dengue, Chagas disease, leishmaniasis, schistosomiasis, tuberculosis and leprosy [4,5].
Chagas disease (American Trypanosomiasis) is anthropozoonosis whose causative agent is protozoan, Trypanosoma cruzi, transmitted to humans via the feces of infected triatomines (barbers). Other contamination pathways include blood transfusion or organ transplants, congenital, indirect contact (via food ingestion) and breast milk [6]. Chagas disease is an important public health problem, especially in endemic countries such as Brazil, Argentina, Chile and Bolivia [7]. According to data from the Pan American Health Organization (PAHO), between six and seven million individuals have been infected and, approximately, 70 million people live in places prone to Chagas infections [7]. Moreover, 30,000 new cases and 14,000 deaths are currently reported per year [8,9]. Overall, Chagas disease represents one of the four major causes of deaths from infectious and parasitic diseases in Brazil [6].
Chagas disease is mainly presented in two phases, acute and chronic. In the acute phase, individuals may present with prolonged fever (more than 7 days), headache, intense weakness, swelling of one eye, swelling and redness at the site of the sting, stomach pain, vomiting and diarrhea. However, in the chronic phase, events related to disturbances in the heart, esophagus and intestine are highlighted [6,10]. There is currently no cure for patients in the chronic phase, and the most serious complication is chronic chagasic cardiopathy, which is highly disabling [11]. This is a concern as currently there appears to be an under diagnosis of Chagas disease [12].
According to the Drugs for Neglected Diseases initiative (DNDi) (2019), this infection is endemic in 21 Latin American countries, causing more deaths than malaria or any other parasitic disease. Further, less than 1% of these patients have access to treatment [9]. In Brazil, approximately 1 million people are estimated to be infected. According to data from the Strategic Management Support Room of the Ministry of Health, 72,084 individuals died between 2001 and 2015, 1187 of which were in the Northern region and 206 in the state of Pará. Besides the Northern region, the Northeast of Brazil is often recognized as one of the other regions in Brazil with the highest number of cases in the country [13].
The Brazilian Unified Health System (SUS) is responsible for providing medicines to treat diseases, which includes benznidazole and nifurtimox for patients with Chagas disease [5]. However, there are concerns with the effectiveness and safety of these medicines, especially, during the chronic phase of the disease limiting their usefulness [10,14]. Consequently, there is a need for effective preventive measures to combat Chagas disease.
Strategies that aim to combat the insect vector (insecticides) in homes in Brazil include the promotion of housing improvement in high-risk areas as well as the encouragement of mosquito nets or wire mesh and individual protection instruments including repellents and long-sleeved clothing. Alongside this, health surveillance and inspections have been intensified at all stages of the food production chain where there is susceptibility to contamination, with special emphasis on places where food is handled [6].
In the last few years, several vaccines against Trypanosoma cruzi infection have been developed [15]. These include the immunotherapeutic vaccines, rTSA-1 and rTc24, which are based on TSA-1 and Tc24 antigens, developed by Villanueva-Lizama and collaborators (2018). Previously, positive results were obtained for immune response induction during clinical phase studies involving 39 participants in Mexico [16]. The importance of studies on the development of effective and safe vaccines for the prevention of the disease is important and could represent an effective relevant strategy for combating infections [17]. We are already seeing this with considerable interest and commercial activities surrounding the development of a vaccine against COVID-19.
Some studies published on the research and development scenario of a Chagas disease vaccine have shown promising results. The TcG2/TcG4 vaccine is an example of such development and protection against several T. Cruzi strains has been demonstrated [18,19]. In addition in a study recently conducted by Berry and colleagues (2019), the Tc24 + E6020-SE vaccine showed satisfactory results in model testing of T. Cruzi-infected mice in the chronic phase of infection. Additionally, reduction of the inflammatory process and cardiac fibrosis, as well as systemic parasitemia were observed [20]. Other vaccines developed in Mexico, rTSA-1 and rTc24, are being considered as more advanced candidates for Chagas disease vaccine development as they have demonstrated good immune response results in a group of 39 people. This finding also supports the combination of two parasitic proteins (TSA-1 and Tc24) for use as potential vaccine candidates in humans [16].
In Brazil, the Medication Market Regulation Chamber (CMED) is responsible for the economic regulation of drugs commercialized in the country. CMED evaluates and establishes the prices of medicines that will be marketed in the country [21]. However, the approval and registration of new medicines including vaccines for commercialization is made by the Health Regulatory Agency (ANVISA) [22]. Consequently, a new technology is only introduced onto the Brazilian market upon compliance with the criteria established by Resolution No. 2 of March 5 2004 guidance [23]. Thereafter, its pricing is defined by CMED. As a vaccine against Chagas disease will be a new product, this technology would be classified as category I. Further, its price cannot be higher than the lowest price of a number of countries including Australia, Canada, France, Greece, Italy, New Zealand, Portugal, Spain and USA [23]. In accordance with the price defined by CMED and for commercialization in the private market, pharmaceutical companies generally submit their new technology to the National Commission for the Incorporation of Technology (CONITEC) for incorporation into the SUS [24].
In the context of limited healthcare resources and growing demand in Brazil [25], it is important to emphasize the importance of undertaking studies in an economic context to support the process of rational decision-making [26,27]. Priority setting is crucial in a country such as Brazil where the public health system caters for over 210 million inhabitants [28]. Accordingly, studies that seek to identify the value of technologies of clinical interest for a given country, such as a vaccine for the prevention of Chagas disease in Brazil, may contribute to future decision-making regarding their pricing.
Willingness to pay (WTP) is a methodology that seeks to estimate the maximum individual value to be allocated to a specific program, medical intervention, or treatment to identify its monetary value. WTP studies enable decision makers to assess a point value, ranges of values, or the positive or negative response to a presented value, contributing to a better perception of an individual's preferences in health decision-making processes [29]. This technique is based on the application of a questionnaire, with prior presentation of the characteristics of the evaluated intervention to the interviewee, in addition to conditions and aspects relevant to the clinical context [30,31]. Importantly, to perform this economic analysis, all participants must receive the same guidance, which requires training for the interviewers [32].
In recent years, this methodological approach has enhanced deliberations regarding the potential value of new vaccines with the first approved dengue vaccine in Brazil [33]. There have also been hypothetical scenarios to help guide future investment and pricing decisions including WTP for a dengue vaccine in countries including the Philippines [34], Indonesia [35], Thailand, Colombia and Vietnam [36], as well as for Ebola [37], HIV [38], malaria [39–42], hepatitis [43], zika [30] and chikungunya [31]. However we are not aware of any studies to date that have evaluated the WTP for a Chagas disease-targeted vaccine. It is important to evaluate the WTP for a hypothetical vaccine for Chagas disease initially by residents of the state of Pará in the Northern region, which comprises seven states including Amazonas, Pará, Acre, Roraima, Rondônia, Amapá and Tocantins, with Pará having the largest number of inhabitants corresponding to 46.68% of the population of this region [44]. The findings from this study may reinforce the need for economic studies to better contribute to the evaluation of new vaccines. Accordingly, methodological approaches, such as WTP may be one of the tools to assist in discussions regarding potential prices for vaccines of relevant infections.
Materials & methods
This study was performed to estimate the WTP of people in Northern Brazil for a hypothetical vaccine to prevent Chagas disease via a contingent valuation analysis. A questionnaire with open and closed questions was used to collect data relevant to individuals who may or may not have had Chagas disease in the past, but were not known to have had the disease at the time of the interview in line with other similar studies [30–33].
Design & study location
The survey was conducted in eleven cities (Belém, Marabá, Parauapebas, Abaetetuba, Rondón do Pará, São Domingos do Araguaia, São João do Araguaia, Baião, Canaã dos Carajás, Jacundá and Itupiranga) in the state of Pará, the ninth most populous state in Brazil. In 2019, this State had 8,602,865 inhabitants, 2,275,032 of which are currently registered in the Metropolitan Region of Belém. Additionally, the Northern region, state of Pará and Brazil are located close to each other and in 2010 had an average Human Development Index (HDI) score of 0.667, 0.646 and 0.737, respectively [45,46].
Despite similar HDI scores, the state of Pará differs from the rest of Brazil in terms of the average per capita income and the social demographic characteristics. In 2018, the monthly per capita income was US$326.40 (R$1,373.00 BRL) for Brazil and US$205.16 (R$863.00 BRL) for Pará [47]. Additionally, of the 26 states of Brazil, Pará holds the nineteenth position in terms of average per capita income of Brazilian cities. However, Pará was responsible for 83% Chagas disease cases in Brazil, making this State highly relevant for this research [6].
The questionnaire (Supplementary Material) used to interview the participants was developed by the research team building on previous publications [30,32–34,36]. Interviews were conducted by undergraduate students in health courses, particularly students with a Bachelor's Degree in Collective Health at the Federal University of Southern and Southeastern Pará (Unifesspa) who were previously trained by the researchers responsible for this study. These researchers applied the methodological approach of WTP, as recommended in previously published studies [30,31,33].
Data collection instrument
The WTP technique involves the application of a questionnaire, with prior presentation to the interviewee of the characteristics of the disease, the intervention required for decision-making process, and the conditions and important aspects of the clinical context of the disease. To use the WTP technique, all interviewees must receive the same information [32]. Consequently, training of the interviewers involved in the survey was required and was conducted prior to the applications in June 2019 at Unifesspa.
The questionnaire comprised the following five sections: questions to test participants' knowledge regarding Chagas disease; information on the disease, intervention and alternatives for preventing the disease; questions to assess their understanding of the information provided; Discrete Choice, Bidding Game and Open-Ended Questions [34] including questions to identify whether individuals would pay US$14.26 (R$60.00 BRL) for a single dose of the hypothetical Chagas disease vaccine and questions to estimate the range of values that respondents would pay for the technology; and a socioeconomic questionnaire.
For the discrete choice technique, the value of US$14.26 (R$60.00 BRL) was established for a single dose of Chagas disease vaccine. This choice was derived based on the Brazilian market involving single-dose vaccines, in consultation with the Price List of the Drug Market Regulation Chamber (CMED) and through the factory price (FP) of vaccines in Brazil [48].
The efficacy of vaccine protection (80%), as well as the possibility of local events (e.g., swelling at the site of application and pain) and information on the disease, epidemiological data and criteria for vaccination were included in the initial stage of the interview. Difficulties associated with questions related to the research context and the socioeconomic questionnaire were explained by the interviewers. An illustration was also used to exemplify and facilitate an understanding of the percentage of protection from the hypothetical vaccine for Chagas disease.
Sampling & selection criteria
The selection of the interviewees was performed in a random manner. Briefly, individuals from high circulation areas, such as squares, parks, markets and fairs, were invited to participate and if they agreed, completed the questionnaire.
If there is a greater uncertainty that 50% of the respondents would agree to pay US$14.26 (R$60.00 BRL; a margin of global error of 4 percentage points at a 95% confidence level), a minimum of 600 respondents would be required in this survey. The number of individuals to be interviewed in each of the eleven cities was defined according to the population size of each of these municipalities [46].
As described, interviewees may or may not have a history of Chagas disease; however, at the time of the interview, they were excluded if they had symptoms or were diagnosed with the disease. As a criterion for participation, individuals had to possess and declare an income, with individuals under 18 years of age and those without income being excluded. Individuals who would not use the vaccine or would not use it even if it were free and those who were willing to pay more than twice their declared monthly income were excluded from the sample, as established for this approach [32] and observed in similar studies [30,31,33,36].
Data analysis
The WTP for a Chagas disease vaccine was estimated from the maximum median value declared by individuals who were willing to pay any amount greater than or equal to zero. The median of the maximum WTP among the groups defined by the covariates was compared using the Mann–Whitney test (two groups) or the Kruskal–Wallis test (three or more groups). The level of significance was 5%. All socioeconomic variables were evaluated and the median ratio of the maximum WTP for the hypothetical Chagas disease vaccine, such as education and per capita family income, were included. To evaluate the median of the maximum disposable value to pay and the per capita family income, the individuals were organized into groups and stratified by per capita wage income (number of minimum wages) into ‘<0–0.25,’ ‘0.25–0.50,’ ‘0.50–0.75’ and ‘0.75–7.5’ groups, with each containing 25% of the sample data. For the correlation involving disposition and schooling, the respondents were stratified by level of schooling: ‘never studied or did not complete primary education,’ ‘completed primary education,’ ‘completed secondary education’ and ‘completed higher education or more.’
The frequency of participants who had private health insurance or were without insurance at the time of the interview was assessed. According to the National Supplementary Health Agency (ANS), which regulates private health insurance in Brazil, private health insurance coverage in Pará comprised 10.3% of its population until March 2019, with 807,453 beneficiaries in the state as of June 2019. However, the national profile was 24.2% of the population (47,053,184 people) in March 2019 [49].
Additionally, the WTP of the interviewees was evaluated controlling for variables including history with the disease, health plan and gender. As a tool for statistical analysis, Microsoft Excel 2010 and Minitab 17 were used. For comparative purposes, the conversion value provided by the Brazilian Central Bank (2020: US$1 = R$4.2064 BRL/Brazilian real) [50] was adopted.
Ethics statement
All interviews were conducted after reading and signing an informed consent form. In addition, all researchers of the project signed a confidentiality agreement prior to the interviews. This study was approved by the Ethics and Research Committee of the Federal University of Pará (UFPA), under CAAE registration number 12943619.5.0000.8607.
Results
Population characteristics
A total of 619 interviews were conducted with individuals aged between 18 and 84 who agreed to participate and answer the questionnaire. Table 1 describes the characteristics of the individuals including in the study. The average age of the interviewees was approximately 36 years; 43.9% [619] of the population were males, 96.8% worked at the time of the interview, 38.1% were self-employed, 3.6% reported being retired and 17.6% had completed higher education or more.
| Variable | n | (%) |
|---|---|---|
| Age in years (mean [SD]) | 36.5 | 5.9 |
| Man | 272 | 43.9 |
| Has children | 380 | 61.4 |
| Education level | ||
| – Had never attended school | 5 | 0.8 |
| – Completed elementary school | 120 | 19.4 |
| – Completed high school | 381 | 61.6 |
| – Completed college or more | 109 | 17.6 |
| Currently working | 599 | 96.8 |
| Have private health insurance | 213 | 34.4 |
| Had Chagas disease | 2 | 0.3 |
| Reported that other people in the household had Chagas disease | 6 | 1 |
| Family income (number of minimal wages†) | ||
| – <1 | 20.0 | |
| – 1–2 | 22.5 | |
| – 2–3 | 7.4 | |
| – 3–5 | 8.7 | |
| – 5–10 | 3.6 | |
| – 10–20 | 1.1 | |
| – >20 | 0.0 |
†
32.3% of the respondents refused to respond to questions regarding family income. 4.4% do not know their family income. The difference to reach 100% for all questions is due to answers such as “don't know” and “don't want to answer” Brazilian minimum wage in 2019 was 998.00 BRL (US$237.25) per month.
Only 0.3% of the participants reported having Chagas disease in the past and 1% reported having an individual with the disease in their home. The profile of respondents with health insurance and per capita family income below five to ten minimum wages was 34.4% and 58.6%, respectively, as shown in Table 1.
WTP for a hypothetical Chagas disease vaccine
Of the 619 study participants, 0.6% said they would not be vaccinated even if the hypothetical vaccine was free. The main reasons were efficacy (25%), safety (50%) and opposition to vaccine use (25%). After descriptive analysis of the data, seven individuals did not meet the eligibility criteria, with four opposed to vaccine use, even if available free of charge, and three individuals reporting a disposition value to pay twice their monthly family income. As a result, 612 interviewees were finally eligible to participate in the WTP study.
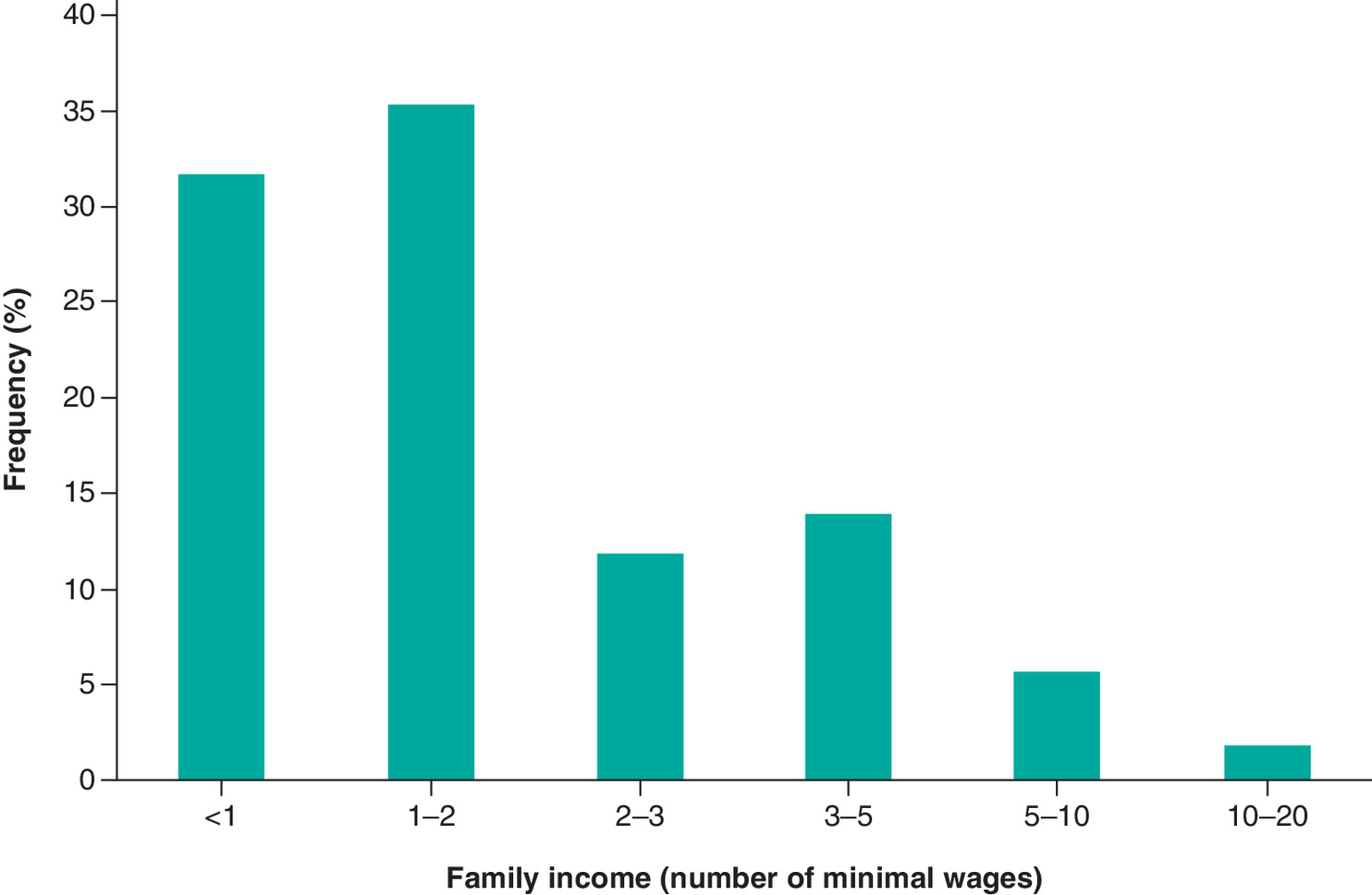
Among the 612 respondents, 43.4% were men, 61.9% had completed high school, 61.5% had children, 97.3% were working at the time of the interview, 3.6% were retired, 35.3% had health insurance and 0.3% already had Chagas disease. The percentage of participants who reported having per capita family income of up to two minimum wages was 35.2% (Figure 1).
From the application of the discrete choice technique, 91.8% of the interviewees were identified to be willing to pay some amount for the vaccine, with 69.4% of the participants willing to pay US$14.26 (R$60.00 BRL) for a single dose of this hypothetical vaccine. Of the 377 respondents who had children, 332 (54.2%) were willing to pay US$14.26 (R$60.00 BRL) to vaccinate their children. The questionnaires revealed that the percentage of respondents who were willing to pay between US$7.13 (R$30.00 BRL) and US$28.52 (R$120.00 BRL) was 43.8%. The minimum and maximum WTP for the hypothetical vaccine was US$0.00 (R$0.00 BRL) and US$475.46 (R$2,000.00 BRL).
The WTP of respondents for the hypothetical Chagas disease vaccine was estimated to be an average of US$23.77 (R$100.00 BRL). Consequently, 50% of the interviewees reported a maximum WTP of US$23.77 or less (Figure 2).
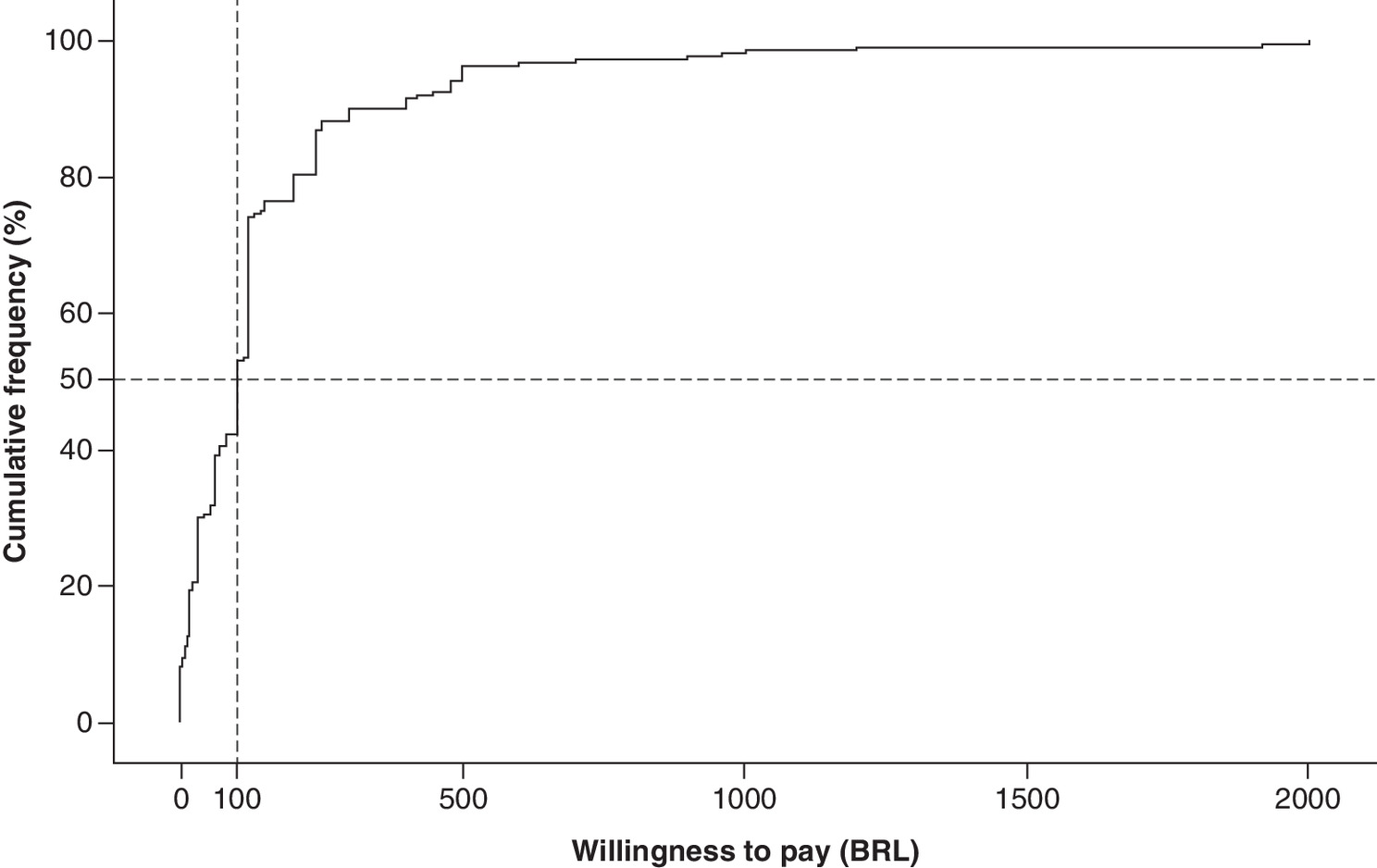
Figure 2. Cumulative percentage of the willingness to pay for a hypothetical Chagas disease vaccine according to the reported maximum values.
BRL: Brazillian real.
The following three variables presented a statistically significant relationship with the maximum value of WTP (p < 0.05): monthly per capita family income (p < 0.001), gender (p = 0.003) and education level (p < 0.001). No statistically significant relationships (p > 0.05) with the maximum WTP (i.e., health plan, age and history) for Chagas disease identified for the remaining variables (Table 2).
| Variable | WTP (US$) | WTP (BRL) | p-value |
|---|---|---|---|
| Gender | 28.52 | 120.00 | 0.003 |
| Individuals who had children | 23.77 | 100.00 | 0.551 |
| Education level | 28.52 | 120.00 | 0.000 |
| Per capita household income | 28.52 | 120.00 | 0.000 |
| Insurance health | 23.77 | 100.00 | 0.245 |
| Working at the moment of the interview | 23.77 | 100.00 | 0.991 |
2020: US$1 = R$4.2064 BRL [50].
BRL: Brazillian real; WTP: Willingness to pay.
Males (US$28.52/R$120.00 BRL) were more willing to pay for the vaccine than females (US$23.77/R$100.00 BRL), with a value p = 0.003. Additionally, individuals who declared a higher monthly per capita household income reported higher WTP values, with median values for each stratification group of US$14.26 (R$60.00 BRL), US$23.77 (R$100.00 BRL) and US$28.52 (R$120.00 BRL; Figure 3).
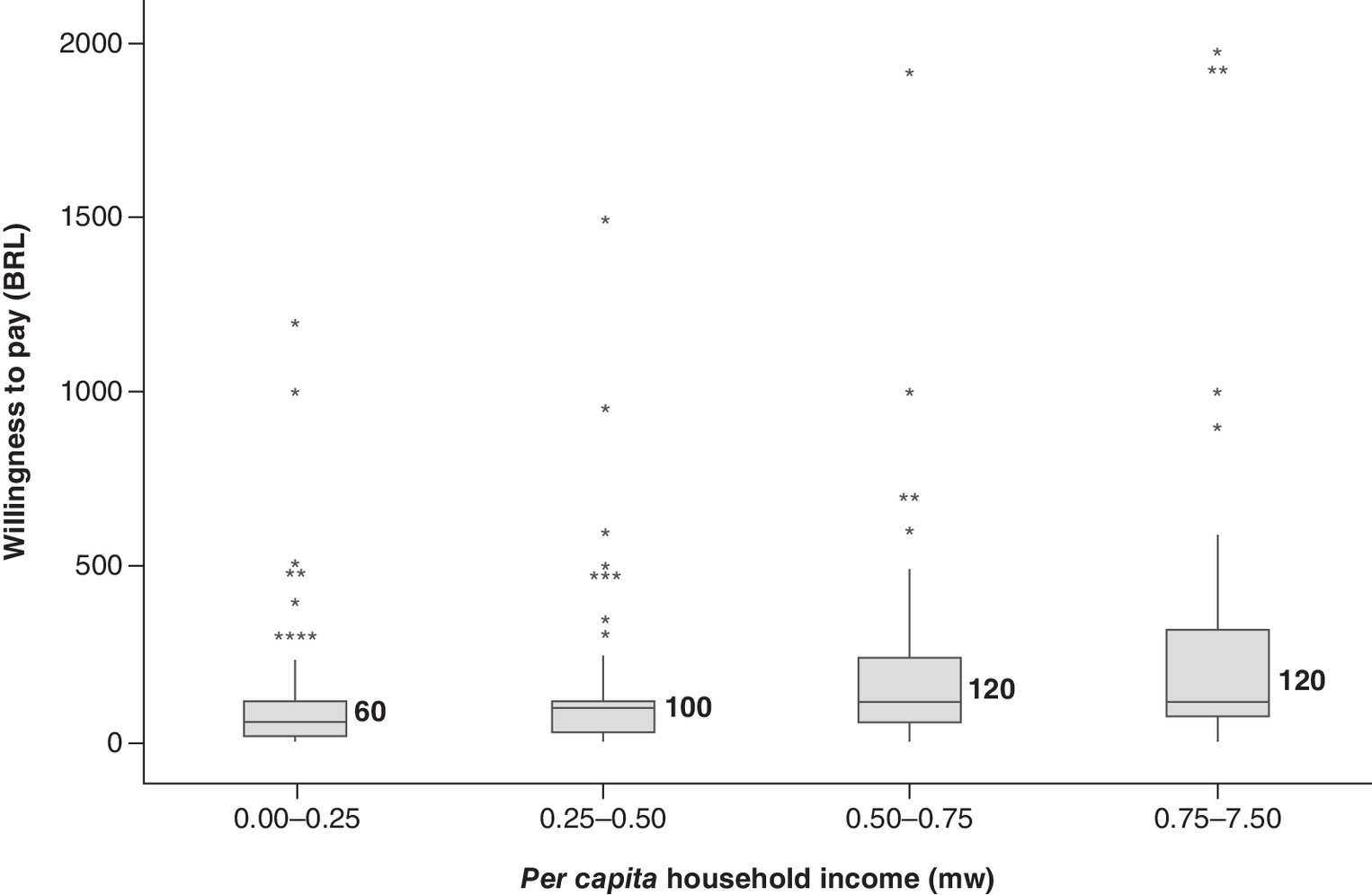
Figure 3. Box plots indicating willingness to pay for a hypothetical vaccine for Chagas according to per capita household income range.
BRL: Brazillian real; mw: Minimum wage.
As shown in Figure 4, individuals with higher educational levels declared a higher WTP for the hypothetical Chagas vaccine (p < 0.001).
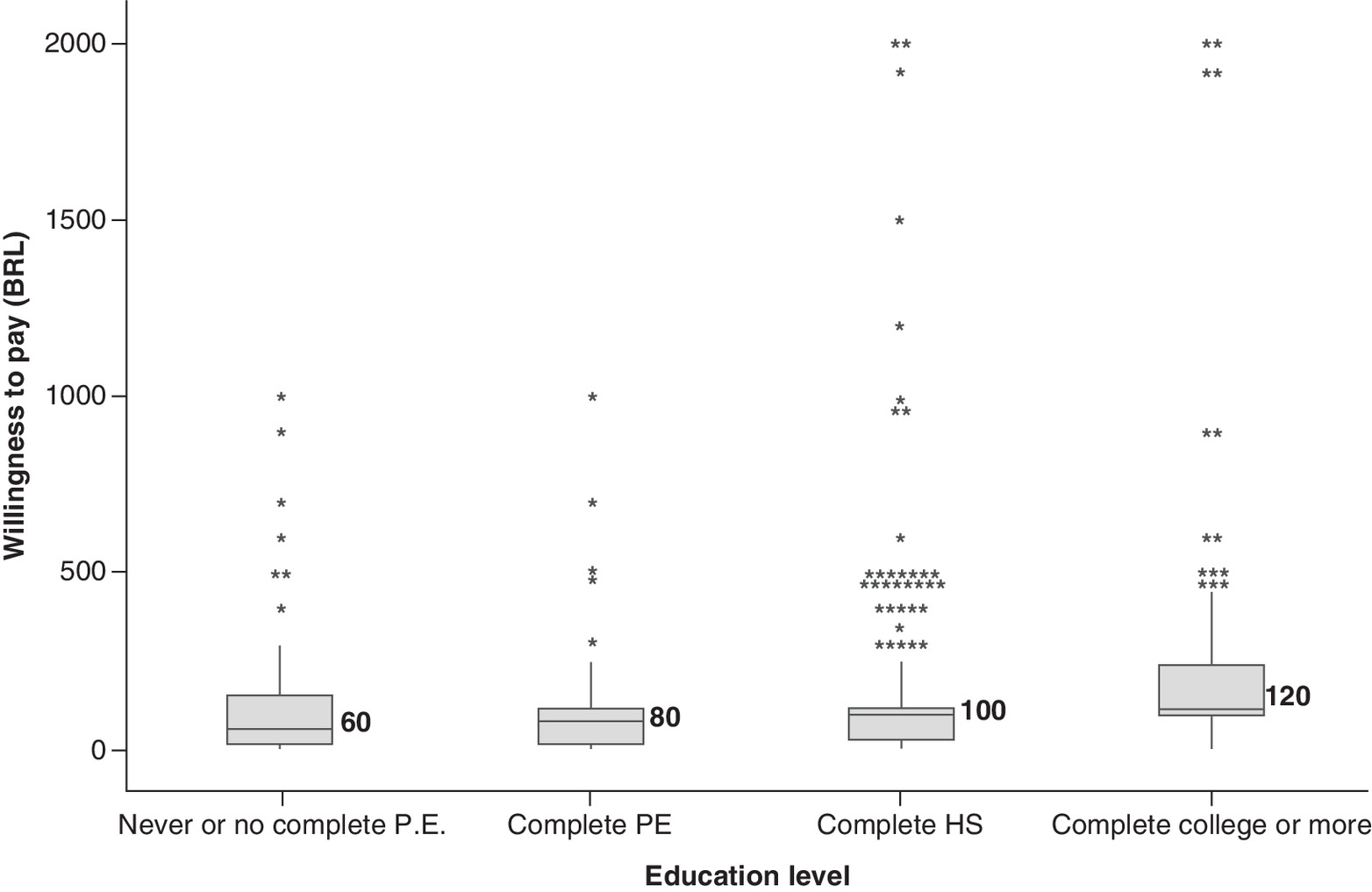
Figure 4. Box plots indicating willingness to pay for hypothetical vaccine for Chagas according to education level.
BRL: Brazillian real; HS: High school; PE: Primary education.
Discussion
This study sought to estimate the willingness of consumers in Northern Brazil to pay for a hypothetical Chagas disease vaccine. Whilst there is currently no licensed vaccine for Chagas disease; we believe in view of ongoing efforts to develop vaccines to prevent this disease, it is important to examine the WTP for a hypothetical Chagas disease vaccine to provide benchmark WTP data to help guide future decision making. A hypothetical efficacy of 80% was based on effectiveness levels of vaccines already incorporated and made available to the Brazilian population by SUS. Previous studies performed by our research group in Brazil also considered a hypothetical scenario of 80% efficacy for a vaccine to prevent chikungunya [31] and zika [30] infections. Some characteristics of the study population that are similar to the profile of the Brazilian population include the high percentage of women (51.9%), low percentage of individuals who have never studied (7.6%), and the close percentage of individuals with complete higher education (16.5%). In addition, 61.9% of the participants had completed high school resembling the largest group (complete high school or equivalent) identified in the National Household Sample Survey conducted by the Brazilian Institute of Geography and Statistics (IBGE) for the state of Pará (22.9%), Northern region (24%) and Brazil (25.2%) [51].
Further, employment was identified as the main form of financial income (72.4%), with the number of retirees being the lowest percentage (20.5%) [52]. Previous studies of WTP for hypothetical vaccines against zika [30] and chikungunya [31] in the country also reported a higher percentage of women (58.2 and 57.3%) and a reduced percentage of individuals who never studied (0.6 and 0.2%). Employment was also the main form of income (71.2 and 87.9%) and the lowest participation of interviewees who reported per capita income of 10 to 20 minimum wages (BRL) (4.3 and 8.9%) or more (0.6 and 1.8%).
In this study, the percentage of respondents who had a health plan was 35.3%, a percentage higher than the national health coverage rate (24.2%), but similar to the health coverage rate in the Metropolitan Region of the capital of Brazil (Brasília) (35.6%) [49]. According to the National Supplementary Health Agency (ANS) (2019), the number of beneficiaries of health care plans in Brazil fell by 1% in the first quarter of 2019 (47.1%) compared with the second quarter of 2018 (47.2%), with variations among regions of the country; this is because the North is responsible for 10.6% of the public of beneficiaries [49]. Notably, the private health market functions as a supplement to the Brazilian public health system while the SUS, created in 1988, is responsible for guaranteeing full, universal and free access for the Brazilian population [53].
According to data from the Notifiable Diseases Information System (SINAN), 2060 cases of Chagas disease were reported from 2008 to 2017 in the North of Brazil, including 65 in the Northeast, 29 in the Center-West, seven in the Southeast and four in the South [54]. Although, cases of Chagas disease have been identified throughout the country, the high epidemiological burden of this infection has been confirmed in the North (95%). Among the states of the region, Pará is the most affected, with, as mentioned, 83% of the national cases [6]. Based on data from 2018, approximately, 361 new cases were reported to be associated with this infection, with Pará having 275 cases [55]. Such a high number of related cases in the state is linked to the occurrence of oral transmission outbreaks [6]. This is because this region has a high consumption of regional foods such as açaí, sugarcane juice and bacaba [56–59]. Based on these findings, we believe it is important to evaluate the WTP for a hypothetical vaccine for Chagas disease initially by residents of the state of Pará in the Northern region, which comprises seven states including Amazonas, Pará, Acre, Roraima, Rondônia, Amapá and Tocantins, with Pará having the largest number of inhabitants (8,602,865) corresponding to 46.68% of the population of this region [44].
The median value of WTP for the hypothetical Chagas disease vaccine was US$23.77 (R$100.00 BRL) for a single dose. The WTP value was defined from the median of the maximum values presented by the interviewees. Notably, this criterion, which has been established in literature [30–33], is intended to avoid discrepant values from the population profile scenario of a study. As recommended in the methodological approach and adopted in our study, interviewees who presented a value of WTP twice as high as their monthly family income per capita (outliers) were excluded from our analysis, as these suggested WTP values were deemed infeasible [26].
Muniz and collaborators (2018), who employed the WTP approach as a paid strategy in Brazil, reported R$100.00 BRL/US$31.34 as the cost for a hypothetical vaccine for zika virus (80% efficacy) [30], similar to our study. Overall, compared with studies conducted for the first vaccine approved for dengue [33] (60% efficacy) and the hypothetical vaccine for the prevention of chikungunya (80% efficacy) [31], a slightly higher value of R$120.00 BRL was obtained in our study. Interestingly in a study conducted in Nigeria for three hypothetical vaccines against malaria, protozoan infection and Chagas disease [60], Udezi et al. (2010) [41] identified a WTP of US$6.77 for vaccine A (75% efficacy), $6.70 for vaccine B (85% efficacy) and US$5.06 for vaccine C (95% efficacy). Notably, WTP studies were conducted with the following scenarios: hypothetical or actual, number of doses, protection and region used. However, WTP estimates may well vary according to the income characteristics of the population [36]. Nevertheless, studies such as Lucas et al. (2007) revealed that lower WTP values of a product or service are observed when participants have more time to evaluate the product/service and this product/service is within their budget constraints [61].
Individuals with a higher per capita household income reported higher WTP (Figure 2), a result similar to that found for the WTP of hepatitis B vaccine by Sardar et al. (2018). In this study, people with higher income levels were willing to pay more for the hepatitis B vaccine in Pakistan. Such findings indicate a direct relationship between the WTP and increased income [43,62]. Based on gender, males in our study were found to be willing to pay more than females (US$28.52/R$120.00 BRL vs US$23.77/R$100.00 BRL). This is similar to the study by Sardar et al. (2018) [43] where males were also more willing to pay more than females. This may reflect the fact that wages of males are typically higher females in Brazil [63,64]. Based on these findings, the higher the income, the greater the WTP mirroring previous studies in Brazil [30,31,33]. Historically, the wage of males has been generally superior to that of females in Brazil, thereby showing a clear difference in income between genders [63,64].
Additionally, individuals with higher educational levels had a higher WTP value for the Chagas disease vaccine (Figure 3) reflecting perhaps greater knowledge about Chagas disease and its implications. This is similar to the findings of Sardar et al. (2018) [43] for a hepatitis B vaccine where there was also a higher level of schooling among the interviewees, which may contributed to their willingness to independently investigate the threats related to hepatitis B and its effects.
Encouragingly, 91.8% of the respondents agreed to pay to be vaccinated, demonstrating high acceptability. This is similar to Ughasoro et al. (2015) [37] who found that 87.5% of the respondents were willing to pay for an Ebola vaccine in Nigeria. In another study conducted by Abdulkadir et al. (2015) [65] for a malaria vaccine in Nigeria, high acceptability was also demonstrated, with 87% of the participants willing to accept the vaccine. Technologies such as vaccines are generally well accepted by the population. Accordingly, efforts and incentives applied to the development of vaccines for disease control are indispensable for public health, thereby requiring investments [66,67]. The National Immunization Program in Brazil, which is considered to be one of the largest programs in the world, is a strategy of the SUS that aims to protect the population from communicable diseases through vaccination of all age groups via annual campaigns [67].
Overall, the development of an effective vaccine against Chagas disease will be important for controlling this infection [17]. Lee et al. (2010) employed a social perspective to investigate the potential economic value of a Trypanosoma cruzi vaccine in Latin America to determine the vaccine's cost–effectiveness. The authors demonstrated that vaccination is very cost-effective in terms of price, effectiveness and risk of infection, ultimately providing cost savings and health benefits, even with a low risk of infection and vaccine efficacy. Such findings ultimately support the development of a human vaccine for Chagas disease. We believe the establishment of economic models prior to the development of a Chagas disease vaccine is advantageous and can help in the decision-making process to derive the potential health and economic benefits. Economic analysis studies help to guide investments as well as the development and implementation of potential vaccines [68].
We are aware this study had limitations. These include some interviewees' inability to understand all the information initially explained (disease, epidemiology, transmission, treatment), which could arise despite efforts to remove all doubts of the participants and ensure prior training of the interviewers. Furthermore, the hypothetical nature of the vaccine's efficacy was stressed and may not reflect reality when a new vaccine becomes available. In addition, since the socioeconomic profile of the Northern region, which is currently considered to have the greatest prevalence of Chagas disease in Brazil, differs from other regions in Brazil, this may also affect the generalizability of the findings. Despite these limitations, we believe this study has provided information that will be of benefit to both the pharmaceutical industry and the Government especially given the high prevalence rates of Chagas disease in the chosen region contributing to future discussions on prices once a vaccine is licensed.
Conclusion
Whilst the number of cases of Chagas has declined in Brazil, it remains an important public health problem in Brazil and other countries. The present study revealed the monetary value of a hypothetical Chagas vaccine at US$23.77 (R$100.00 BRL). As efforts continue in pursuit of developing vaccines against Chagas disease, economic studies with this vaccine will be important to inform future pricing and funding decisions.
Future perspective
Chagas disease will continue to pose an important challenge to health systems in endemic areas since despite efforts to control the disease through vector control. This has not been helped by accelerated urbanization and low adhesion among the population to control measures, which is likely to continue. In addition, it can be said that, although the cases of this infection have reduced in Brazil, Chagas disease remains an important public health problem with records of serious manifestations and deaths not only in Brazil but in other endemic countries, especially, in Latin America. Chagas disease affects, in general, individuals in situations of social vulnerability, such as poverty and lack adequate housing, such conditions that will still remain. This has not been helped by the invisibility of the vast majority of patients given the lack of opportunity for diagnosis, negatively impacting on the chances to success with treatment. In this scenario, the search for a safe, effective and cost-effective Chagas disease vaccines continue to represent an important strategy to control this infection. It is anticipated that during the next 5 years, more advances will be made with vaccine development building on those of Villanueva-Lizama and collaborators [16]. Concerns with the impact of Chagas disease on cardiomyopathy leading to events such as heart failure, arrhythmias, thromboembolism, stroke and sudden death, reinforce the need for vaccines with adequate safety and efficacy. In this context, we recommend that the search for a vaccine and a price based on the profile of consumers continue. In this respect, we continue to support more efforts and government investments from the most affected countries and companies to encourage the development of medicines and vaccines for Chagas disease. This is the first study conducted in the context of the WTP for a hypothetical Chagas disease vaccine, and can contribute to decision-making about potential prices for a future vaccine once it becomes available in Brazil, as well in the discussions in other endemic countries.
•
Chagas disease is a serious public health problem, with around 70 million people at risk of developing the infection worldwide.
•
Endemic in 21 countries in Latin America. It represents one of the four leading causes of death from infectious and parasitic diseases in Brazil.
•
Currently there is no effective vaccine against Chagas disease; however, this could represent an important strategy for controlling the disease.
•
This study cross-sectional estimated the willingness to pay (WTP) of Brazilian respondents for a hypothetical Chagas disease vaccine using a contingent valuation method.
•
A total of 50% of the interviewees, residents in the Northern of Brazil, were willing to pay US$23.77 (100.00 BRL) for a hypothetical vaccine against Chagas disease.
•
The continued occurrence of Chagas disease infection in endemic regions, reinforces the need research into the development of effective and safe vaccines, as well economic studies to contribute to subsequent discussions regarding potential pricing and funding for new vaccines associated to its prevention.
•
Overall, this study can contribute to decision-making about potential prices for a Chagas disease vaccine once it becomes available in Brazil.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (suppl_file.pdf)
- Download
- 108.79 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
OPAS. Tropical Diseases (2018). www.paho.org/bra/index.php?option=com_joomlabook&view=topic&id=57&ite.mid=232
2.
Brasil. Doenças Negligenciadas (2013). https://agencia.fiocruz.br/doenças-negligenciadas
3.
Drugs for Neglected Diseases Initiative. Neglected Patients (2019). www.dndial.org/
4.
Fundação Oswaldo Cruz. Conheça as principais doenças tropicais negligenciadas (2012). www.fiocruz.br/ioc/cgi/cgilua.exe/sys/start.htm?infoid=1585&sid=32
5.
Albuquerque MAC, Dias DM, Vieira LT, Lima CA, da Silva AM. Mortality Trends for Neglected Tropical Diseases in the State of Sergipe, Brazil, 1980–2013. Infect. Dis. Poverty 6(1), 20 (2017).
6.
Brasil. Doença de Chagas: o que é, causas, sintomas, tratamento e prevenção (2020). https://saude.gov.br/saude-de-a-z/doenca-de-chagas
7.
Lidani KCF, Andrade FA, Bavia L, Damasceno FS, Beltrame MH, Messias-Reason IJ, Sandri TL. Chagas disease: from discovery to a global health problem. Front. Public Health 7, 166 (2019).
• Important to complement our knowledge of Chagas disease.
8.
OPAS. Paraguay interrupts Chagas disease transmission at home (2018). www.paho.org/bra/index.php?option=com_content&view=article&id=5736:paraguai-interrompe-transmissao-vetorial-domiciliar-de-doenca-de-chagas&Itemid=812
9.
Drugs for Neglected Dieseases Initiative. Chagas disease (2019). www.dndial.org/doencas/doenca-chagas/
• Important to complement our knowledge of Chagas disease.
10.
Pérez-Molina JA, Molina I. Chagas disease. Lancet 391(10115), 82–94 (2018).
•• Important to complement our knowledge of Chagas disease.
11.
Fundação Oswaldo Cruz. Conheça as principais doenças tropicais negligenciadas, Doença de Chagas (2012). www.fiocruz.br/ioc/cgi/cgilua.exe/sys/start.htm?infoid=1585&sid=32
12.
Tzizik DM, Borchardt RA. Chagas disease: an under-recognized diagnosis. JAAPA 31(12), 30–33 (2018).
13.
Sala de Apoio a Gestão Estratégica. Número de óbitos por doenças infecciosas e parasitárias (2018). https://sage.saude.gov.br/#
14.
Jones K, Versteeg L, Damania A et al. Vaccine-linked chemotherapy improves benznidazole efficacy for acute Chagas disease. Infect Immun. 86(4), e00876–17 (2018).
15.
Beaumier CM, Gillespie PM, Strych U, Hayward T, Hotez PJ, Bottazzi ME. Status of vaccine research and development of vaccines for Chagas disease. Vaccine 34(26), 2996–3000 (2016).
• Important reference source associated with the development of vaccines for Chagas disease.
16.
Villanueva-Lizama LE, Cruz-Chan JV, Aguilar-Cetina ADC et al. Trypanosoma cruzi vaccine candidate antigens Tc24 and TSA-1 recall memory immune response associated with HLA-A and -B supertypes in Chagasic chronic patients from Mexico. PLOS Neglect. Trop. Dis. 12(1), e0006240 (2018).
• Important reference source associated with the development of vaccines for Chagas disease.
17.
Rodríguez-Morales O, Monteón-Padilla V, Carrillo-Sánchez SC et al. Experimental vaccines against Chagas disease: a journey through history. J. Immunol. Res. 2015, 489758 (2015).
18.
Gupta S, Garg NJ. A Two-component DNA-prime/protein-boost vaccination strategy for eliciting long-term, protective T cell immunity against Trypanosoma cruzi. PLoS Pathog. 11(5), e1004828 (2015).
19.
Gupta S, Salgado-Jiménez B, Lokugamage N, Vázquez-Chagoyán JC, Garg NJ. TcG2/TcG4 DNA vaccine induces Th1 immunity against acute Trypanosoma cruzi infection: adjuvant and antigenic effects of heterologous T. rangeli booster immunization. Front. Immunol. 10, 1456 (2019).
20.
Barry MA, Versteeg L, Wang Q et al. A therapeutic vaccine prototype induces protective immunity and reduces cardiac fibrosis in a mouse model of chronic Trypanosoma cruzi infection. PLoS Negl. Trop. Dis. 13(5), e0007413 (2019).
21.
Brasil. Câmara de Regulação do Mercado de Medicamentos (CMED) (2020). http://portal.anvisa.gov.br/cmed
22.
Brasil. Registros de novos medicamentos: saiba o que é preciso (2020). http://portal.anvisa.gov.br/noticias/-/asset_publisher/FXrpx9qY7FbU/content/registro-de-novos-medicamentos-saiba-o-que-e-preciso/219201
23.
Brasil. Resolução CMED n° 2, de 5 de março de 2004 (2004). http://portal.anvisa.gov.br/documents/374947/2932039/Resolu%C3%A7%C3%A3o+n%C2%BA+2%2C+de+5+de+mar%C3%A7o+de+2004.pdf/d50ebc85-5971-4981-bd16-b619780e6df5
24.
Brasil. Comissão Nacional de Incorporação de Tecnologias no Sistema Único de Saúde (CONITEC), a comissão (2020). http://conitec.gov.br/entenda-a-conitec-2
25.
Machado CV, Lima LD, Baptista TWF. Health policies in Brazil in contradictory times: paths and stumbling blocks in the construction of a universal system. Rep. Public Health 33(Suppl. 2), e00129616 (2017).
26.
Oliveira GLA, Guerra Junior AA, Godman B, Acurcio FA. Cost–effectiveness of vildagliptin for people with type 2 diabetes mellitus in Brazil; findings and implications. Expert Rev. Pharmacoecon. Outcomes Res. 17(2), 109–119 (2017).
27.
Lemos LLP, Guerra Júnior AA, Santos M et al. The assessment for disinvestment of intramuscular interferon Beta for relapsing-remitting multiple sclerosis in Brazil. PharmacoEconomics 36(2), 161–173 (2018).
28.
Instituto Brasileiro de Geografia e Estatística. População (2020). www.ibge.gov.br/apps/populacao/projecao/index.html?utm_source=portal&utm_medium=popclock&utm_campaign=novo_popclock
29.
Mould Quevedo JF, Hernández IC, Espinosa JG, Escudero GS. The willingness-to-pay concept in question. Public Health J. 43(2), 352–358 (2009).
• Important to complement our knowledge of willingness to pay (WTP) approach.
30.
Muniz Júnior RL, Godói IP, Reis EA et al. Consumer willingness to pay for a hypothetical Zika vaccine in Brazil and the implications. Expert Rev. Pharmacoecon. Outcomes Res. 19(4), 473–482 (2019).
• Important to complement our knowledge of WTP approach.
31.
Sarmento TTR, Godói IP, Reis EA, Godman B, Ruas CM. Consumer willingness to pay for a hypothetical chikungunya vaccine in Brazil and the implications. Expert Rev. Pharmacoecon. Outcomes Res. (2019).
•• Important to complement our knowledge of WTP approach.
32.
Haab TC, McConnell KE. Valuing Environmental and Natural Resources. Edward Elgar Publishing Limited, UK (2002).
•• Important to complement our knowledge of WTP approach.
33.
Godói IP, Santos AS, Reis EA et al. Consumer willingness to pay for Dengue vaccine (CYD-TDV, Dengvaxia®) in Brazil; implications for future pricing considerations. Front. Pharmacol. 8, 41 (2017).
34.
Palanca-tan R. The demand for a dengue vaccine: a contingent valuation survey in Metro Manila. Vaccine 26(7), 914–923 (2008).
35.
Hadisoemarto PF, Castro MC. Public acceptance and willingness-to-pay for a future dengue vaccine: a community-based survey in Bandung, Indonesia. PLoS Negl. Trop. Dis. 7(9), e2427 (2013).
36.
Lee JS, Mogasale V, Lim JK et al. A multi-country study of the household willingness-to-pay for Dengue vaccines: household surveys in Vietnam, Thailand, and Colombia. PLoS Negl. Trop. Dis. 9(6), e0003886 (2015).
37.
Ughasoro MD, Esangbedo DO, Tagbo BN, Mejeha IC. Acceptability and willingness-to-pay for a hypothetical Ebola virus vaccine in Nigeria. PLOS Negl. Trop. Dis. 9(6), e0003838 (2015).
38.
Cameron MP, Newman PA, Roungprakhon S, Scarpa R. The marginal willingness-to-pay for attributes of a hypothetical HIV vaccine. Vaccine 31(36), 3712–3717 (2013).
39.
Morey ER, Sharma VR, Mills A. Willingness to pay and determinants of choice for improved malaria treatment in rural Nepal. Soc. Sci. Med. 57(1), 155–165 (2003).
40.
Jimoh A, Sofola O, Petu A, Okorosobo T. Quantifying the economic burden of malaria in Nigeria using the willingness to pay approach. Cost. Eff. Resour. Alloc. 5(6), 1478–7547 (2007).
41.
Udezi WA, Usifoh CO, Ihimekpen OO. Willingness to pay for three hypothetical malaria vaccines in Nigeria. Clin. Therapeut. 32(8), 1533–1544 (2010).
42.
Tawiah T, Malam K, Kwarteng A et al. Improving the first-line treatment of febrile illnesses in Ghana: willingness to pay for malaria rapid diagnostic tests at licensed chemical shops in the Kintampo area. Cost Eff. Resour. Alloc. 16, 4 (2018).
43.
Sadar A, Muhammad RY, Azhar A, Waqas M, Gill BA. Willingness to pay for vaccination against hepatitis b and its determinants: the case study of an industrial district of Pakistan. Epidemiol. Biostat. Public Health 15, 4 (2018).
44.
Instituto Brasileiro de Geografia e Estatística. Estimativas da população residente com data de referência em 1° de julho de 2019 (2019). https://central3.to.gov.br/arquivo/461424/
45.
Atlas de desenvolvimento humano no Brasil. Perfil (2013). www.atlasbrasil.org.br/2013/pt/perfil
46.
Instituto Brasileiro de Geografia e Estatística. Cidades e Estados (2020). www.ibge.gov.br/cidades-e-estado/pa/belem.html
47.
Brasil. IBGE divulga o rendimento domiciliar per capita 2018 (2018). https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/23852-ibge-divulga-o-rendimento-domiciliar-per-capita-2018
48.
Brasil. Preços máximos de medicamentos por Princípio Ativo (2016). http://portal.anvisa.gov.br/documents/374947/2829072/LISTA+CONFORMIDADE_201606-20.pdf/af0a54e7-249d-4855-ba9a-419f73249967
49.
Brasil. Cadernos de Informações da Saúde Suplementar – Beneficiários, Operadoras e Planos (2014). www.ans.gov.br/images/stories/Materiais_para_pesquisa/Perfil_setor/Caderno_informacao_saude_suplementar/2014_mes06_caderno_informacao.pdf
50.
Brasil. Banco Central do Brasil. Conversor de Moedas (2020). www.bcb.gov.br/conversao
51.
Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional por Amostra de Domicílios Continua Trimestral, população por níveis de instrução (2019). https://sidra.ibge.gov.br/tabela/5919
52.
Instituto Brasileiro de Geografia e Estatística. Síntese de Indicadores Sociais: Uma Análise das Condições de vida da População Brasileira (2019). https://biblioteca.ibge.gov.br/visualizacao/livros/liv101678.pdf
53.
Brasil. Sistema Único de Saúde (SUS): estrutura, princípios e como funciona (2020). www.saude.gov.br/sistema-unico-de-saude
54.
Sistema de Informação de Agravos de Notificação (SINAN). Distribuição dos Casos de Doença de Chagas Aguda, segundo UF de residência, 2008 a 2017 (2017). www.saude.gov.br/images/pdf/2019/julho/26/CASOS-AGUDOS-CONFIRMADOS-NO-SINAN-POR-UF-DE-RESID--NCIA--2008-A-2017-.pdf
•• Important reference source associated with the epidemiological scenario of Chagas disease in Brazil.
55.
Brasil. Doença de Chagas Aguda (2020). www2.datasus.gov.br/DATASUS/index.php?area=0203&id=29890013&VObj=http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sinannet/cnv/chagas
•• Important reference source associated with the epidemiological scenario of Chagas disease in Brazil.
56.
Shikanai-Yasuda MA, Carvalho NB. Oral transmission of Chagas disease. Clin. Infect. Dis. 54(6), 845–852 (2012).
57.
Barbosa RL, Dias VL, Pereira KS et al. Survival in vitro and virulence of Trypanosoma cruzi in açaí pulp in experimental acute Chagas disease. J. Food Prot. 75(3), 601–606 (2012).
• Important reference source associated with the scenario of Chagas disease in the Northern of Brazil.
58.
Dias JC, Ramos AN Jr, Gontijo ED et al. II Brazilian Consensus on Chagas Disease, 2015. Epidemiol. Health Serv. 25(spe), 7–86 (2016).
• Important reference source associated with the scenario of Chagas disease in Brazil.
59.
Santos VRCD, Meis J, Savino W et al. Acute Chagas disease in the state of Pará, Amazon Region: is it increasing? Mem. Inst. Oswaldo Cruz 113(5), e170298 (2018).
60.
Brasil. Malária: o que é, causas, sintomas, tratamento, diagnóstico e prevenção (2020). https://saude.gov.br/saude-de-a-z/malaria
61.
Lucas ME, Jeuland M, Deen J et al. Private demand for cholera vaccines in Beira, Mozambique. Vaccine 25(14), 2599–2609 (2007).
62.
Kim D, Canh DG, Poulos C et al. Private demand for cholera vaccines in Hue, Vietnam. Value Health 11(1), 119–128 (2008).
63.
Giuberti AC, Menezes-Filho N. Discrimination of income by gender: a comparison between Brazil and the United States. App. Econ. 9(3), 369–384 (2005).
64.
Gomes MR, Souza SCI. Gender wage asymmetries and the regional approach in Brazil: an analysis according to admission to employment and sectors of activity. Cont. Econ. Mag. 22, 3 (2018).
65.
Abdulkadir BI, Ajayi IO. Willingness to accept malaria vaccine among caregivers of children under 5 in the local government area of Ibadan North, Nigeria. Malaria World J. 6, 2 (2015).
66.
Fundação Oswaldo Cruz. Vacinas (2017). http://chagas.fiocruz.br/vacinas/
67.
Brasil. Sobre o programa (2020). www.saude.gov.br/saude-de-a-z/vacinacao/sobre-o-programa/
68.
Lee BY, Bacon KM, Connor DL, Willig AM, Bailey RR. The potential economic value of a Trypanosoma cruzi (Chagas disease) vaccine in Latin America. PLoS Negl. Trop. Dis. 4(12), e916 (2010).
•• Important to complement our knowledge of economic value of a vaccine in Latin America.
Information & Authors
Information
Published In
Pages: 659 - 672
PubMed: 33851872
Copyright
© 2021 Future Medicine Ltd.
History
Received: 4 November 2020
Accepted: 12 March 2021
Published online: 14 April 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Consumer willingness to pay for a hypothetical Chagas disease vaccine in Brazil: a cross-sectional study and the implications. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0241
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ana Cristina de Oliveira Pereira, José Duanne Benevides de Lima, Thais Miranda de Castro, Maria Áurea Catarina Passos Lopes, Mariana Alves Benigno, Rosilene Nascimento da Silva Xavier, Marina Layara Sindeaux Benevides, NEGLIGÊNCIA DAS POLÍTICAS PÚBLICAS RELACIONADAS À DOENÇA DE CHAGAS NO BRASIL: REVISÃO DE ESCOPO, RECIMA21 - Revista Científica Multidisciplinar - ISSN 2675-6218, 10.47820/recima21.v7i4.7476, 7, 4, (e747476), (2026).
- Vinícius Gonçalves Nogueira, Edna Afonso Reis, Brian Godman, Antony Paul Martin, Isabella Piassi Dias Godói, Acceptability and willingness to pay for a hypothetical HIV vaccine in Brazil and the implications: a cross-sectional study, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2024.2384543, 25, 1, (91-100), (2024).
- Francesco Ramponi, Céline Aerts, Paula Sartor, María Jesús Pinazo, Héctor Freilij, Carlos A. Guzmán, Emilio Malchiodi, Elisa Sicuri, Development of vaccines for Chagas disease (CRUZIVAX): stakeholders’ preferences and potential impacts on healthcare, Gaceta Sanitaria, 10.1016/j.gaceta.2022.102275, 37, (102275), (2023).
- Brian Godman, Joseph Fadare, Hye-Young Kwon, Carolina Zampirolli Dias, Amanj Kurdi, Isabella Piassi Dias Godói, Dan Kibuule, Iris Hoxha, Sylvia Opanga, Zikria Saleem, Tomasz Bochenek, Vanda Marković-Peković, Ileana Mardare, Aubrey C Kalungia, Stephen Campbell, Eleonora Allocati, Alice Pisana, Antony P Martin , Johanna C Meyer, Evidence-based public policy making for medicines across countries: findings and implications for the future, Journal of Comparative Effectiveness Research, 10.2217/cer-2020-0273, 10, 12, (1019-1052), (2021).
- Isabella Piassi Dias-Godói, Túlio Tadeu Rocha Sarmento, Edna Afonso Reis, Ludmila Peres Gargano, Brian Godman, Francisco de Assis Acurcio, Juliana Alvares-Teodoro, Augusto Afonso Guerra Júnior, Cristina Mariano Ruas, Acceptability and willingness to pay for a hypothetical vaccine against SARS CoV-2 by the Brazilian consumer: a cross-sectional study and the implications, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2021.1931128, 22, 1, (119-129), (2021).