Shifting demographics and comorbidity burden in adult Chinese urban patients with chronic hepatitis B, 2013 and 2016
Publication: Journal of Comparative Effectiveness Research
Abstract
Chronic hepatitis B demographics and comorbidity data are limited in China. Materials & methods: The China Health Insurance Association claims database from 2013 and 2016 was used to augment the existing data: the proportion of patients aged >45 years increased significantly from 40.3% in 2013 to 49% in 2016 (p < 0.001). Results: Significant increases in multiple comorbidities were observed, including hypertension (9.4–14.5%), hyperlipidemia (4.7–7.0%) and cardiovascular disease (5.7–10%; p < 0.001 for all comparisons). Increases were observed in renal impairment (8.8–10.0%; p < 0.001) and osteoporosis and/or pathologic nontraumatic bone fracture (3.8–7.3%; p < 0.001). Conclusion: Careful selection of treatment options and comorbidity monitoring should be considered when managing adult Chinese patients with chronic hepatitis B.
Worldwide estimates suggest that approximately 250 million individuals have chronic hepatitis B (CHB), and approximately 650,000 die of associated hepatic failure, liver cirrhosis and/or hepatocellular carcinoma (HCC) each year [1,2]. Nearly a third of the global population with CHB live in China, of whom 28 million require treatment and 7 million require immediate treatment due to advanced liver disease and a high risk for developing liver cancer [3,4]. The introduction of a universal vaccine program in China led to a gradual reduction in the prevalence of hepatitis B virus (HBV) carriers from 9.8% in 1992 to 6.1% in 2007–2013 [5,6]. Nevertheless, CHB continues to be endemic in China, imposing the highest disease burden associated with a communicable disease in China, with some estimates suggesting that about 10 million patients with CHB will die by 2030 [4,7].
Treatment for CHB, which may be lifelong, is directed at improving quality of life and survival by maximally suppressing HBV replication in a sustained manner [8]. Appropriate treatment of CHB reduces hepatic inflammation and fibrosis, decreases risk for hepatic failure, slows progression of hepatic decompensation, and reduces the incidence of HCC. Treatment is evolving, and a number of therapies with a high genetic barrier to resistance have been introduced worldwide, including entecavir, available since 2006, and tenofovir disoproxil fumarate since 2008; in late 2018, tenofovir alafenamide, a novel, targeted prodrug of tenofovir, was approved by the China National Medical Products Administration.
In patients with CHB, infection and the resulting liver complications are superimposed over a range of liver-related and nonliver comorbidities that vary in relationship to the underlying infection, and – as in most chronic diseases – these comorbidities accumulate and worsen as patients age. These comorbidities and the concomitant medications used to treat them, have the potential to complicate both the initial selection of appropriate nucleotide/nucleoside analog (NA) therapy as well as ongoing treatment for CHB, and it is thus important to understand the changing regional demographics and clinical characteristics of patients with CHB. It is clear from other studies conducted outside of China that the demographics of the CHB population are shifting substantially, becoming not only older overall, but also subject to a dramatically higher comorbidity burden over time [9].
The characteristics of the Chinese population with HBV are important to understand, particularly because these populations are aging and accumulating comorbidities that may require concomitant treatment. The present study, which leverages data from the China Health Insurance Research Association (CHIRA) annual urban claims database to identify patients with CHB, is the first to provide an assessment of demographic and comorbidity trends in this important population.
Materials & methods
Study objective
This was a retrospective, cross-sectional analysis of the CHIRA annual urban claims databases from 2013 and 2016. The primary objective was to describe the time trend of demographic characteristics and the comorbidity profile among adult CHB patients in China. The research protocol for this study was reviewed and approved by CHIRA.
Database description
The CHIRA annual claims database is generated yearly by randomly selecting 2% of adult urban worker and resident claimants living in national cities (including Beijing, Shanghai, Tianjin and Chongqing) or provincial capital cities, and 5% of claimants living in regional cities in 32 Chinese provinces, and extracting their claims records for the year. In total, data from 90 cities were included in this analysis. The created annual claims database consisted of two datasets: a general dataset that contained demographic information (age, sex and residence), insurance type (urban workers or residents), healthcare settings (hospital tier rank, which ranges from I to III; the higher hospital rank, the larger hospital scale), diagnosis, and medical costs associated with claims and a transaction dataset that consisted of claims records for drug prescriptions, laboratory tests, image tests and other healthcare resources associated with each insurance claim. There are three types of public health insurances in China that together cover at least 95% of the Chinese population [10]: the Urban Employee Basic Medical Insurance (UEBMI), the Urban Resident Basic Medical Insurance (URBMI) and the New Rural Cooperative Medical Scheme (NRCMS). The UEBMI covers urban employees and the URBMI covers those who are not employed (young children, students and nonworking adult urban residents). Once an enrollee has been covered by the UEBMI for >15 years, they will be covered by the same medical insurance for their entire life. In 2011, the UEBMI had 252 million enrollees, the URBMI had 221 million enrollees and the NRCMS had 832 million enrollees [11]. We based the analysis on the UEBMI and URBMI, similar to several published analyses of the CHIRA database [12–14].
Identification of patients with CHB
The diagnosis information in the 2013 and 2016 CHIRA annual claims databases was recorded in Chinese. To facilitate the patient identification and extraction of comorbidity information, this study pooled the diagnosis information contained in the two claims databases and removed the Chinese medicine diagnosis names. The uncoded diagnosis information was then translated to the Chinese version of the International Classification of Diseases, tenth revision (ICD-10) codes published by the Health Ministry of the People’s Republic of China. Duplicated diagnosis codes associated with the same claimants was removed. After conversion to ICD-10, diagnosis codes were assigned to the claimants to create diagnosis datasets for the calendar years of 2013 and 2016, respectively. The two diagnosis datasets were further used to identify patients with CHB using the ICD-10 code for CHB (B18.1). The two diagnosis datasets were also the data source used to identify any comorbidities associated with included CHB patients in this study. This analysis also excluded patients aged <18 years and patients who only had diagnosis information for CHB from pharmacy store claims records, which were deemed insufficiently accurate to determine diagnoses with confidence.
Data extraction
Claims records associated with CHB were extracted to create a study dataset that included patient demographics, converted ICD-10 diagnosis codes, and prescriptions for NAs for the 2013 and 2016 cohorts. Extracted diagnostic codes were cleaned by removing duplications and categorized according to selected common comorbidities in patients with chronic HBV. Liver-related comorbidities were defined according to the ICD-10 codes for cirrhosis, decompensated liver failure, portal hypertension, esophageal varices, ascites, gastrointestinal bleeding, jaundice, HCC and liver transplantation. Renal comorbidities were defined according to ICD-10 codes for chronic kidney disease (CKD), end-stage renal disease, dialysis, chronic pyelonephritis, glomerulonephritis, nephrolithiasis, nephropathy, renal osteodystrophy, proteinuria and renal insufficiency. Diseases related to bone density were defined according to ICD-10 codes for osteoporosis, osteopenia, osteomalacia, bone fracture related to osteoporosis and any ICD-10 codes indicating fracture but not falling into the injury-related fracture categories. Additional comorbidities assessed in this study are listed in Supplementary Table 1. The prescription records associated with the included CHB patients were screened using the generic names of NAs that were approved before 2017 in China for their NA treatment status. These NAs included lamivudine, adefovir, telbivudine, entecavir and tenofovir disoproxil fumarate, which were indicated for treatment of CHB in these patients from the CHIRA database.
Statistical analyses
Continuous variables were summarized with means and standard deviations. Other patient demographic characteristics, comorbidities, NA treatments and liver-related complications were summarized using percentages for distributions. Patient characteristics in the 2013 and 2016 datasets were compared for changes in demographics, comorbidities, NA treatments and liver-related complications. Age group distribution (≥18 to <35 years, ≥35 to <45 years, ≥45 to <55 years, ≥55 to <65 years and ≥65 years) was also evaluated. Analyses used both student’s t-test for continuous variables and the chi-square test for categorical variables. The statistical significance in these comparisons was defined as a two-sided p-value <0.05. All analyses were conducted using the statistical software R, R3.4.0 (R core team, April 2017).
Results
Study population
A total of 15,218 patients from the 2013 dataset and 11,757 patients from the 2016 dataset were identified based on an ICD-10 code indicating a diagnosis of CHB (Figure 1). After excluding claimants identified from pharmacy records as those aged <18 years or for whom an age was not recorded, there were 14,545 patients in the 2013 dataset and 11,648 in the 2016 dataset. The proportion of patients with an ICD-10 code denoting CHB diagnosis decreased from 0.23 to 0.14% in the urban CHIRA database (Figure 1).
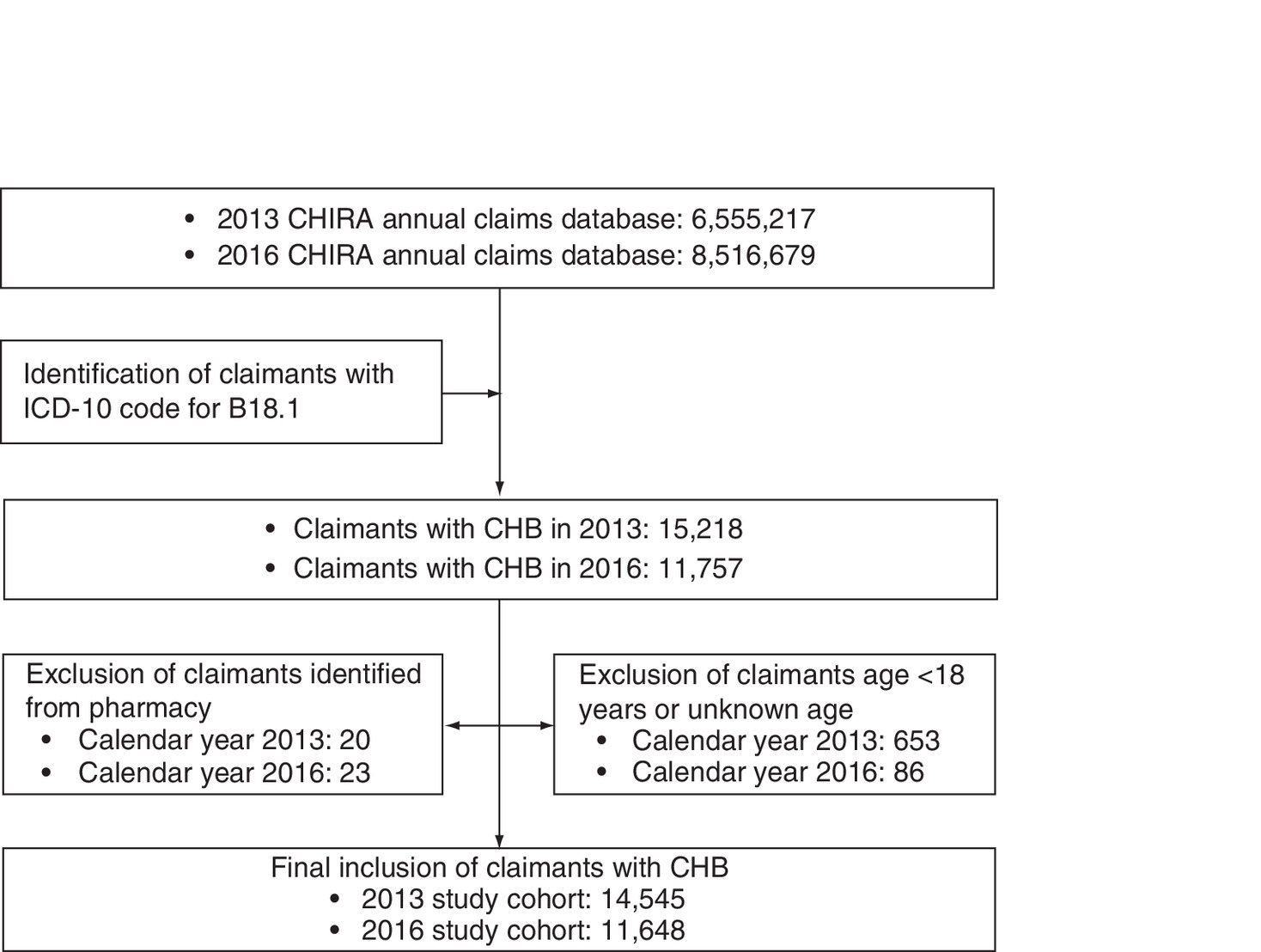
Figure 1. Workflow diagram showing the process in the derivation of the study populations for analysis.
CHB: Chronic hepatitis B; CHIRA: China Health Insurance Research Association; ICD-10: International Classification of Diseases, tenth revision.
Demographics
Age pyramids with the various age groups were created for the 2013 and 2016 cohorts (Figure 2). Age pyramids reflecting the general Chinese population during 2013 and 2016 were also obtained (Figure 2) [15,16]. Between 2013 and 2016, the mean age of urban Chinese patients with CHB increased from 42.4 ± 14.2 years to 45.6 ± 14.0 years (p < 0.001). There was a significant increase in the proportion of patients aged ≥35 years (63.5 vs 73.9%; p < 0.001) and ≥45 years (40.3 vs 49.0%; p < 0.001) from 2013 to 2016 (Figure 2). The percentage of individuals aged ≥45 years also increased in the general Chinese population from 42.6% in 2013 to 46.9% in 2016 (Figure 2). Similar trends in mean age were observed for both male and female CHB patients. The proportions of male patients increased significantly between 2013 and 2016 (15.0 vs 29.4%; p < 0.001; Table 1) and there were also increases in the percentage of patients living in national cities (15.0 vs 29.4%; p < 0.001). The percentage of patients treated at top-ranked (tier 3) hospitals declined significantly from 86.8–69.8% (p < 0.001). In contrast to the general Chinese population where the ratio of males to females was close to 1.0 in all age groups, among CHB patients in the CHIRA database ≥45 years old, the ratio was 1.8 in 2013 and 2016 (Figure 2).
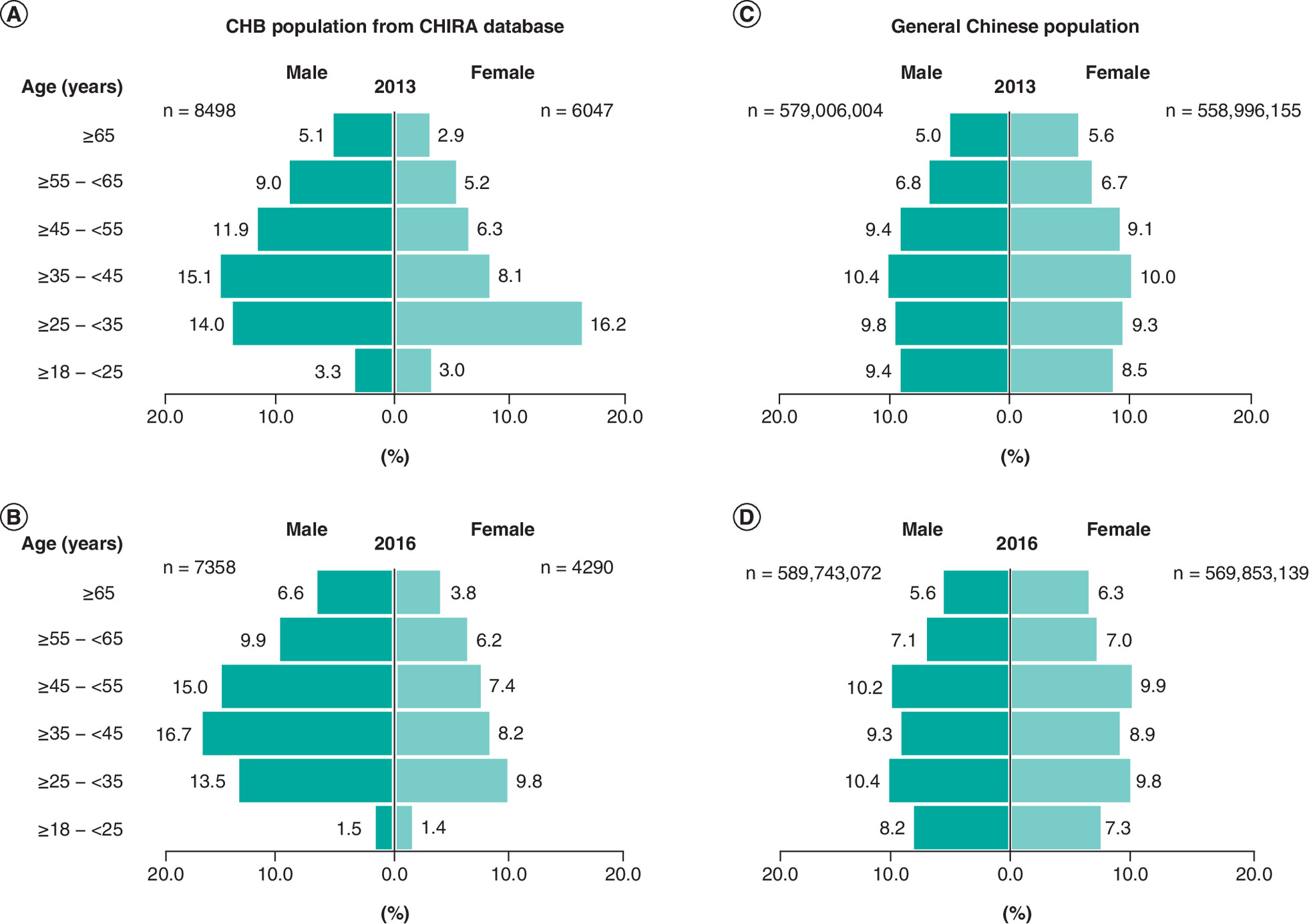
Figure 2. Age pyramid distribution of the 2013 & 2016 chronic hepatitis B cohorts.
(A) Male (n = 8498) and female (n = 6047) adult urban CHB patients from 2013. (B) Male (n = 7358) and female (n = 4290) adult urban CHB patients from 2016. Age pyramid distribution of the general Chinese population, excluding data from people <15 years of age. (C) Male (n = 579,006,004) and female (n = 558,996,155) age distributions for 2013. (D) Male (n = 589,743,072) and female (n = 569,853,139) age distributions for 2016. Data provided from PopulationPyramid.net under Creative Commons License CC-BY-3.0.
CHB: Chronic hepatitis B.
| Patient demographics | 2013 Cohort (n = 14,545) | 2016 Cohort (n = 11,648) | p-value |
|---|---|---|---|
| Mean age, years (SD) | 42.4 (14.2) | 45.6 (14.0) | <0.001 |
| Male sex (%) | 58.4% | 63.2% | <0.001 |
| Insurance plan | |||
| – Employee | 86.8% | 87.6% | 0.077 |
| – Resident | 13.2% | 12.4% | 0.077 |
| Residence city level | |||
| – National | 15.0% | 29.4% | <0.001 |
| – Provincial | 43.7% | 38.4% | <0.001 |
| – Regional | 41.3% | 32.2% | <0.001 |
| Medical setting | |||
| – Tier I hospital | 10.1% | 12.9% | <0.001 |
| – Tier II hospital | 30.9% | 36.9% | <0.001 |
| – Tier III hospital | 86.8% | 69.8% | <0.001 |
| – Community hospital | 16.1% | 25.3% | <0.001 |
| – Outpatient clinics | 7.4% | 6.6% | 0.019 |
| – Pharmacy store | 8.7% | 12.8% | <0.001 |
| – Not reported | 0.2% | 12.0% | <0.001 |
SD: Standard deviation.
Comorbidities
Comorbidities were common in the study population. The proportion of patients with ≥1 comorbid condition increased from 54.1% in 2013 to 61.2% in 2016 (p < 0.001). The percentage of patients with certain common comorbidities significantly increased between 2013 and 2016 including hypertension, nonalcoholic fatty liver disease (NAFLD), endocrine diseases, cardiovascular diseases and hyperlipidemia (Table 2). A number of additional comorbidities also increased in prevalence, including renal impairment (8.8–10.0%; p < 0.001) and osteoporosis and/or pathologic/nontraumatic bone fracture (3.8 vs 7.3%; p < 0.001).
| Comorbidities | 2013 Cohort (n = 14,545) | 2016 Cohort (n = 11,648) | p-value |
|---|---|---|---|
| Nonalcoholic fatty liver disease | 13.9% | 17.0% | <0.001 |
| Hypertension | 9.4% | 14.5% | <0.001 |
| Endocrine disease | 7.8% | 11.1% | <0.001 |
| Renal impairment | 8.8% | 10.0% | <0.001 |
| Cardiovascular diseases | 5.7% | 10.0% | <0.001 |
| Osteoporosis and/or pathologic/nontraumatic bone fracture | 3.8% | 7.3% | <0.001 |
| Hyperlipidemia | 4.7% | 7.0% | <0.001 |
| Diabetes | 3.2% | 3.6% | <0.001 |
Liver-related complications
The percentage of patients with ≥1 liver-related complication increased from 16.4% in 2013 to 21.1% in 2016 (p < 0.001). The percentage of patients with compensated cirrhosis (11.3 vs 15.8%; p < 0.001) and decompensated cirrhosis (6.4 vs 7.2%; p < 0.001) also increased between 2013 and 2016. The distribution of liver-related complications is illustrated in Figure 3.
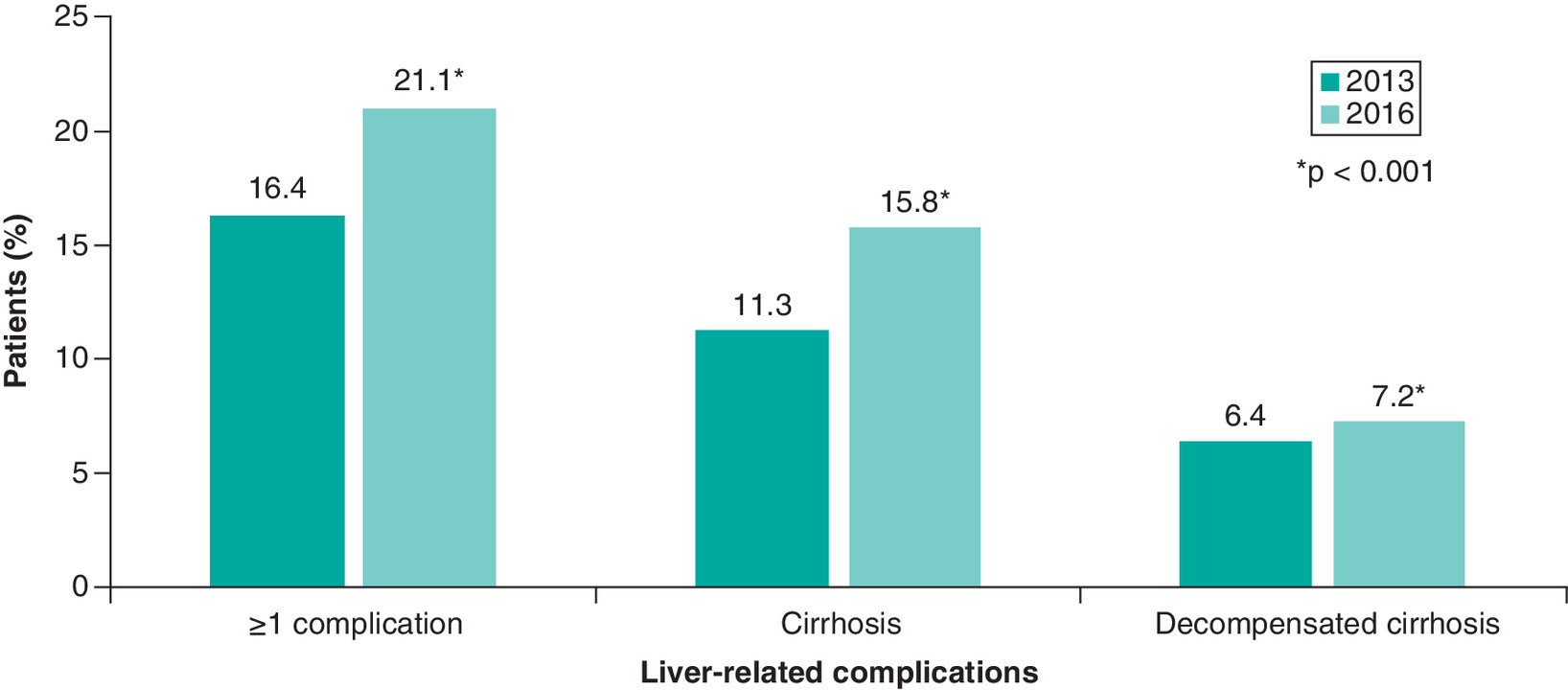
Figure 3. Distribution of liver-related complications in adult urban Chinese patients with chronic hepatitis B, 2013 & 2016.
*p < 0.001.
Distribution of NA therapy
The proportion of patients with ≥1 prescription record for any NA increased significantly from 39.5% in 2013 to 55.2% in 2016 (p < 0.001; Table 3). Thus, the proportion of untreated CHB patients in the 2013 claims database was significantly higher than that in the 2016 claims database (60.5 vs 44.8%, p < 0.001). The proportion of patients receiving prescriptions for four of the five NAs evaluated increased, with the largest increase seen in entecavir prescriptions (22.8–39.6%; p < 0.001) and only small, but statistically significant, increases seen for adefovir, telbivudine and tenofovir disoproxil fumarate. Prescriptions of lamivudine fell significantly from 10.4 to 8.4% (p < 0.001).
| Prescriptions | 2013 Cohort (n = 14,545) | 2016 Cohort (n = 11,648) | p-value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Any NA† | 5741 | 39.5 | 6424 | 55.2 | <0.001 |
| Entecavir | 3319 | 22.8 | 4614 | 39.6 | <0.001 |
| Adefovir | 1789 | 12.3 | 1519 | 13.0 | <0.001 |
| Lamivudine | 1516 | 10.4 | 974 | 8.4 | <0.001 |
| Telbivudine | 536 | 3.7 | 631 | 5.4 | <0.001 |
| Tenofovir | 0 | 0.0 | 131 | 1.1 | <0.001 |
†
Patients could have prescriptions for ≥1 NA in the same year.
NA: Nucleotide/nucleoside analog.
Discussion & conclusion
This large, retrospective study of urban Chinese patients with CHB leveraged the only nationally representative database for urban workers and residents, and is the first study to characterize the demographics, comorbidity burden and recent trends in NA treatment patterns in this population. The data revealed that the Chinese urban population with CHB is aging and that the comorbidity burden is increasing, even over the short time span assessed.
Based on comparisons of the 2013 and 2016 age pyramids of the CHB cohort, there is a trend of decreased number of younger CHB patients between 2013 and 2016 for males and females. In males, there is an increase of CHB in older patients, but this was less obvious in females (Figure 2). The CHB age pyramids in this study differ from the general age pyramids in 2013 and 2016, though a statistical comparison was not carried out. In the general population, there are relatively minor differences between 2013 and 2016 when it comes to the percent composition of each age group, which corresponds to a population that has a net positive increase in the population (i.e., birth rates are higher than mortality rates). In both populations, there is an increase in the percentage who are at least 45 years old, and this shift was more pronounced in the CHB database population. More work is required to assess whether these results suggest an aging CHB population with decreased CHB cases in younger urban Chinese populations; the decrease in proportion of patients in the database with CHB diagnosis may reflect an impact of the efforts to reduce HBV in China coupled with aging of those already infected. Other studies have shown a higher prevalence of HBV in males than in females [17], and this study supports those findings. Almost twice as many patients with CHB aged ≥45 years in the CHIRA database were males. The proportion of male patients with CHB increased significantly between 2013 and 2016 (58.4 vs 63.2%; p < 0.001). While this result suggests gender disparity, it is unclear if this is a result of more men receiving the diagnosis or more seeking medical care. Men are more prone than women to cardiovascular diseases, which could have prompted medical attention and subsequent diagnosis of HBV.
We focused on comorbidities in an urban CHB population, but some evidence suggests that hepatitis B may be more prevalent in rural areas of China. Wang et al. looked at the distribution of HBV infection in urban and rural populations in a recent meta-analysis of 27 studies in the Chinese population from 2013 to 2017, in which HBV prevalence was measured by the detection of the hepatitis B surface antigen; the prevalence of HBV overall was found to be 6.89% (95% CI: 5.84–7.95) with urban prevalence of 3.29% and rural prevalence of 5.86%, and the highest prevalence of HBV infection was reported in western provinces (8.92; 95% CI: 7.19–10.64) [17]. Given the small difference in prevalence between rural and urban populations, a focus on urban patients is unlikely to markedly affect the results. The reason for the increase in CHB patients in national cities observed in our dataset is unknown, but may reflect migratory trends.
The observed comorbidities in this study are reflective of known comorbidities of CHB based on other published studies from around the world. Common comorbidities assessed in various CHB studies in the USA, Saudi Arabia, Taiwan and South Korea were NAFLD, coronary artery diseases, CKD, diabetes, hypertension, osteoporosis and hyperlipidemia [9,18–20]. These results are consistent with data from multiple studies conducted across Asia that together show that the CHB population is rapidly aging and accumulating comorbidities [21]. A recent study evaluated CHB comorbidities in Hong Kong over an 18-year period spanning 2000–2017. The prevalence of hypertension (25.5–28.6%), diabetes (10.6–20.1%), cardiovascular disease (12.5–22.2%) and malignancies (7–23.6%) increased between the initial study period (2000–2004) and the latest data collection period (2014–2017). There was also a statistically significant shift in the age of the HBV population, from 41 ± 15 years in 2000–2004 to 55 ± 15 years in 2014–2017. A second study, conducted in a Korean population, identified a significant increase in age from 47 years in 2007 to 52 years in 2016. As in other studies, the comorbidity burden increased in parallel with age, with significant increases in the percentage of patients with hyperlipidemia, hypertension, diabetes, osteoporosis/bone fracture and CKD [22]. In Taiwan, a retrospective claims review of data from the National Health Insurance Research Database found that the Taiwanese CHB population had aged substantially between 2001 and 2011, at which point nearly 42% of patients were aged ≥55 years. Increases in the percentage of patients with clinically significant comorbidities including CKD, osteoporotic fractures and metabolic syndrome, were also apparent, with the latter increasing almost fourfold over the time period assessed in the analysis [23]. In Japan, an analysis of 13,639 patients that compared the demographics of the CHB population in 2011 and 2016 found that the average age of patients with CHB increased from 62 to 66 years across this brief time period and that the rates of key comorbidities and complications including diabetes (from 8 to 14%), kidney disease (from 4 to 5%), bone fracture (from 5 to 9%) and NAFLD (from 14 to 16%), all increased significantly [24].
Globally, a similar pattern appears. An analysis conducted in the USA compared demographics and comorbidities of CHB patients between 2000 and 2015 and found a similar shift in demographics [9]. Mean age in this US-based study increased from 43.3 years during the 2000–2005 assessment period to 49.1 during the 2011–2015 period. Also consistent with this analysis, the percentage of patients with nonliver comorbidities increased substantially: diabetes by almost fivefold, hypertension by threefold and CKD by 4.5-fold. The prevalence of osteopenia and osteoporosis likewise increased by threefold and 2.5-fold, respectively, in the USA analysis.
Although the time periods assessed in this study were separated by only 3 years, there was a small but significant increase in the percentage of renal disease that is concerning, since renal function decline may be associated with aging and antiviral treatments [25]. Use of NA antiviral treatment also increased over the same time period in the Chinese CHB population. Further, some data suggest that patients with CHB may be fundamentally at greater risk for kidney and bone disease compared with non-CHB controls [26]. For these reasons, the most recent European Association for the Study of the Liver (EASL) guidelines indicate that all patients at risk for renal disease who are on antiviral therapy, as well as all patients treated with tenofovir disoproxil fumarate regardless of renal risk, should undergo baseline and periodic renal monitoring including at least estimated glomerular filtration rate and serum phosphate levels [25].
There was a larger and statistically significant increase in the percentage of patients with bone disease, which may be exacerbated by NA treatment and has also been raised as a concern in updated guidelines [25]. Given that aging is associated with reduced renal function and an increasing prevalence of bone disease, the superimposition of age- and treatment-related changes in renal function and bone health may represent a significant emerging clinical issue as CHB patients continue to age and the proportion of treated patients’ increases.
There was a striking increase in the percentage of patients with NAFLD over the study time period, consistent with recent analyses indicating that the prevalence of NAFLD is increasing globally in non-CHB and CHB populations [27,28]. This finding is concerning, as NAFLD associated with CHB may be associated with an increased risk for end-stage liver disease and death [28]. It is noteworthy that the prevalence of diabetes only increased from 3.2 to 3.6% in this study, yet this may be an underestimate as many physicians may not code comorbidities, such as diabetes, if the primary reason for the visit is CHB. Estimates of diabetes prevalence in the Chinese population were 9.1% overall and 11.4% in the urban population between 2000 and 2014 in a meta-analysis [29] and 12.8% in the general Chinese population in the 2015–2017 period [30], supporting this idea.
The percentage of patients with CHB-related liver complications including cirrhosis and decompensated cirrhosis, increased significantly between 2013 and 2016. There was a small but significant decline in the rate of HCC in this population; however, this estimate may not be accurate because cancer patients are not well captured in the CHIRA dataset.
An analysis of treatment trends found that the percentage of patients receiving any NA therapy increased by nearly 40% even over the relatively short span assessed in this study, from 39.5 to 55.2%. Overall, these results suggest that more CHB patients are being diagnosed and treated, which may be a result of better CHB surveillance in urban China. This may also contribute to the observed increase in the percentage of older patients, which was more dramatic in the CHB patient population than in the general population, and the decrease in tier 3 hospitalizations in this population. While promising, these data show that more than half of Chinese patients with CHB remain untreated. Further, while much of this increase was driven by increased prescription of entecavir, an NA with a high genetic barrier to resistance [31], at least half of the treated patients included in this analysis were still receiving therapy with agents that have a low genetic barrier to resistance (e.g., adefovir, lamivudine and telbivudine) as of 2016. Tenofovir alafenamide, along with entecavir, has particular utility in patients with or at risk for renal or bone disease and is recommended in these patients by the most recent iteration of the EASL guidelines [25].
The trends observed in this study have several important implications for the future management of CHB in Chinese patients. Current Chinese clinical practice guidelines do not recommend routine screening of comorbidities in CHB patients [8]. Increasing age, a greater likelihood of comorbidities, and a consequent increase in the need for comedications raise potential safety risks. Additionally, the observed trends of rapid increases in the percentage of CHB patients with comorbid cardiovascular diseases, chronic renal diseases, NAFLD and osteoporosis in this study clearly demonstrate the need to assess and manage these comorbidities to improve overall patient health outcomes. Routine screening for comorbidities is increasingly important to guide the selection of appropriate NA treatment and manage comorbidities in CHB patients. These data also point to the ongoing need for new CHB therapies with improved safety profiles and high genetic barriers to resistance.
This study was intended as a descriptive analysis of the CHB comorbidity burden in urban Chinese patients and to provide a foundation for future studies. Therefore, the design of this study is accompanied by a number of inherent limitations. First, the CHIRA data claims utilized in this study were specific to CHB, and as such, no matched non-CHB cohort was able to be created for comparison. Therefore, this study was unable to determine the prevalence of comorbidities in the general population in 2013 and 2016. However, the results of this analysis closely resemble trends observed in other studies and in other countries, though more work must be done to verify these trends in the Chinese urban population. Additionally, the lack of a non-CHB control group prevents determination of the effect of age alone on the prevalence of comorbidities in the CHB group. Furthermore, the analysis of this study did not control for other variables such as geographic location or gender, highlighting the need for multivariate analysis and adjusted models in future study designs.
Second, the study periods assessed in this study, 2013 and 2016, were separated by only 3 years. Thus, they provide only a limited snapshot of changes in demographics and comorbidities over a short period of time. It will be crucial to extend the assessment period in future studies so longitudinal trends can be more clearly identified. Nevertheless, the changes observed for age and for many comorbidities were striking and significant and point toward the potential changes in the clinical profile of CHB patients in China over longer assessment periods.
Third, estimates of comorbidity burden may be low because clinicians may not code comorbidities if the primary reason for the visit was for CHB. Furthermore, lack of standardization of Chinese diagnostic information increases the potential for bias introduction during analysis of the CHIRA database, which could be reduced by a greater utilization of international standards such as ICD-10. This study also provides no information on the impact of treatment on renal function or bone disease, as it included a mixed population of treated and untreated patients. This highlights the need for future studies addressing the impact of treatment on these disease states and separation of treated and untreated patient populations.
The use of the CHIRA annual claims database, which included only patients from the two major urban health insurance plans in China, as a data source may result in some degree of selection bias. Further, the data collection design of CHIRA does not allow for tracking previous treatment history or accurately estimate the duration of CHB treatment for individual patients due to the randomized sampling. The design and available data sources precluded following patients longitudinally, pointing to the need for future studies to follow a real-world cohort of Chinese CHB patients with detailed clinical information to address the needs of screening and monitoring comorbidities.
•
This study leveraged the China Health Insurance Research Association annual urban claims databases for two calendar years (2013 and 2016) and showed statistically significant distinct shifts toward increasing age and comorbidity burden in Chinese urban chronic hepatitis B (CHB) patients.
•
Further, these data show that a significant proportion of this patient population remains untreated for CHB, and of those who are treated, many still receive treatments with a low genetic barrier to resistance.
•
As this patient population ages and comorbidities accumulate, it will become even more important that comorbidities are carefully assessed, managed and taken into account when selecting nucleotide/nucleoside analog treatment.
Author contributions
All authors were involved in study protocol, results interpretation and manuscript development. W Chen and L-I Hsu contributed to the data extraction/clean and data analyses. All authors have critically reviewed the manuscript and approved the manuscript submission.
Financial & competing interests disclosure
This study was funded by Gilead Sciences, Inc. J Hou has received research grants and a speaker honorarium from Gilead Sciences, Inc., Bristol Myers Squibb, GSK and Novartis. W Chen is the founder of Normin Health, a consulting firm receiving industry funds to conduct health economics and outcomes research. Y Han has served on advisory boards for Gilead Sciences, Inc., Bristol Myers Squibb, GSK, Roche, AbbVie, Merck Sharpe & Dohme, Abbott and Mylan. L Wang has served on advisory boards for Gilead Sciences, Inc., and has been a speaker for Bristol Myers Squibb, GSK, AbbVie, Merck Sharpe & Dohme, Mylan and Roche. I-H Lee and L-I Hsu are employees of Gilead Sciences, Inc., and own stock in the company. D Xie has received speaker honoraria from Gilead Sciences, Inc., Bristol Myers Squibb, GSK and Novartis. X Yin has no conflict of interest to declare. F Hou has no conflict of interest to declare. Y Yang has received research grants from Gilead Sciences, Inc., and has received speaker honoraria from GSK and Gilead Sciences, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing and editorial support was provided by Impact Communication Partners, Inc.
Ethical conduct of research
The study was approved by CHIRA, which assessed the risk of ethics regarding the use of the urban claims data of CHIRA. The study was performed in compliance with the ethical principles of good clinical practice and according to the ICH Harmonized Tripartite Guideline.
Data sharing statement
The data that support the findings of this study are available from CHIRA but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of CHIRA.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet 386(10003), 1546–1555 (2015).
2.
Lozano R, Naghavi M, Foreman K et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859), 2095–2128 (2012).
3.
World Health Organization. Up to 10 million people in China could die from chronic hepatitis by 2030--urgent action needed to bring an end to the ‘silent epidemic’. www.who.int/china/news/detail/26-07-2016-up-to-10-million-people-in-china-could-die-from-chronic-hepatitis-by-2030-urgent-action-needed-to-bring-an-end-to-the-silent-epidemic-. (26 July 2016)
4.
Chen S, Li J, Wang D, Fung H, Wong LY, Zhao L. The hepatitis B epidemic in China should receive more attention. Lancet 391(10130), 1572 (2018).
5.
Zhang W, Ji Z, Wang L, Xiao D, Yan Y. A meta-analysis of HBsAg-positive rate among general Chinese populations aged 1–59 years. Infect. Dis. (Lond.) 47(12), 878–888 (2015).
6.
Luo Z, Li L, Ruan B. Impact of the implementation of a vaccination strategy on hepatitis B virus infections in China over a 20-year period. Int. J. Infect. Dis. 16(2), e82–e88 (2012).
7.
WHO. Global Hepatitis Report 2017 (2017). www.who.int/hepatitis/publications/global-hepatitis-report2017/en/
8.
Hou J, Wang G, Wang F et al. Guideline of prevention and treatment for chronic hepatitis B (2015 update). J. Clin. Transl. Hepatol. 5(4), 297–318 (2017).
9.
Liu A, Le A, Zhang J et al. Increasing co-morbidities in chronic hepatitis B patients: experience in primary care and referral practices during 2000-2015. Clin. Transl. Gastroenterol. 9(3), 141 (2018).
10.
Yang Y, Zhang J, Du F, Montgomery W, Li H, Flynn JA. Real world evidence in Mainland China: experience with the use of health care claims data. Value Health 17(7), A728 (2014).
11.
Zhao C, Wang C, Shen C, Wang Q. China’s achievements and challenges in improving health insurance coverage. Drug Discov. Ther. 12(1), 1–6 (2018).
12.
Zhang J, Ung COL, Wagner AK, Guan X, Shi L. Medication use during pregnancy in Mainland China: a cross-sectional analysis of a National Health Insurance database. Clin. Epidemiol. 11, 1057–1065 (2019).
13.
Yong M, Xianjun X, Jinghu L, Yunyun F. Effect of health insurance on direct hospitalisation costs for in-patients with ischaemic stroke in China. Aust. Health Rev. 42(1), 39–44 (2018).
14.
Wu P, Xu B, Shen A et al. The economic burden of medical treatment of children with asthma in China. BMC Pediatr. 20(1), 386 (2020).
15.
Population of China 2013 (2013). www.populationpyramid.net/china/2013
16.
Population of China 2016 (2016). www.populationpyramid.net/china/2016
17.
Wang H, Men P, Xiao Y et al. Hepatitis B infection in the general population of China: a systematic review and meta-analysis. BMC Infect. Dis. 19(1), 811 (2019).
18.
Sanai FM, Alghamdi H, Alswat KA et al. Greater prevalence of comorbidities with increasing age: cross-sectional analysis of chronic hepatitis B patients in Saudi Arabia. Saudi J. Gastroenterol. 25(3), 194–200 (2019).
19.
Tseng CH, Hsu YC, Ho HJ, Nguyen MH, Wu CY. Increasing age and non-liver comorbidities in patients with chronic hepatitis B in Taiwan: a nationwide population-based analysis. Dig. Dis. (2020) (Epub ahead of print).
20.
Oh H, Jun DW, Lee IH et al. Increasing comorbidities in a South Korea insured population-based cohort of patients with chronic hepatitis B. Aliment. Pharmacol. Ther. 52(2), 371–381 (2020).
21.
Wong GL, Yuen BW, Tse YK et al. Abstracts. Hepatol Int. 13, 1–266, Abstract no. 290 (2019).
22.
Jun DW, Oh H, Ahn HJ, Kim BO, Nguyen MH. Increased clinical and economic burden of chronic hepatitis B (CHB) patients compared to non-CHB from 2007 to 2016 in Korea. Presented at: Korean Association for the Study of the Liver (KASL). Haeundae-gu, Busan, South Korea(2019).
23.
Hsu Y-C, Ho HJ, Nguen MH, Wu C-Y. Increasing age and non-liver comorbidities in chronic hepatitis B patients in Taiwan: a nationalwide population analysis. Presented at: Asian-Pacific Association for the Study of the Liver 2019 Annual Meeting. Manila, Philippines (2019). (Poster 631).
24.
Yotsuyanagi H, Yatsuhashi H, Kurosaki M, Zur R, Sherman S, Nguyen MH. Increasing age and comorbidities in 13,639 adult patients with chronic hepatitis B (CHB) from 2011 to 2016 in Japan: results of a real-world analysis. Presented at: Asia-Pacific Association for the Study of the Liver Annual Conference 2018. New Delhi, India, (2018) Oral presentation no. O-HBV-36
25.
European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 67(2), 370–398 (2017).
26.
Chen CH, Lin CL, Kao CH. Association between chronic hepatitis B virus infection and risk of osteoporosis: a nationwide population-based study. Medicine (Baltimore) 94(50), e2276 (2015).
27.
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease: meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 64(1), 73–84 (2016).
28.
Lin CW, Huang XL, Liu HL, Wang Y. Interactions of hepatitis B virus infection with nonalcoholic fatty liver disease: possible mechanisms and clinical impact. Dig. Dis. Sci. 60(12), 3513–3524 (2015).
29.
Yang L, Shao J, Bian Y et al. Prevalence of Type 2 diabetes mellitus among inland residents in China (2000-2014): a meta-analysis. J. Diabetes Investig. 7(6), 845–852 (2016).
30.
Li Y, Teng D, Shi X et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ 369, m997 (2020).
31.
Ghany MG, Doo EC. Antiviral resistance and hepatitis B therapy. Hepatology 49(Suppl. 5), S174–S184 (2009).
Information & Authors
Information
Published In
Pages: 647 - 657
PubMed: 33970683
Copyright
© 2021 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 26 May 2020
Accepted: 13 January 2021
Published online: 10 May 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Shifting demographics and comorbidity burden in adult Chinese urban patients with chronic hepatitis B, 2013 and 2016. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0080
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Wei Qiaoying, Fan Lanming, Lian Yang, Li Jia, Sun Qun, Zhou Yuelin, Curative care expenditure across different comorbidity states of chronic hepatitis B: a prevalence study in Sichuan Province, China, BMJ Open, 10.1136/bmjopen-2025-100234, 15, 11, (e100234), (2025).
- Xing Meng, Iain A. Gillespie, Jane Dong, Yi Ning, Stuart Kendrick, Characteristics of patients with chronic hepatitis B infection in China: A retrospective claims database study, Medicine, 10.1097/MD.0000000000036645, 103, 7, (e36645), (2024).
- Yao-Chun Hsu, Daniel Q. Huang, Mindie H. Nguyen, Global burden of hepatitis B virus: current status, missed opportunities and a call for action, Nature Reviews Gastroenterology & Hepatology, 10.1038/s41575-023-00760-9, 20, 8, (524-537), (2023).