Preferences, satisfaction and decision-making processes in osteoporosis treatment: a systematic review of the literature
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To synthesize information available in the literature on patients' preferences and satisfaction with osteoporosis treatment and their unmet needs on the treatment decision-making process. Materials & methods: Systematic literature review consulting international database and grey literature of articles published between January 1, 2009 and January 1, 2019. Results: Nineteen publications were reviewed, 79% of them focused on evaluating the importance that patients attached to the mode and frequency of administration, adverse events and treatment efficacy. 21% of them provided information about treatment satisfaction and 26% regarding unmet needs on treatment-decision making process. Conclusion: Aligning treatment with patients' preferences, promoting physician-patient communication and identifying patients' concerns with treatment may contribute to improve treatment satisfaction and adherence and ultimately achieve the treatment goal.
Osteoporosis is a systemic skeletal disorder characterized by low bone mass and microarchitectural deterioration of bone tissue, with a subsequent increase in bone fragility and susceptibility to fracture [1]. Using the diagnostic criteria of the World Health Organization [2], it was estimated that in the European Union in 2010, 22 million women and 5.5 million men had osteoporosis [3]. Hip fracture is the most severe complication of osteoporosis, and it is associated with a poorer health-related quality of life (HRQoL), higher morbidity and mortality, higher economic cost and in most cases requires hospitalization [4]. Both non-pharmacological (promotion of physical activity, adequate nutrition and cessation of tobacco, alcohol and caffeine consumption) and pharmacological measures are key to reduce the risk of fracture.
Currently, there is a wide range of therapeutic options for osteoporosis; however, treatment adherence is suboptimal, being adherent to treatment less than 70%, as measured by the proportion of days covered (PDC) [5]. The therapeutic algorithm varies depending on the patient's risk of fracture, the objective of prevention (primary or secondary), the contraindications of each drug, possible adverse effects (AEs) [3,6,7] and, potentially, the patient's preferences.
The clinical relationship is evolving toward patient-centered medicine aimed at improving the health outcomes of individual patients, taking into account their preferences, objectives and values, as well as the financial resources available [8]. This model of care encourages physicians and patients to work together to achieve the best possible clinical results [9]. Unlike the traditional biomedical model, patient-centered medicine promotes the participation of patients in clinical decision-making, the personalization of treatment and incorporates patients' preferences in the choice of treatment, intending to improve healthcare outcomes [9].
Since patient preference and satisfaction are important determinants of adherence to therapies for chronic conditions such as osteoporosis, consider patient preference individually when prescribing treatment for osteoporosis is crucial to ensure that long term disease management is effective [10].
Shared physician–patient decision-making in osteoporosis improves three areas: cognitive (improves knowledge and self-perception of the risk of fractures), behavioral (increases compliance and persistence with treatment) and affective (reduces anxiety and conflict in decision-making and increases satisfaction) [11]. Therefore, patients' health outcomes are expected to improve due to their greater involvement in their care. In osteoporosis, where there are many therapeutic options, the patient's participation in decision-making is particularly relevant [9]. Patients' and professionals' perceptions of the disease and treatment do not necessarily coincide [12]. Thus, it is increasingly important to consider patients' perspectives and preferences concerning these matters.
Previous review focus on patients' preferences showed variations in the preferences of patients, suggesting the importance to consider individual preference in decision-making to improve osteoporosis care [13]. Therefore, a greater understanding of how patients with osteoporosis establish their preferences for treatments and perceive their participation in decision-making may contribute to optimizing the development of future therapies, as well as more patient-centered decision-making. This review aims to answer these three questions: ‘What are the most valued characteristics of the treatment of osteoporosis from patients' perspective?’; 'What is their degree of satisfaction with treatment?’ and ‘What are their unmet needs regarding treatment decision-making?' For this purpose, we review and synthesize the information available in clinical trials, observational studies and systematic reviews published in the last 10 years.
Methods
A systematic review of the literature was carried out following the PRISMA recommendations (Preferred Reporting Items for Systematic Reviews and Meta-Analyzes) [14]. The international Medline/Pubmed and Cochrane Library databases were searched. Additionally, a broad search in the grey literature (Google/Google academic) and the review of the bibliographic citations of the key articles selected complimented the systematic search. Depending on the nature of the database consulted, MeSH (Medical Subject Headings) and free-text terms were used, combined with Boolean operators (Table 1).
| N° | Terms related to osteoporosis |
|---|---|
| #1 | ‘osteoporosis’ |
| #2 | ‘osteoporosis’[Mesh] |
| Terms related to treatment | |
| #3 | ‘treatment’ |
| #4 | ‘therapy’ |
| #5 | ‘therapeutics’ |
| #6 | ‘management’ |
| #7 | ‘drug therapy’ |
| #8 | ‘medication’ |
| Terms related to the type of study | |
| #9 | ‘attribute identification’ |
| #10 | ‘clinical decision making’ |
| #11 | ‘conjoint analysis’ |
| #12 | ‘DCE’ |
| #13 | ‘decision aid’ |
| #14 | ‘decision coaching’ |
| #15 | ‘decisional conflict’ |
| #16 | ‘decision making’ |
| #17 | ‘decision support techniques’ |
| #18 | ‘discrete choice’ |
| #19 | ‘discrete choice experiment’ |
| #20 | ‘health care preferences’ |
| #21 | ‘patient centered’ |
| #22 | ‘patient centered care’ |
| #23 | ‘patient involvement’ |
| #24 | ‘patient participation’ |
| #25 | ‘patient satisfaction’[Mesh] |
| #26 | ‘patient satisfaction’ |
| #27 | ‘preference’ |
| #28 | ‘risk-benefit’ |
| #29 | ‘risk preferences’ |
| #30 | ‘shared decision making’ |
| #31 | ‘trade-off’ |
| #32 | ‘willingness to accept’ |
| #33 | ‘willingness to pay’ |
| #34 | ‘WTP’ |
(‘Osteoporosis’[Mesh] OR ‘osteoporosis’) AND (‘Treatment’ OR ‘therapy’ OR ‘therapeutics’ OR ‘management’ OR ‘drug therapy’ OR ‘medication’) AND (‘patient centered’ OR ‘patient centered care’ OR ‘patient involvement’ OR ‘patient participation’ OR ‘shared decision making’ OR ‘Patient satisfaction’[Mesh] OR ‘Patient satisfaction’ OR ‘conjoint analysis’ OR ‘DCE’ OR ‘discrete choice’ OR ‘discrete choice experiment’ OR ‘attribute identification’ OR ‘decision aid’ OR ‘decisional conflict’ OR ‘preference’ OR ‘risk preferences’ OR ‘health care preferences’ OR ‘trade-off’ OR ‘risk-benefit’ OR ‘willingness to pay’ OR ‘WTP’ OR ‘willingness to accept’ OR ‘decision making’ OR ‘clinical decision making’ OR ‘decision coaching’ OR ‘decision support’).
DTE: Discrete choice experiment; WTP: Willingness to pay.
The review period was restricted to articles published between January 1, 2009, and January 1, 2019 (search closing date). A period of 10 years has been considered long enough to cover all the therapeutic alternatives available today. The retrieved publications were peer-reviewed and evaluated as appropriate if they focus on the objective of the review.
After duplicates removal, two researchers independently screened each of the identified publications at two levels. level 1 screening entailed a broad screen based on items title and/or abstract, as available. The full text of all publications selected on level 1 were reviewed for level 2 applying eligibility criteria. Any discrepancies between reviewers were resolved through consensus and, if necessary, by consulting a third reviewer.
Publications that meet these inclusion criteria were included in the review: 1) clinical trials, observational studies and systematic reviews evaluating a) the preferences of patients with osteoporosis regarding treatment characteristics, b) the relevant aspects in the shared decision-making of patients with osteoporosis and c) their satisfaction with the treatment received, 2) conducted in Europe or North America and, 3) published in English or Spanish between January 1, 2009, and January 1, 2019. Conversely, articles in the form of comments, letters to the editor or editorials, narrative reviews and original studies included in systematic reviews selected in the review, were excluded.
Table 2 shows the inclusion criteria following the PICOS (population, intervention, comparator, outcomes and study design) definition.
| Inclusion criteria | |
|---|---|
| Population | Patients with osteoporosis |
| Intervention | Treatments for osteoporosis. All treatments are included. |
| Comparator | – |
| Outcomes | Patients' preferences and satisfaction with osteoporosis treatment Unmet needs the treatment decision-making process |
| Study design | Clinical trials, observational studies and systematic reviews. |
PICOS: Population, intervention, comparator, outcomes and study design.
Selected publications were categorized according to its scope in: ‘Patient preferences for osteoporosis treatments’, ‘Treatment satisfaction’ and ‘Treatment decision-making.’
Two independent reviewers extracted data from selected publications. Discrepancies will be resolved by consensus or by involving a third team member. A standardized data extraction form and data extraction guidelines were developed before data extraction begins. Data regarding author, year of publications and country, study design and methodology, study objective, study population, treatment characteristics evaluated and the main result was extracted.
Due to the different nature of the publications selected and study design, to assess the quality of the study and provide the level of evidence for each publication the criteria of the Oxford Center for Evidence-Based Medicine [15] were followed.
Results
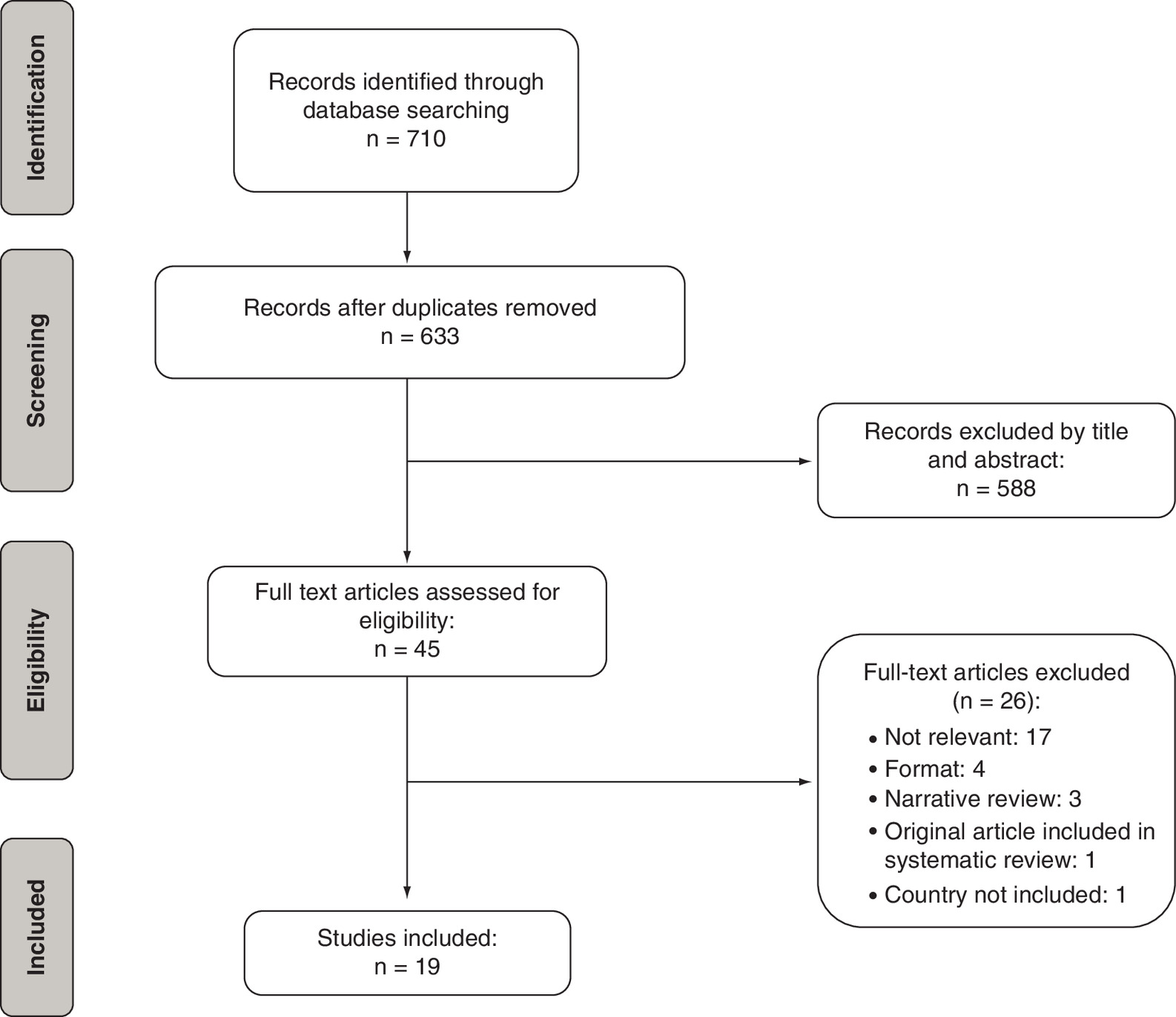
A total of 710 potentially relevant titles were identified in the databases (Figure 1). After debugging, 77 duplicates and 588 articles were eliminated by title and abstract as they were not relevant to the purpose of the review, and 45 publications were considered for full-text reading. After thoroughly reading and applying the inclusion/exclusion criteria, 26 publications were excluded. Finally, a total of 19 publications were selected as they referred to preferences for osteoporosis treatments, relevant aspects in decision-making and satisfaction with treatment (Table 3). The reasons for exclusion are shown in the Supplementary Material.
| Author, year (country)/level of evidence | Study design/ methodology | Scope | Objective of the study | Study population | Main results | Ref. | |
|---|---|---|---|---|---|---|---|
| 1 | Fobelo Lozano et al., 2019 (Multicountry)/1 | Systematic review | Patient preferences for osteoporosis treatments | To assess compliance, as well as patient preferences and satisfaction with once-yearly intravenous zoledronic acid treatment versus another bisphosphonate | 6 RCTs 2 observational studies Adults over 18 with osteoporosis or at high risk of low bone density due to chronic use of glucocorticoids | Besides there is limited evidence available comparing newer osteoporosis therapies, the review highlights the high potential of annual osteoporosis regimen for improving patient adherence. Most studies included in the review pointed that a single annual injection is preferred with respect to other regimens of treatment. Patients appear to prefer less frequent dosing if agents are perceived to be of equivalent benefit as this is less disruptive to their lifestyle. | [16] |
| 2 | Jakobsen et al., 2018 (Denmark)/5 | Qualitative phenomenological study/interviews | Treatment decision-making | To understand how patients experience the diagnosis of OP and describe and identify their needs to promote optimal management of osteoporosis by the health services | 17 women (52–65 years) with DXA T-score <-2.5, without previous fractures, with at least one of the known risk factors for osteoporosis | In general, most patients perceived that during the diagnostic visit they were not prepared to assume and understand the disease, since treatment is prescribed at the same time as diagnosis is made. They would like to have had more information about the disease and treatment options before making the decision about the medication to take, so they could ask informed questions and participate in shared decision-making. | [32] |
| 3 | Jensen et al., 2018a (Denmark)/5 | Qualitative study of group education and individual interviews | Treatment decision-making | To investigate the impact of a multidisciplinary education program in group sessions for patients with and without fractures, in decision-making related to treatment options and lifestyle | 17 patients (14 women and 3 men) | Attending an educational group had a positive impact on patient decision-making by improving patient's information about diagnosis and prevention, exercise, activities of daily living, diet and medication. This greater information contributes to the patient's participation in decision-making on new ways of managing osteoporosis and on how to implement a lifestyle that guarantees bone health. | [31] |
| 4 | Hiligsmann et al., 2017 (Belgium, France, Ireland, Netherlands, Spain, Switzerland and United Kingdom)/5 | Cross-sectional observational/ DCE | Patient preferences for osteoporosis treatments | Estimate and compare the preferences of patients with osteoporosis by the attributes of the treatments in 8 European countries | 1,124 patients, with a sample of between 98 and 257 patients per country. – Women: 85.3%; – Mean age: 65 years – Diagnosis of osteoporosis: 73.9% – Previous fracture: 52.1%; – In treatment for osteoporosis: 55.4% | Patients preferred more effective and less costly treatment (in the three countries where the cost attribute was part of the study). In all countries, they preferred subcutaneous injection every 6 months to weekly oral tablets. In most countries, they also preferred monthly oral tablets and annual intravenous injections over weekly oral tablets. In all countries except Spain, patients placed more importance on GI disorders than on skin reactions or flu-like symptoms. There were statistically significant differences in patients' preferences for anti-osteoporosis medications between countries, especially for the mode of administration. | [18] |
| 5 | Oral et al., 2015 (Turkey and Poland)/3 | Longitudinal crossover RCT | Patient preferences for osteoporosis treatments | Examine compliance, persistence and preferences in OP patients receiving risedronate daily, with a fixed dose of three different time regimens (A: before breakfast; B: between meals; C: before bed) or with a flexible dosage | 448 patients with postmenopausal OP enrolled in 10 centers in Turkey and 9 centers in Poland (baseline sociodemographic characteristics of patients are not described) | Apart from a significantly higher rate in persistence noted in patients under the flexible regimen, flexible and fixed dosing of daily risedronate therapy, similar findings were observed in postmenopausal osteoporotic women in terms of compliance, responder and patient preference rates as well as efficacy on reduction in BTMs. | [24] |
| 6 | Neuner et al., 2014 (USA)/5 | Cross-sectional observational /survey | Patient preferences for osteoporosis treatments | To study the perceptions of patients on the thresholds of fracture risk at 10 years and adverse effects of osteoporosis treatment | 241 women were included in the study: – Average age: 69.4 years – Race: 94.4% white – Diagnosis: osteoporosis (27%), osteopenia (31%), normal BMD (42%); – History of fractures after 40 years: 34% (some) 3% (hip) | The probability of accepting treatment was related to patients' increased risk of fracture, with a readiness to accept treatment (>50% of patients) when the 10-year risk of fracture was >15%. A family history of osteoporosis was also associated with an increased likelihood of treatment acceptance. The effectiveness of treatment and adverse effects were considered by most participants to be important or very important factors in decision-making. The adverse effects considered important/very important were: atrial fibrillation (62%), osteonecrosis of the jaw (53%) and GI symptoms (50%). | [25] |
| 7 | Kendler et al., 2014 (Canada)/3 | Crossed and open RCT | Patient preferences for osteoporosis treatments | To assess patients' perceptions of subcutaneous administration of denosumab or oral alendronate and how these perceptions influence adherence | 250 postmenopausal women with, or at risk of suffering from osteoporosis, were included in the study (the sociodemographic and clinical characteristics of the sample are not detailed in the article) | Participants preferred denosumab to alendronate while on treatment and had more positive perceptions of denosumab than alendronate. | [23] |
| 8 | Hiligsmann et al., 2014 (Netherlands)/5 | Cross-sectional observational/DCE | Patient preferences for osteoporosis treatments | Assess the preferences of patients with or at risk of osteoporosis due to treatment attributes and find out how patients make concessions between attributes | 257 patients: – Average age: 67.1 years – Women: 83.3%; – Diagnosis of osteoporosis: 89.8%; – Probability of major osteoporotic fracture, mean: 14.3% – Years with osteoporosis, average: 8.9 – Patients with treatment. osteoporotic: 69.8% Oral: 72.2%; Subcutaneous: 15.4%; Intravenous: 12.4% | Patients preferred effective (1% risk reduction) and low-cost treatments (€1.00 per month) (p < 0.001). They preferred oral or subcutaneous treatments every 6 months (p < 0.001) to weekly oral treatments. No significant differences were observed between weekly oral and subcutaneous treatments every 3 months (p = 0.21) or intravenous or oral treatments every 12 months (p = 0.17). The least preferred were intravenous every 3 months (p = 0.05). Regarding adverse effects, they preferred to have flu-like symptoms or skin reactions (p < 0.001) rather than GI symptoms In the willingness to pay analysis, patients were willing to pay €3.73/month, to reduce the risk of fracture by 1%, €19.53/month to change monthly oral treatment to subcutaneous every 6 months and €25.20/month to having flu-like symptoms rather than GI side effects. | [17] |
| 9 | Silverman et al., 2013 (USA)/5 | Cross-sectional observational/joint analysis (MaxDiff) | Patient preferences for osteoporosis treatments | To study the preferences of postmenopausal women at risk of osteoporotic fracture in 4 different ethnic groups in the United States | 365 women (100 Caucasian, 100 African American, 85 Hispanic American, 82 Asian) – Average age: 76.7, 79.7, 75.2, 74.7 years, (respectively) – Previous fracture according to FRAX: 45%, 28.7%, 31.7% and 18.5% (respectively) – Average risk of fracture at 10 years: 26.7%, 25.2%, 24.4%, 24.1% (respectively) | All participants indicated efficacy and safety as the most important attributes, however differences between groups of ethnic groups were observed. While Caucasians and African Americans valued safety more than efficacy, Asian and Hispanic women valued efficacy more than safety. Classification MaxDiff. Within safety, the long-term safety of the treatments had more weight than the short-term safety, highlighting their concern with certain effects. long-term adverse events such as stroke, cancer, or atypical fractures. Differences were seen based on socioeconomic status, education, age and previous fracture. | [26] |
| 10 | Hiligsmann et al., 2013 (Netherlands)/5 | Qualitative observational / nominal groups | Patient preferences for osteoporosis treatments | Evaluate the utility of the nominal group technique to choose attributes in DCE | 26 patients participated in the study: – Women: 92%; – Average age: 68.0 years – Diagnosis of osteoporosis: 96% – Years with osteoporosis, average: 10.2 – Previous invoice: 58% – Number of previous invoices, average: 1.04 – Patients under treatment: 96% | Most important treatment characteristics for patients were: 1) effectiveness, 2) adverse effects, 3) administration frequency, 4) administration mode, 5) cost, 6) sequential therapy, 7) administration place, 8) time on the market, 9) brand/generic, 10) monotherapy/combined, 11) action mode and 12) cost to society. | [27] |
| 11 | Vlak et al., 2011 (Croatia)/4 | Observational prospective multicenter open | Patient preferences for osteoporosis treatments & treatment satisfaction | Identify and compare the satisfaction, preferences and tolerability between a monthly-administered bisphosphonate (ibandronate) and a weekly-administered one (alendronate or risedronate) | 434 women were included in the study: 88.7% completed the questionnaire (n = 385) Average age: 66.6 years | Patients expressed preference for monthly bisphosphonate (ibandronate) in comparison with weekly bisphosphonates and found it to be a more convenient method of treatment. The study demonstrated high satisfaction in patients who switched from the weekly to the monthly ibandronate regimen in all aspects of treatment. | [30] |
| 12 | Darba et al., 2011 (Spain)/5 | Cross-sectional observational / DCE | Patient preferences for osteoporosis treatments | Identify preferences for different aspects related to drugs for osteoporosis in Spain | 116 patients (96% women) – Average age: 69 years – Time since the diagnosis of osteoporosis: >10 years (29.7%); 5–10 years (34.55%); <5 years (35.77%). – Previous medication to treat osteoporosis: 95% | The results of this study suggested that patients with osteoporosis and severe osteoporosis attach considerable importance to the route and place of administration of medication for their disease. Patients were willing to pay substantial amounts per month in order to have a subcutaneous injection once daily compared with oral drugs once daily or weekly or an intravenous injection once per year. Patients also were willing to pay for medical support with administration of the drug rather than having to self-administer the drug or having to be hospitalized for a few hours for drug administration. | [29] |
| 13 | Sale et al., 2011 (Canada)/5 | Qualitative phenomenological study | Treatment decision-making | To examine the experiences of patients with the decision to take medication for OP after suffering a fracture | 21 patients (6 men and 15 women) aged between 65 and 88 years who had suffered a fracture in the last 5 years | For 12 participants, the decision whether to take OP medication was relatively easy, involved minimal distress and occurred at the time it was prescribed. For these patients, the relationship with their physician was good and they trusted their criteria. Most made the decision based on the physician's judgment. For the other 9 patients, the decision whether to take medication was more difficult, requiring time and the consideration of several factors. The role of the physician in this group was also influential. However, although some participants trusted and respected their physicians, they demanded additional information and were convinced by them to be able to make a decision. | [33] |
| 14 | Mazor et al., 2010 (USA)/5 | Cross-sectional qualitative observational/telephone interview | Treatment decision-making | Explore the perspective of older women on the prescription of medication for osteoporosis and identify specific beliefs and experiences that influence these views. | 36 women with osteoporosis – 94.4% white – Average age: 73.4 years –Treatment status (self-reported): • Taking a prescription for osteoporosis: 41.7% • Discontinued treatment: 30.6% • Naive: 27.8% | Potential factors that influence on women's decisions about use of prescription osteoporosis medication can be organized into four categories: core beliefs, interaction with physician, personal experience and past behavior and vicarious experience. Women's interactions with their physician appeared to have a substantial impact on their views about osteoporosis and receptiveness to medication. Therefore, older women with osteoporosis need clear information about their condition, including the diagnosis, the implications of the diagnosis, treatment options, medication effectiveness and side effects. | [34] |
| 15 | Kendler et al., 2010 (International)/3 | 2 ECA (DECIDE and STAND) | Patient preferences for osteoporosis treatments & treatment satisfaction | To assess the preference and satisfaction of the patient with osteoporosis treated with denosumab and alendronate | 1,653 patients. – RCT DECIDE: Denosumab: Mean age 64.1 years; Caucasian race 85% and mean years since menopause 16.5 Alendronate: Mean age 64.6 years; Caucasian race 84% and mean years since menopause 17.8 – RCT STAND: Denosumab: Mean age 66.9 years; Caucasian race 94% and mean years since menopause 18.8 Alendronate: Mean age 68.2 years; Caucasian race 92% and mean years since menopause 19.9 | A greater number of patients preferred subcutaneous injection every 6 months (63% with alendronate and 65% with denosumab) than the weekly pill (19%) (p < 0.001). There were significantly more patients more satisfied with the injection every 6 months than with the weekly pills (64%). Both younger (<65 years) and older (≥65 years) patients showed the same preferences or satisfaction with treatment, regardless of whether they had had a previous fracture or not. | [19] |
| 16 | Payer et al., 2009 (Slovakia)/5 | Cross-sectional observational/ preferences questionnaire | Patient preferences for osteoporosis treatments & treatment decision-making | Analyse the reasons why patients with postmenopausal osteoporosis prefer bisphosphonates once a month | 2,035 questionnaires were completed over a 3-month period by patients with a mean age of 64 years The mean duration of bisphosphonate treatment once a month was 9 months (SD 3) | The main reasons why patients chose the monthly dosing regimen were: convenience (69%), simplicity of treatment (59%) and need to take fewer pills (55%) The study also highlights that, in addition to the physician, patients seek alternative sources of information related to their disease/treatment such as friends (29%) and the media (28%). The information related to osteoporosis that the patients most demanded was general information (48%), information on the drug (44%), exercise (54%) and nutrition (51%). | [21] |
| 17 | Kastelan et al., 2009 (Croatia)/4 | Observational prospective multicenter/survey | Patient preferences for osteoporosis treatments & treatment satisfaction | Assess patient preferences for two bisphosphonate administration regimens (weekly vs monthly) | 258 women participated in the study, with a mean age of 66.2 years and 248 completed it | Most patients (94.7%) preferred the monthly regimen and the reasons were: better adjustment to their lifestyle (59.7%), preference for less frequent doses (53.6%) and ease of long-term compliance (53.6%). More than 85% of patients indicated that their quality of life had improved with the monthly dosage, while 9.3% indicated that they had not noticed any change. Of the 242 patients who answered the last question, 93.0% considered the monthly regimen more convenient than the weekly regimen. Satisfaction was significantly higher (on a scale of 0 to 10) for the frequency of monthly administration than for weekly administration (7 vs 8, p < 0.001). Compared with weekly regimen, monthly dosing was associated with significantly higher satisfaction with the treatment and with significantly less adverse events. | [20] |
| 18 | De Bekker-Grob et al., 2009 (Netherlands)/5 | Cross-sectional observational/DCE | Patient preferences for osteoporosis treatments | To evaluate and compare treatment preferences of physicians and patients | 40 physicians and 120 patients (women) with a mean age of 71.8 years | All treatment attributes proved to be important to the preferences of physicians and patients. Physicians attached significantly more importance to the effectiveness of drug treatment and shorter overall treatment duration than patients. The patients accepted less effective, longer-term pharmacological treatment if the treatment did not cause nausea and did not imply an economic cost for them. In general, patients have a more positive attitude towards preventive treatments than physicians. | [28] |
| 19 | Bonnick et al. 2009 (USA)/4 | Open multicenter RCT | Patient preferences for osteoporosis treatments & treatment satisfaction | To assess satisfaction and preferences for the treatment of postmenopausal women after a change of treatment from weekly to monthly oral bisphosphonates | 1,678 patients (women) – Race: white 1,595, black 44, other 39 – Average age: 65.9 years – Primary diagnosis: 64.5% osteoporosis, 35.5% osteopenia – Taking medication: 100% | 70.4% of patients showed an improvement in satisfaction at 6 months after the change of treatment, compared with the data at basal levels. Almost 85% of patients preferred monthly ibandronate treatment, 9.3% weekly treatment and 6.1% showed no preference. The most common reasons for choosing one treatment or another were improvement in lifestyle (monthly treatment: 69.8%; weekly: 64.7%) and ease of following treatment (monthly treatment: 73.5%; weekly: 63.2%). | [22] |
BMD: Bone mineral density; DCE: Discrete choice experiment; GI: Gastrointestinal; OP: Osteoporosis; RCT: Randomized clinical trial; SD: Standard deviation.
Characteristics of reviewed publications
Of the 19 selected publications, 14 (73.7%) corresponded to observational studies, four (21%) were clinical trials and one (5.3%) was a systematic review.
By geographical region, 11 (57.9%) of the publications were studies carried out in Europe, six (31.6%) in North America and two (10.5%) were works carried out internationally.
As regards the articles' level of evidence (LE), 12 (63.2%) had an LE of 5, three (15.8%) an LE of 4, three (15.8%) an LE of 3 and one (5.2%) an LE of 1.
What are the most valued characteristics of the treatment of osteoporosis from the patients' perspective?
Most of the articles reviewed (79%, n = 15) assessed patients' preferences regarding the characteristics of the treatments and explored, which were the most valued characteristics from patients' perspective. Of these, four used a discrete choice experiment (DCE) to establish preferences.
Ten main characteristics that defined treatment for osteoporosis were identified, including mode and frequency of administration, place of administration, convenience, monotherapy/combined therapy, adverse effects, efficacy, cost, the biological mechanism of action (stimulating bone formation or reducing bone resorption), time in the market and generic or original brand drug (Table 4).
| Author, year | Characteristics of the treatment evaluated | Ref. |
|---|---|---|
| Fobelo Lozano et al., 2019 | – Mode and frequency of administration – Convenience | [16] |
| Hiligsmann et al., 2017 | – Efficacy in reducing fracture risk (%) – Adverse effects (GI, flu-like, skin reactions) – Mode and frequency of administration – Monthly cost | [18] |
| Oral et al., 2015 | – Mode and frequency of administration | [24] |
| Neuner et al., 2014 | – Efficacy of treatment (reduction of fracture risk) – Adverse effects (atrial fibrillation, osteonecrosis of the jaw and gastric effects). – Mode and frequency of administration | [25] |
| Kendler et al., 2014 | – Mode and frequency of administration | [23] |
| Hiligsmann et al., 2014 | – Efficacy (reduction of fracture risk) – Cost – Mode and frequency of administration – Adverse effects (GI, flu-like, skin reactions). | [17] |
| Silverman et al., 2013 | – Efficacy of treatment (reduction of fracture risk, new bone formation, increased BMD) – Adverse effects (short- and long-term) – Convenience – Cost – Mode and frequency of administration | [26] |
| Hiligsmann et al., 2013 | – Efficacy (reduction of fracture risk %) – Adverse effects – Frequency of administration – Administration mode – Cost – Sequential therapy – Administration place – Time on the market – Brand/generic – Monotherapy/combined – Mode of action – Cost to society | [27] |
| Vlak et al., 2011 | – Adverse effects – Convenience | [30] |
| Darba et al., 2011 | – Efficacy – Mode and frequency of administration – Place of administration | [29] |
| Kendler et al., 2010 | – Administration mode and frequency | [19] |
| Payer et al., 2009 | – Convenience – Adverse effects | [21] |
| Kastelan et al., 2009 | – Mode and frequency of administration | [20] |
| De Bekker-Grob et al., 2009 | – Efficacy (reduction of hip fracture risk to 10 years) – Side effect (nausea) – Duration of treatment – Administration mode and frequency – Cost to the patient | [28] |
| Bonnick et al. 2009 | – Convenience – Adverse effects (GI, associated fractures, respiratory infection, arthralgia) – Frequency of administration | [22] |
BMD: Bone mineral density.
Most of the studies focused on evaluating the importance given by patients to the mode and frequency of treatment administration (n = 13), the associated AEs (n = 9) and treatment efficacy (n = 7). The importance attached to other treatment characteristics, such as treatment convenience (n = 5) and cost (n = 5) were also evaluated in several studies.
Although there was some heterogeneity between the studies as to which attributes had the greatest weight in patients' decisions, common trends were observed among them.
Regarding the mode and frequency of treatment administration, the results showed that patients gave greater importance to frequency than to the mode of administration, and preferred less frequent administration regimens, regardless of their mode of administration. Thus, monthly, six-monthly or annual administration was preferred to a weekly or daily dosage [16–23]. Specifically, the option most frequently chosen by patients was subcutaneous injection every 6 months, whereas the least frequently chosen was weekly oral tablets [18,19,23]. In fact, in a willingness to pay (WTP) analysis, patients were willing to pay €19.53 per month to switch from monthly oral to the subcutaneous regimen every 6 months [17]. In studies in which the preference for monthly or weekly regimens was studied, most patients chose monthly treatment. The most common reasons why patients chose these treatment regimens were: improved lifestyle, convenience, simplicity/easy-to-follow treatment and the need to take fewer pills [21,22,30]. In studies that assessed all treatment options through a DCE, the preferred choice over weekly oral tablets was subcutaneous injection every 6 months. Most patients also preferred monthly pills or annual intravenous injections over the option of weekly tablets. The least chosen option was intravenous injections every 3 months [17,18]. One of these studies also showed that there were significant differences in preferences regarding the frequency and mode of administration of treatment for osteoporosis between European countries [18].
In a study including two clinical trials, patients' preferences for one injection every 6 months or weekly pills were studied, based on different age groups (<65 and ≥65 years) and the presence of previous fractures. As a result, no significant differences were observed between subgroups. Thus, patients preferred injection every 6 months independently of their age or their history of fractures [19].
When the dosing schedule of monthly tablets (either fixed or flexible-dose type) was examined, no significant differences were seen in terms of preference for one or the other dosing schedule. However, persistence was greater in the flexible regimen. In the flexible regimen, patients preferred to take the medication before breakfast than between meals or before going to bed [24].
Patients attached great importance to adverse events, such as skin reactions, gastrointestinal (GI) problems, flu-like symptoms, osteonecrosis of the jaw and atrial fibrillation. In general, GI AEs were less desirable than skin reactions or flu-like symptoms [18]; in the WTP analysis, patients were willing to pay €25.20 per month to experience flu-like symptoms rather than GI symptoms [17]. Furthermore, patients considered GI symptoms to be important/very important, as well as osteonecrosis of the jaw or atrial fibrillation [25]. Besides, patients gave greater importance to long-term safety (health-related problems such as bone cancer, stroke, associated fractures, etc.) when compared with short-term safety (adverse effects such as skin reactions, flu-like symptoms or GI effects) [26].
The different studies used different measures to assess the efficacy attribute: reduction of the risk of fracture, increases in BMD, or new bone formation [17,18,25–28]. When assessed, patients attached the most significant importance to this attribute [18,26,27], and preferred effective and low-cost treatments [17]. In the WTP analysis, patients were willing to pay €3.73 per month to reduce the risk of fracture by 1% [17].
The cost was also evaluated in a variety of studies as an attribute to establish its impact on patients' treatment choice. In general, patients preferred treatments with a lower monthly cost [17,18,28]. The cost proposed in the different studies ranged from €0.00 to €60.00 per month. In the study conducted by Hiligsmann et al., whose objective was to explore the characteristics of the most important treatments for patients through nominal groups, the cost attribute was the fifth most important in a list of 12 items for patients, behind efficacy (1st), AEs (2nd), frequency of administration (3rd) and mode of administration (4th). Conversely, the cost of treatment for the society came in 12th position, being the attribute least valued by patients [27].
In an observational study that compared patients' and physicians' preferences, it was found that while physicians placed greater importance on treatment efficacy and shorter overall duration, patients were able to accept less effective, longer-term pharmacological treatment provided it did not cause nausea, and it did not involve any cost to them [28]. Furthermore, patients show a more positive attitude towards treatments than physicians [28]. However, in a DCE carried out in Spain, 46% of patients preferred a very effective treatment for reducing fractures despite being associated with adverse effects [29].
Other aspects were assessed to a lesser extent in the studies such as place of administration (home, outpatient, hospital). In one study, patients chose a daily or weekly versus annual treatment if it implied nonhospitalization. In the same study, it was also found that 55% of the patients considered it essential that the drug could be transported without the need for refrigeration [29].
What is the degree of patients' satisfaction with treatment?
Four studies reported data on treatment satisfaction. In general, patient satisfaction with treatment was significantly higher for treatments requiring less frequent administration. In three of the studies that analyzed satisfaction with treatment, weekly and monthly dosages were compared [20,22,30]. Patients' satisfaction increased after shifting from a weekly to a monthly regimen [22,30]. In line, in the study by Kendler et al. [19], results showed that patients were more satisfied with the six-monthly injection than with the weekly tablet, regardless of their age (<65 or ≥65 years) or the previous history of fractures (with or without previous fractures).
Greater satisfaction was usually associated with an improvement in patient-reported HRQoL, mainly because regimens with a lower frequency of administration involved greater convenience for patients [20,22]. Also, monthly dosages were associated with a lower incidence of AEs compared with weekly dosages. In a prospective observational study [20], 5.2% of patients taking bisphosphonate monthly reported AEs, while the figure rose to 22.2% in those taking medication weekly. The monthly dosage was the preferred option for 94.7% of patients. The reasons for this choice were: better adjustment in their lifestyle, preference for less frequent doses and ease of long-term compliance. Authors indicated that greater satisfaction with monthly administration was also associated with greater adherence [20].
What are their unmet needs regarding treatment decision-making?
Five studies evaluated several aspects of the treatment decision-making process. Results from these publications suggest that patients felt that they did not receive enough information to be able to make a properly informed decision. Specifically, they demand more information about the disease, the exercise and the type of diet recommended. Patients' education concerning their disease and treatment encouraged their involvement in decision-making about disease prevention or treatment [31]. Educational sessions also helped patients to understand the importance of lifestyle recommendations [31]. The information related to osteoporosis that the patients most demanded was: general information (48%), information on the drug (44%), exercise (54%) and nutrition (51%) [21].
Patients also remarked that before their diagnostic visit, they had not received sufficient information about the different therapeutic options to be able to raise doubts and/or concerns regarding medication [32].
A good physician–patient relationship helps patients to share their beliefs and doubts about treatments with physicians and to accept the suggestions/recommendations of the latter. In a qualitative phenomenological study, patients with a good relationship with their physicians found it easier to decide whether or not to take a medication, and this decision was made based on the professional's criteria. However, other patients considered that they needed additional information from the physician to convince them to take the medication. Decision-making was much more difficult for these patients [33].
Similarly, women's interaction with their physician appears to have a substantial impact on their views about osteoporosis and receptiveness to treatment. Thus, clear and explicit provider-patient communication about osteoporosis and osteoporosis treatment is important, beginning with the communication of the diagnosis and its implications [34].
Discussion
Shared decision-making between physician and patient is associated with increased treatment adherence and, therefore, better clinical results. Thus, the first step in shared decision-making is to determine patients' preferences and satisfaction with treatment. Although there is some heterogeneity across the studies regarding the attributes that have the greatest weight for patients' decision-making, the information collected in this review suggests that there are common trends, such as patients' preference for less frequent administration regimens; consideration of GI adverse effects as least desirable; and prioritizing efficiency and low cost.
Efficacy is one of the most relevant characteristics for patients. In fact, patients attached greatest importance to efficacy (measured as % reduction in fracture risk, new bone formation or increased BMD) in all the studies that included this attribute in the analysis. However, the importance attached to efficacy was related to patients' perception of the need for treatment or the risk of fracture, in addition to their previous experiences with the disease/treatment. Patients' perception that treatment is not effective, or not necessary, can negatively influence adherence. In this sense, when patients had a good understanding of the efficacy and safety of medications, it could positively impact the choice of treatment, as shown by various studies [35,36]. In one of them, when patients were previously informed about the differences in efficacy between weekly- and monthly-administered bisphosphonates, 82% preferred weekly risedronate that proved more efficacious at reducing the risk of hip, spine collarbone, pelvis, wrist and arm fracture, in contrast to monthly ibandronate, which only reduced the risk of spinal fractures [35]. Therefore, patients' education by healthcare personnel during the shared decision-making process can substantially improve treatment compliance and adherence. For this purpose, educational programs combined with reminder systems (email, telephone contacts) are very useful [37]. For example, a study on medication adherence showed that treatment adherence increased by 57% in a group of osteoporotic patients monitored by a nurse compared with a group without reminders [38].
Osteoporosis patients also attached great importance to the frequency of treatment administration and preferred simpler dosages, regardless of their mode of administration [16–22]. Specifically, patients' option of preference was a biannual subcutaneous injection, whereas the least preferred was weekly oral tablets [18,19]. When monthly or weekly regimens were compared, most patients chose monthly treatment, for reasons such as lifestyle improvement, convenience, simplicity/ease of the following treatment and the need to take fewer pills [21,22]. Less frequently administered treatments were also associated with greater patient satisfaction.
Overall, studies exploring patient satisfaction with the treatment received showed that they were more satisfied with treatments requiring less frequent administration, which was in line with their preferences [19,20,22,30]. These results would agree with studies carried out concerning other chronic and silent diseases, such as diabetes, in which patients preferred less frequent drug administration [39–43]. Thus, in two studies conducted in patients with Type 2 diabetes (Denmark and Sweden), the authors indicated that patients preferred one daily injection over multiple injections and they were willing to pay €38.00 per month in Denmark, and €14.10 in Sweden to avoid one injection per day (for example, 1 vs. 2 injections) [39,41].
Another important aspect for patients is the adverse effects of the treatment, especially GI ones [44–47]. AEs, along with the frequency of administration, play an essential role in treatment adherence. Different studies have shown that the onset of GI side effects is one of the main reasons for discontinuing treatment [44–46,48]. Specifically, in the POSSIBLE-US study, women with GI symptoms at the start of the study were 39% more likely to discontinue their medication within 6 months than those without GI symptoms. Furthermore, lower HRQoL and lower satisfaction with treatment were also observed in these patients [48]. In the study by Hamilton et al. [45], 76% of risedronate discontinuations due to AEs (19%) were due to GI AEs. In another study evaluating the AEs of raloxifene and alendronate, the most common AE that caused discontinuation was also GI disorders [46]. Goldshtein et al. [44] also identified GI AEs as the most common reason for changing or discontinuing oral bisphosphonates (40%). Among patients who were not taking any medication at the time of the study, 26.9% indicated that it was due to GI AEs that had previously caused them. For all the above, the authors conclude that it is essential to emphasize the need for new drugs with better GI tolerability [44].
Patients' satisfaction with treatment was directly associated with their preferences. Treatment that is in line with patient preferences (simpler dosages, mainly) will likely lead to greater satisfaction, and this in turn may lead to an improvement in treatment adherence [20,49]. This increase in satisfaction will be associated with an increase in patient-reported HRQoL, as less frequently administered treatments are more convenient [20,22].
Adherence to osteoporosis medication is crucial to prevent the burden of the disease, both for the patient and their family and society [50]. However, compliance with and adherence to osteoporosis treatment are often inadequate, leading to suboptimal health outcomes, including an increased risk of fracture [49]. As seen above, adherence to treatment among patients with chronic conditions can be influenced by many factors, including the patient's beliefs, preferences and satisfaction with the prescribed treatment. Therefore, it is crucial to bear in mind that, in osteoporosis, as in other chronic and silent diseases, such as hypertension, decision-making about treatment must be aligned to the patient's preferences, since chronic patients must follow lifelong treatment; for this reason, compliance with and medication adherence is very important in these cases [49,51].
Currently, the trend toward patient-centered medicine is characterized by a greater emphasis on the patient's experience rather than their illness, and a more active role for patients in decision-making. Hence, the clinician is increasingly responsible for finding out what patients want, to help them find the right information and support them in the decision-making process [52]. In this review, we have seen that generally speaking, patients feel they do not receive enough information to make a properly informed decision [31,32]. Evidence suggests that patients' education on the different treatment options had a positive impact on their participation in decision-making about the management of the disease [31]. A good physician–patient relationship helps patients to share their beliefs and doubts about treatments with their physician and to accept the suggestions/recommendations of the latter [53,54]. Different studies suggest that to maximize adherence, healthcare providers must understand patients' perceptions of medication, including their belief in the need for treatment and concerns about the adverse effects it may cause [50,55].
The decision support process typically involves a combination of consultation, counselling and decision support tools, providing information on options and outcomes and clarifying each patient's fears [31]. Different studies have shown that decision-making tools increase patients' knowledge about the options available for managing osteoporosis and help them clarify their preferences [56,57]. As has been shown in the reviewed studies, discrete choice questionnaires are very useful to determine patients' preferences and help establish appropriate treatment based on their priorities. Given the high degree of heterogeneity observed about the importance given by patients to each attribute [17], it would be very useful to include tools to help shared decision-making in medical consultations that allow identifying patient preferences. Nowadays, eleven decision support tools are available to inform patient decisions about osteoporosis treatment [57]. Only four of them have proved their clinical effectiveness [57], showing the need to focus further on assessing these tools' effectiveness.
Limitations
This review has several limitations, some of them typical of systematic reviews, such as publication bias. Such bias is due to the fact that many scientific works, especially those with ‘negative’ results (against the hypothesis of the study or what is commonly established) either do not get published or are published in bibliographic sources of less importance than those used. Other limitations are the restriction to papers published in Spanish or English and time horizon (10 years), leading studies with relevant results published in another language or before or/and after the time horizon to being overlooked. Several articles can have been published from review completion (January 1, 2019) to publication.
Despite these limitations, the systematic review is the ideal tool to identify the best available evidence on a topic of interest since, during its development, critical and objective reading of the works included is carried out, at the same time assessing the methodological quality of the selected publications and correctly interpreting the results.
Conclusion
In all the studies that included the efficacy attribute in the analysis, patients awarded it the greatest importance. Regarding mode and frequency administration, the literature reviewed suggests that patients preferred less frequent doses of medication (biannual or monthly) to weekly or daily dosages. GI AEs, meanwhile, may predispose patients to early discontinuation of treatment and, in turn, such AEs are associated with lower HRQoL and satisfaction with treatment.
Differences in preferences were found between patients, underscoring the importance of considering the preferences of individual patients in clinical decision-making. Aligning treatment with patients' preferences can improve patients' satisfaction and adherence to the medication, both of which are of particular importance in the treatment of a chronic condition that requires long-term treatment.
A clear and explicit physician–patient communication about osteoporosis and osteoporosis treatment is crucial to promote patient involvement in the decision-making process. To identify the patient's doubts and concerns about treatment and address them can subsequently improve adherence and ultimately achieve treatment goals in fracture reduction.
•
Most of the articles reviewed (79%, n = 15) assessed patients' preferences regarding the characteristics of the treatments (mode and frequency of treatment administration (n = 13), AEs (n = 9), treatment efficacy (n = 7), treatment convenience (n = 5) and cost (n = 5) and explored which were the most valued characteristics from patients' perspective.
•
Although there is some heterogeneity across the study's results, the information collected in this review suggests that patients prefer less frequent administration regimens; GI adverse effects are least desirable and prioritize efficiency and low cost.
•
Patient satisfaction with treatment was significantly higher for treatments requiring less frequent administration.
•
A good physician–patient relationship helps patients to share their beliefs and doubts about treatments with physicians and to accept the suggestions/recommendations of the latter, thus improving persistence with and medication adherence.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_file.docx)
- Download
- 16.25 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am. J. Med. 94(6), 646–650 (1993).
2.
Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ. Tech. Rep. Ser. 843, 1–129 (1994).
3.
Hernlund E, Svedbom A, Ivergard M et al. Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch. Osteoporos. 8, 136 (2013).
4.
Rizzoli R. Postmenopausal osteoporosis: assessment and management. Best Pract. Res. Clin. Endocrinol. Metab. 32(5), 739–757 (2018).
5.
Kim SC, Kim M-S, Sanfélix-Gimeno G et al. Use of osteoporosis medications after hospitalisation for hip fracture: a cross-national study. Am. J. Med. 128(5), 519–526.e511 (2015).
6.
Lems WF, Dreinhofer KE, Bischoff-Ferrari H et al. EULAR/EFORT recommendations for management of patients older than 50 years with a fragility fracture and prevention of subsequent fractures. Ann. Rheum. Dis. 76(5), 802–810 (2017).
7.
Vidal M, Thibodaux RJ, Neira LFV, Messina OD. Osteoporosis: a clinical and pharmacological update. Clin. Rheumatol. 38(2), 385–395 (2019).
8.
Sacristan JA. Patient-centered medicine and patient-oriented research: improving health outcomes for individual patients. BMC Med. Inform. Decis. Mak. 13, 6 (2013).
• Provides background for patient-centered medicine.
9.
Barry MJ, Edgman-Levitan S. Shared decision making–pinnacle of patient-centered care. N. Engl. J. Med. 366(9), 780–781 (2012).
10.
Reginster JY, Rabenda V, Neuprez A. Adherence, patient preference and dosing frequency: understanding the relationship. Bone 38, S2–S6 (2006).
11.
Lewiecki EM. Risk communication and shared decision making in the care of patients with osteoporosis. J. Clin. Densitom. 13(4), 335–345 (2010).
12.
Alami S, Hervouet L, Poiraudeau S, Briot K, Roux C. Barriers to effective postmenopausal osteoporosis treatment: a qualitative study of patients' and practitioners' views. PLoS OME 11(6), e0158365 (2016).
13.
Hiligsmann M, Bours SPG, Boonen A. A review of patient preferences for osteoporosis drug treatment. Curr. Rheumatol. Rep. 17(6), 61 (2015).
14.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535 (2009).
15.
OCEBM Levels of Evidence Working Group. The Oxford 2011 Levels of Evidence. Oxford Centre for Evidence-Based Medicine. Available at: www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence
16.
Fobelo Lozano MJ, Sanchez-Fidalgo S. Adherence and preference of intravenous zoledronic acid for osteoporosis versus other bisphosphonates. Eur. J. Hosp. Pharm. Sci. Pract. 26(1), 4–9 (2019).
•• Reviews preferences and satisfaction with once-yearly intravenous zoledronic acid treatment versus another bisphosphonate.
17.
Hiligsmann M, Dellaert BG, Dirksen CD et al. Patients' preferences for osteoporosis drug treatment: a discrete-choice experiment. Arthritis Res. Ther. 16(1), R36 (2014).
18.
Hiligsmann M, Dellaert BG, Dirksen CD et al. Patients' preferences for anti-osteoporosis drug treatment: a cross-European discrete choice experiment. Rheumatology (Oxford) 56(7), 1167–1176 (2017).
•• This discrete choice experiment estimates and compare the preferences of patients with osteoporosis by the attributes of the treatments in eight European countries.
19.
Kendler DL, Bessette L, Hill CD et al. Preference and satisfaction with a 6-month subcutaneous injection versus a weekly tablet for treatment of low bone mass. Osteoporos. Int. 21(5), 837–846 (2010).
•• Study that assesses the preference and satisfaction of patients with osteoporosis treated with denosumab and alendronate.
20.
Kastelan D, Lozo P, Stamenkovic D et al. Preference for weekly and monthly bisphosphonates among patients with postmenopausal osteoporosis: results from the Croatian PROMO Study. Clin. Rheumatol. 28(3), 321–326 (2009).
•• Compares weekly vs. monthly administration regimens.
21.
Payer J, Cierny D, Killinger Z, Sulkova I, Behuliak M, Celec P. Preferences of patients with post-menopausal osteoporosis treated with bisphosphonates–the VIVA II study. J. Int. Med. Res. 37(4), 1225–1229 (2009).
22.
Bonnick SL, Silverman S, Tanner SB et al. Patient satisfaction in postmenopausal women treated with a weekly bisphosphonate transitioned to once-monthly ibandronate. J. Womens Health (Larchmt.) 18(7), 935–943 (2009).
23.
Kendler DL, Macarios D, Lillestol MJ et al. Influence of patient perceptions and preferences for osteoporosis medication on adherence behavior in the Denosumab Adherence Preference Satisfaction study. Menopause 21(1), 25–32 (2014).
24.
Oral A, Lorenc R. Compliance, persistence, and preference outcomes of postmenopausal osteoporotic women receiving a flexible or fixed regimen of daily risedronate: a multicenter, prospective, parallel group study. Acta Orthop. Traumatol. Turc. 49(1), 67–74 (2015).
25.
Neuner JM, Schapira MM. Patient perceptions of osteoporosis treatment thresholds. J. Rheumatol. 41(3), 516–522 (2014).
26.
Silverman S, Calderon A, Kaw K et al. Patient weighting of osteoporosis medication attributes across racial and ethnic groups: a study of osteoporosis medication preferences using conjoint analysis. Osteoporos. Int. 24(7), 2067–2077 (2013).
27.
Hiligsmann M, Van Durme C, Geusens P et al. Nominal group technique to select attributes for discrete choice experiments: an example for drug treatment choice in osteoporosis. Patient Prefer. Adherence 7, 133–139 (2013).
•• Shows the most important attributes for patients in osteoporosis treatment in order from 1 to 12.
28.
De Bekker-Grob EW, Essink-Bot ML, Meerding WJ, Koes BW, Steyerberg EW. Preferences of GPs and patients for preventive osteoporosis drug treatment: a discrete-choice experiment. Pharmacoeconomics 27(3), 211–219 (2009).
29.
Darba J, Restovic G, Kaskens L et al. Patient preferences for osteoporosis in Spain: a discrete choice experiment. Osteoporos. Int. 22(6), 1947–1954 (2011).
30.
Vlak T, Kastelan D, Lozo P et al. Monthly or weekly bisphosphonate? Evaluation of satisfaction in patients with postmenopausal osteoporosis using OPSAT-Q questionnaire during the BOOSTER study in Croatia. Clin. Rheumatol. 30(12), 1549–1554 (2011).
31.
Jensen AL, Wind G, Langdahl BL, Lomborg K. The impact of multifaceted osteoporosis group education on patients' decision-making regarding treatment options and lifestyle changes. J. Osteoporos. 2018, 9703602 (2018).
32.
Jakobsen PR, Hermann AP, Sondergaard J, Wiil UK, Dixon RF, Clemensen J. Left in limbo – experiences and needs among postmenopausal women newly diagnosed with osteoporosis without preceding osteoporotic fractures: a qualitative study. Post. Reprod. Health 24(1), 26–33 (2018).
33.
Sale JE, Gignac MA, Hawker G et al. Decision to take osteoporosis medication in patients who have had a fracture and are ‘high’ risk for future fracture: a qualitative study. BMC Musculoskelet. Disord. 12, 92 (2011).
34.
Mazor KM, Velten S, Andrade SE, Yood RA. Older women's views about prescription osteoporosis medication: a cross-sectional, qualitative study. Drugs Aging 27(12), 999–1008 (2010).
35.
Gold DT, Safi W, Trinh H. Patient preference and adherence: comparative US studies between two bisphosphonates, weekly risedronate and monthly ibandronate. Curr. Med. Res. Opin. 22(12), 2383–2391 (2006).
36.
Keen R, Jodar E, Iolascon G et al. European women's preference for osteoporosis treatment: influence of clinical effectiveness and dosing frequency. Curr. Med. Res. Opin. 22(12), 2375–2381 (2006).
37.
Silverman SL, Gold DT. Compliance and persistence with osteoporosis therapies. Curr. Rheumatol. Rep. 10(2), 118–122 (2008).
38.
Clowes JA, Peel NFA, Eastell R. The impact of monitoring on adherence and persistence with antiresorptive treatment for postmenopausal osteoporosis: A randomized controlled trial. J. Clin. Endocrinol. Metab. 89(3), 1117–1123 (2004).
39.
Bogelund M, Vilsboll T, Faber J, Henriksen JE, Gjesing RP, Lammert M. Patient preferences for diabetes management among people with type 2 diabetes in Denmark – a discrete choice experiment. Curr. Med. Res. Opin. 27(11), 2175–2183 (2011).
40.
Boye KS, Matza LS, Walter KN, Van Brunt K, Palsgrove AC, Tynan A. Utilities and disutilities for attributes of injectable treatments for type 2 diabetes. Eur. J. Health Econ. 12(3), 219–230 (2011).
41.
Jendle J, Torffvit O, Ridderstrale M, Lammert M, Ericsson A, Bogelund M. Willingness to pay for health improvements associated with anti-diabetes treatments for people with type 2 diabetes. Curr. Med. Res. Opin. 26(4), 917–923 (2010).
42.
Fifer S, Rose J, Hamrosi KK, Swain D. Valuing injection frequency and other attributes of type 2 diabetes treatments in Australia: a discrete choice experiment. BMC Health Serv. Res. 18(1), 675 (2018).
43.
Rydén A, Chen S, Flood E, Romero B, Grandy S. Discrete choice experiment attribute selection using a multinational interview study: treatment features important to patients with Type 2 diabetes mellitus. Patient 10(4), 475–487 (2017).
44.
Goldshtein I, Rouach V, Shamir-Stein N, Yu J, Chodick G. Role of side effects, physician involvement, and patient perception in non-adherence with oral bisphosphonates. Adv. Ther. 33(8), 1374–1384 (2016).
45.
Hamilton B, Mccoy K, Taggart H. Tolerability and compliance with risedronate in clinical practice. Osteoporos. Int. 14(3), 259–262 (2003).
46.
Turbí C, Herrero-Beaumont G, Cebes J et al. Compliance and satisfaction with raloxifene versus alendronate for the treatment of postmenopausal osteoporosis in clinical practice: an open-label, prospective, nonrandomized, observational study. Clin. Therapeut. 26(2), 245–256 (2004).
47.
Modi A, Sen S, Adachi JD et al. Gastrointestinal symptoms and association with medication use patterns, adherence, treatment satisfaction, quality of life, and resource use in osteoporosis: baseline results of the MUSIC-OS study. Osteoporos. Int. 27(3), 1227–1238 (2016).
48.
Woo C, Gao G, Wade S, Hochberg MC. Gastrointestinal side effects in postmenopausal women using osteoporosis therapy: 1-year findings in the POSSIBLE US study. Curr. Med. Res. Opin. 26(4), 1003–1009 (2010).
49.
Freemantle N, Satram-Hoang S, Tang ET et al. Final results of the DAPS (Denosumab Adherence Preference Satisfaction) study: a 24-month, randomised, crossover comparison with alendronate in postmenopausal women. Osteoporosis Int. 23(1), 317–326 (2012).
50.
Hall SF, Edmonds SW, Lou Y et al. Patient-reported reasons for nonadherence to recommended osteoporosis pharmacotherapy. J. Am. Pharm. Assoc. 57(4), 503–509 (2017).
51.
Montgomery AA, Harding J, Fahey T. Shared decision making in hypertension: the impact of patient preferences on treatment choice. Fam. Pract. 18(3), 309–313 (2001).
52.
Krahn M, Naglie G. The next step in guideline development: incorporating patient preferences. JAMA 300(4), 436–438 (2008).
53.
Iversen MD, Vora RR, Servi A, Solomon DH. Factors affecting adherence to osteoporosis medications: a focus group approach examining viewpoints of patients and providers. J. Geriatr. Phys. Ther. 34(2), 72–81 (2011).
54.
Kendler D, Lillestol MJ, Moffett AH et al. Influence of patient perceptions and preferences about osteoporosis medication on adherence in the denosumab adherence, preference, and satisfaction (DAPS) study. Menopause 19(12), 1390 (2012).
55.
Cranney A, O'connor AM, Jacobsen MJ et al. Development and pilot testing of a decision aid for postmenopausal women with osteoporosis. Patient Educ. Couns. 47(3), 245–255 (2002).
56.
Montori VM, Shah ND, Pencille LJ et al. Use of a decision aid to improve treatment decisions in osteoporosis: the osteoporosis choice randomised trial. Am. J. Med. 124(6), 549–556 (2011).
57.
Paskins Z, Torres Roldan VD, Hawarden AW et al. Quality and effectiveness of osteoporosis treatment decision aids: a systematic review and environmental scan. Osteoporos. Int. 31(10), 1837–1851 (2020).
Information & Authors
Information
Published In
Pages: 629 - 645
PubMed: 33880940
Copyright
© 2021 Future Medicine Ltd.
History
Received: 1 October 2020
Accepted: 12 March 2021
Published online: 21 April 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Preferences, satisfaction and decision-making processes in osteoporosis treatment: a systematic review of the literature. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0216
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- M Premikha, Valentina Ricci, Shu Jun Kan, Phyllis Kim, Translating evidence into primary care: Singapore’s 2025 national osteoporosis guideline and a multilevel framework for assessing guideline impact in mixed health systems, Family Medicine and Community Health, 10.1136/fmch-2025-003802, 14, 3, (e003802), (2026).
- Xavier Nogués Solán, Diana Ovejero, Carmen Gimenez-Argente, Jaime Rodríguez-Morera, Abora Rial-Villavecchia, Eloi García-Vives, María Lourdes Cos, Jade Soldado-Folgado, Mariona Llaberia, Ariadna Brasé Arnau, Irene Petit, Rosa Ana Sabaté, Jose María Mora-Luján, Charlotte Beaudart, Stuart Silverman, Mickael Hiligsmann, Natalia Garcia-Giralt, Preferences of Spanish-speaking patients for communicating fracture risk in osteoporosis. A substudy of the Risk Communication in Osteoporosis study (RICO Study), Revista de Osteoporosis y Metabolismo Mineral, 10.20960/RevOsteoporosMetabMiner.00048, (2024).
- Kyriakos Souliotis, Christina Golna, Christina Poimenidou, Tatiana Drakopoulou, Memi Tsekoura, Damon Willems, Vasileios Kountouris, Polyzois Makras, Disease Burden and Treatment Preferences Amongst Postmenopausal Women with Severe Osteoporosis in Greece, Patient Preference and Adherence, 10.2147/PPA.S385351, Volume 17, (107-118), (2023).