The effect of midodrine on lactate clearance in patients with septic shock: a pilot study
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: The effect of midodrine on lactate clearance has not been assessed in critically ill patients yet. Objective: The goal of this study was to assess the effect of adjunctive midodrine therapy on lactate clearance in patients with septic shock. Materials & methods: Patients with septic shock were assigned to receive either adjunctive midodrine 10 mg three-times a day for 5 days (midodrine group = 15 patients) or not (control group = 13 patients). Results: The lactate clearance was significantly faster in the midodrine group than the control group (p = 0.049) with a large effect size ( = 0.141). Conclusion: When midodrine was added to intravenous vasopressors, it significantly accelerated lactate clearance in patients with septic shock.
Trial registration number: IRCT20100228003449N25 (Clinicaltrials.gov).
Septic shock is a major cause of death in critically ill patients [1]. It also can lead to multi-organ failure [2]. The burden of septic shock is considerable and more than 25,000 dollars for each patient was paid, while the mortality rate is estimated to be more than 50% [3,4].
The pathophysiology of septic shock is complex. Hypovolemia, decreased systemic vascular resistance and myocardial depression are main known pathologic events in septic shock [5]. These finally cause persistent hypotension and high levels of serum lactate that may not be corrected only by fluid resuscitation. Increased serum lactate level is a sign of tissue hypoxemia.
Serum lactate level was proposed as a predictor of complications and mortality in sepsis and septic shock [6]. Later, serial lactate assay was proposed over single serum lactate measurement [7] and lactate clearance has been accepted as an indicator of adequate fluid resuscitation in sepsis [8]. Compared with the earlier markers like central venous oxygen saturation, was more accurate in evaluating effectiveness of fluid therapy in patients with sepsis [9].
According to the latest Surviving Sepsis Campaign; international guidelines for management of sepsis and septic shock; the vasopressor of choice in treatment of septic shock is norepinephrine [10]. If the desired response is not attained, vasopressin or epinephrine can be added. Vasopressor therapy is almost accompanied with various adverse effects. Decreased organ perfusion and tissue ischemia due to excessive vasoconstriction, hyperglycemia, hyperlactatemia and tachyarrhythmia are common [11]. Selection of an appropriate vasopressor in patients with septic shock is a challenging issue [12].
Oral vasopressors may be potential options in management of sepsis and septic shock [13]. Midodrine is an oral vasopressor with alpha-agonist activity that has been approved for management of orthostatic hypotension. It has also shown promising results in management of intradialytic hypotension, hepato-renal syndrome and hypotension in patients with cirrhosis [14]. Recently, it is proposed as an oral vasopressor in management of sepsis and septic shock [15,16]. In patients with septic shock, midodrine decreased intravenous vasopressor requirement and length of intensive care unit (ICU) stay [17,18]. However, the effect of midodrine on the lactate clearance has not been assessed in critically ill patients. The goal of this study was to assess the effect of adjunctive midodrine on the lactate clearance in patients with septic shock.
Materials & methods
Study design
This pilot study was performed in General ICU of Imam Khomeini Hospital Complex, Tehran, Iran, from September 2019 to July 2020. Ethics Committee of Tehran University of Medical Sciences approved the study (IR.TUMS.TIPS.REC.1398.042). This study was registered as a clinical trial (IRCT20100228003449N25).
Patient recruitment
Adult patients (≥18 years old) with diagnosis of septic shock who required intravenous vasopressor to maintain mean arterial blood pressure (MAP) ≥65 mmHg were considered. Persistent hypotension, MAP <65 mmHg and serum lactate level ≥2 mg/dl despite fluid resuscitation was considered as septic shock [10]. Patients were eligible when signed the informed consent documents. If a patient was unconscious, one of the responsible family members signed the informed consent form. Patients who had either of following conditions were excluded; 24 h or more was passed since the diagnosis of septic shock, chronic kidney disease with glomerular filtration rate less than 30 ml/min, neurogenic bladder and urination disorders, peripheral arterial diseases, sclerodermia, heart rate less than 60 beats per min and receiving midordrine before for any other reasons. Patients were randomly assigned to either midodrine or control group according to the simple randomization method.
Treatment protocol
The fluid resuscitation in the first 3 h of the diagnosis of septic shock was done using isotonic saline. Infusion of norepinephrine (NEP) was started at the dose of 10 mcg/min and then was adjusted to maintain MAP above 65 mmHg. Patients in the midodrine group received oral midodrine (10 mg three-times daily) in addition to NEP for up to 5 days. Conscious patients received midodrine orally. For other patients the tablets were crushed and administered through nasogastric tube. Patients in the control group received only NEP.
When fluid and vasopressor therapy were not successful to maintain MAP above 65 mmHg, intravenous hydrocortisone at dose of 200 mg/day in four equally divided doses was added to the treatment regimen. Broad-spectrum antimicrobials were started within the first 3 h of the study considering probable sources of infection. The antimicrobials were de-escalated according to the clinical status of the patients and microbial culture results in the next steps.
Stress ulcer prophylaxis was considered for patients who were on mechanical ventilation for more than 48 h or had coagulopathy (international normalized ratio >1.5, or partial thromboplastin time >two-times the baseline value, platelet count <50,000/μl) or other high-risk conditions [19]. Need for venous thromboembolism prophylaxis was assessed by Padua score [20]. If a patient required analgesic, acetaminophen was considered at first. The next step for analgesia was oral or intravenous opioids. If indicated, fentanyl infusion was stared for sedation. Sedation was adjusted to achieve 0 to -1 score in the Richmond sedation and agitation scale [21].
Calorie requirement of the patients with considering the baseline physiologic stress levels was targeted between 20 and 35 kcal/kg/day. Enteral feeding was considered as preferred route for metabolic support. Prokinetics such as metoclopramide was administered if required. If enteral feeding was not possible, parenteral nutrition was considered.
Data collection
Patients’ demographic characteristics, baseline comorbidities, suspected sources of infection, laboratory data including initial and serial serum lactate values, cell blood count, electrolytes, liver and kidney function tests, inflammatory markers, microbial cultures and outcomes were recorded. Also, vital signs and hemodynamic parameters were closely monitored in daily interval during the study period. All medications and events were recorded during the ICU stay.
Outcome assessment
Lactate clearance was considered as the primary outcome of the study. Serum lactate measurements were considered at baseline and 4, 24 and 28 h after. Nova Stat Strip Xpress Lactate Meters was used for serum lactate measurement. The measurement is through an electrochemical sensor by mixing blood sample with lactate oxidaze. While chemical reaction happens, an electric current is started. Lactate concentration determines the amount of current. The strips detect lactate levels in range of 2.7–180 mg/dl (0.3–20 mmol/l). Lactate measurements were strongly correlated with the reference values (r = 0.92–0.97). Lactate clearance was calculated by the formula below:
Secondary outcome was dose of vasopressor during the intervention period. Also, complications and clinical events during the ICU stay were recorded. Acute kidney injury was defined according to the KDIGO guideline [22]. Hepatic impairment was described as hepatic aminotransferases serum levels above three-times the upper limit of normal or serum total bilirubin above 2 mg/dl [23]. Thrombocytopenia was considered as platelet count below 20,000/μl. Anemia was also defined as hemoglobin below 7 mg/dl. Leukocytosis was regarded as white blood cell count above 12,000 cells/μl.
Patients were followed for 28 days and length of ICU stay and 28-day mortality was reported.
Statistical analysis
Continuous variables were reported as median and interquartile range. Nominal variables were reported as percentage (%). For comparing continuous variables, normal distribution was assessed by Kolmogorov–Smirnov test. If the test was passed, independent sample t-test was performed. Otherwise, Mann–Whitney test was used. Nominal variables were compared by Chi-square test.
The analysis was performed on ‘intention-to-treat’ basis. Lactate clearance was calculated for 0–4, 4–24 and 24–28 h intervals. Repeated measurement analysis of variance was applied to compare changes in the variables during the intervention period. The effect size was calculated as partial Eta squared (). Considering lactate clearance as primary outcome, number of patients in each group, mean changes of lactate clearance and Type 1 error (α = 0.05), power of the study was calculated. All data analyses were conducted using SPSS software (version 21.0).
Results
In the study period 15 patients in the midodrine group and 13 patients in the control group completed the trial (Figure 1). The median age of patients in the midodrine and control group was 58 and 57 years, respectively. Cardiovascular diseases and diabetes mellitus were among the most common comorbidities in both groups. Other baseline characteristics are shown in Table 1.
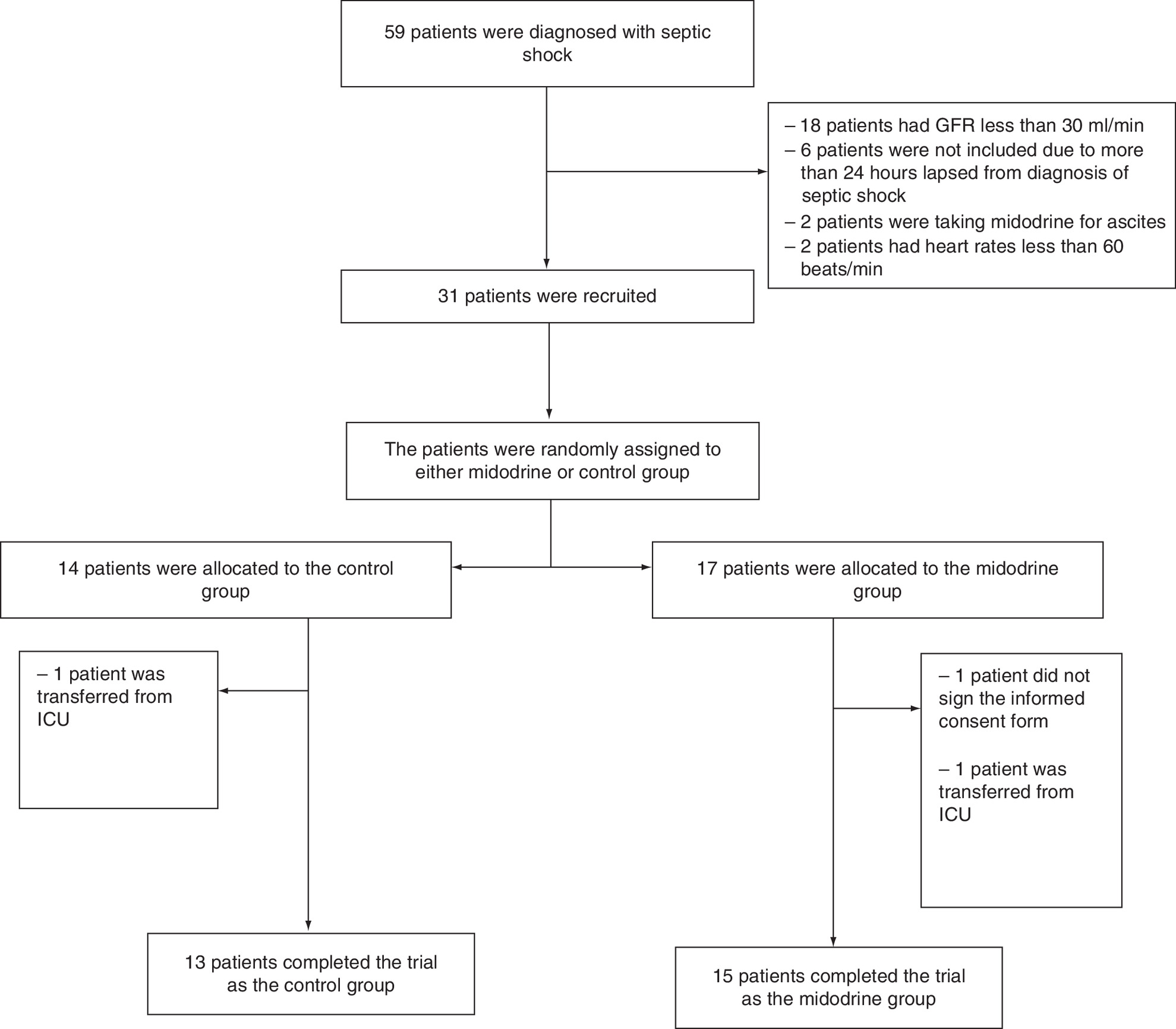
Figure 1. Consort flowchart of study.
GFR: Glomerular filtration rate; ICU: Intensive care unit.
| Parameter | Midodrine group (n = 15), median (IQR) | Control group (n = 13), median (IQR) | p-value |
|---|---|---|---|
| Age (year) | 58 (50–70) | 57 (46–70) | 0.34 |
| Height (cm) | 165 (155–170) | 170 (162–176) | 0.36 |
| Weight (kg) | 70 (65–95) | 75 (70–87) | 0.19 |
| BMI | 27 (20–29) | 25 (24–30) | 0.28 |
| Gender | Male: 8 (53.3) female: 7 (46.7) | Male: 6 (46.2) female: 7 (53.8) | 0.50 |
| Habitual history, n (%) | |||
| – Smoking | 3 (20.0) | 3 (23.1) | 0.60 |
| – Opium | 4 (26.7) | 2 (15.4) | 0.40 |
| – Alcohol | 0 | 0 | - |
| – Drug abuse | 0 | 0 | - |
| Baseline diseases, n (%) | |||
| – Diabetes mellitus | 3 (20) | 5 (38.5) | 0.25 |
| – Cardiovascular diseases | 5 (33.3) | 4 (30.8) | 0.60 |
| – Hypertension | 4 (26.7) | 6 (46.2) | 0.24 |
| – Endocrine disease | 1 (6.7) | 1 (7.7) | 0.72 |
| – Rheumatologic disease | 1 (6.7) | 0 | 0.53 |
| – Renal disease | 2 (13.3) | 4 (30.8) | 0.25 |
| – Liver disease | 4 (26.7) | 3 (23.1) | 0.58 |
| – Respiratory disease | 1 (6.7) | 2 (15.4) | 0.55 |
| – Neuropsychiatric disease | 1 (6.7) | 2 (15.4) | 0.44 |
| – Malignancy | 4 (26.7) | 1 (7.7) | 0.21 |
| – Transplant | 1 (6.7) | 0 | 0.53 |
| – Hematologic disease | 0 | 0 | – |
| Past drug history, n (%) | |||
| – ARB | 5 (33.3) | 4 (30.8) | 0.60 |
| – Beta-blocker | 3 (20) | 7 (53.8) | 0.07 |
| – Metformin | 0 | 2 (15.4) | 0.20 |
| – Insulin | 1 (6.7) | 0 | 0.53 |
| – ASA | 2 (13.3) | 3 (23.1) | 0.42 |
| – NSAIDs | 0 | 1 (7.7) | 0.46 |
| – Corticostroide | 1 (6.7) | 1 (7.7) | 0.72 |
| – Immunosuppressant | 4 (26.7) | 0 | 0.06 |
| – Antibiotics (within past three months) | 3 (20) | 4 (30.8) | 0.41 |
ARB: Angiotensin receptor blocker; ASA: Aspirin; IQR: Interquartile range; NSAID: Nonsteroidal anti-inflammatory drug.
Mean ± standard deviation (SD) of acute physiology and chronic health evaluation II (APACHE II) score at the time of inclusion was 17.06 ± 3.15 in the midodrine group and 16.15 ± 4.01 in the control group (p = 0.10). Also, mean ± SD of baseline sequential organ failure assessment (SOFA) score was 7.50 ± 2.17 in the midodrine group and 8.30 ± 2.25 in the control group (p = 0.99).
Most patients admitted to ICU for postoperative care. Other causes of ICU admission were respiratory failure, decreased level of consciousness and trauma. The probable sources of sepsis were investigated in all patients, although sometimes it was not possible to find the reason (Table 2). No significant difference was between the groups regarding the reasons for ICU admission and sources of sepsis.
| Variable | Midodrine group (n = 15), n (%) | Control group (n = 13), n (%) | p-value |
|---|---|---|---|
| Pneumonia | 1 (6.7) | 5 (38.5) | 0.056 |
| Bacteremia | 1 (6.7) | 0 | 0.53 |
| Intra-abdominal infection | 9 (60) | 7 (53.8) | 0.52 |
| Urinary infection | 1 (6.7) | 0 | 0.53 |
| Fungal infection | 1 (6.7) | 0 | 0.53 |
| Other causes | 2 (13.4) | 1 (7.7) | 0.35 |
Baseline patients’ laboratory data are shown in Table 3. There was no significant difference in terms of the laboratory tests between the groups. The medications that were administered during ICU stay are listed in Table 4. As it is expected, antibiotics are among the frequently administered medications. Data about isolated microorganisms are also summarized in Table 5.
| Lab data | Midodrine group (n = 15), median (IQR) | Control group (n = 13), median (IQR) | p-value |
|---|---|---|---|
| WBC (106/l) | 13,500 (5400–18,700) | 9600 (5300–12,600) | 0.57 |
| Hb (g/l) | 9.7 (8.7–11.4) | 9.9 (9.15–11.25) | 0.83 |
| Plt (109/l) | 252 (161–301) | 205 (100–288.5) | 0.24 |
| Urea (mg/dl) | 49 (29–76) | 69 (43–99) | 0.095 |
| SrCr (mg/dl) | 1.2 (0.9–1.7) | 1.3 (0.85–1.95) | 0.95 |
| Na (mEq/l) | 138 (135–140) | 140 (135–143) | 0.38 |
| K (mEq/l) | 4 (3.5–4.2) | 4 (3.2–4.3) | 0.80 |
| Ca (mg/dl) | 8.2 (7.85–9.05) | 7.5 (7.2–8.3) | 0.15 |
| P (mg/dl) | 3.8 (2.85–4.5) | 3 (2.4–3.6) | 0.056 |
| Mg (mg/dl) | 2.2 (1.8–2.5) | 2.05 (1.8–2.3) | 0.30 |
| AST (U/l) | 33 (29–127) | 21 (17–35) | 0.12 |
| ALT (U/l) | 26 (14–45) | 17 (13–28) | 0.33 |
| Bilirubin (mg/dl) | 1.1 (0.6–2.2) | 0.9 (0.55–1.15) | 0.11 |
| INR | 1.44 (1.26–1.70) | 1.7 (1.37–2.10) | 0.98 |
| Alb (g/dl) | 2.75 (2.17–3.20) | 2.80 (2.50–3.05) | 0.65 |
| ESR (mm/h) | 32 (13–98) | 22 (3–87) | 0.60 |
| CRP (mg/l) | 72 (40–118) | 66 (40–126) | 0.78 |
| PCT (ng/ml) | 7.2 (0.63–15.8) | 3.8 (0.55–12.84) | 0.45 |
ESR: Erythrocyte sedimentation rate; Hb: Hemoglobin; INR: International normalized ratio; IQR: Interquartile range; Plt: Platelet; SrCr: Serum creatinine; WBC: White blood cell count.
| Medication | Midodrine group (n = 15), n (%) | Control group (n = 13), n (%) | p-value |
|---|---|---|---|
| PPI | 15 (100) | 13 (100) | – |
| Heparin | 15 (100) | 13 (100) | – |
| Vancomycine | 10 (66.6) | 8 (61.5) | 0.54 |
| Linezolid | 6 (40) | 6 (46.1) | 0.52 |
| Meropenem | 11 (73.3) | 12 (92.3) | 0.21 |
| Piperacillin-tazobactam | 7 (46.6) | 2 (15.3) | 0.08 |
| Ampisulbactam | 0 | 3 (23.0) | 0.08 |
| Clindamycin | 1 (6.6) | 4 (30.7) | 0.12 |
| Ciprofloxacin | 6 (40) | 4 (30.7) | 0.45 |
| Levofloxacin | 4 (26.6) | 8 (61.6) | 0.069 |
| Colistin | 6 (40) | 4 (30.7) | 0.45 |
| Benzodiazepine | 11 (73.3) | 13 (100) | 0.067 |
| Antipsychotic | 7 (46.6) | 7 (53.8) | 0.50 |
| ARB | 4 (26.6) | 4 (30.7) | 0.56 |
| Betablocker | 4 (26.6) | 5 (38.4) | 0.39 |
| Calcium channel blocker | 1 (6.6) | 3 (23.0) | 0.24 |
| Furosemide | 6 (40) | 6 (46.1) | 0.52 |
| Magnesium infusion | 4 (26.6) | 3 (23.0) | 0.58 |
| Corticosteroid | 12 (80) | 9 (69.2) | 0.41 |
| Caspofungin | 4 (26.6) | 3 (23.0) | 0.58 |
| Amphotricin B | 1 (6.6) | 0 | 0.53 |
ARB: Angiotensin receptor blocker; ICU: Intensive care unit; PPI: Proton pump inhibitor.
| Variable | Midodrine (n = 15), n (%) | Control (n = 13), n (%) |
|---|---|---|
| Source of microorganism | ||
| – Blood | 5 (33.3) | 5 (38.5) |
| – Urine | 5 (33.3) | 2 (15.4) |
| – Tracheal | 5 (33.3) | 8 (61.5) |
| – Other | 3 (20) | 2 (15.4) |
| Isolated microorganism | ||
| – Klebsiella pneumonia | 4 (26.7) | 6 (46.2) |
| – Acinetobacter baumannii | 1 (6.7) | 3 (23.1) |
| – Escherichia coli | 2 (13.3) | 0 |
| – Pseudomonas aeroginusa | 2 (13.3) | 0 |
| – Staphylococcus aureus | 0 | 1 (7.7) |
| – Staphylococcus epidermidis | 2 (13.3) | 4 (30.8) |
| – Entrococcus spp. | 3 (20) | 2 (15.4) |
| – Fungus | 4 (26.7) | 2 (15.4) |
| – Other | 2 (13.3) | 2 (15.4) |
The primary outcome of the study was lactate clearance (Table 6). Although in pairwise comparison, lactate clearance was not significantly different between the groups, however lactate clearance occurred significantly faster in the midodrine group than the control group (p = 0.049) with a large effect size ( = 0.141).
| Outcomes | Midodrine (n = 15), median (IQR) | Control (n = 13), median (IQR) | p-value | |
|---|---|---|---|---|
| Lactate clearance | ||||
| – Baseline serum lactate level (mmol/l) | 3.3 (2.7–5.6) | 3.3 (2.7–4.5) | 0.35 | |
| – Lactate clearance 1 (0–4 h) (%) | 24 (0–48) | -6 (-31 to 17) | 0.92† | 0.049‡ |
| – Lactate clearance 2 (4–24 h) (%) | 28 (0–53) | 7 (-3 to 45) | 0.72† | |
| – Lactate clearance 3 (24–28 h) (%) | 19 (0–50) | 15 (-24 to 37) | 0.2† | |
| Dose of vasopressor (μg/min) through days 1–5 | ||||
| – Day 1 | 10 (8.7–10.5) | 10 (10–10) | 0.96† | 0.15‡ |
| – Day 2 | 9 (5–15) | 13 (5–24) | 0.27† | |
| – Day 3 | 5 (0–10) | 5 (2.5–26) | 0.007† | |
| – Day 4 | 0 (0–5.7) | 3 (0–15) | 0.46† | |
| – Day 5 | 0 (0–5) | 0 (0–15) | 0.32† | |
| Other outcomes | ||||
| – Duration of vasopressor therapy (days) | 4 (2–8) | 5 (3–11) | 0.36 | |
| – Duration of mechanical ventilation (days) | 13 (4–25) | 11 (5–17) | 0.66 | |
| – Length of ICU stay (days) | 8 (4–15) | 12 (4.5–20) | 0.55 | |
| – Reinitiating of vasopressor, n (%) | 4 (26.7%) | 5 (38.5%) | 0.39 | |
| – 28-day mortality | 8 (53.3%) | 9 (69.2%) | 0.32 | |
†
Pairwise comparison.
‡
Between the groups comparison.
ICU: Intensive care unit; IQR: Interquartile range.
The vasopressor dose was significantly different between the groups at third day. Also, more patients in the midodrine group were free from vasopressor at third day compared with the control group (66 vs 46%). However, change in the vasopressor dose was not significantly different between the groups through the study period.
Median (interquartile range) length of ICU stay was 8 (4–15) and 12 (4.5–20) in the midodrine and control group, respectively. Although it was shorter in the midodrine group but the difference was not statistically significant (p = 0.55).
Up to day 28, eight (55.3%) patients in the midodrine group and nine (69.2%) patients in the control group died. However, the difference was not statistically significant (p = 0.32). Bradycardia (as an important side effect of midodrine) was not detected in any patient. Also, other events were comparable between the groups (Table 7).
| Events | Midodrine (n = 15), n (%) | Control (n = 13), n (%) | p-value |
|---|---|---|---|
| Bradycardia† | 0 | 0 | – |
| Acute kidney injury | 6 (40%) | 5 (38.4%) | 0.62 |
| Acute hepatic failure | 3 (20%) | 1 (7.6%) | 0.35 |
| Requirement of dialysis | 2 (13.3%) | 2 (15.3%) | 0.64 |
| Leukocytosis | 7 (46.6%) | 6 (46.1%) | 0.63 |
| Ventilator associated pneumonia | 4 (26.6%) | 8 (61.5%) | 0.069 |
| Urinary tract infection | 1 (6.6%) | 1 (7.6%) | 0.72 |
| Bacteremia | 2 (13.3%) | 4 (30.7%) | 0.25 |
| Fungal infection | 1 (6.6%) | 1 (7.6%) | 0.72 |
| Other infection | 0 | 2 (15.3%) | 0.20 |
| Anemia | 5 (33.3%) | 6 (46.1%) | 0.38 |
| Thrombocytopenia | 3 (20%) | 3 (23.0%) | 0.60 |
| Requirement of CRRT | 0 | 0 | – |
†
Heart rate less than 60 beats per min.
CRRT: Continuous renal replacement therapy.
Discussion
In this study, midodrine accelerated lactate clearance in patients with septic shock when was added to intravenous vasopressors. Also, patients who received midodrine required significantly lower doses of the intravenous vasopressors in the third day of treatment. However, midodrine did not change duration of vasopressor requirement, length of ICU-stay and 28-day mortality. This is the first study that has evaluated the effect of midodrine on lactate elimination in patients with septic shock. Increase in rate of lactate clearance and decrease in vasopressor requirement may be considered as signs of successful resuscitation in patients with septic shock.
Midodrine as an alpha-agonist is used for management of orthostatic hypotension. In addition to its growing use in the treatment of hepatorenal syndrome, it has shown some advantages in other conditions including intradialytic hypotension [24,25].
The increase in serum lactate concentration (hyperlactatemia) was suggested as a marker for diagnosis of severe sepsis [26]. Later, it was shown that serum lactate level may predict mortality in severe sepsis even in patients without shock and organ failure [27]. Next studies have shown that lactate clearance in early phase of septic shock might be more accurate than just a single serum lactate level to predict outcome [7,28]. Lactate clearance is now considered as a laboratory marker for assessing effectiveness of resuscitation in the first phase of septic shock [29].
Not only rate of production but also rate of elimination can affect serum lactate level. In the healthy condition, lactate is predominantly eliminated by hepatic metabolism through monocarboxylate transporters and diffusion phenomenon. Remaining lactate is changed to pyruvate and a minor part is cleared by the kidney (less than 5%) [30]. In the case of critical illness, the role of kidney is upgraded either in excretion (up to 10%) or in metabolism (up to 30%) [31].
Midodrine can improve renal hemodynamic by enhancing renal resistance index and renal perfusion [3,32,33]. It has a supportive role in hepatorenal syndrome [24] and dialysis-related hypotension [25]. Improvement in renal perfusion particularly in critical illnesses can boost elimination of lactate by the kidney. In current study, patients with septic shock in the midodrine group had significantly faster lactate clearance than the control group.
The first study that evaluated role of midodrine in critical illnesses was organized by Levine et al. In this study, patients required lower doses of vasopressors when oral midodrine was added to the treatment regimen [17]. However, type of shock was not defined. In an observational study with large sample size, critically ill patients who had received midodrine, infrequently required additional lower doses of intravenous vasopressors [34].
In our study, patients in the midodrine group received significantly lower doses of vasopressors in the third day of intervention. Although the duration of vasopressor therapy was not significantly different between the groups, more patients in the midodrine group were vasopressor-free after the third day of intervention.
The MIDAS trial assessed midodrine efficacy on discontinuation of intravenous vasopressor in critically ill patients with persistent hypotension. In his trial, time to vasopressor discontinuation or other secondary outcomes did not change when midodrine was added [15]. However, bradycardia was detected in 7.6% of patients in the midodrine group. In our study, bradycardia was not detected in any patient. It may be due to lower dose of midodrine in our investigation in comparison with MIDAS trial (10 mg three-times daily vs 20 mg three-times daily). In MIDAS trial, only 26 patients had septic shock and in subgroup analysis, no beneficial effect of midodrine was detected even in these patients.
It has been suggested that midodrine could be a potential option in management of septic shock through decrease in vasopressor requirement and shortening of length of ICU stay [18]. In current study although was not significant, length of ICU stay was shorter in the midodrine group than the control group. Also all-cause mortality did not significantly differ between the groups. This may be related to comorbidities in the patients. All of patients had at least one major comorbidity and about 57% had at least one serious comorbidity (kidney, liver or respiratory failure or active cancer).
As is expected, antibiotics were frequently administered medications during the ICU stay. At this time, 26.6 and 23% of patients in the midodrine and control group required supplemental magnesium, respectively. Magnesium infusion in order to maintain serum magnesium level above 3 mg/dl can improve lactate clearance [35]. The number of patients who received supplemental magnesium was not significantly different between the groups.
Probable midodrine-related adverse events were closely monitored during the intervention. Bradycardia was detected in 7.6–10% of patients who received midodrine [15,34]. No patient experienced bradycardia in current investigation. Incidence of acute kidney injury in both groups was the same. It should be considered that the patients also received other nephrotoxic agents such as vancomycin, aminoglycosides and diuretics.
The study has some limitations. It was a pilot study with small sample size. Although effect size was considerable but power of the study according to the changes in lactate clearance was 56%. Because of emerging of COVID-19 pandemic, it was not possible to recruit more patients. Higher doses and longer durations of midodrine therapy may be needed to assess potential beneficial effects of midodrine in critically ill patients.
Conclusion
This was a preliminary study to investigate the effect of midodrine on lactate clearance in critically ill patients with septic shock. When midodrine was added to intravenous vasopressors, it significantly accelerated lactate clearance in patients with septic shock. Although, the duration and cumulative dose of intravenous vasopressor did not change significantly but vasopressor dose was significantly lower on third day in the midodrine group than the control group. Mididrine did not significantly improve length of ICU stay and 28-day mortality.
Future perspective
Appropriate dose and duration of midodrine as an adjunctive therapy in management of septic shock should be assessed in future randomized clinical trials. Other remained issue is the best time for initiation of midodrine.
Background
•
The effect of midodrine on lactate clearance has not been assessed in critically ill patients yet.
Objectives
•
The goal of this study was to assess the effect of adjunctive midodrine therapy on lactate clearance in critically ill patients with septic shock.
Methods
•
During a randomized preliminary clinical trial, 28 adult patients with septic shock who required intravenous vasopressor to maintain mean arterial blood pressure ≥65 mmHg were assigned to receive either adjunctive midodrine 10 mg three-times a day for 5 days (midodrine group = 15 patients) or not (control group = 13 patients).
Results
•
Lactate clearance was significantly faster in the midodrine group than the control group (p = 0.049) with a large effect size ( = 0.141). Changes in the vasopressor doses were not significantly different through the study period.
Conclusion
•
When midodrine was added to intravenous vasopressors, it significantly accelerated lactate clearance in patients with septic shock.
Acknowledgments
The Office of the Vice-Chancellor for Research of Tehran University of Medical Sciences, Tehran, Iran supported this work. With thanks of nursing staffs of general ICU of Imam Khomeini Hospital for their kind support.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. Deidentified, individual data that underlie the results reported in this article, along with demographic and lab data will be available on request from scientific institutes or known researchers in this area for meta-analysis or review, with the permission of the authors’ institute. Clinical trial registration number: IRCT20100228003449N25.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Morgan RW, Fitzgerald JC, Weiss SL, Nadkarni VM, Sutton RM, Berg RA. Sepsis-associated in-hospital cardiac arrest: epidemiology, pathophysiology, and potential therapies. J. Crit. Care 40, 128–135 (2017).
2.
Elke G, Bloos F, Wilson DC, Meybohm P. Sep Net Critical Care Trials Group. Identification of developing multiple organ failure in sepsis patients with low or moderate SOFA scores. Crit. Care 22(1), 147 (2018).
3.
Arefian H, Heublein S, Scherag A et al. Hospital-related cost of sepsis: a systematic review. J. Infect. 74(2), 107–117 (2017).
4.
Kadri SS, Rhee C, Strich JR et al. Estimating ten-year trends in septic shock incidence and mortality in United States academic medical centers using clinical data. Chest 151(2), 278–285 (2017).
5.
Russell JA, Rush B, Boyd J. Pathophysiology of septic shock. Crit. Care Clin. 34(1), 43–61 (2018).
6.
Mikkelsen ME, Miltiades AN, Gaieski DF et al. Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock. Crit. Care Med. 37(5), 1670–1677 (2009).
7.
Krishna U, Joshi SP, Modh M. An evaluation of serial blood lactate measurement as an early predictor of shock and its outcome in patients of trauma or sepsis. Indian J. Crit. Care Med. 13(2), 66–73 (2009).
8.
Nguyen HB, Kuan WS, ATLAS (Asia Network to Regulate Sepsis care) Investigator et al. Outcome effectiveness of the severe sepsis resuscitation bundle with addition of lactate clearance as a bundle item: a multi-national evaluation. Crit. Care 15(5), R229 (2011).
9.
Pan J, Peng M, Liao C, Hu X, Wang A, Li X. Relative efficacy and safety of early lactate clearance-guided therapy resuscitation in patients with sepsis: a meta-analysis. Medicine (Baltimore) 98(8), e14453 (2019).
•• This meta-analysis collects the results of seven studies that show lactate clearance-guided resuscitation can decrease in-hospital mortality in a significant manner in comparison with central venous oxygen saturation guided therapy.
10.
Rhodes A, Evans LE, Alhazzani W et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock. Crit. Care Med. 45(3), 486–552 (2017).
11.
Russell JA. Vasopressor therapy in critically ill patients with shock. Intensive Care Med. 45(11), 1503–1517 (2019).
12.
Sacha GL, Bauer SR, Lat I. Vasoactive agent use in septic shock: beyond first-line recommendations. Pharmacotherapy 39(3), 369–381 (2019).
13.
Teboul JL, Duranteau J, Russell JA. Intensive care medicine in 2050: vasopressors in sepsis. Intensive Care Med. 44(7), 1130–1132 (2018).
14.
Gutman LB, Wilson BJ. The role of midodrine for hypotension outside of the intensive care unit. J. Popul. Ther. Clin. Pharmacol. 24(3), e45–e50 (2017).
15.
Santer P, Anstey MH, MIDAS Study Group et al. Effect of midodrine versus placebo on time to vasopressor discontinuation in patients with persistent hypotension in the intensive care unit (MIDAS): an international randomised clinical trial. Intensive Care Med. 46(10), 1884–1893 (2020).
•• This trial was the first clinical trial that examined midodrine in intensive care unit.
16.
Dziuk BD, Iwuji K. Midodrine use in intensive care unit patients recovering from septic shock. Chronicles 6(26), 26–29 (2018).
17.
Levine AR, Meyer MJ, Bittner EA et al. Oral midodrine treatment accelerates the liberation of intensive care unit patients from intravenous vasopressor infusions. J. Critic. Care 28(5), 756–762 (2013).
•• This investigation was the leading observational study that assess the effect of midodrine in decreasing the need for an intravenous vasopressor.
18.
Whitson MR, Mo E, Nabi T et al. Feasibility, utility, and safety of midodrine during recovery phase from septic shock. Chest 149(6), 1380–1383 (2016).
• Shows that the use of midodrine can decrease length of receiving intravenous vasopressor.
19.
Barletta JF, Bruno JJ, Buckley MS, Cook DJ. Stress ulcer prophylaxis. Crit. Care Med. 44(7), 1395–1405 (2016).
20.
Barbar S, Noventa F, Rossetto V et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score. J. Thromb. Haemost. 8(11), 2450–2457 (2010).
21.
Sessler CN, Gosnell MS, Grap MJ et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am. J. Respir. Crit. Care Med. 166(10), 1338–1344 (2002).
22.
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron. Clin. Pract. 120(4), c179–184 (2012).
23.
Lescot T, Karvellas C, Beaussier M, Magder S. Acquired liver injury in the intensive care unit. Anesthesiology 117(4), 898–904 (2012).
24.
Nanda A, Reddy R, Safraz H, Salameh H, Singal AK. Pharmacological therapies for hepatorenal syndrome: a systematic review and meta-analysis. J. Clin. Gastroenterol. 52(4), 360–367 (2018).
25.
Brunelli SM, Cohen DE, Marlowe G, Van Wyck D. The impact of midodrine on outcomes in patients with intradialytic hypotension. Am. J. Nephrol. 48(5), 381–388 (2018).
26.
Revelly JP, Tappy L, Martinez A et al. Lactate and glucose metabolism in severe sepsis and cardiogenic shock. Crit. Care Med. 33(10), 2235–2240 (2005).
27.
Trzeciak S, Dellinger RP, Chansky ME et al. Serum lactate as a predictor of mortality in patients with infection. Intensive Care Med. 33(6), 970–977 (2007).
28.
Arnold RC, Shapiro NI, Emergency Medicine Shock Research Network (EMShockNet) Investigators et al. Multicenter study of early lactate clearance as a determinant of survival in patients with presumed sepsis. Shock 32(1), 35–39 (2009).
29.
Gu WJ, Zhang Z, Bakker J. Early lactate clearance-guided therapy in patients with sepsis: a meta-analysis with trial sequential analysis of randomized controlled trials. Intensive Care Med. 41(10), 1862–1863 (2015).
30.
Phypers B, Tom Pierce JM. Lactate physiology in health and disease. Cont. Edu. Anaesth. Crit. Care Pain 6(3), 128–132 (2006).
31.
Bellomo R. Bench-to-bedside review: lactate and the kidney. Crit. Care 6(4), 322–326 (2002).
• Clarifies the role of kidney in eliminating lactate.
32.
Hamdy MM, Abdel-Azeem EK, Amro H, Abd-Elradya AA. Evaluating the effect of midodrine on renal resistance index in patients with liver cirrhosis and ascites. Al-Azhar. Assiut. Med. J. 14(1), 19–23 (2016).
• This investigation shows that midodrine can improve renal hemodynamics in patients with cirrhosis.
33.
Obiedallah AA, Abdelmohsen E, Kelani AI, Mousa M. Effect of midodrine in patients with liver cirrhosis and refractory ascites. Am. J. Intern. Med. 5(1), 12–17 (2017).
34.
Rizvi MS, Trivedi V, Nasim F et al. Trends in use of midodrine in the ICU: a single-center retrospective case series. Crit. Care Med. 46(7), e628–e633 (2018).
• This research was a large case-series that follow the trend of use of midodrine in intensive care unit in Mayo Clinic.
35.
Noormandi A, Khalili H, Mohammadi M, Abdollahi A. Effect of magnesium supplementation on lactate clearance in critically ill patients with severe sepsis: a randomized clinical trial. Eur. J. Clin. Pharmacol. 76, 175–184 (2020).
• This trial shows that maintaining magnesium above 3 mg/dl in early phase of septic shock can accelerate the elimination of lactate.
Information & Authors
Information
Published In
Pages: 673 - 683
PubMed: 33860672
Copyright
© 2021 Future Medicine Ltd.
History
Received: 2 November 2020
Accepted: 12 March 2021
Published online: 16 April 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The effect of midodrine on lactate clearance in patients with septic shock: a pilot study. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0238
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Rory McDonald, Michael Burns, Adrian Wong, Carolyn Smith, Marlies Ostermann, Sam Hutchings, The effects of vasopressor choice on renal outcomes in septic shock: a systematic review of randomised trials as a guide for future research, Critical Care, 10.1186/s13054-025-05573-7, 29, 1, (2025).
- Madeleine M. Puissant, Kaitlin J Armstrong, Richard R Riker, Samir Haydar, Tania D Strout, Kathryn E Smith, David B Seder, David J Gagnon, Midodrine initiation criteria, dose titration, and adverse effects when administered to treat shock: A systematic review and semi-quantitative analysis, The Journal of Critical Care Medicine, 10.2478/jccm-2025-0007, 11, 1, (5-22), (2025).
- Sebastian J. Kilcommons, Fadi Hammal, Dawn L. Opgenorth, Kirsten M. Fiest, Constantine J. Karvellas, Vincent I. Lau, Erika MacIntyre, Janek Senaratne, Jocelyn Slemko, Wendy Sligl, Fernando Zampieri, D.’Arcy Duquette, Lily T. Guan, Nadia Baig, Sean M. Bagshaw, Oleksa G. Rewa, Midodrine for the early liberation from vasopressor support in the ICU (LIBERATE): a feasibility study, Pilot and Feasibility Studies, 10.1186/s40814-024-01577-2, 10, 1, (2024).
- Sebastian J. Kilcommons, Fadi Hammal, Mostafa Kamaleldin, Dawn L. Opgenorth, Kirsten M. Fiest, Constantine J. Karvellas, Demetrios J. Kutsogiannis, Vincent I. Lau, Erika J. MacIntyre, Bram Rochwerg, Janek M. Senaratne, Jocelyn M. Slemko, Wendy I. Sligl, Xiaoming X. M. Wang, Sean M. Bagshaw, Oleksa G. Rewa, Adjunctive Midodrine Therapy for Vasopressor-Dependent Shock in the ICU: A Systematic Review and Meta-Analysis, Critical Care Medicine, 10.1097/CCM.0000000000006519, 53, 2, (e384-e399), (2024).
- 雪 李, Advances in the Treatment of Septic Shock, Advances in Clinical Medicine, 10.12677/acm.2024.1451528, 14, 05, (1079-1087), (2024).
- Bita Shahrami, Effat Davoudi-Monfared, Zahra Rezaie, Shayesteh Gheibi, Ayda Vakili-Ardabili, Amir Ahmad Arabzadeh, Ali Talebi, Mojtaba Mojtahedzadeh, Management of a critically ill patient with COVID-19-related fulminant myocarditis: A case report, Respiratory Medicine Case Reports, 10.1016/j.rmcr.2022.101611, 36, (101611), (2022).