Cost–effectiveness of long-acting injectable aripiprazole once-monthly 400 mg in bipolar I disorder in the USA
Abstract
Aim: To evaluate the cost–effectiveness of aripiprazole once-monthly 400/300 mg (AOM 400) in maintenance monotherapy treatment of bipolar I disorder (BP-I). Methods: A de novo lifetime Markov model was developed for BP-I using available data for AOM 400 and relevant comparators. Base-case analysis considered costs and outcomes from the US payer perspective. Results: The cost per quality-adjusted life year gained with AOM 400 versus comparators ranged from US$2007 versus oral asenapine to dominance (i.e., lower cost with quality-adjusted life gain) versus long-acting injectable risperidone, paliperidone palmitate, oral cariprazine and best supportive care. Patients treated with AOM 400 were estimated to have fewer mood episodes and hospitalizations per patient (5.37) than comparators (6.33, asenapine or cariprazine; 6.54, risperidone long-acting injectable; 7.64, paliperidone palmitate; and 8.93, best supportive care). Sensitivity analyses showed results were robust to parameter uncertainty. Conclusion: AOM 400 may be considered cost effective in the maintenance monotherapy treatment of BP-I in adults.
Bipolar disorder (BP) is a lifelong mood disorder involving periods of mania, hypomania or depression, causing disruptions to mood and potentially severe impairments in functioning [1,2]. Of the four BP subtypes, bipolar I disorder (BP-I) is considered the most severe. A diagnosis of BP-I by the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria requires the presence of one or more manic episodes, which are characterized by inflated self esteem and disinhibition, severe distractibility, restlessness, difficulty concentrating and – during severe episodes – psychotic symptoms [1].
BP-I is estimated to have a lifetime prevalence of 0.6–2.1% [3,4]. Onset occurs in two age peaks – early adulthood (15–24 years) and in later life (45–54 years) [5] – and is followed by multiple, unpredictable recurrences of mood episodes over the patient's lifetime [6].
BP-I represents a substantial economic burden arising from direct and indirect costs. In a recent cost analysis performed in the USA for the year 2015, the BP-I population had, relative to the general population, excess direct healthcare costs of US$25.2 billion (including pharmacy and general medical services), excess direct nonhealthcare costs of US$6.8 billion (most relating to substance abuse) and excess indirect costs of US$87.8 billion (relating to lost productivity and caregiving) [7]. The average annual excess costs per individual were estimated at US$48,333 [7].
Treatment outcomes in BP remain unsatisfactory [8]. Currently available pharmacological therapies for acute or maintenance treatment include mood stabilizers (e.g., lithium and anticonvulsants) and antipsychotics [8]. In maintenance treatment, patient adherence is commonly low and it is the nonadherent individuals who show the highest hospitalization rates and poorest prognosis [9,10]. A more effective use of pharmacological therapies, including the development of novel formulations for long-term management, provides the opportunity to reduce the burden of BP from both patient and societal perspectives [11,12].
Long-acting injectable (LAI) atypical antipsychotics can be administered – according to their individual formulation – either biweekly, monthly or at longer intervals, in contrast with daily dosing for oral treatments. Aripiprazole is an atypical antipsychotic approved in the USA and other countries as an oral formulation for the treatment of acute manic or mixed episodes of BP-I. Oral aripiprazole also has proven efficacy as a maintenance treatment for BP-I [13–15]. Aripiprazole once-monthly 400/300 mg (AOM 400) is a depot formulation of aripiprazole administered once monthly by intramuscular injection that is approved for the treatment of schizophrenia [16,17] and recently now approved for the maintenance monotherapy treatment of BP-I in adults [16]. A 52-week, double-blind, placebo-controlled, randomized withdrawal study of AOM 400 as a maintenance monotherapy treatment in patients with BP-I demonstrated that AOM 400 delayed the time to, and reduced the rate of, recurrences of mood episodes relative to placebo and was generally safe and well tolerated (NCT01567527; [18]).
The objective of the present analysis was to estimate the cost–effectiveness of AOM 400 in the maintenance monotherapy treatment of BP-I in adults from a US healthcare payer's perspective, relative to comparator treatments: risperidone LAI, paliperidone palmitate, oral cariprazine, oral asenapine and best supportive care (BSC; using placebo as a proxy).
Methods
Model structure
A de novo Markov state transition model was developed with a yearly cycle length, based on review of the published economic models in BP health technology assessment submissions [19], available data for AOM 400 [18] and a previously published study [20]. The model state structure consisted of six states: euthymia while on first-line treatment, euthymia while on subsequent treatment, acute mania, mixed episode, acute depression and death (Figure 1).
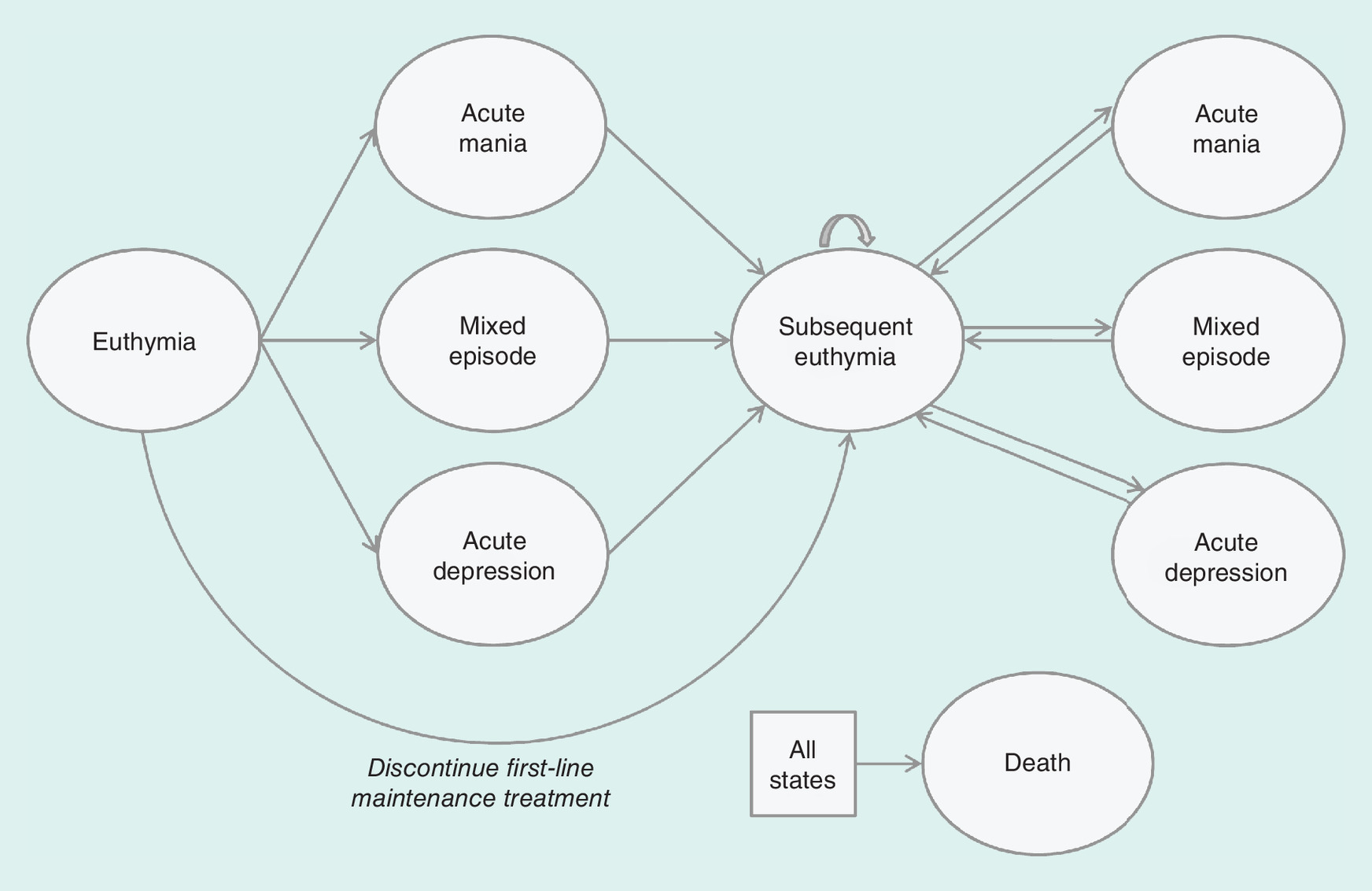
Patients entered the model with a diagnosis of BP-I in the euthymia health state and initiated maintenance treatment with AOM 400 or one of the comparators. The goal of maintenance treatment was to delay the time to relapse (i.e., the occurrence of a mood episode). When a mood episode occurred, patients transitioned from the euthymic state to one of the three episode states (mania, mixed or depression). Patients who experienced a mood episode were assumed to stop maintenance treatment and undergo treatment for the acute episode for one cycle (1 year). Once the episode had resolved (i.e., after one cycle), patients transitioned to the subsequent euthymic state, from which they were at risk of further mood episodes. Multiple mood episodes could occur over the time horizon of the model but no more than one per year. Patients could also discontinue first-line maintenance treatment due to adverse events (AEs) or other reasons and could move directly to the second euthymic state without experiencing a mood episode.
For the base-case model, the time horizon was the patient's lifetime, due to the chronicity of the disease and in line with international guideline recommendations [8]. The base-case model considered all costs and health effects from the perspective of the healthcare payer in the USA. Results are also reported for a 1-year period, to better align with the US payer perspective. Following recommendations of the US Public Health Service Panel, both future costs and health effects were discounted at a rate of 3% [21]. A complete list of inputs, references and distributions for the probabilistic sensitivity analysis (PSA) is included in the Supplementary Tables.
Population
The modeled population included US patients with a diagnosis of BP-I by DSM-5 criteria [22], confirmed by the Mini International Neuropsychiatric Interview [23], and who maintained stability on AOM 400 for at least 8 weeks as in the AOM 400 Phase III study in maintenance monotherapy for BP-I [18]. The age at onset of BP-I was assumed to be 17 years (i.e., an average of the peak age of onset) and 57.5% of patients were assumed to be female as in the AOM 400 Phase III study in maintenance monotherapy for BP-I. The results are analyzed and reported on a per-patient basis.
Treatment comparators
The analysis included branded second-generation atypical antipsychotics: risperidone LAI (the only other LAI currently approved in the USA for maintenance treatment of BP-I), paliperidone palmitate (frequently used off-label for maintenance treatment of BP-I) and cariprazine and asenapine (the only branded oral antipsychotics with an indication for acute treatment of manic or mixed episodes associated specifically with BP-I in adults). BSC was also included in the analysis, using placebo as a proxy.
Input data
Relapse rates
In the absence of head-to-head trials that compare the treatments in the base-case analysis, relapse rates for AOM 400 and BSC were taken from the AOM 400 Phase III study in maintenance monotherapy for BP-I (Tables 1 & 2) [18]. For risperidone LAI and paliperidone palmitate, relative risks of transition from the first euthymic health state were estimated from the clinical systematic literature review published by Miura et al. [24] and multiplied by the relapse rate data for placebo in the AOM 400 Phase III study in maintenance monotherapy for BP-I, which was assumed to be equivalent to placebo in the clinical trials of these comparators [18]. Since paliperidone palmitate is not approved for treatment of BP-I, the relapse rate data for oral paliperidone cited in Miura et al. 2014 was used. It was not possible to obtain adequate data to estimate relapse rates for the oral comparators, cariprazine and asenapine, in patients with BP-I. For these two therapies, the approach taken was to use average estimated rates of relapse for the four oral, atypical antipsychotics from a meta-analysis of the systematic literature review (aripiprazole, olanzapine, paliperidone and quetiapine; [24]) and apply the average rate to the relapse rate data for placebo in the AOM 400 Phase III study in maintenance monotherapy for BP-I [18], as for the previous two comparators (Tables 1 & 2), using the equation:
where ‘mood ep’ = mood episode, which can be mania, depression or mixed.
| Treatment | Rate of relapse from euthymia to a mood episode (1 year) | Ref. | |||
|---|---|---|---|---|---|
| Mania (%) | Depression (%) | Mixed (%) | Total (%) | ||
| AOM 400 | 9.09 | 15.15 | 1.52 | 25.76 | [18] |
| Risperidone LAI | 12.94 | 17.30 | 2.92 | 33.17 | [24] |
| Paliperidone palmitate | 18.06 | 18.73 | 4.08 | 40.87 | [24] |
| Cariprazine | 15.95 | 12.19 | 3.60 | 31.74 | [24] |
| Asenapine | 15.95 | 12.19 | 3.60 | 31.74 | [24] |
| BSC | 30.10 | 14.30 | 6.80 | 51.20 | [18] |
AOM: Aripiprazole once-monthly; BSC: Best supportive care; LAI: Long-acting injectable; RR: Relative risk.
| Treatment | Relapse of mania/mixed episode RR (95% CI) | Relapse of depressive episode RR (95% CI) |
|---|---|---|
| Risperidone LAI vs placebo | 0.43 | 1.21 |
| Aripiprazole vs placebo | 0.51 | 0.91 |
| Olanzapine vs placebo | 0.39 | 0.73 |
| Paliperidone palmitate vs placebo | 0.60 | 1.31 |
| Quetiapine vs placebo | 0.62 | 0.46 |
LAI: Long-acting injectable; RR: Relative risk.
Discontinuation
The model included two types of discontinuation: due to AEs and due to other causes (e.g., lost to follow-up, sponsor discontinued study, patient withdrawn by the investigator, patient withdrew consent and protocol deviation). The model assumed that patients discontinued only after the first episode of euthymia. Table 3 presents the probabilities of discontinuation and the sources for each input.
| Treatment | Probability of discontinuation (1 year) | |||
|---|---|---|---|---|
| Due to adverse events (%) | Ref. | Due to other causes† | Ref. | |
| AOM 400 | 5.26 | [18] | 20.30 | [18] |
| Risperidone LAI | 0.65 | [25] | 19.57 | [26] |
| Paliperidone palmitate‡ | 5.50 | [27] | 19.57 | [26]§ |
| Cariprazine | 12.00 | [28] | 37.74 | [26] |
| Asenapine | 9.00 | [29] | 37.74 | [26] |
| BSC | 0.75 | [18] | 19.55 | [18,26] |
†Other causes include: loss of follow-up, sponsor discontinued study, patient withdrawn by the investigator, patient withdrew consent and protocol deviation.
‡Based on data for schizophrenia.
§Assumed to be the same as risperidone LAI.
AOM: Aripiprazole once-monthly; BSC: Best supportive care; LAI: Long-acting injectable.
Mortality
General population mortality statistics based on the age at onset and sex distribution of the model population were sourced from the most recent US life table published by the National Center for Health Statistics in 2012 [30]. Data on the increased risk of mortality in patients with BP-I (including increased risk of suicide) were obtained from a large Swedish cohort study [31]. The authors estimated the hazard ratio (HR) of death in the general population versus BP population, adjusted for age and other sociodemographics, by gender: 2.03 (95% CI: 1.85–2.23) for males and 2.34 (95% CI: 2.16–2.53) for females. Applying the HR to the general probability of mortality yielded the increased probability of death for the patients in the analysis.
Adverse events
AE rates were derived from the AOM 400 Phase III study in maintenance monotherapy for BP-I and the respective product labels [18,25,27–29]. AE rates were calculated as the number of events divided by the sample size for a specific time period and adjusted to the cycle length of the model. AE rates for paliperidone palmitate in the treatment of schizophrenia were used to estimate the BP rates, as there are no clinical trials for paliperidone palmitate in BP.
Utilities
Health state utility values
The effectiveness of each treatment was evaluated using the quality-adjusted life year (QALY), which was estimated by applying a utility value to each health state in the model, where 1 represents perfect health and 0 represents death. Health state utility values were derived from Soares–Weiser [19] using values taken from Revicki [32] (Supplementary Table 1). The total QALY was calculated as the proportion of patients occupying each health state during each annual cycle accumulated over the time horizon.
AE utility decrements
Utility decrements for treatment-emergent AEs were applied as a one-off event during a model cycle (1 year). The utility decrements were identified using the same method as for the health state utility values (Supplementary Table 3) [32–38].
Sensitivity analysis
Deterministic sensitivity analysis
Deterministic sensitivity analysis (DSA) was performed to identify parameters that exhibit a significant influence on the model results by varying individual input values by ± 20%.
Probabilistic sensitivity analysis
PSA was performed to assess the joint uncertainty surrounding all parameters in the model by assigning predetermined probabilistic distributions and randomly simulating parameter values from these distributions. The choice of probabilistic distributions for each parameter was based on the nature of the data and its constraints and included recommendations from the literature [39]. A lognormal distribution was used to simulate the variation in rates (relapse rates, discontinuation rates and AE rates), probability of mood episode was sampled using a β-distribution, and a γ-distribution was used to simulate the variation in costs and utilities (including disutilities).
Resource identification & costs
Drug acquisition costs
Information on dosing and the number of administrations for each drug were taken from the US FDA labels [25,27–29]. As the comparators have different doses available on the market, the dose mix for treatments was extracted from the Truven MarketScan® Medicaid and Medicare/Commercial Database (Truven Health Analytics, MI, USA) relating to the period 1 July 2015 to 20 June 2016. Unit costs were taken from the RED BOOK™ (Thomson Reuters:PDR Network, NJ, USA) in February 2017 (Supplementary Table 4) [40]. Wholesale acquisition costs were used in the base-case model as this is the most appropriate price benchmark from the US payer perspective. Treatment initiation costs were included for LAI-naive patients per the FDA prescribing information, as LAIs require either an oral overlap or loading doses of the LAI. No treatment initiation costs were necessary for oral comparators.
Drug administration costs
Administration costs were applied for LAIs, as these drugs require a healthcare visit to administer the drug. Administration cost per cycle was calculated as the number of annual visits per the FDA prescribing information and multiplied by the cost per visit (US$26.61), taken from the physician fee schedule (PFS) code: 96372, ‘Therapeutic, prophylactic or diagnostic injection (specify material injected); subcutaneous or intramuscular’ (Supplementary Table 4) [41].
Health state costs
Costs generated by a patient in each 1-year cycle in a euthymic health state included nonpharmaceutical costs (i.e., monitoring costs taken from the Maudsley prescribing guidelines [42] and PFS [41]) and pharmaceutical costs from the RED BOOK (Supplementary Table 4) [40]. The sum of costs incurred by each patient in a euthymic state was US$12,660.
Costs generated by a patient in an acute manic, mixed or depressive state were subdivided into pharmaceutical and hospitalization costs. Pharmaceutical costs were assumed to be incurred through a period of 365.25 days × 10% = 36.53 days for a manic or mixed episode [43] and 365.25 days × 32% = 116.88 days for a depressive episode [6]. The proportion of patients was evenly split between the included pharmaceutical therapies. The number of therapies differed for manic, mixed or depressive episodes. Acquisition costs of treatments were obtained from the RED BOOK [40]. Hospitalization costs were estimated using weighted national estimates from the 2014 Healthcare Cost and Utilization Project National Inpatient Sample from the Agency for Healthcare Research and Quality, with the assumption that 100% of patients would be hospitalized [44]. The sum of costs incurred by each patient in a manic, mixed and depressive episode was US$9819, US$7042 and US$6601, respectively. No costs were assumed for maintenance therapy during a cycle with an acute episode.
AE costs
The costs of AEs were derived using PFS costs (outpatient visits) and the Medi-Span database for the WAC costs (lowest price per day) (Supplementary Table 3). The conservative resource use was determined through discussions with a pharmacist experienced in psychiatry.
Model validation
Key assumptions and data gaps within the economic model are shown in Supplementary Table 5.
Results
Base-case results
Base-case results from the US payer perspective and for a lifetime horizon per-patient basis are shown in Table 4. The cost per QALY gained per patient with AOM 400 versus comparators ranged from US$2007/QALY versus asenapine to being a dominant strategy (i.e., lower costs with QALY gain) versus risperidone LAI, paliperidone palmitate, cariprazine and BSC. The negative incremental costs shown in Table 4 denote that AOM 400 had lower total lifetime costs than those comparators.
| Treatment | Incremental costs (US$) | Incremental QALYs | ICER (US$/QALY) |
|---|---|---|---|
| AOM 400 vs | |||
| Risperidone LAI | -377 | 0.672 | Dominant |
| Paliperidone palmitate | -5969 | 1.182 | Dominant |
| Cariprazine | -3858 | 0.523 | Dominant |
| Asenapine | 1044 | 0.520 | 2007 |
| BSC | -19,594 | 1.966 | Dominant |
AOM: Aripiprazole once-monthly; BSC: Best supportive care; ICER: Incremental cost–effectiveness ratio; LAI: Long-acting injectable; QALY: Quality-adjusted life year.
The costs for each treatment in the main cost categories are shown in Table 5. AOM 400 generated higher acquisition costs but these were offset by lower administration costs compared with risperidone LAI. The lower relapse rates for AOM 400 resulted in lower mood episode-related costs and in accruing lower total costs than the other LAI treatments and BSC.
| Treatment | Acquisition (US$) | Administration (US$) | Adverse events (US$) | Mania episodes (US$) | Depression episodes (US$) | Mixed episodes (US$) | Total costs (US$) |
|---|---|---|---|---|---|---|---|
| AOM 400 | 279,004 | 450 | 71 | 18,619 | 38,810 | 36,352 | 373,305 |
| Risperidone LAI | 255,721 | 926 | 153 | 25,076 | 47,002 | 44,805 | 373,682 |
| Paliperidone palmitate | 246,937 | 320 | 16 | 33,128 | 50,643 | 48,230 | 379,274 |
| Cariprazine | 254,035 | 0 | 42 | 31,231 | 46,240 | 45,616 | 377,164 |
| Asenapine | 249,141 | 0 | 35 | 31,231 | 46,240 | 45,615 | 372,262 |
| BSC | 210,432 | 0 | 34 | 51,537 | 65,150 | 65,746 | 392,899 |
AOM: Aripiprazole once-monthly; BSC: Best supportive care; LAI: Long-acting injectable.
Table 6 details the outcomes for each treatment in the outcome categories for the base case. AOM 400 was estimated to accumulate a higher QALY gain than its comparators and a lower number of hospitalizations. Although AOM 400 generated a slightly higher frequency of AEs in the first year than most of the comparators, it was estimated to avoid a higher number of total mood episodes over the patient's lifetime. Patients treated with AOM 400 were estimated to have 5.37 mood episodes and hospitalizations per patient, fewer than all comparators (6.33 for oral treatments, 6.54 for risperidone LAI, 7.64 for paliperidone palmitate and 8.93 for BSC) for a lifetime horizon. Incremental results for each treatment in the outcome categories are shown in Table 7.
| Treatment | QALY | Life years gained | Number mania episodes | Number depression episodes | Number mixed episodes | Number mood episodes | Number adverse events | Number of hospitalizations |
|---|---|---|---|---|---|---|---|---|
| AOM 400 | 18.32 | 26.53 | 1.90 | 3.16 | 0.32 | 5.37 | 0.83 | 5.37 |
| Risperidone LAI | 17.64 | 26.53 | 2.55 | 3.41 | 0.58 | 6.54 | 1.32 | 6.54 |
| Paliperidone palmitate | 17.13 | 26.53 | 3.37 | 3.50 | 0.76 | 7.64 | 0.20 | 7.64 |
| Cariprazine | 17.79 | 26.53 | 3.18 | 2.43 | 0.72 | 6.33 | 0.35 | 6.33 |
| Asenapine | 17.79 | 26.53 | 3.18 | 2.43 | 0.72 | 6.33 | 0.45 | 6.33 |
| BSC | 16.35 | 26.53 | 5.25 | 2.49 | 1.19 | 8.93 | 0.38 | 8.93 |
AOM: Aripiprazole once-monthly; BSC: Best supportive care; LAI: Long-acting injectable; QALY: Quality-adjusted life year.
| Treatment | Incr. cost (US$)/number of mania episodes | Incr. cost (US$)/number of depression episodes | Incr. cost (US$)/number of mixed episodes | Incr. cost (US$)/number of mood episodes | Incr. cost (US$)/adverse event | Incr. cost (US$)/hospitalizations |
|---|---|---|---|---|---|---|
| AOM 400 vs | ||||||
| Risperidone LAI | 573 | 1485 | 1443 | 321 | 773 | 321 |
| Paliperidone palmitate | 4040 | 17,601 | 13,379 | 2638 | -9444 | 2638 |
| Cariprazine | 3004 | -5287 | 9586 | 4032 | -7971 | 4032 |
| Asenapine | -813 | 1430 | -2594 | -1091 | 2700 | -1091 |
| BSC | 5845 | -29,383 | 22,530 | 5511 | -43,409 | 5511 |
AOM: Aripiprazole once-monthly; BSC: Best supportive care; Incr: Incremental; LAI: Long-acting injectable.
1-year time horizon
Cost–effectiveness data are less robust for shorter time durations, since the benefits of reducing the number of mood episodes, hospitalizations and AEs improve over time. Table 8 presents the results per patient for a 1-year time horizon.
| Treatments | Incremental costs (US$) | Incremental QALYs | ICER (US$) |
|---|---|---|---|
| AOM 400 vs | |||
| Risperidone LAI | 4269 | 0.039 | 108,137 |
| Paliperidone palmitate | 514 | 0.012 | 44,306 |
| Oral cariprazine | 7245 | 0.003 | 2,457,636 |
| Oral asenapine | 11,118 | 0.000 | 210,803,765 |
| BSC | 15,461 | 0.057 | 273,050 |
AOM: Aripiprazole once-monthly; BSC: Best supportive care; ICER: Incremental cost–effectiveness ratio; LAI: Long-acting injectable; QALY: Quality-adjusted life year.
Sensitivity analysis
Deterministic sensitivity analysis
Results of the DSA for AOM 400 versus the comparators are shown as tornado plots in Figures 2–6. The parameters with the highest impact on the results were:
AOM 400 versus risperidone LAI (Figure 2): HRs applied to general mortality, the cost of pharmaceutical maintenance treatment in the euthymic state and the probability of depression for both interventions.
AOM 400 versus paliperidone palmitate (Figure 3): HRs applied to general mortality and the cost of pharmaceutical maintenance treatment in the subsequent euthymic state.
AOM 400 versus cariprazine (Figure 4): HRs applied to general mortality, the discount rate applied to costs and the probability of a depressive episode after the first euthymic state for AOM 400.
AOM 400 versus asenapine (Figure 5): HRs applied to general mortality, the discount rate applied to outcomes and the probability of a depressive episode after the first euthymic state for AOM 400.
AOM 400 versus BSC (Figure 6): the cost of pharmaceutical maintenance treatment in the subsequent euthymic state, the discount rate applied to outcomes, the utility level in euthymia and HRs applied to general mortality for AOM 400.

Figure 2. Tornado diagram: aripiprazole once-monthly 400 mg versus risperidone long-acting injectable (inputs varied ± 20%).
In each one-way sensitivity analysis, negative ICER values represent dominance of AOM 400 versus the comparator, due to less cost and a positive QALY gain.
AOM: Aripiprazole once-monthly; HR: Hazard ratio; ICER: Incremental cost–effectiveness ratio; LAI: Long-acting injectable; QALY: Quality-adjusted life year.
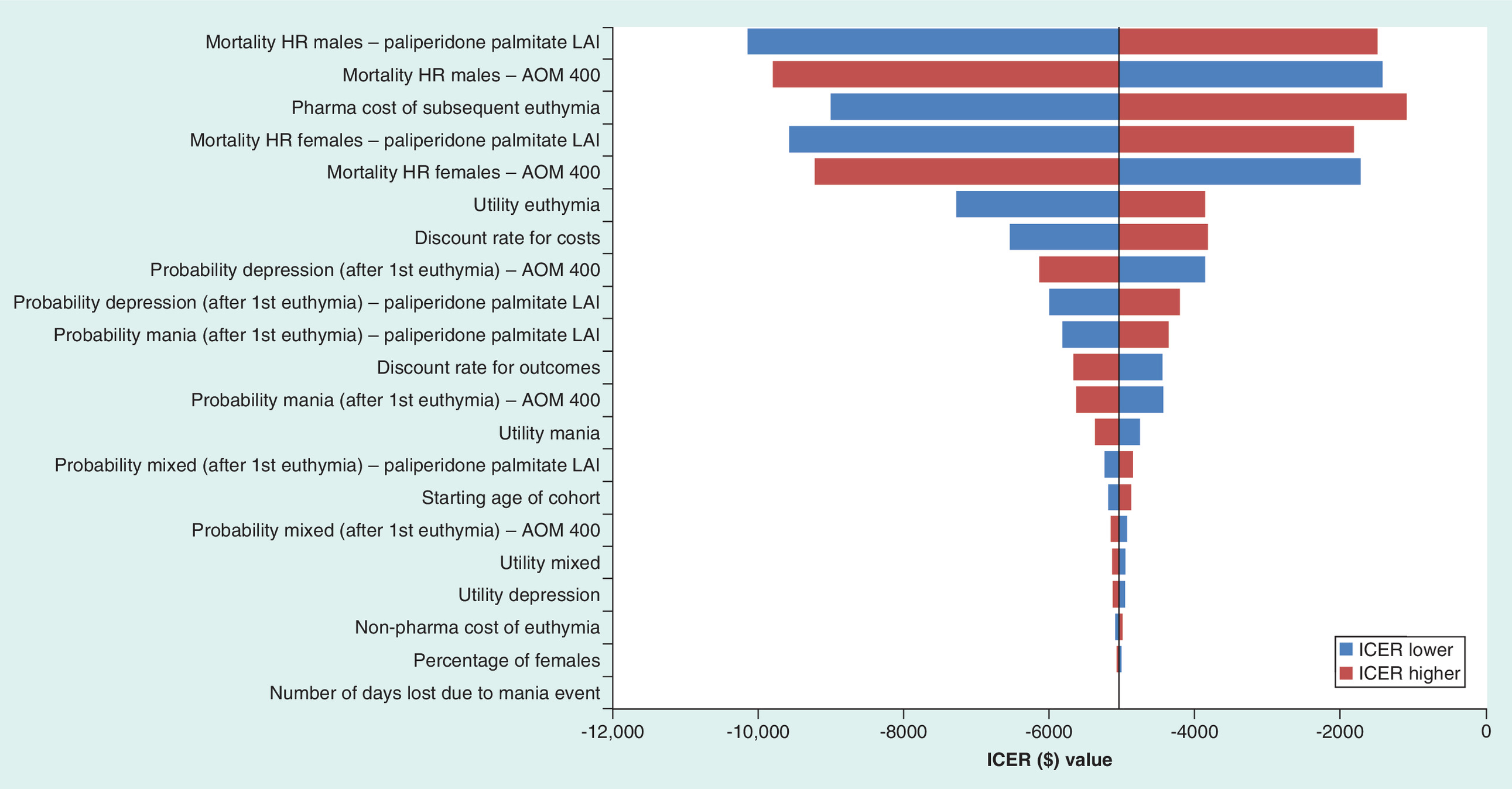
Figure 3. Tornado diagram: aripiprazole once-monthly 400 mg versus paliperidone palmitate (inputs varied ± 20%).
In each one-way sensitivity analysis, negative ICER values represent dominance of AOM 400 versus the comparator, due to less cost and a positive QALY gain.
AOM: Aripiprazole once-monthly; HR: Hazard ratio; ICER: Incremental cost–effectiveness ratio; LAI: Long-acting injectable; QALY: Quality-adjusted life year.
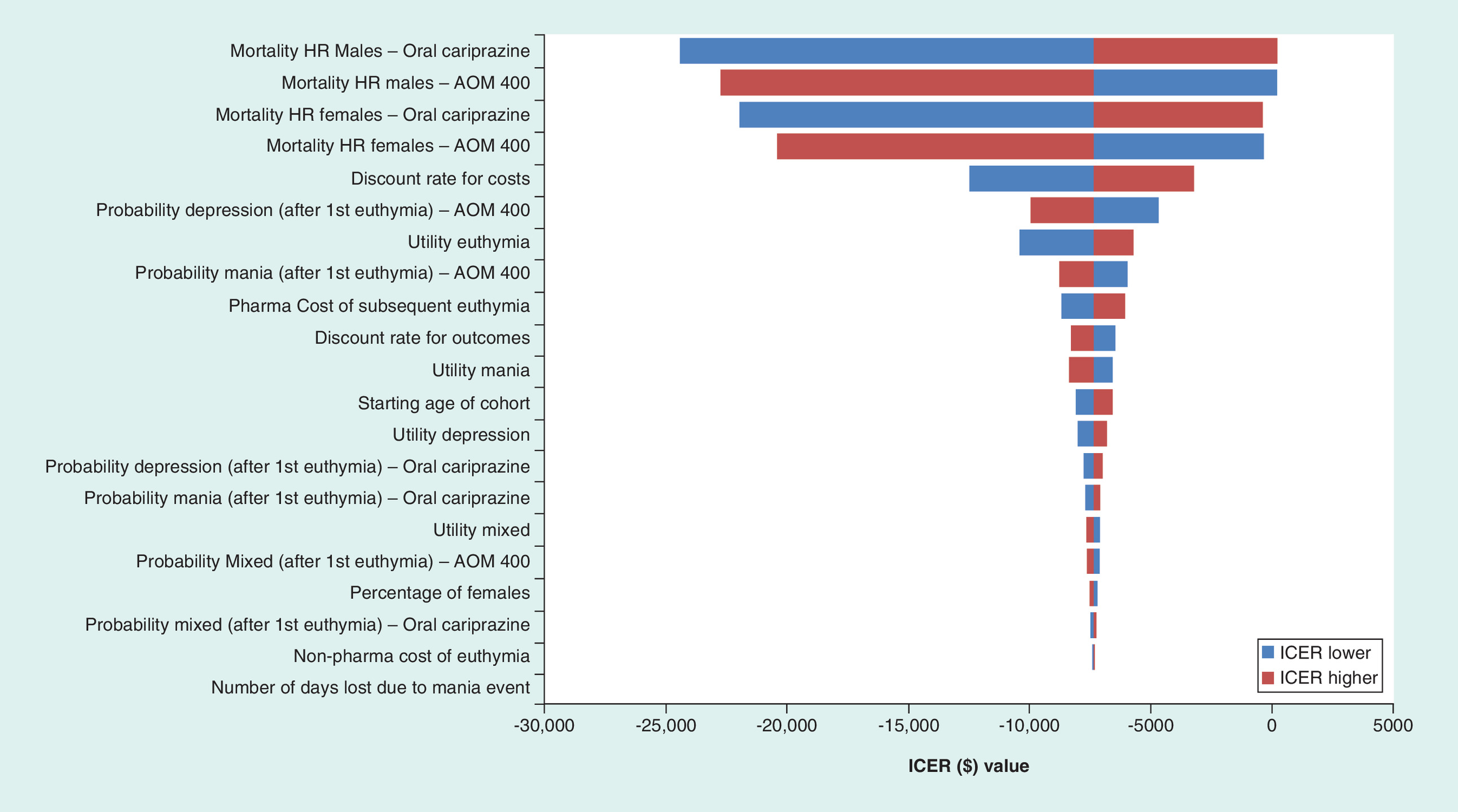
Figure 4. Tornado diagram: aripiprazole once-monthly 400 mg versus cariprazine (inputs varied ± 20%).
In each one-way sensitivity analysis, negative ICER values represent dominance of AOM 400 versus the comparator, due to less cost and a positive QALY gain.
AOM: Aripiprazole once-monthly; HR: Hazard ratio; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.

Figure 5. Tornado diagram: aripiprazole once-monthly 400 mg versus asenapine (inputs varied ± 20%).
In each one-way sensitivity analysis, negative ICER values represent dominance of AOM 400 versus the comparator, due to less cost and a positive QALY gain.
AOM: Aripiprazole once-monthly; HR: Hazard ratio; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
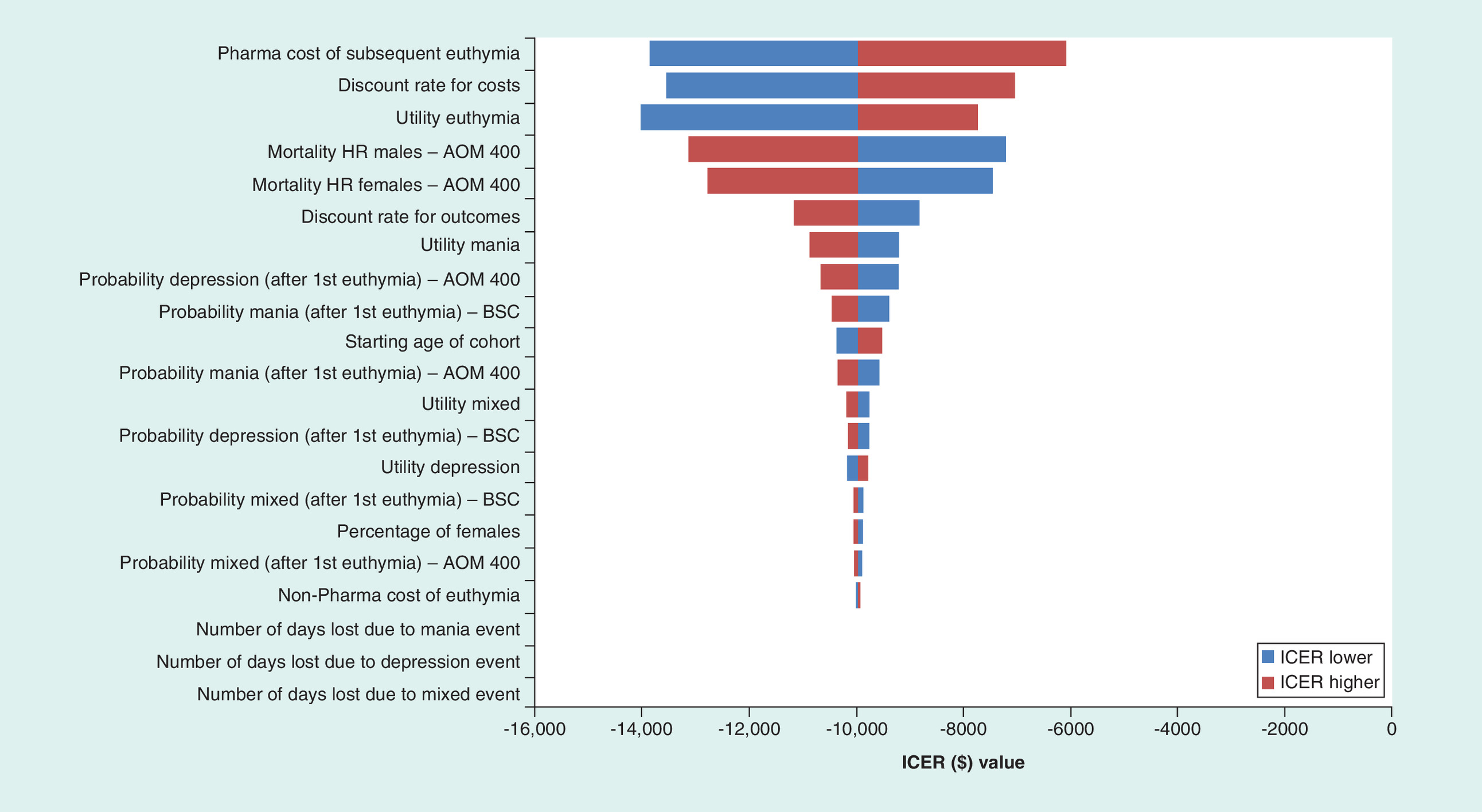
Figure 6. Tornado diagram: aripiprazole once-monthly 400 mg versus best supportive care (inputs varied ± 20%).
In each one-way sensitivity analysis, negative ICER values represent dominance of AOM 400 versus the comparator, due to less cost and a positive QALY gain.
AOM: Aripiprazole once-monthly; BSC: Best supportive care; HR: Hazard ratio; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
Probabilistic sensitivity analysis
Results from the PSA were similar to the DSA results, indicating that uncertainty in the estimation of inputs did not have a significant impact on the base-case results. Cost–effectiveness acceptability curves for AOM 400 and comparators are shown in Figure 7. The cost–effectiveness acceptability curves showed that AOM 400 had a 50, 60 and 70% probability of being cost effective at a willingness to pay threshold of US$12,606, US$25,013 and US$100,000 per QALY gained respectively.
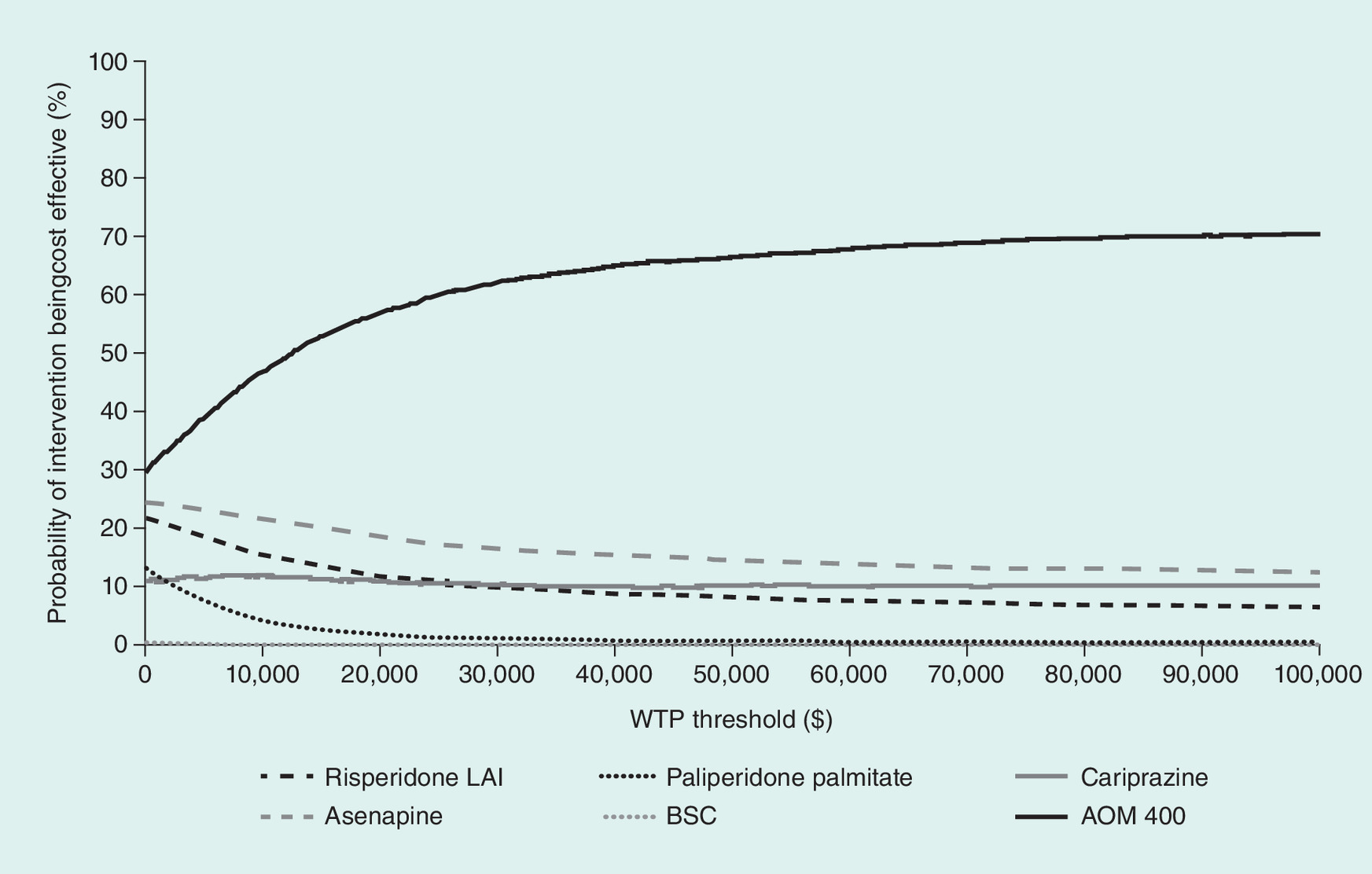
Figure 7. Multiway cost–effectiveness acceptability curve.
The CEAC summarizes the impact of uncertainty on the result of an economic evaluation, plotting a range of cost–effectiveness thresholds (horizontal axis) against the probability that each treatment will be cost-effective at that threshold (vertical axis).
AOM: Aripiprazole once-monthly; BSC: Best supportive care; CEAC: Cost–effectiveness acceptability curve; LAI: Long-acting injectable; WTP: Willingness to pay.
Discussion
LAI AOM 400 was recently approved for the maintenance monotherapy treatment of BP-I in adults within the USA, based on the results of a Phase III trial that demonstrated significant benefit compared with placebo (NCT01567527; [18]).
This cost–effectiveness analysis from a US healthcare payer perspective with a lifetime horizon showed that AOM 400 may be a cost-effective treatment strategy for adults with BP-I. For all but one comparator, treatment with AOM 400 was the dominant treatment strategy, with lower total cost and more QALY gain over comparators. When comparing AOM 400 versus asenapine, the ICER was US$2007 per QALY. Patients treated with AOM 400 were estimated to have fewer mood episodes and fewer hospitalizations per patient than the other comparators analyzed for a lifetime horizon. This reduction in mood episodes and hospitalizations results in clinical benefit and translates into less accumulation of estimated costs of hospitalization and mood event-specific treatments throughout a patient's life.
This is the first cost–effectiveness study of AOM 400 in BP-I. A previous cost–effectiveness study of AOM 400 in schizophrenia performed in the USA reported that AOM 400 consistently provided favorable clinical benefits and was associated with fewer relapses and lower overall treatment costs than paliperidone palmitate [45]. In the UK, another cost–effectiveness study in schizophrenia reported that AOM 400 improved clinical outcomes by reducing relapses per patient relative to other LAIs investigated over the model time horizon; sensitivity analyses highlighted that the probability and the cost of relapse were the main drivers for the cost–effectiveness of AOM 400 [46].
A number of studies have investigated the cost–effectiveness of pharmacological therapies in BP versus placebo or other pharmacological therapies, with variable methodologies and outcomes that limit the conclusions regarding relative cost–effectiveness between these agents (summarized in Abdul Pari 2014 and Mavranezouli 2017 [47,48]). The reviewed studies used model structures that oversimplified the disease: most models did not include the possibility of active maintenance treatment after a relapse (mood episode) and a proportion did not include the ‘death’ state.
The strengths of this model were that it investigated the main goal of therapy (namely, delaying the onset of mood episodes) and the consequences of treatment failure (in terms of multiple mood episodes and subsequent treatments), with the inclusion of the three types of acute mood episodes: manic, mixed and depressive. Limitations of the model were that it assumed transitions between states were not affected by the age of patients or the duration of disease; only one mood episode per year was allowed (which is unlikely in real life); acute mood episodes after the second euthymic state were assumed to have the same characteristics and transition probabilities as those occurring after the first euthymic state; only one subsequent treatment euthymic state was considered; no maintenance therapy was assumed during the 1-year cycle with a mood episode; and assumptions were made for the transition probabilities of the oral comparators (cariprazine and asenapine).
Despite these limitations, the model provided useful information about the cost–effectiveness of maintenance treatment of BP-I. In conclusion, the results show that AOM 400 may be considered cost effective in the maintenance monotherapy treatment of BP-I in adults when compared with alternative branded treatments analyzed from a US payer perspective.
Bipolar I disorder (BP-I) is a lifelong mood disorder with a lifetime prevalence of up to 2.1%.
Aripiprazole once-monthly 400/300 mg (AOM 400) is a depot formulation of aripiprazole recently approved as a maintenance monotherapy treatment of BP-I in adults.
This study estimated the cost–effectiveness of AOM 400 in the maintenance monotherapy treatment of BP-I in adults, relative to treatment comparators, from a US healthcare payer's perspective.
A de novo Markov state transition model was used with a yearly cycle length and lifetime time horizon.
The cost per quality-adjusted life year (QALY) gained with AOM 400 versus comparators ranged from US$2007 per QALY versus oral asenapine to dominance (i.e., lower cost with QALY gain) versus long-acting injectable risperidone, paliperidone palmitate, oral cariprazine and best supportive care.
Patients treated with AOM 400 were estimated to have fewer mood episodes and hospitalizations per patient (5.37) than comparators (6.33, asenapine or cariprazine; 6.54, risperidone long-acting injectable; 7.64, paliperidone palmitate; and 8.93, best supportive care) for a lifetime horizon.
Sensitivity analyses demonstrated that the results were robust to parameter uncertainty.
AOM 400 may be considered a cost-effective maintenance monotherapy treatment of BP-I from a US healthcare payer perspective.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2018-0010
Acknowledgements
Prior presentation: poster presentation at the AMCP Nexus Meeting 2017, Dallas, Texas; October 16–19, 2017.
Financial & competing interests disclosure
This study was funded by Otsuka Pharmaceutical Development & Commercialization and Lundbeck. M Augusto is a full-time employee of PAREXEL International. M Greene, S Min Sweeney and H Waters are full-time employees of Otsuka Pharmaceutical Development & Commercialization, Inc. M Touya is a full-time employee of Lundbeck. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Editorial support for this manuscript was provided by B Wolvey of PAREXEL, which was funded by Otsuka Pharmaceutical Development & Commercialization and Lundbeck.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_materials.docx)
- Download
- 72.55 KB
References
1.
American Psychiatric Association. Practice guideline for the treatment of patients with bipolar disorder (2010). https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/bipolar.pdf.
2.
Geddes JR, Miklowitz DJ. Treatment of bipolar disorder. Lancet 381(9878), 1672–1682 (2013).
3.
Blanco C, Compton WM, Saha TD et al. Epidemiology of DSM-5 bipolar I disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions – III. J. Psychiatr. Res. 84, 310–317 (2017).
4.
Merikangas KR, Jin R, He JP et al. Prevalence and correlates of bipolar spectrum disorder in the World Mental Health Survey Initiative. Arch. Gen. Psychiatry 68(3), 241–251 (2011).
5.
Kroon JS, Wohlfarth TD, Dieleman J et al. Incidence rates and risk factors of bipolar disorder in the general population: a population-based cohort study. Bipolar. Disord. 15(3), 306–313 (2013).
6.
Judd LL, Akiskal HS, Schettler PJ et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch. Gen. Psychiatry 59(6), 530–537 (2002).
7.
Cloutier M, Greene M, Guerin A, Touya M, Wu E. The economic burden of bipolar I disorder in the United States in 2015. J. Affect. Disord. 226, 45–51 (2017).
8.
National Collaborating Centre for Mental Health. The NICE guideline on the assessment and management of bipolar disorder in adults, children and young people in primary and secondary care (2014). www.nice.org.uk/guidance/cg185.
9.
Gaudiano BA, Weinstock LM, Miller IW. Improving treatment adherence in bipolar disorder: a review of current psychosocial treatment efficacy and recommendations for future treatment development. Behav. Modif. 32(3), 267–301 (2008).
10.
Lage MJ, Hassan MK. The relationship between antipsychotic medication adherence and patient outcomes among individuals diagnosed with bipolar disorder: a retrospective study. Ann. Gen. Psychiatry 8, 7 (2009).
11.
Gigante AD, Lafer B, Yatham LN. Long-acting injectable antipsychotics for the maintenance treatment of bipolar disorder. CNS Drugs 26(5), 403–420 (2012).
12.
Samalin L, Nourry A, Charpeaud T, Llorca PM. What is the evidence for the use of second-generation antipsychotic long-acting injectables as maintenance treatment in bipolar disorder? Nord. J. Psychiatry 68(4), 227–235 (2014).
13.
Keck PE Jr, Calabrese JR, Mcintyre RS et al. Aripiprazole monotherapy for maintenance therapy in bipolar I disorder: a 100-week, double-blind study versus placebo. J. Clin. Psychiatry 68(10), 1480–1491 (2007).
14.
Meduri M, Gregoraci G, Baglivo V, Balestrieri M, Isola M, Brambilla P. A meta-analysis of efficacy and safety of aripiprazole in adult and pediatric bipolar disorder in randomized controlled trials and observational studies. J. Affect. Disord. 191, 187–208 (2016).
15.
Muneer A. The treatment of adult bipolar disorder with aripiprazole: a systematic review. Cureus 8(4), e562 (2016).
16.
Abilify Maintena® (Aripiprazole). Otsuka Pharmaceutical Co. Ltd, Tokyo, Japan (2017). www.otsuka-us.com/media/static/Abilify-M-PI.pdf.
17.
Shirley M, Perry CM. Aripiprazole (ABILIFY MAINTENA®): a review of its use as maintenance treatment for adult patients with schizophrenia. Drugs 74(10), 1097–1110 (2014).
18.
Calabrese JR, Sanchez R, Jin N et al. Efficacy and safety of aripiprazole once-monthly in the maintenance treatment of bipolar I disorder: a double-blind, placebo-controlled, 52-week randomized withdrawal study. J. Clin. Psychiatry 78(3), 324–331 (2017).
19.
Soares-Weiser K, Bravo VY, Beynon S et al. A systematic review and economic model of the clinical effectiveness and cost–effectiveness of interventions for preventing relapse in people with bipolar disorder. Health Technol. Assess. 11(39), iii-206 (2007).
20.
Woodward TC, Tafesse E, Quon P, Kim J, Lazarus A. Cost–effectiveness of quetiapine with lithium or divalproex for maintenance treatment of bipolar I disorder. J. Med. Econ. 12(4), 259–268 (2009).
21.
Luce BR, Manning WGJ, Siegel JE, Lipscomb J. Estimating costs in cost–effectiveness analysis. In: Cost–effectiveness in Health and Medicine. Gold MR, Siegel JB, Russell LB, Weinstein MC (Eds). Oxford University Press, NY, USA, 176–213 (1996).
22.
Association AP. Diagnostic and Statistical Manual of Mental Health Disorders. DSM-5 (5th Edition). American Psychiatric Association, Arlington, VA, USA (2013).
23.
Sheehan DV, Lecrubier Y, Sheehan KH et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 59(Suppl. 20), 22–33 (1998).
24.
Miura T, Noma H, Furukawa TA et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis. Lancet Psychiatry 1(5), 351–359 (2014).
25.
Risperdal Consta® (Risperidone) long-acting injection. Janssen Pharmaceuticals Inc., Titusville, NJ, USA (2007). www.janssencns.com/shared/product/risperdalconsta/prescribing-information.pdf.
26.
Kroken RA, Kjelby E, Wentzel-Larsen T, Mellesdal LS, Jorgensen HA, Johnsen E. Time to discontinuation of antipsychotic drugs in a schizophrenia cohort: influence of current treatment strategies. Ther. Adv. Psychopharmacol. 4(6), 228–239 (2014).
27.
Invega Sustenna® (Paliperidone Palmitate) extended-release injectable suspension. Janssen Pharmaceuticals Inc., Titusville, NJ, USA (2009). www.janssenlabels.com/package-insert/product-monograph/prescribing-information/INVEGA+TRINZA-pi.pdf.
28.
Vraylar® (Cariprazine) capsules. Allergan USA Inc., Irvine, CA, USA (2015). www.allergan.com/assets/pdf/vraylar_pi.
29.
Saphris® (Asenapine) sublingual tablets. Merck Sharp & Dohme B.V, NJ, USA (2009). www.accessdata.fda.gov/drugsatfda_docs/label/2015/022117s017s018s019lbl.pdf.
30.
Arias E, Heron M, Xu J. United States life tables, 2012. Natl Vital Stat. Rep. 65(8), 1–65 (2016).
31.
Crump C, Sundquist K, Winkleby MA, Sundquist J. Comorbidities and mortality in bipolar disorder: a Swedish national cohort study. JAMA Psychiatry 70(9), 931–939 (2013).
32.
Revicki DA, Hanlon J, Martin S et al. Patient-based utilities for bipolar disorder-related health states. J. Affect. Disord. 87(2–3), 203–210 (2005).
33.
Lloyd A, Nafees B, Narewska J, Dewilde S, Watkins J. Health state utilities for metastatic breast cancer. Br. J. Cancer 95(6), 683–690 (2006).
34.
National Institute for Health and Clinical Excellence. Dronedarone for the treatment of non-permanent atrial fibrillation. Manufacturer/sponsor submission of evidence [TA197] (2010). www.nice.org.uk/guidance/ta197.
35.
National Institute for Health and Clinical Excellence. Eribulin for the treatment of locally advanced or metastatic breast cancer. Pre-meeting briefing [TA250] (2012). www.nice.org.uk/guidance/ta250.
36.
National Institute for Health and Clinical Excellence. Teriflunomide for treating relapsing–remitting multiple sclerosis (2014). www.nice.org.uk/guidance/ta303.
37.
National Institute for Health and Clinical Excellence. Pixantrone monotherapy for treating multiply relapsed or refractory aggressive non-Hodgkin's B-cell lymphoma – STA report [TA306] (2014). www.nice.org.uk/guidance/ta306.
38.
National Institute for Health and Clinical Excellence. Specification for manufacturer/sponsor submission to NICE. Of evidence [TA303] (2014). www.nice.org.uk/guidance/ta303.
39.
Briggs A, Sculpher M, Claxton K. Decision Modelling for Health Economic Evaluation (Handbooks for Health Economic Evaluation). Oxford University Press, Oxford, UK (2006).
40.
Truven Health Analytics. RED BOOK Online® (2017). http://micromedex.com/products/product-suites/clinical-knowledge/redbook.
41.
Centers for Medicare and Medicaid Services. Physician Fee Schedule (2016). www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/index.html.
42.
Taylor D, Paton C, Kapur S. The Maudsley Prescribing Guidelines in Psychiatry (11th Edition). Wiley-Blackwell, Hoboken, NJ, USA (2012).
43.
Post RM, Denicoff KD, Leverich GS et al. Morbidity in 258 bipolar outpatients followed for 1 year with daily prospective ratings on the NIMH life chart method. J. Clin. Psychiatry 64(6), 680–690 (2003).
44.
Agency for Healthcare Research and Quality. HCUP National Inpatient Sample (2012). www.hcup-us.ahrq.gov/nisoverview.jsp.
45.
Citrome L, Kamat SA, Sapin C et al. Cost–effectiveness of aripiprazole once-monthly compared with paliperidone palmitate once-monthly injectable for the treatment of schizophrenia in the United States. J. Med. Econ. 17(8), 567–576 (2014).
46.
Tempest M, Sapin C, Beillat M, Robinson P, Treur M. Cost–effectiveness analysis of aripiprazole once-monthly for the treatment of schizophrenia in the UK. J. Ment. Health Policy Econ. 18(4), 185–200 (2015).
47.
Abdul Pari AA, Simon J, Wolstenholme J, Geddes JR, Goodwin GM. Economic evaluations in bipolar disorder: a systematic review and critical appraisal. Bipolar Disord. 16(6), 557–582 (2014).
48.
Mavranezouli I, Lokkerbol J. A systematic review and critical appraisal of economic evaluations of pharmacological interventions for people with bipolar disorder. Pharmacoeconomics 35(3), 271–296 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Otsuka Pharm. Dev. & Comm. & Lundbeck.
History
Received: 2 February 2018
Accepted: 28 March 2018
Published online: 25 April 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of long-acting injectable aripiprazole once-monthly 400 mg in bipolar I disorder in the USA. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0010
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mauricio Tohen, Murat Yildirim, Stephanie Loomer, Arun Micheelsen, Kristine Harrsen, Clodagh Beckham, Soma Nag, Dawn Bates, Xavier Guillaume, Pedro Such, Views on an antipsychotic regimen administered once every 2 months: a qualitative interview study of people living with bipolar I disorder, caregivers, and prescribers in the USA and Canada, International Journal of Bipolar Disorders, 10.1186/s40345-026-00414-0, (2026).
- Richard Dodel, Christopher Kruse, Annette Conrads-Frank, Uwe Siebert, Pharmacoeconomics, NeuroPsychopharmacotherapy, 10.1007/978-3-030-62059-2_381, (101-234), (2022).
- John Thornhill, Chloe Orkin, Long-acting injectable HIV therapies: the next frontier, Current Opinion in Infectious Diseases, 10.1097/QCO.0000000000000701, 34, 1, (8-15), (2021).
- John Thornhill, Chloe Orkin, Long-acting injectable HIV therapies: the next frontier: Republication, Current Opinion in HIV and AIDS, 10.1097/COH.0000000000000670, 16, 2, (98-105), (2021).
- Richard Dodel, Christopher Kruse, Annette Conrads-Frank, Uwe Siebert, Pharmacoeconomics, NeuroPsychopharmacotherapy, 10.1007/978-3-319-56015-1_381-1, (1-135), (2020).
- Jean-Michel Azorin, Nicolas Simon, Dopamine Receptor Partial Agonists for the Treatment of Bipolar Disorder, Drugs, 10.1007/s40265-019-01189-8, 79, 15, (1657-1677), (2019).
- Margarida Augusto, Mallik Greene, Maëlys Touya, Samantha Min Sweeney, Heidi Waters, Budget impact analysis of long-acting injectable aripiprazole once-monthly 400 mg in bipolar I disorder in the USA, Journal of Comparative Effectiveness Research, 10.2217/cer-2018-0009, 7, 7, (627-636), (2018).