Comparison of amlodipine versus other calcium channel blockers on blood pressure variability in hypertensive patients in China: a retrospective propensity score-matched analysis
Abstract
Aim: Reducing the fluctuation of blood pressure has recently been recognized as a potential target for improving management of hypertension to prevent cardiovascular events, particularly for strokes. Some randomized controlled trials demonstrated that amlodipine can effectively reduce blood pressure as a well-established, long-acting calcium channel blocker (CCB). However, few data are available for amlodipine on blood pressure variability (BPV) in China in a real-world setting. This study aimed to assess the effect of amlodipine versus other CCB antihypertensive agents on BPV. Materials & methods: A retrospective propensity score-matched analysis was conducted, which retrieved the encounter data from 5582 hypertensive inpatients (with a median age of 69, female percentage of 48%, diastolic blood pressure ≥40 and <150 mmHg; systolic blood pressure (SBP) ≥70 mmHg and <260 mmHg), who had taken at least one antihypertensive agent and completed at least three SBP measurements during the visit. International Classification of Diseases was used to identify the hypertensive patients. BPV was calculated with standard deviation (SD) and coefficient of variation (CV) of SBP during a single inpatient visit. The Propensity Score Matching was used to balance the cohort of patients prescribed amlodipine or other CCBs. A series of appropriate statistical tests were applied to the propensity score-matched samples to examine the different effects on BPV. Additionally, the hypertensive patients with comorbidity such as coronary artery disease, diabetes mellitus, myocardial infarction, heart failure and chronic kidney disease were analyzed. Results: For the hypertensive patients (n = 1756, for each cohort), patients prescribed amlodipine showed lower BPV than patients prescribed other CCBs (12.90 vs 13.76 mmHg, p < 0.05 [SD] and 9.47 vs 10.06, p < 0.05 [CV]). For the hypertensive patients with comorbidity (n = 1080, for each cohort), patients prescribed amlodipine had lower BPV than patients prescribed other CCBs as well (13.24 vs 14.23 mmHg, p < 0.05 [SD] and 9.66 vs 10.28, p < 0.05 [CV]). Conclusion: amlodipine was associated with lower BPV than other CCBs for both hypertensive patients and hypertensive patients with comorbidity.
Hypertension is an important worldwide public health challenge [1]. The benefit of reducing blood pressure (BP) levels in patients with hypertension to prevent cardiovascular events is well proven [2–4]. Nevertheless, recent studies demonstrated that blood pressure variability (BPV) is also an independent risk factor other than average BP for vascular events [5–7]. In the real-world setting, lowering mean BP alone does not account for all damages and outcomes of hypertension, BPV would also need to be controlled and modulated by antihypertensive treatment [8–10]. This condition also occurs for the hypertensive patients with comorbidity. For these patients, routine monitoring of mean BP seemed to be of limited utility, as shown by the action taken for diabetes and vascular disease: in a preterax and diamicron MR controlled evaluation trial, blood-pressure variability is an independent risk factor for macrovascular or microvascular events in patients with Type II diabetes mellitus [11]. BPV needs to be monitored to assess the risk of macrovascular or microvascular events.
BPV has been observed at different interval bases such as 24-h period as short term, day-to-day visit as mid-term, as well as long-term visit. The 24-h ambulatory or long term variability in BP measured at clinic visits has been testified to be associated with cardiovascular and mortality outcomes. For another type of BPV, the BP fluctuation that may occur within a single medical visit, also has been reported to be associated with the risk of stroke and cardiovascular risk factors. Although inconsistent evidence exists, considering it is more easily obtainable in daily practice, it is meaningful to study BP fluctuation within a clinical visit for improving management of hypertension to prevent cardiovascular events.
Given the potential impact of BPV on vascular events, it is important to evaluate whether BPV is differently influenced by the various kinds of antihypertensive medications as well as patient characteristics, such as comorbidity. A recent meta-analysis considering long-term BPV across multiple randomized trials reported that a treatment difference (standard error) for amlodipine versus all active comparators is -1.23 mmHg. Five studies (47,558 BPV-evaluable patients) were included to assess whether patients receiving amlodipine versus other antihypertensive agents had lower BPV after ≥12 weeks of treatment. The results indicated that BPV with amlodipine was significantly lower than atenolol and lisinopril, significantly lower than enalapril in one study and similar to chlorthalidone and losartan [2]. These findings suggest that amlodipine is effective for minimizing BPV. In addition, in the X-CELLENT study (n = 577), the 24-h ambulatory BP measurements before and after 3 months’ treatment showed that amlodipine decreased daytime, night-time, and 24-h systolic BPV, whereas the comparator candesartan did not [12]. For the comparison in the patients with comorbidity, in other words, coronary artery disease, diabetes mellitus (DM), myocardial infarction, heart failure and chronic kidney disease, to our knowledge, there is no study focusing on the comparison of BPV between amlodipine and other antihypertensive agents, especially for calcium channel blocker (CCB) class.
Although the earlier studies indicated amlodipine is superior for reducing BPV for short term and long term, limited study for mid-term BPV has been implemented, especially for the patients with comorbidity. Furthermore, most of study results were from randomized trials or meta-analysis, which cannot reflect the real condition in clinical practice. Thus, the data from the electronic medical record (EMR) database should be examined. It would be beneficial to assess whether amlodipine can result in lower BPV in the real world, especially for the patients with comorbidity. Therefore, the objective of this analysis was to explore whether patients taking amlodipine have a lower BPV compared with those taking other CCB antihypertensive agents in general hypertensive patients and hypertensive patients with comorbidity.
Methods
Cohort design
This was a multicenter, retrospective and observational study conducted from February 2014 to November 2015 at four tertiary hospitals in China. Data from patients’ EMRs were retrieved for analysis in a real-world setting. The primary objective was to compare the BPV between the patients administrated amlodipine and other CCB antihypertensive agents, including felodipine, lacidipine, nimodipine, nifedipine and diltiazem. Moreover, the BPV for patients with five kinds of comorbidities including coronary artery disease, DM, myocardial infarction, heart failure and chronic kidney disease were compared.
Study population
The patients who have been diagnosed with hypertension and have taken at least one antihypertensive agent were initially enrolled in our analysis. International Classification of Diseases (ICD-10) was used to identify the hypertensive patients. Those who completed at least three systolic blood pressure (SBP) measurements during the visit were included. The inclusion criteria also included diastolic blood pressure ≥40 mmHg and <150 mmHg and SBP ≥70 mmHg and <260 mmHg. Whereas the patients who have been administrated amlodipine and the other CCBs during the same visit were excluded in our study. In addition, the patients with white coat hypertension or masked hypertension were not included in the analysis.
The study retrieved 5582 inpatients with essential hypertension which constituted general hypertensive population. ICD-10 was also used to screen the patients with comorbidity which constituted the hypertensive inpatients with comorbidity population, which retrieved 3181 patients. Furthermore, we carried out propensity score matching (PSM) analysis to avoid the potential confounder bias. For general hypertensive patients, the covariates including age, sex, baseline SBP, baseline pulse rate and baseline pulse rate variability (PRV) have been matched. For the patients with comorbidity, the additional covariates of the proportion of five kinds of comorbidities and the proportion of patients’ BP in normal range have been matched.
For the general hypertensive population, a total of 5582 patients were divided according to the agents administrated: 1805 patients for the amlodipine group and 3777 patients for the control group. After PSM, 1756 pairs of patients have been matched for further BPV analysis. The screening flow is described in Figure 1. For hypertensive patients with comorbidity population, after applying the selection criteria, a total of 3181 patients were newly initiated, the amlodipine group and the other CCB groups were identified based on the patients’ administration, which are 1117 and 2064 patients separately. Of all the patients enrolled, 2160 patients in 1080 pairs were finally assigned to each differently treated group. The screening flow is illustrated in Figure 2.
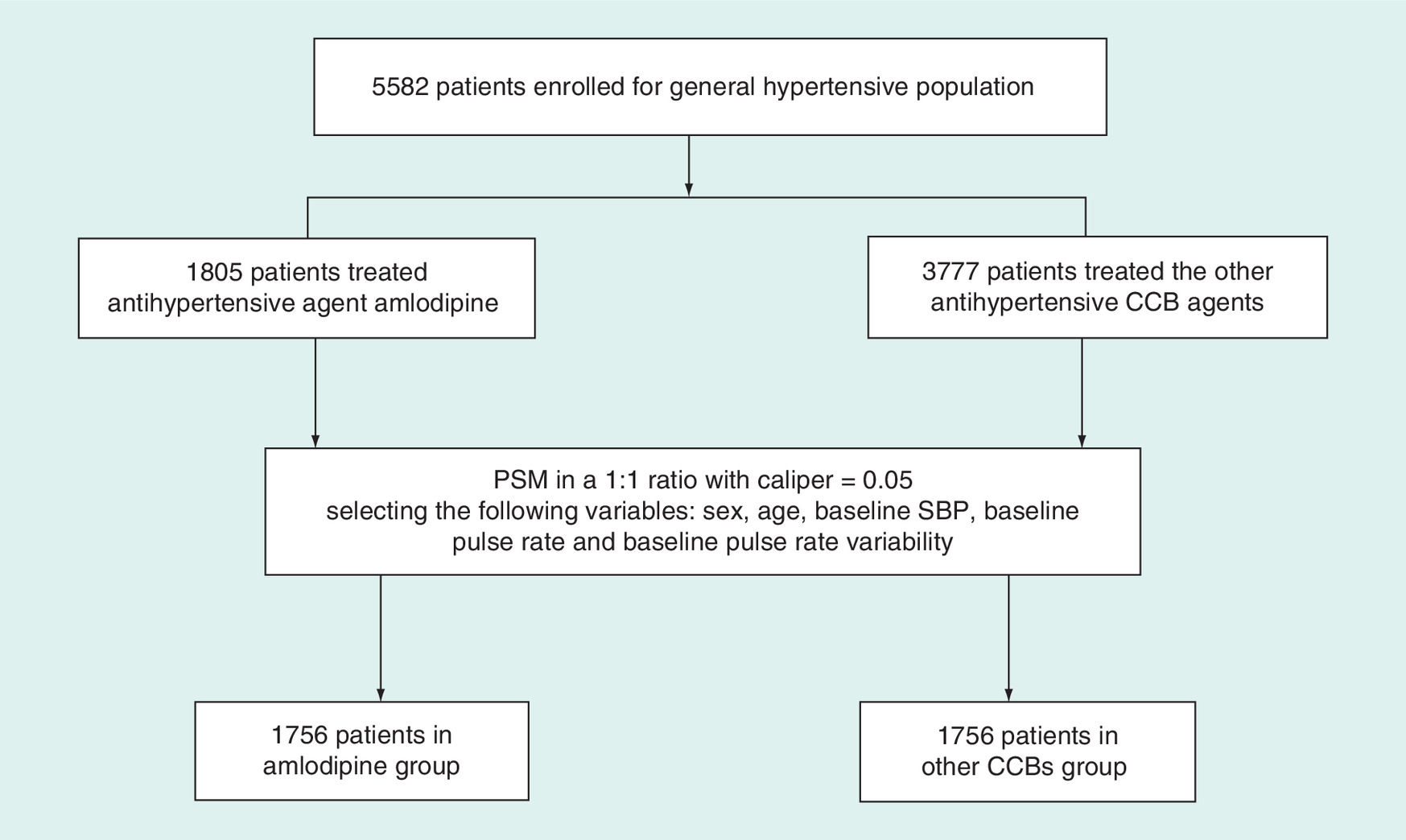
Figure 1. Screen flow for general hypertensive population.
CCB: Calcium channel blocker; PSM: Propensity score matching; SBP: Systolic blood pressure.
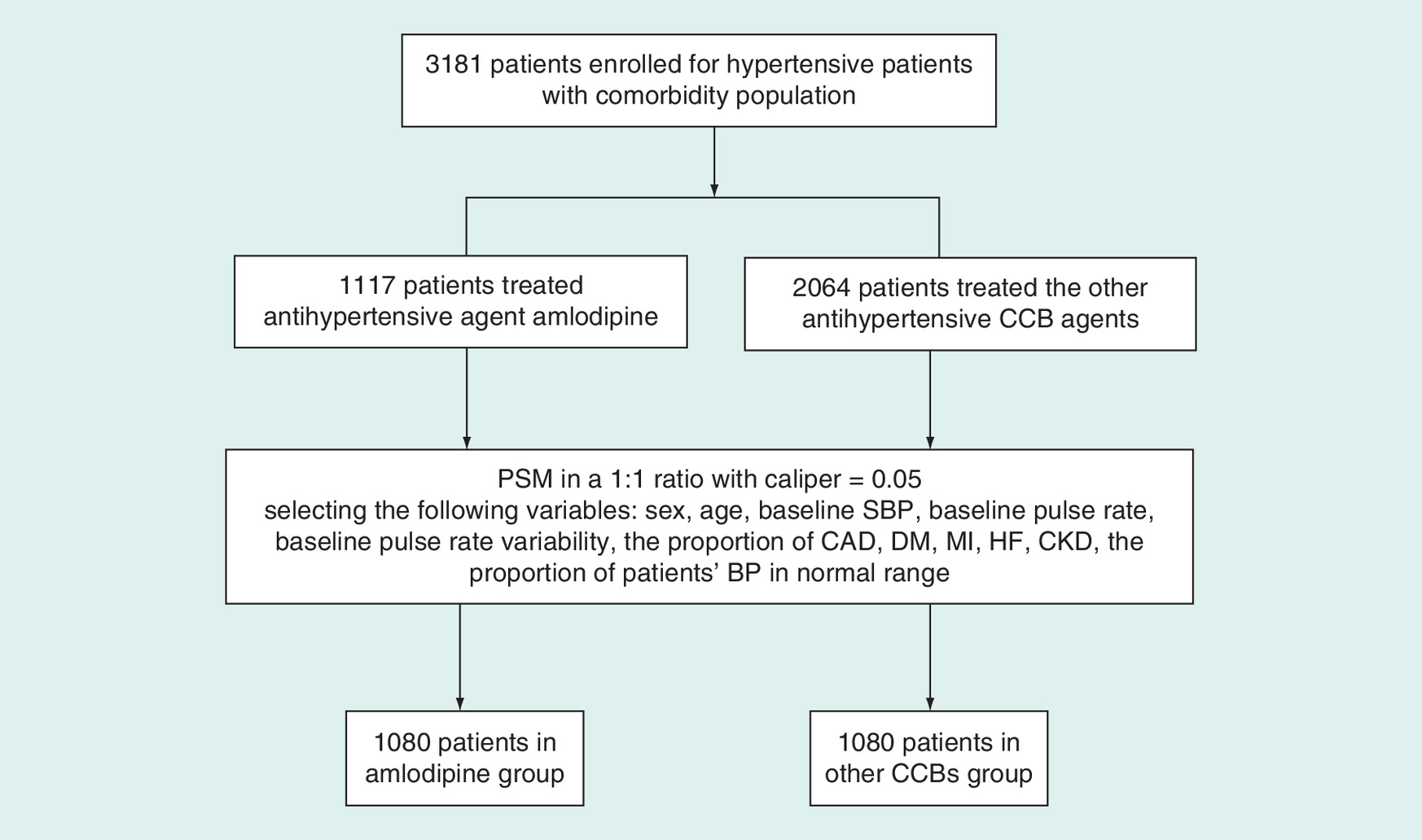
Figure 2. Screen flow for hypertensive patients with comorbidity.
BP: Blood pressure; CAD: Coronary artery disease; CCB: Calcium channel blocker; CKD: Chronic kidney disease; DM: Diabetes mellitus; HF: Heart failure; MI: Myocardial infarction; PSM: Propensity score matching; SBP: Systolic blood pressure.
Effectiveness assessment
BPV were assessed using standard deviation and coefficient of variation of SBP during a single clinical visit.
Statistical analyses
In this study, PSM was used to adjust significant differences in patient characteristics and reduce the influence of possible confounding factors. For the method of PSM, a logistic regression model was calculated with the covariate variables (age, sex, baseline SBP, baseline pulse rate and baseline PRV for general hypertensive population; add the proportion of five kinds of comorbidities and the proportion of patients’ BP in normal range for hypertensive patients with comorbidity population) to obtain the scores. After estimating propensity scores, one-to-one nearest-neighbor matching without replacement was performed with a calliper of width equal to 0.05. The difference of potential confounding variables with p-value of < 0.05 was considered to be statistically significant for each test before and after PSM.
For other statistical methods included in this study, continuous variables are presented as minimum, maximum, mean, standard deviation, median and interquartile range (IQR) per group. Categorical variables are expressed as percentage. For the comparison test, two-tailed Student's t-test for the continuous variables, and Fisher's exact test or χ2 test were used for the categorical variables as appropriate. All tests were two-sided, with statistical significance at p < 0.05. Analyses were conducted with the R statistical package v.2.13.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
PSM results
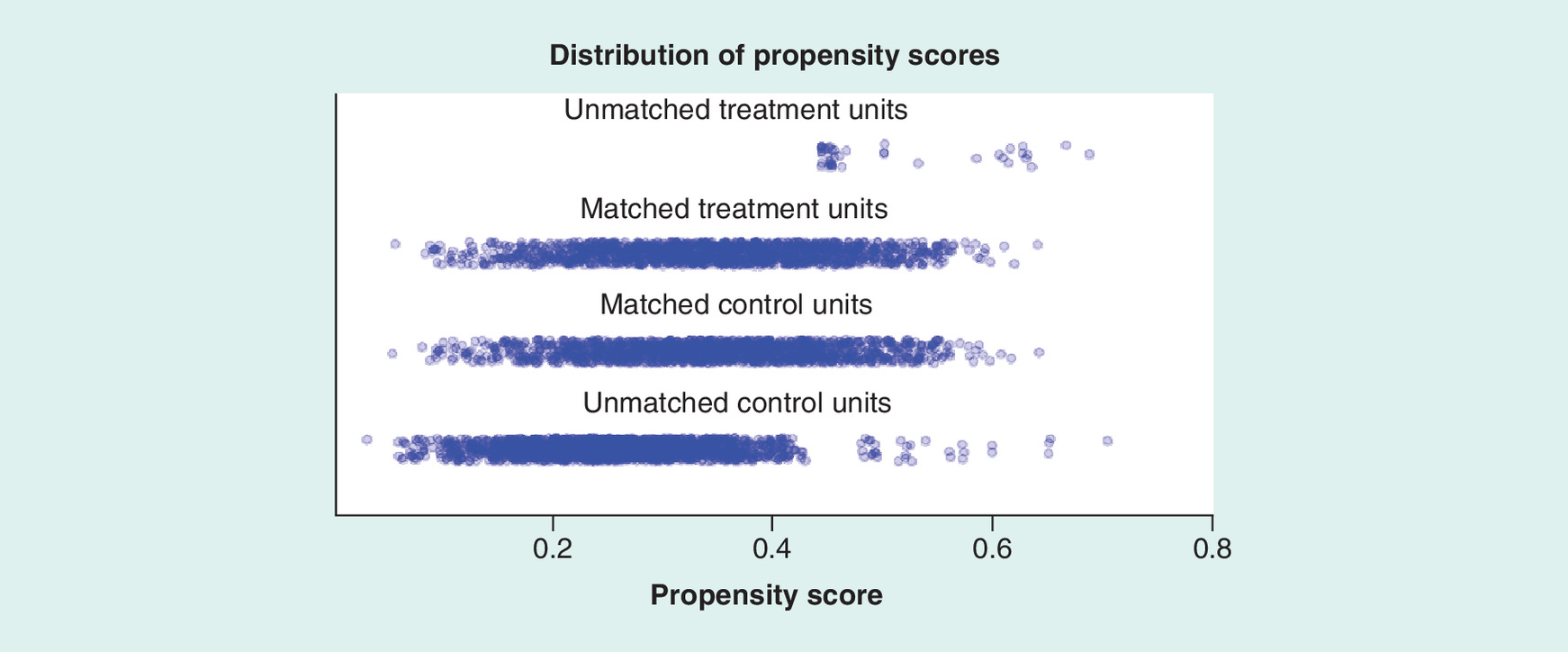
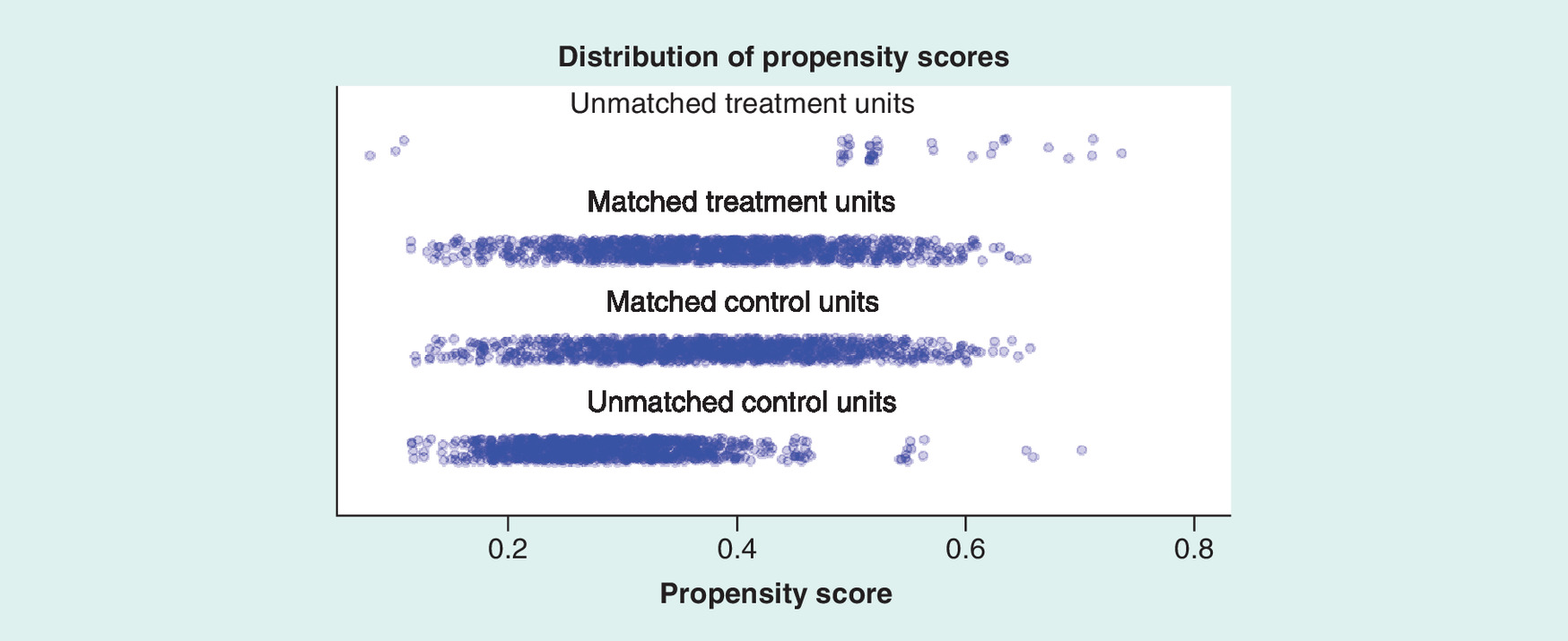
Of the 5582 patients enrolled in general hypertensive population, 1805 and 3777 patients were divided into amlodipine group and control group according to the administration. 3512 patients in 1756 pairs were finally assigned to each differently treated group. Table 1 displays the patient characteristics before and after PSM for two groups. Before PSM, the patients in the amlodipine group were significantly more likely to be older. Additionally, the baseline SBP were significantly lower than the other CCBs group. For the baseline pulse rate and baseline PRV, the patients in amlodipine group have higher values then the control group. After PSM, the age, baseline SBP, pulse rate and PRV were evenly dispersed and did not differ significantly between two groups, validating the propensity score-matched model success (Table 1 & Figure 3). For the hypertensive population with comorbidity, the proportion of five kinds of comorbidities and the proportion of patients’ BP in normal range were the other factors needed to be considered through PSM as covariates besides the covariate variables mentioned above. Table 2 displays patient characteristics before and after PSM for the comorbidity population. Before PSM, all of the covariates have significant difference between two groups. For example, the patients in amlodipine group were significantly older than the control group, the proportion of male and the proportion of the patients who have normal BP in amlodipine group were significantly higher than the control group, the baseline SBP in amlodipine group is significantly lower than the control group, the baseline pulse rate and PRV in amlodipine group were significantly higher than the control group, the distribution of five kinds of comorbidities in amlodipine is significantly different from the distribution in control group. After PSM, the difference existing in the two groups has been balanced for all the covariates (Figure 4). This work ensured that the difference between the two groups is from the administrated agents instead of the bias.
| Characteristic | Amlodipine | Other CCBs | p-value | |
|---|---|---|---|---|
| Before PSM | n | 1805 | 3777 | |
| Age (years), (mean ± SD) | 70.2 ± 12.55 | 65.2 ± 13.37 | < 0.05 | |
| Gender (male), n (%) | 0.5 (0.5) | 0.48 (0.52) | 0.14 | |
| Baseline SBP (mmHg), (mean ± SD) | 135.2 ± 11.77 | 137.7 ± 12.81 | < 0.05 | |
| Baseline pulse rate (beats per minute), (mean ± SD) | 82.5 ± 10.05 | 80.8 ± 8.8 | < 0.05 | |
| Baseline pulse rate variability | 9.4 ± 4.98 | 8.4 ± 4.43 | < 0.05 | |
| After PSM | n | 1756 | 1756 | |
| Age (years), (mean ± SD) | 70 ± 12.52 | 69.2 ± 12.64 | 0.107 | |
| Gender (male), n (%) | 0.5 (0.5) | 0.5 (0.5) | 0.986 | |
| Baseline SBP (mmHg) (mean ± SD) | 135.4 ± 11.72 | 135.9 ± 12.21 | 0.245 | |
| Baseline pulse rate (beats per minute), (mean ± SD) | 82.4 ± 9.95 | 82.3 ± 9.72 | 0.703 | |
| Baseline pulse rate variability | 9.3 ± 4.91 | 9.3 ± 4.71 | 0.890 |
Pulse rate variability was assessed with the same algorithm as blood pressure variability.
CCB: Calcium channel blocker; PSM: Propensity score matching; SBP: Systolic blood pressure; SD: Standard deviation.
| Characteristics | Amlodipine | Other CCBs | p-value | |
|---|---|---|---|---|
| Before PSM | n | 1117 | 2064 | |
| Age (years), (mean ± SD) | 72.2 ± 12.6 | 68.2 ± 12.26 | < 0.05 | |
| Gender (male), n (%) | 0.52 (0.48) | 0.45 (0.55) | < 0.05 | |
| Baseline SBP (mmHg), (mean ± SD) | 136.9 ± 11.99 | 139 ± 13.57 | < 0.05 | |
| BP status (normal), n(%) | 0.62 (0.38) | 0.56 (0.44) | < 0.05 | |
| Baseline pulse rate (beats per minute) | 82.3 ± 9.98 | 81.1 ± 8.93 | < 0.05 | |
| Baseline pulse rate variability | 9.2 ± 5.19 | 8.3 ± 4.39 | < 0.05 | |
| Comorbidity | < 0.05 | |||
| CAD | 0.28 | 0.33 | – | |
| DM | 0.44 | 0.44 | – | |
| MI | 0.03 | 0.02 | – | |
| HF | 0.1 | 0.09 | – | |
| CKD | 0.15 | 0.12 | – | |
| After PSM | n | 1080 | 1080 | – |
| Age (years), (mean ± SD) | 72 ± 12.37 | 71.7 ± 11.73 | 0.652 | |
| Gender (male), n (%) | 0.51 (0.49) | 0.51 (0.49) | 1 | |
| Baseline SBP (mmHg), (mean ± SD) | 137 ± 11.9 | 137.6 ± 13.02 | 0.259 | |
| BP status (Normal), n(%) | 0.62 (0.38) | 0.61 (0.39) | 0.626 | |
| Baseline pulse rate (beats per minute) | 82.3 ± 9.96 | 82.4 ± 9.52 | 0.762 | |
| Baseline pulse rate variability | 9.1 ± 4.96 | 9.1 ± 4.6 | 0.924 | |
| Comorbidity | 0.241 | |||
| CAD | 0.29 | 0.28 | ||
| DM | 0.44 | 0.41 | ||
| MI | 0.03 | 0.03 | ||
| HF | 0.09 | 0.13 | ||
| CKD | 0.15 | 0.15 |
BP: Blood Pressure; CAD: Coronary artery disease; CCB: Calcium channel blocker; CKD: Chronic kidney disease; DM: Diabetes mellitus; HF: Heart failure; MI: Myocardial infarction; PSM: Propensity score matching; SBP: Systolic blood pressure; SD: Standard deviation.
Patient characteristics
Patients’ demographics and characteristics for general hypertensive population and hypertensive patients with comorbidity population were summarized in Table 3. For general hypertensive patients, their mean ages in two groups were all 70 years old (IQR, 63–80 years old for amlodipine group and 62–79 for other CCBs group, respectively). 50.2% were male in amlodipine group and 50.1% in the control group. The age group of 65–80 years old have the highest proportion in two groups. The patients who were concomitant with DM have the highest proportion in five comorbidities. The two groups have similar mean of SBP. For the hypertensive patients with comorbidity population, the mean age was 72 years old for amlodipine group (IQR, 65–81 years old), 72 years old for control group (IQR, 65–80 years old). 51.4% were male in amlodipine group and 51.5% in the control group. The age group of 65–80 years old has the highest proportion in two groups. Of five kinds of comorbidities, nearly half were concomitant with DM. For the mean baseline SBP, there was little difference between two groups.
| General population | With comorbidity | ||||
|---|---|---|---|---|---|
| Demo | Amlodipine (n = 1756) | Other CCBs (n = 1756) | Amlodipine (n = 1080) | Other CCBs (n = 1080) | |
| Age (years) | Mean | 70 | 70 | 72 | 72 |
| SD | 13 | 13 | 12 | 12 | |
| Min | 26 | 23 | 26 | 26 | |
| Q1 | 63 | 62 | 65 | 65 | |
| Median | 72 | 72 | 74 | 73 | |
| Q3 | 80 | 79 | 81 | 80 | |
| Max | 98 | 100 | 98 | 100 | |
| Age group (years) n (%) | <50 | 117 (0.067) | 126 (0.072) | 61 (0.056) | 54 (0.05) |
| ≥50 – <65 | 410 (0.233) | 394 (0.224) | 205 (0.19) | 208 (0.193) | |
| ≥65 – <80 | 757 (0.431) | 811 (0.462) | 472 (0.437) | 516 (0.478) | |
| ≥80 | 472 (0.269) | 425 (0.242) | 342 (0.317) | 302 (0.28) | |
| Gender | Male | 881 (0.502) | 880 (0.501) | 555 (0.514) | 556 (0.515) |
| Female | 875 (0.498) | 876 (0.499) | 525 (0.486) | 524 (0.485) | |
| Comorbidity | CAD | 299 (0.17) | 347 (0.198) | 308 (0.285) | 306 (0.283) |
| DM | 470 (0.268) | 420 (0.239) | 478 (0.443) | 444 (0.411) | |
| MI | 28 (0.016) | 28 (0.016) | 29 (0.027) | 28 (0.026) | |
| HF | 110 (0.063) | 88 (0.05) | 101 (0.094) | 137 (0.127) | |
| CKD | 169 (0.096) | 101 (0.058) | 164 (0.152) | 165 (0.153) | |
| Other | 680 (0.387) | 772 (0.44) | – | – | |
| SBP(mmHg) | Mean (SD) | 136.09 (11.791) | 136.09 (11.791) | 137.04 (11.898) | 137.65 (13.018) |
CAD: Coronary artery disease; CCB: Calcium channel blocker; CKD: Chronic kidney disease; DM: Diabetes mellitus; HF: Heart failure; MI: Myocardial infarction; SBP: Systolic blood pressure; SD: Standard deviation.
Effectiveness assessment
For the comparison of BPV between two groups, the BPV for amlodipine group was significantly lower than the control group no matter for general hypertensive patients or for hypertensive patients with comorbidity, and statistical significance was achieved, as shown in Table 4. This result indicates that the patients treated with amlodipine had a better BPV control than the patients treated with the other CCBs.
| Amlodipine | Other CCBs | Diff. (95% CI) | p-value | ||
|---|---|---|---|---|---|
| General population | n | 1756 | 1756 | – | – |
| SD | 12.90 | 13.76 | -0.86 (-1.26 to -0.47) | < 0.05 | |
| CV | 9.47 | 10.06 | -0.59 (-0.87 to -0.32) | < 0.05 | |
| With comorbidity | n | 1080 | 1080 | – | – |
| SD | 13.24 | 14.23 | -0.98 (-1.52 to -0.44) | < 0.05 | |
| CV | 9.66 | 10.28 | -0.62 (-0.99 to -0.25) | < 0.05 |
CCB: Calcium channel blocker; CV: Coefficient of variation; SD:Standard deviation.
Discussion
This study was undertaken to answer clinical questions regarding BPV for different antihypertensive treatments. Since this study is an observational and retrospective design, the bias is probable. For example, patients with lower BP may have been selected for amlodipine group more frequently than patients with a higher BP in a real world clinical setting. If the selection bias exists, it is difficult to determine that the difference between two groups is due to antihypertensive agents or due to bias. An important aspect of this study is the introduction of PSM methodology in order to reduce bias. To begin with, we investigated the major determinants of BPV from the publications. It was found that age, sex, baseline SBP, pulse rate and PRV were frequently reported in several population studies [13–15]. Therefore, we included these five factors mentioned above in a list of possible confounders for general hypertensive population. For the hypertensive patients with comorbidity, considering the different influences that may be caused from different kinds of comorbidities, the proportion of comorbidity is also regarded as a potential confounder. Additionally, the proportion of patients having the normal BP range has been regarded as the other confounder through PSM. The balance analysis checks if these variables are distributed equally between amlodipine and other CCB groups, the perfect matched results make us believe that the majority of the estimated treatment effect is due to amlodipine treatment rather than confounding.
Hypertension is a risk factor for many diseases. BP goals for patients with hypertension are well defined in current management guidelines. Nevertheless, the BPV has been omitted during treatment, usually in a real-world setting. It is assumed that unexplained differences found between different classes of antihypertensive drugs in their effectiveness for preventing stroke are caused by the class of drugs [16]. Therefore, the appropriate use of antihypertensive drugs and an improved prognosis is challenging for many clinicians. If the BPV could be automatically calculated from EMR data, this would enable doctors to account for both mean and variability in BP concurrently when assessing cardiovascular risk. For example, assuming a standard deviation for variability in SBP of 7 mmHg could be considered at 18% greater risk of cardiovascular disease events than a similar person with the BPV of 2 mmHg. This additional information would have a favourite influence on subsequent risk management [17].
In the analysis of BPV in studies of various patient populations with hypertension, amlodipine was superior to other classes of antihypertensive drugs in reducing BPV. We obtained similar results in our study, amlodipine demonstrates lower BPV than other CCB antihypertensive agents, regardless of the general hypertensive population or the hypertensive patients with comorbidity. For the better effectiveness of amlodipine, there is limited information concerning the underlying mechanism of the superior reduction in BPV for amlodipine. Amlodipine is a well-established, long-acting CCB that effectively reduces BP in hypertension. For the reduction in BPV, Zhang et al. found that it was possibly attributable to lowering BP or ameliorating the autonomic nervous system regulation, or both [12]. In addition, it is reported that short term variability in BP is affected by behavioural, emotional, and postural influences on cardiovascular physiology and cardiac rhythm [17–19]. Furthermore, arterial stiffness also contributes to short and long term variability in BP [20,21]. These findings suggest that amlodipine has better influence on reducing arterial stiffness, arterial compliance improvement, and heart rate regulation.
The present study provided insight for mid-term BPV in patients taking amlodipine or other CCB antihypertensive therapies in a real-world setting. Limitations of this study included five aspects. First, a series of standardized methods to measure BP lacked in this study, for example, the time, position and device of BP measurement were not requested to keep consistency, this usually happens in clinical practice, but this was partially eliminated by the fact that individual patients would likely have been assessed using similar procedures [22]. Second, some lifestyle factors such as smoking habits, alcohol, coffee and psychological stress were not included in the analysis due to nonuniform collection in the EMR. Third, some characteristics including weight, BMI and waist-to-hip ratio were also not included in the study due to missing information for most of the patients. Fourth, the duration for treatment or for measurement may be different for each patient, these kinds of difference were not considered in the analysis. Last, although we applied stringent criteria for inclusion and exclusion in our study, we also used PSM method and a narrow calliper to balance the bias, which sacrificed the sample size used for analysis, selection bias may be hidden among unmeasured covariates that were not included in our data. It is meaningful that we investigate the determinants of BPV firstly, which can determine most of the factors that may cause major influence on BPV.
Conclusion
This study focused on clinically observed hypertension patients, extracted from EMR data in the real-world setting. The patients receiving amlodipine showed lower BPV compared with the patients receiving the other CCB antihypertensive drugs regardless of the general hypertensive population or hypertensive patients within the comorbidities population. These findings suggest that it could be beneficial to use amlodipine to control within-visit BPV compared to the other CCB antihypertensive drugs. However, further investigation needs to be performed to explore whether monotherapy amlodipine or amlodipine combined with the other drugs will obtain better effectiveness in reducing BPV.
Recent studies demonstrated that blood pressure variability (BPV) is also an independent risk factor other than average blood pressure for vascular events.
Limit study about BPV for different kinds of antihypertensive drugs in practical clinical practice were performed.
This study focused on clinically observed hypertension patients extracted from electronic medical record data in the real-world setting. BPV calculating with standard deviation and coefficient of variation of systolic blood pressure during a single inpatient visit were comparing between amlodipine and the other calcium channel blockers (CCB). The general hypertensive population or hypertensive patients within the comorbidities population were included in the analysis. The propensity score matching was conducted to balance the cohort of patients prescribed amlodipine or other CCBs.
The results demonstrated that the patients receiving amlodipine showed lower BPV compared with the patients receiving the other CCB antihypertensive drugs for general hypertensive patients and patients with comorbidities.
These findings suggest that it could be beneficial to use amlodipine to control within-visit BPV compared to the other CCB antihypertensive drugs.
Acknowledgements
We thank B Fa, H Yao and R Xu who performed the statistical analysis and database support at Palan DataRx, and all the participants in the present study for their generous cooperation.
Financial & competing interests disclosure
L Zhang and JK Yang acted as consultants for Pfizer. LT Li and Y Lin are paid consultants to Pfizer. DD Liu, XP Xie and P Dong are employees of Pfizer. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Perkovic V, Huxley R, Wu Y, Prabhakaran D, Macmahon S. The burden of blood pressure-related disease: a neglected priority for global health. Hypertension 50(6), 991–997 (2007).
2.
Wang JG, Yan P, Jeffers BW. Effects of amlodipine and other classes of antihypertensive drugs on long-term blood pressure variability: evidence from randomized controlled trials. J. Am. Soc. Hypertens. 8(5), 340–349 (2014).
3.
Kearney PM, Whelton M, Reynolds K, Whelton PK, He J. Worldwide prevalence of hypertension: a systematic review. J. Hypertens. 22(1), 11–19 (2004).
4.
Turner JR, O'Brien E. Diagnosis and treatment of resistant hypertension: the critical role of ambulatory blood pressure monitoring. J. Clin. Hypertens. 15(12), 868–873 (2013).
5.
Wang J, Shi X, Ma C et al. Visit-to-visit blood pressure variability is a risk factor for all-cause mortality and cardiovascular disease: a systematic review and meta-analysis. J. Hypertens. 35(1), 10–17 (2017).
6.
Blacher J, Safar ME, Ly C, Szabo De Edelenyi F, Hercberg S, Galan P. Blood pressure variability: cardiovascular risk integrator or independent risk factor? J. Hum. Hypertens. 29(2), 122–126 (2015).
7.
Floras JS. Blood pressure variability: a novel and important risk factor. Can. J. Cardiol. 29(5), 557–563 (2013).
8.
Shi R, Liu K, Shi D, Liu Q, Chen X. Effects of amlodipine and valsartan on blood pressure variability and pulse wave velocity in hypertensive patients. Am. J. Med. Sci. 353(1), 6–11 (2017).
9.
Eguchi K, Imaizumi Y, Kaihara T, Hoshide S, Kario K. Comparison of valsartan and amlodipine on ambulatory blood pressure variability in hypertensive patients. Clin. Exp. Hypertens. 38(8), 721–724 (2016).
10.
Karpov YA, Gorbunov VM, Deev AD. Effectiveness of fixed-dose perindopril/amlodipine on clinic, ambulatory and self-monitored blood pressure and blood pressure variability: an open-label, non comparative study in the general practice. High Blood Press. Cardiovasc. Prev. 22(4), 417–425 (2015).
11.
Hata J, Arima H, Rothwell PM et al. Effects of visit-to-visit variability in systolic blood pressure on macrovascular and microvascular complications in patients with Type 2 diabetes mellitus: the ADVANCE trial. Circulation 128(12), 1325–1334 (2013).
12.
Zhang Y, Agnoletti D, Safar ME, Blacher J. Effect of antihypertensive agents on blood pressure variability: the Natrilix SR versus candesartan and amlodipine in the reduction of systolic blood pressure in hypertensive patients (X-CELLENT) study. Hypertension 58(2), 155–160 (2011).
13.
Shin JH, Shin J, Kim BK et al. Within-visit blood pressure variability: relevant factors in the general population. J. Hum. Hypertens. 27(5), 328–334 (2013).
14.
Myers MG, Reeves RA. White coat effect in treated hypertensive patients: sex differences. J. Hum. Hypertens. 9(9), 729–733 (1995).
15.
Su H, Wang J, Zhu Y, Wang G, Cheng X. Discrepancy among three blood pressure readings within one measurement and relevant influencing factors. Blood Press. Monit. 15(3), 152–157 (2010).
16.
Webb AJ, Fischer U, Mehta Z, Rothwell PM. Effects of antihypertensive-drug class on interindividual variation in blood pressure and risk of stroke: a systematic review and meta-analysis. Lancet 375(9718), 906–915 (2010).
17.
Stevens SL, Wood S, Koshiaris C et al. Blood pressure variability and cardiovascular disease: systematic review and meta-analysis. BMJ 354, i4098 (2016).
18.
Parati G, Ochoa JE, Lombardi C, Bilo G. Assessment and management of blood-pressure variability. Nature Rev. Cardiol. 10(3), 143–155 (2013).
19.
Mancia G. Short- and long-term blood pressure variability: present and future. Hypertension 60(2), 512–517 (2012).
20.
Garcia-Garcia A, Garcia-Ortiz L, Recio-Rodriguez JI et al. Relationship of 24-h blood pressure variability with vascular structure and function in hypertensive patients. Blood Press. Monit. 18(2), 101–106 (2013).
21.
Schillaci G, Bilo G, Pucci G et al. Relationship between short-term blood pressure variability and large-artery stiffness in human hypertension: findings from 2 large databases. Hypertension 60(2), 369–377 (2012).
22.
Smith TR, Drozda JP Jr, Vanslette JA, Hoeffken AS, Nicholson RA. Medication class effects on visit-to-visit variability of blood pressure measurements: analysis of electronic health record data in the “real world”. J. Clin. Hypertens. 15(9), 655–662 (2013).
•• This study used the data extracted from an EHR-derived database and revealed that all medication classes (defined by the Systematized Nomenclature of Medicine) were associated with a statistically significant effect on visit-to-visit variability of blood pressure.
23.
Dunnett CW. A multiple comparison procedure for comparing several treatments with a control. J. Am. Stat. Assoc. 50, 1096–1121 (1955).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 14 August 2017
Accepted: 27 March 2018
Published online: 11 June 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison of amlodipine versus other calcium channel blockers on blood pressure variability in hypertensive patients in China: a retrospective propensity score-matched analysis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0063
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Longguo Zhao, Vipin Kumar, Megumi Narisawa, Yanglong Li, Chunzi Jin, Xian Wu Cheng, Systolic Blood Pressure Time in the Target Range and Blood Pressure Variability: The Effects of Amlodipine‐Based Therapy, The Journal of Clinical Hypertension, 10.1111/jch.70160, 27, 10, (2025).
- Jinghan Yang, Shuling Chen, Dajun Chai, Feng Peng, Ningling Sun, Jinxiu Lin, Amlodipine‐Based Therapy and Its Effect on Time in Target Range and Long‐Term Blood Pressure Variability Across Age Groups in Chinese Patients With Primary Hypertension: A Retrospective Study, The Journal of Clinical Hypertension, 10.1111/jch.70151, 27, 9, (2025).
- 俊慧 李, The Impact of Different Antihypertensive Medications on Blood Pressure Variability in Hypertensive Patients and Clinical Application Progress, Advances in Clinical Medicine, 10.12677/acm.2025.151078, 15, 01, (565-572), (2025).
- Anurag Sharma, Tushor Roy, Paramartha Bhattacharya, Dinesh Agarwal, Rohit Kumar, Syed Mujtaba Hussain Naqvi, Rajan Mittal, Stable Angina Pectoris: A Review of Pathophysiology, Diagnosis, and Its Management, Journal of The Association of Physicians of India, 10.59556/japi.72.0704, 72, 11, (92-97), (2024).
- Robert P. Blankfield, Is fluid retention a cardiovascular risk factor?, Clinical Hemorheology and Microcirculation, 10.3233/CH-242128, 88, 2, (277-288), (2024).
- Jae Hoon Kim, Ji Hye Song, MinYoung Kim, Jang Hee Hong, Jung Sunwoo, Jin-Gyu Jung, Pharmacokinetic Comparison of a Fixed-Dose Combination of Candesartan Cilexetil/Amlodipine/Atorvastatin Versus Co-administration of Individual Formulations in Healthy Participants, Advances in Therapy, 10.1007/s12325-024-02869-y, 41, 7, (2808-2825), (2024).
- SungA Bae, Wan Kee Kim, Seng Chan You, Minkwan Kim, In Hyun Jung, Impact of amlodipine on clinical outcomes for heart failure in patients with dilated cardiomyopathy: a Korean nationwide cohort study, Frontiers in Cardiovascular Medicine, 10.3389/fcvm.2023.1305824, 10, (2023).
- Indriastuti Cahyaningsih, Nurul Hikmah, Nurul Maziyyah, Drug-related problems in elderly patients with diabetes: A study in primary health care setting, Journal of Advanced Pharmacy Education and Research, 10.51847/RgpUP8AeB3, 13, 2, (29-34), (2023).
- Marc D Basson, William E Newman, Marilyn G Klug, Correlations Among Visit-to-Visit Blood Pressure Variability and Treatment With Antihypertensive Medication With Long-Term Adverse Outcomes in a Large Veteran Cohort, American Journal of Hypertension, 10.1093/ajh/hpab087, 34, 10, (1092-1099), (2021).
- L. Parker Gregg, S. Susan Hedayati, Hui Yang, Peter N. Van Buren, Subhash Banerjee, Sankar D. Navaneethan, Salim S. Virani, Wolfgang C. Winkelmayer, Carlos A. Alvarez, Association of Blood Pressure Variability and Diuretics With Cardiovascular Events in Patients With Chronic Kidney Disease Stages 1–5, Hypertension, 10.1161/HYPERTENSIONAHA.120.16117, 77, 3, (948-959), (2021).