Budget impact analysis of long-acting injectable aripiprazole once-monthly 400 mg in bipolar I disorder in the USA
Abstract
Aim: To estimate the budget impact (BI) of introducing aripiprazole once-monthly 400 mg/300 mg (AOM 400) in the maintenance monotherapy treatment of bipolar I disorder versus long-acting injectables, oral antipsychotics and best supportive care. Methods: A BI model was developed from a US-payer perspective using treatment-related, hospitalization and adverse event management cost estimates for a hypothetical 1,000,000-member health plan over a 5-year period. Results: Market share of AOM 400 was predicted to increase from 0.6% in Year 1 (current scenario) to 1.3% in Year 5 (predicted scenario), with predicted increases for paliperidone palmitate, asenapine and cariprazine. Treatment-related costs explained the BI increase, while adverse event and hospitalization costs were reduced. The per member per month incremental cost ranged from US$0.06 to US$0.26 in Years 1–5. The largest increases were predicted for paliperidone palmitate. Conclusion: As market shares of atypical antipsychotics are predicted to increase, payers may wish to re-evaluate their use.
Bipolar disorder (BP) is a cyclical mood disorder characterized by periods of mania, hypomania, or depression that may persist over the lifetime of the patient, causing disruption to mood and impaired functioning [1,2]. The most severe subtype is widely recognized to be bipolar I disorder (BP-I), which is diagnosed by a history of one or more manic episodes [1]. The lifetime prevalence of BP-I is estimated at 0.6–2.1% [3,4].
The economic burden of BP-I is demonstrated in a recent cost analysis performed in the USA, which assessed the excess direct and indirect healthcare costs for the population with BP-I compared with the general population for the year 2015 [5]. Excess direct healthcare costs for the BP-I population, including pharmacy and general medical services, were US$25.2 billion, excess direct nonhealthcare costs (most relating to substance abuse) were US$6.8 billion and excess indirect costs relating to lost productivity and caregiving were US$87.8 billion. The study authors concluded that effective treatments and practices should be targeted at improving not only medical resource utilization but also the functional abilities of individuals with BP-I in order to reduce disease burden.
Maintenance therapy is the treatment given to a patient after an acute episode of mania or depression has passed. The main goal of maintenance treatment is to avoid the recurrence of further episodes of mania and depression as well as to minimize ‘subsyndromal’ symptoms of depression. These latter symptoms may impair life quality and functioning but do not fully meet the criteria for a depressive episode. Current treatment approaches in BP-I remain unsatisfactory in large part because of the low rates of patient adherence [6,7]. Long-acting injectable (LAI) formulations of atypical antipsychotics were developed to improve patient adherence and can be administered – according to formulation – either biweekly, monthly or at longer intervals, which provides advantages over the daily dosing of oral treatments [8,9]. Aripiprazole is an atypical antipsychotic approved by the US FDA as an oral formulation for the treatment of acute manic or mixed episodes of BP-I [10]. Oral aripiprazole has proven efficacy also as a maintenance treatment for BP-I [11]. Aripiprazole once-monthly 400 mg/300 mg (AOM 400) is an LAI formulation of aripiprazole that is administered once monthly. A 52-week, double-blind, placebo-controlled, randomized withdrawal trial demonstrated that AOM 400 delayed the time to, and reduced the rate of, recurrence of mood episodes (NCT01567527) [12]. Based on these results, AOM 400 recently received approval from the FDA for the maintenance monotherapy treatment of BP-I in adults [13].
A modeling study from a US healthcare payer perspective concluded that AOM 400 represents a cost-effective maintenance monotherapy treatment of BP-I and is associated with a lower estimated number of mood episodes and hospitalizations than other atypical antipsychotics included in that analysis: namely, risperidone LAI, paliperidone palmitate, cariprazine, asenapine and best supportive care (BSC) [14]. The objective of the present analysis was to evaluate the budget impact (BI) from the healthcare payer perspective of establishing AOM 400 as a maintenance monotherapy treatment of BP-I in adults, when compared with the same comparator treatments as included in the cost–effectiveness analysis mentioned above.
Methods
Modeling approach
A BI model was developed to assess the incremental impact of AOM 400 as a maintenance monotherapy treatment of BP-I in a hypothetical cohort of 1,000,000 insured health plan members (Figure 1). The total costs of maintenance treatment in the current scenario (observed) were compared with a predicted scenario (projected) that included increased uptake of AOM 400 and other branded antipsychotics according to market share estimations over a 5-year-time horizon.
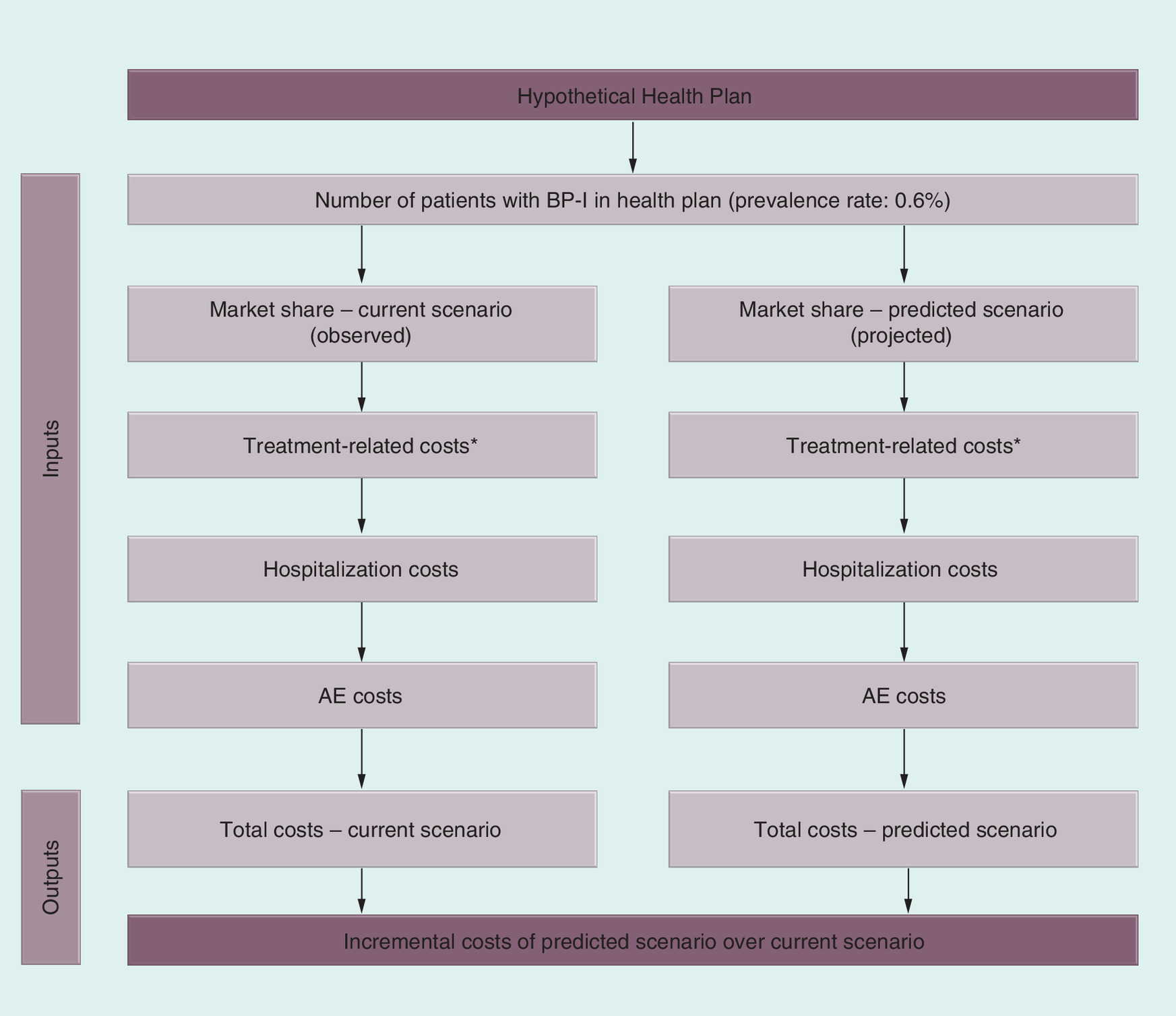
Figure 1. Budget impact model structure.
*Treatment-related cost include: drug acquisition, administration and long-acting injectable treatment-initiation costs.
BP-I: Bipolar I disorder.
The first step in the BI analysis was to estimate the total number of patients eligible to receive maintenance treatment for BP-I; secondly to determine the proportions of patients in both scenarios who would receive each treatment every year for the 5-year time horizon; and finally to estimate the costs associated with drug acquisition, hospitalization and treatment-emergent adverse events (AEs) for each treatment. Discounting was not included.
Population
Treatments included in the analysis
Treatments in the treatment mix included, in addition to AOM 400, the branded LAI atypical antipsychotics: risperidone (the only other LAI approved in the USA for maintenance treatment of BP-I) and paliperidone palmitate (frequently used off-label for maintenance treatment of BP-I) and oral branded atypical antipsychotics: cariprazine and asenapine (the only branded oral antipsychotics with an indication for acute treatment of manic or mixed episodes associated specifically with BP-I in adults). Placebo treatment was used as a proxy for BSC.
Input data
Drug acquisition costs
Information on the dosing and the number of administrations for each drug was taken from the FDA labels. The dose mix for each drug was extracted from Truven MarketScan® Medicaid and Medicare/Commercial Database (Truven Health Analytics, MI, USA) for the period 1 July 2015 to 20 June 2016. Unit costs were from the RED BOOK™ (Thomson Reuters:PDR Network, NJ, USA) accessed in February 2017 [16]. Wholesale acquisition costs (WAC) were used in the base-case model since these are most appropriate from the US healthcare payer perspective (Tables 1 & 2).
| Treatments | WAC (US$) unit cost [16] | Number of administrations per year | Cost per year (US$) |
|---|---|---|---|
| Formulation (% patients) | |||
| AOM 400 | – | – | – |
| 300 mg (17.8) | 1407.59 | 12.00 [13] | 16,891 |
| 400 mg (82.2) | 1876.79 | – | 22,521 |
| Average | 21,522 | ||
| Paliperidone palmitate | |||
| 39 mg (0.3) | 382.89 | 12.00 [17] | 4595 |
| 78 mg (2.0) | 765.82 | – | 9190 |
| 117 mg (23.9) | 1148.74 | – | 13,785 |
| 156 mg (39.5) | 1531.72 | – | 18,381 |
| 234 mg (34.3) | 2297.52 | – | 27,570 |
| Average | 20,205 | ||
| Risperidone LAI | 26.00 [18] | ||
| 12.5 mg (5.7) | 208.25 | – | 5415 |
| 25 mg (32.9) | 416.45 | – | 10,828 |
| 37.5 mg (28.7) | 624.71 | – | 16,242 |
| 50 mg (32.8) | 832.96 | – | 21,657 |
| Average | 15,625 | ||
| Cariprazine | |||
| 1.5 mg (32.5) | 33.54 | 365.25 [19] | 12,249 |
| 3 mg (54.0) | 33.54 | – | 12,249 |
| 4.5 mg (7.9) | 33.54 | – | 12,249 |
| 6 mg (5.5) | 33.54 | – | 12,249 |
| Average | 12,249 | ||
| Asenapine | |||
| 2.5 mg (5.4) | 18.28 | 365.25 [20] | 6676 |
| 5 mg (36.1) | 16.02 | – | 5850 |
| 10 mg (58.5) | 16.02 | – | 5850 |
| Average | 5894 | ||
AOM: Aripiprazole once-monthly; LAI: Long-acting injectable; WAC: Wholesale acquisition cost.
| Treatment | Cost per day (US$) | Duration | Cost of oral overlap (US$) | Ref. |
|---|---|---|---|---|
| Oral aripiprazole prior to AOM 400 | 9.69 | 14 days | 135.71 | [16] |
| Oral risperidone prior to risperidone LAI | 5.60 | 21 days | 117.69 | [16] |
| Treatment | Drug cost (US$) | Administration cost (US$) | Cost of intramuscular overlap (US$) | |
| Initiation dose of paliperidone palmitate lon-acting injectable (234 mg on Day 0; 156 mg on Day 8) | 3829.24 | 53.23 | 3882.47 | [21] |
AOM: Aripiprazole once monthly; LAI: Long-acting injectable.
Treatment initiation costs
Treatment initiation costs of LAIs were included for all LAI-naive patients, based on the US prescribing information for each product; these costs were applied in Year 1 of the BI analysis only, and no treatment initiation costs were included for the oral atypical antipsychotics or BSC (Table 2).
Drug administration costs
Drug administration costs were applied for LAI treatments, as these require healthcare visits. The administration cost per year was calculated as the number of visits, based on the FDA prescribing information, multiplied by the cost per visit (US$26.61), obtained from the physician fee schedule code: 96372, ‘Therapeutic, prophylactic, or diagnostic injection (specify material injected); subcutaneous or intramuscular’ [21].
Adverse event costs
AE rates were derived from product labels and/or clinical trial data of the respective treatments for AEs reported in at least 5% of patients in the trials [12,17–20] and calculated as the number of events divided by the sample size for a specific-time period. AE rates for paliperidone palmitate were estimated using data for schizophrenia, as this drug has not been studied in patients with BP. The costs of AEs were derived using the physician fee schedule for the office visit cost and the Medi-Span database WAC [22] (lower price per day) (Table 3).
| Adverse event | Cost (US$) [22] | Resources use (per year) | AOM 400 (%) [12] | Risperidone LAI (%) [18] | Paliperidone palmitate (%) [17] | Cariprazine (%) [19] | Asenapine (%) [20] | BSC (%) [12] |
|---|---|---|---|---|---|---|---|---|
| Abdominal pain | 103.36 | 2 outpatient visits, 1 course of antacid, 1 short course of pain killer | – | – | – | 2.25 | – | – |
| Agitation | 107.98 | 2 outpatient visits, 1 course of low-dose anxiolytic | – | – | 3.33 | – | – | – |
| Akathisia | 107.98 | 2 outpatient visits, 1 course of low-dose anxiolytic | 21.21 | – | – | 6.58 | – | 12.78 |
| Anxiety | 107.98 | 2 outpatient visits, 1 course of low-dose anxiolytic | 6.82 | – | 2.68 | – | – | 4.51 |
| Constipation | 0.00 | Over-the-counter laxative, every day | – | – | – | 2.73 | – | – |
| Decreased appetite | 0.00 | Short course of nutritional substitute (Fortisip), for 90 days | – | 8.33 | – | – | – | – |
| Diarrhea | 51.68 | 1 outpatient visit, week of daily rehydration fluid, and loperamide | – | – | – | 1.77 | – | – |
| Dizziness | 103.36 | 2 outpatient visits, 1 short course of cinnarizine | – | – | 1.54 | 2.09 | 11.00 | – |
| Dry mouth | 206.72 | 4 outpatient visits, daily biotene gel or lozenges | – | – | – | – | – | – |
| Dyspepsia | 103.36 | 2 outpatient visits, daily antacid | – | – | – | 2.57 | – | – |
| Extrapyramidal disorder | 266.99 | 4 outpatient visits, daily low-dose anxiolytic, daily propranolol | – | 29.17 | 0.89 | 8.83 | – | – |
| Fatigue | 0.00 | Short course of nutritional substitute (Fortisip), for 90 days | – | – | – | 1.44 | – | – |
| Headache | 51.68 | 1 outpatient visit, 1 course of pain killer | – | – | 4.95 | 4.33 | 12.00 | – |
| Hypertension | 211.75 | 4 outpatient visits, daily antihypertensive | – | – | – | 1.44 | – | – |
| ISR | 51.68 | 1 outpatient visit, 1 topical antihistamine cream | – | – | 2.92 | – | – | – |
| Insomnia | 266.99 | 4 outpatient visits, daily low-dose anxiolytic | 7.58 | – | – | 2.73 | 6.00 | 7.52 |
| Nausea | 57.28 | 1 outpatient visit, 1 course of antiemetics | – | – | – | 3.85 | – | – |
| Restlessness | 107.98 | 2 outpatient visits, 1 course of low-dose anxiolytic | – | – | – | 2.25 | – | – |
| Somnolence/sedation | 51.68 | 1 outpatient visit | – | 9.72 | 2.19 | 2.41 | 24.00 | – |
| Tremor | 66.53 | 1 outpatient visit, 90-day course of propranolol | – | 33.33 | – | – | – | – |
| Upper respiratory tract infection | 114.11 | 2 outpatient visits, 2 courses of broad spectrum antibiotics | – | 8.33 | – | – | – | – |
| Vomiting | 54.48 | 1 outpatient visit, 1 course of antiemetics | – | – | 1.46 | 2.89 | – | – |
| Weight increase | 0.00 | No additional action | 23.48 | 9.72 | – | – | 5.00 | 18.05 |
AOM: Aripiprazole once monthly; BSC: best standard of care; ISR: Injection site reaction; LAI: Long-acting injectable.
Hospitalization
The total probability of a mood episode for AOM 400 and placebo (proxy of BSC) was obtained from clinical trial data [12] and is calculated as a sum of their relapse rates. For the other LAIs, the probability of a hospitalization was estimated by using the relapse rate for BSC (placebo as proxy) and multiplying it by the relative risks of relapse into manic, mixed and depressive episodes for each comparator presented in a systematic literature review [23]. For paliperidone palmitate, the relative risk for paliperidone oral was used as a proxy, as no data are available for the LAI formulation. The rate of relapse per mood episode for the two oral comparators was assumed to be the average of the estimated rates within the atypical antipsychotics group (aripiprazole, olanzapine, paliperidone and quetiapine).
Hospitalization costs were included in the BI model as treatment-specific costs, as shown in Table 4. The hospitalization cost for an admission for a principal diagnosis of BD (US$6678.81) was estimated using weighted national estimates from the Healthcare Cost and Utilization Project and National Inpatient Sample [24]. The total cost of hospitalization for each treatment was estimated by multiplying the average cost of a hospitalization by the proportion of the patients who were hospitalized.
| Treatment | Proportion of patients [12,23] | Average cost (US$) [24] | Total hospitalization cost per year (US$) |
|---|---|---|---|
| AOM 400 | 25.76% | 1720 | |
| Paliperidone palmitate† | 40.87% | 2730 | |
| Risperidone LAI | 33.17% | 6678.81 | 2215 |
| Cariprazine | 31.75% | 2120 | |
| Asenapine | 31.75% | 2120 | |
| BSC | 51.20% | 3420 |
†Based on oral formulation because paliperidone palmitate is not approved for bipolar disorder.
AOM: Aripiprazole once-monthly; BSC: Best standard of care; LAI: Long-acting injectable.
Market shares
Market share data in the BI analysis were based on the Truven Health MarketScan Commercial and Medicare Supplemental Data Database, from January 2015 to June 2016, for individuals diagnosed with BP at any point during that time [25]. Market shares for current and predicted scenarios were estimated using the assumptions cited below.
Current scenario
Market share data in the current scenario were based on the period 1 July 2015 to 10 June 2016, the most recent year available, and were assumed to remain stable through the 5-year time horizon (Table 5). The patients not treated with one of the included drugs but with another treatment on the market were assumed to be receiving BSC. Therefore, the market share of BSC was calculated as 1 minus the sum of the other agents’ market shares.
| Treatment | Year 1 (%) | Year 2 (%) | Year 3 (%) | Year 4 (%) | Year 5 (%) |
|---|---|---|---|---|---|
| AOM 400 | 0.59 | 0.59 | 0.59 | 0.59 | 0.59 |
| Paliperidone palmitate | 2.09 | 2.09 | 2.09 | 2.09 | 2.09 |
| Risperidone LAI | 0.70 | 0.70 | 0.70 | 0.70 | 0.70 |
| Cariprazine | 0.04 | 0.04 | 0.04 | 0.04 | 0.04 |
| Asenapine | 1.21 | 1.21 | 1.21 | 1.21 | 1.21 |
| BSC | 95.37 | 95.37 | 95.37 | 95.37 | 95.37 |
AOM: Aripiprazole once-monthly; BSC: Best standard of care; LAI: Long-acting injectable.
Predicted scenario
The absolute difference in market share between 2015–2016 and 2014–2015 was added cumulatively each year to the market share data for 2015–2016 (considered Year 0) to estimate the market shares for each treatment in Years 1–5 (Table 6).
| Treatment | Year 1 (%) | Year 2 (%) | Year 3 (%) | Year 4 (%) | Year 5 (%) |
|---|---|---|---|---|---|
| AOM 400 | 0.74 | 0.90 | 1.04 | 1.19 | 1.33 |
| Paliperidone palmitate | 2.50 | 2.89 | 3.29 | 3.68 | 4.06 |
| Risperidone LAI | 0.57 | 0.45 | 0.32 | 0.20 | 0.08 |
| Cariprazine | 0.09 | 0.13 | 0.17 | 0.21 | 0.25 |
| Asenapine | 1.48 | 1.76 | 2.03 | 2.29 | 2.56 |
| BSC | 94.62 | 93.88 | 93.15 | 92.43 | 91.73 |
AOM: Aripiprazole once-monthly; BSC: Best standard of care; LAI: Long-acting injectable.
Results
Base-case results
Paliperidone palmitate and asenapine were predicted to increase market share during the time horizon of the study, as was AOM 400, although with a lower yearly incremental increase (0.15% for AOM 400 vs 0.39 and 0.27% for paliperidone palmitate and asenapine, respectively). Cariprazine had an estimated yearly incremental increase in market share of 0.04%, while risperidone LAI was the only drug that had an estimated reduction of market share, of 0.13% every year (Table 5).
The total BI of the shift in market shares of maintenance monotherapy treatments for BP-I was US$0.06 per member per month (PMPM) in Year 1, increasing to US$0.26 PMPM by Year 5. The BI specific to AOM 400 increased from US$0.02 in Year 1 to US$0.09 in Year 5, while increases in paliperidone palmitate ranged from US$0.05 to US$0.23, increases in asenapine from US$0.01 to US$0.05, and increases in cariprazine from US$0.00 to US$0.02, all PMPM. Corresponding decreases were noted in risperidone LAI (-US$0.01 to -US$0.6) and BSC (-US$0.01 to -US$0.06) (Figure 2).
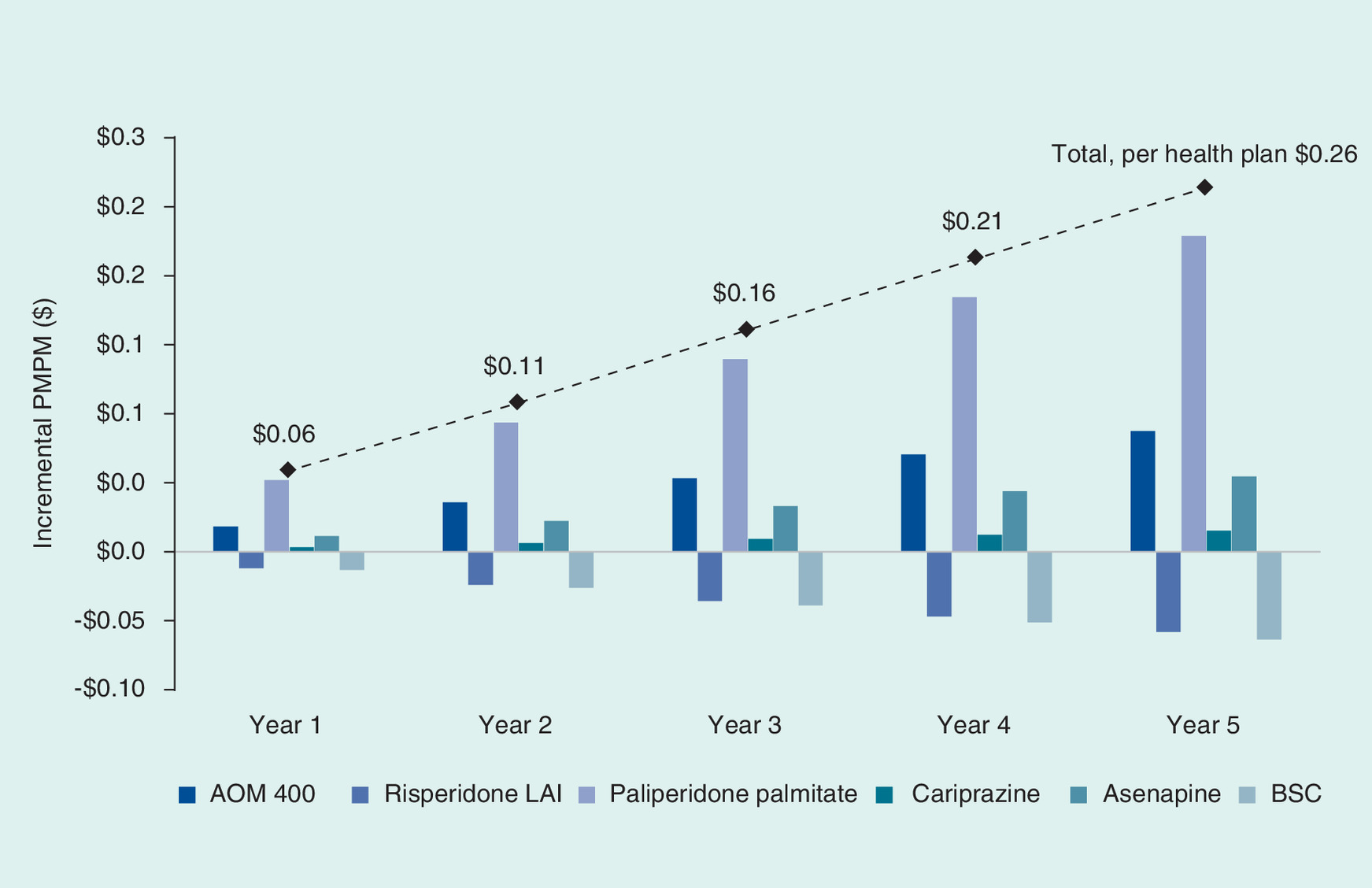
Figure 2. Incremental per member per month (PMPM) by treatment.
AOM: Aripiprazole once-monthly; BSC: Best standard of care; LAI: Long-acting injectable.
The total BI results, categorized by the type of cost, are shown in Table 7. Treatment-related costs were responsible for an increase in BI, while costs related to hospitalization and management of AEs generated cost savings.
| Type of cost | Year 1 (US$) | Year 2 (US$) | Year 3 (US$) | Year 4 (US$) | Year 5 (US$) | |
|---|---|---|---|---|---|---|
| Current scenario | Treatment-related | 5,011,837 | 4,729,693 | 4,729,693 | 4,729,693 | 4,729,693 |
| Adverse events | 233,881 | 233,881 | 233,881 | 233,881 | 233,881 | |
| Hospitalizations | 20,222,328 | 20,222,328 | 20,222,328 | 20,222,328 | 20,222,328 | |
| Total per health plan | 25,468,046 | 25,185,902 | 25,185,902 | 25,185,902 | 25,185,902 | |
| Total per member | 25.47 | 25.19 | 25.19 | 25.19 | 25.19 | |
| Total per member per month | 2.12 | 2.10 | 2.10 | 2.10 | 2.10 | |
| Predicted scenario | Treatment-related | 5,766,873 | 6,122,388 | 6,802,536 | 7,472,216 | 8,131,668 |
| Adverse events | 233,032 | 232,196 | 231,374 | 230,563 | 229,766 | |
| Hospitalizations | 20,174,206 | 20,126,836 | 20,080,201 | 20,034,283 | 19,989,067 | |
| Total per health plan | 26,174,111 | 26,481,420 | 27,114,110 | 27,737,062 | 28,350,501 | |
| Total per member | 26.17 | 26.48 | 27.11 | 27.74 | 28.35 | |
| Total per member per month | 2.18 | 2.21 | 2.26 | 2.31 | 2.36 | |
| Budget impact | Treatment-related | 755,037 | 1,392,695 | 2,072,843 | 2,742,523 | 3,401,975 |
| Adverse events | -849 | -1685 | 2508 | -3318 | -4116 | |
| Hospitalizations | -48,122 | -95,492 | -142,127 | -188,045 | -233,261 | |
| Total per health plan | 706,065 | 1,295,518 | 1,928,208 | 2,551,160 | 3,164,599 | |
| Total per member | 0.71 | 1.30 | 1.93 | 2.55 | 3.16 | |
| Total per member per month | 0.06 | 0.11 | 0.16 | 0.21 | 0.26 |
Discussion
Long-acting injectable AOM 400 was recently approved for the maintenance monotherapy treatment of BP-I in adults in the USA, based on the results of a 52-week Phase III trial that demonstrated significant benefit for AOM 400 compared with placebo (NCT01567527) [12].
A BI analysis was performed from the US healthcare payer perspective to assess the impact of introducing AOM 400 as a maintenance monotherapy treatment of BP-I for a hypothetical health plan of 1,000,000 members. The analysis showed an increased uptake of AOM 400, paliperidone palmitate, asenapine and cariprazine as maintenance treatments for BP-I in the predicted scenario. With this predicted shift in market shares, the overall PMPM cost for all such treatments would increase from US$0.06 in Year 1 to US$0.26 in Year 5. Increases in paliperidone palmitate accounted for the majority of the overall PMPM increase, followed by AOM 400 and asenapine, with a smaller increase resulting from cariprazine. An increase in treatment-related costs in the predicted scenario was partially offset by reductions in hospitalization costs and costs related to management of AEs.
This is the first BI analysis of AOM 400 in BP-I and is one of the few BI studies published for any medication in BP-I in the US setting. This BI analysis has several limitations. We chose the branded agents that were approved and/or have a high market share to be included in the model. Paliperidone palmitate was included as a comparator even though it is not FDA approved for the treatment of BP; however, inclusion was warranted due to the high off-label use in this indication. The probability of any mood episode or relapse rate for AOM 400 and BSC was used as a proxy for hospitalization based on the AOM 400 Phase III study in maintenance monotherapy for BP-I, while probabilities for other agents were derived from a systematic literature review [12,23]. Further analysis would benefit from head-to-head trial data or observational data, which would inform the BP-I relapse rates. The adherence of patients to each intervention was not included in this analysis, due to the lack of adequate data. The hypothesized improvement of adherence with LAI treatments should be explored in future research. Because of the paucity of available data, it was also necessary to assume that all the patients with BP-I were eligible for maintenance treatment with the chosen comparators. We used the past change in rate as a predictor for the future change in rate. Since AOM 400 is already used in the market off-label, we were able to obtain that information readily. There is a limitation to this approach, as we may be underestimating the change in the market share of AOM 400 and overestimating the share of other off-label drugs. Market share data for paliperidone were based on off-label information and may not be reflective of real-world use. Similarly, market share data for cariprazine were based on limited evidence, as it was a more recent market entry. Only branded atypical antipsychotics were included in the model; unbranded agents for the treatment of BP-I were included in the BSC category and not broken out separately. Additional potential areas for further research include healthcare resource use in BP-I in the USA and consideration of the long-term effects of AEs beyond a 5-year-horizon.
In conclusion, this BI analysis predicted that utilizing AOM 400 as a maintenance monotherapy treatment of BP-I in adults would have a lower BI than paliperidone palmitate over a 5-year time horizon, and asenapine and cariprazine would also contribute to the overall estimated BI. Payers may wish to analyze their own data to assess which treatments are being utilized (both on- and off-label) for treatment of BP-I when making formulary decisions.
Bipolar I disorder (BP-I) is recognized to be the most severe bipolar subtype.
Aripiprazole once-monthly 400 mg/300 mg (AOM 400) is a depot formulation of aripiprazole recently approved as a maintenance monotherapy treatment of BP-I in adults.
This study estimated the budget impact of AOM 400 in the maintenance monotherapy treatment of BP-I in adults, relative to treatment comparators, from a US healthcare payer's perspective in a hypothetical cohort of insured 1,000,000 members over a 5-year-time horizon.
Budget impact analysis was used to assess the incremental impact of varying market shares of AOM 400, paliperidone palmitate, risperidone long-acting injectable, asenapine and cariprazine as a maintenance monotherapy treatment of BP-I in a current scenario, compared with a predicted scenario.
The net result is a per member per month cost of US$0.06 in Year 1 increasing to US$0.26 in Year 5.
Increases in paliperidone palmitate's market share accounted for the majority of the overall per member per month increase, followed by lower impact from AOM 400 and asenapine.
The increase in treatment-related costs was partially offset by reductions in hospitalization costs and costs related to adverse event management.
Acknowledgements
Prior presentation: poster presentation at the AMCP Nexus Meeting 2017, Dallas, Texas; 16–19 October 2017.
Financial & competing interests disclosure
This study was funded by Otsuka Pharmaceutical Development & Commercialization and Lundbeck. M Augusto is a full-time employee of PAREXEL International. M Greene, S Min Sweeney and H Waters are full-time employees of Otsuka Pharmaceutical Development & Commercialization, Inc. M Touya is a full-time employee of Lundbeck. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Editorial support for this manuscript was provided by Bill Wolvey of PAREXEL, which was funded by Otsuka Pharmaceutical Development & Commercialization and Lundbeck.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Health Disorders, DSM-5 (5th Edition). American Psychiatric Association, Arlington, VA, USA (2013).
2.
Geddes JR, Miklowitz DJ. Treatment of bipolar disorder. Lancet 381(9878), 1672–1682 (2013).
3.
Blanco C, Compton WM, Saha TD et al. Epidemiology of DSM-5 bipolar I disorder: results from the National Epidemiologic Survey on alcohol and related conditions – III. J. Psychiatr. Res. 84, 310–317 (2017).
4.
Merikangas KR, Jin R, He JP et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch. Gen. Psychiatry 68(3), 241–251 (2011).
5.
Cloutier M, Greene M, Guerin A, Touya M, Wu E. The economic burden of bipolar I disorder in the United States in 2015. J. Affect. Disord. 226, 45–51 (2017).
6.
Gianfrancesco FD, Sajatovic M, Rajagopalan K, Wang RH. Antipsychotic treatment adherence and associated mental health care use among individuals with bipolar disorder. Clin. Ther. 30(7), 1358–1374 (2008).
7.
Lage MJ, Hassan MK. The relationship between antipsychotic medication adherence and patient outcomes among individuals diagnosed with bipolar disorder: a retrospective study. Ann. Gen. Psychiatry 8, 7 (2009).
8.
Gigante AD, Lafer B, Yatham LN. Long-acting injectable antipsychotics for the maintenance treatment of bipolar disorder. CNS Drugs 26(5), 403–420 (2012).
9.
Samalin L, Nourry A, Charpeaud T, Llorca PM. What is the evidence for the use of second-generation antipsychotic long-acting injectables as maintenance treatment in bipolar disorder? Nord. J. Psychiatry 68(4), 227–235 (2014).
10.
US FDA. Abilify (Aripiprazole) tablets (2002). www.accessdata.fda.gov/drugsatfda_docs/nda/2002/21–436_Abilify.cfm.
11.
Keck PE Jr, Calabrese JR, Mcintyre RS et al. Aripiprazole monotherapy for maintenance therapy in bipolar I disorder: a 100-week, double-blind study versus placebo. J. Clin. Psychiatry 68(10), 1480–1491 (2007).
12.
Calabrese JR, Sanchez R, Jin N et al. Efficacy and safety of aripiprazole once-monthly in the maintenance treatment of bipolar I disorder: a double-blind, placebo-controlled, 52-week randomized withdrawal study. J. Clin. Psychiatry 78(3), 324–331 (2017).
13.
Abilify Maintena® (Aripiprazole). Prescribing information. Otsuka Pharmaceutical Co. Ltd, Tokyo, Japan (2017). www.otsuka-us.com/media/static/Abilify-M-PI.pdf.
14.
Augusto M, Greene M, Touya M et al. Cost–effectiveness of long-acting injectable aripiprazole once-monthly 400 mg in bipolar I disorder in the USA. J. Comp. Eff. Res. 7(7), 637–650 (2018).
15.
Merikangas KR, Akiskal HS, Angst J et al. Lifetime and 12-month prevalence of bipolar spectrum disorder in the National Comorbidity Survey replication. Arch. Gen. Psychiatry 64(5), 543–552 (2007).
16.
Truven Health Analytics. RED BOOK online® (2017). http://micromedex.com/products/product-suites/clinical-knowledge/redbook.
17.
Invega Sustenna® (Paliperidone Palmitate) extended-release injectable suspension. Prescribing information. Janssen Pharmaceuticals Inc., Titusville, NJ, USA (2009). www.invegatrinza.com/sites/www.invegatrinza.com/files/prescribing-information-invegasustenna.pdf?v=326.
18.
Risperdal Consta® (Risperidone) long-acting injection. Prescribing information. Janssen Pharmaceuticals Inc., Titusville, NJ, USA (2007). www.janssencns.com/shared/product/risperdalconsta/prescribing-information.pdf.
19.
Vraylar® (Cariprazine) capsules. Prescribing information. Allergan USA Inc., Irvine, CA, USA (2015). www.accessdata.fda.gov/drugsatfda_docs/label/2015/204370lbl.pdf.
20.
Saphris® (Asenapine) sublingual tablets. Prescribing information. Merck Sharp & Dohme B.V, NJ, USA (2009). www.accessdata.fda.gov/drugsatfda_docs/label/2015/022117s017s018s019lbl.pdf.
21.
Centers for Medicare and Medicaid Services. Physician fee schedule (2016). www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/index.html.
22.
Wolters Kluwer. Medi-Span electronic drug file (MED-File) (2018). www.wolterskluwercdi.com/drug-data/medi-span-electronic-drug-file/.
23.
Miura T, Noma H, Furukawa TA et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis. Lancet Psychiatry 1(5), 351–359 (2014).
24.
Agency for Healthcare Research and Quality. HCUP National Inpatient Sample (2012). www.hcup-us.ahrq.gov/nisoverview.jsp.
25.
Taylor D, Paton C, Kapur S. The Maudsley Prescribing Guidelines in Psychiatry (11th Edition). Wiley-Blackwell, Hoboken, NJ, USA (2012).
Information & Authors
Information
Published In
Copyright
© 2018 Otsuka Pharm. Dev. & Comm. & Lundbeck.
History
Received: 2 February 2018
Accepted: 28 March 2018
Published online: 25 April 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Budget impact analysis of long-acting injectable aripiprazole once-monthly 400 mg in bipolar I disorder in the USA. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0009
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Vassiki Sanogo, Reem Dhayan Saud Almutairi, Vakaramoko Diaby, Budget impact of lecanemab for medicare beneficiaries with early Alzheimer’s disease in the United States: a subgroup analysis, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2025.2507427, 25, 10, (1421-1426), (2025).
- Vakaramoko Diaby, Shubhram Pandey, Vassiki Sanogo, Reem Dhayan Almutairi, Yagyesh Kanoria, Soma S. Nag, Budget impact of aripiprazole once every 2 months long-acting injectable for adult patients with bipolar I disorder in the United States, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2025.31.1.60, 31, 1, (60-67), (2025).
- Vakaramoko Diaby, Shubhram Pandey, Vassiki Sanogo, Reem Dhayan Almutairi, Yagyesh Kanoria, Soma S. Nag, Budget impact of aripiprazole once every 2 months long-acting injectable for adult patients with schizophrenia in the United States, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2025.31.1.53, 31, 1, (53-59), (2025).
- Hilary Phelps, Dee Lin, Alex Keenan, Aditya Raju, Danmeng Huang, Chih-Yuan Cheng, Carmela Benson, Budget impact of introducing once-every-6-months paliperidone palmitate in US health care plans, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2023.29.3.303, 29, 3, (303-313), (2023).
- Jean-Michel Azorin, Nicolas Simon, Dopamine Receptor Partial Agonists for the Treatment of Bipolar Disorder, Drugs, 10.1007/s40265-019-01189-8, 79, 15, (1657-1677), (2019).