Comparative cost and clinical effectiveness of clostridial collagenase ointment for chronic dermal ulcers
Abstract
Chronic dermal ulcers affect approximately 2.4–4.5 million people in the USA and are associated with loss of function, decreased quality of life and significant economic burden. Debridement is a critical component of wound care involving removal of nonviable tissue from chronic wounds to stimulate the granulation and epithelialization process. Clostridial collagenase ointment has been used as a method of wound debridement for more than 50 years and is currently the only enzymatic debriding ointment with US FDA approval. This review discusses the results of recent real-world studies that build upon the evidence demonstrating the clinical effectiveness, cost–effectiveness and safety of clostridial collagenase ointment across wound types and care settings.
Background
Chronic dermal ulcers affect approximately 2.4–4.5 million people in the USA [1]. Predominantly affecting older individuals, the prevalence of chronic wounds is increasing with the aging of the population. The growing burden of treating chronic wounds is further exacerbated by increasing healthcare costs and an increase in the incidence of diabetes and obesity [2]. Chronic dermal ulcers (venous leg ulcers [VLUs], diabetic foot ulcers [DFUs] and pressure ulcers [PUs]) can lead to loss of function and productivity, anxiety and decreased quality of life [3]. Direct costs associated with chronic wounds and their care are estimated at more than US$33 billion annually in the USA [4–6]. A recent economic evaluation of Medicare beneficiaries revealed that approximately 14.5% of this population (8.2 million patients) were diagnosed in 2014 with at least one type of wound or wound-related infection, associated with a conservatively estimated cost of care of nearly US$32 billion [7]. These figures underestimate total costs as they do not account for the indirect costs associated with chronic wounds (e.g., loss of productivity, quality of life and absenteeism).
Debridement is a critical component of wound care involving removal of necrotic tissue, foreign debris, bacterial growth and callus from chronic wounds to stimulate the wound granulation, epithelialization and proliferation processes [8]. Methods of debridement include surgery (sharp debridement), enzymatic, autolytic, chemical (antiseptics, polysaccharide beads and pastes), biosurgical (maggots) and mechanical (hydrodebridement) [8]. These methods may be used individually or in combination to optimize the debridement process. The choice of debridement method is based on patient characteristics, wound type, potential for infection and available medical expertise and resources [9]. Sharp debridement removes necrotic tissue from the wound bed via use of scalpels, curettes, etc., and is considered the standard of care in many cases [1]. However, not all patients are surgical candidates, and utilization may be limited further by patients’ bleeding tendency and pain tolerance [10]. Autolytic debridement (AD), promoted by hydrogels or hydrocolloid dressings, relies on the body’s own enzymatic mechanisms to remove necrotic tissue [1,11]. As such, it is time consuming and associated with risk of infection [10]. Enzymatic debridement entails topical application of enzymes (collagenase) to digest and dissolve devitalized tissue in the wound.
Pharmacology of clostridial collagenase ointment
Clostridial collagenase ointment (CCO) is currently the only enzymatic debriding ointment that has US FDA approval and has been used as a method of wound debridement for more than 50 years [12]. Bacterial collagenase isolated from Clostridium histolyticum is a selective enzymatic agent that causes hydrolytic cleavage of collagen molecules, which are a major component of nonviable tissue in the wound bed [13]. CCO effectively and selectively removes detritus without harming healthy tissue, thus contributing to the formulation of granulation tissue and subsequent epithelialization of dermal ulcers [14].
A large body of experimental data suggests that, in addition to its debriding activity, CCO may actively promote healing by potentiating cellular migratory, proliferative and angiogenic responses to injury [13]. Further, CCO may decrease the excessive and prolonged inflammation associated with nonhealing wounds by downregulating inflammatory cytokines [15]. In vitro and in vivo studies suggest that these effects are mediated by biologically active matrix fragments or peptides liberated via specific cleavages made by CCO during the debridement process [13,15]. Unlike endogenous human collagenases, CCO cleaves collagen at multiple sites, thus facilitating the production of multiple bioactive peptides [16]. Galperin et al. demonstrated that in differentiated THP-1 monocytes, clostridial collagenase-digested collagens suppressed lipopolysaccharide-induced release of TNF-α and lL-6 [15]. Furthermore, in 17 patients with DFUs treated with CCO versus hydrogel, the level of analytes associated with resolution of inflammation increased while those associated with inflammation (TNF-α and IL-6) decreased [15].
Pharmacoepidemiology of CCO use
National wound registry data aggregated from electronic health records (EHRs) of hospital-based outpatient wound center patients revealed that between 13 and 20% of more than 28,000 DFUs, VLUs and PUs analyzed were treated with CCO [17–19]. The authors found that healthcare providers are using CCO in more severe, difficult-to-heal wounds; mean wound surface area was significantly larger in DFUs treated with CCO compared with wounds not treated with CCO (7.6 vs 5.4 cm2, respectively; p < 0.0001), and the majority of PU wounds treated with CCO were stages III and IV (60.1 and 29.6%, respectively). In addition, relative to the overall population among all wound types, patients treated with CCO had substantially longer days in service and their wounds were more likely to receive debridement of all methods.
Only a small number of systematic reviews of the medical literature on the safety and effectiveness of CCO have been published in recent years. A systematic review by Ramundo and Gray published in 2009 analyzed 12 retrospective and prospective studies of CCO for treatment of PUs, leg ulcers or burn wounds: 5 randomized controlled trials (RCTs) compared CCO versus placebo and 7 studies compared CCO with alternative active debridement methods (e.g., hydrogel, silver sulfadiazine and autolysis) [20]. The authors determined that CCO is a selective, effective method for debridement of PUs, leg ulcers and burn wounds that has been used safely in adult, geriatric and pediatric populations. A recently published (2017) systematic review and meta-analysis by Patry and Blanchette analyzed 22 RCTs evaluating enzymatic debridement with CCO in all types of wounds and ulcers across all care settings [21]. The authors qualitatively summarized outcomes of collagenase either for wound healing or wound debridement and supported its use for enzymatic debridement in PUs, DFUs and in conjunction with topical antibiotics for burns [21]. Meta-analysis (n = 10 studies) was performed for the risk of adverse events (primary outcomes were not meta-analyzed). An increased risk of adverse events was calculated in patients treated with collagenase compared with alternative therapies (relative risk: 1.79; 95% CI: 1.24–2.59; I2 = 0%; p = 0.002). It should be noted that several studies were excluded from this analysis as two references were based on a single RCT, another RCT compared adverse events between different posology of collagenase and several studies did not report adverse events. Adverse events related to collagenase were seen in 11 of 17 RCTs (10 had values and relationships to adverse events made by authors). Subgroup analysis for significant adverse events related to collagenase or the alternative treatment (cellulitis was the only one suspected upon initial analysis) yielded no statistically significant relationships [21]. An examination of the individual studies included in this adverse event analysis reported infrequent pruritus, rash, edema, erythema (one case in one study), burning sensation at wound site (similar frequency between groups in several studies), burn bed infection (in a single study, seven cases with collagenase vs one case in control group), herpes infection (one case in one study), mild bleeding (one case in one study) and cellulitis (several cases in several studies). However, the risk ratio of developing cellulitis was not found to be statistically significantly different between treatment groups on subgroup analysis by Patry et al. [21–30], and a high risk of bias was noted by the Cochrane risk of bias tool among the majority of RCTs included. The systematic review and meta-analysis contained information from some, but not all, of the more recent studies in the literature as it was limited to RCTs, excluding cohort (prospective or retrospective) studies.
Therefore, we performed a narrative review to discuss the results of more recent real-world studies that expand upon the RCT evidence base, to demonstrate the effectiveness and safety of CCO across wound types (VLU, PU, DFU, burns) and care settings (acute care, postacute care and long-term care) and illustrate the cost–effectiveness of CCO as a debridement option.
Discussion of clinical effectiveness
Several effectiveness studies and cost–effectiveness models reviewed here utilize real-world data from the US Wound Registry (USWR). These studies may be more generalizable to actual practice in hospital outpatient clinics compared with analyses based on RCTs, as the registry includes typical patients often excluded from RCTs [31,32]. As such, the USWR, which harnesses electronic healthcare data at point of care, offers ideal opportunities for comparative effectiveness research in wound care [31–33].
Effectiveness of CCO in debridement of PU
CCO has been studied for the treatment of PUs in several studies, both in the long-term care setting and in the outpatient setting, either as monotherapy versus AD with hydrogel or medicinal honey, or in combination with sharp debridement versus sharp debridement alone (Table 1) [12,34–37].
| Study (year) | Patient population | Study design | Setting | Adjunct to SD | Comparator | End points | Results | Ref. |
|---|---|---|---|---|---|---|---|---|
| Gilligan et al. (2017) | PU (stages II, III and IV) | Retrospective review based on USWR | Hospital outpatient | Not necessarily; SD was permitted but not required by protocol | AD with honey | 100% granulation and epithelialization at 1 year | CCO users had significantly fewer total visits (9.1 vs 12.6; p < 0.001), fewer total selective sharp debridement sessions (2.7 vs 4.4; p < 0.001) and fewer PUs receiving NPWT (29 vs 38%; p = 0.002) versus treatment with honey; CCO-treated PUs achieved faster rates of 100% granulation (255 vs 282 days; p < 0.001) and subsequent epithelialization (288 vs 308 days; p = 0.011) versus PUs treated with medicinal honey CCO-treated PUs were 38% more likely to achieve 100% granulation versus honey-treated PUs at 1 year (p = 0.018) CCO-treated PUs were 47% (p = 0.024) more likely to epithelialize at 1 year compared with PUs treated with honey | [37] |
| Milne et al. (2010) | PU (stages III and IV) | Prospective, randomized, single-blind trial | Long-term care facility | No | Hydrogel | Complete necrotic tissue debridement at day 42 based on weekly photographs evaluated with digital planimetry software, changes in PUSH Tool score and WBS | Ability of CCO to debride nonviable tissue fully within 42 days was superior to hydrogel: 11/13 (85%) versus 4/14 (29%) patients randomized to each modality, respectively, achieved complete debridement Reduction of nonviable tissue was greater on a weekly basis with CCO versus hydrogel (p < 0.009) Overall wound size decreased faster with CCO versus hydrogel (p < 0.009) | [35] |
| Waycaster et al. (2014) | PU (stages III and IV) | Prospective randomized single-blind trial | Long-term care facility | No | Hydrogel | Changes in WBS, tissue granulation, wound surface area and epithelialization | CCO: 2% gain in granulation tissue/day Hydrogel: 1% gain in granulation tissue/day WBS improvements from baseline to week 6 CCO: +4.6 units; hydrogel: +2.6 units Change in wound size from baseline to week 6 CCO: 10.3–2.1 cm2; p = 0.009 Hydrogel: 6.5–3.0 cm2; NS | [36] |
| McCallon and Frilot (2015) | PU | Retrospective cohort study | Long-term acute care hospital | No; adjunct to NPWT | NPWT alone | BWAT | Statistically significantly (p < 0.05) greater speed of wound healing (reduction of BWAT score: -2.34) and reduction of necrotic tissue (reduction of BWAT items 5 and 6: -2.39) with CCO + NPWT versus NPWT alone | [38] |
| Milne et al. (2012) | PU (stages III and IV) | Prospective, continuation of Milne 2010 | Long-term care facilities | No; continuation of Milne 2010 study | Hydrogel | Maintenance debridement, wound closure with CCO compared versus hydrogel from time of necrotic tissue removal up to 84 days from enrollment Assessed by weekly photographs evaluated with digital planimetry software, PUSH Tool score and WBS | No significant difference between groups in days to healing or complete epithelialization. In aggregated Phase I and Phase II data, closure rates at the end of the study: CCO (69%) and hydrogel (21%; p = 0.0213). At time of complete debridement, 7 patients had stage III PUs (4 CCO; 3 hydrogel), 6 patients had stage IV PUs (6 CCO; 0 hydrogel). Greater severity of stage in CCO group (p = 0.03) | [34] |
| Carter et al. (2016) | PU (stage IV) | Retrospective cohort based on USWR | Hospital outpatient | Yes | SD without CCO | Percent of wounds closed; time to wound closure | The proportion of PU closed at 1 or 2 years: CCO versus control: 22.2% (75/337) versus 11.0% (37/336) at 1 year (p < 0.0001) and 26.7% (90/337) versus 13.7% (46/336) at 2 years (p < 0.0001), respectively. The mean time to wound closure within 2 years for stage IV CCO-treated PU was 456 days (95% CI: 415.9–496.0) versus 589 days (95% CI: 553.4–624.5; p < 0.0001). Kaplan–Meier analysis showed that time to wound closure at 1 year was significantly faster for PU treated with CCO versus PU not treated with CCO | [12] |
AD: Autolytic debridement; BWAT: Bates–Jensen Wound Assessment Tool; CCO: Clostridial collagenase ointment; NPWT: Negative-pressure wound therapy; NS: Not significant; PU: Pressure ulcer; PUSH: Pressure Ulcer Scale for Healing; SD: Selective debridement; USWR: United States Wound Registry; WBS: Wound bed score.
Milne et al. conducted a two-phase RCT on 27 patients with PUs residing in a long-term care facility, comparing CCO with AD plus hydrogel [34,35]. In the first phase of the study, which evaluated wound debridement for 6 weeks after randomization (based on Pressure Ulcer Scale for Healing Tool score and Wound Bed Score), CCO was superior to hydrogel in fully debriding nonviable tissue in 11 of 13 (85%) PUs versus 4 of 14 (29%) PUs in patients randomized to each treatment, respectively (p < 0.003). Of note, the mean wound size at baseline was significantly larger in the group treated with CCO (12.29 vs 7.90 cm2, respectively) [35].
The second phase of the study recruited only patients with wounds that were completely debrided in each group 6 weeks after randomization; these patients were followed until wound closure or to day 84 [34]. Patients continued to receive either CCO or hydrogel on a daily basis, even though no visible devitalized tissue was present in the wounds. All patients (n = 3) in the hydrogel group reached complete epithelialization with a mean of 32.6 days, and 9 of 10 patients in the CCO group reached complete epithelialization with a mean of 45 days (p = 0.121; one patient in each group was eliminated within the first week). In aggregating Phase I and Phase II data, the closure rates at the end of the study were superior for collagenase (69%) versus hydrogel (21%; p = 0.0213). The authors concluded that these findings add to the evidence base that facilitating maintenance debridement, either by collagenase or hydrogel, can be used to complete wound closure when utilized in conjunction with a validated predictive wound healing tool that closely monitors therapy.
In a more recent publication, Waycaster et al. [36] report additional details and outcomes assessed in Phase I of the above study that further support the potential of CCO to improve clinical outcomes in patients with PUs in a long-term care setting. Patients treated in Phase I with CCO had a granulation rate approximately twice that of those receiving hydrogel (average 2% gain in granulation tissue per day vs 1% per day, respectively), and showed a significantly greater percentage of granulation tissue formation at week 6 (p = 0.003). Similarly, Wound Bed Score values improved more rapidly among patients treated with CCO, and improvements from baseline to week 6 were greater in patients who received CCO than in those treated with hydrogel (+4.6 vs +2.6 units, respectively). Patients treated with CCO also showed significant reductions in wound surface area from baseline (10.3 cm2) to week 6 (2.1 cm2; p = 0.009), which were not observed in hydrogel-treated patients.
The effectiveness of CCO has also been demonstrated in the hospital outpatient department setting, utilizing real-world data from the USWR [12,37]. Using an EHR purpose-built for wound care documentation, data transmitted to the USWR between 2007 and 2013 yielded 202 patients (337 stage IV PU wounds) treated with CCO plus selective sharp debridement (CCO group) and 232 patients (336 stage IV PU wounds) treated with selective sharp debridement alone (non-CCO group) [12]. The proportion of wounds closed at any time was two times greater in the CCO group compared with the non-CCO group (22.2% [75/337] vs 11.0% [37/336] at 1 year; p < 0.0001 and 26.7% [90/337] vs 13.7% [46/336] at 2 years; p < 0.0001, respectively). Kaplan–Meier analysis showed that time to wound closure at 1 year was significantly faster for PU treated with CCO versus PU not treated with CCO (Figure 1).

Figure 1. Time to wound closure within 2 years (Kaplan–Meier plot).
The + markers indicate where censoring takes place timewise for each of the groups.
CCO: Clostridial collagenase ointment.
Reproduced with permission from [12] © John Wiley and Sons (2016).
Another analysis utilizing the USWR compared the effectiveness of enzymatic debridement with CCO versus AD with medicinal honey in patients with PU [37]. Among 517 CCO-treated PUs (446 patients) and 517 matched corresponding honey-treated PUs (341 patients), CCO-treated PU were 38% more likely to achieve 100% granulation versus honey-treated PU at 1 year (p = 0.018) and 47% (p = 0.024) more likely to epithelialize at 1 year compared with honey-treated PU (Figure 2). CCO users also had significantly fewer total visits (9.1 vs 12.6; p < 0.001), fewer total selective sharp debridements (2.7 vs 4.4; p < 0.001) and fewer PUs requiring negative-pressure wound therapy (NPWT; 29 vs 38%; p = 0.002) compared with medicinal honey users.

Figure 2. Achievement of key wound closure outcomes with clostridial collagenase ointment versus medicinal honey for treatment of pressure ulcers.
(A) Probability of 100% granulation over 365 days (Kaplan–Meier curve). (B) Probability of complete epithelialization over 365 days (Kaplan–Meier curve).
CCO: Clostridial collagenase ointment.
Reproduced with permission from [37] © Mary Ann Liebert, Inc. (2017).
CCO has also been assessed for PU management in the long-term acute care setting in conjunction with NPWT [38]. In a retrospective cohort study of patients (n = 114) in two long-term acute care hospitals, CCO in conjunction with NPWT demonstrated greater speed of wound healing and reduction of necrotic tissue compared with NPWT alone [38]. Of note, sharp debridement was performed in a subgroup of 41 patients. Analysis of this subgroup indicated that, compared with NPWT and sharp debridement alone, PUs treated with sharp debridement, NPWT and CCO demonstrated statistically significant increases in the rate of debridement (lower necrotic score on Bates−Jensen Wound Assessment Tool items 5 and 6) and the rate of healing (overall reduction in Bates−Jensen Wound Assessment Tool score), suggesting a possible synergistic effect between the use of sharp debridement and CCO for treating PU.
Effectiveness of CCO in debridement of DFU in outpatient settings
CCO has been examined for the treatment of DFUs in several studies in the outpatient setting, as monotherapy versus AD, monotherapy versus mechanical debridement (MD) plus selective sharp debridement or in combination with sharp debridement versus sharp debridement alone (Table 2) [15,39–41].
| Study (year) | Patient population | Study design | Setting | Adjunct to SD | Comparator | End points | Results | Ref. |
|---|---|---|---|---|---|---|---|---|
| Motley et al. (2014) | DFU | Prospective, randomized, open-label | Outpatient | Yes | SD without CCO | Percentage change in ulcer area from baseline at the end of the debridement/treatment period (EOT) | Wound area decreased relative to baseline for both the CCO group (-68%, -61%; p < 0.001 vs baseline) and the control group (-36%, -46%; p = NS vs baseline) at EOT and EOS, respectively. Intergroup differences did not reach statistical significance | [39] |
| Tallis et al. (2013) | DFU | Prospective, randomized, open-label | Physician office or hospital outpatient | No | SD and MD with saline gauze (after initial SD in both groups) | Condition of the wound bed at EOT; percentage of reduction in wound area and therapeutic response rates | Decrease from baseline in mean wound area: CCO: -44.9%, p = 0.016 at EOT, and -53.8%, p = 0.012 at EOS Results NS for control group CCO group exhibited a significantly better response rate at the end of follow-up versus the SMG group (0.92 vs 0.75 based on WAT modified from BWAT; p < 0.05) | [40] |
| Galperin et al. (2015) | DFU | Prospective, randomized, open-label | Outpatient | No | Hydrogel | 8-category assessment tool derived from BWAT; wound measurement via ARANTZ Silhouette® digital wound imaging system (Christchurch, New Zealand) | Significant and progressive reduction in mean percentage change from baseline in wound area for CCO for weeks 1 through 4 (-29, -55, -62 and -70%, respectively) Hydrogel: percent change from baseline was significant only at the end of week 1 (-33%) | [15] |
| Jimenez et al. (2017) | DFU | Prospective, randomized, open-label | Outpatient | No | Hydrogel† | Wound area measurement via ARANZ Silhouette digital wound imaging system; visual assessment of granulation | Wound area decreased relative to baseline for both the CCO group (-60%; p < 0.0001; -65%; p < 0.0001) and the control group (-50%; p = 0.0001; -51%; p = 0.0001) after 6 and 12 weeks, respectively. Intergroup differences at 6 and 12 weeks, NS mean percentage reductions for the CCO group were greater than those for the control at all 12 time points (averages: -55 and -41%, respectively) | [41] |
†SD permitted for both groups throughout treatment period at investigators’ discretion.
BWAT: Bates–Jensen Wound Assessment Tool; CCO: Clostridial collagenase ointment; DFU: Diabetic foot ulcer; EOS: End of study; EOT: End of treatment; MD: Mechanical debridement; NS: Not significant; SD: Selective debridement; SMG: Saline-moistened gauze; WAT: Wound Assessment Tool.
In a prospective, randomized, open-label trial by Motley et al. in patients with DFU, enzymatic debridement with CCO in conjunction with serial sharp debridement demonstrated benefit beyond serial sharp debridement with standard care alone [39]. Wound area was statistically significantly decreased from baseline at both end of treatment (6 weeks) and end of study (12 weeks) in the group receiving both CCO and sharp debridement (n = 28; -68 and -61%, respectively; p < 0.001 for both time periods), but not in those receiving only sharp debridement (n = 27; -36 and -46%, respectively). The intergroup difference did not reach statistical significance. On average, ulcers treated with serial sharp debridement plus adjunctive CCO decreased in size more rapidly than ulcers treated without adjunctive CCO debridement, with median time to closure for wounds that healed of 6 weeks for CCO and 8 weeks for control.
Similar CCO benefit was observed in another prospective, randomized, open-label trial comparing CCO monotherapy (n = 24) with a combined therapy of MD (saline-moistened gauze [SMG]) plus selective sharp debridement (n = 24). Only CCO treatment resulted in a statistically significant decrease from baseline in the mean wound area at the end of treatment (-44.9%; p = 0.0164) and at the end of follow-up (-53.8%; p = 0.012) [40]. Corresponding changes for the SMG group were +0.8 and +8.1%.
Jimenez et al. recently assessed outcomes associated with use of CCO in patients with diabetes and DFU in a prospective, randomized, open-label study of 215 patients [41]. All patients received sharp surgical debridement at baseline, then were randomized to receive CCO (n = 106) or standard care (hydrogel daily as needed to maintain wound moisture; n = 109). Sharp debridement was permitted for both treatment groups at the investigators’ discretion. Wound area decreased relative to baseline for both the CCO group (-60%; p < 0.0001 and -65%; p < 0.0001) and the control group (-50%; p = 0.0001 and -51%; p = 0.0001) after 6 and 12 weeks, respectively. While intergroup differences at 6 and 12 weeks did not reach statistical significance, mean percentage reductions in wound area were greater for the CCO group than the control group at all 12 time points (averages: -55 and -41%, respectively). Of note, DFUs that showed no improvement at 4 weeks (n = 24; 12/group) were crossed over to the other treatment group. A numerically greater proportion of subjects who switched to CCO achieved closure (33%) than did those who switched to standard care (8%).
Effectiveness of CCO in debridement of VLUs
Two retrospective cohort studies based on EHRs (2007–2013) of over 9000 patients with VLUs from the USWR demonstrated that VLUs treated with CCO were significantly more likely to improve (i.e., reduced wound surface area) relative to those treated with undifferentiated wound dressings alone (p < 0.05), and significantly more likely to achieve 100% granulation and to epithelialize by the end of therapy compared with wounds treated with medicinal honey (30 vs 19%, respectively, for granulation; p < 0.01 and 45 vs 31%, respectively, for epithelialization; p < 0.0001; Table 3 & Figure 3) [42,43].
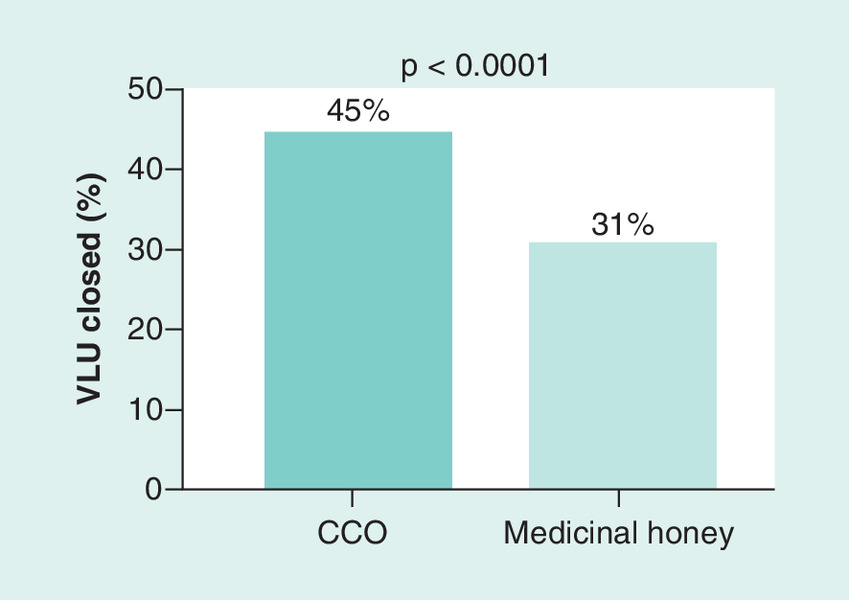
Figure 3. Percentage of venous leg ulcers documented as closed by end of treatment.
CCO: Clostridial collagenase ointment; VLU: Venous leg ulcer.
| Study (year) | Patient population | Study design | Setting | Adjunct to SD | Comparator | End points | Results | Ref. |
|---|---|---|---|---|---|---|---|---|
| Gilligan et al. (2015) | VLU | Retrospective review based on USWR | Hospital outpatient | No | AD with honey | Clinical improvement | Wound closure rates: CCO: 45%; medicinal honey: 31% | [42] |
| Gilligan et al. (2015) | VLU | Retrospective review based on USWR | Hospital outpatient | No | AD with undifferentiated wound dressings alone | Clinical improvement | CCO demonstrated greater clinical improvement than VLU treated with undifferentiated wound dressings (no specific results provided) | [43] |
AD: Autolytic debridement; CCO: Clostridial collagenase ointment; SD: Selective debridement; USWR: United States Wound Registry; VLU: Venous leg ulcer.
Effectiveness of CCO in debridement of burns
The effectiveness of CCO in burn treatment has been demonstrated in several studies compared with surgical excision, silver sulfadiazine or MD, in both the hospital and outpatient burn center (Table 4) [25,29,44–45]. Hansbrough et al. conducted a trial in 79 patients (age range: 5–60 years) with partial-thickness burn wounds in which paired wound sites of comparable size and severity in each patient were randomized to treatment with either CCO with polymyxin B sulfate/bacitracin powder or silver sulfadiazine. Comparison of paired treatment sites within each patient demonstrated that proportionally more CCO-treated sites were cleaned (p < 0.001) and healed (p < 0.001) before similar sites treated with silver sulfadiazine. Time to clean wound bed (mean: 9.3 vs 11.6 days) and time to epithelialization (mean: 19.0 vs 22.1 days) were both numerically faster in sites treated with CCO compared with those treated with silver sulfadiazine, but the difference did not reach statistical significance [25].
| Study (year) | Patient population | Study design | Setting | Adjunct to SD | Comparator | End points | Results | Ref. |
|---|---|---|---|---|---|---|---|---|
| Frye and Luterman (2005) | Burns | Retrospective review | Outpatient burn center | No | MD (WTD) | Hypertrophic scar formation | Saline WTD group: 46 (20.4%) patients developed significant scar postclosure of the wounds. CCO group: 19 (9.2%) patients; p < 0.001 | [44] |
| Hansbrough et al. (1995) | Burns | Prospective | Hospital | No | Silver sulfadiazine | Time to clean wound bed; time to epithelialization | Comparison of paired treatment sites within each patient: wound cleaned first in 47 versus 12% of CCO- and silver sulfadiazine-treated wounds, respectively (p < 0.001). Wound healed first in 42 versus 8% of CCO- and silver sulfadiazine-treated wounds, respectively (p < 0.001). Numerically faster time to clean wound bed (9.3 vs 11.6 days), and for CCO versus silver and faster epithelialization (19 vs 22.1 days) for CCO sites versus silver sulfadiazine sites | [25] |
| Ostlie et al. (2012) | Burns | Prospective, randomized in children | Hospital | No | Silver sulfadiazine | Primary outcome was the need for skin grafting | No difference in need for grafting | [29] |
| Ozcan et al. (2002) | Burns | Prospective, in children | Hospital | No | Surgical excision | Time to achieve a clean wound bed, requirement for blood transfusions, number of excisions per patient, number of patients necessitating tangential excision and/or grafting, wound infections and length of hospital stays | No significant difference in the time to achieve a clean wound bed; hospital stay shorter in CCO group (12.5 vs 20 days; p < 0.01) | [45] |
CCO: Clostridial collagenase ointment; MD: Mechanical debridement; SD: Selective debridement; WTD: Wet to dry.
Another prospective, randomized trial comparing CCO/polymyxin with silver sulfadiazine performed in 100 children with partial-thickness burns found no differences in outcomes in skin graft rates, length of stay and hospital costs between treatment groups [29]. The similarities in overall costs between treatment groups support the finding that the more significant charges of hospital room, treatment room times and operative interventions far outweigh the minimal difference in topical agent expense, so that agent choice should not be determined by agent cost [29].
In a prospective study in 119 children with partial-thickness burns, the use of CCO shortened the hospital stay and reduced the overall need for surgery and blood transfusions [45]. In 78 patients, treatment was initiated with CCO, and in 41 patients (Group S), burn wounds (of similar surface area and wound depth to those treated with CCO) were surgically excised. In 49 of the 78 patients treated with CCO, total removal of eschar was accomplished with CCO alone (this responsive group was Group D). Among the remaining 29 who had initiated treatment with CCO (Group DS), CCO was terminated because of burn wound infection (n = 17) or a manifest need for wound grafting (n = 12). There was no significant difference between the time to achieve a clean wound bed among the three treatment groups (mean: 7.8, 8 and 7 days for Groups D, DS and S, respectively; p > 0.05). Blood transfusion was required in only 1/49 (2%) patients in Group D, compared with 18/29 (62%) patients in Group DS and 30/41 (73%) patients in Group S (p < 0.01 for Group D vs either of the other groups). Mean hospital stay was shortest for Group D (mean 12.5 days; p < 0.01) compared with Group DS (20.7 days) and Group S (20.2 days). The results of these studies suggest that CCO should be considered as the initial treatment of choice for removal of eschar in patients with a partial-thickness burn wound without infection.
CCO for continuous debridement
As demonstrated in several studies discussed above [38,39], CCO is effective either alone or in conjunction with sharp debridement, providing synergistic effects when combined with the latter. An area of more limited study is the effectiveness of CCO in continuous debridement, which is a therapeutic intervention to address the problem of chronic wound beds with absent or slow healing despite appearing to be free from necrotic tissue [34,46]. The chronic wound contains a number of microbial, biochemical and cellular features and abnormalities that prevent or slow its progression to healing despite a seemingly adequate wound bed by appearance [46]. As noted earlier, CCO can potentiate cellular responses vital to wound epithelialization, such as proliferation and migration of keratinocytes and fibroblasts, while decreasing levels of analytes associated with inflammation [15]. As such, it may facilitate wound closure, as demonstrated in the trial by Milne et al. in which continuous debridement with CCO in institutionalized adults with PU resulted in superior wound closure rates from time of necrotic tissue removal to 84 days from enrollment [34].
Discussion of economic analyses
The cost–effectiveness of CCO has been studied for almost two decades. Several early models of debridement methods for treatment of chronic wounds deemed CCO to be the least expensive treatment among the treatment strategies that were compared (autolysis, calcium alginate, wet-to-dry dressings, hydrocolloid dressings and fibrinolysin) [47–49].
Cost–effectiveness of CCO in PU
Among models assessing PU patients, debridement with CCO is the economically dominant wound care strategy compared with other treatment strategies (Table 5). Carter et al. assessed the cost–effectiveness (from a US payer’s perspective; 2015 USD) of adding CCO to selective debridement compared with selective debridement alone (non-CCO) in the treatment of stage IV PU [50]. Outcome data were derived from retrospective deidentified EMRs of patients with stage IV PU from 2007 to 2013 using the USWR [12]. The analysis constructed a three-state Markov model over a 2-year time horizon [50]. Compared with the non-CCO group, CCO incurred lower costs (US$11,151 vs US$17,596) and greater clinical benefit (33.9 vs 16.8 ulcer-free weeks), resulting in an economically dominant treatment option (Figure 4). Over a 2-year period, an additional 17.2 ulcer-free weeks could be gained with a concurrent cost saving of US$6445 for each patient.
| Study (year) | Patient population | Study design | Setting | Adjunct to SD | Comparator | Costing year, currency | Time horizon | End points | Results† | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| Carter et al. (2016) | PU | CEA/Markov model | Hospital outpatient | Yes | SD without CCO | 2015, USD | 2 years | Cumulative costs, ulcer-free weeks, ICERs | ICER for CCO: -US$375 per ulcer | [50] |
| Dreyfus et al. (2017) | PU | Observational database healthcare utilization study | Hospital inpatient and outpatient | Not specified | Medicinal honey | 2015, USD | 6 months | Frequency of inpatient and outpatient revisits up to 6 months after index encounter for CCO versus medicinal honey treatment | Odds for inpatient re-admissions (OR: 1.16; 95% CI: 1.07–1.25) after inpatient index visits, and odds of outpatient re-encounters after inpatient (OR: 1.37; 95% CI: 1.26–1.48) and outpatient (OR: 1.28; 95% CI 1.05–1.57) index visit greats were greater for medicinal honey | [51] |
| Mearns et al. (2017) | PU | CEA/Markov model | Hospital outpatient | No | AD with medicinal honey | 2016, USD | 1 year | Cumulative costs, number of granulation and epithelialized weeks, number of clinic visits and debridements, QALWs, ICERs | CCO: 22.7 QALWs at a cost of US$6161 Medicinal honey: 21.9 QALWs at a cost of US$7149 | [52] |
| Motley et al. (2015) | DFU | CEA alongside an open-label RCT (NCT 01408277) | Outpatient | Yes; SSD + CCO | SSD + investigator-selected supportive care (silver dressings and hydrogels) | 2013, USD | 1 year | Number of epithelialized weeks, cost per DFU, cost per ulcer-free week | Cost per ulcer-free week: US$61 for CCO + SSD versus US$85 for control | [53] |
| Tallis et al. (2013) | DFU | CEA alongside an open-label RCT (NCT 01056198) | Physician office or hospital outpatient | No; surgical debridement + CCO | Surgical debridement + SMG | N/R, USD | 12 weeks | Cost per responder, wound bed condition, percentage of reduction in wound area and therapeutic response rates, tolerability | Direct mean cost per responder in a physician office was US$832 versus US$1042 for CCO versus SMG; in hospital outpatient setting, US$1607 versus US$1980 | [40] |
| Waycaster and Milne (2013) | PU | CEA | Long-term care facilities | No | Hydrogel | N/R, USD | 42 days | Number of granulated wound bed days, cost per patient, ICERs | 42-day results: ICER: CCO: + US$12/granulation day average CER: CCO: US$78/granulation day; hydrogel: US$249/granulation day 84-day results: average CER: CCO: US$6/closed-wound day; hydrogel: US$25/closed-wound day | [9,54] |
†See text for details of other results.
AD: Autolytic debridement; CCO: Clostridial collagenase ointment; CEA: Cost–effectiveness analysis; CER: Cost–effectiveness ratio; DFU: Diabetic foot ulcer; ICER: Incremental cost–effectiveness ratio; N/R, Not reported; OR: Odds ratio; PU: Pressure ulcer; QALW: Quality-adjusted life week; RCT: Randomized controlled trial; SD: Sharp debridement; SMG: Saline-moistened gauze; SSD: Serial sharp debridement; USD: United States dollar.

Figure 4. Cumulative costs with clostridial collagenase ointment added to selective debridement and selective debridement alone (non-clostridial collagenase ointment) over the 2-year period in patients with stage IV pressure ulcers.
Reproduced with permission from [50] © Taylor and Francis, Ltd (2017).
A similarly designed study by Mearns et al. assessed the cost–effectiveness of enzymatic debridement with CCO compared with autolytic treatment with medicinal honey for stage III or IV PU treatment [52]. A Markov model from a US payer perspective (2016 USD) was developed with a base-case of adult patients with PUs treated in a hospital outpatient department. The three health states in the model included inflammation/senescence, granulation/proliferation (patients achieving 100% granulation) and epithelialization, and were based on observed rates from an analysis of patients from the USWR [37]. CCO was the economically dominant strategy, resulting in 22.7 quality-adjusted life weeks at a cost of US$6161 over 1 year, compared with 21.9 quality-adjusted life weeks at a cost of US$7149 for medicinal honey.
Waycaster et al. analyzed the cost–effectiveness of CCO versus AD with a hydrogel dressing using clinical and resource utilization data derived from a US-based, prospective, randomized, two-phase trial [9,54]. Patients were residents of a long-term care center and had stages III and IV PUs with ≥85% necrotic nonviable tissue. In the analysis of Phase I (42-day end point), the average cost per patient for 42 days of PU care in 2012 was US$1817 for CCO and US$1611 for hydrogel, but days spent with a granulated wound were 3.6 times higher with CCO (23.4 vs 6.5) than hydrogel [54]. The incremental cost–effectiveness ratio was US$12, yielding an estimated cost per granulation day more than 3.2 times higher for hydrogel (US$249) versus CCO (US$78). At the end of Phase II of this study, direct cost per patient for PU care was US$2003 for CCO and $5480 for hydrogel, and the number of closed wound days was 1.5 times higher with CCO than hydrogel (317 vs 218 days) [9]. The estimated cost–effectiveness ratio was $6/closed-wound day for CCO and US$25/closed-wound day for hydrogel, indicating a fourfold higher cost per PU-free day for hydrogel versus CCO. These findings demonstrate economic dominance of CCO debridement over AD with hydrogel, which occurs when CCO is both clinically superior and cost effective.
Cost–effectiveness of CCO in DFU
Two cost analyses of CCO debridement in patients with DFU also yielded estimates favoring CCO over alternative debridement methods [40,53]. In an analysis of results from a randomized, open-label trial of 55 patients with DFU using a three-state Markov model, Motley et al. calculated that the number of epithelialized weeks was 25% greater in patients treated with the CCO plus serial sharp debridement (35 weeks) versus other debridement methods (28 weeks) [39,53]. Using a 1-year time horizon from a third-party payer perspective, the expected cost per treated DFU was greater for standard DFU care plus serial sharp debridement compared with CCO plus serial sharp debridement: 2376 versus US$2099, respectively (Figure 5). Cost per ulcer-free week was 40% higher for standard DFU care plus serial sharp debridement versus CCO plus serial sharp debridement (85 vs US$61 per closed-wound week).

Figure 5. Cumulative costs for clostridial collagenase ointment + serial sharp debridement and control (investigator-selected supportive care + serial sharp debridement) treatments.
CCO: Clostridial collagenase ointment; SSD: Serial sharp debridement.
Reproduced with permission from [53] © Elsevier (2015).
Tallis et al. [40] conducted an economic analysis alongside a multicenter, open-label, 12-week RCT of 48 patients with DFU treated with either CCO or SMG after baseline surgical debridement (with further surgical debridement as deemed necessary in either group). Resource use estimates included frequency of selective sharp debridement procedures between groups (mean of 1 and 7 for CCO and SMG groups during the trial, respectively) and physician office visits (6 and 12 during the trial, for CCO and SMG groups, respectively) associated with the evaluation and management of patients with DFU and CCO use. Response rates were categorized as follows: large response (ulcer area reduction from baseline ≥50%), moderate response (ulcer area reduction from baseline <50% but >10%) or stalled response (ulcer area reduction from baseline ≤10%, or increase in size). Direct mean cost per responder for CCO versus SMG was 832 versus US$1042 in the physician office setting and 1607 versus US$1980 in the hospital outpatient setting.
Health resource utilization of CCO
Recently, Dreyfus et al. analyzed the impact of CCO compared with medicinal honey on healthcare utilization among patients with PU in real-world inpatient and outpatient hospital settings [51]. Hospital discharge records (from 2000 to 2016) of patients receiving debridement with an International Classification of Diseases – ninth edition code for PU were extracted from the US Premier Healthcare Database, which contains data from more than 646 million patient encounters (∼1 in every 5 discharges in the nation). The frequency of inpatient and outpatient revisits up to 6 months after an index encounter for CCO-treated PU versus medicinal honey-treated PU was compared with multivariate analysis. Among inpatients, n = 44,725 (60% of discharges) were treated with CCO and n = 3542 (5%) with medicinal honey. Among outpatients, n = 1826 (7%) and n = 773 (3%), respectively, were treated with CCO and medicinal honey. In adjusted models, those treated with medicinal honey had greater odds for inpatient re-admissions (odds ratio [OR]: 1.16; 95% CI: 1.07–1.25) after inpatient index visits, and greater odds for outpatient re-encounters both after inpatient (OR: 1.37; 95% CI: 1.26–1.48) and outpatient (OR: 1.28; 95% CI: 1.05–1.57) index visits during 6 months of follow-up.
Conclusion
As demonstrated by the results of clinical trials and real-world data discussed above, CCO is effective for the debridement of all chronic wounds and burns, and across multiple care settings. Unlike other modalities of debridement, CCO debridement can be used in most patients and can be performed in any care setting, by any caregiver. As such, CCO is an ideal choice both for initial debridement (either alone or in conjunction with initial and/or serial sharp debridement) as well as for continuous debridement. These qualities make CCO suitable for use across the continuum of settings and transitions in wound care patients, from hospital to short-term care facility to home. In addition to its effectiveness when used as monotherapy for debridement, the addition of CCO to selective sharp debridement or to NPWT improves outcomes over either of those modalities used in isolation. All the economic studies of patients with PU and DFU have demonstrated the cost–effectiveness of CCO compared with other treatment strategies. Patients treated with CCO had fewer outpatient re-encounters, fewer clinic visits and debridements and faster rates of epithelialization, all of which translate into cost savings.
Future perspective
Currently, complete wound healing (i.e., skin re-epithelialization without drainage or dressing requirements) is the only FDA-approved ‘hard’ clinical trial end point to demonstrate efficacy for wound treatment products [55]. Consequently, there are no currently FDA-approved end points that might be more suitable for short-term outcomes, such as wound granulation percentage at 4 weeks after first or last CCO application. A group of wound care researchers is currently working with the FDA to approve new clinical-reported outcome and patient-reported outcome end points that may be more suitable end points for clinical trials involving CCO [56].
The USWR is a Qualified Clinical Data Registry (QCDR), a reporting mechanism by which providers participate in the Merit-Based Incentive Payment System. A QCDR is a US Centers for Medicaid and Medicare Services (CMS)-approved entity that collects medical and/or clinical data for the purpose of improving the quality of care furnished to patients. Quality data submitted to a QCDR must include patients across all payers and is not limited to Medicare beneficiaries. Importantly, QCDRs can develop quality measures relevant to a specialty or patient population as the USWR has done for wound care. Quality measures are an increasingly important part of many Medicare payment systems including those for acute care hospitals, long-term care, nursing homes and hospital-based outpatient departments [57]. Patients with chronic wounds are commonly treated in all of these settings; therefore, the near-absence of available wound care quality measures threatens both quality of patient care and reimbursement for wound care services. Among all of these settings, there is only one measure relevant to wound care and that is the counting and staging of pressure ulcers. The only other relevant wound care quality measures are those that practitioners can report through the QCDR. In 2014, the USWR developed a wound debridement quality measure for which it was able to establish a ‘benchmark rate’ in 2016 of 69.8%. Unfortunately, in 2017 this measure was rejected by CMS based on the argument that the high passing rate of the reporting physicians proved a ‘gap in practice’ that no longer existed with regard to debridement. It should be noted that among practitioners not reporting this measure to CMS the passing rate was low. In any case, physicians no longer have a debridement quality measure to inspire best practices in this aspect of wound care. Physicians could satisfy the measure using any method of debridement (e.g., sharp, autolytic, biologic, CCO, etc.) and could thus select the method most appropriate to the clinical situation. Many factors affect the use of CCO. For example, CCO is the only drug in its class, and it has an evidence base demonstrating cost–effectiveness and clinical effectiveness for the debridement of all chronic wounds and burns across multiple care settings. Yet, CCO is considered a tier 3 or tier 4 treatment in outpatient settings for purposes of reimbursement, creating a barrier to approval and reimbursement by payers for its use in wound care.
The European Wound Management Association has produced several documents providing guidance on how to improve evaluations of new treatment strategies regarding outcome measures in both RCTs and clinical studies that will meet the requirements for evidence-based information in wound management [58–60]. Hopefully, these guidance documents will contribute to the development of universal standards for outcome measures within the next 5 years and result in more comparative effectiveness studies that will be the basis for reimbursement of wound care therapies.
Background
The prevalence of chronic dermal ulcers is increasing in light of the aging of the population, and such wounds are associated with loss of function, decreased quality of life and significant direct and indirect costs.
Debridement is a critical component of wound care involving removal of nonviable tissue from chronic wounds to stimulate the wound granulation and epithelialization process.
Clostridial collagenase ointment (CCO) is currently the only enzymatic debriding ointment with US FDA approval.
Experimental data suggest that, in addition to its debriding activity, CCO may actively promote healing by potentiating cellular migratory, proliferative and angiogenic responses to injury. Further, CCO may decrease the excessive and prolonged inflammation associated with nonhealing wounds by downregulating inflammatory cytokines.
Discussion of clinical effectiveness
The effectiveness of CCO for debridement of diabetic foot ulcers, pressure ulcers and venous leg ulcers, as well as burns, has been demonstrated by a number of clinical trials across multiple care settings (i.e., hospital inpatient, outpatient and long-term care facility).
Several of the studies utilize real-world data from the US Wound Registry. These studies may be more generalizable to clinical practice compared with analyses based on controlled clinical trials, as the registry includes typical patients often excluded from randomized controlled trials and reflects actual practice.
CCO has demonstrated clinical effectiveness both alone and in conjunction with sharp debridement, providing synergistic effects when combined with the latter.
Discussion of economic evaluation/burden
Multiple analyses have demonstrated the cost–effectiveness and cost savings, and in some cases, economic dominance of CCO for the management of chronic wounds.
Comparator methods of debridement in these analyses included autolysis with medicinal honey or hydrogel dressing, moistened saline dressing and monotherapy with sharp debridement (compared with addition of CCO to sharp debridement).
Patients treated with CCO had fewer outpatient re-encounters, fewer clinic visits and debridements and spent more weeks in epithelialization, all of which translates into cost savings.
Conclusion
CCO is effective for the debridement of all chronic wounds and burns, and across multiple care settings, both as monotherapy and in conjunction with selective sharp debridement.
CCO has demonstrated cost–effectiveness, and in some cases, shown economic dominance compared with other strategies in the treatment and management of chronic wounds.
Financial & competing interests disclosure
C Waycaster is an employee of Smith & Nephew and may own shares of Smith & Nephew. MJ Carter is a consultant to Smith & Nephew. AM Gilligan is a consultant to Smith & Nephew. ES Mearns is a consultant to Smith & Nephew. CE Fife is a consultant to Smith & Nephew. CT Milne is on the speakers’ bureau for Smith & Nephew. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by Angela Cimmino, PharmD, Fishawack Communications, Conshohocken, PA, USA. This support was funded by Smith & Nephew, Fort Worth, TX, USA.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv. Wound Care (New Rochelle) 4(9), 560–582 (2015).
2.
Sen CK, Gordillo GM, Roy S et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 17(6), 763–771 (2009).
3.
Snyder RJ, Fife C, Moore Z. Components and quality measures of DIME (devitalized tissue, infection/inflammation, moisture balance, and edge preparation) in wound care. Adv. Skin Wound Care 29(5), 205–215 (2016).
• Summarizes the way in which the initial US Wound Registry measures capture aspects of the debridement/devitalized tissue, infection or inflammation, moisture balance and wound edge preparation/wound depth principles, which are poorly represented in the currently approved quality-based measures.
4.
Rice JB, Desai U, Cummings AK, Birnbaum HG, Skornicki M, Parsons N. Burden of venous leg ulcers in the United States. J. Med. Econ. 17(5), 347–356 (2014).
5.
Rice JB, Desai U, Cummings AK, Birnbaum HG, Skornicki M, Parsons NB. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care 37(3), 651–658 (2014).
6.
Russo CA, Steiner C, Spector W. Hospitalizations related to pressure ulcers. HCUP Statistical Brief #64. www.hcup-us.ahrq.gov/reports/statbriefs/sb64.pdf
7.
Nussbaum SR, Carter MJ, Fife CE et al. An economic evaluation of the impact, cost, and medicare policy implications of chronic nonhealing wounds. Value Health (2017) (In press).
8.
Debridement Procedures for Managing Diabetic Foot Ulcers: A Review of Clinical Effectiveness, Cost–Effectiveness, and Guidelines. Canadian Agency for Drugs and Technologies in Health, Ottawa, ON, Canada, (2014).
9.
Waycaster C, Milne CT. Clinical and economic benefit of enzymatic debridement of pressure ulcers compared with autolytic debridement with a hydrogel dressing. J. Med. Econ. 16(7), 976–986 (2013).
10.
Thomas A, Thayer W. Debridement of chronic wounds: a review of past & present treatment strategies. Today’s Wound Clinic 8(5), 1–7 (2014).
11.
Atkin L, Rippon M. Autolysis: mechanisms of action in the removal of devitalised tissue. Br. J. Nurs. 25(Suppl. 20), S40–S47 (2016).
12.
Carter MJ, Gilligan AM, Waycaster CR, Fife CE. Treating pressure ulcers with clostridial collagenase ointment: results from the US Wound Registry. Wound Repair Regen. 24(5), 904–912 (2016).
13.
Sheets AR, Demidova-Rice TN, Shi L, Ronfard V, Grover KV, Herman IM. Identification and characterization of novel matrix-derived bioactive peptides: a role for collagenase from Santyl® ointment in post-debridement wound healing? PLoS ONE 11(7), e0159598 (2016).
14.
Santyl®, package insert. Smith & Nephew, Inc. TX, USA (2014). www.santyl.com/content/pdf/SANTYL_PI.pdf
15.
Galperin RC, Lange DL, Ramsay SJ et al. Anti-inflammatory effects of clostridial collagenase results from in vitro and clinical studies. J. Am. Podiatr. Med. Assoc. 105(6), 509–519 (2015).
• A summary of results from in vitro and clinical studies which support a hypothesis that debridement with clostridial collagenase ointment is associated with decreased inflammation and greater progress toward healing.
16.
Eckhard U, Huesgen PF, Brandstetter H, Overall CM. Proteomic protease specificity profiling of clostridial collagenases reveals their intrinsic nature as dedicated degraders of collagen. J. Proteomics 100, 102–114 (2014).
17.
Gilligan AM, Waycaster C. Pharmacoepidemiology of costridial collagenase ointment for the treatment of diabetic foot ulcers in outpatient care settings. Presented at: ISPOR 20th Annual International Meeting, PA, USA, 16–20 May 2015.
18.
Gilligan AM, Waycaster C. Pharmacoepidemiology of clostridial collagenase ointment for the treatment of pressure ulcers in outpatient care settings. Presented at: ISPOR 20th Annual International Meeting, PA, USA, 16–20 May 2015.
19.
Gilligan AM, Waycaster C. Pharmacoepidemiology of clostridial collagenase ointment for the treatment of venous leg ulcers in outpatient care settings. Presented at: ISPOR 20th Annual International Meeting, PA, USA, 16–20 May 2015.
20.
Ramundo J, Gray M. Collagenase for enzymatic debridement: a systematic review. J. Wound Ostomy Continence Nurs. 36(Suppl. 6), S4–S11 (2009).
21.
Patry J, Blanchette V. Enzymatic debridement with collagenase in wounds and ulcers: a systematic review and meta-analysis. Int. Wound J. (2017) (Epub ahead of print).
•• A thorough systematic review of the literature on the effect of collagenase on all kinds of wounds, compared with an alternative therapy, on wound healing, wound bed characteristics, cost–effectiveness and the occurrence of adverse events.
22.
Alvarez O, Fernandez-Obregon A, Rogers R, Bergamo L, Masso J, Black M. A prospective, randomized, comparative study of collagenase and papain-urea for pressure ulcer debridement. Wounds 14(8), 293–301 (2002).
23.
Aldemir M, Kara IH, Erten G, Tacyildiz I. Effectiveness of collagenase in the treatment of sacrococcygeal pilonidal sinus disease. Surg. Today 33(2), 106–109 (2003).
24.
Burgos A, Gimenez J, Moreno E et al. Cost, efficacy, efficiency and tolerability of collagenase ointment versus hydrocolloid occlusive dressing in the treatment of pressure ulcers. A comparative, randomised, multicentre study. Clin. Drug Investig. 19, 357–365 (2000).
25.
Hansbrough JF, Achauer B, Dawson J et al. Wound healing in partial-thickness burn wounds treated with collagenase ointment versus silver sulfadiazine cream. J. Burn Care Rehabil. 16(3 Pt 1), 241–247 (1995).
26.
Boxer AM, Gottesman N, Bernstein H, Mandl I. Debridement of dermal ulcers and decubiti with collagenase. Geriatrics 24(7), 75–86 (1969).
27.
Soroff HS, Sasvary DH. Collagenase ointment and polymyxin B sulfate/bacitracin spray versus silver sulfadiazine cream in partial-thickness burns: a pilot study. J. Burn Care Rehabil. 15(1), 13–17 (1994).
28.
Varma AO, Bugatch E, German FM. Debridement of dermal ulcers with collagenase. Surg. Gynecol. Obstet. 136(2), 281–282 (1973).
29.
Ostlie DJ, Juang D, Aguayo P et al. Topical silver sulfadiazine vs collagenase ointment for the treatment of partial thickness burns in children: a prospective randomized trial. J. Pediatr. Surg. 47(6), 1204–1207 (2012).
30.
Lee LK, Ambrus JL. Collagenase therapy for decubitus ulcers. Geriatrics 30(5), 91–93, 97–98 (1975).
31.
Serena TE, Fife CE, Eckert KA, Yaakov RA, Carter MJ. A new approach to clinical research: integrating clinical care, quality reporting, and research using a wound care network-based learning healthcare system. Wound Repair Regen. (2017) (Epub ahead of print).
32.
Fife CE, Eckert KA. Harnessing electronic healthcare data for wound care research: standards for reporting observational registry data obtained directly from electronic health records. Wound Repair Regen. (2017) (Epub ahead of print).
33.
Fife CE, Carter MJ. Wound care outcomes and associated cost among patients treated in US outpatient wound centers: data from the US Wound Registry. Wounds 24(1), 10–17 (2012).
• Reports on use of the US Wound Registry to investigate clinical and cost outcomes of a broad population of patients undergoing treatment in 59 outpatient wound centers in 18 states.
34.
Milne CT, Ciccarelli A, Lassy M. A comparison of collagenase to hydrogel dressings in maintenance debridement and wound closure. Wounds 24(11), 317–322 (2012).
35.
Milne CT, Ciccarelli AO, Lassy M. A comparison of collagenase to hydrogel dressings in wound debridement. Wounds 22(11), 270–274 (2010).
36.
Waycaster C, Gilligan A, Milne C. Pressure ulcer treatment in a long-term care setting: wound bed healing with clostridial collagenase ointment versus hydrogel dressing. Chronic Wound Care Manage. Res. 1, 49–56 (2014).
37.
Gilligan AM, Waycaster CR, Bizier R, Chu B-C, Carter MJ, Fife CE. Comparative effectiveness of clostridial collagenase ointment to medicinal honey for treatment of pressure ulcers. Adv. Wound Care 6(4), 125–134 (2017).
38.
McCallon SK, Frilot C. A retrospective study of the effects of clostridial collagenase ointment and negative pressure wound therapy for the treatment of chronic pressure ulcers. Wounds 27(3), 44–53 (2015).
39.
Motley TA, Lange DL, Dickerson JE Jr, Slade HB. Clinical outcomes associated with serial sharp debridement of diabetic foot ulcers with and without clostridial collagenase ointment. Wounds 26(3), 57–64 (2014).
40.
Tallis A, Motley TA, Wunderlich RP et al. Clinical and economic assessment of diabetic foot ulcer debridement with collagenase: results of a randomized controlled study. Clin. Ther. 35(11), 1805–1820 (2013).
41.
Jimenez JC, Agnew PS, Mayer P et al. Enzymatic debridement of chronic nonischemic diabetic foot ulcers: results of a randomized, controlled trial. Wounds (2017) (Epub ahead of print).
• A randomized trial comparing clostridial collagenase ointment applied once daily with standard care consisting of a daily application of a hydrogel as needed to maintain a moist ulcer in 215 patients with diabetic foot ulcer.
42.
Gilligan AM, Carter MJ, Waycaster C, Fife CE. Comparative effectiveness of clostridial collagenase ointment to medicinal honey for treatment of venous leg ulcers in outpatient care settings. Presented at: 7th Annual Symposium on Advanced Wound Care (SAWC), NV, USA, 26–28 September 2015.
43.
Gilligan AM, Waycaster C, Carter MJ, Fife CE. Collagenase ointment for the treatment of venous leg ulcers in outpatient care settings. Presented at: ISPOR 20th Annual International Meeting, PA, USA, 16–20 May 2015.
44.
Frye K, Luterman A. Decreased incidence of hypertrophic burn scar formation with the use of collagenase, an enzymatic debriding agent. Wounds 17(12), 332–336 (2005).
45.
Ozcan C, Ergun O, Celik A, Corduk N, Ozok G. Enzymatic debridement of burn wound with collagenase in children with partial-thickness burns. Burns 28(8), 791–794 (2002).
46.
Falanga V, Brem H, Ennis WJ, Wolcott R, Gould LJ, Ayello EA. Maintenance debridement in the treatment of difficult-to-heal chronic wounds. Recommendations of an expert panel. Ostomy Wound Manage. (Suppl.), 2–13; quiz 14–15 (2008).
47.
Bergemann R, Lauterbach KW, Vanscheidt W, Neander KD, Engst R. Economic evaluation of the treatment of chronic wounds: hydroactive wound dressings in combination with enzymatic ointment versus gauze dressings in patients with pressure ulcer and venous leg ulcer in Germany. Pharmacoeconomics 16(4), 367–377 (1999).
48.
Mosher BA, Cuddigan J, Thomas DR, Boudreau DM. Outcomes of 4 methods of debridement using a decision analysis methodology. Adv. Wound Care 12(2), 81–88 (1999).
49.
Muller E, van Leen MW, Bergemann R. Economic evaluation of collagenase-containing ointment and hydrocolloid dressing in the treatment of pressure ulcers. Pharmacoeconomics 19(12), 1209–1216 (2001).
50.
Carter MJ, Gilligan AM, Waycaster CR, Schaum K, Fife CE. Cost effectiveness of adding clostridial collagenase ointment to selective debridement in individuals with stage IV pressure ulcers. J. Med. Econ. 20(3), 253–265 (2017).
• A three-state Markov model was developed to determine costs and outcomes between the clostridial collagenase ointment and noncollagenase ointment groups over a 2-year time horizon, with outcome data derived from a retrospective clinical study in patients with stage IV pressure ulcers.
51.
Dreyfus J, Delhougne G, James B, Gayle J, Waycaster C. Clostridial collagenase ointment and medicinal honey utilization for pressure injuries in US hospitals. Presented at: 9th Annual Symposium on Advanced Wound Care (SAWC), NV, USA, 20–22 October 2017.
52.
Mearns ES, Liang M, Limone B et al. Cost-effectiveness of clostridial collagenase ointment compared with medicinal honey for treatment of pressure ulcers. Clinicoecon. Outcomes Res. 9, 485–494 (2017).
53.
Motley TA, Gilligan AM, Lange DL, Waycaster CR, Dickerson JE Jr. Cost-effectiveness of clostridial collagenase ointment on wound closure in patients with diabetic foot ulcers: economic analysis of results from a multicenter, randomized, open-label trial. J. Foot Ankle Res. 8, 7 (2015).
54.
Waycaster C, Milne C. Economic and clinical benefit of collagenase ointment compared with a hydrogel dressing for pressure ulcer debridement in a long-term care setting. Wounds 25(6), 141–147 (2013).
55.
Food and Drug Administration (FDA). Guidance for Industry – Guidance for Chronic Cutaneous Ulcer and Burn Wounds – Developing Products for Treatment. (2006). www.fda.gov/downloads/drugs/guidances/ucm071324.pdf
56.
Driver VR, Gould LJ, Dotson P et al. Identification and content validation of wound therapy clinical endpoints relevant to clinical practice and patient values for FDA approval. Part 1. Survey of the wound care community. Wound Repair Regen. (2017) (Epub ahead of print).
57.
Fife CE, Walker D, Thomson B. Electronic health records, registries, and quality measures: What? Why? How? Adv. Wound Care (New Rochelle) 2(10), 598–604 (2013).
58.
Jeffcoate WJ, Bus SA, Game FL, Hinchliffe RJ, Price PE, Schaper NC. Reporting standards of studies and papers on the prevention and management of foot ulcers in diabetes: required details and markers of good quality. Lancet Diabetes Endocrinol. 4(9), 781–788 (2016).
59.
Gottrup F, Appelqvist J, Price P. Outcomes in controlled and comparative studies on non-healing wounds: recommendations to improve the quality of evidence in wound management. J. Wound Care 19(6), 239–268 (2010).
60.
Price P, Gottrup F, Abel M. Study recommendations for clinical investigations in leg ulcers and wound care. J. Wound Care 23(5), S1–S36 (2014).
Information & Authors
Information
Published In
Copyright
© Curtis Waycaster.
History
Received: 24 August 2017
Accepted: 29 September 2017
Published online: 27 October 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative cost and clinical effectiveness of clostridial collagenase ointment for chronic dermal ulcers. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0066
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Pengyu Gong, Fei Wang, Yixin Hua, Jie Ying, Jianxiang Chen, Yiting Qiao, Collagenase-mediated extracellular matrix targeting for enhanced drug penetration and therapeutic efficacy in nanoscale delivery systems for cancer therapy, Journal of Nanobiotechnology, 10.1186/s12951-025-03815-y, 23, 1, (2025).
- Manal Al-Kattan, Afra Baghdadi, Afnan Sahloli, Thermostable Collagenase Derived from Streptomyces scabies Demonstrates Selective Antibacterial Activity Against Infections in Diabetic Foot Ulcers, Applied Microbiology, 10.3390/applmicrobiol5040122, 5, 4, (122), (2025).
- Padakanti Sandeep Chary, Anuradha Urati, Samia Shaikh, Rati Yadav, Valmala Bhavana, Naveen Rajana, Neelesh Kumar Mehra, Nanotechnology-enabled approaches for combating diabetic foot ulcer, Journal of Drug Delivery Science and Technology, 10.1016/j.jddst.2024.106593, 105, (106593), (2025).
- Syeda Yamna Zia, Sofia Ahmed, Hafiza Sumaiyya Jamal, Mehvish Perveen, Muhammad Ali Sheraz, Zubair Anwar, Syed Abid Ali, Formulation development of highly stable collagenase-containing hydrogels for wound healing, Journal of Pharmaceutical Sciences, 10.1016/j.xphs.2025.01.009, 114, 2, (1264-1279), (2025).
- Fatma Çoruk, Sibel Kaymak, Hüseyin Ayhan, Nilufer Vural, Salih Mollahaliloğlu, An overview of leech saliva and cosmetic potential, Eurasian Journal of Biological and Chemical Sciences, 10.46239/ejbcs.1569164, 7, 2, (178-185), (2024).
- Changhui Zhou, Linlin Jiao, Xiaoping Qiao, Weiwei Zhang, Shuangfeng Chen, Chunling Yang, Min Meng, Combined treatment of umbilical cord Wharton’s jelly-derived mesenchymal stem cells and platelet-rich plasma for a surgical patient with hospital-acquired pressure ulcer: a case report and literature review, Frontiers in Bioengineering and Biotechnology, 10.3389/fbioe.2024.1424941, 12, (2024).
- Esmail M. El-Fakharany, Hamada El-Gendi, Ahmed K. Saleh, Mohamed H. El-Sayed, Adel I. Alalawy, Rasha Jame, Mahmoud A. Abdelaziz, Shareefa Ahmed Alshareef, Yousra A. El-Maradny, The use of proteins and peptides-based therapy in managing and preventing pathogenic viruses, International Journal of Biological Macromolecules, 10.1016/j.ijbiomac.2024.132254, 270, (132254), (2024).
- É. M. Nasibov, Z. K. Nikitina, Production and Properties of Aspergillus fumigatus Collagenolytic Proteinase, Pharmaceutical Chemistry Journal, 10.1007/s11094-023-02985-z, 57, 7, (1070-1074), (2023).
- Ju. O. Ivankova, B. B. Sysuev, S. B. Evseeva, The Quality Risk Assessment of Paralithodes Camtschaticus Collagenase Gel in the Process of Pharmaceutical Development, Drug development & registration, 10.33380/2305-2066-2023-12-3-66-71, 12, 3, (66-71), (2023).
- Muzammil Husain, Yogeeta O. Agrawal, Antimicrobial Remedies and Emerging Strategies for the Treatment of Diabetic Foot Ulcers, Current Diabetes Reviews, 10.2174/1573399818666220228161608, 19, 5, (2023).