Treatment of tardive dyskinesia with tetrabenazine or valbenazine: a systematic review
Abstract
Up to 30% of patients taking antipsychotics may develop tardive dyskinesia (TD). Recent evidence-based recommendations demonstrate an unmet need for effective TD management. This systematic review was designed to update the evidence for TD treatment, comparing two vesicular monoamine transporter 2 (VMAT2) inhibitors, tetrabenazine and valbenazine. Of 487 PubMed/Embase search results, 11 studies met the review criteria. Valbenazine efficacy was demonstrated in rigorously designed clinical trials that meet the guidelines for AAN Class I evidence. Due to differences in study designs and a lack of standardized and controlled trials with tetrabenazine, a formal meta-analysis comparing the agents was not possible. However, valbenazine appears to have fewer side effects and a more favorable once-daily dosing regimen for the treatment of TD.
First draft submitted: 15 August 2017; Accepted for publication: 14 September 2017; Published online: 2 October 2017
Tardive dyskinesia (TD) is an involuntary movement disorder induced by prolonged exposure to dopamine receptor blocking agents (DRBAs), including antipsychotics and antiemetics [1,2]. Research shows that the prescription of antipsychotics alone increased more than threefold over 10 years; conservative estimates thus indicate that approximately 5 million patients have been exposed to antipsychotics in the United States (US) [3]. Given that the estimated global mean prevalence of TD is 30% in studies of patients currently treated with a first-generation antipsychotic and 21% in those currently treated with a second-generation antipsychotic, this disorder remains a significant problem for psychiatric patients who may experience stigma, embarrassment, and impairment in social functioning (and sometimes physical functioning) as a consequence of developing TD [4]. While the prevalence of TD has been extensively studied, the associated healthcare burden is the subject of continuing investigation [3–5]. Previous studies have shown that the presence of TD in patients with schizophrenia may correlate with impaired cognition, poor response to treatment, greater risk of relapse, longer hospital stays, lower quality of life and functioning, a progressive course, and increased mortality [6].
Through the mechanism of blocking dopamine receptors, antipsychotics have proven to be highly effective and essential drugs for controlling psychotic symptoms in patients with conditions such as schizophrenia and bipolar disorder [7–10]. However, dopamine is also involved as a key neurotransmitter in other neural pathways, notably the motor circuit [7,11]. Blockade in the motor circuit may lead to upregulation and hypersensitivity of post-synaptic dopamine receptors, resulting in an increase of dopaminergic signaling and the emergence of abnormal movements associated with TD [10,12].
Vesicular monoamine transporters (VMATs) are presynaptic intracellular transmembrane proteins that have a critical role in the packaging, storage and release of dopamine and other monoamines [13]. Inhibition of VMAT2, which is the predominant isoform in the brain, interferes with dopamine uptake and storage in presynaptic vesicles, leaving dopamine to be metabolized by monoamine oxidase in the cytoplasm. The resulting decrease in dopamine concentrations available for release in the synapse [14] counteracts the heightened dopaminergic activity that follows prolonged dopamine receptor blockade, and thereby may diminish the hyperkinetic symptoms associated with TD. VMAT2 inhibitors have shown promise in the treatment of hyperkinetic movement disorders, with tetrabenazine (XENAZINE®) and deutetrabenazine (AUSTEDO™) approved in the USA for the treatment of Huntington's chorea, and more recently, valbenazine (INGREZZA®) and deutetrabenazine (AUSTEDO™) approved for treatment of TD [15–17].
Developed in the 1950s [18], tetrabenazine is currently approved for the treatment of moderate to severe TD in some countries, and has been used and studied off-label for TD in the USA [19,20]. Tetrabenazine undergoes rapid absorption and metabolism with a half-life of approximately 10 h [21], and requires multiple daily dosing [20]. As a consequence of this rapid metabolism, chorea has been shown to recur within 12–18 h after the last dose of tetrabenazine [20]. Tetrabenazine binds selectively to VMAT2, but it is the dihydrotetrabenazine (HTBZ) metabolites that have the main pharmacologic effects. However, some of these metabolites (i.e., different HTBZ stereoisomers) have affinity for other off-target receptors [22], possibly contributing to unwanted side effects that can be dose-limiting and possibly confound treatment efforts [20,23,24]. In addition, due to its tolerability and pharmacokinetic profile, use of tetrabenazine for Huntington's disease includes recommendations for CYP2D6 genotyping to screen for poor metabolizer status when exceeding doses of 50 mg/day [15].
Recognizing that TD was an important unmet medical need and that a proven TD treatment would be an important pharmacological development, the US FDA granted breakthrough status to valbenazine in 2015 and approval as a treatment for TD in 2017 [2,25]. Valbenazine is a novel and highly selective VMAT2 inhibitor that is rapidly absorbed but more slowly metabolized, with a half-life of approximately 20 h that supports once-daily dosing [22,26]. Valbenazine has two major metabolites: [+]-α-HTBZ (or R,R,R-HTBZ), which is formed by hydrolysis and is a common metabolite with tetrabenazine, and NBI-136110, which is formed by mono-oxidation. Studies have shown that these two metabolites have no affinity for other unintended targets [22]. This pharmacologic profile contributes to a lower potential for side effects and reduced concerns over pharmacokinetic drug interactions or the need to screen for CYP2D6 polymorphisms.
Due to the resurgence of interest in TD, a systematic review was conducted to consolidate available clinical outcomes from published trials for tetrabenazine, which is currently being used off-label, and valbenazine, which was recently approved, in the treatment of TD. To meet the needs of formulary review committees as well as clinicians, the original intent of this review was to provide a body of evidence to enable a direct comparison between tetrabenazine and valbenazine. The review was carried out with the intent of executing a meta-analysis of efficacy and safety data extracted from published clinical trials.
Methods
Search strategy
The PubMed and Embase databases were searched for English language publications in the date range of 1 January 1980–31 March 2017. Since reports have already been published that have reviewed earlier studies of TD with tetrabenazine [27], studies published prior to 1980 were excluded from analysis with the intention of minimizing historical bias and enhancing comparability in methodology with the more recent valbenazine trials. Search strings for each database were ‘valbenazine AND tardive dyskinesia’ and ‘tetrabenazine AND tardive dyskinesia’. Duplicate results from these four separate searches were removed.
Criteria for study selection
Studies were selected for inclusion if they were a randomized controlled trial, single-arm study, cohort study, case series (with more than or equal to ten TD cases) or retrospective chart review. Case reports with less than ten TD cases, meta-analyses, reviews, animal studies, modeling studies, pharmacokinetic studies, chromatography studies, child/pediatric studies, guidelines, articles and letters were excluded. Results from the literature searches (i.e., study titles and/or abstracts) were screened to remove irrelevant studies based on the exclusion criteria. Results of this screening process were then further assessed by evaluating full-text articles for eligibility.
Data extraction & analysis
Full-text versions of selected studies were assessed to determine study design, sample size, study sites (single, multiple), comparator(s), efficacy and safety outcomes. For studies that reported the treatment of several movement disorders, only efficacy results pertaining to TD were reviewed and summarized. Based on available information, safety results were reviewed and summarized for the overall study population (i.e., any movement disorder) or only for the TD population. A meta-analysis of treatment effects was originally planned. However, as reported below, differences in study design did not allow for any meaningful comparisons across studies. Therefore, only a descriptive review of the studies is provided.
Results
Search strategy results
The initial database searches yielded 487 results, 83 of which were duplicates and thus excluded from screening. Screening of titles and abstracts resulted in the exclusion of an additional 391 studies. A total of 13 studies met criteria for this systematic review upon screening and full-text articles were assessed for eligibility (Figure 1). Four studies were identified for valbenazine: one open-label extension to a Phase II study [28]; two randomized, double-blind, placebo-controlled trials [26,29]; and one double-blind extension to a Phase III study [30]. Eligibility assessment of these studies resulted in the exclusion of the open-label extension study [28]. Because this open-label study was only presented orally in a platform session at the 2016 American Academy of Neurology (AAN) Annual Meeting, information about the methods and results were limited. Nine studies were identified for tetrabenazine: one double-blind, crossover study [31]; and eight open-label studies, which included two case series [32,33], three long-term studies [34–36] and three retrospective chart reviews [37–39]. Full-text review resulted in the exclusion of one open-label case series [32] because only four of the 14 TD patients were treated with tetrabenazine.
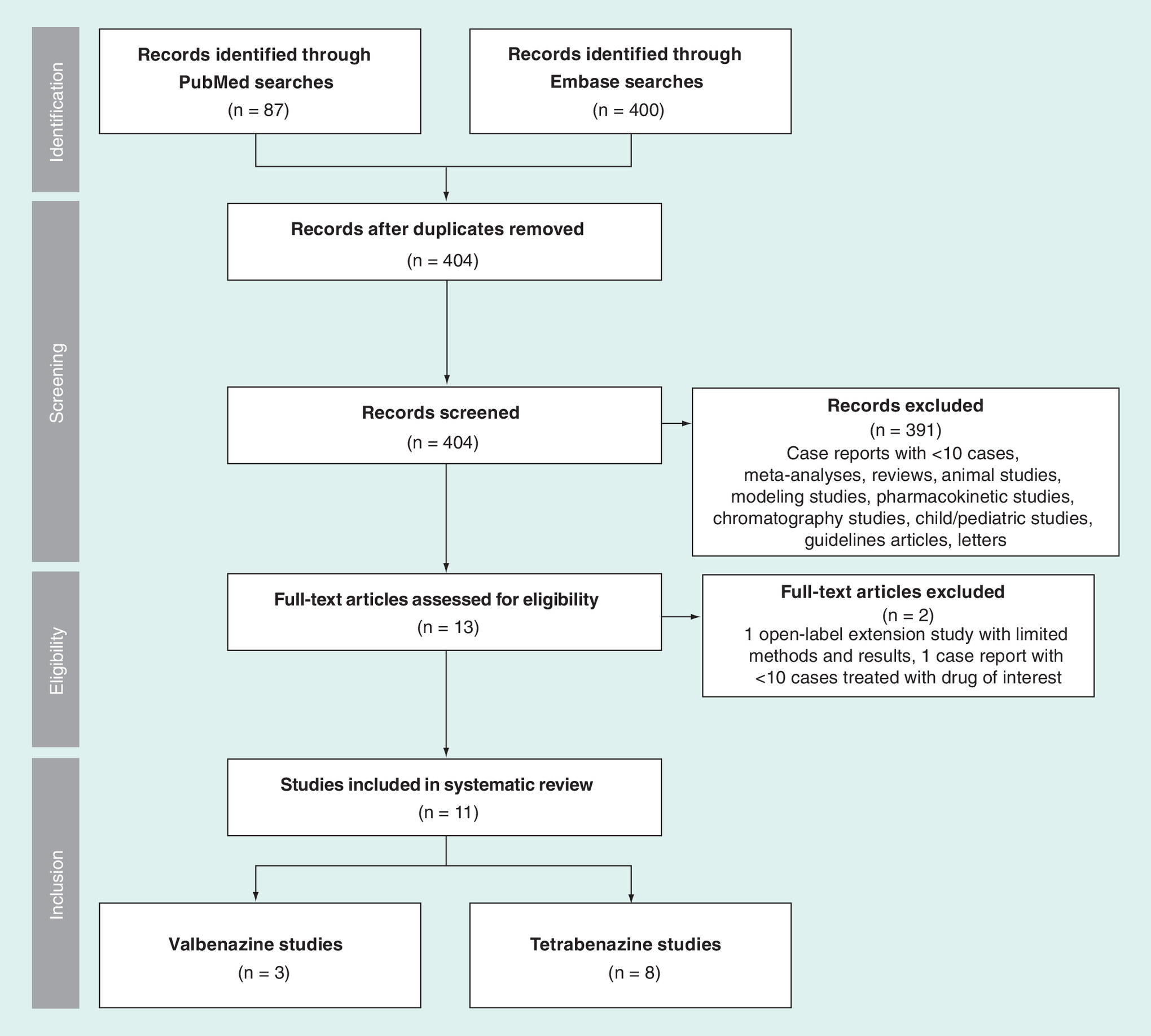
Figure 1. Results of systematic review.
Search terms: ‘valbenazine AND tardive dyskinesia’, ‘tetrabenazine AND tardive dyskinesia’. Search criteria: English language, date range 1 January 1980–31 March 2017.
A summary of the studies that met all inclusion criteria is presented in Table 1. Sample size, drug dose, duration of treatment and assessment tools varied greatly across studies. No head-to-head studies were available that compared the two interventions.
| Study (year) | Design | Duration† | Population‡ | Intervention§ | Comparator§ | Ref. |
|---|---|---|---|---|---|---|
| Valbenazine | ||||||
| O'Brien et al. (2015) KINECT 2 | Randomized, double-blind, placebo-controlled • Efficacy (AIMS) scored by two blinded video raters at baseline, weeks 2, 4 and 6 • Safety included adverse event monitoring | Treatment duration: up to 6 weeks | TD (n = 100) | Valbenazine QD 25–75 mg/day (n = 51) | Placebo (n = 49) | [29] |
| Hauser et al. (2017) KINECT 3 | Randomized, double-blind, parallel-group, placebo-controlled • Efficacy (AIMS) scored by two blinded video raters at baseline, weeks 2, 4 and 6 • Safety included adverse event monitoring | Treatment duration: up to 6 weeks | TD (n = 227) | Valbenazine QD 80 mg/day (n = 79) 40 mg/day (n = 72) | Placebo (n = 76) | [26] |
| Grigoriadis et al. (2016) KINECT 3 Extension | Double-blind extension of KINECT 3 • Effectiveness (AIMS) scored by two blinded video raters at weeks 8, 16, 32, 48 and 52 • Safety included adverse event monitoring | Treatment duration: up to 48 weeks plus 4-week washout | TD (n = 198) | Valbenazine QD 80 mg/day (n = 101) 40 mg/day (n = 97) | None | [30] |
| Tetrabenazine | ||||||
| Asher & Aminoff (1981) | Blinded crossover¶ • Efficacy (five-category rating) scored by two blinded video raters, week 3 (active) and week 6 (placebo) • Safety included side-effect monitoring | Treatment duration: 3–24 days (titration) plus 3 weeks (stable dose) plus 3 weeks (placebo crossover) | TD (n = 12) Total (n = 32) | Tetrabenazine BID 25–200 mg/day (n = 12) (mean dose: 175 mg/day) | Placebo (n = 12) (crossover) | [31] |
| Watson et al. (1988) | Open-label, case series • Efficacy (5-point scale) in patients successfully treated with tetrabenazine was scored by an unreported number of video raters at baseline and during treatment • Safety included side-effect monitoring | Treatment duration: NR; case series follow-up duration: up to 4 years | TD (n = 23) | Tetrabenazine QD or TID: 37.5–150 mg/day (n = 23) (mean dose: 91.3 mg/day) | None | [33] |
| Jankovic & Orman (1988) | Open-label, long-term • Efficacy (5-point scale)# scored by one video rater at baseline, 6 weeks, and every 3 months • Safety included side-effect monitoring | Treatment duration: 21.1 months†† | TD (n = 44) Total (n = 217) | Tetrabenazine: 25–100 mg/day (n = 44) (mean dose: 97.4 mg/day) | None | [34] |
| Jankovic & Beach (1997) | Open-label, long-term • Efficacy (5-point scale)# scored by one video rater at baseline, and every 3–6 months • Safety included side-effect monitoring | Mean treatment duration: 35.4 months | TD (n = 93) Total (n = 400) | Tetrabenazine: 25–200 mg/day (n = 93)‡‡ (mean maximum dose: 96.9 mg/day) | None | [35] |
| Ondo et al. (1999) | Open-label, long-term • Efficacy (AIMS) scored by one blinded video rater at baseline and ∼3 months • Safety included adverse event monitoring | Mean treatment duration: 20.3 weeks | TD (n = 20) | Tetrabenazine TID: 25–150 mg/day (n = 20) (mean dose: 57.9 mg/day) | None | [36] |
| Paleacu et al. (2004) | Open-label, retrospective chart review • Efficacy (CGIC) composite score of patient/caregiver • Safety included side-effect monitoring | Mean treatment duration, 22 months; chart review period: 4 years | TD (n = 17) Total (n = 118) | Tetrabenazine BID or TID: 12.5–150 mg/day (n = 17) (mean dose: 76.2 mg/day) | None | [37] |
| Kenney et al. (2007) | Open-label, retrospective chart review • Efficacy (5-point scale)# scored by chart review at baseline, and every 3–6 months • Outcomes noted upon withdrawal • Safety included adverse event monitoring | Mean treatment duration: 2.3 years; chart review period: 8 years | TD (n = 149) Total (n = 490) | Tetrabenazine: 12.5–300 mg/day (n = 149) (mean dose, 60.4 mg/day)§§ | None | [38] |
| Miguel et al. (2017) | Open-label, retrospective chart review • Efficacy (three-category rating) scored by chart review at baseline and during treatment • Outcomes noted upon withdrawal • Safety included side-effect monitoring | Mean treatment duration: 40 months; chart review period: 9 years | TD (n = 35) Total (n = 111) | Tetrabenazine: 6.25–225 mg/day (n = 35) (mean maximum daily dose: 37.5 mg/day) | None | [39] |
†Dosing frequency, mean dose and/or maximum dose are indicated as reported; some publications do not specify frequency or mean dose.
‡Some studies included patients with other movement disorders (e.g., dystonia, chorea, tic, myoclonus). For these studies a total population and TD population are reported.
§Intervention and comparator n-values are reported for TD patients only.
¶Patients were switched to placebo after 3 weeks of stable-dose tetrabenazine treatment; clinical significance of tetrabenazine treatment was based on TD severity being improved relative to both baseline and placebo treatment.
#These studies utilized the same 5-point scale to determine efficacy of treatment.
††Mean or median not specified.
‡‡May include many of the 44 patients from the earlier study, Jankovic & Orman (1988).
§§Mean dose of all patients in this study who had a hyperkinetic movement disorder.
AIMS: Abnormal Involuntary Movement Scale; BID: Twice daily; CGIC: Clinical Global Impression of Change; NR: Not reported; QD: Once daily; TD: Tardive dyskinesia; TID: Thrice daily.
Review of tetrabenazine studies
The tetrabenazine studies included one double-blind, crossover study (n = 12) and seven open-label studies (Total n = 381; range, n = 17–149). Tetrabenazine doses ranged from 6.25 to 300 mg/day (mean doses: 37.5–175 mg/day), administered one- to three-times daily. Tetrabenazine was generally well tolerated and effective in the treatment of TD. The most common side effects were parkinsonism, drowsiness/fatigue and depression, and authors of the studies generally agreed that tetrabenazine side effects were dose related and reversible.
Two open-label studies of tetrabenazine were conducted solely in TD patients. The most recent of these was a study by Ondo et al. [36] that included 20 patients with TD and used the Abnormal Involuntary Movement Scale (AIMS) as an outcome measure. In addition to TD, 45% of patients also showed mild evidence of parkinsonism, and 25% had akathisia at baseline. Participants were required to stop DRBA medications and other TD treatments for ≥30 days prior to starting tetrabenazine (mean dose: 57.9 mg/day; mean treatment duration: 20.3 weeks). Participants in this study were diagnosed with a psychiatric disorder or symptoms (unspecified psychosis, schizophrenia, bipolar disorder, agitation), gastrointestinal disorder or organic brain disorder. Cessation of antipsychotic medications is often not practical in patients with chronic psychotic disorders due to the risk of relapse, and it may have confounded treatment results due to unmasking or worsening of existing TD. TD severity was assessed by a single-blinded investigator who rated videos using the standardized AIMS, both at baseline and at approximately 3 months after commencing treatment. Significant improvement (p < 0.001) on the motor section of the AIMS was demonstrated at the end of treatment versus baseline values; no patient had unchanged or worsened TD (Table 2). The most common adverse events (≥10%) were sedation and parkinsonism (Table 3).
| Study (year) | Efficacy summary | Ref. |
|---|---|---|
| Valbenazine | ||
| O'Brien et al. (2015) KINECT 2† | AIMS score, LS mean change from baseline to week 6 (primary end point): -0.2 placebo, -2.6 valbenazine (p = 0.001) AIMS response at week 6 (≥50% improvement from baseline): 19% placebo, 49% valbenazine (p = 0.002) CGI-TD score, LS mean at week 6: 3.1 placebo, 2.2 valbenazine (p < 0.001) CGI-TD response at week 6 (‘much improved’ or ‘very much improved’): 16% placebo, 67% valbenazine (p < 0.001) | [29] |
| Hauser et al. (2017) KINECT 3† | AIMS score, LS mean change from baseline to week 6 (primary end point): -0.1 placebo, -3.2 valbenazine 80 mg (p < 0.001) AIMS score, LS mean change from baseline to week 6: -0.1 placebo, -1.9 valbenazine 40 mg (p = 0.002) CGI-TD score, LS mean at week 6: 3.2 placebo, 2.9 valbenazine 80 mg (ns), 2.8 valbenazine 40 mg (ns) AIMS response at week 6 (≥50% improvement from baseline): 9% placebo, 40% valbenazine 80 mg (p < 0.001), 24% valbenazine 40 mg (p = 0.02) | [26] |
| Grigoriadis et al. (2016) KINECT 3 Extension | AIMS score, mean change from baseline to week 48: -4.8 valbenazine 80 mg, -3.0 valbenazine 40 mg CGI-TD score, mean at week 48, 2.1 valbenazine 80 mg, 2.4 valbenazine 40 mg AIMS response at week 48 (≥50% improvement from baseline): 52% valbenazine 80 mg, 28% valbenazine 40 mg CGI-TD response at week 48 (‘much improved’ or ‘very much improved’): 76% valbenazine 80 mg, 59% valbenazine 40 mg After treatment washout (week 52), increases in AIMS and CGI-TD response rates indicated that TD severity was reverting toward baseline levels | [30] |
| Tetrabenazine ‡ | ||
| Asher & Aminoff (1981) | Improvement scale with five possible categories: marked, moderate, slight, none, worse Marked or moderate improvement with tetrabenazine: 60% of ten patients who completed the study No change with tetrabenazine: 40% of ten patients (two discontinued and were not included in these analyses) | [31] |
| Watson et al. (1988) | 5-point severity scale: score range, 0 (none) to 4 (severe) Score of 3 or 4 (moderate/severe) at baseline: 83% of 23 patients Score of 1 or 2 (none/minimal) after tetrabenazine: 87% of 23 patients | [33] |
| Jankovic & Orman (1988) | 5-point global response scale: score range, 1 (marked reduction in abnormal movements and excellent improvement in function) to 5 (worsening in movement disorder and some deterioration in function) Mean score after tetrabenazine: 2.3 in 44 patients Score of 1 or 2 (marked/moderate improvement): 71% of 44 patients | [34] |
| Jankovic & Beach (1997) | 5-point global response scale: score range, 1 (marked reduction in abnormal movements and excellent improvement in function) to 5 (worsening in movement disorder and some deterioration in function) Score of 1 (marked improvement) after tetrabenazine: 89% of 93 patients Score of 2 (moderate improvement) after tetrabenazine: 4% of 93 patients | [35] |
| Ondo et al. (1999) | AIMS total score: assessed by patients (self-rating) and video raters Mean percent improvement with tetrabenazine (self-raters): 60% improvement (from 9.1 to 3.6; p < 0.001) Mean percent improvement with tetrabenazine (video raters): 54% improvement (from 17.9 to 8.2; p < 0.001) | [36] |
| Paleacu et al. (2004) | 7-point CGIC score: range, -3 (marked worsening) to +3 (marked improvement) Score of 1 (mild improvement) after tetrabenazine: 18% of 17 patients Score of 2 (moderate improvement) after tetrabenazine: 35% of 17 patients Score of 3 (marked improvement) after tetrabenazine: 6% of 17 patients | [37] |
| Kenney et al. (2007) | 5-point global response scale: score range, 1 (marked reduction in abnormal movements and excellent improvement in function) to 5 (worsening in movement disorder and some deterioration in function) Score of 1 or 2 (marked/moderate improvement) after initiating tetrabenazine: 84% of 149 patients Score of 1 or 2 (marked/moderate improvement) after long-term tetrabenazine: 86% of 149 patients | [38] |
| Miguel et al. (2017) | 3-category response scale: 1 (improved and asymptomatic), 2 (improved but symptomatic), 3 (poor or no clinical response) Score of 1 or 2 (any improvement) after tetrabenazine: 77% of 35 patients | [39] |
†Significance in these studies is reported as compared with placebo.
‡All tetrabenazine studies except Watson et al. (1988) and Ondo et al. (1999) included patients with other hyperkinetic disorders; results are only presented for patients with tardive dyskinesia.
AIMS: Abnormal Involuntary Movement Scale; CGIC: Clinical Global Impression of Change; CGI-TD: Clinical Global Impression of Change-Tardive Dyskinesia; LS: Least square; ns: Not significant; PGIC: Patient Global Impression of Change.
| Study (year) | Safety summary | Ref. |
|---|---|---|
| Valbenazine | ||
| O'Brien et al. (2015) KINECT 2 | Discontinuation due to TEAEs: 10% placebo, 10% valbenazine Serious TEAEs: 4% placebo, 0% valbenazine Any TEAE: 33% placebo, 49% valbenazine Three most common TEAEs with valbenazine: fatigue (10 vs 4% placebo), headache (10 vs 4% placebo), decreased appetite (8 vs 0% placebo) | [29] |
| Hauser et al. (2017) KINECT 3 | Discontinuation due to TEAEs: 5% placebo, 6% valbenazine 40 mg, 6% valbenazine 80 mg Serious TEAEs: 4% placebo, 6% valbenazine 40 mg, 8% valbenazine 80 mg Any TEAE: 43% placebo, 40% valbenazine 40 mg, 51% valbenazine 80 mg Three most common TEAE with valbenazine (combined 40 and 80 mg): somnolence (5 vs 4% for placebo), akathisia (3 vs 1% for placebo), dry mouth (3 vs 1% for placebo) | [26] |
| Grigoriadis et al. (2016) KINECT 3 Extension† | Discontinuation due to TEAEs: 13% valbenazine 40 mg, 18% valbenazine 80 mg Serious TEAEs: 13% valbenazine 40 mg, 16% valbenazine 80 mg Any TEAE incidence: 62% valbenazine 40 mg, 76% valbenazine 80 mg Four most common TEAEs (combined 40 and 80 mg): headache (7%), urinary tract infection (7%), diarrhea (6%), dizziness (6%) | [30] |
| Tetrabenazine ‡ | ||
| Asher & Aminoff (1981) | Discontinued study due to side effects: 9% of 32 total patients treated with tetrabenazine Three most common side effects: 30% drowsiness, 12% drooling, 9% parkinsonism | [31] |
| Watson et al. (1988) | Two reported side effects in 23 TD patients treated with tetrabenazine: 9% drooling, 4% parkinsonism with tremor | [33] |
| Jankovic & Orman (1988) | Three most common side effects in 217 total patients treated with tetrabenazine: 24% parkinsonism, 13% drowsiness/fatigue, 11% depression | [34] |
| Jankovic & Beach (1997) | Discontinued study due to side effects: 23% of 400 total patients treated with tetrabenazine Three most common side effects: 37% drowsiness/fatigue, 29% parkinsonism, 15% depression Incidence of side effects may have been high because treatment strategy was to increase dose until evidence of efficacy or intolerability | [35] |
| Ondo et al. (1999) | Of 20 TD patients treated with tetrabenazine, 1 discontinued due to sedation Five patients reported mild sedation Five patients had evidence of mild parkinsonism (based on neurologic examination) | [36] |
| Paleacu et al. (2004) | Discontinued study due to side effects: 3.5% of 118 total patients treated with tetrabenazine; 12% of 17 TD patients (both TD patients discontinued for somnolence and weakness) Four most common side effects in 118 total patients: 6% somnolence/weakness/apathy, 5% parkinsonism, 2% depression, 2% akathisia | [37] |
| Kenney et al. (2007) | Discontinued study due to adverse events: 17% of 448 total patients Four most common adverse events: 25% drowsiness, 15% parkinsonism, 8% depression, 8% akathisia Age was found to be a significant predictor of parkinsonism (p < 0.0001) | [38] |
| Miguel et al. (2017) | Discontinuation due to adverse events: 16% of 108 total patients treated with tetrabenazine; 23% of 40 TD patients Reported adverse events in all patients: 27% parkinsonism, 13% psychiatric disorder, 2% other movement disorder (not specified), 10% other side effects (not specified) Reported adverse events in TD patients: 35% parkinsonism, 8% psychiatric disorder, 3% other movement disorder (akathisia), 8% other side effects (somnolence, rash, mental confusion) | [39] |
†Safety results not reported in Grigoriadis et al. (2016); results were provided by Neurocrine Biosciences, Inc. (data on file).
‡All tetrabenazine studies except Watson et al. (1988) and Ondo et al. (1999) included patients with other hyperkinetic disorders; based on availability, safety results are presented for all patients and/or TD patients as indicated. Descriptive terms (‘side effects’ or ‘adverse events’) are based on terminology used in the published study.
TD: Tardive dyskinesia; TEAE: Treatment-emergent adverse event.
The second study that included only TD patients was a case series by Watson et al. [33] that included 23 patients with TD who were treated with tetrabenazine (mean dose: 91.3 mg/day; mean treatment duration not reported). Severity of involuntary movements was evaluated in three regions (face/mouth/tongue, trunk, limbs) using a 5-point involuntary movement scale (0 = none, 1 = minimal, 2 = mild, 3 = moderate, 4 = severe) and video recordings made for each patient before and during treatment. All patients in this study showed improvement with tetrabenazine treatment (range: 1–4 points) (Table 2). Side effects were minimal (all ≤10%), and the most common events were drooling and parkinsonism with tremor (Table 3).
The remaining studies were conducted in patients with various movement disorders, including TD. Among them was a crossover study by Asher and Aminoff [31] that enrolled patients with a diagnosis of TD (n = 12), Huntington's disease or dystonia. The specific psychiatric diagnoses of participants were not reported, but stable doses of antipsychotics and other medication were allowed throughout. In TD patients, the tetrabenazine mean dose was 175 mg/day. Study participants were informed of the crossover design, but were not told whether they started with tetrabenazine or placebo (although all were started on tetrabenazine) and when the crossover occurred. Participants were videotaped at baseline, 3 weeks (end of tetrabenazine treatment) and 6 weeks (end of placebo crossover); videotapes were reviewed by two blinded investigators who rated TD severity as slight, moderate or marked. The study used a 5-category rating system (marked, moderate, slight, none, worse) to assess treatment response (Table 2). Clinical significance of tetrabenazine treatment was based on TD severity being improved relative to both baseline and placebo treatment. Six of 12 patients showed marked or moderate improvement (50%). Tetrabenazine did not produce behavioral changes in participants with TD, and alteration of concomitant antipsychotics was not needed. Across all participants, the most common side effects (≥10%) were drowsiness, drooling and parkinsonism (Table 3).
Three open-label studies, conducted at a single site, investigated the effects of long-term tetrabenazine treatment on patients with TD, dystonia, Huntington's disease, Tourette's syndrome, myoclonus, tics and other movement disorders. The use of concomitant medications and specific psychiatric disorders were not reported in these studies. Response to tetrabenazine was scored approximately every 3–6 months by a single examiner, using a 5-point Likert scale to rate abnormal movements (1 = marked improvement, 2 = moderate improvement, 3 = mild to moderate improvement, 4 = poor or no improvement, 5 = worsening). In the 1988 study [34], 44 patients with TD received tetrabenazine 25–100 mg/day, with a mean treatment duration of 21.1 months. The majority of patients showed moderate to marked improvement of TD (Table 2). In the 1997 study [35], which appears to have included patients from the 1988 study who were still receiving treatment, the mean maximum tetrabenazine dose in patients with TD (n = 93) was 96.9 mg/kg and the mean treatment duration was 35.4 months. The percentage of patients who had moderate to marked improvement in this study was similar to the earlier study (93 and 71%, respectively; Table 2). The 2007 retrospective chart review [38] did not include patients who commenced treatment prior to 1997, thus excluding patients from the previous reports. The mean dose was 60.4 mg/day and mean duration was 2.3 years (all movement disorder patients, n = 490). Response rates did not vary over time, with the majority of TD patients showing moderate to marked improvement both after initiating treatment, and after long-term treatment with tetrabenazine (Table 2). Adverse events that occurred in ≥10% of tetrabenazine-treated patients (all movement disorders) in these studies were parkinsonism, drowsiness/fatigue, depression, insomnia and nervousness/anxiety (Table 3). Up to 23% of patients discontinued tetrabenazine treatment due to adverse events.
The tetrabenazine studies also included retrospective chart reviews by Paleacu et al. [37] and Miguel et al. [39]. Both studies examined the effects of tetrabenazine on TD and other movement disorders in patients who did not respond to other medications. The use of concomitant medications and specific psychiatric diagnoses were not reported in either study. In the chart review by Paleacu et al. [37], mean treatment duration was 22 months and mean dose was 76.2 mg/day (all movement disorder patients, n = 188). Improvement of movement disorders was rated using a Clinical Global Impression of Change scale, with scores ranging from -3 (marked worsening) to +3 (marked improvement). Approximately 60% of patients included in this chart review showed any improvement (mild, moderate and marked) of TD (Table 2). Side effects included somnolence, weakness, apathy and parkinsonism, but none of the reported side effects occurred in >10% of all patients (Table 3). In the chart review by Miguel et al. [39], mean treatment duration was 40 months and mean maximum daily dose was 37.5 mg/day (TD patients, n = 35). Clinical response was based on comparison of baseline with follow-up visits using a 3-category rating system (improved and asymptomatic, improved but symptomatic, poor or no clinical response). Charts showed that the majority of patients with TD exhibited clinically meaningful improvement based on assessment of any improvement with treatment (Table 2). The most common adverse events (≥10%) were parkinsonism, depression, anxiety and worsening of pre-existing psychiatric disorder (Table 3).
In addition to examining the effects of tetrabenazine on TD and other movement disorders, Kenney et al. [38] and Miguel et al. [39] reported the effects of treatment cessation. Both studies showed that movement disorder severity reverted when tetrabenazine was interrupted for as little as 1 week or discontinued permanently.
Review of valbenazine studies
The valbenazine studies included: two randomized, double-blind, placebo-controlled trials, both with 6-week treatment duration; and one long-term, uncontrolled, extension trial with treatment of up to 48 weeks (Total n = 327). Valbenazine was administered once daily in all studies. In the Phase II study (KINECT 2; n = 100) [29], doses ranged from 25 to 75 mg/day and 76% of subjects reached maximum dose. In the Phase III study (KINECT 3; n = 227) [26] and its long-term extension (n = 198) [30], valbenazine-treated patients received 40 or 80 mg/day.
The valbenazine studies included adults with TD and stable schizophrenia/schizoaffective disorder or mood disorder. Stable regimens of concomitant medications for management of medical and psychiatric disorders were allowed. Changes in TD were assessed by consensus between two centralized video raters using standardized AIMS [40] assessments at baseline and at each study visit. Central AIMS video raters were blinded to treatment and to study visit.
Change in the AIMS total score (items 1–7) from baseline to week 6 was the primary end point for KINECT 2 and KINECT 3, and both studies showed significant improvement in ratings of severity of TD with valbenazine compared with placebo (p < 0.001; Table 2). Least squares mean differences between valbenazine and placebo were 2.4 in KINECT 2 and 3.1 (with the 80 mg/day dose) in KINECT 3. The long-term KINECT 3 extension study showed sustained improvement in the AIMS total scores through the end of valbenazine treatment (week 48), but TD reverted toward baseline levels of severity 4 weeks after treatment withdrawal at the end of the trial (week 52) (Table 2). The percentages of participants achieving a rigorous AIMS response threshold, defined as a ≥50% total score improvement from baseline, were significantly higher with valbenazine compared with placebo in both studies (KINECT 2, 49 vs 18%; KINECT 3, 40% [80 mg/day] and 24% [40 mg/day] vs 9%; all p < 0.05).
The Clinical Global Impression of Change-TD (CGI-TD) [40], which was scored by an onsite investigator who was blinded to treatment, indicated clinically meaningful but not statistically significant improvements with valbenazine compared with placebo in KINECT 3 (Table 2). In the KINECT 2 study, however, results for CGI-TD response, defined as a rating of ‘much improved’ or ‘very much improved’ (score ≤ 2), were significantly greater for valbenazine compared with placebo (p < 0.001), and significantly more patients showed a response with valbenazine (67 vs. 16%, p < 0.0001).
Similarly, in the KINECT 3 extension study, improvements in scores from baseline through week 48 were maintained in AIMS total and the CGI-TD scores (Table 2). The proportion of patients maintaining a response was sustained based on both the CGI-TD scores (76% [80 mg/day]; 59% [40 mg/day]) and ≥50% improvement in AIMS scores (52% [80 mg/day]; 28% [40 mg/day]).
Valbenazine was generally well tolerated, especially considering that most participants were taking a concomitant antipsychotic medication (KINECT 2, ≥40% of patients; KINECT 3, 86% of patients) [26,29]. The most common adverse events that were reported with valbenazine were fatigue, headache, somnolence and reduced appetite (all ≤10%) (Table 3). In the long-term extension study, headache and urinary tract infection (7% each) were the most common adverse events. Psychiatric status remained stable throughout valbenazine treatment and no other clinically relevant safety signals were observed.
Discussion
This review demonstrates that published studies of tetrabenazine and valbenazine in the treatment of TD were widely different in design, treatment duration, daily dosing/administration, allowance of concomitant psychiatric medications, methods for clinical evaluation, outcome measurements and patient characteristics including the presence or absence of underlying psychiatric disease. Because of these differences, conducting a direct comparison by means of a formal meta-analysis was not feasible; nor has any study been conducted that directly compares tetrabenazine with valbenazine in the treatment of TD or any hyperkinetic movement disorder. However, given the current resurgence of interest in VMAT2 inhibitors for the treatment of TD, a descriptive and comparative review of these studies is warranted.
Tetrabenazine is approved in the USA only for the treatment of chorea associated with Huntington's disease [15], but is commonly used off-label for TD. The tetrabenazine studies reported here demonstrated significant improvement in TD, although none of the studies included randomization or parallel-group placebo controls, and the studies varied widely in use of prospective versus retrospective designs, standardized outcome measures (e.g., AIMS), blinded conditions, videotaping and adequately powered sample sizes (only two studies included >50 patients with TD) [35,38]. Two long-term studies reported that TD severity reverted when tetrabenazine was discontinued, though this was noted through retrospective chart review and not investigated as part of the study design [38,39]. Tetrabenazine required dosing up to three-times daily, but was reported to be generally safe and well tolerated both short- and long term. The maximum daily dose for tetrabenazine as indicated for the treatment of Huntington's chorea was generally adhered to in all studies, except in Asher and Aminoff [31] where the recommended maximum daily dose was exceeded almost twofold. Nearly all studies with tetrabenazine documented changes in psychiatric status (depression) and secondary movement disorders (parkinsonism, akathisia) as frequent side effects of treatment. Adverse events were found to be dose related and reversible upon dose reduction. Limited information is available regarding the reasons for study discontinuation, but they include side effects, intolerability, lack of efficacy and travel/financial difficulties [35,38].
Valbenazine was recently approved in the USA for the treatment of adults with TD [17]. The randomized and controlled studies included in this systematic review demonstrated significant improvement in ratings of the severity of TD with valbenazine when compared with placebo [26,29]. In KINECT 3, the mean change from baseline in AIMS total score and AIMS ≥ 50% response indicated an effect with valbenazine after 2 weeks of treatment [26]. Preliminary results from the long-term study showed sustained improvement of TD, with decline toward baseline TD levels following treatment withdrawal [17,30], suggesting that ongoing treatment is required to maintain symptom reduction. Final reports for this study and additional long-term studies are pending (i.e., a 52-week open-label study [NCT02405091] and a 72-week rollover study [NCT02736955]). Valbenazine required only once-daily dosing, and was reported to be safe and well tolerated both short and long term. Importantly, psychiatric status was not altered by valbenazine and no safety signals were detected for secondary abnormal movements (i.e., parkinsonism, akathisia), even with the use of concomitant antipsychotic medications. The most common reasons for study discontinuation were withdrawal of consent, adverse events and loss to follow-up [26,35]. More research is needed to address some important questions about valbenazine and other VMAT2 inhibitors. Key topics include complete recovery or remission of TD symptoms, effects of valbenazine across different body regions (e.g., orofacial region versus limbs), and factors that may affect treatment response (e.g., demographics, TD severity and duration, DRBA type and duration of treatment).
The current systematic review highlights some of the key methodological differences between published clinical studies of tetrabenazine and valbenazine. As summarized in the evidence-based AAN guidelines for TD treatment, tetrabenazine studies present Class III and IV evidence, with a resultant Level C recommendation (possibly effective) [27]. Based on the trial design, it seems reasonable to expect that the valbenazine studies would constitute Class I evidence (i.e., randomized controlled trial in a representative population with clearly defined eligibility criteria, a clearly defined primary outcome, blinded treatment allocation and adequate sample size for drop-outs and statistical testing), which would be translatable to Level A evidence for treatment recommendation (i.e., established efficacy for the given condition/disorder in a specified population).
For this review, one aspect of the AAN Class I criteria that may warrant additional discussion is the requirement that the clinical trial be conducted in a representative population with presentation of relevant baseline characteristics. By clearly defining TD (based on prior DRBA exposure and AIMS assessment), including patients with a psychiatric diagnosis (i.e., schizophrenia, schizoaffective disorder, mood disorder), and allowing concomitant psychiatric medications including both first- and second-generation antipsychotics, the valbenazine trials were specifically designed to be reflective of real-world patients. In contrast, the tetrabenazine studies largely omitted any reporting of psychiatric status and concomitant medication use in their patient populations; moreover, many of the studies included patients with an array of abnormal movement disorders. In addition, the AIMS was used in all valbenazine trials to assess TD at baseline, and evaluate postbaseline improvements, whereas only one tetrabenazine study implemented this scale to evaluate efficacy [36]. The American Psychiatric Association has emphasized the importance of utilizing standardized scales for TD evaluation in clinical research [41] and the FDA currently requires that TD trials use the AIMS to demonstrate efficacy.
Differences in dosing and administration are another important clinical and formulary consideration. As reported in this systematic review, the tetrabenazine studies used doses ranging from 6.25 to 300 mg/day, administered up to three-times daily. In contrast, once-daily dosing of valbenazine may improve medication adherence, particularly in patients with psychiatric disorders [38,39]. There is no established dose of tetrabenazine specifically for TD, which may have contributed to the wide variance in tetrabenazine dosing regimens used in reported studies [42,43]. From a formulary perspective, unit dose costs can be estimated for valbenazine but not for tetrabenazine.
Finally, this review highlights some of the key differences between the two drugs in terms of side effects and patient safety. One important distinction is the association between tetrabenazine and secondary movement disorders such as parkinsonism and akathisia in patients with TD, which were negligible in the valbenazine studies. Other potential differences that have been identified by the FDA based on their review of clinical trial results with tetrabenazine in Huntington's disease versus valbenazine in TD, which may not be exactly comparable, can be found in the product labels (e.g., no black-box warning for suicidality/depression or any other warning/precautions for valbenazine) [15,17].
Limitations
As is often the case with systematic reviews [44], one of the main limitations of this analysis was the paucity of details available in some publications, especially the observational tetrabenazine studies. Moreover, as discussed earlier, the heterogeneity of the studies precluded the possibility of conducting a more formal meta-analysis. Therefore, only descriptive summaries could be provided and any interpretation of the results should be considered qualitative in nature. Although purposefully broad search terms were used to capture as many potential articles of interest within PubMed and Embase (i.e., the most frequently used literature databases in the USA), it is possible that this review did not include relevant publications that were only indexed in other databases. However, it seems reasonable to assume that the publications included in this review are adequately representative.
Conclusion
Studies of tetrabenazine and valbenazine for TD indicate that both VMAT2 inhibitors have published evidence of efficacy in the treatment of TD. However, the overall evidence for the efficacy of tetrabenazine is limited by the lack of randomized and placebo-controlled trials, differences across available studies (e.g., no standard dosing, differences in patient selection criteria), and no standardized outcome measures for assessing TD [41]. As would be expected with a recently approved medication, the clinical trials confirming the efficacy of valbenazine in the treatment of TD were larger, well controlled and more rigorously designed than the studies with tetrabenazine. Since the trial design and resultant data available for the two agents varied greatly, a meta-analysis and direct comparison were not possible. However, evidence from the clinical trials suggests that valbenazine is better tolerated and easier to administer, as predicted by the relative pharmacokinetics and off-target binding properties of the two drugs. Ongoing and future research on the effects of VMAT2 inhibitors on TD and other movement disorders is warranted.
Future perspective
Tetrabenazine has been used off-label to treat TD for decades, but valbenazine was recently approved for treatment of TD in adults. Evidence for the effectiveness of these drugs provides support for the mechanism of VMAT2 inhibition as a rational strategy for reducing the severity of TD movements. The approval of valbenazine in the context of the unmet need for treatment of TD, which interferes with social and occupational functioning for thousands of patients receiving antipsychotic therapy, is likely to transform clinical practice. No studies are yet available that directly compare the effects of valbenazine and tetrabenazine in patients with TD. Another VMAT2 inhibitor, deutetrabenazine, has been approved for the treatment of chorea in Huntington's disease, and more recently for TD, based on the results of two clinical trials (NCT02195700, NCT02291861) [45,46]. With publication of these controlled clinical studies for deutetrabenazine, a future meta-analysis of VMAT2 inhibitors specific for the treatment of TD may be possible.
Background
Tardive dyskinesia (TD) associated with chronic exposure to dopamine-receptor blocking drugs may have a significant effect on social and occupational functioning.
A systematic review was conducted to summarize clinical studies results for two vesicular monoamine transporter 2 inhibitors, tetrabenazine and valbenazine, with the intent to execute a meta-analysis.
Results
Systematic PubMed and Embase searches (January 1980–March 2017) yielded 487 results; 11 studies were included for review.
Treatment with once-daily valbenazine (three studies) indicated clinically meaningful and statistically significant improvements in TD severity relative to placebo. Valbenazine was safe and well tolerated, both in short- and long-term studies. The most common adverse events were fatigue, headache and somnolence.
Tetrabenazine (eight studies), which required dosing of one- to three-times daily, also significantly improved TD and was well tolerated. The most common adverse events were parkinsonism, drowsiness/fatigue and depression.
Conclusion
Results of this systematic review showed the valbenazine studies to be larger and more rigorously designed than the earlier tetrabenazine studies, providing robust evidence in support of the recent US FDA decision affirming valbenazine as the first approved treatment for TD.
Since the study designs and subjects were vastly different, a meta-analysis or other direct comparison of the two agents was not possible.
Financial & competing interests disclosure
This study was funded by Neurocrine Biosciences, Inc., San Diego, CA, USA. SN Caroff is a consultant to Neurocrine Biosciences Inc., and TEVA Pharmaceutical Industries, and received a research grant from Neurocrine Biosciences, Inc. S Aggarwal is an employee of NOVEL Health Strategies LLC. C Yonan is an employee of Neurocrine Biosciences, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing and editorial assistance was provided by Wendy van der Spuy of Prescott Medical Communications Group, Inc. (Chicago, IL, USA) with support from Neurocrine Biosciences, Inc.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Jankovic J. Dopamine depleters in the treatment of hyperkinetic movement disorders. Expert Opin. Pharmacother. 17(18), 2461–2470 (2016).
2.
Müller T. Valbenazine granted breakthrough drug status for treating tardive dyskinesia. Expert Opin. Invest. Drugs 24(6), 737–742 (2015).
3.
Cloud LJ, Zutshi D, Factor SA. Tardive dyskinesia: therapeutic options for an increasingly common disorder. Neurotherapeutics 11(1), 166–176 (2014).
4.
Carbon M, Hsieh CH, Kane JM, Correll CU. Tardive dyskinesia prevalence in the period of second-generation antipsychotic use: a meta-analysis. J. Clin. Psychiatry 78(3), e264–e278 (2017).
•• Meta-analysis of tardive dyskinesia (TD) prevalence in antipsychotic-treated patients.
5.
Yeomans K, Lenderking WR, Ross L, Shalhoub H, Yonan C. Real-world evaluation screening study and registry of dyskinesia in patients taking antipsychotic agents: the RE-KINECT study [poster PRM5]. Value Health 20(5), A311 (2017).
6.
Caroff SN, Davis VG, Miller DD et al. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J. Clin. Psychiatry 72(3), 295–303 (2011).
7.
Boyd KN, Mailman RB. Dopamine receptor signaling and current and future antipsychotic drugs. Handb. Exp. Pharmacol. (212), 53–86 (2012).
8.
Waln O, Jankovic J. An update on tardive dyskinesia: from phenomenology to treatment. Tremor Other Hyperkinet. Mov. (New York, NY) pii:tre-03-161-4138-1 (2013).
9.
Mehta SH, Morgan JC, Sethi KD. Drug-induced movement disorders. Neurol. Clin. 33(1), 153–174 (2015).
10.
Sethi KD. Movement disorders induced by dopamine blocking agents. Semin. Neurol. 21(1), 59–68 (2001).
11.
Witter DP, Holbert RC, Suryadevara U. Pharmacotherapy for the treatment of tardive dyskinesia in schizophrenia patients. Expert Opin. Pharmacother. 18(10), 965–972 (2017).
12.
Aosaki T, Miura M, Suzuki T, Nishimura K, Masuda M. Acetylcholine-dopamine balance hypothesis in the striatum: an update. Geriatr. Gerontol. Int. 10(Suppl. 1), S148–S157 (2010).
13.
Eiden LE. The vesicular neurotransmitter transporters: current perspectives and future prospects. FASEB J. 14(15), 2396–2400 (2000).
14.
Eiden LE, Weihe E. VMAT2: a dynamic regulator of brain monoaminergic neuronal function interacting with drugs of abuse. Ann. NY Acad. Sci. 1216, 86–98 (2011).
15.
Xenazine, prescribing information. Lundbeck, IL, USA (2015).
16.
Austedo, prescribing information. Teva Pharmaceuticals USA, Inc., PA, USA (2017).
17.
Ingrezza, prescribing information. Neurocrine Biosciences, Inc., CA, USA (2017).
18.
Paleacu D. Tetrabenazine in the treatment of Huntington's disease. Neuropsychiatr. Dis. Treat. 3(5), 545–551 (2007).
19.
Xenazine®25 mg. Summary of product characteristics. Lundbeck UK LLP, St. Albans, UK. www.lundbeck.com/upload/us/files/pdf/Products/Xenazine_SPC_GB_EN.pdf.
20.
Kaur N, Kumar P, Jamwal S, Deshmukh R, Gauttam V. Tetrabenazine: spotlight on drug review. Ann. Neurosci. 23(3), 176–185 (2016).
21.
Yero T, Rey JA. Tetrabenazine (xenazine), an FDA-approved treatment option for Huntington's disease-related chorea. P T 33(12), 690–694 (2008).
22.
Grigoriadis DE, Smith E, Hoare SR, Madan A, Bozigian H. Pharmacologic characterization of valbenazine (NBI-98854) and its metabolites. J. Pharmacol. Exp. Ther. 361(3), 454–461 (2017).
23.
Chen JJ, Ondo WG, Dashtipour K, Swope DM. Tetrabenazine for the treatment of hyperkinetic movement disorders: a review of the literature. Clin. Ther. 34(7), 1487–1504 (2012).
24.
Jankovic J, Clarence-Smith K. Tetrabenazine for the treatment of chorea and other hyperkinetic movement disorders. Expert Rev. Neurother. 11(11), 1509–1523 (2011).
25.
Davis MC, Miller BJ, Kalsi JK, Birkner T, Mathis MV. Efficient trial design – FDA approval of valbenazine for tardive dyskinesia. N. Engl. J. Med. 376(26), 2503–2506 (2017).
26.
Hauser RA, Factor SA, Marder SR et al. KINECT 3: a Phase 3 randomized, double-blind, placebo-controlled trial of valbenazine for tardive dyskinesia. Am. J. Psychiatry 174, 476–484 (2017).
•• Phase III trial of valbenazine in adults with TD.
27.
Bhidayasiri R, Fahn S, Weiner WJ, Gronseth GS, Sullivan KL, Zesiewicz TA. Evidence-based guideline: treatment of tardive syndromes: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 81(5), 463–469 (2013).
28.
Bari M, Shiwach R, Jimenez R, Siegert S, O'Brien C. Open-label extension of KINECT: a Phase II study of valbenazine (NBI-98854) for tardive dyskinesia. Neurology 86(16 Suppl.), S27 (2016).
29.
O'Brien CF, Jimenez R, Hauser RA et al. NBI-98854, a selective monoamine transport inhibitor for the treatment of tardive dyskinesia: a randomized, double-blind, placebo-controlled study. Mov. Disord. 30(12), 1681–1687 (2015).
• Phase II trial of valbenazine in adults with TD.
30.
Grigoriadis D, Comella C, Remington G, Jimenez R, Burke J, O'Brien C. Efficacy of valbenazine (NBI-98854) in subjects with tardive dyskinesia: results of a long-term extension study (KINECT 3 Extension) [poster M151]. Neuropsychopharmacology 41(Suppl. S1), S213 (2016).
•• Long-term study of valbenazine in adults with TD [full publication pending].
31.
Asher SW, Aminoff MJ. Tetrabenazine and movement disorders. Neurology 31(8), 1051–1054 (1981).
32.
Fahn S. Long-term treatment of tardive dyskinesia with presynaptically acting dopamine-depleting agents. Adv. Neurol. 37, 267–276 (1983).
33.
Watson MW, Skelton D, Jamali F. Treatment of tardive dyskinesia: preliminary report on use of tetrabenazine. Can. J. Psychiatry 33(1), 11–13 (1988).
34.
Jankovic J, Orman J. Tetrabenazine therapy of dystonia, chorea, tics, and other dyskinesias. Neurology 38(3), 391–394 (1988).
35.
Jankovic J, Beach J. Long-term effects of tetrabenazine in hyperkinetic movement disorders. Neurology 48(2), 358–362 (1997).
36.
Ondo WG, Hanna PA, Jankovic J. Tetrabenazine treatment for tardive dyskinesia: assessment by randomized videotape protocol. Am. J. Psychiatry 156(8), 1279–1281 (1999).
37.
Paleacu D, Giladi N, Moore O, Stern A, Honigman S, Badarny S. Tetrabenazine treatment in movement disorders. Clin. Neuropharmacol. 27(5), 230–233 (2004).
38.
Kenney C, Hunter C, Jankovic J. Long-term tolerability of tetrabenazine in the treatment of hyperkinetic movement disorders. Mov. Disord. 22(2), 193–197 (2007).
39.
Miguel R, Mendonca MD, Barbosa R et al. Tetrabenazine in treatment of hyperkinetic movement disorders: an observational study. Ther. Adv. Neurol. Disord. 10(2), 81–90 (2017).
40.
Guy W, National Institute of Mental Health, Psychopharmacology Research Branch, Early Clinical Drug Evaluation Program. ECDEU Assessment Manual for Psychopharmacology. US Dept. of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs, MD, USA (1976).
41.
The American Psychiatric Association Task Force on Tardive Dyskinesia. Tardive Dyskinesia: A Task Force Report Of The American Psychiatric Association. The Association (1992).
42.
Pfeiffer PN, Ganoczy D, Valenstein M. Dosing frequency and adherence to antipsychotic medications. Psychiatr. Serv. 59(10), 1207–1210 (2008).
43.
Medic G, Higashi K, Littlewood KJ, Diez T, Granstrom O, Kahn RS. Dosing frequency and adherence in chronic psychiatric disease: systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 9, 119–131 (2013).
44.
Bartolucci AA, Hillegass WB. Overview, strengths, and limitations of systematic reviews and meta-analyses. In: Evidence-Based Practice: Toward Optimizing Clinical Outcomes. Chiappelli F et al. (Eds). Springer Berlin Heidelberg Berlin, Heidelberg, Germany, 17–33 (2010).
45.
Fernandez HH, Factor SA, Hauser RA et al. Randomized controlled trial of deutetrabenazine for tardive dyskinesia: the ARM-TD study. Neurology 88(21), 2003–2010 (2017).
• Phase II/III trial of deutetrabenazine in adults with TD.
46.
Anderson KE, Stamler D, Davis MD et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, Phase III trial. Lancet Psychiatry 4(8), 595–604 (2017).
• Phase III trial of deutetrabenazine in adults with TD.
Information & Authors
Information
Published In
Copyright
© 2017 Saurabh Aggarwal.
History
Published online: 2 October 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Treatment of tardive dyskinesia with tetrabenazine or valbenazine: a systematic review. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0065
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Omar Ismail, Karam Albdour, Yazan Jaber, Kamel Jaber, Ameen Alsaras, Efficacy and safety of different pharmacological interventions in the treatment of tardive dyskinesia: a systematic review and network meta-analysis, European Journal of Clinical Pharmacology, 10.1007/s00228-026-04039-1, 82, 5, (2026).
- Lilian Ebner, Ariadne Kaylor, Angela Essa, Erica Greenberg, Jeremiah M. Scharf, Tricky “Ticcy” Case: Tics/Tourette Syndrome with Co-occurring OCD, Pediatric Neuropsychiatry, 10.1007/978-3-032-10099-3_3, (25-34), (2026).
- Roongroj Bhidayasiri, Jin Kiat Ang, Kok Yoon Chee, Roger Ho, Ahmad Shahir bin Mawardi, Adhi Wibowo Nurhidayat, Pongsatorn Paholpak, Pornjira Pariwatcharakul, Thitima Sanguanvichaikul, Eng Khean Ung, Natalia Dewi Wardani, Brian Yeo, Enriching Global Perspectives Through a Regional Lens: Recognition, Assessment, and Management of Tardive Dyskinesia in Southeast Asia, Journal of Movement Disorders, 10.14802/jmd.25146, 19, 1, (11-18), (2026).
- Fruzsina Maácz, Erika Gyöngyi Bán, Attila Brassai, Beáta Sperlágh, E. Sylvester Vizi, The role of the vesicular monoamine transporter 2 in the inhibitory effect of tetrabenazine and valbenazine compared to reserpine on the vesicular release of monoamine transmitters, Frontiers in Cellular Neuroscience, 10.3389/fncel.2025.1648613, 19, (2025).
- Fumiaki Yano, Yasunori Oda, Yuki Hirose, Fumiaki Yamasaki, Yusuke Nakata, Tomihisa Niitsu, Acute exacerbation of major depressive disorder following valbenazine treatment for tardive dyskinesia: A case report, Psychiatry and Clinical Neurosciences Reports, 10.1002/pcn5.70204, 4, 3, (2025).
- Nicholas Coyne, Emma Coyne, Michael Watcher, Ankit Chalia, Michael Ang-Rabanes, Raja Mogallapu, Remission of Aripiprazole-induced Tardive Dyskinesia with Valbenazine and Vitamin E Combination Therapy: A Case Report, American Journal of Psychiatry and Neuroscience, 10.11648/j.ajpn.20251303.11, 13, 3, (77-84), (2025).
- Liana S Rosenthal, Mena Farag, N Ahmad Aziz, Jee Bang, Vesicular monoamine transport inhibitors: current uses and future directions, The Lancet, 10.1016/S0140-6736(25)01072-4, 406, 10503, (650-664), (2025).
- Yaodong Xian, Jinxiu Hu, Xueying Yang, Yan Ding, Wei Li, Lanying Liu, A case of Jin's three-needle therapy for Tardive dyskinesia, Brain Behavior and Immunity Integrative, 10.1016/j.bbii.2025.100118, 10, (100118), (2025).
- Why the new definition of “anhedonia” misses the mark on dopamine function: Studies of effort-based aspects of motivation and selection of voluntary physical activity, The Handbook of Dopamine, 10.1016/B978-0-443-29867-7.00014-1, (345-356), (2025).
- Pál Tod, Anita Varga, Viktor Román, Balázs Lendvai, Roland Pálkovács, Beáta Sperlágh, E. Sylvester Vizi, Tetrabenazine, a vesicular monoamine transporter 2 inhibitor, inhibits vesicular storage capacity and release of monoamine transmitters in mouse brain tissue, British Journal of Pharmacology, 10.1111/bph.17348, 181, 24, (5094-5109), (2024).
- See more