Real-world adherence and economic outcomes associated with paliperidone palmitate versus oral atypical antipsychotics in schizophrenia patients with substance-related disorders using Medicaid benefits
Abstract
Aim: Compare medication utilization, costs and healthcare resource use in schizophrenia patients with substance-related disorders initiated on once-monthly paliperidone palmitate (PP1M) or an oral atypical antipsychotic (OAA). Materials & methods: Data from six Medicaid states (07/2009–03/2015) were used to compare outcomes between PP1M and OAA patients. Results: PP1M patients had higher 12-month antipsychotic adherence and persistence than OAA patients. PP1M patients had lower medical (mean monthly cost difference [MMCD] = US$-191, p = 0.020), higher pharmacy (MMCD = US$250, p < 0.001) and similar total costs (MMCD = US$59, p = 0.517) during the overall follow-up. PP1M patients had lower rates of outpatient visits and inpatient days but higher rates of mental health-related utilization. Conclusion: PP1M was associated with higher antipsychotic adherence and persistence, and similar total costs versus OAA.
First draft submitted: 14 June 2017; Accepted for publication: 25 July 2017; Published online: 15 August 2017
It is estimated that nearly half of patients with schizophrenia have co-occurring substance-related disorders (i.e., ‘dual diagnosis’) [1,2]. In one of the largest assessments to date, patients with psychotic disorders were found to be approximately four to five-times more likely to report smoking, heavy alcohol use, heavy cannabis use and recreational drug use compared with patients without a psychotic disorder [2]. Patients with schizophrenia often experience poor clinical outcomes, with a recent cohort study by Crump et al. demonstrating that patients with schizophrenia die 12–15 years earlier as compared with the general population [3]. Comorbid substance-related disorders have been shown to be powerful drivers of poorer clinical outcomes, including nonadherence to medication [4–6], disease relapse [7,8] and mortality [9] among patients with schizophrenia, making this a particularly vulnerable and challenging-to-treat subpopulation. The impacts of substance use on disease management, specifically on adherence and relapse, are complex and hypothesized to result from both the impacts of active substance use on cognition and judgment and from the direct psychotogenic effects of some substances (e.g., cannabis) [10]. Consequently, recent studies have called for an increased focus on patients with co-occurring schizophrenia and substance-related disorders for developing and evaluating potential interventions.
While treating patients with comorbid schizophrenia and substance-related disorders can be challenging, consistent antipsychotic pharmacotherapy remains a fundamental and critical aspect of treatment. Long-acting injectable therapies (LAI) may facilitate improvements in adherence and persistence to medication [11] thereby reducing the risk of relapse, which may enable additional treatment of comorbid substance use disorders [7,12]. Once-monthly paliperidone palmitate (PP1M) is an LAI that may improve adherence [11], reduce hospitalizations [13,14] and lower medical costs [13–15] compared with oral atypical antipsychotics (OAA) among patients with schizophrenia.
Clinical trials such as those evaluating PP1M are often conducting within a restricted study population (e.g., a Phase III controlled trial comparing PP1M to placebo excluded patients with active substance use) [16]. A more recent prospective clinical trial conducted in a more representative sample of patients (i.e., including patients with substance-related disorders) demonstrated symptom improvement associated with PP1M [17]. However, there remains a need to better understand the impact of PP1M specifically within the population of patients with schizophrenia and comorbid substance-related disorders. Therefore, the aim of the present study is to compare medication utilization, Medicaid spending, and healthcare resource use in schizophrenia patients with substance-related disorders initiated on PP1M or an OAA.
Materials & methods
Data source
Deidentified medical and prescription drug claims from Medicaid databases from six US states (Iowa, Kansas, Mississippi, Missouri, New Jersey, Wisconsin) from July 2009 to March 2015 were used (of note, the end of data availability was March 2014 for New Jersey and December 2013 for Wisconsin). Available data included patient eligibility (e.g., age, gender, enrollment start/end dates, and date/year of death, if applicable), medical claims (e.g., type of service, dates of service, International Classification of Diseases, 9th revision, clinical modification [ICD-9-CM] diagnoses, Current Procedural Terminology procedure codes and Healthcare Common Procedure Coding System codes) and prescription drug claims (e.g., days supplied, date of dispensing, units and National Drug Codes).
Study design
A retrospective longitudinal cohort study design was used to compare patients diagnosed with schizophrenia and substance-related disorder(s) (i.e., drug or alcohol-related disorders) who were initiated on either PP1M or an OAA. Initiation of PP1M or an OAA was defined as having at least two pharmacy and/or medical claims for PP1M or the same OAA agent within 90 days in the year 2010 or after (the first of the two claims was defined as the index date). Patient characteristics were described for the 6 months prior to the index date (baseline period). All patients were required to have a minimum of 12 months of continuous insurance eligibility postindex date.
Patient selection
For inclusion in the study, patients were required to have: at least two pharmacy and/or medical claims for PP1M or the same OAA agent (i.e., aripiprazole, asenapine maleate, iloperidone, lurasidone, olanzapine, paliperidone, quetiapine fumarate, risperidone or ziprasidone) within 90 days in the year 2010 or after (the first of the two claims was defined as the index date); no claim for the index agent (PP1M or OAA) in the baseline period; at least two claims with a diagnosis for schizophrenia at any time, with at least one claim occurring during the baseline period; at least two diagnoses for substance-related disorder(s) at any time, including at least one diagnosis during the baseline period; and at least 6 months of continuous enrollment before the index date and at least 12 months of follow-up after the index date. Patients were also required to be 18–64 years of age as of the index date and patients were excluded if they had any claim for an LAI (i.e., haloperidol, fluphenazine, aripiprazole, olanzapine, paliperidone or risperidone LAI) during the baseline period. Prior use of oral antipsychotics including OAAs was permitted given that LAIs are rarely used as first-line therapies [18], but was adjusted for as per the Statistical Analysis section. Schizophrenia diagnoses were identified using ICD-9-CM codes 295.xx. Substance-related disorders were identified using the ICD-9-CM codes listed in Supplementary Table 1.
Study measures
The primary outcomes of this study were adherence and persistence to the index antipsychotic and to any antipsychotic; all-cause healthcare costs; and healthcare resource use. Adherence and persistence were assessed during a fixed 12-month period following the index date. Adherence was defined as having a proportion of days covered (PDC) by medication ≥80% and was calculated as the numbers of nonoverlapping days of supply of available medication divided by 365 days. PDC was also compared between cohorts as a continuous variable. Persistence was defined as having no continuous gap in days of supply of medication ≥90 days. Cost and healthcare resource use outcomes were assessed during the follow-up period spanning from the index date up to the end of follow-up (i.e., the earliest of Medicaid disenrollment, death or the end of data availability). Costs were grouped into pharmacy costs and medical costs (by type). Categories for medical costs and healthcare resource use included: outpatient visits, emergency room visits, inpatient visits, skilled nursing and long-term care admissions, mental health institute admissions, one-day mental health institute outpatient visits, homecare services and other services.
Other medication utilization measures evaluated at 12 months included the number of antipsychotic claims, the number of unique antipsychotic agents received, the number of index antipsychotic claims, duration (days) of continuous exposure to the index antipsychotic (i.e., no gap ≥30, 60 or 90 days) and the presence of antipsychotic polypharmacy (i.e., overlapping coverage of ≥2 unique antipsychotic agents for ≥60 consecutive days with no more than a 7-day gap).
As a sensitivity analysis, adherence was also described using the medication possession ratio (MPR) at 12 months, which was defined as the sum of the days of supply of medication dispensed divided by the number of days between the first fill and the earliest of the end of follow-up or the last refill plus the days of supply of the last refill. MPR values >100% (i.e., ‘overadherent’) were truncated at 100%. As a sensitivity analysis, persistence was also described using no gap ≥30 days or ≥60 days.
Statistical analysis
Descriptive statistics for baseline characteristics and medication utilization measures included means, medians and standard deviations (SD) for continuous variables and frequencies and proportions for categorical variables. Statistical comparisons of baseline characteristics between cohorts used standardized differences (Stdiff), where a Stdiff ≥10% was considered clinically meaningful [19,20]. Medication utilization measures (including adherence and persistence) were compared between cohorts using chi-squared tests for categorical variables and t-tests for continuous variables. For medical claims of injectable antipsychotic agents (including PP1M), the number of days of supply was imputed based on the mode observed for each specific agent in the prescription drug claims portion of the database. Notably, these values corresponded to the indicated treatment duration (e.g., 28 days for PP1M) for all LAIs.
Multivariate adjustment (controlling for age, gender, race, state, region, year of index date, presence of dual insurance eligibility coverage, Quan-CCI, comorbidities, baseline use of atypical antipsychotics, presence of antipsychotic polypharmacy, total pharmacy costs, total medical costs, the number of mental health institute visits, the number of one-day mental health institute visits and the number of substance-related inpatient visits) was conducted for cost and healthcare resource use outcome measures. Medical and pharmacy costs were compared using multivariate ordinary least squares regression (mean monthly cost differences [MMCD]). Pharmacy costs did not include any Medicaid mandated or negotiated rebates for branded products. All cost outcomes were analyzed as per member per month, and adjusted for inflation using the medical care component of the Consumer Price Index to 2015 US dollars. For healthcare resource use, rates of events (i.e., the number of events divided by the number of months of follow-up) were compared using multivariate Poisson regression (incidence rate ratios [IRR]). Variable follow-up between patients was accounted for by computing costs using per patient per month and by including a person-time offset term in Poisson regression models for healthcare resource use. Cost and healthcare resource use confidence intervals and p-values were obtained from a nonparametric bootstrap procedure (n = 499 replications). No adjustments were made for multiple comparisons. All analyses were performed using SAS software, Version 9.3 of the SAS System for Windows, SAS Institute, Inc., NC, USA.
As this was an analysis of claims data, IRB approval was not required. Per Title 45 of CFR, Part 46.101(b)(4), the administrative claims data analysis of our study is exempt from the IRB review for two reasons: it is a retrospective analysis of existing data (hence, no patient intervention or interaction); no patient-identifiable information is included in the claims dataset.
Results
Baseline patient characteristics
A total of 351 patients receiving PP1M and 4869 patients receiving OAA fully met inclusion criteria and were included in the study (Figure 1). Patients initiated on PP1M were younger (mean age (median): 38.4 (37.2) vs 41.9 (43.5), Stdiff = 30%) and generally had a lower burden of physical comorbidities (e.g., mean Quan-Charlson comorbidity index: 0.5 vs 1.1, Stdiff = 36%; Table 1).
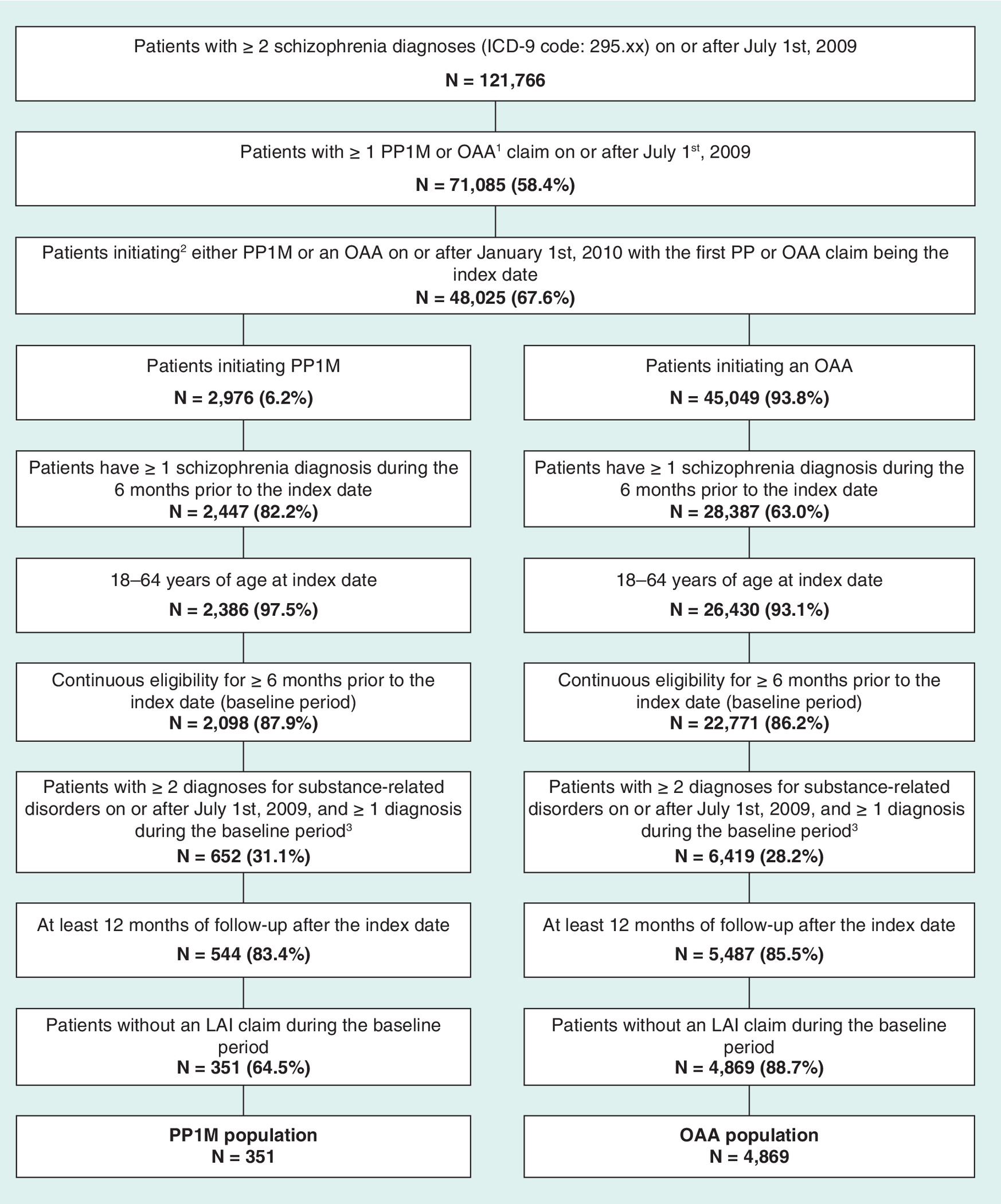
Figure 1. Identification of the study population.
1. OAA agents included aripiprazole, asenapine maleate, iloperidone, lurasidone, olanzapine, paliperidone, quetiapine fumarate, risperidone and ziprasidone.
2. Initiation of an antipsychotic agent is defined as having ≥2 claims for the same agent within 90 days and no claim of the same agent during the 6 months before the first claim.
3. Diagnoses for substance-related disorders were identified using the presence of a medical claim with a relevant International Classification of Diseases, 9th revision, clinical modification (ICD-9-CM) diagnosis code (list provided in Supplementary Table 1).
ICD-9-CM: International Classification of Diseases, 9th revision, clinical modification; LAI: Long-acting injectable therapy; OAA: Oral atypical antipsychotic; PP1M: Once-monthly paliperidone palmitate.
| PP1M (n = 351) | OAA (n = 4869) | Std diff | |
|---|---|---|---|
| Age at index date (years), mean ± SD (median) | 38.4 ± 11.5 (37.2) | 41.9 ± 11.4 (43.5) | 30.1%† |
| Age categories, N (%): | |||
| – 18–24 | 50 (14.2) | 447 (9.2) | 15.8%† |
| – 25–34 | 102 (29.1) | 1058 (21.7) | 16.9%† |
| – 35–44 | 83 (23.6) | 1155 (23.7) | 0.2% |
| – 45–54 | 89 (25.4) | 1621 (33.3) | 17.5%† |
| – 55–64 | 27 (7.7) | 588 (12.1) | 14.7%† |
| Female, N (%) | 101 (28.8) | 2005 (41.2) | 26.2%† |
| State, N (%): | |||
| – Iowa | 11 (3.1) | 230 (4.7) | 8.2% |
| – Kansas | 41 (11.7) | 384 (7.9) | 12.8%† |
| – Mississippi | 36 (10.3) | 406 (8.3) | 6.6% |
| – Missouri | 166 (47.3) | 2130 (43.7) | 7.1% |
| – New Jersey | 60 (17.1) | 1278 (26.2) | 22.4%† |
| – Wisconsin | 37 (10.5) | 441 (9.1) | 5.0% |
| Region characteristics, N (%): | |||
| – Urban | 189 (53.8) | 2868 (58.9) | 10.2%† |
| – Suburban | 86 (24.5) | 1213 (24.9) | 1.0% |
| – Rural | 76 (21.7) | 788 (16.2) | 14.0%† |
| Capitated or dual coverage, N (%) | 228 (65.0) | 3315 (68.1) | 6.6% |
| Year of index date, N (%): | |||
| – 2010 | 151 (43.0) | 2279 (46.8) | 7.6% |
| – 2011 | 94 (26.8) | 1344 (27.6) | 1.8% |
| – 2012 | 52 (14.8) | 811 (16.7) | 5.1% |
| – 2013 | 36 (10.3) | 335 (6.9) | 12.1%† |
| – 2014 | 18 (5.1) | 100 (2.1) | 16.6%† |
| Quan-CCI, mean ± SD (median) | 0.5 ± 1.2 (0.0) | 1.1 ± 1.7 (0.0) | 35.5%† |
| 5 most frequent types of schizophrenia disorder (ICD-9-CM)1, N (%): | |||
| – Schizoaffective disorder (295.7) | 178 (50.7) | 2833 (58.2) | 15.0%† |
| – Unspecified schizophrenia (295.9) | 153 (43.6) | 2105 (43.2) | 0.7% |
| – Paranoid type schizophrenia (295.3) | 191 (54.4) | 2000 (41.1) | 26.9%† |
| – Other specified types of schizophrenia (295.8) | 21 (6.0) | 293 (6.0) | 0.1% |
| – Schizophrenic disorder, residual type (295.6) | 17 (4.8) | 200 (4.1) | 3.6% |
| Antipsychotic use, N (%) | 217 (61.8) | 2553 (52.4) | 19.1%† |
| PDC for any antipsychotic agent ≥80%2, N (%) | 62 (28.6) | 763 (29.9) | 48.0%† |
| Healthcare resource utilization (≥1 visit), N (%): | |||
| – Outpatient visits | 299 (85.2) | 4350 (89.3) | 12.5%† |
| – Emergency room visits | 206 (58.7) | 206 (58.7) | 3.4% |
| – Inpatient visits | 203 (57.8) | 3188 (65.5) | 15.8%† |
| – Skilled nursing and long-term care admissions | 6 (1.7) | 221 (4.5) | 16.3%† |
| – Mental health institute admissions | 210 (59.8) | 2223 (45.7) | 28.7%† |
| – One-day mental health institute visits | 246 (70.1) | 2805 (57.6) | 26.2%† |
| – Homecare services | 75 (21.4) | 1356 (27.8) | 15.1%† |
| – Other services | 91 (25.9) | 1475 (30.3) | 9.7% |
| Monthly healthcare cost (US$ 2015), mean ± SD (median): | |||
| – Pharmacy and medical costs | 2310 ± 2942 (1246) | 3011 ± 4726 (1655) | 17.8%† |
| – Pharmacy costs | 287 ± 537 (39) | 332 ± 728 (40) | 7.0% |
| – Medical costs | 2022 ± 2818 (1022) | 2679 ± 4610 (1353) | 17.2%† |
| Observation period (months), mean ± SD (median) | 37.8 ± 15.1 (38.3) | 39.1 ± 14.2 (40.0) | 9.2% |
†Indicates standardized difference ≥10%.
1Note that types of schizophrenia disorder are not mutually exclusive.
2Defined as the number of nonoverlapping days of supply of antipsychotic medication divided by a fixed period (i.e., 6 months).
OAA = Oral atypical antipsychotic; PDC: Proportion of days covered; PP1M = Once-monthly paliperidone palmitate; Quan–CCI: Quan–Charlson comorbidity index; SD: Standard deviation; Std diff: Standardized difference.
During the baseline period, PP1M patients were more likely to have a diagnosis of paranoid-type schizophrenia (54 vs 41%, Stdiff = 27%), less likely to have a diagnosis of schizoaffective disorder (51 vs 58%, Stdiff = 15%) and had more antipsychotic use (e.g., proportion with any antipsychotic use: 66 vs 53%, Stdiff = 25%; Table 1). Among patients with antipsychotic use at baseline, the proportion of patients adherent to any antipsychotic was similar between PP1M and OAA cohorts (29 vs 30%, Stdiff = 2.9%; Table 1).
Adherence & persistence
At 12 months postindex, a higher proportion of PP1M patients were adherent on the index antipsychotic (PDC ≥ 80%: 29 vs 18%; p < 0.001) or on any antipsychotic (PDC ≥ 80%: 39 vs 31%; p = 0.001) compared with OAA patients (Table 2). When treated as a continuous variable, PP1M patients had a higher mean PDC compared with OAA patients both for the index antipsychotic (mean (median): 54% (53%) vs 46% (40%); p < 0.001) and for any antipsychotic (mean (median): 65% (70%) vs 59% (58%); p < 0.001; Table 2). When MPR was examined in a sensitivity analysis for adherence, PP1M patients were found to be more likely to be adherent (MPR ≥80%) to the index antipsychotic (65 vs 58%; p = 0.005) and to any antipsychotic (68 vs 62%; p = 0.025), consistent with the primary analysis (Table 2).
| PP1M (n = 351) | OAA (n = 4869) | p-value | |
|---|---|---|---|
| Number of antipsychotic claims, mean ± SD (median) | 13.3 ± 8.7 (12.0) | 13.9 ± 12.1 (11.0) | 0.180 |
| Number of unique antipsychotic agents received, mean ± SD (median) | 2.2 ± 1.3 (2.0) | 2.1 ± 1.2 (2.0) | 0.974 |
| Number of index antipsychotic claims, mean ± SD (median) | 8.1 ± 4.3 (8.0) | 7.5 ± 5.5 (6.0) | <0.001† |
| Duration (days) of continuous exposure to the index antipsychotic, mean ± SD (median): | |||
| – No gap ≥30 days | 65 ± 56 (55) | 60 ± 51 (45) | 0.614 |
| – No gap ≥60 days | 188 ± 127 (148) | 148 ± 114 (108) | <0.001† |
| –No gap ≥90 days | 223 ± 128 (217) | 181 ± 119 (144) | <0.001† |
| Antipsychotic polypharmacy present1, N (%) | 77 (21.9) | 1207 (24.8) | 0.231 |
| PDC (%) for index antipsychotic medication2, mean ± SD (median): | 54.2 ± 29.6 (53.4) | 45.8 ± 28.2 (40.3) | <0.001† |
| – PDC ≥80%, N (%) | 100 (28.5) | 879 (18.1) | <0.001† |
| MPR (%) for index antipsychotic medication3, mean ± SD (median): | 79.5 ± 25.1 (90.0) | 76.7 ± 26.6 (87.7) | 0.475 |
| – MPR ≥80%, N (%) | 229 (65.2) | 2804 (57.6) | 0.005† |
| Persistence in index antipsychotic treatment4, N (%): | |||
| – No gap ≥30 days | 87 (24.8) | 736 (15.1) | <0.001† |
| – No gap ≥60 days | 141 (40.2) | 1193 (24.5) | <0.001† |
| – No gap ≥90 days | 166 (47.3) | 1547 (31.8) | <0.001† |
| PDC (%) for any antipsychotic medication2, mean ± SD (median): | 64.9 ± 27.3 (70.1) | 59.0 ± 28.0 (58.1) | <0.001† |
| – PDC ≥80%, N (%) | 137 (39.0) | 1497 (30.7) | 0.001† |
| MPR (%) for any antipsychotic medication3, mean ± SD (median): | 82.9 ± 23.9 (98.8) | 79.9 ± 25.7 (95.7) | 0.192 |
| – MPR ≥80%, N (%) | 240 (68.4) | 3037 (62.4) | 0.025† |
| Persistence in any antipsychotic treatment4, N (%): | |||
| – No gap ≥30 days | 117 (33.3) | 1271 (26.1) | 0.003† |
| – No gap ≥60 days | 186 (53.0) | 1965 (40.4) | <0.001† |
| – No gap ≥90 days | 209 (59.5) | 2432 (49.9) | <0.001† |
†Indicates the p-value was <0.05 (versus OAA).
1Antipsychotic polypharmacy is defined as having ≥60 consecutive days with overlapping coverage of ≥2 unique antipsychotic agents and no more than a 7-day gap.
2PDC was defined as the sum of nonoverlapping days of available medication divided by a fixed period of time (12 months).
3MPR was defined as the sum of the days of supply of medication dispensed divided by the number of days between the first fill and the last refill plus the days of supply of the last refill.
4Persistence was defined as not having any gap more than 30, 60 or 90 days between the days of supply of medication refills.
MPR: Medication possession ratio; OAA: Oral atypical antipsychotics; PDC: Proportion of days covered; PP1M: Once-monthly paliperidone palmitate; SD: Standard deviation.
PP1M patients were also more likely than OAA patients to be persistent (i.e., no gap ≥90 days) on the index antipsychotic (47 vs 32%; p < 0.001) or on any antipsychotic (60 vs 50%; p < 0.001 at 12 months) (Table 2). In a sensitivity analysis using no gap ≥30 days or no gap ≥60 days to define persistence, PP1M patients were consistently more likely to be persistent than OAA patients (both for the index antipsychotic and any antipsychotic; Table 2).
Other medication utilization measures
On average, PP1M patients had similar numbers of antipsychotic claims compared with OAA patients and both groups received approximately two unique antipsychotic agents per patient (Table 2). However, PP1M patients had more claims for the index antipsychotic (mean (median): 8.1 (8) vs 7.5 (6); p < 0.001) and a longer duration of continuous exposure to the antipsychotic (e.g., using no gap ≥90 days, mean (median): 223 (217) days vs 181 (144) days; p < 0.001; Table 2). A lower proportion of PP1M patients had antipsychotic polypharmacy compared with OAA patients, although the difference was not significant (22 vs 25%; p = 0.231; Table 2).
All-cause healthcare costs
During follow-up and after adjustment, PP1M patients had lower medical costs (MMCD = US$-191; p = 0.020) but higher pharmacy costs (MMCD = US$250; p < 0.001), resulting in no significant difference in total healthcare costs (MMCD = US$59; p = 0.517; Figure 2). Medical cost savings appeared driven by lower inpatient costs (MMCD = US$-152; p = 0.016) and homecare costs (MMCD = $-42; p = 0.016). Emergency room costs (MMCD = US$-12; p = 0.008) were also significantly lower for PP1M patients. Costs for one-day mental institute visits were higher for PP1M than for OAA patients (MMCD = US$28; p = 0.004; Figure 2). Unadjusted monthly costs and cost differences are included in Supplementary Table 2.
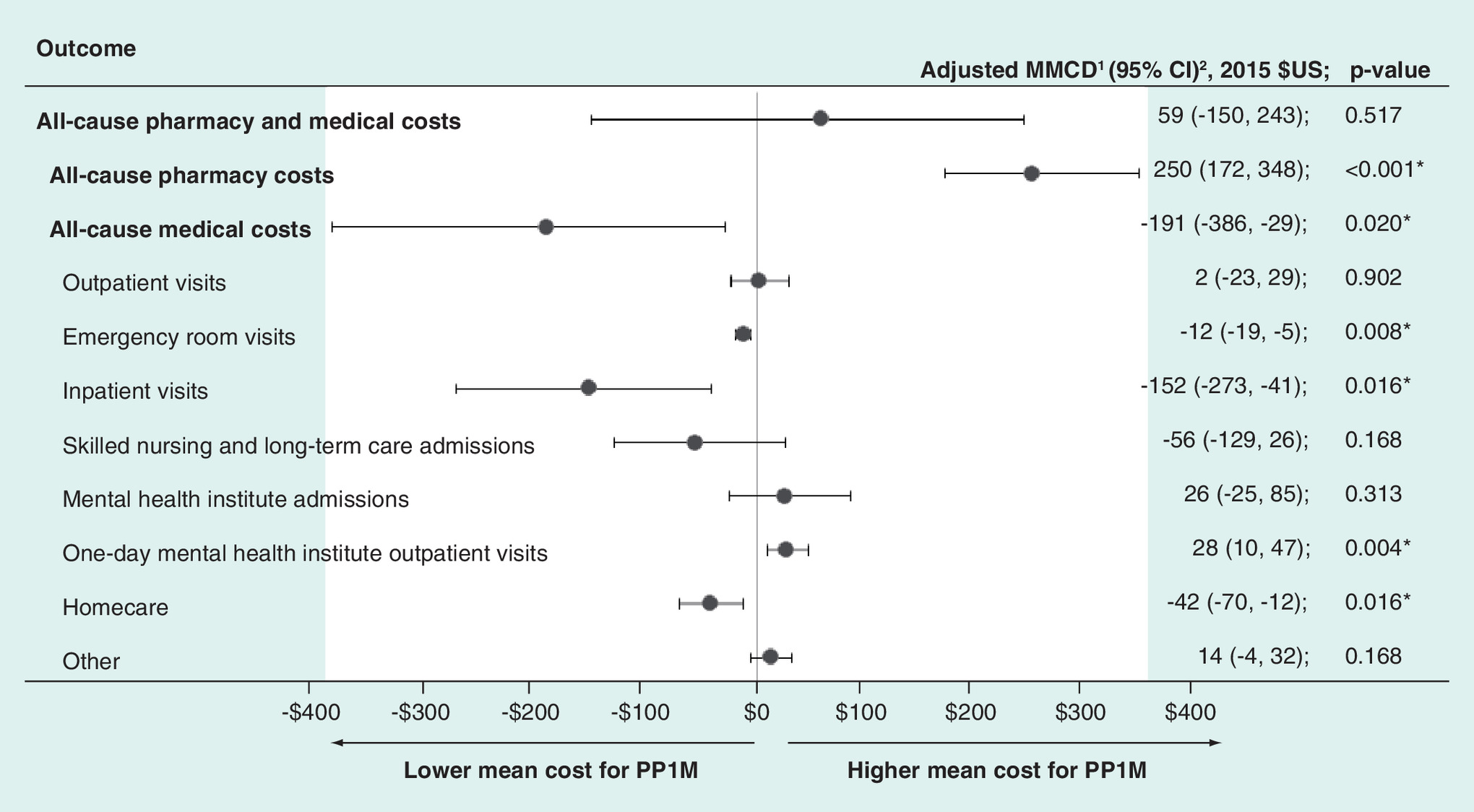
Figure 2. Adjusted mean monthly cost differences comparing patients with co-occurring schizophrenia and substance-related disorders initiated on once-monthly paliperidone palmitate or an oral atypical antipsychotic, evaluated during the overall follow-up.
1. Outcomes were assessed using multivariable linear regression models adjusted for: age, gender, race, state, region, year of index date, presence of dual insurance eligibility, Quan–CCI, comorbidities (cardiovascular disease, diabetes), baseline use of atypical antipsychotics, presence of antipsychotic polypharmacy, total pharmacy costs, total medical costs, the number of mental health institute visits, the number of 1-day mental health institute visits and the number of substance-related inpatient visits.
2. Based on a nonparametric bootstrap procedure (n = 499 samples).
*p < 0.05 (vs OAA).
CI: Confidence interval; MMCD: Mean monthly cost difference; OAA: Oral atypical antipsychotics; PP1M: Once-monthly paliperidone palmitate.
Healthcare resource use
Results comparing healthcare resource use between PP1M and OAA patients are shown in Figure 3. PP1M patients had significantly lower rates of outpatient visits (IRR = 0.90; p = 0.036) and inpatient days (IRR = 0.72; p = 0.016). However, rates of mental institute days (IRR = 1.34; p < 0.001) and one-day mental institute admissions (IRR = 1.17; p < 0.001) were higher for PP1M patients than for OAA patients (Figure 3). Unadjusted rates and IRRs for healthcare resource use are included in Supplementary Table 3.
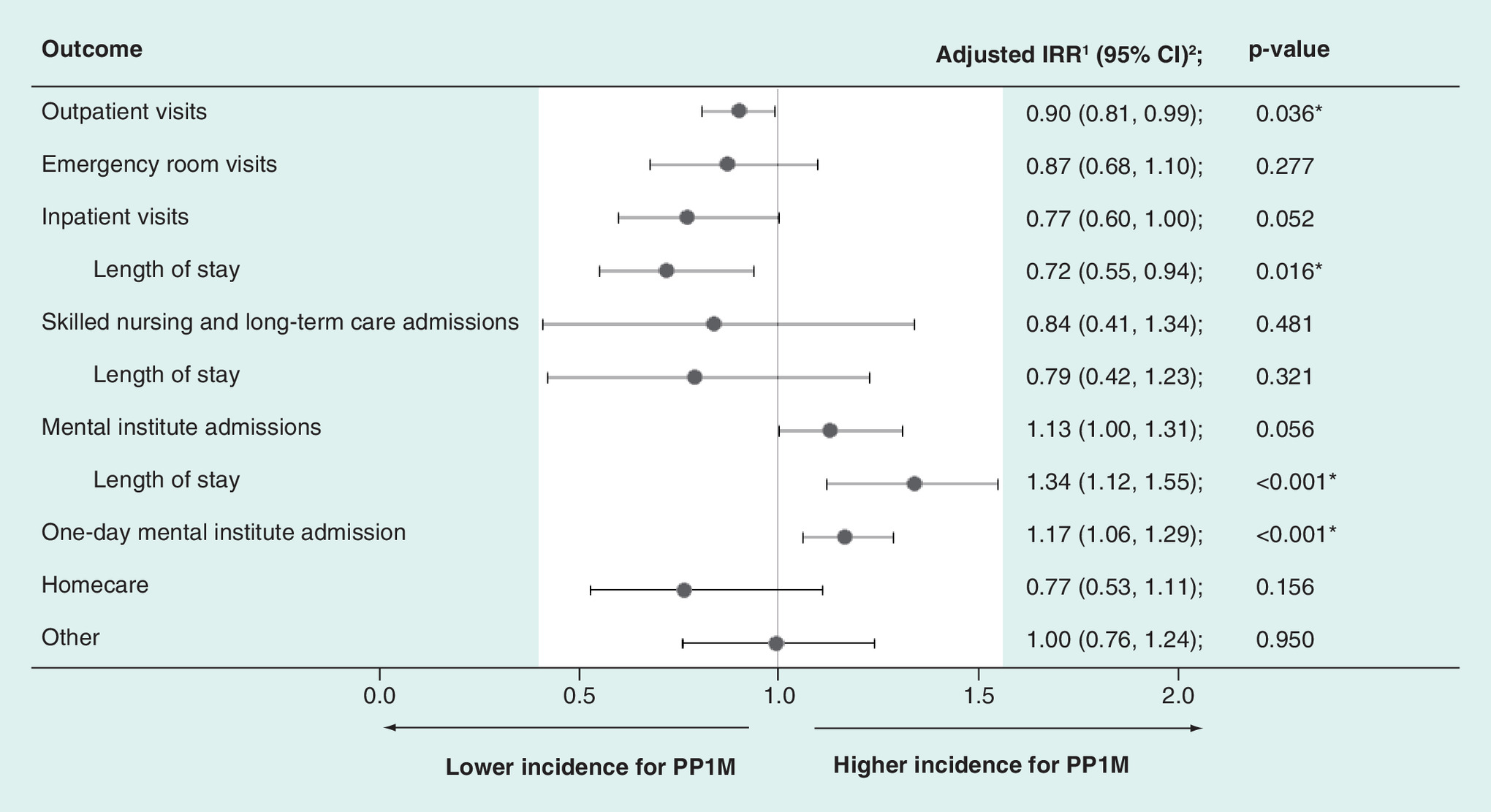
Figure 3. Adjusted incidence rate ratios comparing patients with co-occurring schizophrenia and substance-related disorders initiated on once-monthly paliperidone palmitate or an oral atypical antipsychotic, evaluated during the overall follow-up.
1. Outcomes were assessed using multivariable Poisson regression models adjusted for: age, gender, race, state, region, year of index date, presence of dual insurance eligibility, Quan-CCI, comorbidities (cardiovascular disease, diabetes), baseline use of atypical antipsychotics, presence of antipsychotic polypharmacy, total pharmacy costs, total medical costs, the number of mental health-institute visits, the number of one-day mental health-institute visits, and the number of substance-related inpatient visits.
2. Based on a non-parametric bootstrap procedure (n = 499 samples).
*p < 0.05 (vs OAA).
CI: Confidence interval; IRR: Incidence rate ratio; OAA: Oral atypical antipsychotics; PP1M: Once-monthly paliperidone palmitate.
Discussion
The findings of the present study demonstrate that in a real-world population of patients with schizophrenia and comorbid substance-related disorders, patients who were initiated on PP1M were more adherent to therapy and were more likely to remain on therapy up to 12 months postindex date. Furthermore, PP1M was associated with lower medical costs over patients’ follow-up compared with OAA. There may be several reasons for the observed benefits in the present study. First, by providing consistent and extended serum levels of antipsychotic medication, PP1M may provide some protection from the psychotogenic effects of substances of abuse. Alternately, while some substances of abuse may be associated with less regular medication adherence even without direct psychotogenic effects, PP1M's pharmacokinetic profile eliminates the need for a person to consume daily medications so long as they are receiving their scheduled monthly doses.
These findings are in agreement with previous retrospective studies which have demonstrated that PP1M is associated with improved adherence [11], reduced hospitalizations [13,14] and lower medical costs [13–15] in real-world populations of patients with schizophrenia. Importantly, the present findings highlight consistent trends within the difficult-to-treat subpopulation of patients with schizophrenia and substance-related disorders. This is in good agreement with existing evidence supporting limited difference in the efficacy (in terms of symptom management and global improvement) of antipsychotic therapy in patients with co-occurring substance use disorders as compared with the general population with schizophrenia [21,22]. Furthermore, the present findings underscore that despite barriers to effective clinical management posed by substance-related disorders, such as the acute impacts of substance use on cognition as well as the psychotogenic effects of some substances [10], treatment with PP1M was associated with improved antipsychotic adherence.
While efficacy may be similar for patients with and without co-occurring substance-related disorders, when differences in treatment duration have been taken into account, substance use consistently predicts poorer adherence and higher rates of discontinuation [4–6]. In a recent pooled analysis of two randomized trials (total n = 1154), substance use was associated with reduced adherence which sequentially predicted earlier discontinuation [23]. Indeed in the current analysis, antipsychotic adherence rates (∼30–40%) in patients with co-occurring substance-related disorders, were lower than those observed among a recently studied population with and without substance-related disorders treated with PP1M following a recent hospitalization (51%) [11]. Patients with poor adherence to therapy are considered appropriate candidates for LAIs such as PP1M. Furthermore, antipsychotics are recommended in patients with schizophrenia – both for those with and without substance-related disorders. These factors combined with the fact that adherence and discontinuation issues are especially prevalent in patients with substance-related disorders suggest an important potential role for LAIs in this population. Indeed, several authors have expressed similar viewpoints [24–26]; however, the paucity of evidence on the use of LAIs in these patients is frequently highlighted in the literature.
The present study addresses a critical gap in the literature by providing real-world evidence to support the hypothesis that the use of an LAI, specifically PP1M, in patients with schizophrenia and co-occurring substance use disorders, is associated with improved adherence and reduced medical costs when compared with oral antipsychotics. Very few studies have examined this to date, and of those that have, many had small sample sizes, limited follow-up and did not include newer LAI agents such as PP1M [27–29]. One randomized trial of long-acting versus oral risperidone in patients with co-occurring alcohol use disorder (n = 95) did not find evidence to support that the long-acting formulation decreased alcohol consumption or resulted in better symptoms than the oral formulation but did find improvements in adherence associated with LAI [27]. Two small open-label studies have shown improved psychiatric symptoms associated with the use of flupenthixol (a first-generation LAI) in patients with cocaine-related disorders/use (n = 8) [28] and in patients with alcohol dependence (n = 27) [29]. A later open-label randomized trial by Rubio et al. found that risperidone LAI (n = 57) was associated with less illicit drug use and longer time to relapse as compared with zuclopenthixol LAI (n = 58), which they found to predict better symptom scores and compliance with a substance use management program [30]. One recent observational study among US veterans diagnosed with schizophrenia and substance abuse found that PP1M was associated with improvements in treatment adherence and medical cost savings [31]. However, to the best of our knowledge, no other real-world studies have compared adherence and economic outcomes between patients initiated on PP1M versus OAA within the population diagnosed with co-occurring substance-related disorders.
The main strengths of the present study include the comprehensive look at adherence and persistence, the findings for which were robust to sensitivity analyses using MPR and different gap lengths, respectively. Furthermore, these findings demonstrated that higher adherence associated with PP1M was consistent whether adherence was considered for the index agent alone or for all antipsychotics. The present study also showed that higher adherence for all antipsychotics did not appear to be driven by more polypharmacy in these patients. The examination of economic outcomes, including both medical and pharmacy costs, are another key strength that adds to the literature. In order to capture economic impacts of treatment that may not be observable over a restricted and relatively short-term follow-up, patients’ overall follow-up (∼38–39 months) was used to evaluate economic outcomes. The authors hypothesize that lower medical costs for PP1M patients may have been the result of higher adherence and persistence on treatment which may have avoided relapse and subsequent hospitalizations or other visits. While we observed reductions in inpatient visits associated with PP1M, we also observed higher rates of mental health-related admissions. This is an interesting finding that we believe may reflect diversions of care from less to more specialized facilities. However, it deserves additional investigation in future research to understand whether these differences reflect any differences in the quality or appropriateness of care, or if they may partially reflect differences in the mode of administration of these therapies (e.g., PP1M administered in an outpatient setting). The higher pharmacy costs observed for PP1M patients are likely related to the higher level of antipsychotic adherence and persistence in patients treated with PP1M (i.e., patients were on treatment for a longer period of time and had more medication available within the first 12 months). Of note, costs used did not account for mandatory discounts on branded pharmaceutical products for Medicaid [32] and other negotiated rebates with manufacturers which may have led to an overestimation of pharmacy costs; this is likely to have disproportionately affected the PP1M cohort, thus underestimating the benefits of PP1M. However, future studies would benefit from examining longer follow-up periods in order to understand whether higher pharmacy costs during the initial 1–2 years after treatment may translate to lower polypharmacy, and better outcomes (and thus, perhaps, lower medical costs) over the long term.
While this study represents an important contribution to the literature in an understudied topic, we believe that future studies are still needed to generate evidence related to the use of PP1M and other LAIs in this population. Specifically, clinical outcomes that may be subsequent to adherence, such as relapse and rehospitalization, should be key outcomes in future investigations. Furthermore, while the present study focused on PP1M, it would be important to know whether similar findings are observed across other second-generation LAI agents, particularly given the differences observed in previous studies (not restricted to patients with co-occurring substance use) [11].
Study limitations
This study is subject to several limitations that warrant discussion. First, as with all retrospective administrative claims data, the study results may be subject to selection bias and residual confounding due to unmeasured confounders, though a large number of covariates were included in the multivariate analyses. In particular, there may be residual bias related to ‘confounding by indication’, which refers to confounding introduced because of differences in the underlying population who may be prescribed PP1M versus OAA. Claims databases may also contain inaccuracies or omissions in diagnoses and other variables, although this is not expected to be differential between cohorts.
The present study examined patients with co-occurring substance-related disorders which may consist of a heterogeneous group of patients who may have varying levels of severity of their disorders and who use different substances. Also, substance-related disorders may be undercoded in the data, particularly for certain substances such as nicotine/tobacco which are commonly used by these patients. Thus, we expect that the present population (who are required to have at least two diagnoses for a substance-related disorder during the study period) may over represent severe patients (i.e., those most likely to receive a diagnosis) while excluding some patients with mild disorders. A prior validation study has suggested that ICD codes may have high specificity for identifying selected substance-related disorders, although the predictive value of such algorithms may vary across patient populations [33]. Further study is needed to examine whether the particular codes used in this investigation have a high sensitivity and specificity for substance-related disorders in this population.
In addition, included patients were required to have at least two dispensings of the index medication to confirm that they indeed were being treated with that agent; however as a result, some patients with very poor adherence or persistence (i.e., those who did not return for a second dispensing) were excluded. Last, given that specific criteria were applied to identify this population and given that a Medicaid payer's perspective was used, these findings may not be generalizable to other populations, including other Medicaid states. Moreover, cost and resource use outcomes may not account for services that were not insured through Medicaid coverage.
Conclusion
Among Medicaid beneficiaries diagnosed with schizophrenia and substance-related disorders, patients initiated on PP1M were more likely to be adherent and persistent to antipsychotics after 12 months. After adjustment, PP1M patients had lower medical costs during their overall follow-up compared with patients initiated on an OAA. Higher pharmacy costs among PP1M patients appeared to be fully offset by medical cost savings prior to accounting for any discounts or rebates. PP1M patients had fewer inpatient visits but more one-day mental health institute admissions. This shift in healthcare resource use may suggest that more PP1M patients’ inpatient admissions were diverted to more specialized, community-based care. Future studies are needed to further understand the potential value of PP1M and other LAIs in this vulnerable subpopulation of patients with schizophrenia and co-occurring substance-related disorders.
Future perspective
Patients with co-occurring substance-related disorders comprise a large proportion of the population with schizophrenia and account for an even larger proportion of the schizophrenia-related disease burden. Given the changing landscape of available antipsychotic treatments (including the approval of PP1M and once-every-3-month paliperidone palmitate [PP3M]), this area of research is likely to continue to evolve and expand. Both clinical and real-world studies are expected to continue to inform how clinicians and health policy makers can better serve this vulnerable subpopulation of patients with schizophrenia and co-occurring substance-related disorders.
Adherence & persistence
At 12 months, patients initiated on once-monthly paliperidone palmitate (PP1M) were more likely to be adherent and persistent on the index antipsychotic and on any antipsychotic, regardless of the measures used (i.e., proportion of days covered or medication possession ratio ≥80% for adherence, and no gap ≥30, 60 or 90 days for persistence).
Findings for adherence and persistence did not appear to be driven by differences in antipsychotic polypharmacy between cohorts.
Other medication utilization measures
At 12 months, PP1M patients had similar numbers of antipsychotic claims compared with oral atypical antipsychotics (OAA) patients and both groups received approximately two unique antipsychotic agents per patient.
PP1M patients had more claims for the index antipsychotic and were treated continuously for a longer period.
All-cause healthcare costs
During the follow-up and after adjustment, PP1M patients had lower medical costs but higher pharmacy costs, resulting in no significant difference in total healthcare costs.
Lower medical costs appeared driven by lower inpatient and homecare costs; PP1M patients also had lower emergency room costs. However, one-day mental institute visit costs were higher for PP1M versus OAA patients.
Healthcare resource use
Different patterns of healthcare resource use were seen between cohorts.
For example, PP1M patients had lower rates of outpatient visits and inpatient days, while having higher rates of mental institute-related visits and days.
Conclusion
Among Medicaid beneficiaries diagnosed with schizophrenia and substance-related disorders, patients initiated on PP1M were more likely to be adherent and persistent to antipsychotics after 12 months.
Compared with OAA, PP1M was also associated with lower medical costs which appeared to completely offset higher pharmacy costs prior to any rebates or discounts.
Shifting patterns in healthcare resource use may suggest that PP1M patients’ inpatient admissions were diverted to more specialized, community-based care. Future studies are needed to further understand the relationship between treatment and changing healthcare resource use in this population.
Acknowledgements
Previous presentation: Part of the material in this manuscript has been presented at the 29th American Psychiatric Association (APA) Annual Meeting, 20–24 May 2017, San Diego, CA, USA.
Authors’ contributions
All authors contributed to the conception and design of the current study. Analyses were carried out by M-H Lafeuille, R Kamstra and S Tiggelaar. All authors were involved in interpreting the findings and drafting the manuscript, and all approve the final version.
Financial & competing interests disclosure
M-H Lafeuille, R Kamstra, S Tiggelaar and P Lefebvre are employees of Analysis Group, Inc., a consulting company that has received research grants from Janssen Scientific Affairs, LLC, to conduct this study. K Joshi, Y Yue, E Kim and N Tandon are employees and stockholders of Johnson & Johnson. This research was funded by Janssen Scientific Affairs, LLC. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
As this was an analysis of claims data, IRB approval was not required. Per Title 45 of CFR, Part 46.101(b)(4), the administrative claims data analysis of our study is exempt from the IRB review for two reasons: it is a retrospective analysis of existing data (hence, no patient intervention or interaction); no patient-identifiable information is included in the claims dataset.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 29.97 KB
References
1.
Barnett JH, Werners U, Secher SM et al. Substance use in a population-based clinic sample of people with first-episode psychosis. Br. J. Psychiatry 190, 515–520 (2007).
2.
Hartz SM, Pato CN, Medeiros H et al. Comorbidity of severe psychotic disorders with measures of substance use. JAMA Psychiatry 71(3), 248–254 (2014).
3.
Crump C, Winkleby MA, Sundquist K, Sundquist J. Comorbidities and mortality in persons with schizophrenia: a Swedish national cohort study. Am. J. Psychiatry 170(3), 324–333 (2013).
4.
Colizzi M, Carra E, Fraietta S et al. Substance use, medication adherence and outcome one year following a first episode of psychosis. Schizophr. Res. 170(2), 311–317 (2016).
5.
Perkins DO, Gu H, Weiden PJ, McEvoy JP, Hamer RM, Lieberman JA. Predictors of treatment discontinuation and medication nonadherence in patients recovering from a first episode of schizophrenia, schizophreniform disorder, or schizoaffective disorder: a randomized, double-blind, flexible-dose, multicenter study. J. Clin. Psychiatry 69(1), 106–113 (2008).
6.
MacEwan JP, Forma FM, Shafrin J, Hatch A, Lakdawalla DN, Lindenmayer J-P. Patterns of adherence to oral atypical antipsychotics among patients diagnosed with schizophrenia. J. Manag. Care Spec. Pharm. 22(11), 1349–1361 (2016).
7.
Olivares JM, Sermon J, Hemels M, Schreiner A. Definitions and drivers of relapse in patients with schizophrenia: a systematic literature review. Ann. Gen. Psychiatry 12(1), 32 (2013).
8.
Ascher-Svanum H, Zhu B, Faries DE et al. The cost of relapse and the predictors of relapse in the treatment of schizophrenia. BMC Psychiatry 10, 2 (2010).
9.
Hjorthøj C, Østergaard MLD, Benros ME et al. Association between alcohol and substance use disorders and all-cause and cause-specific mortality in schizophrenia, bipolar disorder, and unipolar depression: a nationwide, prospective, register-based study. Lancet Psychiatry 2(9), 801–808 (2016).
10.
Winklbaur B, Ebner N, Sachs G, Thau K, Fischer G. Substance abuse in patients with schizophrenia. Dialogues Clin. Neurosci. 8(1), 37 (2006).
11.
Marcus SC, Zummo J, Pettit AR, Stoddard J, Doshi JA. Antipsychotic adherence and rehospitalization in schizophrenia patients receiving oral versus long-acting injectable antipsychotics following hospital discharge. J. Manag. Care Spec. Pharm. 21(9), 754–769 (2015).
12.
Haddad P, Brain C, Scott J. Nonadherence with antipsychotic medication in schizophrenia: challenges and management strategies. Patient Relat. Outcome Meas. 5, 43 (2014).
13.
Lafeuille M-H, Grittner AM, Fortier J et al. Comparison of rehospitalization rates and associated costs among patients with schizophrenia receiving paliperidone palmitate or oral antipsychotics. Am. J. Heal. Pharm. 72(5), 378–389 (2015).
14.
Baser O, Xie L, Pesa J, Durkin M. Healthcare utilization and costs of veterans health administration patients with schizophrenia treated with paliperidone palmitate long-acting injection or oral atypical antipsychotics. J. Med. Econ. 18(5), 357–365 (2014).
15.
Xiao Y, Muser E, Lafeuille M-H et al. Impact of paliperidone palmitate versus oral atypical antipsychotics on healthcare outcomes in schizophrenia patients. J. Comp. Eff. Res. 4(6), 579–592 (2015).
16.
Nasrallah HA, Gopal S, Gassmann-Mayer C et al. A controlled, evidence-based trial of paliperidone palmitate, a long-acting injectable antipsychotic, in schizophrenia. Neuropsychopharmacology 35(10), 2072–2082 (2010).
17.
Hargarter L, Cherubin P, Bergmans P et al. Intramuscular long-acting paliperidone palmitate in acute patients with schizophrenia unsuccessfully treated with oral antipsychotics. Prog. Neuropsychopharmacol. Biol. Psychiatry 58, 1–7 (2015).
18.
Patel MX, Taylor M, David AS. Antipsychotic long-acting injections: mind the gap. Br. J. Psychiatry Suppl. 52, S1–S4 (2009).
19.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. Academic Press, Inc., Toronto, Canada (1977).
20.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 46(3), 399–424 (2011).
21.
Wobrock T, Falkai P, Schneider-Axmann T et al. Comorbid substance abuse in first-episode schizophrenia: effects on cognition and psychopathology in the EUFEST study. Schizophr. Res. 147(1), 132–139 (2013).
22.
Swartz MS, Wagner HR, Swanson JW et al. The effectiveness of antipsychotic medications in patients who use or avoid illicit substances: results from the CATIE study. Schizophr. Res. 100(1–3), 39–52 (2008).
23.
Czobor P, Van Dorn RA, Citrome L, Kahn RS, Fleischhacker WW, Volavka J. Treatment adherence in schizophrenia: a patient-level meta-analysis of combined CATIE and EUFEST studies. Eur. Neuropsychopharmacol. 25(8), 1158–1166 (2015).
24.
Koola MM, Wehring HJ, Kelly DL. The potential role of long-acting injectable antipsychotics in people with schizophrenia and comorbid substance use. J. Dual Diagn. 8(1), 50–61 (2012).
25.
Velligan DI, Weiden PJ, Sajatovic M et al. Strategies for addressing adherence problems in patients with serious and persistent mental illness: recommendations from the expert consensus guidelines. J. Psychiatr. Pract. 16(5), 306–324 (2010).
26.
Portilla Fernández A, Reula L, Manrique Astiz E et al. The role of long-acting antipsychotic treatment in schizophrenia with comorbid drug use. The case of paliperidone palmitate. Eur. Psychiatry 33, S681 (2017).
27.
Green AI, Brunette MF, Dawson R et al. Long-acting injectable vs oral risperidone for schizophrenia and co-occurring alcohol use disorder: a randomized trial. J. Clin. Psychiatry 76(10), 1359–1365 (2015).
28.
Levin FR, Evans SM, Coomaraswammy S, Collins ED, Regent N, Kleber HD. Flupenthixol treatment for cocaine abusers with schizophrenia: a pilot study. Am. J. Drug Alcohol Abuse. 24(3), 343–360 (1998).
29.
Soyka M, Aichmüller C, v Bardeleben U et al. Flupenthixol in relapse prevention in schizophrenics with comorbid alcoholism: results from an open clinical study. Eur. Addict. Res. 9(2), 65–72 (2003).
30.
Rubio G, Martínez I, Ponce G, Jiménez-Arriero MA, López-Muñoz F, Álamo C. Long-acting injectable risperidone compared with zuclopenthixol in the treatment of schizophrenia with substance abuse comorbidity. Can. J. Psychiatry 51(8), 531–539 (2006).
31.
Lefebvre P, Muser E, Joshi K et al. Impact of paliperidone palmitate versus oral atypical antipsychotics on health care resource use and costs in veterans with schizophrenia and comorbid substance abuse. Clin Ther. 39 (7), 1380–1395 (2017).
32.
Medicaid Drug Rebate Program (2016). www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Benefits/Prescription-Drugs/Medicaid-Drug-Rebate-Program.html
33.
Kim HM, Smith EG, Stano CM et al. Validation of key behaviourally based mental health diagnoses in administrative data: suicide attempt, alcohol abuse, illicit drug abuse and tobacco use. BMC Health Serv. Res. 12(1), 18 (2012).
Information & Authors
Information
Published In
Copyright
© 2018 Marie-Hélène Lafeuille.
History
Published online: 15 August 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world adherence and economic outcomes associated with paliperidone palmitate versus oral atypical antipsychotics in schizophrenia patients with substance-related disorders using Medicaid benefits. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0043
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- María Vidal-Millares, Sergio Salgado-Santamaría, Javier Vicente-Alba, Ana María Gago-Ageitos, María del Carmen García-Mahía, Indalecio Homero Carrera-Machado, Antipsicóticos de larga duración en patología dual: evolución de 5 años, Revista Colombiana de Psiquiatría, 10.1016/j.rcp.2024.04.007, 55, 1, (51-59), (2026).
- Jeffrey A. Lieberman, Alana Mendelsohn, Terry E. Goldberg, Robin Emsley, Preventing disease progression in schizophrenia: What are we waiting for, Journal of Psychiatric Research, 10.1016/j.jpsychires.2024.12.042, 181, (716-727), (2025).
- Sarah Pratt, Melanie Bennett, Mary F. Brunette, Scott Stroup, Diana O. Perkins, Lisa B. Dixon, Chapter 10. Co-occurring Disorders and Conditions, The American Psychiatric Association Publishing Textbook of Schizophrenia, Second Edition, 10.1176/appi.books.9781615379194.lg10, (205-249), (2024).
- Leslie Citrome, Mark Suett, Kelli Franzenburg, Roy Eshet, Anna Elgart, Glen Davis 3rd, Eran Harary, Orna Tohami, Marko Mychaskiw, John Kane, TV-46000, A Long-Acting Subcutaneous Antipsychotic Agent, Demonstrated Improved Patient-Centered Outcomes in Patients with Schizophrenia, Neuropsychiatric Disease and Treatment, 10.2147/NDT.S459104, Volume 20, (1901-1917), (2024).
- Jacqueline Pesa, Zhiwen Liu, Alex Z. Fu, Alicia K. Campbell, Richard Grucza, Racial disparities in utilization of first-generation versus second-generation long-acting injectable antipsychotics in Medicaid beneficiaries with schizophrenia, Schizophrenia Research, 10.1016/j.schres.2023.09.033, 261, (170-177), (2023).
- Christoph U. Correll, Carmela Benson, Bruno Emond, Charmi Patel, Marie-Hélène Lafeuille, Dee Lin, Laura Morrison, Isabelle Ghelerter, Patrick Lefebvre, Panagiotis Mavros, Comparison of clinical outcomes in patients with schizophrenia following different long-acting injectable event-driven initiation strategies, Schizophrenia, 10.1038/s41537-023-00334-3, 9, 1, (2023).
- Cristiana Montemagni, Elisa Del Favero, Elena Cocuzza, Flavio Vischia, Paola Rocca, Effect of long-acting injectable antipsychotics on hospitalizations and global functioning in schizophrenia: a naturalistic mirror-image study, Therapeutic Advances in Psychopharmacology, 10.1177/20451253221122526, 12, (2022).
- Young-Chul Chung, Yen Kuang Yang, Ahmad Hatim Sulaiman, Paul Bergmans, Wilson Tan, Asian Subgroup Analysis of the REMISSIO Study: A Long-Term Efficacy and Safety Study of Paliperidone Palmitate 3-month Formulation in Patients with Stable Schizophrenia in a Naturalistic Clinical Setting, Clinical Psychopharmacology and Neuroscience, 10.9758/cpn.2022.20.3.427, 20, 3, (427-439), (2022).
- Maryia Zhdanava, H Lynn Starr, Patrick Lefebvre, Todor I Totev, Aditi Shah, Kristy Sheng, Dominic Pilon, Understanding the Health System Conditions Affecting the Use of Long-Acting Injectable Antipsychotics in the Treatment of Schizophrenia in Clinical Practice: A US Healthcare Provider Survey, Neuropsychiatric Disease and Treatment, 10.2147/NDT.S369494, Volume 18, (1479-1493), (2022).
- Chizimuzo T.C. Okoli, Amani Kappi, Tianyi Wang, Andrew Makowski, Andrew T. Cooley, The effect of long‐acting injectable antipsychotic medications compared with oral antipsychotic medications among people with schizophrenia: A systematic review and meta‐analysis, International Journal of Mental Health Nursing, 10.1111/inm.12964, 31, 3, (469-535), (2021).