Nine years of comparative effectiveness research education and training: initiative supported by the PhRMA Foundation
Abstract
The term comparative effectiveness research (CER) took center stage with passage of the American Recovery and Reinvestment Act (2009). The companion US$1.1 billion in funding prompted the launch of initiatives to train the scientific workforce capable of conducting and using CER. Passage of the Patient Protection and Affordable Care Act (2010) focused these initiatives on patients, coining the term ‘patient-centered outcomes research’ (PCOR). Educational and training initiatives were soon launched. This report describes the initiative of the Pharmaceutical Research and Manufacturers Association of America (PhRMA) Foundation. Through provision of grant funding to six academic Centers of Excellence, to spearheading and sponsoring three national conferences, the PhRMA Foundation has made significant contributions to creation of the scientific workforce that conducts and uses CER/PCOR.
Gaining momentum since the passage of the Medicare Prescription Drug, Improvement and Modernization Act of 2003 [1], the mandate to conduct comparative effectiveness research (CER) took center stage with passage of the American Recovery and Reinvestment Act (ARRA) of 2009 [2]. The focus of CER on understanding real world effectiveness of treatments soon evolved into a related concept that embraced the patient as central to decision making healthcare informed by ‘patient-centered outcomes research’ (PCOR), which was a central feature of the Patient Protection and Affordable Care Act, passed on 23 March 2010 [3].
The Federal Coordinating Council on CER, created under the ARRA, defines CER as “the conduct and synthesis of research comparing the benefits and harms of various interventions and strategies for preventing, diagnosing, treating and monitoring health conditions in real-world settings” [4]. The companion Institute of Medicine report, published shortly thereafter, recommended a portfolio of 100 study topics related to a variety of diseases, research methods and care models important to the US population [5]. The purpose of CER is to improve health outcomes by developing and disseminating evidence-based information to patients, clinicians and other decision makers about which interventions are most effective for which patients under specific circumstances [4]. PCOR introduces additional, critical facets to decision making in healthcare that focus on the patient perspective and their family – what matters, to which patients, when/under what circumstances [6]. It is an important step toward personalized medicine, seeking to elucidate more than heterogeneous treatment effects and quantifying risk and benefit. PCOR recognizes that patients differ in their willingness to trade off certain risks and benefits, and it affects decision making across the lifespan, and for many life and death decisions, only the patient can or should decide.
Although, not a new idea at the time, the US$1.1 billion in federal funding provided by passage of the ARRA and the establishment of the Patient-Centered Outcomes Research Institute (PCORI) were the impetus for increased enthusiasm for the conduct of CER/PCOR on the part of scientists representing multiple disciplines. Coupled with this enthusiasm came the need to both augment and accelerate the number of scientists trained to conduct and disseminate CER/PCOR to address the nation's healthcare needs [7]. It was immediately apparent that there would be primarily two primary groups of stakeholders – those conducting and disseminating the research; and those making healthcare decisions at the point of care, both clinicians and their patients.
Scientists conducting CER eagerly embraced the idea of their work being neatly and newly packaged as CER/PCOR and many identified with the need to provide enhanced training to their graduate and health professional students. To that end, many academic institutions have tailored at least some of their course offerings to advance CER/PCOR and many professional societies have done the same, some with support from nonprofit foundations. One of these initiatives was envisioned by CER/PCOR scientists working largely in the area of pharmaceuticals, and was supported by the Pharmaceutical Research and Manufacturers Association of America (PhRMA) Foundation [8].
The PhRMA Foundation's 9-year initiative in CER/PCOR began with the convening of an inaugural consensus development conference (2009) and published report (2011) wherein CER/PCOR scientists reached agreement on a model graduate curriculum for CER/PCOR (Figure 1) [9]. This was followed by the PhRMA Foundation's request for proposals (RFP) that subsequently funded a total of six academic Centers of Excellence in CER/PCOR between 2012 and 2015. In the intervening years, the PhRMA Foundation hosted two national invitational conferences to facilitate discourse about a model graduate level curriculum in CER/PCOR. The first of these two conferences (2014) focused on developing a curriculum for training research scientists to conduct and disseminate CER/PCOR, and was titled, “Curricular Advances for Patient-Centered Comparative Effectiveness Research”. The second conference (2017) focused on optimizing the uptake and use of CER/PCOR by decision-makers and patients, and was titled, “Comparative Effectiveness and Patient-Centered Outcomes Research: Enhancing Uptake and Use by Patients, Clinicians and Payers”. In the following report, each component of this initiative is described chronologically.
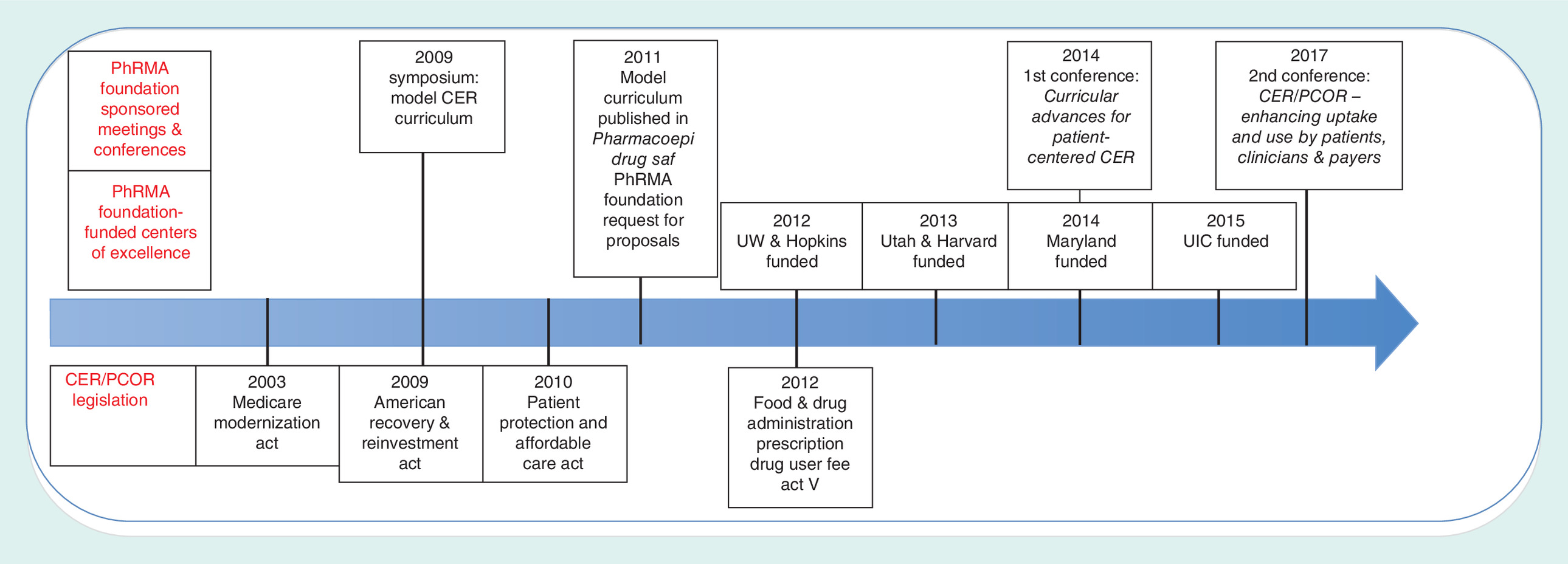
Figure 1. Timeline of activities: Pharmaceutical Research and Manufacturers Association of America Foundation comparative effectiveness research education and Training Initiative.
CER: Comparative effectiveness research; PCOR: Patient-centered outcomes research; PhRMA: Pharmaceutical Research & Manufacturers Association; Pharmacoepi Drug Safety: Pharmacoepidemiology and drug safety; UIC: University of Illinois at Chicago; UW: University of Washington.
Inaugural Consensus Development Conference (2009): Pharmaceutical Research & Manufacturers Association of America Foundation Sponsored Model Curriculum Project
In March 2009, the PhRMA Foundation's Health Outcomes Research Committee recommended establishment of a Center of Excellence for CER Education Grant Program, and commenced the writing of an RFP to fund academic Centers of Excellence that would develop and teach CER curricula. Leading pharmaceutical CER/PCOR scientists were invited by E Cannon, then Executive Director (now President) of the PhRMA Foundation and JP Gagnon to join this workgroup [9]. The 17-member panel for the program consisted of academicians, industry scientists, professional association leaders and a federal agency program officer. Members represented the disciplines of medicine, pharmacy, clinical epidemiology, pharmacoepidemiology, pharmacoeconomics, informatics, information sciences and health services research. Consensus development involved completion of a premeeting survey and attendance at an in-person meeting, and culminated in a written consensus report. The premeeting survey used a nominal group process to identify knowledge areas, skills and abilities required to competently conduct or expertly utilize CER/PCOR [10].
In December 2009, the panel met at the PhRMA Foundation's headquarters in Washington DC to discuss the results of the survey and design the model curriculum. Key knowledge areas identified including an understanding of observational research methods, data resources, and the USA healthcare system. Identified skills and abilities included data management, critical evaluation of the literature, development of analytic plans and the ability to interpret findings and the impact of those findings on insurance products [7,9]. It was here where the concepts of dissemination and implementation science and translational science came into focus [7]. The panel saw the need for both didactic and active learning experiences and emphasized a role for real world data. Although, the experience of the panel was largely in the realm of pharmaceuticals, members clearly saw the need to broaden the reach of CER/PCOR to include diagnostics, devices, behavioral and educational interventions and health-system delivery changes. Although, there was sentiment among panel members of the need for a structured doctoral program in CER/PCOR, they also realized that several academic centers already teach these concepts; for them, simple adjustments to current offerings would be all that would be needed.
Responding to the call: the Pharmaceutical Research & Manufacturers Association Foundation's request for proposals for “Development of a Center of Excellence for a Comparative Effectiveness Research Educational Program”
In an effort to integrate this multidisciplinary field into a cohesive whole, in 2011, the PhRMA Foundation put forth a call to academic centers to develop degree-granting programs in CER/PCOR. To be funded by a 3-year grant to develop and implement a detailed CER curriculum, requirements of the RFP were directly aligned with the report of the Model Curriculum Project. The goals of the RFP were eightfold: to develop programs that train scholars who conduct rigorous, useful and effective CER; to produce high quality researchers who are capable of interpreting and integrating CER into practice; to provide resources to develop corroborating evidence on the usefulness and value of CER; to convene public forums to educate the broader public about CER; to collectively establish a core CER curriculum for the nation; to sponsor lectures in regional and national venues to promote thoughtful discussions about important CER topics; to determine workload needs for CER; and to use electronic means to make the results of CER training materials widely accessible to the public. Eligible academic institutions were those who offered degree granting programs with an existing NIH- or Agency for Healthcare Research and Quality (AHRQ)-funded CER research or training program and the capacity to develop this degree granting program using existing tenure-track faculty. Award selection criteria were also established. The RFP was available for four annual cycles and a total of six academic Centers of Excellence were funded during that time: University of Washington (UW) and Johns Hopkins University (2012), University of Utah and Harvard TH Chan School of Public Health (2013), University of Maryland (2014), and University of Illinois at Chicago (2015). Each Center of Excellence tailors their program offerings to their institution-specific needs and resources. A short description of each is provided below (Table 1).
| Descriptor | University of Washington | Johns Hopkins University | Harvard University | University of Utah | University of Maryland | University of Illinois at Chicago |
|---|---|---|---|---|---|---|
| Year funded | 2012 | 2012 | 2013 | 2013 | 2014 | 2015 |
| School/department(s) | Pharmaceutical Outcomes Research & Policy Program (PORPP), School of Pharmacy; Department of Health Services, School of Public Health | Center for Health Services and Outcomes Research (CHSOR), School of Public Health | Program on Pharmaco-epidemiology and CER, TH Chan Harvard School of Public Health | Department of Pharmacotherapy, Division of Public Health/Department of Family Medicine, MS in Clinical Investigation, School of Medicine | Pharmaceutical Health Services Research, School of Pharmacy | Pharmacy Systems, Outcomes and Policy, School of Pharmacy |
| Program name | Center of Excellence in CER | CER Center of Excellence | CER Educational Center of Excellence | Technology Oriented CER (TOCER) | Patient-Centered Research for Outcomes, Effectiveness and Measurement (PROEM) | – |
| Primary educational offering | Graduate certificate in CER | Certificate in CER | Concentration within PhD/MS programs | Certificate in CER | Concentration within PhD/MS programs; mini-courses within existing online MS program; basic online training program | MS degree in CER |
| Training researchers or users of CER | Researchers | Researchers | Researchers | Researchers | Researchers and decision makers called to interpret and use CER/PCOR | Clinician researchers and employees of pharmaceutical firms |
| Number of credits | 16-18 | 21 | 40-80 | – | – | Core: 20 Elective: 12 |
CER: Comparative effectiveness research; CHSOR: Center for Health Services and Outcomes Research; MS: Masters; PCOR: Patient-centered outcomes research; PORPP: Pharmaceutical Outcomes Research & Policy Program; PROEM: Patient-Centered Research for Outcomes, Effectiveness and Measurement; TOCER: Technology oriented CER.
University of Washington (2012)
The University of Washington Center of Excellence in CER leverages existing expertise from within the multidisciplinary UW Centers for Comparative and Health System Effectiveness Alliance. The Center trains across the disciplines of epidemiology, biostatistics, health economics and outcomes research, informatics and health services research. The Comparative and Health System Effectiveness Alliance links capacity and resources across UW, Fred Hutchinson Cancer Research Center, Veterans Affairs Puget Sound Health System and Kaiser Permanente Washington (formerly Group Health) Research Institute. Led by EB Devine, L Garrison, and A Basu, faculty developed a CER Certificate of advanced study for graduate students already enrolled in the Pharmaceutical Outcomes Research and Policy Program or the Department of Health Services. The 16–18-credit certificate requires numerous prerequisites and students take advanced coursework in decision modeling/value of information, evidence synthesis (network meta-analysis), Bayesian statistics, and causal inference. Incorporation of a course in data science is currently under discussion. To date, ten students have completed their PhD having earned the CER certificate; two additional students are currently enrolled in the certificate program. A series of weekly CER seminars throughout each year provides a venue for students and faculty alike to present CER-related ‘works in progress’.
Johns Hopkins University (2012)
The Hopkins CER Center of Excellence is housed in the existing Center for Health Services and Outcomes Research, led by Director, A Wu and Associate Directors, J Segal and J Marstellar. J Segal leads the CER Center of Excellence. The centerpiece of the Hopkins' CER program is a 21-credit certificate in CER, which can either be completed as a stand-alone certificate online, or used to fulfill requirements for a CER track within the existing Masters of Public Health degree. The curriculum brings together coursework in health status and patient outcomes, epidemiology, informatics, research ethics, evidence synthesis, econometrics, pharmacoepidemiology, decision sciences and research methods. Two courses, developed with the new funding from the PhRMA Foundation, rounded out the offerings – an “Introduction to Comparative Effectiveness and Outcomes Research” and “Evaluating Quality Improvement and Patient Safety Programs”. The certificate can be completed online. The CER center also sponsors an ongoing series of seminars under the umbrella of the Center for Health Services and Outcomes Research.
Harvard TH Chan School of Public Health (2013)
The Harvard CER Educational Center of Excellence is led by S Hernandez-Diaz. As with UW and Hopkins, Harvard also has a long-standing presence in conducting research and offering training in epidemiology, biostatistics and health economics and outcomes research. The goal of this CER Educational Center is to provide an integrated training, including specialized curriculum with core and elective coursework and supervised research by multiple faculty at the Program on Pharmacoepidemiology and CER at the Harvard School of Public Health and at the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women's Hospital. The Dean's 2010 initiative in CER positioned Harvard well to receive the PhRMA Foundation award in 2013. Since then, the Doctoral and Master programs offer courses specifically developed to teach cutting-edge methodology for CER, and some existing courses were expanded to include more PCOR aspects. Over time, the theme of big data science has featured more prominently with the addition of courses on healthcare database analytics. Moreover, students can take advanced courses on related areas such as causal inference, decision science, clinical trials or meta-analysis. Harvard has also offered symposia on CER methods for therapeutic and preventive interventions, drug safety management and patient oriented benefit risk evaluation. Five graduate students have received direct support from the PhRMA Foundation grant; many others have benefitted from the program.
University of Utah (2013)
With their PhRMA Foundation support, the University of Utah established the “Technology-Oriented CER (TOCER) Training Program”. Led by D Brixner, to meet center objectives, the Utah faculty established a new course in healthcare data analytics, a second course in decision analysis and cost–effectiveness analysis, and a third in the use of secondary data sources for TOCER. They also enhanced an existing course in CER methods. Utah draws students form the Department of Pharmacotherapy, Division of Public Health in the Department of Family Medicine and from the Master of Science in Clinical Investigation Program, School of Medicine. Faculty at Utah have been active in the CER Collaborative, a joint initiative of the Academy of Managed Care Pharmacy (AMCP), the International Society for Pharmacoeconomics and Outcomes Research (ISPOR), and the National Pharmaceutical Council (NPC) [11]. The Collaborative has developed tools, resources and training materials to promote greater uniformity and transparency in the evaluation and use of evidence for coverage and healthcare decision-making. Three students are currently pursuing the CER certificate while completing their PhD in the Department of Pharmacotherapy.
University of Maryland (2014)
The University of Maryland launched the Patient-Centered Research for Outcomes, Effectiveness, and Measurement (PROEM) center with Dr Eleanor Perfetto as lead faculty. This Center of Excellence focuses on patient centeredness, and faculty strongly advocate for patient engagement as the first step in any CER activity. The PROEM trains both CER/PCOR scientists and decision-makers who interpret and use CER/PCOR, including patients and advocates. Program offerings include a CER/PCOR concentration within existing PhD and Masters (MS) programs (started in 2016), an annual summer institute, a basic, online CER/PCOR training program offering continuing education credits, and post-doctoral fellowships. Three new graduate courses were developed: Introduction to CER/PCOR, Quality and Quality Measurement, and Health Outcomes Measurement. Novel features of the PROEM Center of Excellence include a PCOR training program for rare-disease patient advocates [12], and collaboration with the currently AHRQ-funded, PATIENTS Program (PI: Mullins) [13] and US FDA-funded M-CERSI (PI: Polli) [14]. It also serves as the coordinating center for the CER collaborative' s online, continuing-education courses for its CER certificate program [11]. PROEM has benefitted from formal feedback provided by both internal and external advisory boards, comprised of colleagues from academia, industry, and the public sector, which have provided suggestions for improvement as PROEM's offerings were developed.
University of Illinois at Chicago (2015)
The sixth and final center to be funded was the University of Illinois at Chicago (UIC). Based in the Pharmacy Systems, Outcomes and Policy group, co-principal investigators Drs Glen Schumock and Simon Pickard lead this Center of Excellence. UIC's accomplishments featured the development of a new, online MS degree in CER. The purpose of the program is to provide individuals with the skills and knowledge relevant to conducting CER for application in the pharmaceutical and healthcare industries, and is intended primarily for individuals already working in a pharmaceutical or medical product company, government agency, or in a healthcare provider organization. Because it is 100% online, students can be located anywhere in the USA or abroad, and can finish the program at their own pace. The first class will matriculate in Fall 2017. The curriculum is comprised of 20 core and 12 elective credit hours (32 hours in total), and requires completion of a CER capstone project. Among its other aims, the UIC Center had a lead role in the second invitational conference in 2017. It conducted a weekly seminar series on CER and related research for faculty, graduate students, and other researchers. The center also convened workshops of clinical pharmacists and residents to train them in CER best practices. With direction from and external advisory board, the Center was successful in meeting its core aims.
First Invitational Conference (2014): “Curricular Advances for Patient-Centered Comparative Effectiveness Research”
In 2013, the directors of the first two CER Centers of Excellence that were funded (UW, Hopkins), joined with E Cannon and JP Gagnon to plan a national invitational conference intended to strengthen the proposed elements of a CER/PCOR curriculum and to allow the funded centers to share their experiences in implementing these in real-world and diverse academic settings. Funding for the conference was provided by a small conference grant awarded by AHRQ (PI: Segal), and a similar grant from PCORI (PI: Cannon). The PhRMA Foundation also supported the conference. Invited stakeholders were 120 key individuals from academia, educational accrediting bodies, industry, federal and state governments, professional societies, and the private sector; together, representing over 50 organizations. Attendees convened at the offices of the Pew Charitable Trust in January 2014 to address the five conference objectives: review existing competencies proposed for CER; describe existing curricula used to achieve these competencies; identify curricular enhancements; identify workforce needs; and discuss unique methodologic issues of CER unaddressed by related disciplines.
Over the two days of the conference, the directors of the five then funded, Centers of Excellence shared their curricular and training approaches, and leaders from AHRQ, PCORI, FDA, Centers for Medicare and Medicaid Services, industry and academia shared their perspectives. Keynote speakers addressed incorporating CER into policy-making (G Wilensky) and discussed the future of CER (M McClellan). Attendees broke into small groups to discuss the issues at hand. Conference findings included that CER/PCOR is an increasingly multidisciplinary science for which researchers must possess both a breadth of overall knowledge and sufficient depth in one or more areas of expertise. Identified gaps in methods training included patient engagement, decision sciences, dissemination and implementation science, and the use of big data.
CER centers of excellence strategic evaluation
In early 2015, the PhRMA Foundation solicited a strategic evaluation of the CER/PCOR Centers of Excellence Training Programs from Avalere Health [15]. Published in May 2015, findings from the report revealed that the Centers of Excellence have operationalized the objectives outlined in the PhRMA Foundation's original RFP. The report further suggested that faculty at the Centers of Excellence were appreciative of the support provided by this initiative, and vision of the Foundation for development of CER curriculum nationally, as this initiative still appears unique in the academic landscape. The flexibility afforded each Center of Excellence in crafting its program around current offerings, existing strengths and available resources has contributed to the success of the program, as opposed to a ‘one size fits all’ approach. All Centers of Excellence have been able to build on strong foundations and pre-existing programs in CER/PCOR. The report noted specifically that several Centers of Excellence have leveraged resources from the existing graduate programs to train researchers in CER; those that developed online programs focused primarily on training users of CER. As the Centers of Excellence have employed a variety of approaches, the combined offerings of all six centers meets, and often exceeds, the eight objectives outlined in the original RFP. A major finding of the report was that addressing the needs of users of CER remains an important gap. Report authors recommended the conduct of a follow-on conference, one that focused on training users of CER.
Second Invitational Conference (2017): “Comparative Effectiveness & Patient-Centered Outcomes Research: Enhancing Uptake & Use by Patients, Clinicians & Payers”
Funding for the second invitational conference was again provided by the PhRMA Foundation, this time with in-kind support from AMCP. The conference planning committee was led by the directors of the UIC Center of Excellence (Schumock and Pickard), assisted by Dr Perfetto (University of Maryland, MD, USA), along with E Cannon, JP Gagnon, a faculty liaison from the first conference (Devine) and a representative from AMCP (Saha). As the conference title makes clear, the conference focused on enhancing the uptake and use of CER/PCOR by patients, clinicians and payers. Details of the conference proceedings are found in the two companion papers in this series [16,17].
Discussion
In launching the CER Education and Training Initiative, the PhRMA Foundation has added to its long-standing and highly successful funding portfolio another landmark program. In sponsoring three seminal conferences and one conference report, and providing seed funding for six academic Centers of Excellence, the foundation has made significant inroads into moving the field of CER/PCOR forward for both research scientists who conduct CER/PCOR and clinicians and patients who use CER/PCOR.
In turn, the six Centers of Excellence each function within their own sphere of influence in training scientists and advancing knowledge and use of CER/PCOR. Each Center of Excellence offers similar coursework and extends its reach through seminars and symposia. Yet, each tailors its offerings to the unique strengths of the offering academic institution. Four Centers of Excellence enhance existing PhD and MS tracks with a CER/PCOR concentration, but do not offer degree-granting programs. Four programs focus on training researchers to conduct CER, two train clinician users of CER. Three centers offer their coursework online. Overall, the Centers of Excellence have largely met the intent and objectives of the PhRMA Foundation's initiative. Today, each center continues to train both those who conduct and use CER, continually evolving to meet the training needs of both in this dynamic healthcare environment. The identification of barriers, existing shortfalls in the use of CER, and suggestions for how to bridge these, were provided at the second conference. It is now up to the six centers, as well as many other academic centers, professional organizations and academic institutions to continue to meet these challenges.
The PhRMA Foundation initiative complements several other major CER/PCOR initiatives that were undertaken within this same timeframe. One effort was led by the members of the Clinical and Translational Science Award (CTSA) Workgroup for CER Education, Training and Workforce Development, of the National Center for Advancing Translational Sciences (NCATS) of the NIH. These investigators proposed preliminary competencies for CER. The group distinguished applied competencies (skills needed by those conducting CER) from Foundational competencies (those needed by both practitioners and users of CER) [18]. The list developed for the PhRMA Foundation's initiative is comprised of the same overarching categories as those developed by those involved in the NCATS initiative; indeed some of the scientists served on both groups.
A second initiative was led from the AHRQ Effective Healthcare Program and took the form of useful guidance. Two of these publications are titled, “Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide” [19] and “Methods Guide for Effectiveness and Comparative Effectiveness Reviews” [20]. More recently, a third initiative has been led by PCORI and has taken the form of the PCORI Methodology Standards, which has now evolved to include 48 standards covering 12 topical areas [21]; a companion academic curriculum has since been developed [22]. These AHRQ and PCORI guidance documents are widely used by research scientists who conduct CER/PCOR. The fourth initiative has been led by the AMCP. This professional society created a CER addendum to their existing AMCP format for Formulary Submissions [23]. The AMCP format is used to facilitate formulary decision-making on the part of Pharmacy & Therapeutics Committees. Relatedly, the AMCP/ISPOR/NPC CER Collaborative rounds out the list [11]. The AMCP format and the CER collaborative both focus on training users of CER/PCOR. Importantly, further efforts are needed to better integrate patients into CER/PCOR studies – from identifying research questions of meaning to patients to disseminating these findings in ways that are easily interpretable and accessible to patients.
While the field of PCOR is still in its relative infancy, its scope is enormous and it continues to expand. Much work remains to be done, and will involve many. For example, Academy Health now offers an annual conference on dissemination and implementation science [24]. In 2016, AHRQ launched the Patient-Centered Outcomes Research Clinical Decision Support Learning Network, to give patients and providers tools to make more informed decisions [25]. Clearly, one of the key priorities for the future is identify and prioritize areas where CER/PCOR evidence has the greatest potential to guide decision making and investments in healthcare.
Conclusion
Beginning in 2009, the PhRMA Foundation launched an ongoing, robust initiative to develop training and educational programs in the field of CER/PCOR. Now completed, while the results of this unique initiative are evident and have made a significant contribution to the national landscape of CER/PCOR, the work is ongoing and requires the efforts of numerous academic institutions, government programs, professional organizations and foundations.
Future perspective
In the past 8 years, methods for conducting CER have advanced and are now widely accepted for use in healthcare decision-making. PCOR is rapidly evolving, with the realization of the importance of the patient's perspective being increasingly recognized over time. With the era of ‘big data’ upon us, the evidence available to conduct CER will become voluminous, and methods to properly and appropriately analyze these data will continue to advance. The patient's voice will likely become ever more central to healthcare decision making. The field continues to evolve and expand, requiring the commitment of numerous academic centers, governmental programs, professional organizations and foundations to improve patient-centeredness and increase efficiencies in the healthcare system.
Comparative effectiveness research (CER) and patient-centered outcomes research (PCOR) took center stage with passage of the American Recovery and Reinvestment Act (2009) and Patient Protection and Affordable Care Act (2010), respectively.
The companion US$1.1 billion in funding (2009) prompted the launch of initiatives to train the scientific workforce capable of conducting and using CER/PCOR.
This report describes the unique initiative of the Pharmaceutical Manufacturers Research and Manufacturers Association of America (PhRMA) Foundation, which provided grant funding to seed six academic Centers of Excellence in CER/PCOR, and spearheaded and sponsored three national invitational conferences to advance the conduct and use of CER.
The six academic Centers of Excellence are positioned at the University of Washington, Johns Hopkins University, University of Utah, Harvard University, University of Maryland, and University of Illinois at Chicago. Each academic center built on their unique existing strengths to augment their training offerings in CER/PCOR.
Attendees at the first conference developed a model curriculum for CER/PCOR. Attendees at the second conference identified gaps in current methods training that include patient engagement, decision sciences, dissemination and implementation science, and the use of big data. They also identified the need for training users of CER/PCOR.
Attendees at the third and final conference identified an ongoing need to better understand what matters most to patients, and to provide, succinct, accessible and interpretable evidence that supports patient decision-making.
Through this unique initiative, the PhRMA Foundation has made significant contributions to creation of the scientific workforce that conducts and uses CER/PCOR and has highlighted improvements that can be made as the field continues to evolve.
Acknowledgements
We thank E Cannon, President of the PhRMA Foundation for her generous support and outstanding leadership, JP Gagnon for his commitment and vision, and our many colleagues who have helped to realize the vision of this national initiative in CER education, specifically A Basu (UW) and SH Diaz (PI: Harvard). We thank E Law (UIC) for his helpful comments on this manuscript.
Financial & competing interests disclosure
EB Devine, LP Garrison, E Perfetto, AS Pickard, GT Schumock, JB Segal and D Brixner are principal investigators for their respective CER Centers of Excellence, originally funded by the PhRMA Foundation. E Perfetto is an employee of the National Health Council, a multistakeholder membership organization that receives dues and sponsorship funding from a wide range of organizations. Members and sponsors are listed on the NHCouncil.org website. E Cannon is President of the PhRMA Foundation. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Medicare prescription drug, improvement, and modernization Act of 2003 (2003), 108–173. Public Law.
2.
H.R. 1. American Recovery and Reinvestment Act, of 2009 (2009), 111–115. Public Law.
3.
H.R. 3590. Patient Protection and Affordable Care Act (2010), 111–148. Public Law.
4.
Conway PH, Clancy C. Comparative-effectiveness research – implications of the Federal Coordinating Council's report. New Engl. J. Med. 361, 328–330 (2009).
• Provides an introduction and definition of comparative effectiveness research (CER).
5.
Sox HC, Greenfield S. Initial national priorities for comparative effectiveness research. Institute of Medicine. National Academies Press, Washington DC, USA (2009).
• Explains and lists the priority topics for CER.
6.
Patient-Centered Outcomes Research Institute (PCORI). www.pcori.org/about-us
• Describes Patient-Centered Outcomes Research Institute and provides a definition of patient-centered outcomes research.
7.
Lawrence W. Starting the conversation. Pharmacoepidemiol. Drug Saf. 20, 807–809 (2011).
8.
Pharmaceutical Research and Manufacturers Association of America Foundation. www.phrmafoundation.org/
9.
Murray MD. Curricular considerations for pharmaceutical comparative effectiveness research. Pharmacoepidemiol. Drug Saf. 20, 797–804 (2011).
• This is publication that emanated from the Pharmaceutical Research & Manufacturers Association Foundation's Inaugural CER Conference in 2009.
10.
Jones J, Hunter D. Consensus methods for medical and health services research. BMJ 311(7001), 376–380 (1995).
11.
• This is a national initiative to educate and train users of CER.
12.
PCOR Training: A Program for Rare Disease Patient Advocates. www.pcori.org/research-results/2015/pcor-training-program-rare-disease-patient-advocates
13.
University of Maryland PATIENTS Program. www.umaryland.edu/champions/patients-program/
14.
CERSI: Center of Excellence in Regulatory Science and Implementation. University of Maryland. www.cersi.umd.edu
15.
PhRMA Foundation – CER Centers of Excellence strategic evaluation. Key findings (2015). Avalere.com
16.
Schumock GT, Pickard AS. Comparative effectiveness and patient-centered outcomes research: enhancing uptake and use by patients, clinicians and payers. J Comp Eff Res. 7(2), (2018) (Epub ahead of print).
17.
Law E, Harrington R, Alexander GC, Saha S, Oehrlein E, Perfetto EM. Increasing uptake of comparative effectiveness and patient-centered outcomes research among stakeholders: insights from conference discussion. J Comp Eff Res. 7(2), (2018) (Epub ahead of print).
18.
Segal JB, Kapoor W, Carey T et al. For the workgroup on education, training, and workforce development of the clinical and translational science awards consortium key function committee for comparative effectiveness research. Preliminary competencies for comparative effectiveness research. Clin. Transl. Sci. 5, 476–479 (2012).
• This is an important contribution that highlights the need to train the CER workforce.
19.
Developing a Protocol for Observational Comparative Effectiveness Research: A User's Guide. Velentgas P, Dreyer NA, Nourjah P, Smith SR, Torchia MM (Eds). Agency for Healthcare Research and Quality, Rockville, MD, USA, AHRQ Publication No. 12(13)-EHC099 (January 2013). www.effectivehealthcare.ahrq.gov/Methods-OCER.cfm
20.
Methods guide for effectiveness and comparative effectiveness reviews. Agency for Healthcare Research and Quality, Rockville, MD, USA, AHRQ Publication No. 10(14)-EHC063-EF (2014). www.effectivehealthcare.ahrq.gov
21.
PCORI Methodology Standards. www.pcori.org/research-results/research-methodology/pcori-methodology-standards
• The Patient-Centered Outcomes Research Institute Methodology Standards have set the standard for methods to be used in CER.
22.
PCORI Methodology Standards Academic Curriculum. www.pcori.org/research-results/research-methodology/methodology-standards-academic-curriculum
23.
The AMCP Format for Formulary Submissions. Version 4.0. www.amcp.org/FormatV4/
24.
About D & I Science. Academy health. www.academyhealth.org/node/4536
25.
Patient-centered outcomes research clinical decision support learning network. Agency for Healthcare Research and Quality. https://healthit.ahrq.gov/ahrq-funded-projects/patient-centered-outcomes-research-clinical-decision-support-learning-network
Information & Authors
Information
Published In
Copyright
© 2018 Emily Beth Devine.
History
Received: 30 July 2017
Accepted: 20 November 2017
Published online: 21 February 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Nine years of comparative effectiveness research education and training: initiative supported by the PhRMA Foundation. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0059
Export citation
Select the citation format you wish to export for this article or chapter.