Elranatamab versus physician’s choice of treatment in patients with triple-class exposed/refractory multiple myeloma: an updated matching-adjusted indirect comparison
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Despite the availability of novel treatment options for patients with triple-class exposed/refractory multiple myeloma, there is a lack of consensus on the optimal regimen. A previous unanchored matching-adjusted indirect comparison (MAIC) of the MagnetisMM-3 (NCT04649359) and LocoMMotion (NCT04035226) study reported significant improvements in progression-free survival (PFS) and overall survival (OS) with elranatamab versus physician’s choice of treatment. Materials & methods: We conducted an updated MAIC based on more recent data (28.4 months for MagnetisMM-3). Following reweighting of MagnetisMM-3 individual patient data to match the LocoMMotion population, the effective sample size was 64 for PFS and 63 for OS in the base-case analysis. Results: Consistent with the original MAIC, significantly improved PFS (hazard ratio [HR] [95% confidence interval (CI)]: 0.32 [0.21, 0.50], p < 0.01) and OS (HR [95% CI]: 0.50 [0.33, 0.78], p < 0.01) were observed with elranatamab versus physician’s choice of treatment. The robustness of the results was demonstrated in sensitivity analyses in which missing baseline characteristics data for elranatamab were imputed. Conclusion: Overall, the findings of this study align with and add confidence to the conclusions of the previous MAIC that elranatamab is associated with significantly improved outcomes versus standard treatment, supporting the value to elranatamab for the treatment of patients with triple-class exposed/refractory multiple myeloma.
Plain language summary
What is this article about?
Multiple myeloma (MM) is a blood cancer that becomes harder to treat after multiple therapies stop working. Patients with triple-class exposed/refractory (TCE/R) MM have already received treatments from the three main drug classes used for MM, but their cancer has either not responded or has come back. These patients have very few treatment options and tend to have poor outcomes. Elranatamab is a type of treatment called a bispecific antibody, which helps the immune system recognize and attack MM cells in patients with TCE/R MM. This study indirectly compared elranatamab to a physician’s choice of treatment (PCT) based on data from a prospective study LocoMMotion. Since there are no clinical trials that directly compare elranatamab to PCT, a methodology known as matching-adjusted indirect comparison was conducted. This method helps account for differences between the patient groups in the two studies, making the comparison as fair and accurate as possible.
What were the results?
The results showed that elranatamab had significantly longer survival outcomes compared with PCT, based on longer-term follow-up data from the elranatamab clinical trial.
What do the results mean?
These findings suggest that elranatamab may be a more effective treatment option than current standard therapies for patients with TCE/R MM.
Multiple myeloma (MM) has a poor prognosis and remains incurable despite the availability of a range of treatment options; there is a need for new, effective treatments for patients who have been exposed to and/or become refractory to a proteasome inhibitor, an immunomodulatory drug, and a monoclonal antibody, also known as triple-class exposed/refractory (TCE/R) MM [1]. In recent years, novel treatment options have demonstrated promising efficacy for the treatment of patients with TCE/R MM in clinical trials, including chimeric antigen receptor T-cell therapies, as well as GPRC5D-targeted therapies [2–4]. Elranatamab, a bispecific antibody targeting B-cell maturation antigen (BCMA) and CD3 receptors, received FDA and EMA approval in 2023 for the treatment of adult patients with TCE/R MM based on the results of the MagnetisMM-3 trial (NCT04649359) [5,6]. However, there is currently no consensus on the optimal standard of care (SoC) treatment for patients with TCE/R MM.
To investigate the current SoC landscape, the prospective and non-interventional LocoMMotion (NCT04035226) study collected data on physician’s choice of treatment (PCT) for patients with TCE/R MM across Europe and the US for a follow-up period of 26.4 months [7]. A total of 91 unique SoC regimens were reported in a 2024 publication of the LocoMMotion study results, including corticosteroids, proteasome inhibitors, immunomodulatory drugs, alkylating agents, and anti-CD38 monoclonal antibodies [7].
In order to compare the relative efficacy of treatments for which no head-to-head trials have been conducted, matching-adjusted treatment comparisons (MAIC) can be applied [8]. MagnetisMM-3 is a single-arm trial and therefore it was not possible to create a connected network (i.e. no common comparator) between studies. Therefore, to compare the relative effectiveness of elranatamab in MagnetisMM-3 with PCT in LocoMMotion, we conducted an unanchored MAIC [9]. The results of the MAIC demonstrated that elranatamab was associated with significantly improved objective response rate, complete or stringent complete response rate, progression-free survival (PFS), and overall survival (OS) in comparison with PCT.
Since the original MAIC, longer-term data have been published for MagnetisMM-3 [10]. Therefore, to assess whether the results of the original MAIC are applicable to longer-term trial data from MagnetisMM-3, we conducted an updated MAIC.
Materials & methods
This analysis was conducted in R Studio in alignment with the example code from the National Institute for Health and Care Excellence Decision Support Unit 18 [8,11]. Data with a median follow-up of 26.4 months from LocoMMotion and 28.4 months from MagnetisMM-3 (versus 14.7 months for MagnetisMM-3 in the previous analysis [9]) were used to estimate PFS and OS hazard ratio (HR) with 95% confidence interval (CI) for elranatamab versus PCT.
MagnetisMM-3 individual patient data (BCMA naive, n = 123) were reweighted to match the LocoMMotion patient population (n = 248). Age, median time since diagnosis, International Staging System disease stage, extramedullary disease, number of prior lines of therapy, Eastern Cooperative Oncology Group performance status, creatinine clearance, penta-refractory status, and sex (OS only) were included following the previous unanchored MAIC study [9]. These variables were identified as key prognostic variables or effect modifiers based on the univariate Cox regressions of the MagnetisMM-3 patient data or the previous systematic literature review, and clinical experts further validated them. These key baseline demographics were subsequently adjusted to account for discrepancies between the study populations. A sensitivity analysis was conducted to increase the effective sample size by imputing missing baseline characteristics for elranatamab using random observations from the observed data from MagnetisMM-3. This allowed for the preservation of data distribution, as it imputed values included in the dataset with the assumption of missing at random.
Results
The results of this analysis are presented in Table 1, with Kaplan–Meier curves for the base-case analysis presented in Figure 1. The effective sample size for PFS and OS were 64 and 63, respectively, in the base-case analysis (70 and 69, respectively, in the sensitivity analysis). All HR p-values demonstrated significantly longer PFS and OS with elranatamab versus PCT, with two-sided p-values <0.01 in the base-case analysis. Results were also consistent across the naive and sensitivity analyses, with HRs significantly in favor of elranatamab compared with PCT.
| Outcome and analysis | ESS† | HR (95% CI) | p-value |
|---|---|---|---|
| PFS | |||
| Naive comparison | 123 | 0.42 (0.31, 0.57) | <0.01 |
| Base case | 64 | 0.32 (0.21, 0.50) | <0.01 |
| Sensitivity (imputation) | 70 | 0.29 (0.19, 0.43) | <0.01 |
| OS | |||
| Naive comparison | 123 | 0.66 (0.49, 0.89) | <0.01 |
| Base case | 63 | 0.50 (0.33, 0.78) | <0.01 |
| Sensitivity (imputation) | 69 | 0.48 (0.32, 0.72) | <0.01 |
†
ESS represents the number of independent unweighted individuals required to achieve the same precision as the weighted sample estimate. It was calculated as the square of the sum of weights divided by the sum of the squared weights. The ESS increased in the sensitivity analysis compared with the base case due to the imputation of the missing values.
CI: Confidence interval; ESS: Effective sample size; HR: Hazard ratio; OS: Overall survival; PCT: Physician’s choice of treatment; PFS; Progression-free survival.
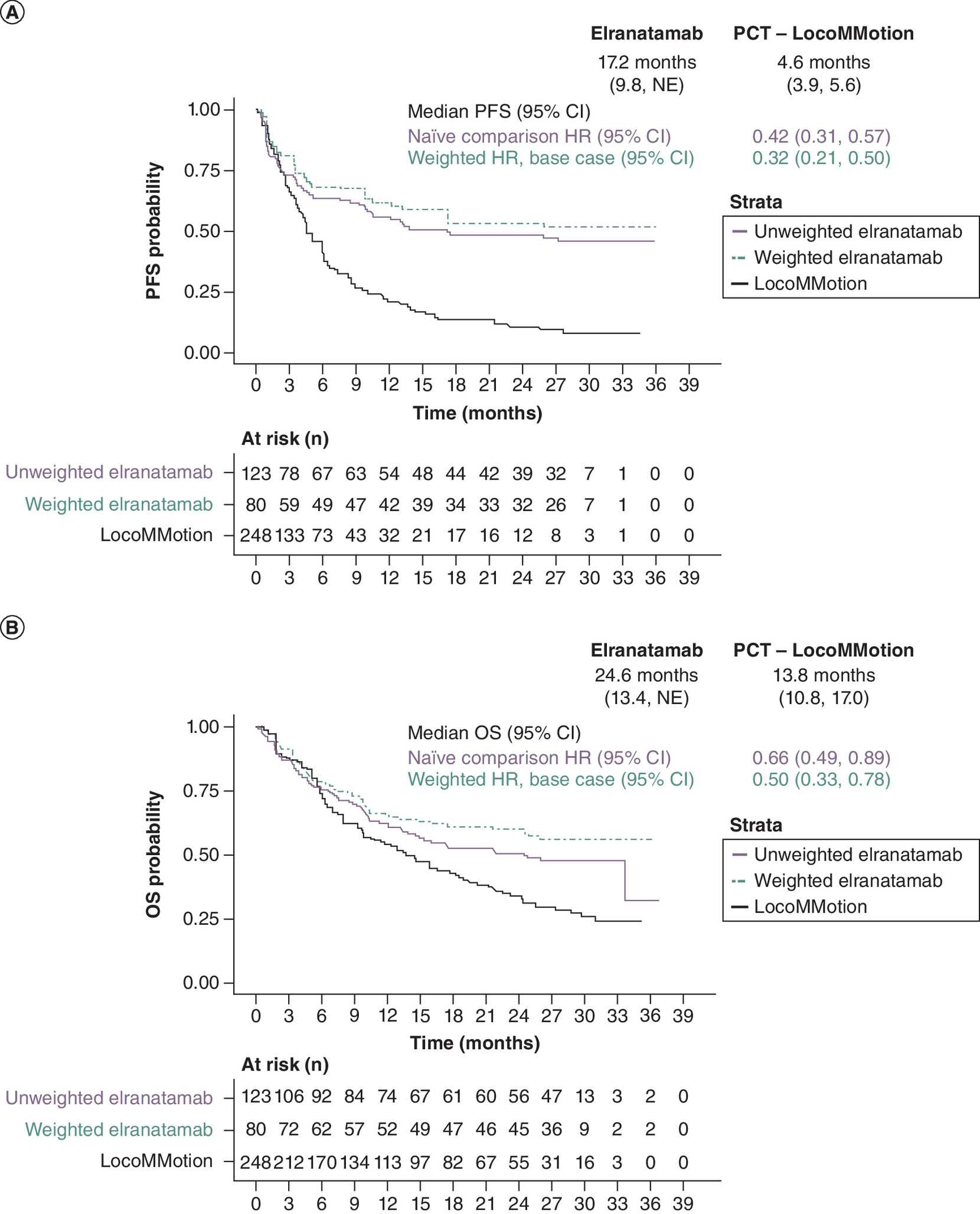
Figure 1. Adjusted Kaplan–Meier curves.
(A) progression-free survival and (B) overall survival in the base-case analysis. The number at risk shown for ‘weighted elranatamab’ was the weighted number of patients at risk over time, based on the weights directly derived from the MAIC.
CI: Confidence interval; HR: Hazard ratio; OS: Overall survival; NE: Not evaluable; PCT: Physician’s choice of treatment; PFS: Progression-free survival.
Discussion
Consistent with the previously published MAIC comparing the effectiveness of elranatamab with PCT among patients with TCE/R MM, this MAIC based on long-term (>28 months) follow-up data from MagnetisMM-3 demonstrated significantly improved PFS and OS with elranatamab versus PCT across all analyses. In comparison with the previously published results [9], these results show an increased precision through smaller CIs for the OS endpoint, and consistent results for the PFS endpoint.
Our indirect comparison confirmed the relative treatment effect of elranatamab in a clinical setting. However, real-world evidence on elranatamab remains limited, although we anticipate data will emerge in the near future. Recent data on the compassionate use of elranatamab in France are supporting its efficacy and safety in very heavily pretreated patients with aggressive and rapidly progressive disease [12].
Given the clinical importance of OS improvement, our results need to be contextualized alongside other novel BCMA-directed immunotherapies, including chimeric antigen receptor-T therapies, bispecific antibodies, and bispecific antibodies targeting GPRC5D, which have also demonstrated PFS and OS benefits in patients with TCE/R MM.
Our findings should be considered alongside the limitations previously described in the original MAIC, such as the limitation that it is only possible to adjust for baseline variables reported in both trials (e.g., cytogenetic risk was not reported in LocoMMotion, so it was excluded from the MAIC, leading to bias).
Despite the limitations of this study, this MAIC analysis provides insight into the comparative effectiveness of elranatamab versus physician’s choice of treatment as captured in the LocoMMotion study for patients with TCE/R MM, which is valuable considering the lack of clarity on the optimal strategy for this difficult-to-treat and poorly prognosed population.
Summary points
•
An unanchored matching-adjusted indirect comparison was used to evaluate elranatamab, based on the MagnetisMM-3 trial, versus physician’s choice of therapy from the LocoMMotion study in patients with triple-class exposed/refractory multiple myeloma.
•
This is an updated analysis of a previously published matching-adjusted indirect comparison, with longer follow-up data from MagnetisMM-3 (median follow-up time of 28.4 months).
•
After adjustment of key prognostic variables, elranatamab was shown to have a significantly longer overall survival and progression-free survival.
•
Compared with the previously published results, these findings demonstrate improved precision with smaller confidence intervals for the overall survival endpoint, along with consistent outcomes for the progression-free survival endpoint.
•
Potential bias remains due to the inability to adjust for prognostic variables not reported in both studies (e.g., cytogenetic risk).
Acknowledgments
The results of this study have, in part, been submitted as an abstract for presentation at the 66th American Society of Hematology Annual Meeting and Exposition 2024 (ASH 2024), 7–10 December 2024 in San Diego, CA, USA. The authors thank Sally Neath, Cytel UK, for Medical Writing assistance during the development of this manuscript.
Financial disclosure
This study was funded by Pfizer. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
I Mol and Y Hu report employment by Cytel, which received consulting fees from Pfizer related to the study. TW LeBlanc reports honoraria for consulting/advisory boards from AbbVie, Agilix, Agios/Servier, Astellas, AstraZeneca, Beigene, BlueNote, BMS/Celgene, CareVive, Flatiron, Genentech, GSK, Lilly, Meter Health, Novartis, and Pfizer; speaking-related honoraria from AbbVie, Agios, Astellas, BMS/Celgene, and Incyte; equity interest in Dosentrx (stock options in a privately held company); royalties from UpToDate; research funding from AbbVie, American Cancer Society, AstraZeneca, BMS, Deverra Therapeutics, Duke University, GSK, Jazz Pharmaceuticals, Leukemia and Lymphoma Society, National Institute of Nursing Research/National Institutes of Health, and Seattle Genetics. JC Cappelleri, H Chu, G Nador, D Aydin, IP Cruz, and P Hlavacek report employment by Pfizer and equity holding in Pfizer. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing assistance was provided by Sally Neath, Cytel UK, funded by Pfizer.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them and that the use of these shared data is in accordance with the terms (if any) agreed upon their receipt. The source of these data is: MagnetisMM-3 (NCT04649359). Upon request, and subject to review, Pfizer will provide the data that support the findings of this study. Subject to certain criteria, conditions, and exceptions, Pfizer may also provide access to the related individual de-identified participant data. See https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Mikhael J. Treatment options for triple-class refractory multiple myeloma. Clin. Lymphoma Myeloma Leuk. 20(1), 1–7 (2020).
2.
Munshi NC, Anderson LD Jr, Shah N et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N. Engl. J. Med. 384(8), 705–716 (2021).
3.
Berdeja JG, Madduri D, Usmani SZ et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase Ib/II open-label study. Lancet 398(10297), 314–324 (2021).
4.
Chari A, Minnema MC, Berdeja JG et al. Talquetamab, a T-cell-redirecting GPRC5D bispecific antibody for multiple myeloma. N. Engl. J. Med. 387(24), 2232–2244 (2022).
5.
Lesokhin AM, Tomasson MH, Arnulf B et al. Elranatamab in relapsed or refractory multiple myeloma: phase II MagnetisMM-3 trial results. Nat. Med. 29(9), 2259–2267 (2023).
• Presents the study results of MagnetisMM-3 based on the 15-month data cut off.
6.
US Food and Drug Administration. Highlights of prescribing information. ELREXFIO (elranatamab-bcmm) injection, for subcutaneous use. Initial US approval: 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761345s000lbl.pdf
7.
Mateos MV, Weisel K, De Stefano V et al. LocoMMotion: a study of real-life current standards of care in triple-class exposed patients with relapsed/refractory multiple myeloma – 2-year follow-up (final analysis). Leukemia 38(12), 2554–2560 (2024).
•• Presents the study results of the LocoMMotion study based on the 2-year follow-up data.
8.
Phillippo D, Ades T, Dias S, Palmer S, Abrams KR, Welton N. NICE DSU Technical Support Document 18: methods for population-adjusted indirect comparisons in submissions to NICE. (2016). Available from: https://research-information.bris.ac.uk/ws/portalfiles/portal/94868463/Population_adjustment_TSD_FINAL.pdf
9.
Mol I, Hu Y, LeBlanc TW et al. A matching-adjusted indirect comparison of the efficacy of elranatamab versus physician's choice of treatment in patients with triple-class exposed/refractory multiple myeloma. Curr. Med. Res. Opin. 40(2), 199–207 (2024).
•• Presents the results of the previous matching-adjusted indirect comparison conducted between elranatamab versus physician’s choice of treatment based on the LocoMMotion study.
10.
Tomasson MH, Iida S, Niesvizky R et al. Long-term survival and safety of elranatamab in patients with relapsed or refractory multiple myeloma: update from the MagnetisMM-3 study. Hemasphere 8(7), e136 (2024).
•• Presents the longer follow-up study results of the MagnetisMM-3 trial.
11.
Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for population-adjusted indirect comparisons in health technology appraisal. Med. Decis. Making 38(2), 200–211 (2018).
12.
Malard F, Bobin A, Labopin M et al. Elranatamab monotherapy in the real-word setting in relapsed-refractory multiple myeloma: results of the French compassionate use program on behalf of the IFM. Blood Cancer J. 14(1), 219 (2024).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 18 December 2024
Accepted: 19 March 2025
Published online: 7 April 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Elranatamab versus physician’s choice of treatment in patients with triple-class exposed/refractory multiple myeloma: an updated matching-adjusted indirect comparison. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0236
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Dawud Ellayan, Therapy update: An introduction to the pharmacology, safety, and efficacy of bispecific antibodies in relapsed or refractory multiple myeloma, American Journal of Health-System Pharmacy, 10.1093/ajhp/zxag203, (2026).
- Shahrier Hossain, Giada Bianchi, Elranatamab: A novel B-cell maturation T-cell engager, Human Vaccines & Immunotherapeutics, 10.1080/21645515.2026.2694852, 22, 1, (2026).
- Finn Segers, Michel Delforge, Antibody-Drug Conjugates, T-Cell Engager Bispecific Antibodies and Chimeric Antigen Receptor T Cells for Multiple Myeloma: What’s the Current Status?, Targeted Oncology, 10.1007/s11523-025-01189-7, (2026).