Healthcare costs and treatment patterns associated with glucagon-like peptide 1 receptor agonist use among patients with metabolic dysfunction-associated steatohepatitis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: While only recently approved for the treatment of metabolic dysfunction-associated steatohepatitis (MASH), many patients with MASH have taken glucagon-like peptide-1 receptor agonists (GLP-1 RAs) for the treatment of comorbid Type 2 diabetes (T2D) or obesity. This real-world study evaluated treatment patterns, weight loss, healthcare resource utilization, and costs among patients with MASH who initiated GLP-1 RAs. Materials & methods: In a linked electronic health records (Veradigm Network EHR) and claims (Komodo Health) dataset, we identified adults (≥18 years old) with a MASH diagnosis who initiated GLP-1 RA treatment (1 July 2018 to 30 April 2023; index date = date of the first GLP-1 RA claim). Patients with other causes of liver disease or severe complications from MASH were excluded. We required ≥12 months of continuous enrollment pre- (baseline) and post-index (follow-up). Patients were stratified into high and low-dose subgroups. We also identified a comparator cohort of patients who initiated a different class of T2D medication (DPP4, SGLT2, or sulfonylurea) during the same time period. We captured patient characteristics, change in BMI, GLP-1 RA treatment patterns, liver-related events, healthcare utilization, and costs. Results: We identified 10,316 patients with MASH who initiated a GLP-1 RA (high dose: 2043 [19.8%]; low dose: 8273 [80.2%]) and 2915 who initiated a non-GLP-1 RA T2D medication. GLP-1 RA users were 52.7 years old and 64.3% female. A 5.8% decrease in the percentage of patients with class III obesity was observed among GLP-1 RA users (10.7% among high-dose users; 0.8% among non-users). Overall, 56.1% of GLP-1 RA users discontinued during the 12-month follow-up. Total costs among GLP-1 RA users and non users were $20,912 and $19,019 in the baseline period and $27,586 and $24,917 in the follow-up period, respectively. Medical costs among GLP-1 RA users were $16,293 (baseline) and $16,886 (follow-up). Results were similar for high and low-dose subgroups. Conclusion: Although some patients with MASH on GLP-1 RAs, particularly those taking higher dosages, may achieve weight loss, outcomes remain suboptimal with frequent discontinuation and high healthcare costs. Real-world GLP-1 RA utilization may be insufficient for resolving chronic metabolic issues, including MASH.
Plain language summary: An analysis of costs and medication usage among people with metabolic dysfunction-associated steatohepatitis who were prescribed glucagon-like peptide-1 receptor agonists
What is this article about?
Metabolic dysfunction-associated steatohepatitis (MASH) is a liver disease that gets worse over time. MASH can lead to serious complications such as liver failure. Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are used to treat obesity and Type 2 diabetes, which are common among people with MASH. This article is about the usage of GLP-1 RAs among people diagnosed with MASH. We looked at patient characteristics, BMI, patterns of medication treatment, reasons for discontinuation and changes in healthcare use and costs after starting GLP-1 RA. We also captured similar data for people who started a different Type 2 diabetes treatment to provide additional context.
What were the results?
People with MASH who took GLP-1 RA tended to lose weight, measured as a decrease in the percentage of patients with a very high BMI (≥40). This was not observed in people who started a different Type 2 diabetes treatment. More than half of people who started GLP-1 RAs stopped treatment for at least 45 days within 1 year. Roughly half of people who stopped treatment did not restart treatment. Side effects were the most common reason for stopping treatment. Total healthcare costs were $27,586, and nonmedicine-related costs were $16,886 in the year after starting treatment.
What do the results mean?
GLP-1 RA may be effective in promoting weight loss among people with MASH, but these medications may not address other issues among people with MASH as healthcare use and costs remain high.
Metabolic dysfunction-associated steatohepatitis (MASH) is the inflammatory subtype of metabolic dysfunction-associated steatotic liver disease (MASLD) [1,2]. MASH is associated with progressive fibrosis of the liver, which can lead to cirrhosis, hepatocellular cancer and end-stage liver disease requiring liver transplantation [2]. While the overall estimated prevalence of MASH is 3–5% [3], this rises to 37% among patients with a comorbid diagnosis of Type 2 diabetes and 33% among patients who are overweight or obese [4,5]. The combination of an aging population with the dual epidemics of Type 2 diabetes and obesity resulted in a projected doubling of the prevalence of MASH between 2015 and 2030 [6].
Weight loss, through a combination of a healthy diet and regular exercise, is the recommended first-line therapy for MASLD [7–9]. Studies have shown dose-dependent improvements in markers of liver damage with increasing weight loss, with a ≥5% reduction being associated with reduced liver lipid content, a 7–10% reduction being associated with reduced inflammation, and a ≥10% reduction being associated with improvements in fibrosis [10–12]. However, this degree of weight loss is difficult to achieve and maintain with behavioral changes alone [12].
First approved in 2005 for the treatment of Type 2 diabetes [13], several glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and other incretin mimetics have demonstrated efficacy in promoting weight loss, particularly when prescribed at higher dosages [14]. Improvements in cardiovascular outcomes among patients with Type 2 diabetes have been well characterized [15,16], and recent clinical trials have demonstrated promising results on steatohepatitis resolution without worsening of fibrosis [17–20].
While no GLP-1 RAs were approved for the treatment of MASH at the time this study was conducted, current guidelines for the management of MASH recommend prescribing GLP-1 RAs in patients who have an approved indication for treatment, namely, comorbid Type 2 diabetes or obesity [7–9]. The primary objective of this study was to evaluate baseline characteristics, treatment patterns, changes in BMI, healthcare resource utilization and healthcare costs among patients with MASH initiating treatment with GLP-1 RAs.
Materials & methods
Data sources & ethical compliance
This retrospective, observational cohort study leveraged electronic health records (EHR) from the Veradigm Network EHR linked to insurance claims data spanning 1 July 2017, through 30 April 2024. The deidentified linked dataset was prepared by the data providers, and the proprietary methods used to generate the dataset from the source data were not disclosed to the authors.
The linked dataset only contains deidentified data as per the de-identification standard defined in Section §164.514(a) of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy Rule. Because this study used only deidentified patient records, it is no longer subject to the HIPAA Privacy Rule and is therefore exempt from Institutional Review Board approval. This study was conducted in compliance with the Declaration of Helsinki and followed the STROBE guidelines for reporting observational research studies [21].
Study cohorts
Using structured EHR and claims data, we identified two cohorts of patients with MASH. The first was the main study cohort, comprised of individuals starting a GLP-1 RA, and the second was a comparator cohort, comprised of individuals initiating a different class of diabetes treatment (dipeptidyl peptidase 4 [DPP4] inhibitor, sodium-glucose cotransporter-2 [SGLT2] inhibitor, or sulfonylurea). In line with other investigators, these comparators were selected because, like GLP-1 RA, they are often positioned as add-on therapies in the treatment of Type 2 diabetes [22]. The purpose of the comparator cohort was to provide additional context for interpreting the cost outcomes, as healthcare costs among MASH patients vary by comorbidity burden [23,24].
To do this, we identified individuals with a claim for a GLP-1 RA, DPP4, SGLT2, or sulfonylurea between 1 July 2018 and 30 April 2023, as well as a medical claim or EHR record with the International Classification of Diseases, 10th edition, Clinical Modification diagnosis K75.81 before their index date. The K75.81 code has been used by clinicians to code for both MASH and its predecessor term, nonalcoholic steatohepatitis [25,26]. For individuals with a GLP-1 RA prescription, the index date was the date of the earliest GLP-1 RA claim between 1 July 2018 and 30 April 2023. For all other individuals, the index date was the date of the earliest claim for a new qualifying class of antidiabetic medication (DPP4, SGLT2, or sulfonylurea) between 1 July 2018 and 30 April 2023. To create a meaningful index date, patients could only index on a medication if they had no prior claims for a medication in that class at any time in their available data.
We excluded individuals who had a claim for a GLP-1 RA anytime before the index date or were less than 18 years old on the index date. Patients were excluded if they had a diagnosis of viral hepatitis, alcoholism or alcoholic liver disease, opioid disorders, Type 1 diabetes, gestational diabetes or bariatric surgery at any time in their available data or if they had a diagnosis of cirrhosis, decompensated cirrhosis, ascites, encephalopathy, varices, liver transplant or hepatic cell carcinoma at any time before the index date. To ensure that the opportunity for data capture was consistent across individuals in the study, we also required a minimum of 12 months of continuous enrollment in claims before (baseline period) and after (follow-up period) the index date. The codes used in cohort selection are reported in Supplementary Table 1.
The GLP-1 RA cohort was further segmented into two groups based on GLP-1 RA dose intensity: high or low. The cutoffs used to determine the dose intensity of each GLP-1 RA are reported in Supplementary Table 2.
Time periods
The index date was the first claim for a patient’s index medication. The baseline period was the 12 months preceding the index date, and the follow-up period was the 12 months following and inclusive of the index date. Created a 24-month analytic period for each patient. All study variables were captured using only data from the 24-month analytic period.
Study variables
Demographic characteristics, including age, sex, race, ethnicity, geographic region, insurance type and year of index, were measured on the index date. Where height and weight values were available in the EHR, BMI was calculated for the baseline and follow-up periods. Patients were categorized by BMI using cutoffs defined by the US Centers for Disease Control and Prevention: underweight (BMI <18.5), healthy weight (18.5 ≤ BMI <25), overweight (25 ≤ BMI <30), obese (30 ≤ BMI), class 1 obesity (30 ≤ BMI <35), class 2 obesity (35 ≤ BMI <40) or class 3 obesity (40 ≤ BMI) [27]. Other clinical characteristics were measured during the 12-month baseline period and included the Charlson Comorbidity Index (CCI) [28], the Diabetes Complications Severity Index (DCSI) [29] and its individual components, cardiovascular-related conditions (cardiovascular disease, coronary artery disease, Type 2 diabetes, hypercholesterolemia, hyperlipidemia, primary hypertension and metabolic syndrome [by diagnosis code]), and related treatments (antidiabetics [excluding GLP-1 RA], antihypertensives, statin [high and low/moderate]) [30]. The DCSI and individual components are only reported among the subset of patients with a diagnosis of Type 2 diabetes in the 12-month baseline period. New diagnoses of cirrhosis, decompensated cirrhosis, liver transplant and hepatic cell carcinoma were captured in the 12-month follow-up period. Diagnoses were captured using both EHR and claims data.
GLP-1 RA treatment patterns, including adherence, discontinuation and days of use, were captured in the 12-month follow-up period. For adherence, we measured the proportion of days covered (PDC), which was calculated by dividing the days' supply of all GLP-1 RAs during the follow-up period by 365. PDC was capped at 1. Patients with a PDC ≥0.8 were considered adherent. For discontinuation, we captured the time to discontinuation using both a 45-day allowable gap and a 60-day allowable gap. Changes in dosing or switches to a new GLP-1 RA were not considered discontinuation events unless they coincided with a gap in therapy. We also captured whether patients restarted a GLP-1 RA after discontinuation and the time to restart. Medication usage and treatment patterns were captured using only claims data.
We captured all-cause healthcare utilization and costs in the 12-month baseline and follow-up periods. Utilization and costs were measured using medical and pharmacy claims data, and captured all prescriptions, services, procedures, facility and other medical fees billed to the insurance provider. We did not calculate proxy costs for encounters that occurred in the EHR but did not have a corresponding claim. Costs are reported per-person per-year and were adjusted to 2024 US dollars using the medical care component of the Consumer Price Index.
Diagnoses were captured using both EHR and claims data. Medications, treatment patterns, healthcare utilization and cost data were captured using only claims data.
Exploratory analysis
We conducted an exploratory analysis of reasons for GLP-1 RA discontinuation using data extracted from clinical notes in the EHR. Using only the EHR data, we identified patients with ≥1 GLP-1 RA prescription, a documented end date of treatment, and a clinical note on the end date. We restricted to patients who were ≥18 years old and had a diagnosis of MASH. We also excluded patients with cirrhosis, Type 1 diabetes or gestational diabetes at any time. We identified notes with the name of a GLP-1 RA and one of several stop terms (stop, stopped, discontinued, discontinue, discontinuation, d/c, gap, quit), and snippets of 150 characters from the deidentified free text fields were examined for common reasons for discontinuation. A subanalysis was performed on patients stratified by time to discontinuation: ≤6 months or >6 months.
Data analysis
Continuous measures are presented as means and standard deviations (SD), while categorical measures are presented as counts and percentages. For cost variables, we also report the median and interquartile range. All results are reported descriptively. The non-GLP-1 RA cohort was included to provide context for interpreting the results of the GLP-1 RA cohort. No direct comparisons are made between these two cohorts. Descriptive statistics were generated using SAS V9.4.
Results
We identified 10,316 individuals with MASH who newly initiated a GLP-1 RA and an additional 2915 individuals with MASH who newly initiated a different class of diabetes medication (DPP4, SGLT2 or sulfonylurea). Among those who initiated a GLP-1 RA, 2043 (19.8%) were on a high dose, and 8273 (80.2%) were on a low dose (Figure 1).

Figure 1. Cohort Identification.
aThe index date for glucagon-like peptide-1 receptor agonists (GLP-1) users was the earliest GLP-1 RA prescription between 1 July 2018 and 30 April 2023. For people without a GLP-1 RA prescription, the index date was the earliest claim for a new dipeptidyl peptidase (DPP4) inhibitor, sodium-glucose cotransporter-2 (SGLT2) inhibitor or sulfonylurea prescription between 1 July 2018 and 30 April 2023.
EHR: Electronic health record; GLP-1 RA: Glucagon-like peptide-1 receptor agonist; MASH: Metabolic dysfunction-associated steatohepatitis.
Patients with MASH in the GLP-1 RA cohort were, on average, 52.7 (SD: 11.3) years old and 64.3% female (Table 1). Among those in the GLP-1 RA cohort, 59.4% were White, 45.1% lived in the South and 70.5% had commercial insurance. By contrast, patients in the non-GLP-1 RA cohort were, on average, 57.7 (SD: 12.1) years old, 53.5% female, 50.8% White, 36.2% in the South and 51.9% on commercial insurance. Among patients on a high-dose GLP-1 RA, 83.3% had commercial insurance, and only 8.9% were insured through Medicaid.
| GLP-1 RA non-users | GLP-1 RA users | |||
|---|---|---|---|---|
| Any dose | High dose | Low dose | ||
| n = 2915 | n = 10,316 | n = 2043 | n = 8273 | |
| Age, mean (SD) | 57.7 (12.1) | 52.7 (11.3) | 50.3 (10.7) | 53.3 (11.3) |
| Female, n (%) | 1558 (53.5) | 6637 (64.3) | 1358 (66.5) | 5279 (63.8) |
| Race, n (%) | ||||
| Asian | 229 (7.9) | 417 (4.0) | 76 (3.7) | 341 (4.1) |
| African–American/Black | 133 (4.6) | 423 (4.1) | 81 (4.0) | 342 (4.1) |
| Other | 473 (16.2) | 1397 (13.5) | 244 (11.9) | 1153 (13.9) |
| White | 1482 (50.8) | 6126 (59.4) | 1260 (61.7) | 4866 (58.8) |
| Unknown/not reported | 598 (20.5) | 1953 (18.9) | 382 (18.7) | 1571 (19.0) |
| Ethnicity, n (%) | ||||
| Hispanic | 278 (9.5) | 776 (7.5) | 127 (6.2) | 649 (7.8) |
| Non-Hispanic or unknown | 2637 (90.5) | 9540 (92.5) | 1916 (93.8) | 7624 (92.2) |
| Geographic region, n (%) | ||||
| North East | 608 (20.9) | 1849 (17.9) | 327 (16.0) | 1522 (18.4) |
| Midwest | 511 (17.5) | 1913 (18.5) | 379 (18.6) | 1534 (18.5) |
| South | 1054 (36.2) | 4653 (45.1) | 986 (48.3) | 3667 (44.3) |
| West | 672 (23.1) | 1672 (16.2) | 305 (14.9) | 1367 (16.5) |
| Other/unknown | 70 (2.4) | 229 (2.2) | 46 (2.3) | 183 (2.2) |
| Insurance type, n (%) | ||||
| Commercial | 1514 (51.9) | 7268 (70.5) | 1702 (83.3) | 5566 (67.3) |
| Medicare | 793 (27.2) | 1471 (14.3) | 158 (7.7) | 1313 (15.9) |
| Medicaid | 602 (20.7) | 1565 (15.2) | 181 (8.9) | 1384 (16.7) |
| Other/unknown | 6 (0.2) | 12 (0.1) | 2 (0.1) | 10 (0.1) |
| Year of index date, n (%) | ||||
| 2018 | 222 (7.6) | 434 (4.2) | 29 (1.4) | 405 (4.9) |
| 2019 | 485 (16.6) | 1130 (11.0) | 77 (3.8) | 1053 (12.7) |
| 2020 | 605 (20.8) | 1401 (13.6) | 66 (3.2) | 1335 (16.1) |
| 2021 | 741 (25.4) | 2612 (25.3) | 252 (12.3) | 2360 (28.5) |
| 2022 | 749 (25.7) | 3881 (37.6) | 1250 (61.2) | 2631 (31.8) |
| 2023 | 113 (3.9) | 858 (8.3) | 369 (18.1) | 489 (5.9) |
GLP-1 RA: Glucagon-like peptide-1 receptor agonist; SD: Standard deviation.
Mean CCI ranged from 1.5 to 1.8, and mean DSCI ranged from 0.9 to 1.2, depending on the cohort (Table 2). In all cohorts, the most common DCSI dimensions were neuropathy (18.2%–23.3%) and nephropathy (12.5–14.8%). Overall, 75.3% of the GLP-1 RA cohort and 80.3% of the non-GLP-1 RA cohort had a diagnosis of cardiovascular disease, while 75.6% and 86.7% had a diagnosis of Type 2 diabetes in the 12-month baseline period. Among those on a high-dose GLP-1 RA, 66.9% had a baseline diagnosis of cardiovascular disease, and 47.0% had a baseline diagnosis of Type 2 diabetes. While hyperlipidemia and primary hypertension were present in 60.4%–74.4% of each cohort, less than 10% of any cohort had a diagnosis code for metabolic syndrome.
| GLP-1 RA non-users | GLP-1 RA users | |||
|---|---|---|---|---|
| Any dose | High dose | Low dose | ||
| n = 2915 | n = 10,316 | n = 2043 | n = 8273 | |
| CCI, mean (SD) | 1.8 (1.7) | 1.7 (1.6) | 1.5 (1.5) | 1.7 (1.6) |
| DCSI†, mean (SD) | 1.2 (1.5) | 1.0 (1.4) | 0.9 (1.3) | 1.0 (1.4) |
| DCSI conditions†, n (%) | ||||
| Retinopathy/ophthalmic | 197 (7.8) | 630 (8.1) | 63 (6.6) | 567 (8.3) |
| Nephropathy | 375 (14.8) | 1017 (13.0) | 120 (12.5) | 897 (13.1) |
| Neuropathy | 484 (19.2) | 1770 (22.7) | 175 (18.2) | 1595 (23.3) |
| Cerebrovascular disease | 20 (0.8) | 46 (0.6) | 3 (0.3) | 43 (0.6) |
| Cardiovascular | 306 (12.1) | 680 (8.7) | 80 (8.3) | 600 (8.8) |
| Peripheral vascular disease | 300 (11.9) | 699 (9.0) | 81 (8.4) | 618 (9.0) |
| Metabolic | 46 (1.8) | 189 (2.4) | 26 (2.7) | 163 (2.4) |
| CV-related conditions, n (%) | ||||
| Cardiovascular disease | 2341 (80.3) | 7768 (75.3) | 1367 (66.9) | 6401 (77.4) |
| Coronary artery disease | 67 (2.3) | 115 (1.1) | 13 (0.6) | 102 (1.2) |
| Diabetes, Type 2 | 2526 (86.7) | 7803 (75.6) | 960 (47.0) | 6843 (82.7) |
| Hypercholesterolemia | 484 (16.6) | 1749 (17.0) | 324 (15.9) | 1425 (17.2) |
| Hyperlipidemia | 2124 (72.9) | 7121 (69.0) | 1252 (61.3) | 5869 (70.9) |
| Hypertension(primary) | 2168 (74.4) | 7179 (69.6) | 1233 (60.4) | 5946 (71.9) |
| Metabolic syndrome | 77 (2.6) | 719 (7.0) | 184 (9.0) | 535 (6.5) |
| Related treatments, n (%) | ||||
| Any antidiabetic (except GLP-1 RA) | 2153 (73.9) | 7784 (75.5) | 995 (48.7) | 6789 (82.1) |
| Any antihypertensive | 2168 (74.4) | 7530 (73.0) | 1305 (63.9) | 6225 (75.2) |
| Statin | ||||
| Low/moderate dose‡ | 1187 (40.7) | 3766 (36.5) | 543 (26.6) | 3223 (39.0) |
| High dose‡ | 592 (20.3) | 2041 (19.8) | 319 (15.6) | 1722 (20.8) |
†
The Diabetes Complications Severity Index (DCSI) and components were only reported among patients with evidence of a Type 2 diabetes diagnosis.
‡
Statin dose intensity was calculated using peak average daily dose for any prescribed statin, with thresholds aligned with Quek, et al. [26]. High doses were defined as follows: atorvastatin ≥30 mg daily; rosuvastatin ≥15 mg daily; simvastatin ≥60 mg daily.
CCI: Charlson Comorbidity Index; CV: Cardiovascular; GLP-1 RA: Glucagon-like peptide-1 receptor agonists; SD: Standard deviation.
Baseline use of antihypertensive and non-GLP-1 RA antidiabetic medications mirrored the incidence of primary hypertension and Type 2 diabetes, respectively (Table 2). In the baseline period, 36.5% of the GLP-1 RA cohort and 40.7% of the non-GLP-1 RA cohort had claims for low to moderate-dose statins, while 19.8% and 20.3% had claims for a high-dose statin.
Among the roughly a third of patients with a BMI value, 86.6% of the overall GLP-1 RA cohort had a BMI indicative of obesity in the baseline period, and 80.1% had a BMI indicative of obesity in the follow-up period (Figure 2). In the subset of patients who received a high-dose GLP-1 RA, mean (SD) BMI was 36.1 (4.5) in the baseline period and 34.6 (5.0) in the follow-up period (Supplementary Table 3). In this subgroup, the percentage of patients with class III obesity decreased by 10.7 percentage points from 36.6% to 25.9%, while the percentage of patients who were overweight increased by 8.6 percentage points from 7.3% to 15.9% suggesting an overall shift in BMI.
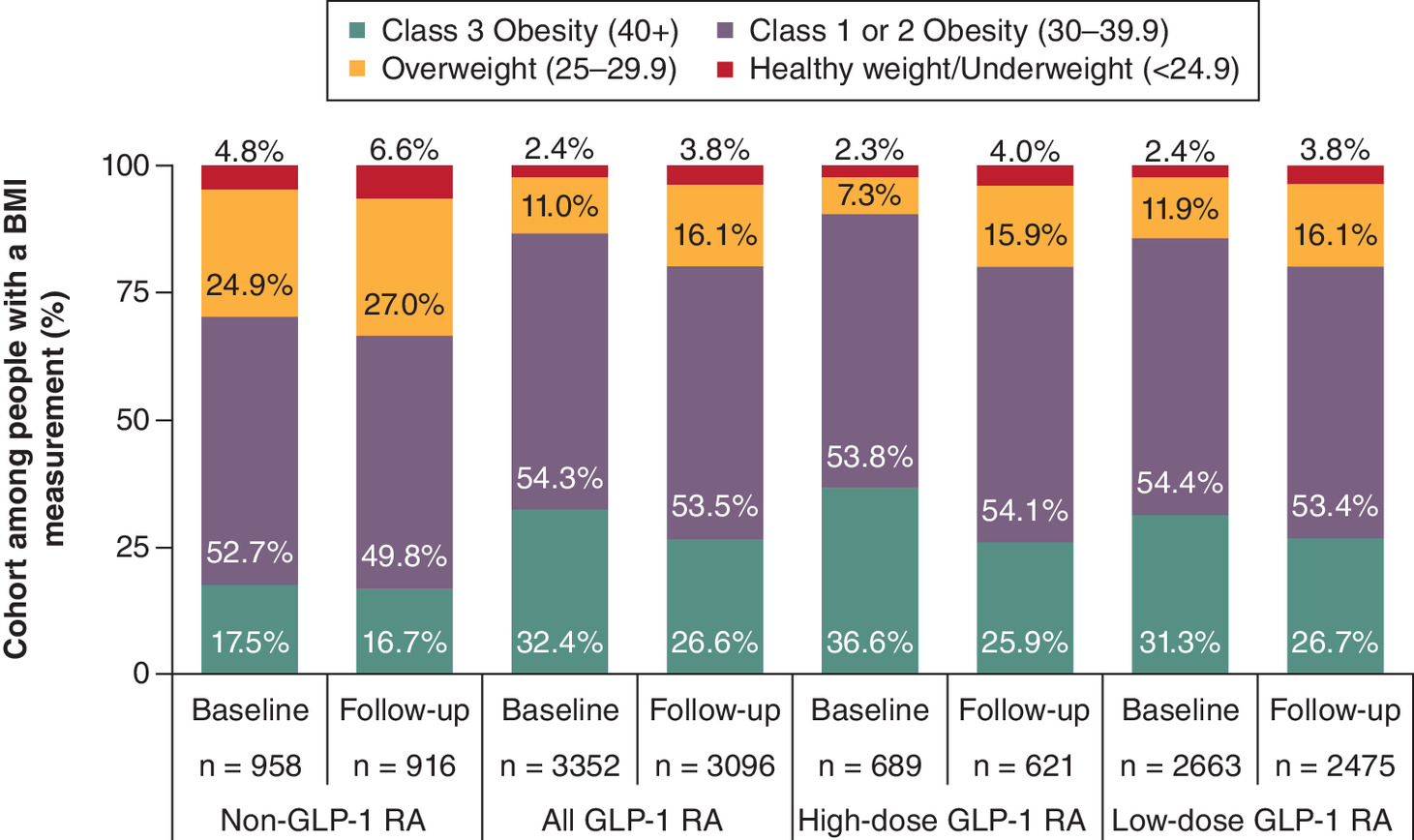
Figure 2. BMI in the baseline and follow-up periods.
GLP-1 RA: Glucagon-like peptide-1 receptor agonists.
To assess the frequency of costly liver-related complications in the follow-up period we also explored incident liver-related diagnoses in the follow-up period (Supplementary Table 4). During the 12-month follow-up period, 1.8% of the non-GLP-1 RA cohort had an incident diagnosis of cirrhosis and 1.3% had an incident diagnosis of hepatic decompensation. Similarly, 1.7% of the GLP-1 RA cohort had an incident diagnosis of cirrhosis, and 0.9% had an incident diagnosis of hepatic decompensation. The mean time from index treatment event to diagnosis was 5–6 months.
GLP-1 RA treatment patterns
The majority of patients with MASH who were taking a GLP-1 RA were adherent to treatment (PDC ≥ 0.8) over the 12-month follow-up period, ranging from 53.0% of the low-dose subgroup to 59.1% of the high-dose subgroup (Table 3). However, using a 45-day allowable gap, a majority of patients discontinued GLP-1 RA therapy during follow-up, including 57.1% of the low-dose subgroup and 52.2% of the high-dose subgroup. The mean time to discontinuation was 4–5 months. Of those who discontinued, 46.8% of the low-dose subgroup and 56.4% of the high-dose subgroup restarted on a GLP-1 RA within the follow-up period, typically within about 3 months after discontinuing. The dosage at restart was not assessed. Similar trends were observed using a 60-day allowable gap.
| GLP-1 RA users | |||
|---|---|---|---|
| Any dose | High dose | Low dose | |
| Treatment patterns | n = 10,316 | n = 2043 | n = 8273 |
| Adherence | |||
| Proportion of days covered, mean (SD) | 0.71 (0.32) | 0.76 (0.29) | 0.70 (0.33) |
| Adherent, n (%) | 5588 (54.2) | 1207 (59.1) | 4381 (53.0) |
| Discontinuation | |||
| ≥45 day gap | |||
| Discontinued, n (%) | 5788 (56.1) | 1067 (52.2) | 4721 (57.1) |
| Months to discontinuation, mean (SD) | 4.4 (3.3) | 4.9 (3.3) | 4.4 (3.3) |
| Restart after discontinuation, n (%) | 2809 (48.5) | 602 (56.4) | 2207 (46.8) |
| Months to restart, mean (SD) | 3.2 (2.1) | 3.1 (2.1) | 3.2 (2.1) |
| ≥60 day gap | |||
| Discontinued, n (%) | 5076 (49.2) | 916 (44.8) | 4160 (50.3) |
| Months to discontinuation, mean (SD) | 4.3 (3.1) | 4.8 (3.2) | 4.2 (3.1) |
| Restart after discontinuation, n (%) | 2128 (41.9) | 456 (49.8) | 1672 (40.2) |
| Months to restart, mean (SD) | 3.8 (2.1) | 3.7 (2.1) | 3.8 (2.1) |
GLP-1 RA: Glucagon-like peptide-1 receptor agonists; SD: Standard deviation.
Reasons for discontinuation
In an exploratory analysis of reasons for discontinuation of GLP-1 RA using 363 clinical notes extracted from 266 patients, side effects/adverse events were the most commonly documented reason for stopping therapy (n = 129 [35.5%]) (Supplementary Table 5). Side effects or adverse events were reported as the reason for discontinuation among 39.1% of those who discontinued within the first 6 months and among 33.0% of those who discontinued after 6 months. Other common reasons included switched medications (15.2%) and cost/insurance barriers (8.8%). The analysis was not designed to determine if patients were switching to a different GLP-1 RA or a different class of medications.
Healthcare utilization & costs
During the baseline period, 12.0% of the non-GLP-1 RA cohort and 7.8% of the GLP-1 RA cohort had at least one inpatient admission, 26.6% and 27.3% had an emergency department visit, and over 98% had an outpatient visit and other outpatient service (Supplementary Table 6). Trends were similar in the follow-up period, with 11.0% of the non-GLP-1 RA cohort and 7.2% of the GLP-1 RA cohort having at least one inpatient admission, while 27.6% and 26.4% had an emergency department visit. Patients with MASH had, on average, 13.9–17.8 outpatient visits, 13.3–14.0 other outpatient services and 15.0–17.7 unique drug formulas during the baseline period, along with 15.0–17.5 outpatient visits, 12.5–15.4 other outpatient services and 18.2–20.0 unique drug formulas during the follow-up period.
Mean (SD) all-cause costs in the baseline period were $20,912 ($77,882) in the overall GLP-1 RA cohort, $19,865 ($41,141) in the high-dose subgroup, and $21,170 ($84,532) in the low-dose subgroup (Figure 3). In the follow-up period, costs were $27,586 ($54,262) in the overall GLP-1 RA cohort, $28,082 ($49,631) in the high-dose subgroup, and $27,464 ($55,348) in the low-dose subgroup. For comparison, baseline and follow-up costs in the non-GLP-1 RA cohort were $19,019 ($50,196) and $24,917 ($69,706), respectively. Total costs after removing the top 1% of spenders and median costs are reported in Supplementary Table 5. While these cost estimates were lower than the main analysis, descriptive increases between baseline and follow-up were observed across all cohorts.
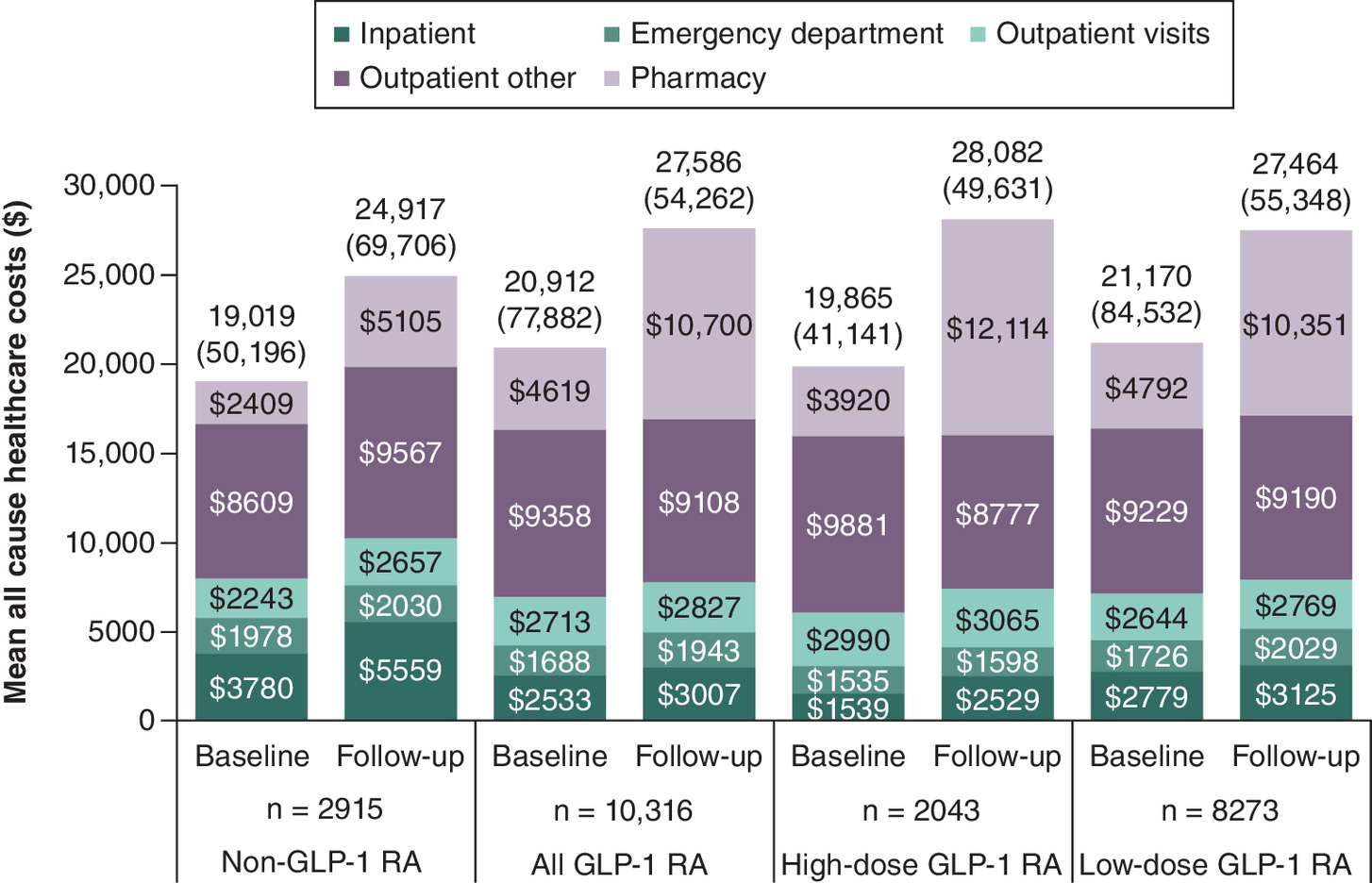
Figure 3. Mean all-cause healthcare resource utilization in the baseline and follow-up periods.
GLP-1 RA: Glucagon-like peptide-1 receptor agonists.
In the GLP-1 RA cohort, mean (SD) pharmacy costs were $4619 ($49,140) in the baseline period and $10,700 ($18,238) in the follow-up period. In the baseline period, the largest category of costs in all cohorts was other outpatient services, with mean (SD) costs of $9358 ($46,284) and $8609 ($36,819) for the GLP-RA and non-GLP-1 RA cohorts, respectively. In the follow-up period, these costs were $9108 ($34,299) and $9567 ($41,905), respectively. Overall, mean medical costs, i.e., non-pharmacy-related healthcare costs, were $16,293 in the baseline period and $16,886 in the follow-up period among all patients prescribed GLP-1 RA, $15,945 and $15,969 among patients in the high-dose subgroup, and $16,378 and $17,113 among patients in the low-dose subgroup.
Discussion
MASH is a growing threat to public health, and its increasing healthcare costs remain a major unmet need. Our study of a large cohort of 10,316 US patients with MASH who initiated treatment with GLP-1 RAs yielded three key findings. First, while the use of high-dose GLP-1 RAs was associated with a 10% reduction in the percentage of patients with class III obesity, roughly 80% of patients with MASH with a documented BMI who took high-dose or low-dose GLP-1 RA had a BMI ≥30 in the follow-up period. Second, over 50% of individuals who started a GLP-1 RA discontinued within the first 12 months. Third, the observed trends of GLP-1 RA use were not associated with a decrease in medical cost among patients with MASH in either the high or low-dose subgroups, suggesting that GLP-1 RA therapy was not leading to the resolution of medical issues, including liver-related events.
Weight loss
The weight loss effects of GLP-1 RAs have been well documented among patients with a high BMI. In a retrospective analysis of patients in a large integrated US healthcare system who initiated a GLP-1 RA at a dosage appropriate for glycemic control (n = 2405), 26.3% of patients lost at least 5% of their body weight 56 weeks after treatment initiation [31]. Similar results were seen in an analysis of the UK Clinical Practice Research Datalink, in which 33.4% of patients with Type 2 diabetes who initiated a GLP-1 RA lost at least 5% of their body weight within a year [32]. One study of 810 patients in the US with Type 2 diabetes who initiated a GLP-1 RA found that adherent patients lost twice as much weight in a year as nonadherent patients (4.3 vs 1.9 kg) [33]. In this study, we observed improved BMI among those who were treated with GLP-1 RAs, particularly among those receiving a high dose. Specifically, among those with documented BMI, we observed a doubling in the proportion with BMI <24.9 (2.3–4.0%) and BMI 25–29.9 (7.3–15.9%), with a reduction among those with BMI ≥ 40 (36.6–25.9%).
Adherence & discontinuation
The anticipated benefits from GLP-1 RAs on MASH resolution stem from the associated weight loss; however, evidence suggests that patients tend to regain weight after discontinuing GLP-1 RAs [34–36]. The high rates of discontinuation observed in this and other studies suggest that in the real world, patients may not sustain GLP-1 RA treatment for sufficient time to achieve the benefits observed in clinical trials. In general, rates of adherence to (53–59%) and discontinuation of (52–57%) GLP-1 RAs in this population of patients with MASH in this study were similar to prior reports among patients with Type 2 diabetes (adherence: 34–51%; discontinuation: 36–59%) [37–39]. An exploratory analysis found that side effects and adverse events were the most commonly documented reasons for discontinuing GLP-1 RAs, followed by switched medications and cost/insurance barriers. A more comprehensive analysis of discontinuation is planned to explore associations with dosage, active ingredient, insurance type and other factors.
In this study, we observed a mean PDC of 0.70 at 12 months for patients initiating GLP-1 RAs. Estimates from prior studies of patients with Type 2 diabetes range from 0.65 for all new starts to 0.75 for patients with at least 2 GLP-1 RA prescriptions [37,38]. While these values may seem high relative to the observed adherence values, the threshold for being adherent is a PDC ≥0.8. PDC also does not account for discontinuation or gaps in therapy. For example, a patient who discontinued after 9 months of continuous therapy and a patient who took a GLP-1 RA for 6 months and then switched to a different GLP-1 RA after a 3-month gap in therapy would both have a PDC of 0.75 and be considered to have discontinued and been nonadherent. Alternatively, patients switching between dosages or active ingredients may be filling prescriptions more frequently, resulting in a stockpile of medication. To account for this, we capped the PDC at 1; however, a patient who took a GLP-1 RA for 3 months and then switched to a different GLP-1 RA after a 3-month gap in therapy but managed to stockpile an extra month of medication would have a PDC of 0.83 and would be considered to be adherent but have discontinued therapy. Further research into the details of GLP-1 RA treatment patterns is required to better understand how these medications are being used in the real world.
Cost
Mean cost estimates in this study for patients with MASH taking GLP-1 RAs ranged between $19,865 (high-dose GLP-1 RA cohort) and $21,170 (low-dose GLP-1 RA cohort) in the baseline period and between $27,464 (low-dose GLP-1 RA cohort) and $28,082 (high-dose GLP-1 RA cohort) in the follow-up period. The increase from baseline to follow-up was primarily driven by pharmacy costs, as mean medical costs among patients who indexed on GLP-1 RA were $16,293 in the baseline and $16,886 in the follow-up. While we did not observe a decrease in medical costs among patients who received a high-dose GLP-1 RA, we did not stratify these results by change in BMI. Future studies should explore medical costs among patients who were persistent on therapy and among those who did or did not achieve weight loss targets.
These estimates of total costs in the baseline period are comparable to, but on the higher end of, prior estimates of uncomplicated MASH, which ranged from $16,744 to $22,953 [40–42]. This likely reflects the higher incidence of comorbid diabetes in this study cohort compared with the overall MASH population. In a prior analysis, 56.8% of patients with MASH had a comorbid diagnosis of Type 2 diabetes, and a comorbid diagnosis of Type 2 diabetes was associated with a 63% incremental increase in costs over a diagnosis of MASH alone [24]. In that study mean costs among patients with MASH and Type 2 diabetes were $22,213. Therefore, to contextualize the costs of patients initiating GLP-1 RA, this analysis also reported costs among a comparator cohort of patients with MASH who were initiating a different second-line treatment for Type 2 diabetes. In this non-GLP-1 RA cohort, mean costs were $19,019 in the baseline period and $24,917 in the follow-up period.
Limitations
This study is subject to the standard limitations of a retrospective database study, including data entry errors, missing data and coding limitations. More specific limitations include the fact that patients with MASH were identified by diagnosis code and not biopsy, even though biopsy is required for a definitive diagnosis. This was because biopsies are not widely conducted, and the results are not available in the structured data fields. Instead, we used the K75.81 diagnosis code for identifying patients, which is the recommended approach for identifying patients with MASH in retrospective database studies [25,26]. However, reliance on a documented MASH diagnosis will exclude individuals at a high risk of undiagnosed MASH, such as those with multiple other metabolic conditions. It should also be noted that, prior to 2023, the condition now known as MASH was referred to as nonalcoholic steatohepatitis. Both terms refer to the same underlying condition and are documented with the same ICD-10-CM code [25,26,43].
This analysis also does not capture MASH stage as the results of biopsy and alternative measures of MASH resolution, such as magnetic resonance imaging proton-density-fat-fraction, are not frequently performed, and when performed, the results are not captured in the structured data fields. While some lab data is available in the data source, we did not attempt to stratify patients by disease severity using noninvasive scoring systems. Without staging information, it is not possible to predict the expected incidence of severe liver outcomes in the follow-up period. Furthermore, BMI values could only be calculated for a subset of the study population, and as this missingness may be nonrandom, there is the potential for bias in the results of the changes in BMI analysis. While it is not possible to know in which direction this might bias the results, the percentage of documented BMI was similar across cohorts. Furthermore, patients may be misclassified into an incorrect BMI category if there were errors in documented height and weight.
In addition, this study was not structured to identify patients at a particular point in their patient journey, so it likely includes patients ranging from mild to severe fibrosis. Therefore, costs are an average across the broad MASH population, resulting in wide SDs. As we restricted to individuals with 24 months of continuous health insurance, costs may not be representative of uninsured individuals or those with less stable insurance who could not qualify for this study. The costs analysis was descriptive, and there was no inferential testing of differences between the GLP-1 RA cohort and the non-GLP-1 RA cohort. This was because critical variables that would impact treatment selection, including insurance plan formulary, treatment indication and drug availability, were not available in the dataset leveraged for this analysis.
It should be noted that while the non-GLP-1 RA cohort was selected based on initiation of a second-line therapy for Type 2 diabetes, 13% did not have a diagnosis code indicating Type 2 diabetes during the 12-month baseline period. This is likely due to three factors: the diagnosis being present but not documented during the 12-month baseline period, the index medication being prescribed for an indication other than diabetes, or a documentation error. Note that the baseline period did not include the index date, which may contribute to the undercounting of comorbid Type 2 diabetes.
Furthermore, a 12-month follow-up is likely not sufficient for the development of new liver-related outcomes, and any outcomes first reported in the follow-up period were likely present but undiagnosed in the baseline period. In addition, the exclusion of individuals based on their medical history may reduce the generalizability of our findings, particularly with regard to individuals with other etiologies of liver disease as well as those with a history of severe complications from MASH.
Finally, the notes analysis was exploratory and on a different population than the rest of the study. Patients could qualify for the notes analysis even if they did not qualify for the overall study because there was no requirement for insurance coverage or continuous enrollment. The purpose of the exploratory analysis was to inform future studies and provide general context not to reflect directly on the other study findings.
Conclusion
Some patients with MASH on GLP-1 RAs, particularly those taking higher dosages, may achieve weight loss. However, discontinuation was common, and from this descriptive analysis, no change in medical costs or differences in liver-related events compared with non-GLP-1 RA patients with MASH were observed in the follow-up period. This suggests that in a real-world setting, chronic metabolic issues, including MASH, persist after initiation of GLP-1 RA therapy.
Summary points
•
Due in part to their efficacy in promoting weight loss, there is interest in glucagon-like peptide-1 receptor agonists (GLP-1 RAs) as a treatment for metabolic dysfunction-associated steatohepatitis (MASH).
•
In Phase II clinical trials, some GLP-1 RAs have demonstrated the potential for promoting steatohepatitis resolution without worsening of fibrosis among patients with MASH who were adherent to treatment for a year.
•
GLP-1 RAs are currently prescribed to many patients with MASH who have a comorbid diagnosis of an approved indication, such as Type 2 diabetes or obesity.
•
This study used real-world data from electronic health records and healthcare claims to examine patient characteristics, treatment patterns, healthcare utilization and healthcare costs among patients with MASH for initiated GLP-1 RAs on either a high or low dose.
•
The percentage of patients with class III obesity was lower by 5.8% in the follow-up period among all patients with MASH taking GLP-1 RA and was lower by 10.7% among those taking a high dose.
•
A majority of patients discontinued GLP-1 RA treatment within the first 12 months, and less than half of those who discontinued restarted treatment; the mean time to discontinuation was 4 months.
•
Nonpharmacy related healthcare costs were $16,293 in the baseline period and $16,886 in the follow-up period among patients prescribed GLP-1 RAs.
•
Overall, while weight loss benefits were observed, many patients discontinued therapy before the 1 year, and medical costs remained high in the follow-up period, suggesting that chronic metabolic conditions were persisting despite GLP-1 RA treatment.
Author contributions
EB Tapper, T Marlin, M Bonafede, Y Kim contributed to the conceptualization of the study. N Zeng and R Carter were responsible for data handling and formal analysis of the data. All authors contributed to the development of the methodology implemented in the study, data visualization, interpretation of the results and writing and revising of the manuscript.
Acknowledgments
The authors thank the following employees of Veradigm for their contributions to the study: Matt Chang for QA'ing the data analysis, Dave Lewandowski for programming support and Amanda Manfredo for the code that pulled the note snippets. This support was funded by Madrigal Pharmaceuticals. The authors also thank Jesse Fishman for his contributions to the study while he was an employee of Madrigal Pharmaceuticals.
Financial disclosure
This study and publication costs were funded by Madrigal Pharmaceuticals, Inc.
Competing interests disclosure
T Marlin, N Zeng, R Carter, JP Winer-Jones and M Bonafede are employees of Veradigm, which received fees from Madrigal Pharmaceuticals related to this work. Y Kim is an employee of Madrigal Pharmaceuticals. EB Tapper is an employee at the University of Michigan, which received unrestricted financial support to the institution related to this work. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Editorial support was provided by Maryam Ajose, an employee of Veradigm. These services were funded by Madrigal Pharmaceuticals.
Ethical conduct of research
The linked dataset only contains deidentified data as per the de-identification standard defined in Section §164.514(a) of the HIPAA Privacy Rule. The process by which the data are deidentified is attested to through a formal determination by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule. Because this study used only deidentified patient records, it is therefore no longer subject to the HIPAA Privacy Rule and is therefore exempt from Institutional Review Board approval and for obtaining informed consent according to US law. This study was conducted in compliance with the Declaration of Helsinki and used only deidentified data.
Data sharing statement
The data that support the findings of this study were used under license from Veradigm and Komodo Health. Due to data use agreements and their proprietary nature, restrictions apply regarding the availability of the data. Further information is available from the corresponding author.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Rinella ME, Lazarus JV, Ratziu V et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 78(6), 1966 (2023).
2.
Sheka AC, Adeyi O, Thompson J, Hameed B, Crawford PA, Ikramuddin S. Nonalcoholic steatohepatitis: a review. JAMA 323(12), 1175–1183 (2020).
3.
Estes C, Anstee QM, Arias-Loste MT et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J. Hepatol. 69(4), 896–904 (2018).
4.
Younossi ZM, Golabi P, de Avila L et al. The global epidemiology of NAFLD and NASH in patients with Type 2 diabetes: a systematic review and meta-analysis. J. Hepatol. 71(4), 793–801 (2019).
• Review of prevalence of Type 2 diabetes among patients with metabolic dysfunction-associated steatohepatitis (MASH).
5.
Quek J, Chan KE, Wong ZY et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 8(1), 20–30 (2023).
• Review of the prevalence of obesity among patients with MASH.
6.
Estes C, Razavi H, Loomba R, Younossi Z, Sanyal AJ. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 67(1), 123–133 (2018).
7.
European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO). EASL-EASD-EASO clinical practice guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). Obesity Facts 17(4), 374–443 (2024).
8.
Rinella ME, Neuschwander-Tetri BA, Siddiqui MS et al. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 77(5), 1797–1835 (2023).
9.
Cusi K, Isaacs S, Barb D et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the diagnosis and management of nonalcoholic fatty liver disease in primary care and endocrinology clinical settings: co-sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr. Pract. 28(5), 528–562 (2022).
10.
Koutoukidis DA, Koshiaris C, Henry JA et al. The effect of the magnitude of weight loss on non-alcoholic fatty liver disease: a systematic review and meta-analysis. Metabolism 115, 154455 (2021).
11.
Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 149(2), 367–378.e5 (2015).
12.
Malespin MH, Barritt AS, Watkins SE et al. Weight loss and weight regain in usual clinical practice: results from the TARGET-NASH observational cohort. Clin. Gastroenterol. Hepatol. 20(10), 2393–2395.e4 (2022).
13.
Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of Type 2 diabetes – state-of-the-art. Molecular Metabolism 46, 101102 (2021).
14.
Popoviciu M-S, Păduraru L, Yahya G, Metwally K, Cavalu S. Emerging role of GLP-1 agonists in obesity: a comprehensive review of randomised controlled trials. Int. J. Mol. Sci. 24(13), 10449 (2023).
15.
Bethel MA, Patel RA, Merrill P et al. Cardiovascular outcomes with glucagon-like peptide-1 receptor agonists in patients with Type 2 diabetes: a meta-analysis. Lancet Diabetes Endocrinol. 6(2), 105–113 (2018).
16.
Michos ED, Lopez-Jimenez F, Gulati M. Role of glucagon-like peptide-1 receptor agonists in achieving weight loss and improving cardiovascular outcomes in people with overweight and obesity. J. Am. Heart Assoc. 12(11), e029282 (2023).
17.
Newsome PN, Buchholtz K, Cusi K et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N. Engl. J. Med. 384(12), 1113–1124 (2021).
18.
Mantovani A, Petracca G, Beatrice G, Csermely A, Lonardo A, Targher G. Glucagon-like peptide-1 receptor agonists for treatment of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: an updated meta-analysis of randomized controlled trials. Metabolites 11(2), 73 (2021).
19.
Volpe S, Lisco G, Fanelli M et al. Once-weekly subcutaneous semaglutide improves fatty liver disease in patients with Type 2 diabetes: a 52-week prospective real-life study. Nutrients 14(21), 4673 (2022).
20.
Sanyal AJ, Newsome PN, Kliers I et al. Phase III trial of semaglutide in metabolic dysfunction–associated steatohepatitis. N. Engl. J. Med. 392(21), 2089–2099 (2025).
•• Phase III trial results of SC semaglutide efficacy among patients with MASH.
21.
Elm E von, Altman DG, Egger M et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 4(10), e296 (2007).
22.
Kanwal F, Kramer JR, Li L et al. GLP-1 receptor agonists and risk for cirrhosis and related complications in patients with metabolic dysfunction-associated steatotic liver disease. JAMA Intern. Med. 184(11), 1314–1323 (2024).
23.
Younossi ZM, Tampi RP, Racila A et al. Economic and clinical burden of nonalcoholic steatohepatitis in patients with Type 2 diabetes in the U.S. Diabetes Care 43(2), 283–289 (2020).
24.
Fishman J, Tapper EB, Dodge S et al. The incremental cost of non-alcoholic steatohepatitis and Type 2 diabetes in the United States using real-world data. Curr. Med. Res. Opin. 39(11), 1425–1429 (2023).
25.
Hagström H, Adams LA, Allen AM et al. Administrative coding in electronic health care record-based research of NAFLD: an expert panel consensus statement. Hepatology 74(1), 474–482 (2021).
26.
Hagström H, Adams LA, Allen AM et al. The future of International Classification of Diseases coding in steatotic liver disease: an expert panel Delphi consensus statement. Hepatol Commun. 8(2), e0386 (2024).
• Expert consensus on billing codes to be used to identify likely patients with MASH.
27.
Centers for Diease Control and Prevention. Adult BMI Categories (2024). Available from: https://www.cdc.gov/bmi/adult-calculator/bmi-categories.html
28.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson Comorbidity Index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
29.
Glasheen WP, Renda A, Dong Y. Diabetes complications severity index (DCSI)—update and ICD-10 translation. J. Diabetes Complications 31(6), 1007–1013 (2017).
30.
Quek RGW, Fox KM, Wang L, Li L, Gandra SR, Wong ND. A US claims-based analysis of real-world lipid-lowering treatment patterns in patients with high cardiovascular disease risk or a previous coronary event. Am. J. Cardiol. 117(4), 495–500 (2016).
31.
White GE, Shu I, Rometo D, Arnold J, Korytkowski M, Luo J. Real-world weight-loss effectiveness of glucagon-like peptide-1 agonists among patients with Type 2 diabetes: a retrospective cohort study. Obesity 31(2), 537–544 (2023).
32.
Weiss T, Yang L, Carr RD et al. Real-world weight change, adherence, and discontinuation among patients with Type 2 diabetes initiating glucagon-like peptide-1 receptor agonists in the UK. BMJ Open Diabetes Res. Care 10(1), e002517 (2022).
33.
Carls GS, Tan R, Zhu JY et al. Real-world weight change among patients treated with glucagon-like peptide-1 receptor agonist, dipeptidyl peptidase-4 inhibitor and sulfonylureas for Type 2 diabetes and the influence of medication adherence. Obes. Sci. Pract. 3(3), 342–351 (2017).
34.
Jensen SBK, Blond MB, Sandsdal RM et al. Healthy weight loss maintenance with exercise, GLP-1 receptor agonist, or both combined followed by one year without treatment: a post-treatment analysis of a randomised placebo-controlled trial. eClinicalMedicine 69, 102475 (2024).
35.
Wilding JPH, Batterham RL, Davies M et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension. Diabetes Obes. Metab. 24(8), 1553–1564 (2022).
36.
Rubino D, Abrahamsson N, Davies M et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA 325(14), 1414–1425 (2021).
37.
Do D, Lee T, Peasah SK, Good CB, Inneh A, Patel U. GLP-1 receptor agonist discontinuation among patients with obesity and/or Type 2 diabetes. JAMA Netw. Open 7(5), e2413172 (2024).
• Prior estimates of GLP-1 discontinuation in patients with obesity or Type 2 diabetes.
38.
Weiss T, Carr RD, Pal S et al. Real-world adherence and discontinuation of glucagon-like peptide-1 receptor agonists therapy in Type 2 diabetes mellitus patients in the United States. Patient Prefer. Adherence 14, 2337–2345 (2020).
39.
Polonsky WH, Arora R, Faurby M, Fernandes J, Liebl A. Higher rates of persistence and adherence in patients with Type 2 diabetes initiating once-weekly vs daily injectable glucagon-like peptide-1 receptor agonists in US clinical practice (STAY study). Diabetes Ther. 13(1), 175–187 (2022).
40.
Tapper EB, Bonafede M, Fishman J et al. Healthcare resource utilization and costs of care in the United States for patients with non-alcoholic steatohepatitis. J. Med. Econ. 26(1), 348–356 (2023).
• Prior study on overall costs of patients with MASH stratified by fibrosis-4 score.
41.
Wong RJ, Kachru N, Martinez DJ, Moynihan M, Ozbay AB, Gordon SC. Real-world comorbidity burden, health care utilization, and costs of nonalcoholic steatohepatitis patients with advanced liver diseases. J. Clin. Gastroenterol. 55(10), 891–902 (2021).
42.
Gordon SC, Fraysse J, Li S, Ozbay AB, Wong RJ. Disease severity is associated with higher healthcare utilization in nonalcoholic steatohepatitis medicare patients. Am. J. Gastroenterol. 115(4), 562–574 (2020).
43.
Rinella ME, Sookoian S. From NAFLD to MASLD: updated naming and diagnosis criteria for fatty liver disease. J. Lipid Res. 65(1), 100485 (2024).
Information & Authors
Information
Published In
Copyright
© 2025 Madrigal Pharmaceuticals, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 23 November 2024
Accepted: 28 August 2025
Published online: 6 October 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Healthcare costs and treatment patterns associated with glucagon-like peptide 1 receptor agonist use among patients with metabolic dysfunction-associated steatohepatitis. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0223
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Xiurong Wu, Yang Qiu, Rui Dai, Zixu Huang, Jinghan Wang, Xiantao Yan, Xiangzhen Nie, Ronghan Liu, Bioactive aporphines and flavonoids from a fermented beverage target metabolic inflammatory pathways in obesity and type 2 diabetes, Scientific Reports, 10.1038/s41598-025-30778-9, 16, 1, (2025).