Cost-effectiveness analysis of endoscopic sinus surgery versus external approach for sinonasal inverted papilloma
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Sinonasal inverted papilloma is a benign yet locally aggressive tumor with potential for recurrence. Surgical resection is the primary treatment, and both endoscopic sinus surgery (ESS) and external approaches are employed depending on tumor location and stage. While clinical outcomes of both techniques have been studied, their economic implications remain underexplored. Materials & methods: A retrospective cost-effectiveness analysis was conducted on 50 patients treated for histologically confirmed inverted papilloma between 1995 and 2018. Patients underwent either ESS or an external approach. Direct medical costs were calculated from hospital records, and effectiveness was measured by 5-year disease-free survival (DFS). Cost-minimization and cost-effectiveness analyses were performed, including subgroup evaluation by Krouse stage. Results: The median total cost was significantly lower for the endoscopic group (€7567.23) compared with the external group (€11,456.40; p = 0.018). Endoscopic surgery resulted in an average savings of approximately €4000 per patient over a 5-year period. In localized disease tumors (Krouse I–II), ESS was both less costly and equally effective. Although the external approach showed a slightly higher DFS (77.2 vs 67.8%), the incremental cost-effectiveness ratio (ICER) was €40,837.13, suggesting limited cost-justification for this benefit. Conclusion: Endoscopic surgery resulted in an average saving of approximately €4000 per patient over a 5-year period. While external approaches showed slightly better disease-free survival, the endoscopic technique proved significantly more cost-effective, offering a better balance between clinical outcomes and resource use.
Plain language summary
What is this article about?
This study compares two surgical techniques used to treat a rare nasal tumor called inverted papilloma. The two techniques are: endoscopic sinus surgery, which is minimally invasive and performed through the nose, and external surgery, which requires an incision on the face. We wanted to find out which method is more cost-effective, meaning which offers better value by balancing results and expenses.
What were the results?
We studied 50 patients treated at a single hospital. We found that the endoscopic technique was significantly less expensive, saving about €4000 per patient over 5 years, compared with the external approach. While the external surgery had a slightly higher tumor control rate (77 vs 68%), it also involved longer hospital stays and higher overall costs.
What do the results mean?
The endoscopic approach is more cost-effective in most cases, especially in patients with localized-stage tumors. These results support using the endoscopic method as the first choice when technically possible. Understanding the economic impact of each technique can help hospitals and surgeons make better decisions that balance clinical outcomes with responsible healthcare spending.
Inverted papilloma (IP) is a rare benign tumor of the Schneiderian epithelium that originates in the nasal cavity and paranasal sinuses [1]. The WHO classifies IP as one of three types of Schneiderian papillomas, inverted, exophytic and oncocytic variants [2]. IP accounts for approximately 0.4–4.7% of all surgically resected sinonasal tumors, with an estimated incidence of 0.74 to 2.3 cases per 100,000 population per year [3]. These tumors are locally aggressive, with a tendency for recurrence and a potential association with squamous cell carcinoma [4].
Surgical resection remains the cornerstone of treatment. The choice of surgical technique depends primarily on tumor location, extent and site of attachment. Historically, external approaches such as lateral rhinotomy, Caldwell–Luc procedures and open medial maxillectomy were widely used [5]. Endoscopic endonasal surgery is now considered the gold standard [6,7]. External approaches are reserved for tumors involving the frontal sinus, orbit, for example and are now considered complementary to the endoscopic approach when complete resection cannot be achieved endonasally [8,9]. Medial maxillectomy is currently performed predominantly via the endoscopic route, offering improved visualization and lower morbidity [10].
Recent systematic reviews and meta-analyses confirm that endoscopic resection is associated with reduced morbidity and lower recurrence in appropriately selected patients. Bhattacharyya’s meta-analysis showed a significantly lower recurrence rate with endoscopic techniques [11], while Geiger et al. demonstrated equivalent outcomes in frontal sinus IP between endoscopic and combined approaches [12]. Additionally, Kim et al. reported a 44% relative reduction in recurrence risk favoring EES over external surgery [13]. These findings are consistent with prior research showing recurrence rates between 12.8 and 18.8%, depending on the technique and extent of resection [14,15].
Economic considerations in surgical management of inverted papilloma
Modern healthcare systems require clinical decisions that balance therapeutic effectiveness with cost-efficiency. Economic evaluations, including cost-minimization and cost-effectiveness analyses are essential for comparing treatments that may offer similar clinical outcomes but differ in resource use, operative time, complication rates and hospital costs. IP is surgically treated either through an endoscopic or an external approach, depending on tumor location and extent. While both techniques have been extensively evaluated in terms of clinical results, their economic impact remains insufficiently studied [16–19].
Materials & methods
Study design & patient selection
This retrospective observational study included patients diagnosed with histologically confirmed sinonasal IP who underwent surgical treatment at a single tertiary center between January 1995 and December 2018. Inclusion criteria comprised patients aged 18 years or older with complete medical records and a minimum follow-up of 12 months. Patients were excluded if records were incomplete or follow-up was insufficient.
Treatment groups
Patients were categorized into two groups based on the surgical technique employed:
•
External approach group: included lateral rhinotomy, Caldwell–Luc procedures and open medial maxillectomy.
•
Endoscopic approach group: included endonasal endoscopic resections without external incisions.
All procedures were performed by experienced otolaryngologists, and the decision regarding surgical approach was influenced by tumor stage, location and institutional availability of endoscopic technology during the early years of the cohort.
Data collection & sources
Demographic variables (age and sex), as well as clinical and surgical data, were retrieved from institutional electronic health records and operative reports. Tumors were classified according to the Krouse staging system into localized-stage (T1–2) and extensive stage (T3–4), based on preoperative imaging and intraoperative findings. Postoperative complications and tumor recurrences were confirmed through follow-up nasal endoscopy and radiologic assessment during routine surveillance. Cost data were obtained from hospital billing records and included all direct medical expenses incurred during the 5-year follow-up. DFS was defined as the absence of endoscopically or radiologically confirmed tumor recurrence within 60 months postoperatively.
Outcome measures
The primary outcome was the total direct medical cost per patient, expressed in euros. This included costs related to outpatient visits, imaging, surgical intervention, hospitalization, management of complications and follow-up care. These costs were used to perform a cost-minimization and cost-effectiveness analysis.
Clinical effectiveness was assessed using the 5-year disease-free survival rate, derived from recurrence and reintervention data. The DFS values for each group were used to calculate the mean cost per unit of effectiveness and the incremental cost-effectiveness ratio (ICER).
Additional clinical variables were analyzed to support the interpretation of the economic findings. These included operative time, length of hospital stay, acute postoperative complications, number of ICU days, blood transfusion requirement, recurrence events and reinterventions.
Economic analysis
A cost-minimization analysis was performed under the assumption of comparable recurrence rates between surgical techniques. Direct medical costs included outpatient visits, imaging studies, surgical procedures, hospitalization, management of complications and follow-up care. The detailed breakdown of cost components is presented in Table 1.
| Process | Cost (€) |
|---|---|
| First ENT consultation | 217.41 |
| Follow-up ENT consultation | 108.71 |
| Operating room hour | 723.78 |
| Days hospital stay | 2189.04 |
| Day in ICU/REA | 4272.0 |
| CT scan (face/paranasal sinuses) | 125.51 |
| MRI (face) | 288.16 |
| Blood transfusion | 326.0 |
Breakdown of healthcare services included in the direct cost calculation per patient over a 5-year follow-up.
ENT: Ear, nose and throat specialist; ICU: Intensive care unit; REA: Reanimation unit.
Additionally, a cost-effectiveness analysis was conducted using 5-year disease-free survival as the effectiveness measure. The cost-effectiveness ratio was calculated in euros per DFS achieved. An ICER was also computed by dividing the difference in mean costs between approaches by the corresponding difference in DFS.
Statistical analysis
Statistical analysis was performed using STATA version 18. Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed variables were compared using Student’s t-test; nonparametric data were analyzed using the Mann–Whitney U test. Categorical variables were compared with Chi-squared or Fisher’s exact test, as appropriate. All tests were two-tailed and significance was set at p < 0.05. Cost data were reported as mean, median and 10% trimmed mean to reduce the influence of outliers.
Ethics approval
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the institutional ethics committee. Due to its retrospective nature, informed consent was waived by the ethics committee due to the retrospective design and anonymized data.
Results
Patient demographics
A total of 50 patients diagnosed with sinonasal IP were included in the study and followed for 5 years. The cohort consisted of 18 women (36%) and 32 men (64%), with a mean age of 58.2 years (SD ± 13.16), ranging from 25 to 80 years.
Surgical approach & patient distribution
Patients were divided into two groups according to the surgical approach:
The external approach group included 22 patients (6 women and 16 men) with a mean age of 60.73 years (SD ± 11.87). Procedures in this group involved Caldwell–Luc, lateral rhinotomy with medial maxillectomy and/or ethmoidectomy, and Lynch frontal-ethmoidectomy. All these surgeries were performed between 1996 and 2008 as primary interventions.
The endoscopic approach group consisted of 28 patients (12 women and 16 men) with a mean age of 56.36 years (SD ± 14.59). From 2009 onward, all primary procedures were performed using EES. External approaches were used only as complementary strategies in anatomically complex or advanced cases.
Tumor location & surgical approach
Before 2009, the choice of surgical approach was not primarily determined by tumor location but rather by the availability of endoscopic techniques at the institution. During this period, EES was not yet fully implemented, and therefore, external approaches were the standard regardless of tumor site.
From 2009 onward, the situation reversed: all primary procedures were performed endoscopically, and external approaches were reserved as complementary tools in selected complex cases, typically for tumors with frontal sinus involvement, orbital extension or invasion of the posterior/lateral maxillary wall. This transition reflects advancements in instrumentation, imaging and surgical expertise that enabled broader use of minimally invasive techniques.
Regarding anatomical distribution, among the nine patients with frontal sinus involvement, eight (88.9%) were treated via external approaches and only one (11.1%) endoscopically. Similarly, all tumors with orbital extension and the majority of those involving lateral or posterior maxillary walls were approached externally. In contrast, tumors limited to the nasal cavity, anterior ethmoid or medial maxilla were predominantly treated endoscopically.
Surgical time & hospital stay
The comparison between external and endoscopic surgical approaches reveals significant differences in surgical duration and hospital stay period. Patients undergoing the endoscopic approach had a significantly longer surgical time (median of 3.00 h) compared with those treated with the external approach (median of 2.00 h), with a p-value of <0.001 according to the Mann–Whitney U test. Conversely, hospital stay duration was notably shorter for the endoscopic approach (median of 1.00 day) compared with the external approach (median of 3.00 days), also with a p-value of <0.001, as shown in Table 2. Additionally, operative time varied according to tumor implantation site. Cases involving the frontal sinus or multiple sinus extensions had significantly longer operative times (median: 3.5 h), compared with tumors limited to the nasal cavity, anterior ethmoid or medial maxillary wall, which had a median duration of 2.0 h (p < 0.01). This suggests that anatomical complexity and tumor extent also influenced surgical duration, beyond the type of approach used.
| Variable | External | Endoscopic | Total | p-value |
|---|---|---|---|---|
| Surgical time, h | 2.00 [1.50, 3.00] | 3.00 [3.00, 3.50] | 3.00 [2.00, 3.00] | <0.001 |
| Hospital stay length, days | 3.00 [3.00, 4.00] | 1.00 [1.00, 1.00] | 1.50 [1.00, 3.00] | <0.001 |
| n | 22 (44.0%) | 28 (56.0%) | 50 (100.0%) |
Values expressed as median (interquartile range).
Comparison of operative duration and length of hospital stay between patients undergoing endoscopic vs external surgical resection for sinonasal inverted papilloma.
Acute complications, requirement for emergency surgery, blood product transfusion, number of days in ICU/REA
In most patients, no acute complications were reported based on the surgical approach they underwent. Only two orbital complications were documented in the endoscopic approach (7.1%), two cases of epistaxis in total (4.0%), and one cerebrospinal fluid fistula in the endoscopic approach (2.0%). Acute complications were resolved either during surgery or through conservative management. No significant differences were found between the groups (Table 3). According to the collected data, no patients required emergency surgery following either external or endoscopic approaches. Only one patient treated with the external approach required a blood product transfusion and a 1-day stay in the ICU/REA. No significant differences were found between the two groups (Table 4).
| Variable | External | Endoscopic | Total | p-value |
|---|---|---|---|---|
| None | 20 (90.9%) | 24 (85.7%) | 44 (88.0%) | 0.803 |
| Epistaxis | 1 (4.5%) | 1 (3.6%) | 2 (4.0%) | |
| CSF fistula | 0 (0.0%) | 1 (3.6%) | 1 (2.0%) | |
| Orbital complications | 1 (4.5%) | 2 (7.1%) | 3 (6.0%) |
Frequency of acute postoperative complications observed in each surgical group.
CSF: Cerebrospinal fluid.
| Variable | External | Endoscopic | Total | p-value |
|---|---|---|---|---|
| Emergency surgery | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Blood product transfusion | 1 (4.5%) | 0 (0.0%) | 1 (2.0%) | 0.254 |
| ICU/REA | 1 (4.5%) | 0 (0.0%) | 1 (2.0%) | 0.254 |
| Days in ICU/REA | 1 (100.0%) | 0 (0.0%) | 1 (100.0%) |
Incidence of blood transfusions, intensive care admissions and emergency interventions following surgery.
ICU: Intensive care unit; REA: Reanimation unit.
Recurrences
Among the 50 patients studied, 30.0% experienced recurrences, with a slightly higher distribution in the endoscopic approach group (35.7%) compared with the external approach group (22.7%), although this difference was not statistically significant (p = 0.279). Regarding the number of recurrences, 77.3% of patients in the external approach group and 64.3% in the endoscopic approach group had no recurrences (p = 0.320). Patients with a single recurrence were similarly distributed (22.7% in the external vs 21.4% in the endoscopic group), whereas multiple recurrences (two or more) were more frequent in the endoscopic group. Regarding surgical reintervention, 15 patients (30.0%) required a single reintervention, distributed as five patients (22.7%) in the external approach group and 10 patients (35.7%) in the endoscopic approach group. Additionally, five patients (10.0%) required two reinterventions, with one patient (4.5%) in the external group and four patients (14.3%) in the endoscopic group. Only two patients (4.0%) in the endoscopic group required three reinterventions. The statistical test for reinterventions yielded a p-value of 0.029, indicating a significantly higher need for reinterventions in the endoscopic group (Table 5). Using these data, the 5-year DFS rate was calculated as 0.7727 (95% CI: 0.5374–0.8985) for the external approach and 0.6786 (95% CI: 0.4732–0.8180) for the endoscopic approach.
| Variable | External | Endoscopic | Total | p-value |
|---|---|---|---|---|
| Recurrences – yes | 5 (22.7%) | 10 (35.7%) | (30%) | 0.279 |
| Recurrences, n | ||||
| 0 | 17 (77.3%) | 18 (64.3%) | 35 (70.0%) | 0.320 |
| 1 | 5 (18.2%) | 10 (35.7%) | 15 (30.0%) | |
| 2 | 1 (4.5%) | 4 (14.3%) | 5 (10.0%) | |
| 3 | 0 (0.0%) | 2 (7.1%) | 2 (4.0%) | |
| Reinterventions, n | ||||
| 1 | 5 (22.7%) | 10 (35.0%) | 15 (30.0%) | 0.29 |
| 2 | 1 (4.5%) | 4 (14.3%) | 5 (6.0%) | |
| 3 | 0 (0.0%) | 2 (7.1%) | 2 (4.0%) | |
| n | 22 (44.0%) | 28 (56.0%) | 50 (100.0%) | |
Rates and number of recurrences and surgical reinterventions during the 5-year follow-up period for both surgical techniques.
Recurrence was also influenced by tumor location. Patients with frontal sinus involvement or multifocal disease (Krouse stage III) had a recurrence rate of 42.8%, compared with 25.0% in patients with tumors limited to the nasal cavity or medial maxillary wall (Krouse stages I–II), a difference that reached statistical significance (p = 0.045). These findings underscore the importance of both surgical technique and anatomical implantation site in recurrence outcomes.
Economic analysis
Median costs by approach
The results show that the median total cost for the external approach was €11,456.40, with an interquartile range of €8756.68 to €15,794.40. For the endoscopic approach, the median cost was €7567.23, with an interquartile range of €6444.51 to €10,483.12. The combined median cost for both approaches was €9512.89, with an interquartile range of €6820.82 to €13,224.87. Statistical analysis revealed a significant difference in costs between the two approaches (p = 0.018) (Table 6).
| Approach | n (%) | Median total cost (interquartile range) | p-value |
|---|---|---|---|
| External | 22 (44.0%) | €11,456.40 (€8756.68–15,794.40) | 0.018 |
| Endoscopic | 28 (56.0%) | €7567.23 (€6444.51–10,483.12) | |
| Total | 50 (100.0%) | €9512.89 (€6820.82–13,224.87) |
Comparison of total median costs per patient over 5 years for endoscopic vs external surgical techniques.
Subgroup analysis by tumor stage: economic comparison
To ensure a valid comparison between surgical techniques, patients were grouped according to Krouse stage. Among patients with localized-stage tumors (Krouse I–II, n = 36), 23 underwent endoscopic surgery and 13 external surgery. The mean cost per patient was significantly lower for the endoscopic group (€8774.75) compared with the external group (€12,143.31), with a median difference of over €3500.
For extensive-stage tumors (Krouse III, n = 14), five patients were treated endoscopically and nine externally. The mean cost for the endoscopic group was €15,767.49, while the external group averaged €16,838.80. Both techniques required substantial resource use, but cost differences were less pronounced than in localized-stage disease. These findings highlight that in localized-stage disease, endoscopic surgery offers a clear economic advantage, whereas in advanced tumors, both techniques are resource-intensive, with cost differences being marginal.
Cost-minimization analysis
The formula used for this analysis:
Where C_external represents the mean cost of the external approach and C_endoscopic represents the mean cost of the endoscopic approach. The mean costs obtained were €14,064.19 for the external approach and €10,023.46 for the endoscopic approach. Applying the formula, the cost difference (ΔC) is
This indicates that the endoscopic approach is €4040.73 less expensive per patient over the 5-year follow-up period compared with the external approach. If evenly distributed, this difference would correspond to an average saving of approximately €808.15 per patient per year. However, this annualized figure should be interpreted cautiously, as most costs are concentrated around the surgical event and immediate postoperative period. Confidence intervals for the mean costs and the 10% trimmed mean confirmed the significance of these differences.
The cost ratio was also calculated:
This indicates that the cost of the external approach is 1.40-times higher than the endoscopic approach, consistent across both the original mean and the trimmed mean.
Cost-effectiveness analysis
Mean ratio
The formula used: mean ratio = cost (y)/effect (j).
Using the 10% trimmed mean costs and disease-free survival rates:
•
External approach: Mean ratio external = 13,360.98€/0.772 = 17,306.97€/DFS
•
Endoscopic approach: Mean ratio endoscopic = 9522.29€/0.678 = 14,004.68€/DFS
The results indicate that the endoscopic approach is more cost-effective, requiring €14,004.68 per unit of effectiveness compared with €17,306.97 for the external approach.
Incremental cost-effectiveness ratio
The formula used:
Substituting the values:
The ICER of €40,837.13 indicates that achieving one additional unit of disease-free survival with the external approach compared with the endoscopic approach incurs a significant additional cost.
The comparison evaluates the two surgical approaches in terms of cost and 5-year disease-free survival. While the external approach offers slightly higher survival (77.2%), it is associated with a significantly higher cost (€13,360.98). In contrast, the endoscopic approach, with lower costs (€9522.29) and a survival rate of 67.8%, proves to be more cost-effective. These findings are further illustrated in the cost-effectiveness curve (Figure 1), which plots the average cost per patient against the 5-year DFS for each surgical technique. As depicted, the endoscopic approach is positioned closer to the origin, indicating superior cost-effectiveness compared with the external approach.
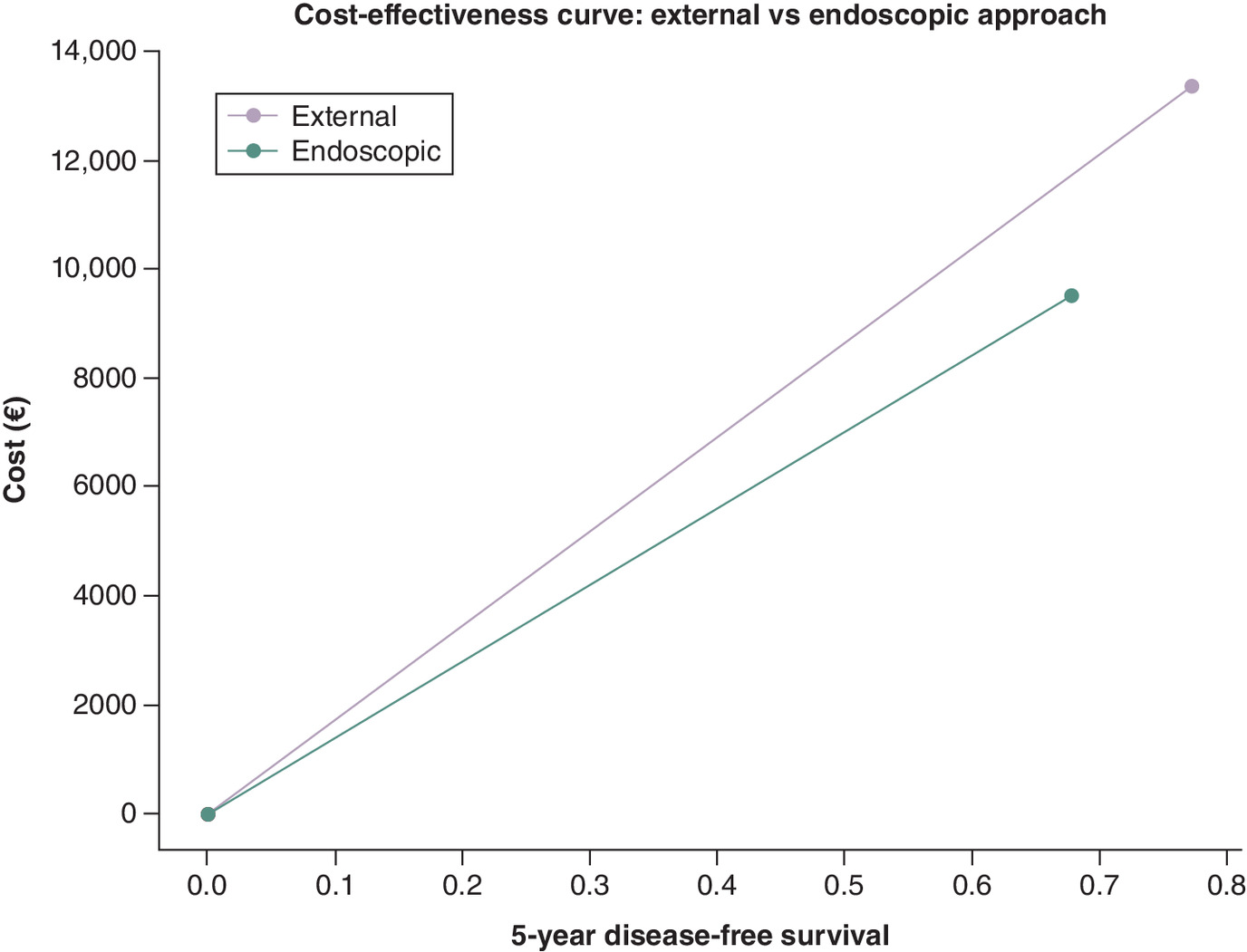
Figure 1. Cost-effectiveness curve comparing external and endoscopic surgical approaches for sinonasal inverted papilloma.
The x-axis represents 5-year disease-free survival; the y-axis shows the average cost per patient (euros). The endoscopic approach demonstrates lower costs and comparable clinical effectiveness.
Discussion
In contemporary healthcare, constrained resources necessitate that clinical decision-making integrates both efficacy and cost considerations. Economic evaluations, such as cost-minimization and cost-effectiveness analyses, have become essential tools for comparing medical interventions, especially when different techniques offer comparable clinical outcomes but differ in resource use, complication rates and hospitalization costs [20–22].
This study focused exclusively on the direct healthcare costs associated with surgical management of sinonasal IP, contrasting endoscopic and external approaches. Cost identification followed national recommendations for economic evaluation of new healthcare interventions [23], including expenses related to imaging, surgery, hospitalization and follow-up. Notably, instead of using the diagnosis-related groups system, which standardizes cost per pathology but often fails to reflect individual variability, our analysis manually calculated the total direct cost per patient, as detailed in Table 1. This individualized approach revealed that endoscopic surgery was 33.95% less expensive than external techniques, a statistically significant difference.
Technology introduces new challenges in prioritizing resource allocation. In this context, cost-effectiveness analysis offers a more nuanced view, considering both cost and clinical benefit, and it has been increasingly applied in rhinology and sinus surgery decision-making [24]. In our study, the primary effectiveness measure was 5-year DFS. The endoscopic approach demonstrated a more favorable cost-effectiveness profile by achieving similar DFS at lower cost. Although the external approach showed a modest DFS advantage, the calculated ICER indicated that the additional cost for this benefit was disproportionately high and possibly unjustifiable under typical willingness-to-pay thresholds. However, these results must be interpreted with caution. Patients treated with the external approach were part of the earlier cohort, prior to 2009, when endoscopic surgery was not yet fully established in our institution. During that period, limited access to nasofibroscopy and less structured follow-up protocols may have influenced outcome measures, including recurrence detection. These historical factors reduce the comparability of the two groups and reinforce the need for temporally contextualized interpretation. Moreover, hospitalization length had a marked impact on costs. The median hospital stay for endoscopic surgery was 1 day versus 3 days for external surgery, reinforcing the economic efficiency of the minimally invasive technique.
To date, no economic studies have specifically compared these two surgical techniques for IP. However, analogous data from chronic rhinosinusitis (CRS) surgeries offer valuable context. Bhattacharyya et al. reported a cost of $7726 (€6945) for ESS and postoperative care over 45 days [25], while Au and Rudmik found an outpatient ESS cost of CAD $3510 (€2332) in Canada [26]. A recent study by Ge et al. analyzing over 6000 US patients undergoing ESS for CRS with polyps reported a mean cost of $14,697 (€13,511), which rose to $23,605 (€21,717) in cases with major complications [27]. In our series, four endoscopically treated patients experienced complications. The only case of cerebrospinal fluid leak was managed during the same procedure; other complications, such as epistaxis and orbital issues, were resolved conservatively without additional surgery. The highest associated complication cost (€19,836.28) remained below the US average for major events.
Furthermore, Bhattacharyya et al. highlighted the substantial economic burden and resource utilization in patients with CRS and nasal polyps, emphasizing the importance of optimizing surgical selection [28]. Compared with these international figures, our study demonstrated lower overall costs for endoscopic procedures, suggesting that in our setting, endoscopic IP surgery is cost-efficient and safe.
Impact of tumor stage on surgical cost
Tumor stage is a critical variable in surgical planning and cost estimation. Using the Krouse classification, we observed that localized-stage IPs (I–II) treated endoscopically incurred significantly lower costs than those treated externally, supporting endoscopic surgery as a cost-effective first-line approach in these cases. Conversely, extensive-stage tumors (Krouse III) required greater resource utilization regardless of technique, with only marginal cost differences between surgical approaches. These findings underscore that tumor stage, not surgical technique alone, is a major driver of cost in IP management. Therefore, future cost-effectiveness analyses should adjust for disease stage to avoid biased conclusions.
Limitations
This study has inherent limitations due to its retrospective, nonrandomized design. The surgical approach was not randomly assigned but depended on local practice and technological availability, particularly in earlier years. The transition from external to endoscopic techniques occurred around 2008, resulting in temporal confounding between technique and outcomes. Implantation site, a key predictor of recurrence and operative complexity, was also not uniformly distributed: frontal sinus and orbit-invading tumors were predominantly treated externally, further complicating comparative analysis. Additionally, while tumor stage was controlled using the Krouse classification, exact implantation sites were inconsistently documented, limiting finer stratification. Cost analysis was based on hospital billing data and did not include indirect costs, such as patient productivity loss or long-term follow-up beyond 5 years. Lastly, the relatively small sample size, especially in extensive-stage subgroups, limits statistical power. These factors should be considered when interpreting the findings.
Future prospective studies, ideally multicentric and stratified by both stage and implantation site, are necessary to confirm the economic and clinical advantages of each approach in managing sinonasal IP.
Conclusion
The cost-minimization analysis demonstrated that endoscopic surgery is significantly more economical than the external approach, even after adjusting for outliers. Cost ratio calculations further confirmed that external techniques are consistently more expensive. Moreover, the endoscopic approach provided superior economic value per unit of clinical effectiveness, measured as 5-year disease-free survival. Although the external approach yielded a slightly higher survival rate, the ICER revealed that this marginal benefit required a disproportionately higher cost. These findings support the endoscopic technique as the more cost-effective surgical option for the management of sinonasal IP.
Summary points
•
Sinonasal inverted papilloma is a rare but locally aggressive tumor that requires surgical treatment.
•
Two main surgical approaches are used: external surgery and endoscopic sinus surgery.
•
This study retrospectively analyzed 50 patients treated between 1995 and 2018 in a single tertiary center.
•
Endoscopic sinus surgery (ESS) resulted in significantly lower direct healthcare costs, saving approximately €4000 per patient over a 5-year period.
•
The external approach offered marginally better disease-free survival, but at a high incremental cost-effectiveness ratio, limiting its cost-effectiveness.
•
Cost-effectiveness was especially favorable for ESS in localized-stage tumors (Krouse I–II).
•
Extensive-stage tumors (Krouse III) incurred high costs regardless of the surgical technique.
•
These findings support ESS as the preferred first-line treatment when technically feasible, balancing clinical outcomes and healthcare resource use.
Financial disclosure
This publication was supported by IIS Biobizkaia through funding provided by the Research Committee of OSI Bilbao-Basurto.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the institutional ethics committee. Due to its retrospective nature, informed consent was waived by the ethics committee due to the retrospective design and anonymized data.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Lawson W, Schlecht NF, Brandwein-Gensler M. The role of the Schneiderian membrane in the pathogenesis of sinonasal papillomas. Laryngoscope 118(2), 291–296 (2008).
2.
Hunt JL, el-Naggar A, Slootweg PJ, Chan JKC. Sinonasal papilloma, inverted type. In: WHO Classification of Tumors: Head and Neck. IARC Press, Paris, France, 18–19 (2017).
3.
Vrabec DP. The inverted Schneiderian papilloma: a 25-year study. Laryngoscope 104(5 Pt 1), 582–587 (1994).
4.
Nudell J, Chiosea S, Thompson LDR. Carcinoma ex-Schneiderian papilloma (malignant transformation): a clinicopathologic and immunophenotypic study of 20 cases combined with a comprehensive review of the literature. Head Neck Pathol. 8(3), 269–286 (2014).
5.
Bishop JA. OSPs and ESPs and ISPs, Oh My! An update on sinonasal (Schneiderian) papillomas. Head Neck Pathol. 11(3), 269–277 (2017).
6.
Sham CL, Woo JK, van Hasselt CA. Endoscopic resection of inverted papilloma of the nose and paranasal sinuses. J. Laryngol. Otol. 112(8), 758–764 (1998).
7.
Kamel RH. Endoscopic medial maxillectomy: a minimally invasive approach for maxillary sinus pathology. J. Laryngol. Otol. 124(4), 400–404 (2010).
8.
Castelnuovo P, Dallan I, Locatelli D et al. Endoscopic management of sinonasal malignancies: 10-year experience. Am. J. Rhinol. Allergy 25(3), 208–216 (2011).
9.
Busquets JM, Hwang PH. Endoscopic resection of sinonasal inverted papilloma: a meta-analysis. Otolaryngol. Head Neck Surg. 134(3), 476–482 (2006).
10.
Sun W, Zhang Y, Li S, Xu X, Xu G. Endoscopic medial maxillectomy: indications, technique, and outcomes. Am. J. Otolaryngol. 42(3), 102920 (2021).
11.
Bhattacharyya N. Endoscopic resection of sinonasal inverted papilloma: systematic review and meta-analysis. Otolaryngol. Head Neck Surg. 164(1), 16–24 (2021).
•• This meta-analysis is a cornerstone reference supporting the superior recurrence outcomes of endoscopic resection in sinonasal inverted papilloma (IP).
12.
Geiger G, Thomann I, Wellenstein D, Plettenberg A, Vogl TJ, Knoop H. Endoscopic sinus surgery in frontal sinus inverted papilloma: a systematic review. J. Pers. Med. 15(2), 183 (2025).
13.
Kim DY, Lee SH, Cho JH, Chung YS. Endoscopic versus external resection of sinonasal inverted papilloma: meta-analysis. Egypt. J. Otolaryngol. 38(1), 71 (2022).
• Highlights comparative effectiveness between surgical techniques, reinforcing the study’s rationale.
14.
Sauter A, Matharu R, Hörmann K, Naim R. Current advances in the basic research and clinical management of sinonasal inverted papilloma. Oncol. Rep. 17, 495–504 (2007).
15.
Lombardi D, Tomenzoli D, Butta L, Bizzoni A, Farina D, Nicolai P. Limitations and complications of endoscopic surgery for treatment of sinonasal inverted papilloma: a reassessment after 212 cases. Head Neck 33, 1154–1161 (2011).
16.
Sacristán JA, Ortún V, Rovira J, Prieto L, García Alonso F. Evaluación económica en medicina. Med. Clin. (Barc) 122(10), 379–382 (2004).
17.
Diaz-de-Cerio P, Preciado J, Santaolalla F, Sanchez-Del-Rey A. Cost-minimisation and cost-effectiveness analysis comparing transoral CO2 laser cordectomy, laryngofissure cordectomy and radiotherapy for the treatment of T1-2, N0, M0 glottic carcinoma. Eur. Arch. Otorhinolaryngol. 270(4), 1181–1188 (2013).
18.
Adamiak G. Methods for the economic evaluation of health care programmes, 3rd ed. J. Epidemiol. Community Health 60(9), 822–823 (2006).
19.
Martínez MM, Bosco G, Amarillo E et al. Eficacia del tratamiento quirúrgico del papiloma invertido nasosinusal. Rev. ORL 13(4), 277–287 (2022).
• Provides a recent Spanish-language analysis on surgical efficacy for sinonasal IP, supporting regional context.
20.
Ohki M, Kikuchi S. Sinonasal inverted papilloma: efficacy of demucosation to reduce recurrence after surgical managements. Indian J. Otolaryngol. Head Neck Surg. 71(Suppl. 3), 2186–2193 (2019).
21.
Caulley L, Rodin D, Kilty S, Randolph G, Hunink MG, Shin JJ. Evidence-based medicine in Otolaryngology part 10: cost-effectiveness analyses in Otolaryngology. Otolaryngol. Head Neck Surg. 161(3), 375–387 (2019).
•• Key reference for understanding the role and methodology of cost-effectiveness in ear, nose and throat surgical interventions.
22.
Pinto Prades JL, Sánchez Martínez FI. Métodos para la evaluación económica de nuevas prestaciones. Ministerio de Sanidad y Consumo, Madrid, Spain (2003).
23.
Prieto L, Sacristán JA, Antoñanzas F, Rubio-Terrés C, Pinto JL, Rovira J. Análisis coste-efectividad en la evaluación económica de intervenciones sanitarias. Med. Clin. 122(13), 505–510 (2004).
24.
Rudmik L. Health economics in rhinology: cost-effectiveness analyses in chronic rhinosinusitis and beyond. Curr. Opin. Otolaryngol. Head Neck Surg. 22(3), 231–236 (2014).
•• Provides a conceptual framework for economic analysis in rhinology, applicable to studies comparing surgical interventions.
25.
Bhattacharyya N, Orlandi RR, Grebner J, Martinson M. Cost burden of chronic rhinosinusitis: a claims-based study. Otolaryngol. Head Neck Surg. 144(3), 440–445 (2011).
• Supports external cost comparisons and underscores the economic relevance of sinonasal procedures.
26.
Au J, Rudmik L. Cost of outpatient endoscopic sinus surgery from the perspective of the Canadian government: a time-driven activity-based costing approach. Int. Forum Allergy Rhinol. 3(9), 748–754 (2013).
• Provides international costing benchmarks for endoscopic sinus surgery (ESS), useful for comparative interpretation.
27.
Ge W, Wang D, Chuang CC et al. Real-world cost of nasal polyps surgery and risk of major complications in the United States: a descriptive retrospective database analysis. Clinicoecon. Outcomes Res. 15, 209–211 (2023).
• A large-scale, recent cost analysis offering critical insights into ESS outcomes and complications.
28.
Bhattacharyya N, Villeneuve S, Joish VN et al. Cost burden and resource utilization in patients with chronic rhinosinusitis and nasal polyps. Laryngoscope 129(9), 1969–1975 (2019).
• Adds perspective on economic burden and healthcare utilization for chronic nasal disease, contextualizing the importance of surgical cost-efficiency.
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 28 June 2025
Accepted: 27 August 2025
Published online: 1 October 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost-effectiveness analysis of endoscopic sinus surgery versus external approach for sinonasal inverted papilloma. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0109
Export citation
Select the citation format you wish to export for this article or chapter.