Budesonide/formoterol versus salmeterol/fluticasone for asthma in children: an effectiveness and safety analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: The efficacy of budesonide + formoterol therapy compared with high-dose salmeterol + fluticasone therapy plus short-acting β-agonist (SABA) has not been evaluated specifically in children. Objectives: To evaluate the efficacy and safety of budesonide + formoterol combination therapy two times a day plus as needed compared with salmeterol + fluticasone two times a day plus SABA (as needed) in children in China. Methods: This prospective cohort study included 164 children with persistent asthma (aged 12–17 years) who had experienced a minimum of one asthma exacerbation in 12 months prior to the study. The primary outcome was the time to the first severe exacerbation. Results: Eighty-two children were assigned to each of two groups. The exacerbation rate per 100 patients per year was not found to be significantly different. The number of patients with hospitalization/emergency room therapy was lower in budesonide + formoterol group, but the risk difference was not statistically significant. Asthma control measures showed comparable effects. Both treatments were well-tolerated. Conclusion: No significant differences were observed in the outcome measures between the groups. Budesonide + formoterol therapy is a favorable approach in terms of a low load of ICS, steroid exposure, need for multiple inhalers and cost.
Asthma is a common and significant chronic disease globally, with a considerable increase in prevalence in the last 20 years, mainly in children [1]. Such a rise in pediatric asthma has been noted in many studies conducted in China [2,3]. According to modern guidelines, the asthma management goal is to improve disease control for an extended time and effectively address asthma worsening, thereby averting severe exacerbations [4,5]. Combination treatment of inhaled corticosteroid (ICS) with a long-acting β-agonist (LABA) is the recommended maintenance dose of therapy when asthma control with low-dose ICS alone is not achievable [5–7]. Asthma surveys have indicated that most patients utilizing an ICS alone or ICS + LABA combination nevertheless need short-acting β-agonist (SABA) treatment, with higher percentages showing night-time awakening, daytime symptoms and hospital admissions due to asthma [6,8,9].
There are two options available for the management of residual symptoms in patients utilizing the ICS + LABA combination. One choice is the increased ICS + LABA fixed-dose combination (budesonide + formoterol or salmeterol + fluticasone) maintenance dose, aimed at progressive stabilization of the disease process, thereby minimizing the need for short-acting reliever treatment. Another choice that is more patient-centered is the use of budesonide + formoterol for maintenance as well as relief [6,10]. Utilization of budesonide + formoterol combination for maintenance and reliever treatment depends on quicker and as-needed ICS + LABA adjustments, in contrast with SABA treatment, to fine-tune control of asthma. This method demonstrated a substantial reduction in severe exacerbations when compared with ICS + LABA + SABA therapy [6,11–14]. This new administration approach is now supported in updated guidelines by the Global Initiative for Asthma (GINA) as an effective method for the prevention of asthma exacerbations and improvement in control [5].
In a large, double-blind study by Kuna et al. [14], budesonide (160 μg) + formoterol (4.5 μg) combination therapy two-times a day (b.i.d.) and as needed decreased rates of exacerbation by 28–39% in comparison to either budesonide (320 μg) + formoterol (9 μg) b.i.d. or salmeterol (50 μg) + fluticasone (250 μg) b.i.d. plus SABA (terbutaline), as needed. Comparative results were shown in an open-label study by Vogelmeier et al. [13], with a 22% reduction in the exacerbation rate against salmeterol + fluticasone dose titration therapy. In the above study, only around 40% of patients receiving salmeterol + fluticasone therapy were titrated to higher doses (50 μg + 5 00 μg), which might have led to suboptimal control. However, in a double-blind study by Bousquet et al. [6] budesonide + formoterol therapy reduced exacerbation incidence compared with high-dose salmeterol + fluticasone therapy.
To the best of our knowledge, no study has been conducted specifically in children to evaluate the effect of budesonide + formoterol therapy and high-dose salmeterol + fluticasone therapy. This prospective study aimed to evaluate the efficacy as well as the safety of budesonide (160 μg) + formoterol (4.5 μg) combination therapy b.i.d. plus as needed compared with salmeterol (50 μg) + fluticasone (500 μg) b.i.d. plus SABA (as needed) in children in China.
Methods
Ethical approval & consent
This prospective cohort study was performed in the Department of Pediatrics of the authors' institute from January 10, 2017 to July 20, 2019. The hospital's ethics review board approved the study and the Helsinki Declaration (2008) guidelines [15] were followed. Patient confidentiality was strictly maintained. Informed consent was obtained from all participants and parents/legal guardians, as needed. The study adhered to the research laws of China.
Study cohorts
The study patients included outpatient children with persistent asthma aged 12–17 years, who had received ICS or ICS + LABA combination therapy for a minimum of three months. Exclusion criteria were the use of systemic corticosteroids in the 30 days prior to the study, recent respiratory infection, use of β-blocking agents and smoking history. All participants had forced expiratory volume in 1 second (FEV1) on prebronchodilator testing ≥50% of predicted normal values along with ≥12% reversibility post 1 mg terbutaline, and one or more asthma exacerbations in the 12 months prior to study inclusion. Patients were also required to have taken an as-needed reliever (terbutaline) for >4 of the last 7 days, but with not more than 8 inhalations per day. Patients in one group were given budesonide (160 μg) + formoterol (4.5 μg) combination therapy (Symbicort® Turbuhaler®) b.i.d. plus as needed; the other group received salmeterol (50 μg) + fluticasone (500 μg; Seretide™ Diskus™) b.i.d. plus terbutaline (0.4 mg per inhalation for relief of symptoms) for a period of six months.
Data collection
Demographic and clinical data were collected from the review of medical charts.
Outcome measurements
The primary outcome measure was the time to the first severe exacerbation, which was defined as asthma deterioration that lead to hospitalization/emergency room therapy and/or usage of oral corticosteroid therapy for a minimum of three days. Secondary outcomes were the time to the first hospitalization/emergency room therapy, the rate of hospitalization/emergency room therapies and the rate of severe exacerbations (as the same composite).
Asthma diary records by patients included measures of daily control such as peak expiratory flow, symptoms of asthma, use of relievers and nighttime awakenings because of asthma symptoms. From this data, asthma control days (no asthma symptoms, night awakenings and no as-needed drug usage) were calculated. The Simplified Asthma Control Questionnaire (ACQ-5), constituting five questions on the control of symptoms, was completed by patients. Scoring was on a 0–6 scale, with ‘0’ representing good control and “6” representing poor control. The ACQ-5 overall score is the average of the five responses.
Statistical analysis
Categorical variables are represented in percentages, whereas continuous variables are presented as means with ranges. Kaplan–Meier curves were used to describe the time to the first severe exacerbation. The Cox model was used for treatment group comparison. The comparison of the rate of severe exacerbations was performed using the Poisson regression model. Analysis of variance was used for between-group comparison of other measures (i.e., spirometry, symptoms of asthma, peak expiratory flows, as-needed drug usage and ACQ-5 scores). Analyses of all data were performed in IBM SPSS Statistics for Windows software (version 20.0; IBM Corp., NY, USA). p-values < 0.05 were deemed statistically significant.
Results
A total of 164 patients were enrolled in this study; 82 patients received budesonide + formoterol therapy and 82 patients received high-dose salmeterol + fluticasone + SABA therapy. The demographic and clinical data for patients were comparable between the groups (Table 1). The maintenance therapy adherence reported by caregivers or adolescents was found to be high (93% mean use).
| Characteristics | Budesonide + formoterol therapy (n = 82) | Salmeterol + fluticasone + SABA therapy (n = 82) |
|---|---|---|
| Age (years) | 14 (12–17) | 14 (12–17) |
| Male (n) | 52 (63.4%) | 49 (59.75%) |
| Diagnosis time† (years) | 8 (0–17) | 8 (0–17) |
| Exacerbations in last year | 1.5 (1–9) | 1.7 (1–19) |
| ICS usage at entry (μg/day) dosage | 652.4 (250–1000) | 683.6 (200–1125) |
| LABA usage at entry | 111 (45.12%) | 105 (42.68%) |
| FEV1 (l) | 2.12 (1.08–3.25) | 2.14 (1.12–3.36) |
| FEV1, % predicted | 73.2 (51–108) | 75.5 (50–130) |
| FEV1, reversibility % | 24.5 (7–99) | 24.4 (7–95) |
Values are expressed as mean (range) or n (%).
†
Median value with range.
FEV1: Forced expiratory volume in 1 s; ICS: Inhaled corticosteroid; LABA: Long-acting β-agonist; SABA: Short-acting β-agonist.
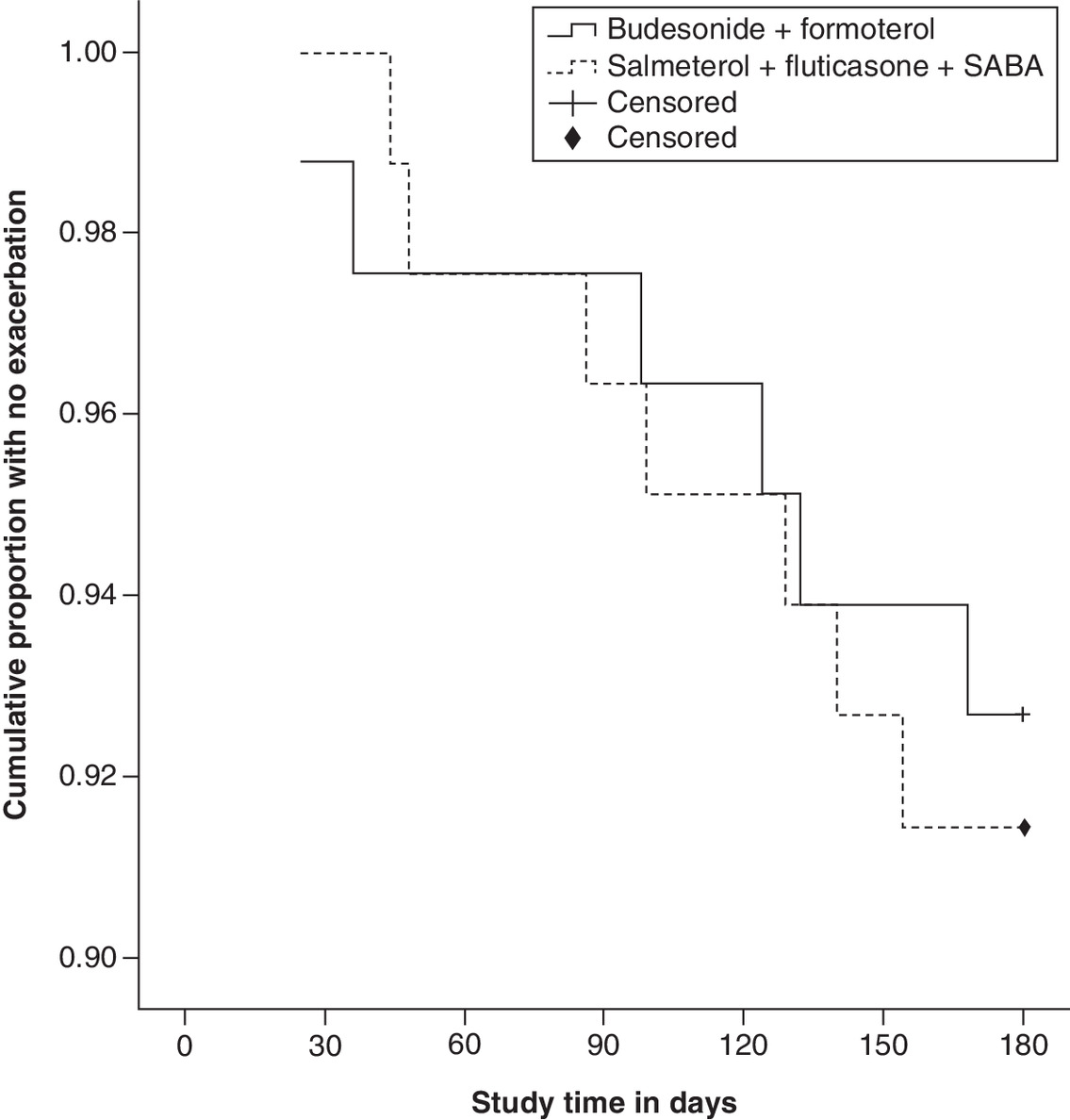
The data on severe exacerbation burden are presented in Table 2. The primary outcome (i.e., the time to the first exacerbation between therapy groups) was not significantly different (hazard ratio [HR]: 0.85; 95% CI: 0.29–2.55; p = 0.779) between groups. Six patients on budesonide + formoterol therapy and seven patients on salmeterol + fluticasone + SABA therapy experienced a total of 15 and 18 exacerbations, respectively. Although the Kaplan-Meier plot for the time to the first exacerbation demonstrated a prolonged time to the first exacerbation for budesonide + formoterol therapy, the exacerbation rate per 100 patients per year was not found to be significantly different (15 vs 18; p = 0.602; Figure 1). The number of patients receiving hospitalization or emergency room therapy was lower in the budesonide + formoterol therapy group (2; 2.44%) than in the salmeterol + fluticasone + SABA therapy group (4; 4.88%), but the difference in risk was not statistically significant (HR: 0.49; 95% CI: 0.09–2.72; p = 0.422).
| Event | Budesonide + formoterol therapy (n = 82) | Salmeterol + fluticasone + SABA therapy (n = 82) | Hazard ratio (95% CI) | p-value |
|---|---|---|---|---|
| Severe asthma exacerbation | ||||
| Number of patients | 6 (7.31%) | 7 (8.53%) | 0.85 (0.29–2.55) | 0.779 |
| Rate/100 patients/year | 15 | 18 | 0.83 (0.43–1.5) | 0.602 |
| Number of events | 7 | 9 | ||
| Hospitalization/ER therapy | ||||
| Number of patients | 2 (2.44%) | 4 (4.88%) | 0.49 (0.09–2.72) | 0.422 |
| Rate/100 patients/year | 5 | 9 | 0.56 (0.25–1.61) | 0.271 |
| Number of events | 3 | 5 |
Cox proportional hazards model was used for the time to first severe asthma exacerbation for therapy comparison.
Relative rate comparison was conducted using Poisson regression.
ER: Emergency room; SABA: Short-acting β-agonist.
Asthma control measures depicted in Table 3 showed comparable effects between groups. An increase in the number of asthma control days from baseline (6.1% vs 6.1%) to 43.9% in the budesonide + formoterol group and 45.1% in salmeterol + fluticasone + SABA group was noted. ACQ-5 scores showed similar improvement in control of asthma (decreased in both groups from baseline [1.82 vs 1.86] to 1.06 vs 1.14) with no statistically significant differences found between groups.
| Outcome | Budesonide + formoterol therapy (n = 82) | Salmeterol + fluticasone + SABA therapy (n = 82) | Therapy comparison (95% CI) | p-value |
|---|---|---|---|---|
| Symptoms of asthma | ||||
| Total score (0–6 scale) | ||||
| Baseline | 1.95 | 1.92 | -0.04 (-0.32–0.12) | 0.326 |
| During therapy | 0.93 | 0.98 | ||
| Symptom-free days | ||||
| Baseline | 9.8% | 10.9% | -0.42 (-2.8–1.9) | 0.584 |
| During therapy | 45.1% | 46.3% | ||
| Nighttime awakenings | ||||
| Baseline | 31.7% | 32.9% | -2.1 (-3.3–0.4) | 0.276 |
| During therapy | 10.9% | 13.4% | ||
| Asthma control days | ||||
| Baseline | 6.1% | 6.1% | -0.6 (-3.4–2.1) | 0.521 |
| During therapy | 43.9% | 45.1% | ||
| As-needed drug usage | ||||
| Number of inhalations per day | ||||
| Baseline | 2.08 | 2.14 | -0.11 (-0.32–0.04) | 0.242 |
| During therapy | 0.75 | 0.87 | ||
| As-needed drug-free days | ||||
| Baseline | 10.9% | 10.9% | -0.5 (-3.2–1.1) | 0.266 |
| During therapy | 57.3% | 58.5% | ||
| Number of events | ||||
| ACQ-5 (0–6 scale) | ||||
| Baseline | 1.82 | 1.86 | -0.07 (-0.21–0.06) | 0.473 |
| During therapy | 1.06 | 1.14 | ||
| PEF (l/min) | ||||
| Morning | ||||
| Baseline | 345.3 | 342.2 | 0.5 (-8.2–9.8) | 0.533 |
| During therapy | 378.5 | 377.7 | ||
| Evening | ||||
| Baseline | 349.4 | 350.1 | 1.1 (-1.8–5.6) | 0.664 |
| During therapy | 382.7 | 381.8 |
Analysis of variance was used for between group comparison.
ACQ-5: Asthma Control Questionnaire; PEF: Peak expiratory flow; SABA: Short-acting β-agonist.
Peak expiratory flows in both the morning and evening showed an increase in both groups but with statistically insignificant differences found between the groups. The as-needed drug-free days were found to be 57.3% of days in the budesonide + formoterol group and 58.5% of days in the salmeterol + fluticasone + SABA group, with a mean number of inhalations per day of 0.75 versus 0.87, respectively. The use of oral steroids for exacerbations was seen in 5 (6.1%) of the budesonide + formoterol group patients and in 6 (7.3%) of the salmeterol + fluticasone + SABA group patients. The difference in mean daily ICS doses (as per beclomethasone dipropionate [BDP]-equivalent doses) was statistically significant (lower in the budesonide + formoterol group). The fluticasone mean dose was 1000 μg/day (2000 μg BDP-equivalent dose) whereas the budesonide mean dose was 720 μg/day (1126 μg BDP-equivalent dose) with a reduction of 44% in the BDP-equivalent dose (p < 0.05).
From medical records, adverse events were found to have occurred in 21 (25.61%) patients receiving budesonide + formoterol and in 23 (28.05%) patients taking salmeterol + fluticasone + SABA. Serious adverse events (1 [1.22%; pharyngitis] in the budesonide + formoterol group; 2 [2.44%; sinusitis and bronchitis] in the salmeterol + fluticasone + SABA group) were comparable between the groups. There were no discontinuations and none of the events were fatal in either group. All included patients completed the study (Figure 1).
Discussion
This prospective study comparing patients receiving either budesonide + formoterol or salmeterol + fluticasone + terbutaline (as needed) demonstrated improvement in symptoms of asthma, as-needed drug usage and lung function in both groups. However, the differences regarding time to the first severe exacerbation (primary outcome) and the time to the first hospitalization/emergency room therapy, the rate of hospitalization/emergency room therapies and the rate of severe exacerbations were not statistically significant. Around 57.3% of days were as-needed-reliever free in the budesonide + formoterol group patients and 58.5% of days in the salmeterol + fluticasone + SABA group patients with an insignificant difference between the groups. The mean usage of relievers was comparable too, with close to one dose per day (0.75 vs 0.87) in both groups. The general use pattern and lack of overuse of relievers in the present study were in line with other studies conducted in adults and adolescents [6,14,16].
Even with a lower ICS dose in the budesonide + formoterol group, no significant differences were seen between the two therapy groups with respect to symptoms of asthma or the ACQ-5 questionnaire. This indicates that the two groups received effective therapy for asthma. After treatment, nearly half of the days fell into the category of asthma control days (43.9 vs 45.1%) from the baseline of 6.1% for both groups. Both treatments were found to be well tolerated with regard to adverse events, thereby showing a favorable safety profile, as demonstrated in prior studies [6,13,14,16,17].
Though there was no difference in the exacerbation rate reduction between therapy groups, which was inconsistent with a study in adults and adolescents [6], the convenience factor of utilizing only one inhaler for treatment as well as maintenance and relief is not to be undervalued. Additional considerations during therapy decision-making are the low load of ICS and comparatively lower costs. In a randomized controlled trial, higher doses of inhaled budesonide demonstrated a reduction in eosinophilic inflammation within a period of 6 h [18]. In a few studies, as-needed usage of budesonide showed rapid airway vasoconstriction thereby reducing airway edema [19,20]. Budesonide + formoterol showed full protection from late-phase allergen bronchoconstrictor responses compared with either budesonide or formoterol treatment in one study [21].
In the case of as-needed usage of formoterol, switching from terbutaline to formoterol resulted in effective asthma exacerbation reduction in adult patients on budesonide + formoterol therapy in one study [12]. A recent systematic review on children showed a comparable number of exacerbations with budesonide + formoterol therapy and salmeterol + fluticasone therapy. However, fewer patients receiving budesonide + formoterol group experienced hospitalization/emergency room therapy in comparison to the salmeterol + fluticasone group [17]. The present study on children showed no significant differences in any outcome measures between groups. This might suggest the avoidance of increased dosage and exposure to steroids when the same efficacy and safety can be achieved with budesonide + salmetorol as maintenance and reliever.
Limitations of the present study include the possibility of recall bias and the accuracy of reported drug usage. This was a single-center observational study with a small number of patients, so the generalizability of the present results is limited. Meaningful statistical analysis was not possible due to the small sample size. In conclusion, no significant differences were observed in the primary outcome of the time to the first severe exacerbation or other outcome measures between budesonide + formoterol therapy and salmeterol + fluticasone + terbutaline therapy. Budesonide + formoterol therapy seems to be a favorable approach in terms of a low load of ICS, steroid exposure, need for multiple inhalers and costs, respectively.
•
This is the first prospective study conducted specifically in Chinese children that evaluated the effect of budesonide + formoterol therapy and high-dose salmeterol + fluticasone therapy.
•
No significant differences were observed in the time to the first severe exacerbation or other outcome measures between the groups.
•
Both treatments were found to be well tolerated as measured by adverse events.
•
The maintenance therapy adherence was found to be high (93% mean use).
Author contributions
All authors contributed equally.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
The Global Asthma Report 2018. Global Asthma Network, Auckland, New Zealand (2018) www.globalasthmareport.org/Global%20Asthma%20Report%202018.pdf
2.
Li F, Zhou Y, Li S et al. Prevalence and risk factors of childhood allergic diseases in eight metropolitan cities in China: a multicenter study. BMC Public Health 11, 437 (2011).
• On childhood asthma in China.
3.
Xiang L, Zhao J, Zheng Y et al. Uncontrolled asthma and its risk factors in Chinese children: a cross-sectional observational study. J. Asthma 53(7), 699–706 (2016).
• On childhood asthma in China.
4.
Bousquet J, Clark TJ, Hurd S et al. GINA guidelines on asthma and beyond. Allergy 62(2), 102–112 (2007).
5.
Global Initiative for Asthma. Global strategy for asthma management and prevention. (2020). https://ginasthma.org/wp-content/uploads/2020/04/GINA-2020-full-report_-final-_wms.pdf
•• Asthma guidelines.
6.
Bousquet J, Boulet LP, Peters MJ et al. Budesonide/formoterol for maintenance and relief in uncontrolled asthma vs. high-dose salmeterol/fluticasone [published correction appears in Respir Med. 102(6), 937–8 (2008)]. Respir. Med. 101(12), 2437–2446 (2007).
•• Study on similar drug combination comparison.
7.
Expert Panel Report 3: guidelines for the Diagnosis and Management of Asthma (EPR-3: Full report 2007) [Internet]. USDepartment of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program, Bethesda, MD, USA (2007). www.nhlbi.nih.gov/sites/default/files/media/docs/EPR-3_Asthma_Full_Report_2007.pdf
•• Asthma guidelines.
8.
Partridge MR, van der Molen T, Myrseth SE, Busse WW. Attitudes and actions of asthma patients on regular maintenance therapy: the INSPIRE study. BMC Pulm. Med. 6, 13 (2006).
9.
Lai CK, De Guia TS, Kim YY et al. Asthma control in the Asia-Pacific region: the asthma insights and reality in Asia-Pacific study. J. Allergy Clin. Immunol. 111(2), 263–268 (2003).
10.
Bateman ED, Boushey HA, Bousquet J et al. Can guideline defined asthma control be achieved? The Gaining Optimal Asthma ControL study. Am. J. Respir. Crit. Care Med. 170, 836–844 (2004).
11.
O'Byrne PM, Bisgaard H, Godard PP et al. Budesonide/formoterol combination therapy as both maintenance and reliever medication in asthma. Am. J. Respir. Crit. Care Med. 171(2), 129–136 (2005).
• Study on one of the studied drug combinations.
12.
Rabe KF, Atienza T, Magyar P, Larsson P, Jorup C, Lalloo UG. Effect of budesonide in combination with formoterol for reliever therapy in asthma exacerbations: a randomized controlled, double-blind study. Lancet 368(9537), 744–753 (2006).
13.
Vogelmeier C, D'Urzo A, Pauwels R et al. Budesonide/formoterol maintenance and reliever therapy: an effective asthma treatment option? Eur. Respir. J. 26(5), 819–828 (2005).
14.
Kuna P, Peters MJ, Manjra AI et al. Effect of budesonide/formoterol maintenance and reliever therapy on asthma exacerbations. Int. J. Clin. Pract. 61(5), 725–736 (2007).
15.
World Medical Association. Declaration of Helsinki, Ethical Principles for Medical Research involving human subjects. (2008) www.wma.net/wp-content/uploads/2016/11/DoH-Oct2008.pdf
16.
Louis R, Joos G, Michils A, Vandenhoven G. A comparison of budesonide/formoterol maintenance and reliever therapy vs. conventional best practice in asthma management. Int. J. Clin. Pract. 63(10), 1479–1488 (2009).
•• Study on one of the studied drug combinations.
17.
Jorup C, Lythgoe D, Bisgaard H. Budesonide/formoterol maintenance and reliever therapy in adolescent patients with asthma. Eur. Respir. J. 51(1), 1701688 (2018).
•• Study on one of the studied drug combinations in subjects of interest.
18.
Gibson PG, Saltos N, Fakes K. Acute anti-inflammatory effects of inhaled budesonide in asthma: a randomized controlled trial. Am. J. Respir. Crit. Care Med. 163(1), 32–36 (2001).
19.
Barnes PJ. Scientific rationale for using a single inhaler for asthma control. Eur. Respir. J. 29(3), 587–595 (2007).
20.
Mendes ES, Pereira A, Danta I, Duncan RC, Wanner A. Comparative bronchial vasoconstrictive efficacy of inhaled glucocorticosteroids. Eur. Respir. J. 21(6), 989–993 (2003).
21.
Duong M, Gauvreau G, Watson R et al. The effects of inhaled budesonide and formoterol in combination and alone when given directly after allergen challenge. J. Allergy Clin. Immunol. 119(2), 322–327 (2007).
Information & Authors
Information
Published In
Pages: 1283 - 1289
PubMed: 34668718
Copyright
© 2021 Future Medicine Ltd.
History
Received: 11 June 2021
Accepted: 30 September 2021
Published online: 20 October 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Budesonide/formoterol versus salmeterol/fluticasone for asthma in children: an effectiveness and safety analysis. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0142
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Te-Jung Kung, Ching-Fu Weng, Shan-Chieh Wu, Fang-Ju Lin, Comparative effectiveness of fixed-dose inhaled corticosteroid/long-acting beta-agonist therapy in adult patients with asthma, Annals of Allergy, Asthma & Immunology, 10.1016/j.anai.2025.09.019, 136, 1, (75-84.e10), (2026).
- Gizem Koken, Sinem Polat Terece, Ceren Varer Akpinar, Hacer Ilbilge Ertoy Karagol, Arzu Bakirtas, ICS-LABA Fixed-Dose Combinations: Preferred Controller in 6-11-year-olds with Persistent Asthma, International Archives of Allergy and Immunology, 10.1159/000544938, (1-11), (2025).
- Keruo Zhou, Min Zhang, Chenyu Zuo, Xiazhen Xie, Jianwei Xuan, Cost-effectiveness analysis of budesonide/formoterol SMART therapy versus salmeterol/fluticasone plus as-needed SABA among patients ≥12 years with moderate asthma from the Chinese societal perspective, Journal of Medical Economics, 10.1080/13696998.2024.2385191, 27, 1, (1018-1026), (2024).