An observational cohort study of pelvic floor photobiomodulation for treatment of chronic pelvic pain
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This research is the first to evaluate the effectiveness of trans-vaginal photobiomodulation therapy (TV-PBMT) for chronic pelvic pain. Materials & methods: Observational analysis of 128 women, undergoing TV-PBMT for chronic pelvic pain. Minimal clinically important difference, defined as ≥2-point drop on a 0–10 numeric pain rating scale (NPRS), and effect size Cohen d coefficient, was calculated over nine treatments for overall pain, and pain with activities. Results: Compared with baseline, 64.5% of women showed improvement in overall pain, pain with bowel movement, intercourse, exercise, urination, sitting and vulvar pain (minimal clinically important difference = -2.4, -2.0, -2.4, -2.1, -2.1, -2.0, -3.1; d = 0.9, 0.7, 0.9, 0.7, 0.7, 0.7, 0.9) by treatment 9. Conclusion: In this cohort, TV-PBMT resulted in improvement of pelvic pain without serious adverse events.
Lay abstract
Low-level laser is a therapy that can help pain, but this type of treatment has not been available to women with chronic pelvic pain because traditional laser devices cannot access the pelvic structures. In this research we studied a novel low-laser device that can be used in the vagina, to treat pain arising from pelvic organs and muscles. Our preliminary research shows that this approach significantly reduced pelvic pain, and pain with activities such as exercise, urination, bowel movements and intercourse, in two-thirds of women who completed the therapy.
Chronic pelvic pain (CPP) affects nearly 15% of US women [1] and often it is caused by a variety of conditions, including interstitial cystitis/bladder pain syndrome (IC/BPS), irritable bowel syndrome, endometriosis and vulvodynia [2,3]. In settings where women with CPP are routinely evaluated with a standardized pelvic examination, 50–90% also present with musculoskeletal pain [3–6]. Myofascial pelvic pain (MFPP) and myofascial pelvic floor dysfunction are related terms used to describe musculoskeletal pelvic pain that can manifest as pain with sitting, intercourse, urination, defecation and physical activity, and is commonly associated with symptoms such as urinary urgency, frequency, constipation, sexual dysfunction or physical disability [7,8]. Because of its complexity, CPP has few treatment options. Pelvic physical therapy (PT) is one of the primary treatments recommended for CPP, especially when CPP is accompanied by MFPP or myofascial pelvic floor dysfunction. However, a 2019 systematic review of PT interventions for CPP concluded that, due to heterogeneity and poor methodological quality, the evidence does not support the use of PT for the management of CPP [9]. A recent randomized controlled trial of manual PT in patients with pelvic pain and IC/BPS found that 59% of women reported a clinically meaningful reduction in pain, yet, manual therapy was not superior to the control group [10]. Another large study found that only 20% of patients are compliant with PT. Although more high-quality research is needed, it appears that lack of standardized treatment protocols, poor compliance with therapy, and lack of access to specialized therapists, are significant barriers to using PT for treatment of CPP.
Photobiomodulation (PBM), previously referred to as low-level laser therapy, is a form of near-infrared (NIR) light therapy shown in several systematic reviews to improve pain in musculoskeletal and arthritic conditions such as low back pain, fibromyalgia, knee and shoulder pain [11–13]. The NIR light triggers biochemical changes within cells, where the photons are absorbed by chromophores and initiate a chain of intracellular chemical reactions [14]. PBM uses nonionizing light energy, in a nonthermal process, to affect the mitochondrial chromophore cytochrome c oxidase (COX) [15]. Mitochondria are considered ‘power plants’ within our cells because they can use oxidative phosphorylation to convert food and oxygen into energy in the form of ATP [14]. Nitric oxide (NO), is a mitochondrial waste product that is capable of binding to COX and displacing oxygen, especially in injured or hypoxic cells [16]. It is believed that PBM photo-dissociates NO from COX resulting in the release of NO [17] and increased production of ATP. NO is a powerful relaxer of both smooth and skeletal muscle, and it is also capable of reducing muscle pain and improving circulation to oxygen-deprived tissues [14,18,19]. Additional benefits are believed to be secondary to activation of various transcription factors that result from mitochondrial stimulation as well as the modulation of reactive oxygen species [20].
Based on the reported benefits of PBM for treating nonpelvic pain, a trans-vaginal photobiomodulation (TV-PBM) laser system was developed for the treatment of CPP [21]. This novel system, SoLá Pelvic Therapy (Uroshape, LLC, FL, USA), has been used since 2019, on-label, by gynecologists for the temporary relief of pelvic muscle spasms and pain. The SoLá Pelvic Therapy Laser is a nonablative class IV NIR laser capable of transmitting both 810 and 980 nm wavelengths to pelvic structures [21]. The nonionizing and nonthermal effect emitted by the device avoids the serious side effects such as vaginal scarring and burns reported [22] when traditional lasers (CO2 and Er:Yag lasers) are used to treat vaginal conditions such as atrophy, laxity and incontinence [23,24].
The application of PBM to the pelvis and its impact on CPP has not yet been studied in humans, thus, the overarching goal of our research is to provide the first real-world evidence on the effects of TV-PBM for the treatment of CPP. The specific goals of this preliminary, observational study are to describe the baseline characteristics of patients who chose this type of therapy; determine the average numbers of treatments used, compared with manufacturer recommendations (compliance); determine if PBM results in clinically meaningful decreases in overall (general) pelvic pain and symptom-specific pain (e.g., pain during urination, defecation or intercourses) and describe adverse events.
Materials & methods
This study is a before-and-after secondary analysis of de-identified data, prospectively collected from patients undergoing PBM therapy with a SoLá Pelvic Therapy device in 13 geographically diverse gynecology practices (Northeast, Southwest, West, Southeast and Midwest). SoLá Therapy uses a 15 W diode laser, that emits 810 and 980 nm wavelengths in a spherical energy array, through a proprietary, single-use, sterile, vaginal probe. The device has a touch screen interface that allows for collection of patient demographics, symptoms and pain severity using a numeric rating 0–10 scale (NRS). Severity data is collected for overall pain, and pain with exercise, sitting, standing, urination, bowel movements, intercourse and vulvar pain. This information is entered into the device by the patient before each treatment. The data from each patient is used to create a limited dataset (all PHI removed except the date and a random identifier number) that is encrypted, coded and transmitted to a Health Insurance Portability and Accountability Act (HIPAA) compliant server. Prior to starting treatment all patients sign an informed consent and release, authorizing the use of the limited dataset. After patient assessment, the single-use sterile probe is lightly lubricated and gently inserted into the vagina. The device then auto-calculates and sets dosing parameters (power and treatment time) utilizing vaginal length and proprietary trans-vaginal PBM dosing tables. The manufacturer recommends a protocol consisting of nine treatments administered over 3–4 weeks. The manufacturer’s instructions also specify that the device should be used in female patients with CPP confirmed by single-digit palpation of the pelvic muscles (levator ani, coccygeus, obturator).
Our analysis was confined to the limited dataset obtained from the manufacturer under a business associate agreement; dataset ID LDSET 103. Secondary analysis of a de-identified dataset by third-party investigators does not meet the Common Rule’s definition of research. Furthermore, the SoLá Therapy device is not investigational, and the data is collected as part of normal, routine, clinical care. Thus, IRB and human subject protection regulations do not apply to this analysis.
The primary outcome of interest was change in overall pain level from baseline (treatment number 1) compared with treatment number 9. In order to assess pain level change from baseline over time, we excluded those patients who had just started therapy (less than three treatments). Secondary outcomes included change in pain with exercise, sitting, standing, urination, bowel movements, intercourse and vulvar pain. Pain was measured using a NRS accompanied by descriptors ranging from ‘no pain’ at 0 to ‘worst pain’ at 10. Minimal clinically important difference (MCID) was used to define pain reduction of 2 or more NRS points, or a reduction of at least 30%. This MCID has been shown by prior research to consistently represent what patients with musculoskeletal chronic pain describe as ‘much better’ improvement [25,26].
Statistical significance was determined using Chi2 and Fisher’s Exact test (when cells contained <10 observations) for categorical variables. The paired t-test was used to analyze continuous, normally distributed variables such as age, and one sample Wilcoxon ranked sum t-test for nonparametric continuous variables such as pain levels (0–10). Statistical significance was set at a two-tailed alpha level of 0.05 and power of 80%. Effect size, an additional measure used to describe degree of improvement, was measured using Cohen d coefficient and interpreted as low effect size if d <0.2, medium if 0.2 < d <0.8, and high if d >0.8. To analyze the relationship between improvement in pain and baseline diagnosis or pain severity, we used simple logistic regression modeling where the outcome of interest was categorized as improved = 1 if the pain level improved 2 or more NRS points and improved = 0 if the pain level improved by <2 points. The analysis was conducted using Epi Info™ version 7.2 and STATA 16 (StataCorp, LLC, TX, USA), whereas graphs were created using Microsoft Excel.
Results
The limited dataset consisted of 144 female patients who were consecutively treated with the SoLá device from 21 June 2019 to 21 November 2020. Of the 144, 10.4% (n = 15) were excluded; eight stopped therapy after two treatments and seven stopped after the first treatment (two stopped due to an increase in pain, and five trialed the device without further treatments because free trials were allowed by the manufacturer during the first few months of commercialization). Since we had baseline characteristics for all patients who used the SoLá device at least once, we were able to compare characteristics of those who were included versus those excluded from the analysis (Table 1).
| Baseline characteristic | Included Completed ≥3 treatments (n = 128) | Excluded Completed ≤2 treatments (n = 15) | p-value |
|---|---|---|---|
| Mean age in years (SD) | 44.3 (15.1) | 39.73 (11.81) | 0.182 |
| Had previous physical therapy, n (%) | 94 (73.4) | 9 (60.0) | 0.274 |
| Reported receiving a prior diagnosis of, n (%)‡ | |||
| – Endometriosis | 18 (14.1) | 6 (40.0) | 0.021† |
| – IC/BPS | 56 (43.8) | 4 (26.7) | 0.027† |
| – Vulvodynia | 43 (33.6) | 6 (40.0) | 0.774 |
| – Myalgia | 97 (75.8) | 10 (66.7) | 0.443 |
| – Dyspareunia | 65 (50.8) | 8 (53.5) | 0.852 |
| – Vaginismus | 22 (17.2) | 7 (46.7) | 0.007† |
| Overall pain level mean, SD | 6.1 (2.6) | 6.7 (3.1) | 0.077 |
| Overall pain duration, n (%) | 0.718 | ||
| – Less than 1 year | 27 (21.1) | 1 (16.7) | |
| – More than 1 year but less than 2 years | 11 (8.6) | 1 (16.7) | |
| – More than 2 years but less than 3 years | 13 (10.2) | 2 (13.3) | |
| – More than 3 years but less than 4 years | 17 (13.3) | 2 (13.3) | |
| – More than 4 years | 60 (46.9) | 9 (60.0) | |
| Pain level with bowel movements mean (SD), n | 4.6 (3.1), 85 | 6.3 (3.6), 9 | 0.208 |
| Pain level with intercourse mean (SD), n | 6.7 (2.5), 100 | 7.2 (2.5), 14 | 0.702 |
| Pain level with exercise mean (SD) | 5.8 (2.8), 106 | 2.9 (3.1), 9 | 0.103 |
| Pain level with urination mean (SD), n | 5.0 (3.2), 84 | 5.3 (3.5), 11 | 0.246 |
| Pain level with sitting mean (SD), n | 6.0 (3.0), 106 | 5.0 (3.5), 11 | 0.388 |
| Pain level with standing mean (SD), n | 5.2 (2.1), 95 | 4.5 (3.9), 8 | 0.471 |
| Vulvar pain mean (SD), n | 5.8 (2.6), 90 | 4.7 (2.8), 10 | 0.266 |
Pain level as measured by 0–10 NRS.
†
p < 0.05.
‡
Patients may have had more than one diagnosis.
IC/BPS: Interstitial cystitis/bladder pain syndrome; NRS: Numeric rating 0–10 scale; SD: Standard deviation.
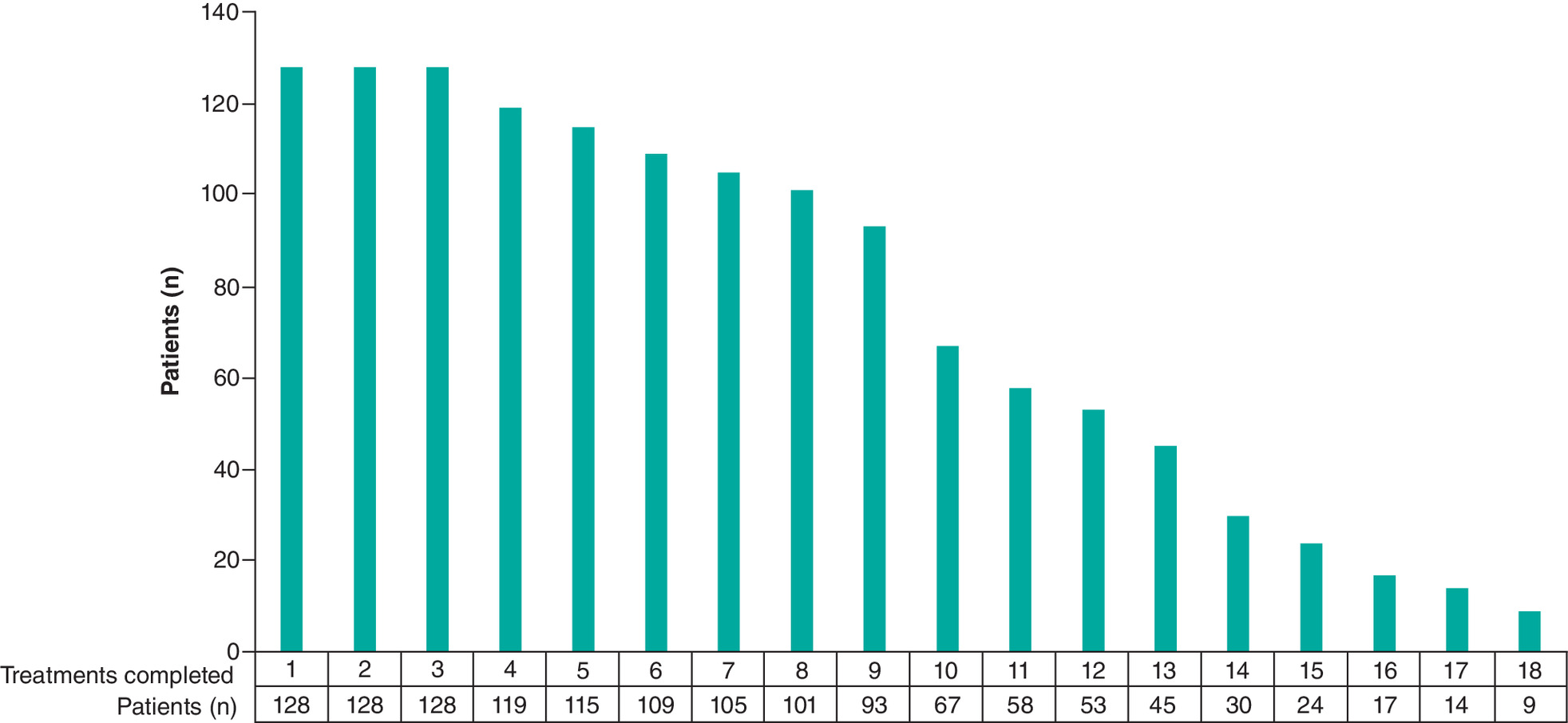
Of the 128 patients included, 93.0% (n = 119) completed four treatments, 89.8% completed five treatments, 72.7% (n = 93) completed all nine recommended treatments, and 52.3% (n = 67) opted for additional therapy beyond nine treatments (Figure 1). At baseline, in addition to overall pain, 66.4% (n = 85) also reported pain with bowel movements, 78.1% (n = 100) pain with intercourse, 82.8% (n = 106) pain with exercise, 65.6% (n = 84) pain with urination, 82.8% (n = 106) pain with sitting, 74.2% (n = 95) pain with standing and 70.3% (n = 90) had vulvar pain. Statistically significant differences in types of pain diagnosis were found between those who were included versus excluded, such that the excluded group had a higher proportion of women with endometriosis, IC/BPS and vaginismus. However, there was no difference in overall pain level or symptom-specific pain levels (Table 1).
Mean changes in overall pain and symptom-specific pain severity are presented in Figure 2. For the entire cohort, the largest improvement in overall pain level was noted within the first four treatments (mean NRS = 6.6 ± 2.6 after treatment 1 to mean NRS = 4.4 ± 2.6 after treatment 4; p < 0.000; MCID = -2.7; d = 0.9). Additional but smaller reductions in pain levels continued with further treatment. Changes in NRS comparing treatment 1 to treatment 9 are presented in Figure 3. Sample sizes for each symptom are also shown in Figure 3. Post-hoc sample size calculations were not necessary since we found statistically meaningful reductions in all outcomes of interest.
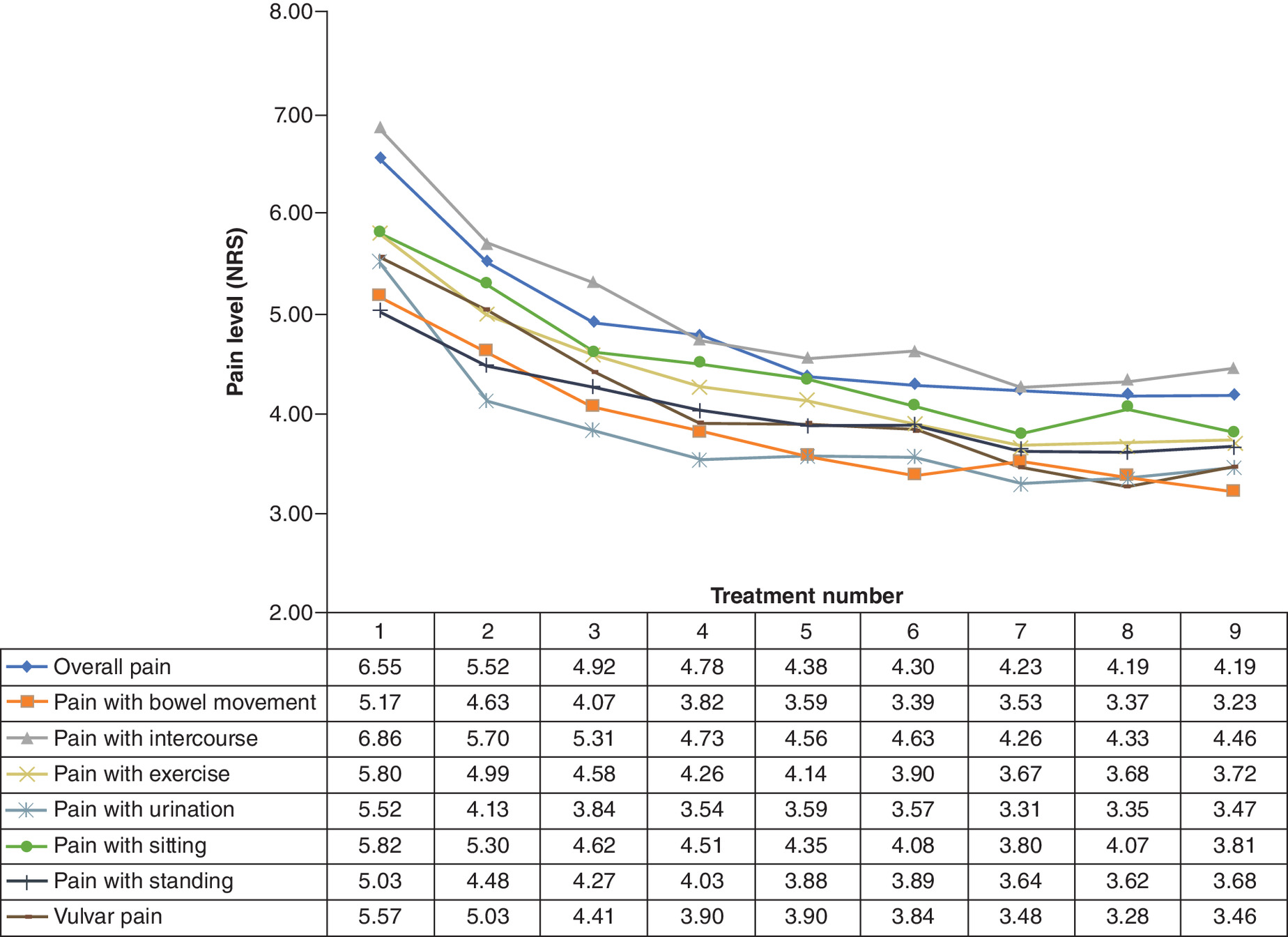
Figure 2. Change in mean pain levels through the course of nine treatments.
Overall pain: n = 93; pain with bowel movement: n = 63; pain with intercourse: n = 72; pain with exercise: n = 79; pain with urination: n = 61; pain with standing: n = 69; pain with sitting: n = 76; vulvar pain: n = 65.
NRS: Numeric rating 0–10 scale.

MCID, % reduction and effect size (Cohen d coefficient) were calculated for each pain outcome as follows: overall pain, MCID = -2.4, 36.0%, d = 0.9; pain with bowel movement, MCID = -2.0, 37.5%, d = 0.7; pain with intercourse, MCID = -2.4, 35.0%, d = 0.9; pain with exercise, MCID = -2.1, 48.8%, d = 0.7; pain with urination, MCID = -2.1, 37.3%, d = 0.7; pain with sitting, MCID = -2.0, 34.6%, d = 0.7; pain with standing, MCID = -1.4, 26.8%, d = 0.5 and vulvar pain MCID = -3.1, 55.4%, d = 0.9.
Clinically significant improvement in overall pain was reported by 59.1% (n = 68) of the 115 women who completed 5 treatments and 64.5% (n = 60) of the 93 women who completed nine treatments. Women previously diagnosed with pelvic floor myalgia had greater odds of improvement (odds ratio = 4.8, 95% CI: 1.3–17.7) as did women with vaginismus (odds ratio = 5.6, 95% CI: 5.6–27.1). These findings persisted after adjusting for age, prior PT and additional pain diagnoses such as endometriosis, dyspareunia and IC/BPS. Overall pain duration and severity of pain with defecation, urination, intercourse, sitting, standing and vulvar pain, did not significantly impact odds of improvement.
During the study period, there were no serious adverse events reported. However, of the 144 patients that received at least one treatment, minor adverse events were reported as follows: 6.9% (n = 10) had a temporary increase in pain, 2.1% (n = 3) had an increase in bladder symptoms, 13.2% (n = 19) had temporary noninfectious vaginal discharge and 1.4% (n = 2) were diagnosed with a urinary tract infection (UTI) around the time of treatment.
Discussion
Although PBM has been shown to be an effective treatment for a variety of musculoskeletal and arthritic chronic pain conditions [11–13], to our knowledge, this is the first study evaluating PBM for the treatment of CPP. In this cohort, more than 90% of women who tried one treatment continued beyond three treatments. The women in our analysis had a wide-ranging prevalence of self-reported pain co-morbidities (44% IC/BPS, 14% endometriosis, 50% dyspareunia, 70% vulvar pain) and symptom-specific pain (66% pain with bowel movements, 78% pain with intercourse, 83% pain with exercise, 66% pain with urination, 83% pain with sitting and 74% pain with standing). Eighty percent had pain lasting longer than 1 year. The combination of complex symptomatology and prolonged pain indicates that the study cohort is representative of women with CPP found in primary care practices as well as in highly specialized centers [2,27–32]. Thus, our findings should be generalizable to patients who are considering PBM therapy in both settings.
Once therapy was initiated, compliance with treatment was high; 93% complete four treatments, 90% completed five and 73% completed all nine treatments. Two large observational, uncontrolled, studies assessed the issue of compliance with pelvic floor PT, the primary treatment recommended for women with MFPP. Woodburn and colleagues studied over 660 patients referred to pelvic PT and found that only 20% of patients are compliant with the recommended length of treatment [33]. A similar study performed in a diverse urban group of 180 women showed that only 29% were compliant with pelvic floor PT [34]. Although we did not directly compare PBM with PT, it is reassuring to find that compliance with PBM was much higher than reported for PT. Factors that may help with compliance include ease of use (the vaginal probe is only 2 cm wide), short treatment time (treatments last only 2–4 min) and financial incentive since patients paid out-of-pocket for their treatments.
In 2004, a randomized trial of pelvic Thiele massage concluded that an undisclosed percentage of patients showed statistical, but not clinically meaningful, improvements in pain [35]. A subsequent trial of global therapeutic massage versus myofascial PT concluded that 26 and 59% of patients reported clinically meaningful pain improvement after 12 weeks of therapy [10]. The difference was not statistically significant. Our study shows that clinically significant improvement in overall pain was reported by nearly 65% of the women who completed the recommended therapy. Over the course of nine treatments, significant reductions were also found in severity of vulvar pain, as well as pain with exercise, bowel movements, urination, intercourse and sitting. The largest difference in pain improvement was noted between treatments 1 and 5, with additional but smaller improvement continuing to treatment 9. At last, odds of improvement were highest for women previously diagnosed with pelvic floor myalgia and vaginismus suggesting that PBM may be working to affect pelvic floor muscle function.
This study has several limitations inherent to observational uncontrolled studies, including the inability to establish a causal link between the use of TV-PBM and improvement in pain. Other factors such as repeated interaction with a healthcare provider may play a role in symptom improvement independent of the use of PBM. The diagnosis of myofascial CPP (based on single-digit pelvic examination) was not systematically confirmed, instead, we relied on patients and providers to comply with recommended protocols. The prevalences of the additional pain co-morbidities may represent overestimates since we relied on patient recall. The use of a 0–10 NRS is not adequate to measure many aspects of response to therapy such as physical and sexual function. Nor were we able to measure changes in affective components or psychological distress related to pain. At last, the study period is limited the 3–4 weeks required for each patient to complete nine treatments, thus we cannot comment on how long the therapeutic effect lasts.
Strengths of the study include a sample size large enough to allow us evaluate and find statistically and clinically significant differences across several variables. The number of excluded women was small and demographically similar to those who were included. Although the diagnoses of endometriosis, IC/BPS and vaginismus were more prevalent in the excluded group, women with those diagnoses who chose to continue therapy did well; women with vaginismus had greater odds of improvement while women with endometriosis and IC/BPS did equally well (compared with those without these diagnoses).
All outcomes were reported by patients (instead of healthcare providers) and collected in real-world clinical settings which may make our conclusions generalizable to similar populations of patients suffering with CPP. The 144 women in this cohort underwent 1386 treatments over a period of nearly 1.5 years. As expected, the complication rates were low and the most commonly reported side effect was temporary noninfectious vaginal discharge. Although larger studies are needed, this initial report should alleviate concerns for major complications such as vaginal burns or scarring described with ablative vaginal laser therapy [23,24].
In summary, the management of CPP is a burdensome condition that challenges patients and providers alike; few treatment options are available and most have not been shown to be of significant benefit [36]. TV-PBM, and the novel SoLá Pelvic Therapy device, may be an alternative for the treatment of CPP that is well tolerated, has minimal adverse events, and can be incorporated into clinical care. The findings obtained from this cohort are limited but reassuring. Controlled studies and randomized controlled trials are needed in order to determine the efficacy of PBM for the treatment of myofascial CPP. The data provided in this manuscript, and the fact that treatments can be easily standardized into a study protocol, should facilitate future studies.
Future perspective
CPP is a debilitating condition with few treatment options. Technologies, such as PBM, that are emerging for the treatment of pain are not available to women with CPP because pelvic structures are difficult to access and there is a paucity of research that focuses on this type of pain. Our research shows that trans-vaginal photobiomodulation for pelvic pain is both possible and promising. We provide the first evidence for the effectiveness of this type of therapy and provide data to support future randomized clinical studies.
•
In this cohort of women with chronic pelvic pain, trans-vaginal photobiomodulation significantly reduced overall pelvic pain, pain with sitting, standing, urination, defecation, intercourse and vulvar pain.
•
In over 1800 treatments reported in this study, trans-vaginal photobiomodulation therapy using a non-ablative, non-thermal low-level laser, was effective without serious adverse events.
Author contributions
N Kohli was directly involved in project development, data collection, manuscript writing. B Jarnagin and AR Stoehr contributed to data collection and manuscript editing. G Lamvu was directly involved in data analysis, manuscript writing and editing.
Financial & competing interests disclosure
All authors currently use SoLá therapy in their clinical practices. AR Stoehr, MD received honoraria for discussing SoLá Therapy with peers on behalf of UroShape, LLC. G Lamvu is Chief Scientific Officer for SoLá Therapy, LLC. She also serves as Chair of the Board of the International Pelvic Pain Society, on the board of SOLVD Health, as a research consultant for Abbvie, and Myovant. She is also an educational consultant for Medical Learning Institute Peer Review. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
Original research using data obtained from the manufacturer of the SoLá device. This data is publicly available through a manufacturer request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Mathias SD, Kuppermann M, Liberman RF, Lipschutz RC, Steege JF. Chronic pelvic pain: prevalence, health-related quality of life, and economic correlates. Obstet. Gynecol. 87(3), 321–327 (1996).
2.
Zondervan KT, Yudkin PL, Vessey MP et al. Chronic pelvic pain in the community--symptoms, investigations, and diagnoses. Am. J. Obstet. Gynecol. 184(6), 1149–1155 (2001).
3.
Lamvu G, Carrillo J, Ouyang C, Rapkin A. Chronic pelvic pain in women: a review. JAMA 325(23), 2381–2391 (2021).
4.
Fitzgerald CM, Neville CE, Mallinson T, Badillo SA, Hynes CK, Tu FF. Pelvic floor muscle examination in female chronic pelvic pain. J. Reprod. Med. 56(3–4), 117–122 (2011).
5.
Mieritz RM, Thorhauge K, Forman A, Mieritz HB, Hartvigsen J, Christensen HW. Musculoskeletal dysfunctions in patients with chronic pelvic pain: a preliminary descriptive survey. J. Manipulative Physiol. Ther. 39(9), 616–622 (2016).
6.
Sedighimehr N, Manshadi FD, Shokouhi N, Baghban AA. Pelvic musculoskeletal dysfunctions in women with and without chronic pelvic pain. J. Bodyw. Mov. Ther. 22(1), 92–96 (2018).
7.
Bonder JH, Chi M, Rispoli L. Myofascial pelvic pain and related disorders. Phys. Med. Rehabil. Clin. N. Am. 28(3), 501–515 (2017).
8.
Lamvu G, Carrillo J, Witzeman K, Alappattu M. Musculoskeletal considerations in female patients with chronic pelvic pain. Semin. Reprod. Med. 36(2), 107–115 (2018).
9.
Fuentes-Marquez P, Cabrera-Martos I, Valenza MC. Physiotherapy interventions for patients with chronic pelvic pain: a systematic review of the literature. Physiother. Theory Pract. 35(12), 1131–1138 (2019).
10.
FitzGerald MP, Payne CK, Lukacz ES et al. Randomized multicenter clinical trial of myofascial physical therapy in women with interstitial cystitis/painful bladder syndrome and pelvic floor tenderness. J. Urol. 187(6), 2113–2118 (2012).
11.
Clijsen R, Brunner A, Barbero M, Clarys P, Taeymans J. Effects of low-level laser therapy on pain in patients with musculoskeletal disorders: a systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 53(4), 603–610 (2017).
12.
Glazov G, Yelland M, Emery J. Low-level laser therapy for chronic non-specific low back pain: a meta-analysis of randomised controlled trials. Acupunct. Med. 34(5), 328–341 (2016).
13.
Yeh SW, Hong CH, Shih MC, Tam KW, Huang YH, Kuan YC. Low-level laser therapy for fibromyalgia: a systematic review and meta-analysis. Pain Physician 22(3), 241–254 (2019).
14.
Cotler HB, Chow RT, Hamblin MR, Carroll J. The use of low level laser therapy (LLLT) for musculoskeletal pain. MOJ Orthop. Rheumatol. 2(5), 00068 (2015).
15.
Anders JJ, Lanzafame RJ, Arany PR. Low-level light/laser therapy versus photobiomodulation therapy. Photomed. Laser Surg. 33(4), 183–184 (2015).
16.
Brown GC. Nitric oxide regulates mitochondrial respiration and cell functions by inhibiting cytochrome oxidase. FEBS Lett. 369(2–3), 136–139 (1995).
17.
Lane N. Cell biology: power games. Nature 443(7114), 901–903 (2006).
18.
de Freitas LF, Hamblin MR. Proposed mechanisms of photobiomodulation or low-level light therapy. IEEE J. Sel. Top Quantum Electron. 22(3), 7000417 (2016).
19.
Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 4(3), 337–361 (2017).
20.
Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR. The nuts and bolts of low-level laser (light) therapy. Ann. Biomed. Eng. 40(2), 516–533 (2012).
21.
Zipper R, Pryor B. Evaluation of a novel deep tissue transvaginal near-infrared laser and applicator in an ovine model. Lasers Med. Sci. (2021) (Epub ahead of print).
22.
Preti M, Vieira-Baptista P, Digesu GA et al. The clinical role of LASER for vulvar and vaginal treatments in gynecology and female urology: an ICS/ISSVD best practice consensus document. Neurourol. Urodyn. 38(3), 1009–1023 (2019).
23.
Alshiek J, Garcia B, Minassian V et al. Vaginal energy-based devices. Female Pelvic Med. Reconstr. Surg. 26(5), 287–298 (2020).
24.
Preti M, Vieira-Baptista P, Digesu GA et al. The clinical role of LASER for vulvar and vaginal treatments in gynecology and female urology: an ICS/ISSVD best practice consensus document. J. Low Genit. Tract. Dis. 23(2), 151–160 (2019).
25.
Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 94(2), 149–158 (2001).
26.
Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur. J. Pain 8(4), 283–291 (2004).
27.
American College of Obstetricians and Gynecologists. Chronic Pelvic Pain: ACOG Practice Bulletin, Number 218. Obstet. Gynecol. 135(3), e98–e109 (2020).
28.
Allaire C, Williams C, Bodmer-Roy S et al. Chronic pelvic pain in an interdisciplinary setting: 1-year prospective cohort. Am. J. Obstet. Gynecol. 218(1), 114 e1–e12 (2018).
29.
Bachmann GA, Rosen R, Arnold LD et al. Chronic vulvar and other gynecologic pain: prevalence and characteristics in a self-reported survey. J. Reprod. Med. 51(1), 3–9 (2006).
30.
Haggerty CL, Peipert JF, Weitzen S et al. Predictors of chronic pelvic pain in an urban population of women with symptoms and signs of pelvic inflammatory disease. Sex. Transm. Dis. 32(5), 293–299 (2005).
31.
Lamvu G, Williams R, Zolnoun D et al. Long-term outcomes after surgical and nonsurgical management of chronic pelvic pain: one year after evaluation in a pelvic pain specialty clinic. Am. J. Obstet. Gynecol. 195(2), 591–598 (2006).
32.
Trutnovsky G, Plieseis C, Bjelic-Radisic V, BertholinyGalvez MC, Tamussino K, Ulrich D. Vulvodynia and chronic pelvic pain in a gynecologic outpatient clinic. J. Psychosom. Obstet. Gynaecol. 40(3), 243–247 (2019).
33.
Woodburn KL, Tran MC, Casas-Puig V, Ninivaggio CS, Ferrando CA. Compliance With Pelvic Floor Physical Therapy in Patients Diagnosed With High-Tone Pelvic Floor Disorders. Female Pelvic Med Reconstr Surg. 27(2), 94–97 (2019).
34.
Shannon MB, Genereux M, Brincat C et al. Attendance at prescribed pelvic floor physical therapy in a diverse, urban urogynecology population. PM R 10(6), 601–606 (2018).
35.
Oyama IA, Rejba A, Lukban JC et al. Modified Thiele massage as therapeutic intervention for female patients with interstitial cystitis and high-tone pelvic floor dysfunction. Urology 64(5), 862–865 (2004).
36.
Agency for Healthcare Research and Quality. Effectiveness of treatments for noncyclic chronic pelvic pain in adult women. Comparative Effectiveness Review Summary Guides for Clinicians. MD, USA (2012). https://effectivehealthcare.ahrq.gov/products/pelvic-pain/research
Information & Authors
Information
Published In
Pages: 1291 - 1299
PubMed: 34490787
Copyright
© 2021 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 August 2021
Accepted: 19 August 2021
Published online: 7 September 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
An observational cohort study of pelvic floor photobiomodulation for treatment of chronic pelvic pain. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0187
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Rocío Martín-Valero, Antonia M. Ruiz-Moreno, Pablo J. Gallardo-García, María Dolores Martínez Colmena, Catalina Muñoz Pagan, Pedro González-Rojas, Paloma Ortega Quiñonero, A Randomized Controlled Pilot Trial Evaluating the Efficacy of Intravaginal and Extravaginal K-Laser Therapy as a Personalized Non-Hormonal Treatment for Genitourinary Syndrome of Menopause, Journal of Personalized Medicine, 10.3390/jpm16070378, 16, 7, (378), (2026).
- Ashley Lauver, David Addison, Jadyn Anderson, BreAnna Boyle, Halley McDonald, Daniela Rizzo, Angela Schraml, Corinne Jedynak-Bell, Trina Mansour, John Ashurst, Emerging treatment options for vaginismus: a comprehensive review of current evidence and future directions, Journal of Osteopathic Medicine, 10.1515/jom-2025-0204, (2026).
- Laura Ferreira de Rezende, Vanessa Fonseca Vilas Boas, Juliana Lenzi, Regiane Luz Carvalho, Evidencias sobre el Uso de la Fotobiomodulación para la Disfunción Sexual en Mujeres con Cáncer de Mama en Tratamiento con Hormonoterapia: Revisión Integradora de la Literatura, Revista Brasileira de Cancerologia, 10.32635/2176-9745.RBC.2026v72n1.5333ES, 72, 1, (e015333), (2026).
- Laura Ferreira de Rezende, Vanessa Fonseca Vilas Boas, Juliana Lenzi, Regiane Luz Carvalho, Evidence for the Use of Photobiomodulation in Sexual Dysfunction in Women with Breast Cancer Undergoing Hormone Therapy: Literature Integrative Review, Revista Brasileira de Cancerologia, 10.32635/2176-9745.RBC.2026v72n1.5333EN, 72, 1, (e015333), (2026).
- Laura Ferreira de Rezende, Vanessa Fonseca Vilas Boas, Juliana Lenzi, Regiane Luz Carvalho, Evidências para o Uso da Fotobiomodulação para Disfunção Sexual em Mulheres com Câncer de Mama em Uso de Hormonioterapia: Revisão Integrativa da Literatura, Revista Brasileira de Cancerologia, 10.32635/2176-9745.RBC.2026v72n1.5333, 72, 1, (2025).
- Iris Wenyu Zhou, Anthony Lin Zhang, Miranda Sin-Man Tsang, Charlie C. Xue, Vitamin D for primary dysmenorrhea and endometriosis-related pain – A systematic review of registered RCTs, PLOS ONE, 10.1371/journal.pone.0321393, 20, 4, (e0321393), (2025).
- Flavia I Antonio, Caroline Pukall, Linda McLean, Photobiomodulation therapy for the treatment of vulvar pain among those with provoked vestibulodynia: a randomized controlled trial, The Journal of Sexual Medicine, 10.1093/jsxmed/qdaf011, 22, 4, (579-587), (2025).
- Lisa A. Miller, Laser Therapy for Urinary Conditions, Laser Therapy in Veterinary Medicine, 10.1002/9781394205356.ch15, (186-192), (2025).
- Lauren Cosgriff, Aparna Ramanathan, Cheryl B. Iglesia, Pelvic Floor Disorders and Sexual Function, Obstetrics and Gynecology Clinics of North America, 10.1016/j.ogc.2024.02.001, 51, 2, (241-257), (2024).
- Isabela Oliveira Gomes, Maria Gabriela Baumgarten Kuster Uyeda, Osmar Ferreira Rangel Neto, Samantha Karlla Lopes de Almeida Rizzi, Uso do LED Terapêutico após Vaporização de Lesões Verrucosas com Laser de CO2: Relato de Caso, Revista Brasileira de Cancerologia, 10.32635/2176-9745.RBC.2024v70n1.4593, 70, 1, (2024).