Steroid switching in dystrophinopathy treatment: a US chart review of patient characteristics and clinical outcomes
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To describe reasons for switching from prednisone/prednisolone to deflazacort and associated clinical outcomes among patients with Duchenne and Becker muscular dystrophy (DMD and BMD, respectively) in the USA. Methods: A chart review of patients with DMD (n = 62) or BMD (n = 30) who switched from prednisone to deflazacort (02/2017–12/2018) collected demographic/clinical characteristics, reasons for switching, outcomes and common adverse events. Results: The mean ages at switch were 20.1 (DMD) and 9.2 (BMD) years. The primary physician-reported reasons for switching were ‘to slow disease progression’ (DMD: 83%, BMD: 79%) and ‘tolerability’ (67 and 47%). Switching was ‘very’ or ‘somewhat’ effective at addressing the primary reasons in 90–95% of patients. Conclusion: Physician-reported outcomes were consistent with deflazacort addressing patients' primary reasons for switching.
Duchenne muscular dystrophy (DMD) and Becker muscular dystrophy (BMD) are X-linked, degenerative muscle disorders caused by mutations of the DMD gene. In the USA, DMD occurs in approximately one in every 3500 male births while BMD is rarer, occurring in one in every 18,000 to 30,000 male births [1–3]. The hallmarks of the two dystrophinopathies are similar, but DMD is associated with more severe symptoms and a more aggressive clinical course than BMD [4]. Early signs, such as frequent falls and difficulty keeping up with peers, appear at age 2–3 years among those with DMD, while the appearance of symptoms in those with BMD is far more variable (i.e., age 5–60 years) [4,5]. Ambulatory function may improve in younger patients with DMD due to age-related growth and development, however, disease progression eventually reverses these gains, and loss of ambulation with progressive involvement of upper limb function usually occurs between age 9 and 14 years [6–9]. Patients with BMD typically remain ambulatory until at least age 16 years and commonly into adulthood [2]. Cardiac involvement is common in both dystrophinopathies. Few patients with DMD survive past age 30 years, although those with BMD may survive into their 40s and beyond [2,10,11].
There is currently no cure for dystrophinopathies. Corticosteroid treatment is the standard of care for patients with DMD. Its use has been associated with better functional outcomes, including delaying loss of ambulation and other symptoms, while possibly lengthening survival [12–14]. Information about the efficacy of corticosteroids in patients with BMD is more limited, but it is used in real world clinical practice [15]. In the USA, the corticosteroids prednisone/prednisolone and deflazacort are currently used to delay disease progression, and the American Academy of Neurology practice guidelines classifies both of these drugs as being ‘possibly effective’ and potentially showing benefit on markers of disease progression such as the 6-minute walk test (6MWT) and other timed function tests [12]. While prednisone/prednisolone has long been available as a generic drug, deflazacort became widely available in February 2017 when it was approved by the USA Food and Drug Administration (FDA) for the treatment of DMD [16]. Some patients with dystrophinopathy were already receiving deflazacort either through clinical trials or international importation, but FDA approval resulted in a universal choice of corticosteroid treatments for patients with dystrophinopathy [17]. Access to deflazacort may depend on insurance status, copayments and access to patient support programs. There is evidence of differences in the clinical outcomes and adverse events (AEs) associated with the use of prednisone/prednisolone or deflazacort for patients with DMD. In a randomized trial, deflazacort was associated with less weight gain than prednisone/prednisolone over the first year of treatment [13]. A recent meta-analysis of placebo arm data from Phase III clinical trials found that patients with DMD receiving deflazacort experienced significantly slower rates of functional decline over 48 weeks than those receiving prednisone/prednisolone [18]. Similar differences were observed in multi-center [13] and single-center [19] real-world studies.
In clinical practice, following FDA approval of deflazacort for DMD, some physicians switched their patients from prednisone/prednisolone to deflazacort. It is important to understand the clinical outcomes of patients who switched to deflazacort and whether switching therapies met physician expectations. In addition, there is a need to investigate the outcomes associated with corticosteroid use in a representative sample of patients from both community and academic treatment centers to complement the wealth of studies from larger academic care centers [13,19]. To this end, we assessed patients with DMD or BMD from academic and community sites across the USA who switched from prednisone to deflazacort.
Materials & methods
Study design
This study was a retrospective chart review of patients with dystrophinopathies in the USA who were treated with prednisone/prednisolone before being switched to deflazacort. Physicians treating eligible patients were recruited from a nationwide panel of neurologists. Physicians were characterized in terms of their years in practice, institution setting (academic/community), USA geographic region, annual volume of patients with dystrophinopathy and whether they participated in a deflazacort early access program (EAP). Participating physicians also completed a brief survey on their typical practices for steroid treatment of dystrophinopathies.
This study was reviewed by the New England Institutional Review Board and received approval on 31 December 2019.
Study population
Male patients who met the following physician-reported criteria at the time of data collection in early 2020 were eligible for study inclusion: genetically confirmed diagnosis of a dystrophinopathy (and subsequent diagnosis of DMD or BMD based on clinical presentation) and switched from receiving prednisone/prednisolone to deflazacort as treatment for a dystrophinopathy between February 2017 (after FDA approval) and December 2018. Patients were only eligible if they were receiving commercial deflazacort available following FDA approval; patients that were receiving deflazacort as part of the EAP were not included in this study. The study periods included the time the patient was on prednisone (prednisone period) and the time following the switch to deflazacort (deflazacort period).
Study measures
Patient and disease characteristics were entered into a web-based case report form (see the appendix for the case report form). Characteristics included ages at diagnosis of dystrophinopathy, steroid initiation and switching and at loss of ambulation (if applicable). Additional patient characteristics were collected at the at the closest clinic visit date to steroid switching during the prednisone treatment period and the last available clinic visit during the deflazacort treatment period. This information included duration of use and initial dosing level and frequency (daily vs other) for both prednisone and deflazacort. In addition, to the extent recorded in charts, data were extracted on patient height and weight, Clinical Global Impression (CGI) of improvement score, timed function tests results (rise from supine, sit to stand, 4-stair climb, 10-m walk/run, 30-feet walk/run), North Star Ambulatory Assessment, the 6MWT, Brooke scale, Performance of Upper Limb and ambulatory status as well as pulmonary and cardiac function. For each patient, physicians were also asked to report the primary reasons for switching and an overall assessment of whether switching addressed those primary reasons.
AE occurrence was collected for AEs listed on the labels of deflazacort (Cushingoid appearance, weight gain, increased appetite, upper respiratory tract infection, cough, frequent urination, hirsutism, central obesity and nasopharyngitis) and prednisone (fluid retention, alteration in glucose tolerance, elevation in blood pressure, behavioral and mood changes and increased appetite and weight gain). For each AE, whether or not the event was recorded in the medical records during the prednisone or deflazacort periods was collected.
Data collection
Data were collected by inviting physicians to participate in chart extraction via partnership with Schlesinger Group, which maintains a nationwide panel of verified physicians who have agreed to receive invitations for chart extraction and surveys. Invitations and screening questions were sent to approximately 100 physicians (including neurologists, pediatric neurologists and rehabilitation doctors) treating patients with dystrophinopathies (e.g., DMD and BMD) throughout the USA. Physicians were provided with a standardized case report form to use for chart data entry. Automated logic checks were conducted during data entry. The information was also reviewed for quality and errors by the authors, which led to several anomalous data entries being converted to missing data (see the Supplemental Methods for details on patient exclusions due to data quality concerns).
Statistical analysis
Physician characteristics were summarized overall and by practice setting; patient characteristics were summarized overall and stratified by dystrophinopathy type. The reasons patients switched from prednisone to deflazacort were summarized along with physicians' perspective on the effectiveness of switching to deflazacort. Information collected during each steroid period, such as the CGI of improvement and AE occurrence, was described for the subgroup with greater than or equal to 3 months of treatment on both prednisone and deflazacort. Further subgroup analyses were also conducted stratified by reason for switch.
Results
Physician characteristics
A total of 55 neurologists (20% identifying as pediatric neurologists) contributed data for 104 males with dystrophinopathies who switched from prednisone to deflazacort (Table 1). The regions of practice were distributed across the USA. On average, the physicians had approximately 15 years in clinical practice and treated 37 patients with dystrophinopathies per year. The most common practice setting was private community institutions (40%) followed by private academic institutions (29%). Physician characteristics were generally similar across the various practice settings, although those in academic settings had a higher proportion of non-ambulatory patients under their care than those in the community setting (53 vs 42% of patients annually). Approximately half of the physicians had participated in EAPs for deflazacort; this percentage was higher among physicians in academic settings (59%) versus community settings (35%).
| Physicians | Overall (n = 55) | Community setting (n = 27) | Academic setting (n = 28) |
|---|---|---|---|
| Specialty, n (%) | |||
| – Neurologist | 44 (80.00) | 22 (81.48) | 22 (78.57) |
| – Pediatric neurologist | 11 (20.00) | 5 (18.52) | 6 (21.43) |
| Years in practice (n) | |||
| – Mean (SD) | 15.05 (6.04) | 15.41 (5.94) | 14.71 (6.22) |
| Practice setting, n (%) | |||
| – Private community institution | 22 (40.00) | 22 (81.48) | 0 (0.00) |
| – Private academic institution | 16 (29.09) | 0 (0.00) | 16 (57.14) |
| – Public academic institution | 12 (21.82) | 0 (0.00) | 12 (42.86) |
| – Public community institution | 5 (9.09) | 5 (18.52) | 0 (0.00) |
| Sex, n (%) | |||
| – Male | 37 (74.00) | 17 (70.83) | 20 (76.92) |
| – Female | 13 (26.00) | 7 (29.17) | 6 (23.08) |
| Practice region, n (%) | |||
| – Midwest | 16 (30.77) | 6 (24.00) | 10 (37.04) |
| – South | 16 (30.77) | 7 (28.00) | 9 (33.33) |
| – West | 12 (23.08) | 7 (28.00) | 5 (18.52) |
| – Northeast | 8 (15.38) | 5 (20.00) | 3 (11.11) |
| Patients with dystrophinopathies per year (n) | |||
| – Mean (SD) | 37.24 (30.31) | 35.89 (30.20) | 38.54 (30.91) |
| Patients non-ambulatory (%) | |||
| – Mean (SD) | 47.56 (24.22) | 42.19 (19.26) | 52.75 (27.55) |
| Participation in the deflazacort early-access program, n (%) | |||
| – Yes | 20 (47.62) | 7 (35.00) | 13 (59.09) |
| – No | 22 (52.38) | 13 (65.00) | 9 (40.91) |
| Average completion time per chart (h)‡ | |||
| – Mean (SD) | 1.49 (2.25) | 1.38 (1.81) | 1.59 (2.61) |
| – Patients | Overall (n = 92) | BMD (n = 30) | DMD (n = 62) |
| Race, n (%) | |||
| – White | 68 (78.16) | 25 (86.21) | 43 (74.14) |
| – Hispanic | 9 (10.34) | 1 (3.45) | 8 (13.79) |
| – Black or African–American | 5 (5.75) | 2 (6.90) | 3 (5.17) |
| – More than one race | 4 (4.60) | 0 (0.00) | 4 (6.90) |
| Ethnicity, n (%) | |||
| – Non-Hispanic | 69 (85.19) | 27 (96.43) | 42 (79.25) |
| – Hispanic | 12 (14.81) | 1 (3.57) | 11 (20.75) |
| Insurance type, n (%) | |||
| – Private | 68 (82.93) | 23 (82.14) | 45 (83.33) |
| – Non-private | 14 (17.07) | 5 (17.86) | 9 (16.67) |
| Age at initial presentation of dystrophinopathy symptoms (years) | |||
| – Mean (SD) | 5.46 (4.19) | 8.27 (5.74) | 4.10 (2.19) |
| Disease duration prior to prednisone/prednisolone recommendation§ (years) | |||
| – Mean (SD) | 0.29 (5.89) | 0.48 (9.81) | 0.66 (2.37) |
| Loss of ambulation, n (%) | |||
| – Yes | 20 (21.74) | 5 (16.67) | 15 (24.19) |
| – No | 72 (78.26) | 25 (83.33) | 47 (75.81) |
| Age at loss of ambulation (years) | |||
| – Mean (SD) | 11.25 (10.37) | 18.15 (18.96) | 8.95 (4.54) |
| Mutation type, n (%) | |||
| – Deletion amenable to exon skipping | 22 (37.29) | 6 (28.57) | 16 (42.11) |
| – Deletion not amenable to exon skipping | 22 (37.29) | 7 (33.33) | 15 (39.47) |
| – Duplication | 7 (11.86) | 3 (14.29) | 4 (10.53) |
| – Nonsense | 5 (8.47) | 2 (9.52) | 3 (7.89) |
| – Other | 3 (5.08) | 3 (14.29) | 0 (0.00) |
| Mutated exons, n (%) | |||
| – 1 | 9 (17.31) | 9 (47.37) | 0 (0.00) |
| – 51 | 8 (15.38) | 1 (5.26) | 7 (21.21) |
| – 25 | 3 (5.77) | 3 (15.79) | 0 (0.00) |
| – 44–55 | 4 (7.69) | 0 (0.00) | 4 (12.12) |
| – 2 | 3 (5.77) | 0 (0.00) | 3 (9.09) |
| – Other¶ | 3 (5.77) | 1 (5.26) | 2 (6.06) |
†
Percentages are calculated out of the subgroup of patients with non-missing responses.
‡
Average survey completion times greater than 1 day (24 h) were set to missing; these times likely represent instances of physicians opening the survey, pausing midway through and returning at a later date and are not reflective of the typical total time to complete a chart.
§
Genetically confirmed.
¶
The ‘other’ mutation type category included patients with the following mutated exons: 3, 4, 5, 7, 8, 10, 12, 15, 20, 23, 26, 29, 40, 41, 44, 46, 47, 48, 53, 55, 58, 66 and 70. In each of these groups, there were fewer than three patients.
BMD: Becker muscular dystrophy; DMD: Duchenne muscular dystrophy; SD: standard deviation.
Patient characteristics
Among the 92 patients with chart data included in the study, 62 had a diagnosis of DMD and 30 had a diagnosis of BMD recorded in their charts (Table 1). Patients were predominately white (overall: 78%, DMD: 74%, BMD: 86%) and non-Hispanic (85%, 79% and 96%, respectively). The majority were privately insured (>80% across groups). The average age at the initial presentation of dystrophinopathy symptoms was 4.1 years for patients with DMD and 8.3 years for patients with BMD. Loss of ambulation was more common among patients with DMD (24%) than with BMD (17%), with mean ages at loss of ambulation of 9 and 18 years, respectively. Mutations amenable to exon skipping were more prevalent among patents with DMD, which is consistent with BMD being an in-frame mutation.
Reasons for switching to deflazacort
The most common reasons for switching to deflazacort are listed in Table 2. For patients with DMD, physicians reported ‘desire to slow disease progression’ as one of the top two reasons for switching to deflazacort in 83% of patients and ‘tolerability issues’ in 67% of patients. In approximately a third of patients, physicians reported ‘parent/caregiver preference/request’ or ‘patient preference/request’ as one of the top two reasons for switching. Over 95% of physicians said they viewed switching to deflazacort as ‘very effective’ or ‘somewhat effective’ for their patients with DMD.
| Parameter | BMD (N = 30) | DMD (N = 62) |
|---|---|---|
| Most common reasons for switching to deflazacort† | ||
| – Desire to slow disease progression | 23 (79.31%) | 49 (83.05%) |
| – Tolerability issues | 14 (46.67%) | 41 (67.21%) |
| – Parent/caregiver preference or request | 11 (37.93%) | 20 (33.33%) |
| – Patient preference or request | 11 (37.93%) | 12 (20.00%) |
| Overall perspective | ||
| Physician's perspective on the effectiveness of switching to deflazacort | ||
| – Somewhat effective | 19 (63.33%) | 36 (58.06%) |
| – Very effective | 8 (26.67%) | 24 (38.71%) |
| – Not effective | 3 (10.00%) | 2 (3.23%) |
†
Percentages are calculated out of the subgroup of patients with non-missing responses.
BMD: Becker muscular dystrophy; DMD: Duchenne muscular dystrophy.
Similarly, for patients with BMD, physicians reported ‘desire to slow disease progression’ as one of the top two reasons for switching to deflazacort in 79% of patients and ‘tolerability issues’ in 47% of patients. Physicians reported ‘parent/caregiver preference/request' and/or 'patient preference/request' as one of the top two reasons for switching in 38% of patients. Overall, 90% of physicians said they viewed switching to deflazacort as 'very effective' or 'somewhat effective' for their patients with BMD.
Steroid-specific patient characteristics
Patients with DMD
Patient characteristics during the prednisone and deflazacort treatment periods are summarized in Table 3. At prednisone initiation (mean age: 6 years), 36 patients with DMD had weight-based dosing information available, with an average dose of 0.8 mg/kg. By the time of the latest visit recorded in the prednisone treatment period, the average dose was approximately 0.9 mg/kg. The majority of patients with weight-based dosing available were prescribed a daily regimen (n = 35 [95%]). At the time of switch, patients had been treated with prednisone for an average of 2.7 years, with a range from about a month to 13 years.
| Parameters | BMD | DMD | ||
|---|---|---|---|---|
| Prednisone | Deflazacort | Prednisone | Deflazacort | |
| Age at initiation (years) | ||||
| – Mean (SD) | 13.40 (12.83) | 20.10 (11.84) | 6.15 (4.46) | 9.18 (6.43) |
| – Median | 9.83 | 18.37 | 5.06 | 7.64 |
| – Range | (0.83, 51.82) | (5.46, 53.08) | (0.91, 28.23) | (1.58, 38.60) |
| – Total non-missing, n | 30 | 30 | 62 | 62 |
| Duration of use (years) | ||||
| – Mean (SD) | 5.26 (4.97) | 0.45 (0.29) | 2.66 (3.21) | 0.51 (0.35) |
| – Median | 4.34 | 0.44 | 1.60 | 0.52 |
| – Range | (0.10, 19.66) | (0.00, 0.96) | (0.07, 13.06) | (0.00, 1.00) |
| Total non-missing, n | 30 | 30 | 62 | 62 |
| Initial dosing level (mg/kg) | ||||
| – Mean (SD) | 0.84 (0.14) | 0.89 (0.14) | 0.83 (0.29) | 0.92 (0.28) |
| – Median | 0.75 | 0.90 | 0.75 | 0.90 |
| – Range | (0.75, 1.20) | (0.50, 1.20) | (0.30, 2.00) | (0.50, 2.00) |
| Total non-missing, n | 15 | 16 | 36 | 42 |
| Initial dosing frequency, n (%) | ||||
| – Daily | 9 (60.00) | 12 (85.71) | 35 (94.59) | 13 (65.00) |
| – Other | 6 (40.00) | 2 (14.29) | 2 (5.41) | 7 (35.00) |
| – Total non-missing, n | 15 | 14 | 37 | 20 |
| Patient weight (kg) | ||||
| – Mean (SD) | 46.74 (22.62) | 48.51 (23.58) | 30.57 (11.03) | 32.01 (9.54) |
| – Range | (13.61, 90.72) | (13.61, 95.25) | (17.00, 60.00) | (13.15, 53.00) |
| – Total non-missing, n | 22 | 22 | 33 | 31 |
| Patient height (cm) | ||||
| – Mean (SD) | 158.29 (8.66) | 162.25 (11.73) | 126.65 (19.93) | 131.91 (16.55) |
| – Range | (137.16, 170.18) | (139.70, 190.50) | (91.44, 172.72) | (96.52, 162.56) |
| – Total non-missing, n | 14 | 14 | 21 | 19 |
BMD: Becker muscular dystrophy; DMD: Duchenne muscular dystrophy; SD: standard deviation.
At deflazacort initiation (mean age: 9 years old), 42 patients with DMD had weight-based dosing information available, with an average dose of 0.9 mg/kg. By the time of the latest visit recorded in the deflazacort treatment period, the average dose was still 0.9 mg/kg. Thirty patients (71% of those with data available) had initial doses in the range of 0.85–0.95 mg/kg. At the time of chart data extraction, patients had been treated with deflazacort for an average of 6 months, with a range of 1 day to 1 year.
Patients with BMD
At prednisone initiation (mean age: 13 years), 15 patients with BMD had weight-based dosing information available, with an average dose of 0.8 mg/kg. By the time of the latest visit recorded in the prednisone period, the average dose was 0.9 mg/kg. The majority of patients with weight-based dosing available were prescribed a daily regimen (n = 9 [60%]). At the time of switch, patients had been treated with prednisone for an average of 5.3 years, with a range from about a month to almost 20 years.
At deflazacort initiation (mean age: 20 years), 14 patients with BMD had weight-based dosing information available with an average dose of 0.9 mg/kg. By the time of the latest visit recorded in the deflazacort period, the average dose was still 0.9 mg/kg. The majority of patients with weight-based dosing available were prescribed a daily regimen (n = 9 [56%]). At the time of chart data extraction, patients had been treated with deflazacort for an average of almost 6 months, with a range of 1 day to almost 1 year.
CGI scores for improvement
The physician-recorded CGI scores for improvement among patients treated with both prednisone and deflazacort for ≥3 months are shown in Figure 1A (DMD) & B (BMD). Among patients with DMD with CGI data available in charts (n = 23 for the prednisone period and n = 22 for deflazacort), 18.2% of those receiving deflazacort had physician-reported measures of ‘very much improved’ compared with 0% of those on prednisone. Conversely, 4.3% of patients with DMD on prednisone had scores of ‘much worse’ compared with 0% of those on deflazacort. A similar trend of improvement was noted for patients with BMD (n = five patients with CGI data available): 100% of patients receiving deflazacort were scored by physicians as ‘very much improved’ or ‘much improved’, compared with 0% of those on prednisone.
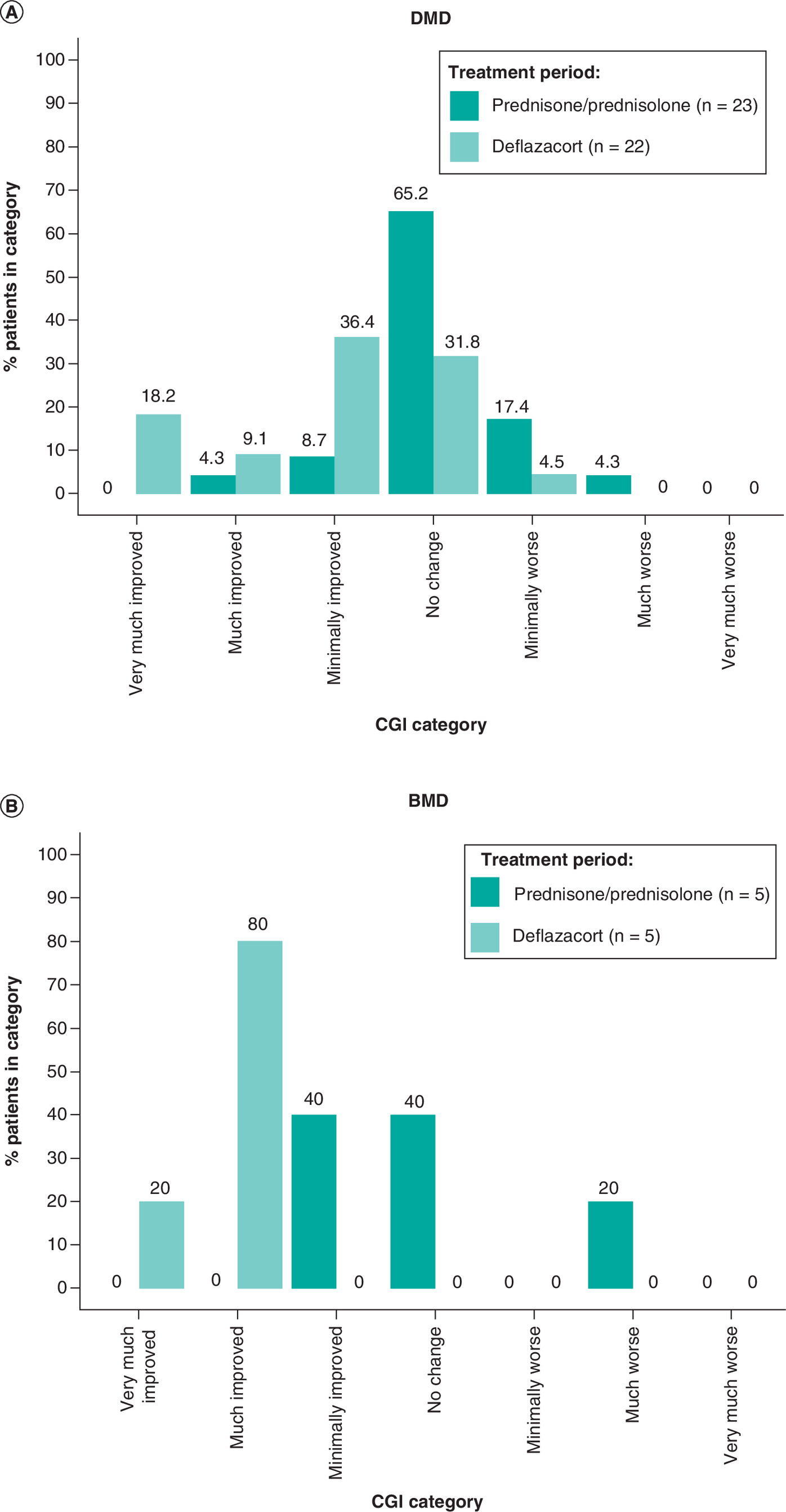
Figure 1. CGI scores for patients.
(A) DMD or (B) BMD treated with prednisone or deflazacort for ≥3 months.
BMD: Becker muscular dystrophy; CGI: Clinical Global Impression; DMD: Duchenne muscular dystrophy.
Adverse effects
AEs with the highest prevalence recorded in the charts among patients treated with prednisone and deflazacort for ≥3 months are shown in Figure 2A (DMD) & B (BMD). For patients with DMD, weight gain, increased appetite, fluid retention, central obesity, increased blood pressure and decreased bone density were all more common during the prednisone period compared with the deflazacort period (Figure 2A). Notably, no patients with DMD had recorded decreased bone density or fluid retention during the deflazacort period. A similar trend was observed among patients with BMD (Figure 2B), and all AEs were more common during the prednisone period. No patients with BMD had recorded central obesity, increased blood pressure or decreased bone density during the deflazacort period.
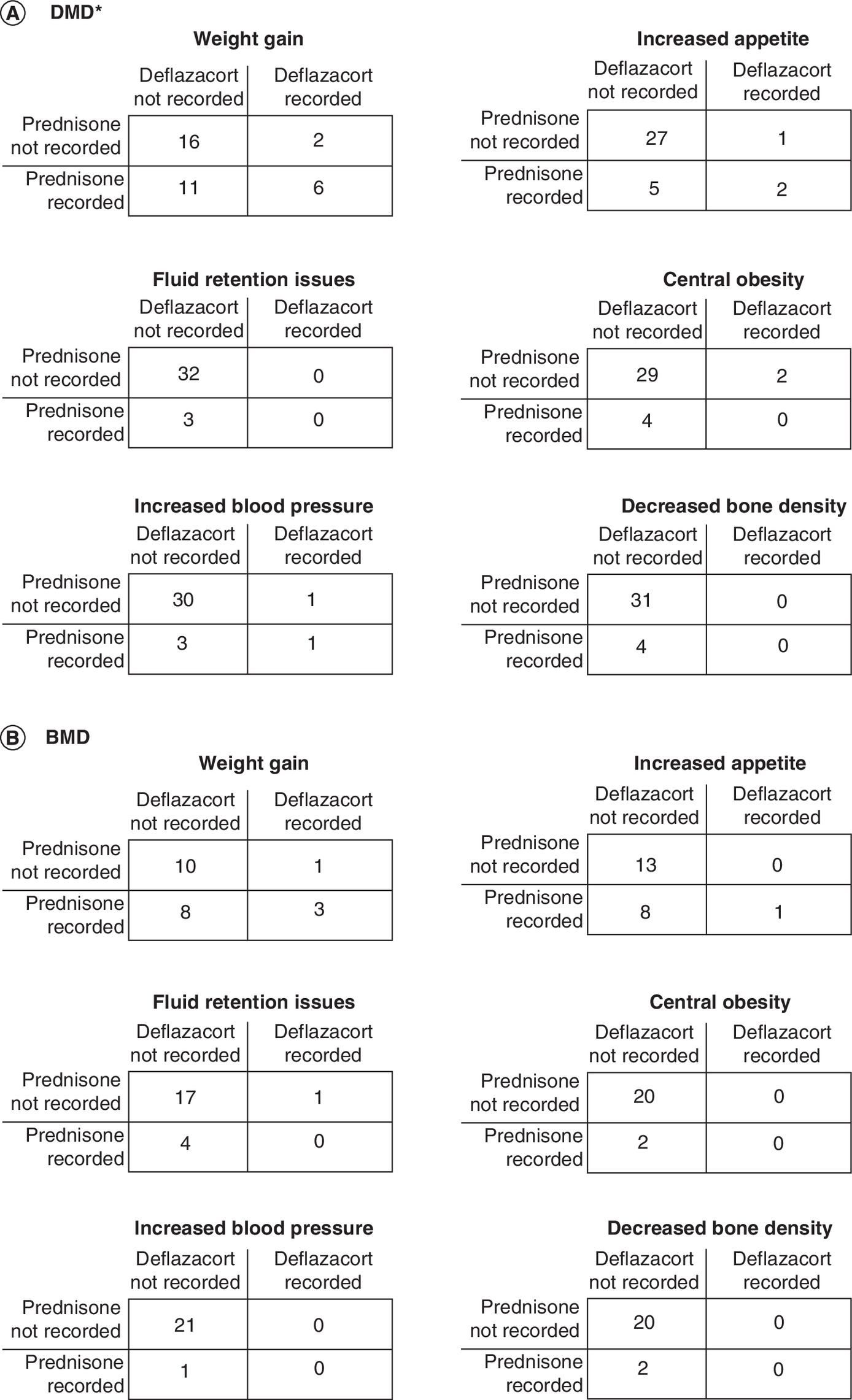
Figure 2. Adverse events among patients.
(A) DMD† or (B) BMD‡ treated with prednisone and deflazacort for ≥3 months. Prednisone outcomes are juxtaposed with deflazacort outcomes in this figure, but these counts cannot be considered a head-to-head comparison because patients were treated for different amounts of time, and this study only includes patients who switched from prednisone to deflazacort.
†There were n = 35 patients in the prednisone/prednisolone period and n = 35 in the deflazacort period.
‡There were n = 22 patients in the prednisone/prednisolone period and n = 22 in the deflazacort period.
BMD: Becker muscular dystrophy; DMD: Duchenne muscular dystrophy.
In addition to the six most prevalent AEs recorded in medical records, we investigated reported behavioral/mood changes given the importance of this outcome to families and caregivers [20]. Behavioral/mood changes were recorded as an AE for four patients. Of these, three patients reported the AE during the prednisone and one during the deflazacort treatment periods. All four patients reported mild severity for this AE. Of the patients who reported experiencing behavioral/mood changes while being treated with prednisone, one discontinued treatment, one switched to a different therapy and one adjusted the dosage of the existing treatment. The chart of the patient who reported the behavioral/mood changes while being treated with deflazacort stated that no change in deflazacort treatment was made.
CGI scores for patients who switched due to a desire to slow disease progression
The physician-recorded CGI scores of the subset of patients who switched to deflazacort due to the desire to slow disease progression, and received deflazacort for ≥3 months, are shown in Figure 3. The results indicate that patients largely experienced improvement after switching to deflazacort, with approximately 43% achieving scores of ‘very much improved’ or ‘much improved’. No patients were recorded with worsening disease symptoms after switching to deflazacort.
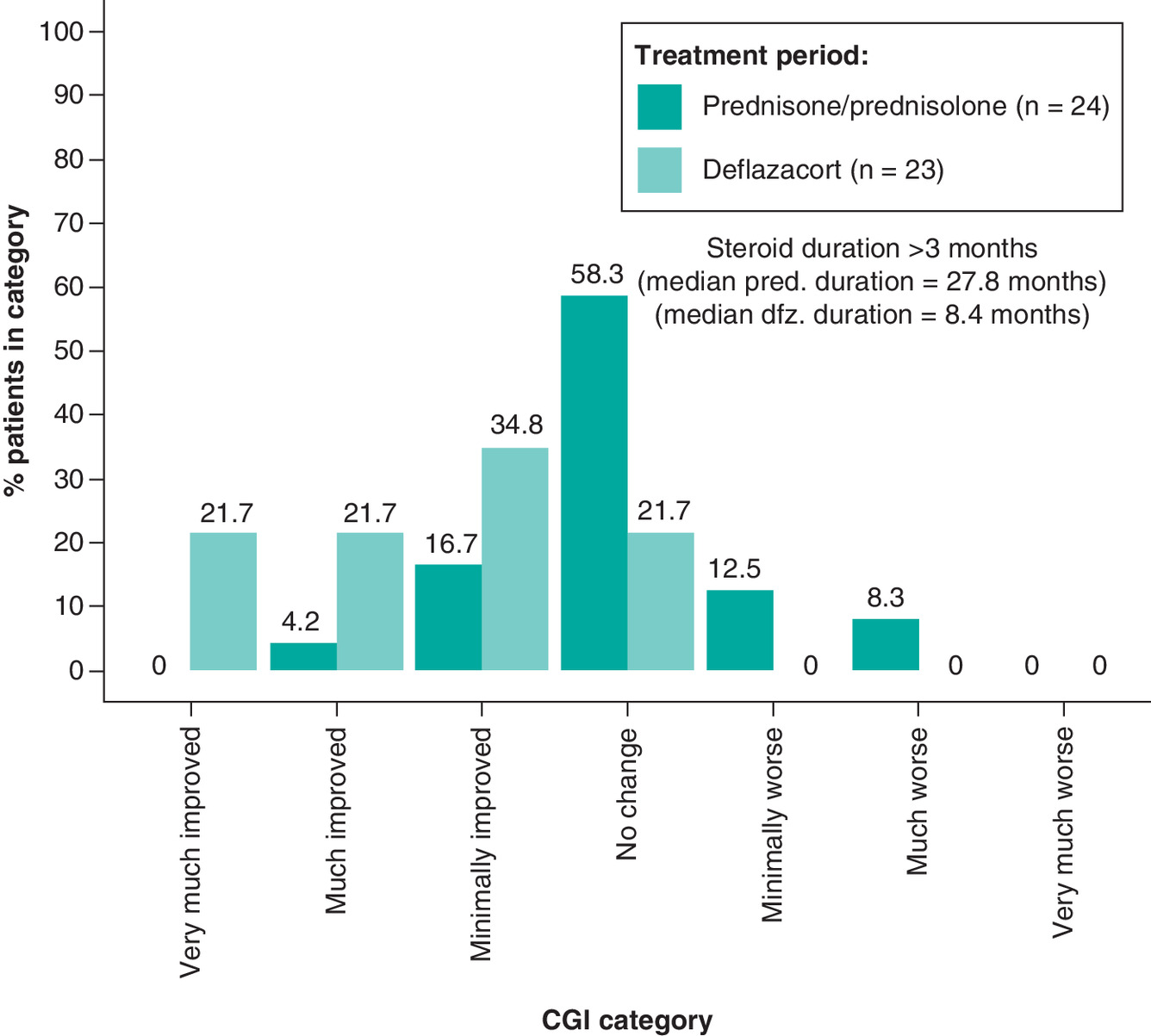
Figure 3. CGI scores for patients treated with prednisone and deflazacort for ≥3 months and switched due to a desire to slow disease progression.
CGI: Clinical Global Impression.
AEs among patients who switched due to tolerability issues
The AEs among patients treated with prednisone who switched to deflazacort due to tolerability issues, and received deflazacort for ≥3 months, are shown in Figure 4. Across all six AEs, patients experienced fewer AEs during the deflazacort period compared with the prednisone period. The most common AE in both periods was weight gain, although the number of patients with this AE was nearly half that in the deflazacort period. No patients experienced decreased bone density during the deflazacort period.

Figure 4. Adverse events among patients treated with prednisone and deflazacort for ≥3 months who switched due to tolerability issues.
†Prednisone outcomes are juxtaposed with deflazacort outcomes, but these counts cannot be considered a head-to-head comparison because patients were treated for different amounts of time and this study only included patients who switched from prednisone to deflazacort.
‡There were n = 36 patients in the prednisone/prednisolone period and n = 36 in the deflazacort period.
Data availability
As shown in Supplementary Table 1, there was a lack of consistency regarding the collection of ambulatory, pulmonary and cardiac measures across treatment centers and practices. In both the prednisone and deflazacort treatment periods, overall ambulatory status was commonly collected (i.e., in 87 and 88% of patients, respectively) while more specific timed function tests were rarely administered with the exception of rise from supine time, which was collected in roughly a quarter of patients across both periods.
Discussion
DMD and BMD are progressively debilitating dystrophinopathies for which corticosteroid treatment is the current standard of care. Since deflazacort was approved by the FDA in 2017, more patients with dystrophinopathies have switched from prednisone to deflazacort. It is important to understand the real-world clinical outcomes of these patients both in terms of efficacy and safety. This retrospective chart review of 92 patients with DMD or BMD who switched from prednisone to deflazacort during the period from February 2017 to December 2018 found that the primary reasons physicians switched patients to deflazacort were the desire to slow disease progression and tolerability issues on prednisone. The results indicated that, on average, physician-reported outcomes were consistent with deflazacort addressing the primary reasons for switching, with the CGI results supporting this trend in the subset of patients with available data. While the shorter deflazacort treatment period (i.e., follow-up time after switching) available after switching but prior to chart extraction does not allow for a direct comparison of AE incidence across the two treatment periods, on average, patients with DMD and BMD experienced fewer AEs after switching to deflazacort compared with prednisone.
Both prednisone and deflazacort have well-known safety profiles, and while corticosteroids improve muscle function and strength, long-term use as a treatment for dystrophinopathies may result in weight gain, decreased bone density, elevated blood pressure, increased appetite, central obesity or Cushingoid appearance, among other possible AEs [21,22]. These AEs are listed on the labels of prednisone and deflazacort [16,23], and have been noted as common ones in a Cochrane review of the literature by Matthews et al. [22], justifying their focus in the present study. In general, the typical AEs associated with corticosteroid use, particularly in the case of weight gain, were more common during the prednisone period versus the deflazacort period. A similar finding regarding lower incidence of weight gain among patients with DMD using deflazacort compared with prednisone was also reported in a placebo-controlled Phase III trial by Griggs et al. [13]. Longer-term follow-up will be needed to fully characterize the tolerability of switching to deflazacort in real-world clinical practice.
The present results are also consistent with the trend of improvement reported by Griggs et al. among patients with DMD receiving deflazacort or prednisone; over 52 weeks on therapy, those using deflazacort (0.9 mg/kg) demonstrated continued improvements in muscle strength while those on prednisone experienced worsening of muscle strength [13]. Similarly, a recent study of patients with DMD treated at Cincinnati Hospital Medical Center reported that patients who received deflazacort were older at loss of ambulation (i.e., it was delayed) and had better ambulatory function compared with prednisone-treated patients [19]. A 2020 systematic literature review of the safety and efficacy of deflazacort for DMD reported that deflazacort was associated with improved functional outcomes, delayed onset of cardiomyopathy, reduction in scoliosis surgery and improved survival [24]. Thus, the trend exhibited in the present study of better CGI scores following deflazacort treatment is consistent with the prior literature which assessed specific functional changes in clinical trials and prospective databases, and contributes a new perspective specific to patients who switched from prednisone to deflazacort in a broad, representative sample of clinical practice.
An important contribution of this study is an understanding as to whether expectations were met after switching from prednisone to deflazacort. In both patient cohorts, over 90% of physicians said they viewed the effectiveness of switching to deflazacort as ‘very’ or ‘somewhat’ effective for their patients with dystrophinopathy. In the analysis of outcomes based on physician-reported CGI in the subset of patients with this data available, patients who switched due to desire to slow disease progression appear to have improved on average. Similarly, patients who switched due to tolerability issues with prednisone appear to have experienced fewer AEs on average during their time on deflazacort compared with prednisone. Thus, during the first few months after switching to deflazacort, physicians' expectations for their patients' outcomes after switching to deflazacort appear to have been met for the majority of patients.
This study benefits from several strengths, including the breadth of the data. Charts were collected from all regions of USA, across a broad and representative set of practices (e.g., both academic and community) to form the most representative real-world evidence available. These centers are not always the ones contributing to well-regarded high-quality databases (e.g., the Cooperative International Neuromuscular Research Group [CINRG]). Prior natural history studies of patients with DMD may be considered to have used less representative data sources as they are primarily gathered from a single database/setting (e.g., Cincinnati Children's Medical Hospital), include patients outside the USA, and/or focus on larger academic centers (e.g., CINRG and the ongoing FOR-DMD trial). Due to the breadth and variety of practices included in this study, there was heterogeneity in the availability of data with regards to outcome measurements across sites contributing the charts. In particular, there were no standardized measurements of function or ambulation collected across sites, illustrating that in real-world clinical practice these outcomes (i.e., North Star Ambulatory Assessment, timed function tests, etc.) may not be routinely collected (see Supplementary Table 1). In addition, the present study also included patients with BMD, a rare dystrophinopathy, contributing vital information regarding the use of corticosteroids in this under-studied population.
The present results should also be interpreted in light of several limitations. First, as with all retrospective chart review studies, there is the possibility of missing data or errors in coding. However, the data were reviewed following chart abstraction and a conservative approach was taken to either censure aspects of data suspected to be in error or the entire patient chart. Second, there was marked heterogeneity in what was measured and recorded in charts, and very few functional measures were measured consistently across all centers. For instance, timed function tests and measures of cardiac and lung function were not available in the majority of cases (see Supplementary Table 1) and were thus not summarized in this study. This is a result of the absence of standardized instruments to measure key outcomes among patients with DMD and BMD, as well as inconsistent testing practices in the real world. Third, the short follow-up on deflazacort may not have allowed enough time to observe all changes in disease progression or the onset of new AEs. In addition, the assessments of AEs were based on what was available in patient charts, so prevalence may have been underestimated. In particular, bone density scans are often conducted annually and, thus, there may not have been time to observe changes in bone density during the deflazacort period. Longer-term studies of patients with dystrophinopathies who switch to deflazacort are needed to support the present findings.
Conclusion
In conclusion, in this real-world retrospective chart review of patients with DMD or BMD who switched to deflazacort from prednisone, the majority of switching aimed to improve benefit–risk and delay disease progression. During the 6-month average follow-up after switching, physician-reported outcomes were consistent with deflazacort addressing the primary reasons for switching. Real-world recording of specific clinical measures was heterogeneous across care centers but, when measures were available, they were consistent with the overall physician assessment. Future real-world studies with longer follow-up times on deflazacort are needed to comprehensively characterize the impact of switching from prednisone to deflazacort on patients with dystrophinopathy.
Future perspective
As deflazacort is now approved by the FDA for DMD, patients in the USA with dystrophinopathies now have the universal choice to switch from prednisone to deflazacort if they wish. Our study provides a preliminary snapshot of switching behavior, the reasons for switching and associated clinical outcomes in the real world. Overall, on average, the switch to deflazacort addressed the physician-recorded reasons for switching. Additional real-world data is needed to understand longer-term treatment patterns and outcomes, and future studies would benefit from greater consistency in real-world clinical measures.
•
Deflazacort was recently approved for Duchenne muscular dystrophy (DMD) in the USA, providing patients with dystrophinopathies the opportunity to switch from prednisone/prednisolone steroid treatment to deflazacort.
•
This real-world study describes reasons for switching from prednisone/prednisolone to deflazacort and associated clinical outcomes among patients with DMD or Becker muscular dystrophy (BMD) in the USA.
•
Demographic/clinical characteristics, reasons for switching, outcomes (i.e., Clinical Global Impression of Improvement [CGI]) and common adverse events (AEs) were summarized from a chart review of 55 neurologists treating patients with DMD or BMD who switched from prednisone to deflazacort (02/2017–12/2018); a subgroup with ≥3 months on both steroids was described separately.
•
For patients with DMD (n = 62) and BMD (n = 30), the primary reasons physicians listed for switching were ‘desire to slow disease progression’ (83 and 79%, respectively) and ‘tolerability issues’ (67 and 47%).
•
Switching was ‘very’ or ‘somewhat’ effective at addressing the primary reasons in 90–95% of patients and AE occurrence was lower during the deflazacort period for both patient cohorts.
•
These findings were similar for the subgroup (n = 57) with ≥3 months on both steroids.
•
Among the charts with CGI recorded, most patients' disease progression improved or stabilized.
•
Thus, the majority of switching from prednisone to deflazacort aimed to improve benefit–risk and delay progression, and physician-reported outcomes were consistent with deflazacort addressing the primary reasons for switching.
Author contributions
All authors contributed to the conception or design of the work; the acquisition, analysis or interpretation of data for the work; the drafting the work or revising it critically for important intellectual content; and approved the final version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Financial & competing interests disclosure
This study was funded by PTC Therapeutics, Inc. C Santos, B Pfister, R Able are employees of PTC Therapeutics, Inc. and hold stock/options. J Marden, H Lane, M Somma, J Zhao and J Signorovitch are employees of Analysis Group, Inc., which has received consulting fees from PTC Therapeutics, Inc. J Parsons has received research funding from PTC Therapeutics, Inc., Sarepta and Pfizer, and has received consulting fees from PTC Therapeutics, Inc. and Sarepta unrelated to this work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by S Batts, an employee of Analysis Group, Inc. Support for this assistance was provided by PTC Therapeutics, Inc.
Ethical conduct of research
This study was reviewed by the New England Institutional Review Board and received approval on 31 December 2019. The authors state that they have followed the principles outlined in the Declaration of Helsinki for all human experimental investigations.
Data sharing statement
Data available on request from the authors.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplemental materials.docx)
- Download
- 17.09 KB
References
Papers of special note have been highlighted as: • of interest
1.
Hoffman EP, Brown RH Jr, Kunkel LM. Dystrophin: the protein product of the Duchenne muscular dystrophy locus. Cell 51(6), 919–928 (1987).
2.
National Institute of Health (Genetic and Rare Disease Information Center). Becker muscular dystrophy. https://rarediseases.info.nih.gov/diseases/5900/becker-muscular-dystrophy
3.
Romitti PA, Zhu Y, Puzhankara S et al. Prevalence of Duchenne and Becker muscular dystrophies in the United States. Pediatrics 135(3), 513–521 (2015).
4.
Darras BT, Menache-Starobinski CC, Hinton V, Kunkel LM. Chapter 30 – dystrophinopathies. In: Neuromuscular Disorders of Infancy, Childhood, and Adolescence (2nd Edition). Darras BT, Jones HR, Ryan MM, Devivo DC (Eds). Academic Press, CA, USA, 551–592 (2015).
5.
Emery AEH, Muntoni F, Quinlivan R. Duchenne Muscular Dystrophy (4th Edition). Oxford University Press, UK (2015).
6.
Ricotti V, Ridout DA, Scott E et al. Long-term benefits and adverse effects of intermittent versus daily glucocorticoids in boys with Duchenne muscular dystrophy. J. Neurol. Neurosurg. Psych. 84(6), 698–705 (2013).
• Assessed the use of glucocorticoids in Duchenne muscular dystrophy (DMD) in the UK and compared the benefits and risk of daily versus intermittent prednisolone regimens. Adverse effects (AEs) were more common in daily versus intermittant use, but boys with intermmitent use declined faster (per NorthStar Ambulatory Assessment) after age 7 years.
7.
Pane M, Fanelli L, Mazzone ES et al. Benefits of glucocorticoids in non-ambulant boys/men with Duchenne muscular dystrophy: a multicentric longitudinal study using the Performance of Upper Limb test. Neuromuscul. Disord. 25(10), 749–753 (2015).
• Assessed the effect of glucocorticoids on upper limb function (per performance of upper limb test) in 91 non-ambulant DMD boys and adults aged between 11 and 26 years. The 12-month changes ranged between -20 and 4 (mean -4.4), with -3.79 in the glucocorticoid group, -5.52 in those who discontinued at loss of ambulation and -4.44 in the treatment-naïve group.
8.
Mazzone E, Bianco F, Main M et al. Six minute walk test in type III spinal muscular atrophy: a 12-month longitudinal study. Neuromuscul. Disord. 23(8), 624–628 (2013).
9.
Seferian AM, Moraux A, Annoussamy M et al. Upper limb strength and function changes during a one-year follow-up in non-ambulant patients with Duchenne muscular dystrophy: an observational multicenter trial. PLoS ONE 10(2), e0113999 (2015).
10.
Passamano L, Taglia A, Palladino A et al. Improvement of survival in Duchenne muscular dystrophy: retrospective analysis of 835 patients. Acta Myol. 31(2), 121–125 (2012).
11.
Muntoni F, Torelli S, Ferlini A. Dystrophin and mutations: one gene, several proteins, multiple phenotypes. Lancet Neurol. 2(12), 731–740 (2003).
12.
Gloss D, Moxley RT 3rd, Ashwal S, Oskoui M. Practice guideline update summary: corticosteroid treatment of Duchenne muscular dystrophy: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 86(5), 465–472 (2016).
13.
Griggs RC, Miller JP, Greenberg CR et al. Efficacy and safety of deflazacort vs prednisone and placebo for Duchenne muscular dystrophy. Neurology 87(20), 2123–2131 (2016).
• This Phase III, double-blind, randomized study assessed the safety and efficacy of deflazacort and prednisone versus placebo in 196 boys with DMD (aged 5–15 years). After 12 weeks of treatment, prednisone and both doses of deflazacort improved muscle strength versus placebo; at 52 weeks, deflazacort was associated with less weight gain than prednisone.
14.
Birnkrant DJ, Bushby K, Bann CM et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation, endocrine, and gastrointestinal and nutritional management. Lancet Neurol. 17(3), 251–267 (2018).
15.
Matthews DJ, James KA, Miller LA et al. Use of corticosteroids in a population-based cohort of boys with Duchenne and Becker muscular dystrophy. J. Child Neurol. 25(11), 1319–1324 (2010).
16.
United States Food and Drug Administration. Highlights of prescribing information: emflaza (deflazacort). https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/208684s000,208685s000lbl.pdf
17.
Center for Drug Evaluation and Research. Approval package for Emflaza (deflazacort). https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/208684,208685Orig1s000Approv.pdf
18.
Mcdonald CM, Sajeev G, Yao Z et al. Deflazacort vs prednisone treatment for Duchenne muscular dystrophy: a meta-analysis of disease progression rates in recent multicenter clinical trials. Muscle Nerve 61(1), 26–35 (2020).
• This meta-analysis characterized disease progression among boys receiving deflazacort versus prednisone/prednisolone in two DMD clinical trials. It found that deflazacort-treated patients experienced significantly lower functional decline over 48 weeks.
19.
Marden JR, Freimark J, Yao Z, Signorovitch J, Tian C, Wong BL. Real-world outcomes of long-term prednisone and deflazacort use in patients with Duchenne muscular dystrophy: experience at a single, large care center. J. Comp. Eff. Res. 9(3), 177–189 (2020).
• Assessed outcomes among 435 boys with DMD receiving deflazacort or prednisone in real-world practice. Deflazacort was also associated with a lower risk of scoliosis and better ambulatory function, greater % lean body mass, shorter stature and lower weight, after adjusting for age and steroid duration.
20.
Poysky J. Behavior patterns in Duchenne muscular dystrophy: Report on the Parent Project Muscular Dystrophy behavior workshop 8–9 of December 2006, PA, USA. Neuromuscul. Disord. 17(11), 986–994 (2007).
21.
Torgan C. National Institute of Arthritis and Musculoskeletal and Skin Diseases. Optimizing steroid treatment for Duchenne muscular dystrophy. https://www.niams.nih.gov/newsroom/spotlight-on-research/optimizing-steroid-treatment-duchenne-muscular-dystrophy
22.
Matthews E, Brassington R, Kuntzer T, Jichi F, Manzur AY. Corticosteroids for the treatment of Duchenne muscular dystrophy. Cochrane Database Syst. Rev. 5(5), CD003725 (2016).
23.
United States Food and Drug Administration. Highlights of prescribing information: rayos (prednisone). https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/202020s000lbl.pdf
24.
Bylo M, Farewell R, Coppenrath VA, Yogaratnam D. A review of deflazacort for patients with Duchenne muscular dystrophy. Ann. Pharmacother. 54(8), 788–794 (2020).
• Reviews the pharmacology, pharmacokinetics, efficacy, safety, dosage and administration and other considerations of deflazacort treatment. It summarizes the evidence that deflazacort shows improved functional outcomes, delayed onset of cardiomyopathy, reduction in scoliosis surgery and improved survival.
Information & Authors
Information
Published In
Pages: 1065 - 1078
PubMed: 34275333
Copyright
© 2021 Analysis Group, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 7 May 2021
Accepted: 18 June 2021
Published online: 19 July 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Steroid switching in dystrophinopathy treatment: a US chart review of patient characteristics and clinical outcomes. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0110
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Alexis T Mickle, Karissa M Johnston, Kristen L Ricchetti-Masterson, Andrew R Kennedy, Sarah GC Korpach, Katherine L Gooch, The natural history of Becker muscular dystrophy: A systematic literature review, Journal of Neuromuscular Diseases, 10.1177/22143602261420045, (2026).
- Craig M McDonald, Jessica R Marden, Perry B Shieh, Brenda L Wong, Henry Lane, Adina Zhang, Ha Nguyen, Molly Frean, Panayiota Trifillis, Karyn Koladicz, James Signorovitch, Disease progression rates in ambulatory Duchenne muscular dystrophy by steroid type, patient age and functional status, Journal of Comparative Effectiveness Research, 10.57264/cer-2022-0190, 12, 4, (2023).
- Jing Liu, Jeffrey S. Barrett, Efthimia T. Leonardi, Lucy Lee, Satrajit Roychoudhury, Yong Chen, Panayiota Trifillis, Natural History and Real‐World Data in Rare Diseases: Applications, Limitations, and Future Perspectives, The Journal of Clinical Pharmacology, 10.1002/jcph.2134, 62, S2, (2022).
- Perry B Shieh, Gary Elfring, Panayiota Trifillis, Claudio Santos, Stuart W Peltz, Julie A Parsons, Susan Apkon, Basil T Darras, Craig Campbell, Craig M McDonald, Richard J Barohn, Enrico Bertini, Kate Bushby, Brigitte Chabrol, Emma Ciafaloni, Jaume Columer, Giacomi Pietro Comi, Anne Connolly, Richard S Finkel, Kevin M Flanigan, Nathalie Goemans, Michela Guglieri, Susan T Iannaccone, Kristi J Jones, Petra Kaufmann, Janbernd Kirschner, Jean K Mah, Katherine Mathews, Eugenio Mercuri, Francesco Muntoni, Yoram Nevo, Andrés Nascimento Osorio, Yann Péréon, Rosaline Quinlivan, J. Ben Renfroe, Barry Russman, Monique Ryan, Jacinda Sampson, Ulrike Schara, Kathryn Selby, Thomas Sejersen, Douglas M Sproule, H. Lee Sweeney, Már Tulinius, Juan J Vilchez, Giuseppe Vita, Thomas Voit, Stephanie Burns-Wechsler, Brenda Wong, Ted Abresch, Erik K Henricson, Kim Coleman, Michelle Eagle, Julaine Florence, Ed Gappmaier, Craig McDonald, Hoda Z Abdel-Hamid, Richard J Barohn, Enrico Bertini, Clemens Bloetzer, Kate Bushby, Russell J Butterfield, Brigitte Chabrol, Jong-Hee Chae, Giacomi Pietro Comi, Jahannaz Dastgir, Isabelle Desguerre, Raul G Escobar, Erika Finanger, Richard S Finkel, Kevin M Flanigan, Nathalie Goemans, Michela Guglieri, Peter Heydemann, Imelda Hughes, Susan T Iannaccone, Kristi J Jones, Anna Kaminska, Peter Karachunski, Janbernd Kirschner, Martin Kudr, Timothy Lotze, Jean K Mah, Katherine Mathews, Eugenio Mercuri, Francesco Muntoni, Yoram Nevo, Andrés Nascimento Osorio, Yann Péréon, Alexandra Prufer de Queiroz Campos Araujo, J. Ben Renfroe, Maria Bernadete Dutra de Resende, Monique Ryan, Jacinda Sampson, Ulrike Schara, Kathryn Selby, Thomas Sejersen, H. Lee Sweeney, Gihan Tennekoon, Haluk Topaloglu, Ricardo Erazo Torricelli, Már Tulinius, Juan J Vilchez, Giuseppe Vita, Thomas Voit, Brenda Wong, Lindsay N Alfano, Michelle Eagle, Meredith K James, Linda Lowes, Anna Mayhew, Elena S Mazzone, Leslie Nelson, Kristy J Rose, Meta-analyses of deflazacort versus prednisone/prednisolone in patients with nonsense mutation Duchenne muscular dystrophy, Journal of Comparative Effectiveness Research, 10.2217/cer-2021-0018, 10, 18, (1337-1347), (2021).