Meta-analyses of deflazacort versus prednisone/prednisolone in patients with nonsense mutation Duchenne muscular dystrophy
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Compare efficacies of deflazacort and prednisone/prednisolone in providing clinically meaningful delays in loss of physical milestones in patients with nonsense mutation Duchenne muscular dystrophy. Materials & methods: Placebo data from Phase IIb (ClinicalTrials.gov Identifier: NCT00592553) and ACT DMD (ClinicalTrials.gov Identifier: NCT01826487) ataluren nonsense mutation Duchenne muscular dystrophy clinical trials were retrospectively combined in meta-analyses (intent-to-treat population; for change from baseline to week 48 in 6-min walk distance [6MWD] and timed function tests). Results: Significant improvements in change in 6-min walk distance with deflazacort versus prednisone/prednisolone (least-squares mean difference 39.54 m [95% CI: 13.799, 65.286; p = 0.0026]). Significant and clinically meaningful improvements in 4-stair climb and 4-stair descend for deflazacort versus prednisone/prednisolone. Conclusion: Deflazacort provides clinically meaningful delays in loss of physical milestones over 48 weeks compared with prednisone/prednisolone for patients with nonsense mutation Duchenne muscular dystrophy.
Duchenne muscular dystrophy (DMD) is a rare and fatal X-linked disorder that affects one in every 3600–6000 live male births and is characterized by progressive muscle weakness and degeneration [1,2]. The current standard of care for DMD includes treatment with the glucocorticoids prednisone, prednisolone or deflazacort [3] although only deflazacort is currently approved by the US FDA for treating patients with DMD. Glucocorticoids used across the lifespan of DMD patients are associated with improvements in strength and function, health-related quality of life and survival [4]. These agents can slow the decline in muscle strength and motor function, and delay loss of ambulation (LoA), development of scoliosis, loss of pulmonary function and cardiomyopathy [2,4–6].
The challenges of conducting a clinical trial in patients with rare diseases such as DMD include maximizing sample sizes of patients, which is particularly important because of heterogeneity in clinical progression [7]. Meta-analyses allow for robust estimates of the effect size of an intervention based on combined evidence from individual trials [8], and they are often employed in the study of rare diseases [9].
However, relatively few studies have evaluated the efficacy of deflazacort versus prednisone/prednisolone directly in the DMD population [10]. Furthermore, the available studies have used a range of different dosing regimens and outcome measures, and included patients with varying DMD genotypes, making direct comparisons difficult.
Patients in the placebo arms of recently completed DMD trials are required to be on stable glucocorticoids at trial entry and can continue using stable doses of glucocorticoids for the duration of the trials [10]. In a recent meta-analysis [10] of 131 patients with varying DMD genotypes from the placebo arms of two DMD trials [11,12], deflazacort-treated patients experienced significantly less functional decline over 48 weeks than prednisone/prednisolone-treated patients [10].
In the present study, we assessed the efficacy of deflazacort versus prednisone/prednisolone in slowing disease progression in a more genetically uniform population of patients with nonsense mutation DMD (nmDMD). The current meta-analyses used data from the placebo arms of two previously published studies in patients with nmDMD [11,13].
Patients & methods
Study inclusion criteria
We conducted a combined literature search of Ovid MEDLINE® and EMBASE® (1 January 2000–30 November 2020) to identify articles comparing deflazacort and prednisone/prednisolone in patients with DMD or nmDMD. The search strategy is presented in Supplementary Tables 1 & 2. This search identified 11 articles comparing deflazacort and prednisone/prednisolone in DMD. These studies included randomized trials [14–16], post hoc analyses of placebo-arm data from industry-sponsored trials [10,17] and observational studies [4,18–22].
The identified studies included patients with different DMD genotypes, were of varying duration, used different dosing regimens and assessed different outcomes. Only one of the 11 identified studies reported results from a randomized trial in patients with nmDMD. This was a post hoc analysis of the Phase III Ataluren Confirmatory Trial in Duchenne Muscular Dystrophy (ACT DMD) trial (ClinicalTrials.gov Identifier: NCT01826487) that assessed the efficacy and safety of deflazacort and prednisone/prednisolone in the placebo arm over 48 weeks [17]. However, the authors had also available an unpublished subanalysis from the placebo arm of the Phase IIb ataluren study (ClinicalTrials.gov Identifier: NCT00592553) [13] assessing the efficacy of deflazacort versus prednisone/prednisolone. This analysis shared common end points with the post hoc analysis of the ACT DMD trial [17]; i.e. change from baseline in 6-minute walk distance (6MWD) and timed function tests (TFTs) over 48 weeks. We, therefore, performed a meta-analysis on patients randomized to placebo receiving deflazacort or prednisone/prednisolone in the ACT DMD trial and the unpublished subanalysis from the Phase IIb trial in these meta-analyses; only the end points common to both studies are included in this report.
Study design
The two trials included were of similar design, both being randomized, double-blind, placebo-controlled, 48-week, multicenter trials of ataluren in patients with nmDMD [11,13]. The meta-analyses included data from the placebo arms of these studies and retrospectively analyzed data according to drug therapy initiated before the start of the trials. Both trials enrolled boys with nmDMD, confirmed by gene sequencing, with phenotypic evidence of dystrophinopathy, elevated serum creatine kinase levels and difficulty with ambulation. The Phase IIb trial enrolled boys aged ≥5 years, with a 6MWD of ≥75 m at screening [13]. The inclusion criteria for the ACT DMD trial were narrower than those of the Phase IIb trial, including boys aged ≥7 and ≤16 years, with a 6MWD of both ≥150 m and ≤80% of that predicted for their age and height [11]. The ACT DMD trial also specified that patients should be receiving concomitant glucocorticoid therapy at a stable dose for at least 6 months prior to study entry; this criterion was not specified in the Phase IIb trial, but 71% of patients in that trial were receiving glucocorticoids [11,13]. Full inclusion and exclusion criteria of the two trials have been published previously [11,13].
Data extraction
The trial sponsor analyzed the data and included all individual patient trial data from patients in both trials who had received placebo for 48 weeks as described in the study design. The following information was collated: patient baseline characteristics and demographics; change from baseline to week 48 in 6MWD (the primary end point in both trials); change from baseline to week 48 in time taken to walk/run 10 m (a secondary end point in both trials); time taken to climb 4 stairs (a secondary end point in both trials); and time taken to descend 4 stairs (a secondary end point in both trials). The time needed to rise from the floor was not analyzed, as 15 of the 57 (26.3%) patients in the Phase IIb study were unable to rise from the floor at baseline. These efficacy end points were chosen because they were common to both trials. Safety outcomes, assessed throughout both trials, were also summarized.
Data analyses
The meta-analyses were performed in compliance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2009 guidelines, where applicable [23]. No assessment of publication bias was possible because our meta-analysis only included two trials. These meta-analyses were performed using a fixed-effects model, whereby for each study the point estimate was given a weight equal to the inverse of the variance of the point estimate. We have previously used this statistical approach when assessing the efficacy of ataluren versus placebo in a recent meta-analysis of the same two trials [24]. Outcomes for the 6-minute walk test and TFTs (10 m walk/run, 4-stair climb and 4-stair descend) are reported as the least-squares (LS) mean difference ± 95% CI [25]. The nominal p-values for these outcomes were obtained by converting the LS mean difference to a 2-sided z-statistic [11].
The meta-analyses used only data from patients randomized to placebo in the intent-to-treat population of the Phase IIb and ACT DMD trials. Inclusion of patients from the Phase IIb trial was restricted to those who met the entry criteria for the ACT DMD trial (aged ≥7 and ≤16 years, diagnosed with nmDMD, with a baseline 6MWD of both ≥150 m and ≤80% of that predicted for age and height, and receiving concomitant glucocorticoid therapy). Heterogeneity was assessed by computing the I2 statistic and the probability of there being significant between-studies differences.
Results
Demographics & patient disposition
Baseline characteristics were well balanced between those taking deflazacort and prednisone/prednisolone in the intent-to treat populations of both trials (Table 1). Of the 114 placebo patients from ACT DMD included in these meta-analyses, 53 were using deflazacort and 61 were using prednisone/prednisolone. Similarly, in the Phase IIb study, of the 40 patients in the placebo arm, 17 received deflazacort and 23 received prednisone/prednisolone. The study participants all had a point mutation leading to a premature stop codon. The point mutations were located in exons 1–39 for 57.9 and 59.6%, and exons 40–79 for 42.1 and 40.4% of the patients in the placebo arm of the Phase IIb (n = 57) and ACT DMD trials (n = 114), respectively. In the Phase IIb trial, no patients discontinued because of an adverse event (AE). In the ACT DMD trial, one patient treated with deflazacort discontinued owing to an AE (disease progression).
| Characteristic | Phase IIb | ACT DMD | ||
|---|---|---|---|---|
| Deflazacort (n = 17) | Prednisone/prednisolone (n = 23) | Deflazacort (n = 53) | Prednisone/prednisolone (n = 61) | |
| Age, years | ||||
| Mean (SD) | 9.1 (2.9) | 8.3 (1.5) | 9.2 (1.7) | 8.8 (1.6) |
| Range | 6, 15 | 5, 11 | 7, 14 | 7, 13 |
| Age group, n (%) | ||||
| – <9 years | 8 (47.1) | 12 (52.2) | 23 (43.4) | 30 (49.2) |
| – ≥9 years | 9 (52.9) | 11 (47.8) | 30 (56.6) | 31 (50.8) |
| Race, n (%) | ||||
| – White | 16 (94.1) | 22 (95.7) | 46 (86.8) | 39 (63.9) |
| – Black/African American | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (1.6) |
| – Asian | 1 (5.9) | 0 (0.0) | 4 (7.5) | 2 (3.3) |
| – Hispanic | 0 (0.0) | 0 (0.0) | 3 (5.7) | 5 (8.2) |
| – Other | 0 (0.0) | 1 (4.3) | 0 (0.0) | 4 (6.6) |
| – Missing | 0 (0.0) | 0 (0.0) | 0 (0.0) | 10 (16.4) |
| Weight, kg | ||||
| – Mean (SD) | 29.9 (9.9) | 31.0 (9.2) | 30.9 (11.9) | 30.5 (9.2) |
| – Range | 17.9, 50.1 | 19.2, 54.6 | 18.1, 68.0 | 18.2, 59.8 |
| Height, cm | ||||
| Mean (SD) | 123.1 (0.2) | 124.3 (10.4) | 127.0 (10.6) | 125.7 (10.4) |
| Range | 106.0, 141.0 | 107.0, 148.0 | 106.7, 148.7 | 101.8, 151.0 |
| BMI, kg/m2 | ||||
| – Mean (SD) | 19.2 (4.2) | 19.7 (3.4) | 18.6 (4.7) | 19.0 (3.5) |
| – Range | 14.1, 28.6 | 14.0, 25.6 | 13.0, 36.0 | 13.1, 27.1 |
| Corticosteroid use prior to baseline, n (%) | ||||
| – 6 to <12 months | 1 (5.9) | 5 (21.7) | 7 (13.2) | 11 (18.0) |
| – ≥12 months | 16 (94.1) | 18 (78.3) | 46 (86.8) | 50 (82.0) |
| Location of point mutations, n (%) | ||||
| – Exons 1 to 39 | 9 (52.9) | 14 (60.9) | 36 (67.9) | 32 (52.5) |
| – Exons 40 to 79 | 8 (47.1) | 9 (39.1) | 17 (32.1) | 29 (47.5) |
ACT DMD: Ataluren Confirmatory Trial in Duchenne Muscular Dystrophy; SD: Standard deviation.
Dosing
Daily dosing was the most common dosing regimen for deflazacort and prednisone/prednisolone. The mean daily deflazacort doses were 0.785 mg/kg in the Phase IIb trial and 0.695 mg/kg in the ACT DMD trial (87.2 and 77.2% of the recommended starting dose of 0.90 mg/kg for deflazacort, respectively). The mean daily prednisone/prednisolone doses were 0.684 mg/kg in the Phase IIb trial and 0.515 mg/kg in the ACT DMD trial (91.2 and 68.7% of the recommended starting dose of 0.75 mg/kg for prednisone, respectively).
6MWD & TFTs
Treatment differences for the 6MWD favored deflazacort versus prednisone/prednisolone and are presented in Figure 1. For the Phase IIb trial, the LS mean difference was 57.20 m (95% CI: 9.32, 105.08; p = 0.021); for ACT DMD, this difference was 31.58 m (95% CI: 0.22, 62.94; p = 0.048). In the meta-analysis, the LS mean difference was 39.54 m (95% CI: 13.80, 65.29; p = 0.0026).
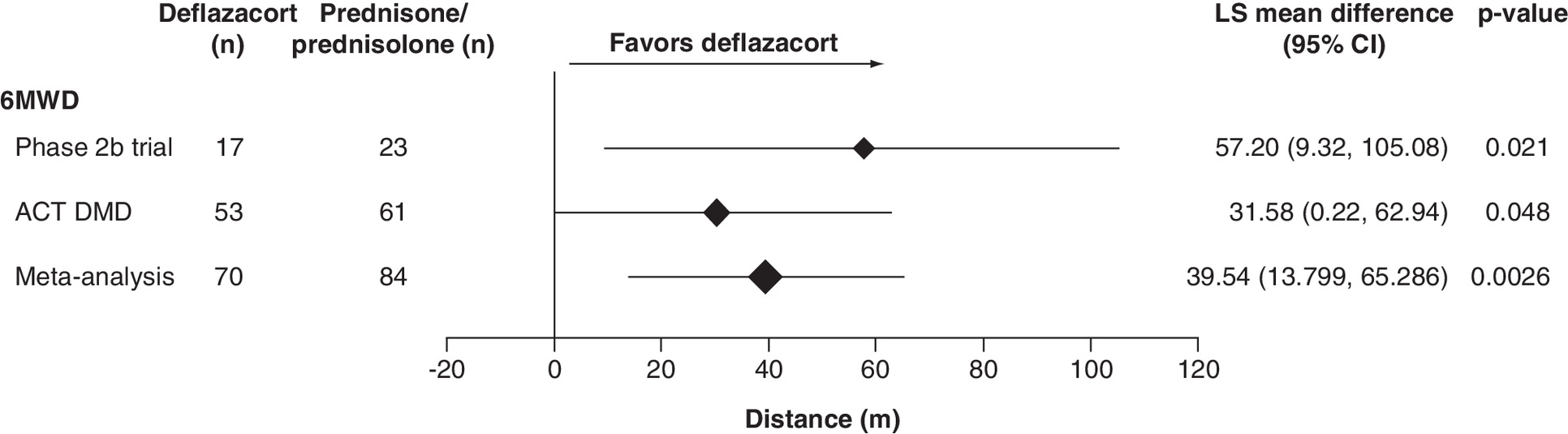
Figure 1. Least-squares mean difference in change from baseline to week 48 in 6MWD.
LS mean difference presented for 6-min walk distance between patients receiving deflazacort and those receiving prednisone/prednisone, assessed by meta-analysis of the ITT population using a fixed-effects model.
6MWD: 6-min walk distance; ACT DMD: Ataluren Confirmatory Trial in Duchenne Muscular Dystrophy; ITT: Intent-to-treat; LS: Least-squares.
Similarly, treatment differences for the 10 m walk/run favoring deflazacort over prednisone/prednisolone were recorded for the Phase IIb trial, ACT DMD and the meta-analysis population. However, the differences were not statistically significant (Figure 2). Treatment differences for the 4-stair climb favored deflazacort over prednisone/prednisolone, and the differences were significant among patients from ACT DMD (2.88 s [95% CI: 0.48, 5.27; p = 0.019]) and in the meta-analysis (2.73 s [95% CI: 0.72, 4.70; p = 0.0079]; Figure 2). A statistically significant treatment difference in the 4-stair descend also favored deflazacort over prednisone/prednisolone in the meta-analysis (2.38 s [95% CI: 0.31, 4.46; p = 0.0244]; Figure 2).

Figure 2. Least-squares mean difference in change from baseline to week 48 in timed function tests.
LS mean differences presented for 10 m walk/run, 4-stair climb and 4-stair descend between patients receiving deflazacort and those receiving prednisone/prednisone, assessed by meta-analyses of the ITT population using a fixed-effects model.
ACT DMD: Ataluren Confirmatory Trial in Duchenne Muscular Dystrophy; ITT: Intent-to-treat; LS: Least-squares.
Analyses of heterogeneity showed that between-studies differences were not statistically significant for any of the outcomes (6MWD and TFTs).
Safety
The most common treatment-emergent AEs reported for the as-treated patients in these trials and for the meta-analysis patients are listed in Table 2. It should be noted that AEs reported here are from ataluren studies and, thus, AEs associated with either glucocorticoid may be underreported. Treatment with deflazacort and prednisone/prednisolone over the 48-week trial was generally well tolerated, and most AEs were mild to moderate in severity. There were no discontinuations owing to AEs among patients in the Phase IIb trial. One placebo-allocated patient receiving deflazacort in the ACT DMD trial discontinued because of an AE (disease progression). There were no reports of patients in the placebo arms of either trial receiving either deflazacort or prednisone experiencing weight gain. Mood swings were reported by one placebo-allocated patient receiving deflazacort in the Phase IIb trial, which was resolved, and two placebo-allocated patients receiving deflazacort in the ACT DMD trial (one was resolved and the other was recovering at the end of the trial).
| TEAE, n (%) | Phase IIb | ACT DMD | Meta-analysis population | |||
|---|---|---|---|---|---|---|
| Deflazacort (n = 17) | Prednisone/prednisolone (n = 23) | Deflazacort (n = 53) | Prednisone/prednisolone (n = 62) | Deflazacort (n = 70) | Prednisone/prednisolone (n = 85) | |
| Vomiting | 8 (47) | 5 (22) | 10 (19) | 11 (18) | 18 (26) | 16 (19) |
| Headache | 5 (29) | 7 (30) | 10 (19) | 11 (18) | 15 (21) | 18 (21) |
| Nasopharyngitis | 5 (29) | 3 (13) | 6 (11) | 17 (27) | 11 (16) | 20 (24) |
| Pain in extremity | 3 (18) | 1 (4) | 6 (11) | 8 (13) | 9 (13) | 9 (11) |
| Cough | 4 (24) | 5 (22) | 5 (9) | 8 (13) | 9 (13) | 13 (15) |
| Diarrhea | 3 (18) | 9 (39) | 5 (9) | 5 (8) | 8 (11) | 14 (16) |
| Pyrexia | 4 (24) | 3 (13) | 4 (8) | 8 (13) | 8 (11) | 11 (13) |
| Constipation | 3 (6) | 1 (4) | 4 (8) | 6 (10) | 7 (10) | 7 (8) |
| Influenza | 3 (18) | 4 (17) | 3 (6) | 2 (3) | 6 (9) | 6 (7) |
| Pain in abdomen‡ | 4 (24) | 3 (13) | 0 (0) | 18 (29) | 4 (6) | 21 (25) |
| Fall | 1 (6) | 3 (13) | 8 (15) | 12 (19) | 9 (13) | 15 (18) |
| Back pain | 2 (12) | 3 (13) | 2 (4) | 6 (10) | 4 (6) | 9 (11) |
| Nausea | 1 (6) | 3 (13) | 3 (6) | 4 (6) | 4 (6) | 7 (8) |
| Upper RTI | 3 (18) | 4 (17) | 0 (0) | 6 (10) | 3 (4) | 10 (7) |
| Gastroenteritis | 1 (6) | 3 (13) | 2 (4) | 3 (5) | 3 (4) | 6 (7) |
| Bronchitis | 2 (12) | 2 (9) | 1 (2) | 2 (3) | 3 (4) | 4 (5) |
| Rhinorrhea | 2 (12) | 2 (9) | 1 (2) | 2 (4) | 3 (4) | 4 (5) |
| Abdominal discomfort | 2 (12) | 2 (9) | 0 (0) | 0 (0) | 2 (3) | 2 (2) |
| Dizziness | 2 (12) | 1 (4) | 0 (0) | 1 (2) | 2 (3) | 2 (2) |
| Rash | 2 (12) | 1 (4) | 0 (0) | 2 (3) | 2 (3) | 3 (4) |
| Excoriation | 2 (12) | 0 (0) | 0 (0) | 1 (2) | 2 (3) | 1 (1) |
| Procedural pain | 1 (6) | 6 (26) | 0 (0) | 0 (0) | 1 (1) | 6 (7) |
| Muscle spasms | 1 (6) | 4 (17) | 0 (0) | 1 (2) | 1 (1) | 4 (5) |
| Flatulence | 1 (6) | 3 (13) | 0 (0) | 1 (2) | 1 (1) | 4 (5) |
| Ear infection | 0 (0) | 4 (17) | 1 (2) | 0 (0) | 1 (1) | 4 (5) |
| Scar | 0 (0) | 3 (13) | 0 (0) | 0 (0) | 0 (0) | 3 (4) |
†
Incidence of ≥10% in either subgroup in either trial.
‡
Including upper abdomen.
ACT DMD: Ataluren Confirmatory Trial in Duchenne Muscular Dystrophy; RTI: Respiratory tract infection; TEAE: Treatment-emergent adverse event.
Discussion
The meta-analyses of the two trials reported here showed that deflazacort conferred clinically meaningful delays in the loss of motor function, including a statistically significant 39.5 m treatment benefit on the primary end point of 6MWD when compared with prednisone/prednisolone over 48 weeks. We also show significant treatment benefits with deflazacort versus prednisone/prednisolone for the secondary end points of 4-stair climb and 4-stair descend for the intent-to-treat population. The treatment differences both exceeded the 1.5 s estimate for clinically meaningful difference in TFTs [11,13,26].
Primary and post hoc studies of patients receiving deflazacort or prednisone/prednisolone, either in the placebo arm or as the primary intervention, are included in Supplementary Table 3. Only two clinical trials of patients with nmDMD were available for inclusion in these meta-analyses at the time of analysis: the ataluren Phase IIb trial and the ACT DMD Phase III trial [11,13]. This is therefore the third time that the placebo arm of the ACT DMD Phase III trial has been used in a post hoc analysis in order to compare deflazacort and prednisone/prednisolone [10,17].
A recent meta-analysis of two Phase III, placebo-controlled trials in DMD, reported a greater efficacy for deflazacort than prednisone/prednisolone [10]. Like the present study, this meta-analysis also used data from the placebo arm of the ACT DMD trial; and additionally included data from the placebo arm of a trial of tadalafil in patients with broad genotypes of DMD [10–12]. Approximately half of the population in that meta-analysis had nmDMD, as only three patients with nonsense/missense mutations in the DMD gene were included from the tadalafil study (n = 116; nonsense/missense mutation DMD; n = 3) [10–12]. The current analyses differ in that their focus is entirely on patients with nmDMD. As is the case with the present article, the meta-analysis recently published by McDonald and colleagues also reported a lesser decline in physical functioning among patients treated with deflazacort compared with those treated with prednisone/prednisolone [10]. Patients treated with deflazacort declined, on average, 28.3 m less on the 6MWD, 2.9 s less on rise from supine, 2.3 s less on the 4-stair climb and 2.9 points less on the North Star Ambulatory Assessment linearized score than did those treated with prednisone/prednisolone. No safety data were reported. The present meta-analysis, therefore, confirms a treatment benefit of deflazacort compared with prednisone in a more homogenous population of patients with nmDMD only; these results suggest that the benefit of deflazacort is evident regardless of DMD mutation type. It could be of interest to further investigate differences in corticosteroid benefit by corticosteroid type and duration in DMD patients stratified by other markers of disease severity aside from mutation type such as genetic modifiers, and by stage of disease progression (i.e., early ambulatory, late ambulatory and nonambulatory phases).
Additional studies in DMD have shown greater benefits with deflazacort compared with prednisone/prednisolone. The Cooperative International Neuromuscular Research Group Duchenne Natural History Study, analyzing data from 340 patients with varying DMD genotypes, found that daily deflazacort treatment significantly delayed the age at LoA by more than 2 years (median age 13.9 vs 11.2 years for those given daily prednisone/prednisolone) [19]. A 10-year, prospective, natural history study observed that deflazacort significantly increased age at LoA, age at loss of supine to stand and age at loss of hand-to-mouth function when compared with prednisone/prednisolone [4]. FOR DMD, a double-blind, randomized Phase III clinical trial investigating the optimal glucocorticoid regimen of deflazacort or prednisone in boys aged 4–7 years old with DMD is ongoing [27]. This study aims to determine which regimen (daily deflazacort 0.9 mg/kg versus daily prednisone 0.75 mg/kg versus intermittent prednisone 0.75 mg/kg [10 days on, 10 days off] improves muscle strength the most and causes the fewest side effects over 36 months; however, it should be noted that these younger patients are still making maturational and developmental muscle gains in the absence of any glucocorticoid treatment, making it difficult to attribute treatment effect.
Different pharmacologic properties of deflazacort versus prednisone/prednisolone [28–30], leading to greater bioavailability of deflazacort to muscle fibers, might explain the consistent differences in efficacy observed across the two trials included in the present meta-analysis. An alternative explanation proposed by Bello and colleagues suggests that the differences in preservation of function are due to different adherence to care standards and/or greater tolerance of higher dosing with deflazacort [19]. However, the dosing of glucocorticoids used (relative to suggested dosing) was not substantially different in the two trials included in the present meta-analysis, apart from the lower dosing per kg body weight for both glucocorticoid types in the ACT DMD trial, which might be attributed to the older patient population enrolled. In addition, the international distribution of sites for both trials resulted in deflazacort being readily available at the majority of sites, making differences in socio-economic status or adherence to care standards less influential on these analyses.
The two studies included in these meta-analyses limited enrollment to patients with nmDMD. Other studies, along with the above-mentioned meta-analysis of data from the Phase III tadalafil trial and ACT DMD, that did not restrict enrollment according to mutation status, also observed greater efficacy with deflazacort compared with prednisone/prednisolone for delaying loss of physical function in patients with DMD [4,10,15,21]. Of note, McDonald et al. (2018) [4] and Marden et al. [21] were long-term studies that followed up large cohorts of patients for at least 10 years. Another recent real-world study describing reasons for DMD and Becker muscular dystrophy patients in the US switching from prednisone/prednisolone to deflazacort showed that physician-reported outcomes were consistent with deflazacort addressing patients’ primary reasons for switching [31]. On the basis of these previous findings and the known pharmacological effects of deflazacort, it is expected that ambulatory patients with DMD caused by other types of DMD mutations would also derive greater functional benefits from deflazacort than from prednisone/prednisolone [10–12].
The strengths of the present meta-analyses include the similarity of design of the two trials and the validity of combining results, which was supported by the absence of statistical heterogeneity between the two trials for any of the end points. Limitations consist of those inherent in the individual trials included in the current meta-analyses. These include the natural history of DMD vis a vis the 48-week duration of evaluation. Current regulatory guidelines for trials in DMD recommend a longer duration of evaluation, if possible, to evaluate long-term efficacy [32,33]. The duration of prior treatment with glucocorticoids was not ascertained in these studies with precision. Patients in the two trials received deflazacort or prednisone/prednisolone according to their current treatment when entering the study [11,13]. Therefore, the meta-analyses data are not based on randomized assignment of these glucocorticoids, but are derived from real-world use of these agents in nmDMD. Other limitations were that neither cardiomyopathy nor pulmonary function was assessed and that there was a lack of diversity in racial composition in the two trials. An additional limitation is that both studies were designed as ataluren trials and the AEs for each glucocorticoid in these analyses may be underreported. Finally, these studies were confined to children with nmDMD aged 7 years and older with a 6MWD greater than or equal to 150 m. The relative efficacy of the two glucocorticoids was not assessed in ambulatory children younger than 7 years, in those with more severe impairment or nonambulatory patients.
Conclusion
These meta-analyses demonstrate that, in ambulatory patients with nmDMD, deflazacort provides a clinically meaningful delay in the loss of physical functioning compared with prednisone/prednisolone, as measured by primary and secondary end point data from two clinical trials. In these studies, deflazacort and prednisone/prednisolone were generally well tolerated by patients with nmDMD. Future trials should assess the relative benefits of deflazacort over a longer duration of treatment, and prespecify patient subgroups for analysis based on baseline disease severity characteristics and length of glucocorticoid treatment.
•
Long-term glucocorticoid treatment is a standard of care and delays the loss of physical milestones in patients with Duchenne muscular dystrophy (DMD).
•
We aimed to compare the efficacy of deflazacort and prednisone/prednisolone in providing clinically meaningful delays in loss of physical milestones in patients with nonsense mutation Duchenne muscular dystrophy.
•
Placebo data from Phase IIb (ClinicalTrials.gov Identifier: NCT00592553) and ACT DMD (ClinicalTrials.gov Identifier: NCT01826487) ataluren nonsense mutation Duchenne muscular dystrophy clinical trials were retrospectively combined in meta-analyses examining intent-to-treat populations of both trials.
•
Placebo trial baseline demographics and characteristics were similar between the deflazacort- and prednisone-treated patients.
•
Significant improvements in change in 6MWD with deflazacort versus prednisone/prednisolone were observed.
•
Significant and clinically meaningful improvements were also observed for deflazacort versus prednisone/prednisolone for the timed function tests of 4-stair climb and 4-stair descend.
•
Deflazacort provides clinically meaningful delays in loss of physical milestones compared with prednisone/prednisolone for patients with nonsense mutation Duchenne muscular dystrophy over 48 weeks.
Author contributions
G Elfring, P Trifillis, C Santos and SW Peltz substantially contributed to the conception and design of the work, as well as the analysis and interpretation of data. PB Shieh, J Parsons, S Apkon, B Darras, C Campbell and CM McDonald substantially contributed to the analysis and interpretation of data. All authors contributed to the writing and review of each draft of the manuscript and approved the final version. All authors gave their agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors thank the patients and their families for their participation in these studies and the individuals who were instrumental in the conduct and the collection of data, particularly the principal investigators, supporting investigators, clinical coordinators, clinical evaluators and study coordinators. We thank R Weiss (University of Utah, UT, USA) for DMD gene sequencing and the patient advocacy organizations (including V Cwik and the Muscular Dystrophy Association, and P Furlong and the Parent Project Muscular Dystrophy) for the collaboration and support that made these trials possible. We also thank J McIntosh, E O'Mara and M Souza, who were former employees of PTC Therapeutics, for their important contributions to this study.
Financial & competing interests disclosure
This research was funded by PTC Therapeutics, Inc., and did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors. C Campbell has received grants from and has acted as a consultant to PTC Therapeutics, and has been a clinical trial investigator for Acceleron, AMO, Biogen, Biomarin, BMS, Catabasis, Cytokinetics, Pfizer, PTC Therapeutics, Sarepta, Wave and Roche. He did not receive any personal compensation for these activities. B Darras reports, for the last year, advisory boards for AveXis, Biogen, Cytokinetics, Dynacure, Genentech, Roche and Sarepta Therapeutics. Over the last 2 years, he has participated in advisory boards for AveXis, Biogen, Cytokinetics, Dynacure, Genentech, PTC Therapeutics, Roche and Sarepta Therapeutics. He has also received research support from the National Institutes of Health/National Institute of Neurological Disorders and Stroke, the Slaney Family Fund for SMA, the SMA Foundation and Working on Walking Fund; grants from Biogen, CureSMA and Ionis Pharmaceuticals, Inc. during CHERISH, CS2, CS11 and CS12 studies and ENDEAR, and also from AveXis, Cytokinetics, Fibrogen, PTC Therapeutics, Roche, Santhera Pharmaceuticals, Sarepta Therapeutics and Summit Therapeutics. He reports no personal financial interests in any of these companies. PB Shieh has served as an ad hoc advisory board member for AveXis, Biogen, Marathon, PTC Therapeutics and Sarepta Therapeutics, but he has no financial interests in these companies. He has received research support from Biogen and Ionis Pharmaceuticals for their SMA studies, as well as from BMS/Roche for their DMD/myostatin clinical trial, Cytokinetics for their SMA clinical trial, Pfizer for their DMD/myostatin clinical trial, PTC Therapeutics for their DMD/ataluren trial, Sanofi/Genzyme for their Pompe clinical trial, Sarepta Therapeutics for their DMD clinical trials and Summit Therapeutics for their DMD clinical trial. CM McDonald has served as a compensated consultant for clinical trials for PTC Therapeutics, and outside the submitted work as a consultant for Astellas, Biomarin, Capricor, Catabasis, Cytokinetics, Eli Lilly, Edgewise Therapeutics, Epirium Bio (formerly Cardero Therapeutics), FibroGen, Italfarmaco, Marathon, Pfizer, Santhera Pharmaceuticals and Sarepta Therapeutics. He serves on external advisory boards related to Duchenne muscular dystrophy with compensation from Capricor, Eli Lilly, PTC Therapeutics, Santhera Pharmaceuticals and Sarepta Therapeutics, and held grants from NIDILRR, Parent Project Muscular Dystrophy US, the US Department of Education/NIDRR, US NIH/NIAMS and the US Department of Defense during the time of the study. J Parsons has served as an ad hoc scientific advisory board member for AveXis, Biogen, Genentech and Sarepta Therapeutics. She has been a clinical investigator for PTC Therapeutics and Sarepta Therapeutics for their DMD clinical trials. She has no financial interests in these companies. S Apkon has served as a consultant for Biogen. She has received research support from BMS/Roche for their DMD/myostatin clinical trial, PTC Therapeutics for their DMD/ataluren trials and Sarepta Therapeutics for their DMD/eteplirsen clinical trials. She has not received personal payment for these activities. G Elfring, P Trifillis, C Santos and SW Peltz are employees and stockholders of PTC Therapeutics, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Professional medical writing assistance was provided by A Skorupa of EnlightenMed, LLC, and Tove Anderson of PharmaGenesis London, and was funded by PTC Therapeutics, Inc. The authors provided the initial outline draft and worked with A Skorupa to produce the first full draft of this manuscript. Editorial support was provided by PharmaGenesis London, and was funded by PTC Therapeutics, Inc.
Ethical conduct of research
Both trials were performed in accordance with the Declaration of Helsinki (2000) and the principles of Good Clinical Practice. The trials and any changes to the protocols were approved by the local regulatory authorities and the institutional review board/ethics committee of each site. Written informed consent/assent was obtained from all patients/guardians in both trials. The two trials were registered (ClinicalTrials.gov: NCT00592553 and NCT01826487).
Data sharing statement
Individual de-identified participant data or any patient-level data behind the results reported in this article will not be made available; only the results of this study will be shared, since this article reports on meta-analyses of data from previously published trials. The protocols and statistical analysis plans of the two trials discussed in this article will be made available following article publication with no defined end date. Access to the protocols and statistical analysis plans will be provided upon request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
1.
Bushby K, Finkel R, Birnkrant DJ et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol. 9(1), 77–93 (2010).
2.
Birnkrant DJ, Bushby K, Bann CM et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation, endocrine, and gastrointestinal and nutritional management. Lancet Neurol. 17(3), 251–267 (2018).
3.
Birnkrant DJ, Bushby K, Bann CM et al. Diagnosis and management of Duchenne muscular dystrophy, part 3: primary care, emergency management, psychosocial care, and transitions of care across the lifespan. Lancet Neurol. 17(5), 445–455 (2018).
4.
McDonald CM, Henricson EK, Abresch RT et al. Long-term effects of glucocorticoids on function, quality of life, and survival in patients with Duchenne muscular dystrophy: a prospective cohort study. Lancet 391(10119), 451–461 (2018).
5.
Gloss D, Moxley RT 3rd, Ashwal S, Oskoui M. Practice guideline update summary: corticosteroid treatment of Duchenne muscular dystrophy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 86(5), 465–472 (2016).
6.
Barber BJ, Andrews JG, Lu Z et al. Oral corticosteroids and onset of cardiomyopathy in Duchenne muscular dystrophy. J. Pediatr. 163(4), 1080–1084 e1081 (2013).
7.
Desguerre I, Christov C, Mayer M et al. Clinical heterogeneity of duchenne muscular dystrophy (DMD): definition of sub-phenotypes and predictive criteria by long-term follow-up. PLoS ONE 4(2), e4347 (2009).
8.
Gopalakrishnan S, Ganeshkumar P. Systematic reviews and meta-analysis: understanding the best evidence in primary healthcare. J. Family Med. Prim. Care 2(1), 9–14 (2013).
9.
Friede T, Rover C, Wandel S, Neuenschwander B. Meta-analysis of few small studies in orphan diseases. Res. Synth. Methods 8(1), 79–91 (2017).
10.
McDonald CM, Sajeev G, Yao Z et al. Deflazacort vs prednisone treatment for Duchenne muscular dystrophy: a meta-analysis of disease progression rates in recent multicenter clinical trials. Muscle Nerve 61(1), 26–35 (2020).
11.
McDonald CM, Campbell C, Torricelli RE et al. Ataluren in patients with nonsense mutation Duchenne muscular dystrophy (ACT DMD): a multicentre, randomised, double-blind, placebo-controlled, Phase III trial. Lancet 390(10101), 1489–1498 (2017).
12.
Victor RG, Sweeney HL, Finkel R et al. A Phase III randomized placebo-controlled trial of tadalafil for Duchenne muscular dystrophy. Neurology 89(17), 1811–1820 (2017).
13.
Bushby K, Finkel R, Wong B et al. Ataluren treatment of patients with nonsense mutation dystrophinopathy. Muscle Nerve 50(4), 477–487 (2014).
14.
Bonifati MD, Ruzza G, Bonometto P et al. A multicenter, double-blind, randomized trial of deflazacort versus prednisone in Duchenne muscular dystrophy. Muscle Nerve 23(9), 1344–1347 (2000).
15.
Griggs RC, Miller JP, Greenberg CR et al. Efficacy and safety of deflazacort vs prednisone and placebo for Duchenne muscular dystrophy. Neurology 87(20), 2123–2131 (2016).
16.
Karimzadeh P, Ghazavi A. Comparison of deflazacort and prednisone in Duchenne muscular dystrophy. Iran. J. Child Neurol. 6(1), 8 (2012).
17.
Shieh PB, McIntosh J, Jin F et al. Deflazacort vs prednisone/prednisolone for maintaining motor function and delaying loss of ambulation: a post hoc analysis from the ACT DMD trial. Muscle Nerve 58(5), 639–645 (2018).
18.
Balaban B, Matthews DJ, Clayton GH, Carry T. Corticosteroid treatment and functional improvement in Duchenne muscular dystrophy: long-term effect. Am. J. Phys. Med. Rehabil. 84(11), 843–850 (2005).
19.
Bello L, Gordish-Dressman H, Morgenroth LP et al. Prednisone/prednisolone and deflazacort regimens in the CINRG Duchenne Natural History Study. Neurology 85(12), 1048–1055 (2015).
20.
Lamb MM, West NA, Ouyang L et al. Corticosteroid treatment and growth patterns in ambulatory males with duchenne muscular dystrophy. J. Pediatr. 173, 207–213 e203 (2016).
21.
Marden JR, Freimark J, Yao Z, Signorovitch J, Tian C, Wong BL. Real-world outcomes of long-term prednisone and deflazacort use in patients with Duchenne muscular dystrophy: experience at a single, large care center. J. Comp. Eff. Res. 9(3), 177–189 (2020).
22.
Rice ML, Wong B, Horn PS, Yang MB. Cataract development associated with long-term glucocorticoid therapy in Duchenne muscular dystrophy patients. J AAPOS 22(3), 192–196 (2018).
23.
Moher D, Liberati A, Tetzlaff J, Altman DG. Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535 (2009).
24.
Muntoni F, Mercuri E, Luo G et al. Meta-analyses of ataluren in patients with nonsense mutation Duchenne muscular dystrophy. Neuromuscular Disord. 28(Suppl. 1), S12 (2018).
25.
Stanley TD, Doucouliagos H. Neither fixed nor random: weighted least squares meta-analysis. Stat. Med. 34(13), 2116–2127 (2015).
26.
McDonald CM, Henricson EK, Abresch RT et al. The 6-minute walk test and other clinical endpoints in duchenne muscular dystrophy: reliability, concurrent validity, and minimal clinically important differences from a multicenter study. Muscle Nerve 48(3), 357–368 (2013).
27.
ClinicalTrials.gov. Finding the optimum regimen for Duchenne muscular dystrophy (FOR-DMD) (2021). https://clinicaltrials.gov/ct2/show/NCT01603407
28.
Assandri A, Buniva G, Martinelli E, Perazzi A, Zerilli L. Pharmacokinetics and metabolism of deflazacort in the rat, dog, monkey and man. Adv. Exp. Med. Biol. 171, 9–23 (1984).
29.
Markham A, Bryson HM. Deflazacort. A review of its pharmacological properties and therapeutic efficacy. Drugs 50(2), 317–333 (1995).
30.
Nayak S, Acharjya B. Deflazacort versus other glucocorticoids: a comparison. Indian J. Dermatol. 53(4), 167–170 (2008).
31.
Marden JR, Santos C, Pfister B et al. Steroid switching in dystrophinopathy treatment: a US chart review of patient characteristics and clinical outcomes. J. Comp. Eff. Res. (2021) (Epub ahead of print).
32.
U.S. Food and Drug Administration. Duchenne muscular dystrophy and related dystrophinopathies: developing drugs for treatment guidance for industry (2018). www.fda.gov/ucm/groups/fdagov-public/@fdagov-drugs-gen/documents/document/ucm450229.pdf
33.
European Medicines Agency. Guideline on the clinical investigation of medicinal products for the treatment of Duchenne and Becker muscular dystrophy (2015). www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2015/12/WC500199239.pdf
Information & Authors
Information
Published In
Pages: 1337 - 1347
PubMed: 34693725
Copyright
© 2021 Shieh et al. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 22 January 2021
Accepted: 2 September 2021
Published online: 25 October 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Meta-analyses of deflazacort versus prednisone/prednisolone in patients with nonsense mutation Duchenne muscular dystrophy. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0018
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ayesha Siddika, Joël Rousseau, Félix Veillette, Camille Bouchard, Yaoyao Lu, Jacques P. Tremblay, Gene Editing Strategies for Duchenne Muscular Dystrophy: From Molecular Mechanisms to Clinical Translation, Cells, 10.3390/cells15100852, 15, 10, (852), (2026).
- Aradhana Rohil, Gautam Kamila, Sheffali Gulati, Status of Clinical Care of Duchenne Muscular Dystrophy: Global Perspective and Situation in India, Indian Journal of Pediatrics, 10.1007/s12098-025-05975-z, 93, S1, (81-90), (2026).
- Shiny Thomas, Tahereh Neyaz, Kristin M. Conway, Aida Soim, Paul A. Romitti, Carla Zingariello, Joshua R. Mann, Trends in Corticosteroid Use Among Males With Duchenne Muscular Dystrophy (DMD) During 2000-2015: Data From the MD STAR net , Journal of Child Neurology, 10.1177/08830738251367466, (2025).
- H Lawrence Remmel, Sandra Hammer, Laurence Neff, Olivier Dorchies, Leonardo Scapozza, Dirk Fischer, Steven Quay, A Hypothesized Therapeutic Role of (Z)-Endoxifen in Duchenne Muscular Dystrophy (DMD), Degenerative Neurological and Neuromuscular Disease, 10.2147/DNND.S496904, Volume 15, (1-15), (2025).
- John F. Brandsema, Basil T. Darras, Dystrophinopathies, Rosenberg's Molecular and Genetic Basis of Neurological and Psychiatric Disease, 10.1016/B978-0-443-19176-3.00001-7, (535-561), (2025).
- Satish V. Khadilkar, Rakhil S. Yadav, Bhagyadhan A. Patel, Satish V. Khadilkar, Rakhil S. Yadav, Bhagyadhan A. Patel, Dystrophinopathies: Duchenne and Becker Muscular Dystrophies, Neuromuscular Disorders, 10.1007/978-981-97-9010-4_17, (211-233), (2024).
- Mohamed Said Ibrahim, Omar Ahmed Abdelwahab, Bashaer Elawfi, Fatmaelzahraa Yasser Ali, Sarah Amro, Shrouk F. Mohammed, Nour Shaheen, Ahmed Negida, Martin Arndt, Mido Max Hijazi, Jochen Schaefer, Timo Siepmann, Meta-analysis of the efficacy and safety of vamorolone in Duchenne muscular dystrophy, Neurological Sciences, 10.1007/s10072-024-07939-1, 46, 5, (2249-2262), (2024).
- Eszter Czifrus, Daniel J. Berlau, Corticosteroids for the treatment of Duchenne muscular dystrophy: a safety review, Expert Opinion on Drug Safety, 10.1080/14740338.2024.2394578, 23, 10, (1237-1247), (2024).
- Qin Wang, Yaqing Zeng, Linna Jiao, Jianli He, Baoyi Li, Yihua Guo, Zhibin Song, Efficacy and safety of different doses of vamorolone in boys with Duchenne muscular dystrophy: a systematic review and network meta-analysis, Frontiers in Neurology, 10.3389/fneur.2024.1456559, 15, (2024).
- Gustavo Simões Carnivali, Carlos Cristiano Borges, Method to link medicines to diseases using multiplex networks, Computer Methods in Biomechanics and Biomedical Engineering, 10.1080/10255842.2024.2362860, 28, 14, (2212-2225), (2024).
- See more