Estimating the risk of thrombotic events in people with congenital hemophilia A using US claims data
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Compare thrombotic risk in people with congenital hemophilia A (PwcHA) to the general non-hemophilia A (HA) population. Patients & methods: US claims databases were analyzed to identify PwcHA. Incidence rates of myocardial infarction, pulmonary embolism, ischemic stroke, deep vein thrombosis and device-related thrombosis were compared with a matched cohort without HA. Results: Over 3490 PwcHA were identified and 16,380 individuals matched. PwcHA had a similar incidence of myocardial infarction and pulmonary embolism compared with the non-HA population, but a slightly higher incidence of ischemic stroke and deep vein thrombosis. The incidence of device-related thrombosis was significantly higher in PwcHA. Conclusion: This analysis suggests that PwcHA are not protected against thrombosis, and provides context to evaluate thrombotic risk of HA treatments.
Hemophilia A (HA) is an X-linked hereditary disorder mainly affecting males, characterized by deficiency or dysfunction of coagulation factor VIII (FVIII) [1]. The hypocoagulable state of people with hemophilia A (PwHA) manifests as excessive, recurrent bleeding due to trauma and spontaneous bleeding into the soft tissues, joints and muscles [2]. It has been speculated that this hypocoagulable state could protect against thrombotic events (TEs), such as myocardial infarction (MI) [3], although epidemiological studies provide conflicting conclusions on the risk [4–6].
Traditional treatment for PwHA is FVIII replacement therapy, administered intravenously on demand or prophylactically for treatment and prevention of bleeding events, respectively [7]. Around 30% of people with severe HA develop inhibitors against FVIII, rendering FVIII replacement therapy ineffective [8], and are consequently treated with bypassing agents (BPAs) [9]. In recent years, nonfactor therapies (approved and undergoing investigation) with novel mechanisms of action or delivery have been developed, including small interfering RNA and antibody therapies [10]. These treatments restore hemostatic balance by replacing or substituting for the missing procoagulant or by inhibiting the action of the natural anticoagulants [11]. To date, the humanized bispecific monoclonal antibody emicizumab is the only approved nonfactor therapy for the treatment of HA [12]. Such novel therapeutics have facilitated a paradigm shift toward sustained therapeutic plasma levels, hemostasis or both instead of the peaks and troughs characteristic of traditional FVIII replacement [13]. It has been shown that the minimal FVIII level in the trough period can increase breakthrough bleeding risk [14], although there is no consensus on the critical FVIII threshold for bleed protection [15].
In a person without HA, the hemostatic system is tightly regulated so that coagulation occurs in the instance of an injury, but is not activated spontaneously in the absence of trauma [11]. When treatment for HA is initiated, normal coagulation should resume and prevent spontaneous bleeding [11]. Shifting the hemostatic balance too far in the opposite direction could promote a hypercoagulable state, increasing the thrombotic tendency, a recognized paradox in therapeutic approaches to inherited hemorrhagic and thrombotic disorders [11,16]. Indeed, elevated FVIII levels (>150 IU/dl) in the general population are associated with increased risk of TEs such as deep vein thrombosis (DVT); this pattern has been verified in numerous independent studies and is dose-dependent [17]. Thus, contrary to the bleeding episodes seen as the principal hallmark of HA, both arterial and venous TEs have also been reported in PwHA [18,19]. Multiple factors are thought to be involved in the occurrence of TEs in PwHA; namely, long-term use of central venous access devices (CVADs), reduced mobility due to joint disease or as a precautionary measure, other inherited or acquired prothrombotic risk factors (e.g., major surgery), and finally, the procoagulant therapies used to treat HA [18]. TEs have occurred after the administration of FVIII replacement therapies [19], BPAs [18,19], and the combination of a BPA, specifically activated prothrombin complex concentrate, and emicizumab [20]; although these events are rare. However, the relationship between HA treatment and TEs is complex, as the baseline thrombotic risk of PwHA is unknown [19] and good-quality evidence is lacking due to a dearth of large-scale studies, incomplete or unreliable reporting of existing comorbidities or other risk factors, and the difficulty of excluding treatment-associated risk [21].
Studies investigating TEs in PwHA have typically focused on cardiovascular risk, with inconsistent results [3–6,22,23]. Multiple studies, including a cohort study of female hemophilia carriers in The Netherlands [23] and a US-based cross-sectional analysis of PwHA or hemophilia B [6], have indicated that hemophilia provides some level of protection from cardiovascular TEs and mortality, presumably due to the lifelong hypocoagulability accompanying this disorder. This hypothesis has been strengthened by findings that alternative risk factors for cardiovascular mortality are still common in people with hemophilia, suggesting that it is not the absence of risk accounting for a lower cardiovascular mortality rate, but the protective effect of the hypocoagulable state [22]. In 2014, a review of cardiovascular risk in PwHA agreed with these findings, but nonetheless suggested that more research is required [3].
Other studies have directly contradicted this hypothesis [4,5]. In a retrospective analysis of claims data from the MarketScan Commercial and Medicare Research Databases from 2007 to 2009, aiming to quantify cardiovascular comorbidities in PwHA, PwHA (n = 2506) had a higher prevalence of ischemic stroke, arterial thrombosis and venous thrombosis compared with a non-HA population matched according to age, geographical location and health plan type (n = 7518) [4]. A prospective population-based study in The Netherlands likewise found no evidence of a protective effect of HA on atherosclerosis [5]. It should also be considered that PwHA who have cardiovascular risk factors may not receive the same interventions, such as antiplatelet or anticoagulation therapy, as the non-HA population, due to the challenge of balancing the equilibrium between thrombosis and hemorrhage risk [3]. As a result of the opposing and limited evidence, it is unknown whether TE risk differs in PwHA compared with the general non-HA population.
A preliminary study using a traditional approach to claims-based data analysis was conducted using the US IBM MarketScan Commercial Database and/or Medicare Supplemental Database to establish the risk of MI in people with congenital HA (PwcHA) [24]. However, to better identify PwcHA, the authors then applied a refined machine learning approach [24]. While a traditional approach to data analysis relies on a previously designed model with input from experts, a machine learning system begins with the outcome variables (in this case, identification of PwcHA), and automatically searches for predictor variables and how they interact with each other. Machine learning algorithms have the benefit of adapting over time as more data are inputted to increase their accuracy [25]. When the IBM MarketScan database was assessed using a machine learning approach, no increased risk of MI for PwcHA compared with a matched non-HA cohort was found [24]. While previous studies using administrative databases have been hampered by the lack of an accurate method for the identification of PwHA [26], this approach utilized a validated algorithm developed by Lyons et al., with over 90% specificity [26].
While limitations of this prior analysis did not affect the preliminary conclusions about MI [24], this subsequent analysis seeks to broaden the scope to other TEs of interest to the hemophilia community. The analysis reported here expands on the aforementioned preliminary study, using the machine learning approach to assess the risk of arterial and venous TEs, including MI, pulmonary embolism (PE), ischemic stroke, DVT and device-related thrombosis in PwcHA compared with individuals with no evidence of HA.
Materials & methods
Identification of PwcHA
A cohort of PwcHA was identified based on the following criteria: a confirmed diagnosis of congenital HA between 1 January 2000 and 30 June 2019; ≥1 medical or pharmacy claim for FVIII therapy, activated prothrombin complex concentrate, or activated FVII therapy; or ≥1 medical or pharmacy claim for FVIII/von Willebrand disease therapy and no diagnosis of von Willebrand disease; or ≥1 medical or pharmacy claim for desmopressin and ≥1 medically attended visit with a diagnosis of HA in the same claim line; or ≥1 medically attended visit with a HA diagnosis. Identification codes can be found elsewhere [26]. PwcHA were not stratified by HA treatment. The earliest date for fulfilling any of these inclusion criteria was deemed the individual’s index date. Individuals were required to have at least 183 days of continuous enrollment around the index date, with the index date occurring anytime within the 183 days. Ethical approval and informed consent were not required due to the nature of this study.
Cohort matching
Five cohorts were defined to investigate the risk of five main types of TE (MI, PE, ischemic stroke, DVT and device-related thrombosis); for each cohort, any person with a previous occurrence of the TE being investigated was excluded to eliminate bias of pre-disposition to that particular TE. International Classification of Disease (ICD)-9 and ICD-10 codes were used to identify the TEs (Supplementary Table 1), as well as HIV and hepatitis C status (Supplementary Table 2). The previously validated HA classification algorithm by Lyons et al. [26], set to 98.5% specificity and 77.8% sensitivity, was applied. Five matched cohorts of individuals with no evidence of HA in the study period were then randomly selected from the MarketScan database and frequency-matched to the HA cohorts by age, sex, insurance type, region, enrollment length, diabetes status and hypertensive status at an approximately 1:5 ratio, excluding any person with a previous occurrence of the TE being investigated.
Statistical analysis
A Poisson regression model was fitted to estimate the adjusted incidence rate ratio (IRR); the model was adjusted for all the covariates used for cohort matching (age, sex, insurance type, region, enrollment length, diabetes status and hypertensive status) as well as HIV and hepatitis C status at baseline, with age as a time-varying covariate.
Results
Population disposition
Across the five cohorts, 3498 PwcHA were identified with a ≥90% probability of being true PwcHA and over 16,380 non-HA individuals were matched; the five PwcHA cohorts and matched cohorts each comprised a slightly different number of individuals, due to the exclusion of individuals with previous evidence of that TE (Figure 1). Disposition was similar across all cohorts, including age, regional location within the US, insurance coverage and length of insurance enrollment (Table 1). Across the cohorts, 6.4–6.8% and 6.4–6.7% of the HA and non-HA populations, respectively, had evidence of diabetes, and 18.6–18.9% and 18.7–19.0% had evidence of hypertension.
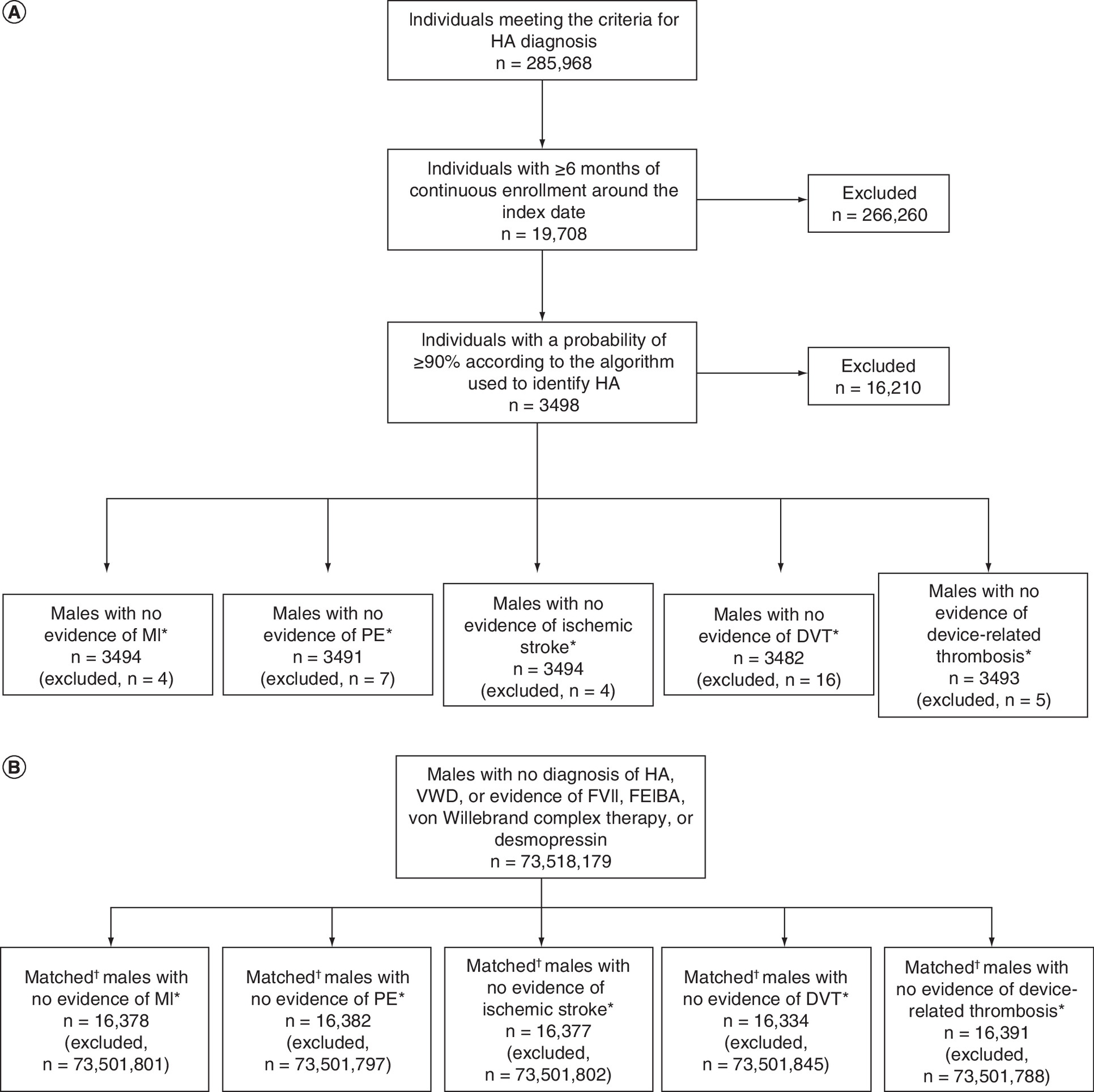
Figure 1. Attrition of study population.
(A) PwHA. (B) Matched non-HA population.
*No evidence of the TE being investigated between enrollment start and prior to index date.
†Individuals were matched on year of birth, year of enrollment, region, health plan and evidence of diabetes and hypertension at any time point during enrollment. Diabetes and hypertension had to be determined at any time point during enrollment before proceeding with the matching algorithm, as the index date was assigned after matching to a case.
FEIBA: Factor eight inhibitor bypassing activity; HA: Hemophilia A; PwHA: People with hemophilia A; TE: Thrombotic event; VWD: von Willebrand disease.
| MI | PE | Ischemic stroke | DVT | Device-related | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| HA (n = 3494) | Non-HA (n = 16,378) | HA (n = 3491) | Non-HA (n = 16,382) | HA (n = 3494) | Non-HA (n = 16,377) | HA (n = 3482) | Non-HA (n = 16,334) | HA (n = 3493) | Non-HA (n = 16,391) | |
| Sex, male, % | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Age, years, n (%) <18 18–35 36–45 46–55 56–65 66–75 ≥76 | 1481 (42.4) 1084 (31.0) 353 (10.1) 307 (8.8) 175 (5.0) 50 (1.4) 44 (1.3) | 6780 (41.4) 5155 (31.5) 1660 (10.1) 1470 (9.0) 867 (5.3) 220 (1.3) 226 (1.4) | 1481 (42.4) 1084 (31.1) 353 (10.1) 306 (8.8) 174 (5.0) 51 (1.5) 42 (1.2) | 6780 (41.4) 5155 (31.5) 1663 (10.2) 1470 (9.0) 860 (5.2) 230 (1.4) 224 (1.4) | 1480 (42.4) 1084 (31.0) 354 (10.1) 307 (8.8) 175 (5.0) 50 (1.4) 44 (1.3) | 6773 (41.4) 5154 (31.5) 1670 (10.2) 1475 (9.0) 871 (5.3) 212 (1.3) 222 (1.4) | 1479 (42.5) 1083 (31.1) 353 (10.1) 305 (8.8) 174 (5.0) 50 (1.4) 38 (1.1) | 6770 (41.4) 5148 (31.5) 1665 (10.2) 1461 (8.9) 858 (5.3) 224 (1.4) 208 (1.3) | 1479 (42.3) 1083 (31.0) 354 (10.1) 307 (8.8) 176 (5.0) 51 (1.5) 43 (1.2) | 6768 (41.3) 5150 (31.4) 1670 (10.2) 1477 (9.0) 872 (5.3) 231 (1.4) 223 (1.4) |
| US region, n (%) Northeast North central South West Unknown | 767 (22.0) 1008 (28.8) 852 (24.4) 796 (22.8) 71 (2.0) | 3590 (21.9) 4730 (28.9) 4008 (24.5) 3700 (22.6) 350 (2.1) | 766 (21.9) 1005 (28.8) 853 (24.4) 796 (22.8) 71 (2.0) | 3589 (21.9) 4725 (28.8) 4016 (24.5) 3702 (22.6) 350 (2.1) | 768 (22.0) 1007 (28.8) 853 (24.4) 795 (22.8) 71 (2.0) | 3593 (21.9) 4717 (28.8) 4020 (24.5) 3697 (22.6) 350 (2.1) | 764 (21.9) 1003 (28.8) 853 (24.5) 791 (22.7) 71 (2.0) | 3578 (21.9) 4716 (28.9) 4017 (24.6) 3673 (22.5) 350 (2.1) | 767 (22.0) 1009 (28.9) 850 (24.3) 796 (22.8) 71 (2.0) | 3596 (21.9) 4739 (28.9) 4003 (24.4) 3703 (22.6) 350 (2.1) |
| Insurance, n (%) MarketScan CCAE MarketScan Medicare | 3388 (97.0) 106 (3.0) | 15896 (97.1) 482 (2.9) | 3386 (97.0) 105 (3.0) | 15892 (97.0) 490 (3.0) | 3389 (97.0) 105 (3.0) | 15907 (97.1) 470 (2.9) | 3382 (97.1) 100 (2.9) | 15867 (97.1) 467 (2.9) | 3387 (97.0) 106 (3.0) | 15900 (97.0) 491 (3.0) |
| Enrollment length, years† Mean (SD) Median (Q1, Q3) | 4.2 (3.5) 2.8 (1.4–4.8) | 3.6 (3.2) 2.7 (1.3–4.8) | 4.2 (3.5) 3.0 (1.7–5.6) | 3.6 (3.2) 2.6 (1.3–4.8) | 4.2 (3.5) 3.0 (1.7–5.6) | 3.6 (3.2) 2.6 (1.3–4.8) | 4.2 (3.5) 3.0 (1.7–5.6) | 3.6 (3.2) 2.7 (1.3–4.8) | 4.2 (3.5) 3.0 (1.7–5.6) | 3.6 (3.2) 2.6 (1.3–4.8) |
| Evidence of diabetes,‡ n (%) | 233 (6.7) | 1079 (6.6) | 230 (6.6) | 1070 (6.5) | 229 (6.6) | 1057 (6.5) | 223 (6.4) | 1038 (6.4) | 237 (6.8) | 1104 (6.7) |
| Evidence of hypertension,‡ n (%) | 658 (18.8) | 3073 (18.8) | 661 (18.9) | 3105 (19.0) | 659 (18.9) | 3079 (18.8) | 649 (18.6) | 3056 (18.7) | 661 (18.9) | 3106 (18.9) |
For each cohort, any person with a previous occurrence of the TE being investigated was excluded.
†
Continuous enrollment that is at least 183 days long and encompasses the index date.
‡
Evidence of diabetes and/or hypertension was assessed at any timepoint during the enrollment period.
CCAE: Commercial Claims and Encounters Data; DVT: Deep vein thrombosis; HA: Hemophilia A; MI: Myocardial infarction; PE: Pulmonary embolism; Q: Quarter; SD: Standard deviation; TE: Thrombotic event.
Myocardial infarction
For the MI cohort, four PwcHA were excluded as they had history of MI, leaving a final cohort of 3494 PwcHA and a matched non-HA cohort of 16,378. The crude incidence rate of MI events for PwcHA was 0.23/100 person-years (PY) (95% CI, 0.15–0.32), compared with 0.19/100 PY (95% CI, 0.15–0.23) for the matched cohort; the incidence rate in both cohorts generally increased with age, as expected (Table 2; Figure 2), in line with the proportion who experienced an MI event during the study period (Table 3). The adjusted IRR was 1.23 (95% CI, 0.82–1.86), indicating that there was no difference in the rate of MI in PwcHA versus a matched non-HA control (Table 4).
| Age groups | MI | PE | Ischemic stroke | DVT | Device-related | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| HA | Non-HA | HA | Non-HA | HA | Non-HA | HA | Non-HA | HA | Non-HA | |
| <18 years n Follow-up, years Crude rate/100 PY (95% CI) | 2 5536 0.04 (0.00–0.10) | 2 20,770 0.01 (0.00–0.03) | 0 5542 N/A | 0 20,538 N/A | 3 5529 0.05 (0.01–0.13) | 1 20,383 0.0 (0.00–0.02) | 3 5522 0.05 (0.01–0.13) | 3 20,728 0.01 (0.00–0.03) | 36 5437 0.66 (0.46–0.90) | 3 20,803 0.01 (0.00–0.03) |
| 18–35 years n Follow-up, years Crude rate/100 PY (95% CI) | 3 3086 0.10 (0.02–0.23) | 3 11,481 0.03 (0.01–0.06) | 3 3087 0.10 (0.02–0.23) | 5 11,345 0.04 (0.01–0.09) | 1 3087 0.03 (0.00–0.12) | 2 11,264 0.02 (0.00–0.05) | 4 3084 0.13 (0.04–0.28) | 13 11,398 0.11 (0.06–0.18) | 4 3076 0.13 (0.04–0.28) | 3 11,417 0.03 (0.01–0.06) |
| 36–45 years n follow-up, years Crude rate/100 PY (95% CI) | 5 1357 0.37 (0.12–0.75) | 10 5462 0.18 (0.09–0.31) | 2 1370 0.15 (0.02–0.41) | 8 5754 0.14 (0.06–0.25) | 1 1379 0.07 (0.00–0.27) | 6 5499 0.11 (0.04–0.21) | 6 1355 0.44 (0.16–0.86) | 8 5421 0.15 (0.06–0.27) | 3 1372 0.22 (0.05–0.53) | 1 5439 0.02 (0.00–0.07) |
| 46–55 years n Follow-up, years Crude rate/100 PY (95% CI) | 5 1293 0.39 (0.13–0.79) | 29 5503 0.53 (0.35–0.74) | 1 1282 0.08 (0.00–0.29) | 11 5500 0.20 (0.10–0.33) | 8 1285 0.62 (0.27–1.12) | 22 5299 0.42 (0.26–0.61) | 5 1284 0.39 (0.13–0.80) | 13 5500 0.24 (0.13–0.38) | 11 1267 0.87 (0.43–1.45) | 7 5575 0.13 (0.05–0.23) |
| 56–65 years n Follow-up, years Crude rate/100 PY (95% CI) | 6 688 0.87 (0.32–1.70) | 19 2702 0.70 (0.42–1.05) | 1 698 0.14 (0.00–0.53) | 7 2699 0.26 (0.10–0.48) | 7 684 1.02 (0.41–1.91) | 25 2704 0.92 (0.60–1.32) | 8 670 1.19 (0.52–2.15) | 14 2677 0.52 (0.29–0.83) | 1 696 0.14 (0.00–0.53) | 7 2748 0.25 (0.10–0.48) |
| 66–75 years n Follow-up, years Crude rate/100 PY (95% CI) | 6 224 2.68 (0.98–5.22) | 11 897 1.23 (0.61–2.05) | 1 245 0.41 (0.01–1.51) | 6 984 0.61 (0.22–1.19) | 5 237 2.11 (0.69–4.33) | 16 962 1.66 (0.95, 2.57) | 2 236 0.85 (0.10–2.36) | 15 921 1.63 (0.91–2.55) | 0 247 N/A | 2 1013 0.20 (0.02–0.55) |
| ≥76 years n Follow-up, years Crude rate/100 PY (95% CI) | 1 160 0.63 (0.02–2.31) | 15 792 1.89 (1.06–2.96) | 2 155 1.29 (0.16–3.60) | 7 760 0.92 (0.37–1.72) | 11 127 8.63 (4.31–14.43) | 22 735 2.99 (1.88–4.37) | 3 141 2.12 (0.44–5.12) | 11 717 1.53 (0.77–2.56) | 1 159 0.63 (0.02–2.32) | 5 788 0.63 (0.21–1.30) |
| All N Follow-up, years Crude rate/100 PY (95% CI) | 28 12,343 0.23 (0.15–0.32) | 89 47,607 0.19 (0.15–0.23) | 10 12,379 0.08 (0.04–0.14) | 44 47,580 0.09 (0.07–0.12) | 36 12,328 0.29 (0.20–0.39) | 94 46,845 0.20 (0.16–0.24) | 31 12,292 0.25 (0.17–0.35) | 77 47,362 0.16 (0.13–0.20) | 56 12,255 0.46 (0.35–0.58) | 28 47,783 0.06 (0.04–0.08) |
For each cohort, any person with a previous occurrence of the TE being investigated (e.g., MI, PE, ischemic stroke, DVT, device-related thrombosis) was excluded.
DVT: Deep vein thrombosis; HA: Hemophilia A; MI: Myocardial infarction; N/A: Not applicable; PE: Pulmonary embolism; PY: Person-years; TE: Thrombotic event.
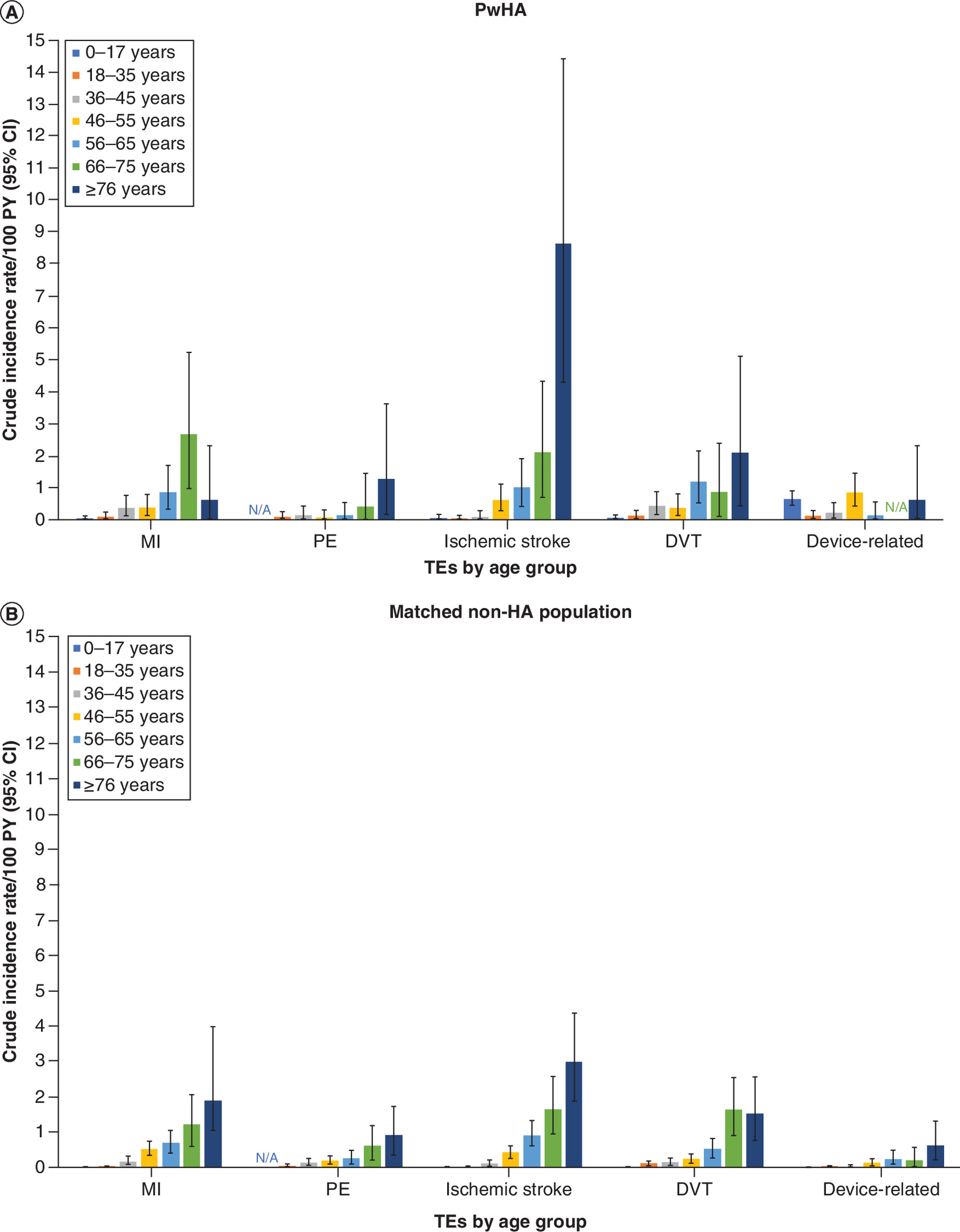
Figure 2. Crude incidence rates/100 person-years of thrombotic events by age group.
(A) PwHA. (B) Matched non-HA population.
HA: Hemophilia A; PwHA: People with hemophilia A; PY: Person-years; TE: Thrombotic event.
| Age groups | MI | PE | Ischemic stroke | DVT | Device-related | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| HA | Non-HA | HA | Non-HA | HA | Non-HA | HA | Non-HA | HA | Non-HA | |
| <18 years n At risk population % (95% CI) | 2 1481 0.14 (0.02–0.38) | 2 6780 0.03 (0.00–0.08) | 0 1481 0.00 (0.00–0.00) | 0 6780 0.00 (0.00–0.00) | 3 1480 0.20 (0.04–0.49) | 1 6773 0.01 (0.00–0.05) | 3 1479 0.20 (0.04–0.49) | 3 6770 0.04 (0.01–0.11) | 36 1479 2.43 (1.70–3.29) | 3 6768 0.04 (0.01–0.11) |
| 18–35 years n At risk population % (95% CI) | 3 1084 0.28 (0.06–0.67) | 3 5155 0.06 (0.01–0.14) | 3 1084 0.28 (0.06–0.67) | 5 5155 0.10 (0.03–0.20) | 1 1084 0.09 (0.00–0.34) | 2 5154 0.04 (0.00–0.11) | 4 1083 0.37 (0.1–0.81) | 13 5148 0.25 (0.13–0.41) | 4 1083 0.37 (0.10–0.81) | 3 5150 0.06 (0.01–0.14) |
| 36–45 years n At risk population % (95% CI) | 5 353 1.42 (0.46–2.90) | 10 1660 0.60 (0.29–1.03) | 2 353 0.57 (0.07–1.58) | 8 1663 0.48 (0.21–0.87) | 1 354 0.28 (0.01–1.04) | 6 1670 0.36 (0.13–0.70) | 6 353 1.70 (0.62–3.31) | 8 1665 0.48 (0.21–0.87) | 3 354 0.85 (0.17–2.04) | 1 1670 0.06 (0.00–0.22) |
| 46–55 years n At risk population % (95% CI) | 5 307 1.63 (0.53–3.34) | 29 1470 1.97 (1.32–2.75) | 1 306 0.33 (0.01–1.21) | 11 1470 0.75 (0.37–1.25) | 8 307 2.61 (1.13–4.70) | 22 1475 1.49 (0.93–2.18) | 5 305 1.64 (0.53–3.36) | 13 1461 0.89 (0.47–1.43) | 11 307 3.58 (1.79–5.99) | 7 1477 0.47 (0.19–0.88) |
| 56–65 years n At risk population % (95% CI) | 6 175 3.43 (1.26–6.67) | 19 867 2.19 (1.32–3.28) | 1 174 0.57 (0.01–2.12) | 7 860 0.81 (0.33–1.52) | 7 175 4.00 (1.61–7.46) | 25 871 2.87 (1.86–4.10) | 8 174 4.60 (1.98–8.29) | 14 858 1.63 (0.89–2.59) | 1 176 0.57 (0.01–2.10) | 7 872 0.80 (0.32–1.50) |
| 66–75 years n At risk population % (95% CI) | 6 50 12.00 (4.40–23.34) | 11 220 5.00 (2.50–8.36) | 1 51 1.96 (0.05–7.23) | 6 230 2.61 (0.96–5.07) | 5 50 10.0 (3.25–20.48) | 16 212 7.55 (4.31–11.67) | 2 50 4.00 (0.48–11.14) | 15 224 6.70 (3.75–10.49) | 0 51 0.00 (0.00–0.00) | 2 231 0.87 (0.10–2.41) |
| ≥76 years n At risk population % (95% CI) | 1 44 2.27 (0.06–8.38) | 15 226 6.64 (3.71–10.39) | 2 42 4.76 (0.58–13.27) | 7 224 3.13 (1.26–5.83) | 11 44 25.00 (12.48–41.80) | 22 222 9.91 (6.21–14.46) | 3 38 7.89 (1.63–19.01) | 11 208 5.29 (2.64–8.84) | 1 43 2.33 (0.06–8.58) | 5 223 2.24 (0.73–4.59) |
| All N At risk population % (95% CI) | 28 3494 0.80 (0.53–1.12) | 89 16,378 0.54 (0.44–0.66) | 10 3491 0.29 (0.14–0.49) | 44 16,382 0.27 (0.20–0.35) | 36 3494 1.03 (0.72–1.39) | 94 16,377 0.57 (0.46–0.70) | 31 3482 0.89 (0.60–1.23) | 77 16,334 0.47 (0.37–0.58) | 56 3493 1.60 (1.21–2.05) | 28 16,391 0.17 (0.11–0.24) |
For each cohort, any person with a previous occurrence of the TE being investigated (e.g., MI, PE, ischemic stroke, DVT, device-related thrombosis) was excluded.
DVT: Deep vein thrombosis; HA: Hemophilia A; MI: Myocardial infarction; PE: Pulmonary embolism; TE: Thrombotic event.
| TE | Adjusted IRR (95% CI) |
|---|---|
| MI | 1.23 (0.82–1.86) |
| PE | 0.89 (0.45–1.77) |
| Ischemic stroke | 1.48 (1.01–2.16) |
| DVT | 1.53 (1.00–2.32) |
| Device-related thrombosis | 7.93 (5.00–12.59) |
For each cohort, any person with a previous occurrence of the TE being investigated (e.g., MI, PE, ischemic stroke, DVT, device-related thrombosis) was excluded. Rates were adjusted by evidence of HIV or hepatitis C in the 6 months prior to index date.
DVT: Deep vein thrombosis; HA: Hemophilia A; HIV: Human immunodeficiency virus; IRR: Incidence rate ratio; MI: Myocardial infarction; PE: Pulmonary embolism; TE: Thrombotic event.
Pulmonary embolism
A total of seven PwcHA with a history of PE were excluded; the remaining 3491 PwcHA and 16,382 matched individuals with no evidence of HA formed the two cohorts. A similar incidence rate for PE was seen for both cohorts (PwcHA, 0.08 [95% CI, 0.04–0.14] vs matched population, 0.09 [95% CI, 0.07–0.12]), which increased with age (Table 2; Figure 2). The adjusted IRR was 0.89 (95% CI, 0.45–1.77), again suggesting there is no difference in the rate of PE in PwcHA compared with the general population.
Ischemic stroke
Four PwcHA were excluded from the cohorts measuring the incidence of ischemic stroke, leaving 3494 PwcHA and 16,377 in the matched non-HA population. A slightly higher incidence rate of ischemic stroke was seen in PwcHA (0.29/100 PY [95% CI, 0.20–0.39]) compared with the matched non-HA population (0.20/100 PY [95% CI, 0.16–0.24]; Table 2; Figure 2), supported by an adjusted IRR of 1.48 (95% CI, 1.01–2.16). The incidence of ischemic stroke rose with age (Table 2; Figure 2), with rates of 8.63/100 PY (95% CI, 4.31–14.43) and 2.99/100 PY (95% CI, 1.88–4.37) in those who were at least 76 years old in PwcHA and the matched non-HA population, respectively.
Deep vein thrombosis
The cohorts to investigate the risk of DVT comprised 3482 PwcHA (16 excluded) and 16,334 matched individuals without HA. As for ischemic stroke, the analysis suggested a slightly higher incidence rate for DVT in PwcHA (0.25/100 PY [95% CI, 0.17–0.35]) compared with the matched non-HA population (0.16/100 PY [95% CI, 0.13–0.20]) (Table 2; Figure 2), underpinned by an adjusted IRR of 1.53 (95% CI, 1.00–2.32). As for the other TEs, the incidence of DVT increased with age for both populations (Table 2).
Device-related thrombosis
A total of 3493 PwcHA (five excluded) and 16,391 of the matched non-HA population comprised the cohorts for comparison of device-related thrombosis. The incidence rate for device-related thrombosis in PwcHA was substantially higher than for the matched non-HA population (0.46/100 PY [95% CI, 0.35–0.58] vs 0.06/100 PY [95% CI, 0.04–0.08], respectively), reflected by a significant adjusted IRR of 7.93 (95% CI, 5.00–12.59). In the general population, the rate of device-related thrombosis increased with age (Table 2; Figure 2), from 0.01/100 PY (95% CI, 0.00–0.03) for those 0–17 years of age, to 0.63/100 PY (95% CI, 0.21–1.30) for those ≥76 years of age. In contrast, there was no clear age-related trend for PwcHA: the rate of device-related thrombosis in PwcHA was 0.66/100 PY (95% CI, 0.46–0.90) compared with 0.63/100 PY (95% CI, 0.02–2.32) for those who were 0–17 and ≥76 years of age, respectively (Table 2; Figure 2). Adjusted IRR rates by age can be seen in Supplementary Table 3.
Discussion
This claims-based data analysis evaluated the risk of five key types of TE in PwcHA: MI, PE, stroke, DVT and device-related thrombosis, using the IBM Marketscan Commercial Database and/or Medicare Supplemental Database. A machine learning approach was used, with a previously validated HA classification algorithm [26], enabling greater accuracy in identifying PwHA compared with previous studies. Additional strengths of this analysis were the cohort matching, in which the non-HA population were matched for age, sex, insurance type, region, enrollment length, and diabetes and hypertensive status; and the exclusion of individuals who had previously experienced each type of TE, to remove any bias of pre-disposition.
As expected, the incidence of all TEs increased with age (a prothrombotic risk factor) [27], except for device-related thrombosis in PwcHA. A significantly higher proportion of PwcHA experienced a device-related thrombosis compared with the matched non-HA population (IRR: 7.93 [95% CI, 5.00–12.59]). This was expected, as PwcHA often require a CVAD to administer prophylaxis or immune tolerance therapy [28]. It is known that these devices carry a risk of thrombosis, due to the combination of the thrombogenic potential of the CVAD with regular administration of clotting factor concentrates, which predisposes the site around the tip of the catheter to thrombus formation [29]. Indeed, CVADs are relatively contraindicated in individuals with a history of thrombosis due to device-related large vessel occlusion [28]. This risk is believed to be higher with external catheters, particularly peripherally inserted central catheters [30], rather than implanted ports [29]. CVADs are especially likely to be fitted in children with HA, in whom repeated venipuncture is frequently challenging due to the potentially traumatic nature of the procedure [29]. This could explain the substantially higher rate of device-related thrombosis in 0–17-year-old PwcHA (IRR: 46.56 [95% CI, 14.31–151.48]) compared with the matched non-HA population of 0–17-year-olds, and provides a reason for the lack of correlation between the risk of device-related thrombosis and age in PwcHA. There was little to no difference between PwcHA and the general population in the rate of device-related thrombosis by the age of 56 or older; this may reflect that the causes of device-related thrombosis in elderly PwcHA are due to other devices that are also more frequently used in the general population, such as pacemakers or other cardiac interventions [31]. Unfortunately, the exact cause is unknown, as the device associated with the TE could not be identified using the existing ICD codes.
The incidences of ischemic stroke and DVT were slightly higher in the HA population compared with the general non-HA population. This was unexpected; it may be a phenomenon related to HA caused by the regular FVIII replacement therapies that many PwcHA receive, as FVIII levels are a recognized risk factor for both ischemic stroke and DVT [32,33]. As the FVIII levels of PwcHA receiving replacement FVIII are typically still subnormal [13], it could be theorized that this is related to the ‘peak’ that occurs shortly after administration, or in the case of surgery, the high doses of FVIII administered prophylactically to reduce hemorrhage risk [34]. Hence, the question of whether the administration of FVIII concentrates contributes to the risk of TEs, even if FVIII levels are not in the supraphysiological range, should be further investigated. Alternatively, it may be that the individuals in whom these events occur have other risk factors for ischemic stroke and DVT, and yet do not receive appropriate prophylaxis or interventions due to their underlying HA (e.g., a person with severe HA in hospital for a surgery where prophylactic anticoagulants might otherwise be given); this highlights the value of a multidisciplinary approach to risk management in PwcHA. Furthermore, PwcHA may be more susceptible to some types of TE, such as DVT, due to a risk-averse attitude to physical activity and a more sedentary lifestyle [35]. It is also possible that severe FVIII defects such as large Xq28 lesions may have impacted the number of cerebral angiopathies occurring in the HA population due to BRCC3 defect-related moyamoya syndrome [36,37]. This possibility cannot be explored in this study as the presence of genetic biomarkers is not included in administrative claims data. Nevertheless, given the rarity of this condition [38], the authors believe it is unlikely to have had a significant influence on the findings reported here. The remainder of the TEs, MI and PE, had similar incidence rates in the HA population and the matched non-HA population. These TEs may be caused in PwcHA by the same risk factors as in the general non-HA population, for example: hyperlipidemia, smoking, diabetes, hypertension, and obesity for arterial TEs; trauma or fractures, surgery, hormonal therapy, pregnancy, hypercoagulability and age for venous TEs [27].
Overall, these data do not demonstrate evidence of the theorized protective effect of a hypocoagulable state among PwcHA at a population level [3]; however, as the overwhelming majority of PwcHA included in this analysis may be presumed to be receiving some form of treatment for their HA, the thrombotic risk found here includes treatment-associated risk and is not reflective of the baseline thrombotic risk in PwcHA. Treatments for HA are designed to restore hemostatic function, and in doing so, may align thrombotic risk for PwcHA with that of the general population when used prophylactically or on demand, removing or reducing any presumed protective effect of a hypocoagulable state [16]. Additionally, it is thought that the peaks achieved through traditional FVIII replacement therapy may influence thrombotic risk, particularly in situations that would typically require anticoagulant therapy such as surgeries or atrial fibrillation [39]. The questions of whether pharmacokinetic-based dosing of FVIII may help maintain the hemostatic equilibrium [34], or whether nonfactor therapies that achieve partially restored hemostatic potential through sustained therapeutic plasma levels may have a different impact [40], remain unanswered. The prothrombotic effect of HA therapies may be of greater concern for individuals with severe HA receiving intensive procoagulant treatment of factor replacement therapy and/or BPAs. Hence, it is important that PwcHA are informed of the typical risk factors for TEs. This analysis provides a foundation for the risk of TEs in PwcHA, enabling comparison with the thrombotic risk of new treatments within clinical trial programs and subsequently as they become available on the market. As such, any significantly increased risk associated with a particular treatment can be signaled.
Limitations of these results include those usually associated with secondary, claims-based data: the findings are only directly applicable to the insured population; the identification of PwcHA is dependent on the specificity of the algorithm used; the identification of TEs is dependent on the accuracy of professional ICD coding (for example, codes to identify ischemic stroke were used, but some incidences of hemorrhagic stroke may be included if the codes are not completely accurate); and the outcomes of clinical cases are unknown [41]. Although the codes for the different TEs in this analysis are mutually exclusive, coding practices are difficult to assess, and a single event could be coded across multiple types by the billing coder. Moreover, secondary data use studies do not control for, nor analyze the contribution of, lifestyle-related confounders, such as smoking, drinking, exercise and BMI. In the machine learning approach taken here, the identification of PwcHA was based on a probabilistic algorithm set with relatively low sensitivity (77.8%) but high specificity (98.5%); while this approach improves the accuracy of the analysis, the results could still be subject to inadvertent selection bias due to an overly cautious approach to false positives. However, a small number of people without HA or with acquired HA may still be included. Due to the rarity of TEs, the number of TEs that occurred in this large population was still fairly low; therefore, it is possible that some high-risk individuals may have influenced the analysis.
Other limitations include restrictions of the MarketScan database; for example, the population entirely comprises people with private healthcare insurance, and the ethnicities of individuals were not available (a notable factor, as the prevalence of TEs varies significantly among different ethnic populations [42,43], which may impact the findings as it was not accounted for in the population matching). Additionally, the population identified in this study is skewed toward the younger age groups (although individuals had to have 6 months of continuous data before HA diagnosis), presumably due to the majority being drawn from the commercial database for those covered by employer-sponsored private health insurance, with only a small number being from the Medicare database for retirees. A younger population with private healthcare insurance may not be representative of the general US population, restricting the universal applicability of the TE incidence rates reported here. It should also be noted that PwcHA were not stratified by disease severity, so it is unknown if individuals with severe HA may be at greater risk of TEs compared with individuals with mild HA, or vice versa.
Finally, any treatments PwcHA were receiving were not considered, although it can be presumed that the overwhelming majority would be receiving treatment of some type for their HA; thus, it was not possible to establish the baseline thrombotic risk of PwcHA or compare this to the treatment-associated risk. However, as uncontrolled HA is a life-threatening condition, it would be extremely difficult, and unethical, to identify and study PwcHA who were receiving no interventions for their disease. Other variables that may affect TE incidence, such as corticosteroid usage, cancers, surgeries, traumas and statin usage, were not controlled for, as the results of this study were intended to describe the rate of TEs in the HA population rather than to establish causation. The thrombotic risk may also differ between PwcHA treated on demand versus prophylactically or by the intensity of dosing regimens, which this study did not account for. In future studies, it may be beneficial to measure adherence and persistence to procoagulant treatment, to examine any possible association with the rate of TEs in PwcHA.
Conclusion
In conclusion, this analysis of US claims data from 2000–2019 suggests that having HA does not protect against four key types of TEs: MI, ischemic stroke, DVT and PE. These data suggest PwcHA do not have a significantly different risk of MI or PE, but did exhibit a slightly increased risk of ischemic stroke and DVT, compared with the non-HA population, which may warrant further investigation. Furthermore, the analysis found an increased risk of device-related thrombosis; this finding was expected, as devices such as CVADs are often used for the administration of treatment in PwcHA, particularly in young children, and PwcHA are therefore much more likely to be using such a device compared with the general population. To the authors’ knowledge, this analysis represents the largest real-world data study investigating TEs in the HA population. While every effort was taken to mitigate the effects of confounders and bias, the results should be interpreted cautiously given the limitations of a secondary data use study, and in the context of this study’s set objective to describe TE risk in the HA population. It is hoped that future studies will further explore the causes behind these risk rates, to address factors that are speculated upon here.
It is important that PwcHA are aware of the thrombotic risk associated with devices such as CVADs and intensive procoagulant regimens, as well as general prothrombotic risk factors, and should be supported in reducing those that are modifiable. Moreover, a multidisciplinary approach should be taken in situations where PwcHA may be at risk of thrombosis, such as when procoagulant therapies would ordinarily be administered, to ensure their condition is adequately managed. Finally, these data provide crucial context for examining the thrombotic risk of current and future treatments for HA, so that any excessive risk of TEs associated with a particular treatment can be recognized.
•
It has long been speculated that people with congenital hemophilia A (PwcHA) may have some degree of protection from thrombotic events, due to the hypocoagulable state caused by hemophilia A (HA).
•
However, the evidence is conflicting; it is unclear if this protection exists and how it may translate into a real-world setting in which PwcHA receive treatment for their condition.
•
This research compares the risk of five types of thrombotic events (TEs): myocardial infarction, pulmonary embolism, ischemic stroke, deep vein thrombosis and device-related thrombosis, between PwcHA and a matched non-HA population.
•
Data from the US MarketScan Commercial and Medicare Research Databases spanning 19 years (2000–2019) and including over 3490 PwcHA and 16,380 matched non-HA individuals were analyzed to comprise the largest real-world data study investigating thrombotic events in PwcHA to date.
•
As expected, the incidence of all TEs increased with age (a prothrombotic risk factor), except for device-related thrombosis in PwcHA.
•
A significantly higher proportion of PwcHA experienced a device-related thrombosis compared with the matched non-HA population, likely because PwcHA often require a central venous access device to administer prophylaxis or immune tolerance therapy.
•
The incidences of ischemic stroke and deep vein thrombosis were slightly higher in the HA population compared with the matched non-HA population.
•
Myocardial infarction and pulmonary embolism had similar incidence rates in the HA population and the matched non-HA population.
•
Evidence herein indicates that the theoretical protection from TEs due to a hypocoagulable state is unsubstantiated, or, that the protection afforded is negated by the use of hemostatic treatments.
•
PwcHA should be monitored for thrombotic risk factors, and the thrombotic risk of HA treatments evaluated.
Author contributions
I Faghmous, C Flores, AM Patel and P Kuebler contributed to the initial design and concept of this study. C Flores performed the data analysis. All authors interpreted the data and critically reviewed and approved the manuscript prior to submission. All authors agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank C Sima and K Sarouei for their contributions to the initial concept and groundwork of this study.
Financial & competing interests disclosure
This work was supported by F. Hoffmann-La Roche Ltd. None of the authors received honoraria or fees for their contribution to the development of this manuscript. I Faghmous is a previous employee of F. Hoffmann-La Roche Ltd and Gilead Sciences, Inc. F Nissen is a current employee of F. Hoffmann-La Roche Ltd. P Kuebler is a current employee of and holds shares in Genentech, Inc. C Flores is a current employee of Genesis Research. AM Patel is a current employee of Genentech, Inc. SW Pipe has received consultancy and honoraria from Apcintex Ltd., Bayer AG, BioMarin Pharmaceutical, Catalyst Biosciences, CSL Behring, HEMA Biologics Inc., F. Hoffmann-La Roche Ltd., Freeline Therapeutics, Novo Nordisk, Pfizer Inc., Sangamo Therapeutics Inc., Sanofi, Takeda Pharmaceutical Company Ltd., Spark Therapeutics Inc. and uniQure NV; has received research funding from Siemens AG; and is a member of the board of directors/advisory committee for the Medical and Scientific Advisory Council to the National Hemophilia Foundation and the Medical Advisory Board to World Federation of Hemophilia. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support for the development of this manuscript, under the direction of the authors, was provided by P Tate of Ashfield MedComms, an Ashfield Health company, and funded by F. Hoffmann-La Roche Ltd.
Ethical conduct of research
Institutional review board approval and informed consent were not required due to the nature of this study.
Data sharing statement
Data are available from the US IBM MarketScan Commercial Database and Medicare Supplemental Database. The ICD-9-CM and ICD-10-CM code listings used can be found in Supplementary Tables 1 & 2.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 54.34 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Franchini M, Mannucci PM. Past, present and future of hemophilia: a narrative review. Orphanet J. Rare Dis. 7, 24 (2012).
2.
Srivastava A, Santagostino E, Dougall A et al. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia 26(S6), 1–158 (2020).
3.
Kamphuisen PW, ten Cate H. Cardiovascular risk in patients with hemophilia. Blood 123(9), 1297–1301 (2014).
• Summarizes important background context on risk of thrombotic events (TEs), such as myocardial infarction in people with hemophilia, speculating that their hypocoagulable state could offer protection against thrombus formation.
4.
Pocoski J, Ma A, Kessler CM, Boklage S, Humphries TJ. Cardiovascular comorbidities are increased in U.S. patients with haemophilia A: a retrospective database analysis. Haemophilia 20(4), 472–478 (2014).
•• This study of US claims data from 2007 to 2009 quantified cardiovascular comorbidities in people with hemophilia A (PwHA, n = 2506) compared with a matched non-hemophilia A (HA) population (n = 7518) and found that the former had a higher prevalence of ischemic stroke, arterial thrombosis and venous thrombosis.
5.
Tuinenburg A, Rutten A, Kavousi M et al. Coronary artery calcification in hemophilia A: no evidence for a protective effect of factor VIII deficiency on atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 32(3), 799–804 (2012).
•• This population-based imaging study in The Netherlands found no evidence of a protective effect of HA against atherosclerosis.
6.
Sood SL, Cheng D, Ragni M et al. A cross-sectional analysis of cardiovascular disease in the hemophilia population. Blood Adv. 2(11), 1325–1333 (2018).
7.
Franchini M, Mannucci PM. Hemophilia A in the third millennium. Blood Rev. 27(4), 179–184 (2013).
8.
Gomez K, Klamroth R, Mahlangu J, Mancuso ME, Mingot ME, Ozelo MC. Key issues in inhibitor management in patients with haemophilia. Blood Transfus. 12(Suppl. 1), S319–S329 (2014).
9.
Shapiro AD, Mitchell IS, Nasr S. The future of bypassing agents for hemophilia with inhibitors in the era of novel agents. J. Thromb. Haemost. 16(12), 2362–2374 (2018).
10.
Spadarella G, Di Minno A, Milan G et al. Paradigm shift for the treatment of hereditary haemophilia: towards precision medicine. Blood Rev. 39, 100618 (2020).
11.
Callaghan MU, Sidonio R, Pipe SW. Novel therapeutics for hemophilia and other bleeding disorders. Blood 132(1), 23–30 (2018).
12.
Kitazawa T, Esaki K, Tachibana T et al. Factor VIIIa-mimetic cofactor activity of a bispecific antibody to factors IX/IXa and X/Xa, emicizumab, depends on its ability to bridge the antigens. Thromb. Haemost. 117(7), 1348–1357 (2017).
13.
Weyand AC, Pipe SW. New therapies for hemophilia. Blood 133(5), 389–398 (2019).
14.
Ljung R, Fischer K, Carcao M et al. Practical considerations in choosing a factor VIII prophylaxis regimen: role of clinical phenotype and trough levels. Thromb. Haemost. 115(5), 913–920 (2016).
15.
Lambert T, Benson G, Dolan G et al. Practical aspects of extended half-life products for the treatment of haemophilia. Ther. Adv. Hematol. 9(9), 295–308 (2018).
16.
Wolberg AS, Aleman MM, Leiderman K, Machlus KR. Procoagulant activity in hemostasis and thrombosis: virchow's triad revisited. Anesth. Analg. 114(2), 275–285 (2012).
• Considers the pathophysiologic mechanisms underlying TEs, providing important theory behind how a hypercoagulable state and thrombotic tendency could develop if the hemostatic balance is shifted too far with therapeutic approaches to inherited hemorrhagic and thrombotic disorders.
17.
Jenkins PV, Rawley O, Smith OP, O'Donnell JS. Elevated factor VIII levels and risk of venous thrombosis. Br. J. Haematol. 157(6), 653–663 (2012).
18.
Franchini M. Thrombotic complications in patients with hereditary bleeding disorders. Thromb. Haemost. 92(08), 298–304 (2004).
19.
Ruiz-Sáez A. Thrombosis in rare bleeding disorders. Hematology 17(Suppl. 1), S156–S158 (2012).
• Describes the conditions and risk factors associated with thrombosis in PwHA.
20.
Oldenburg J, Mahlangu JN, Kim B et al. Emicizumab prophylaxis in hemophilia A with inhibitors. N. Engl. J. Med. 377(9), 809–818 (2017).
21.
Makris M. Thrombosis in bleeding disorders. In: The ISTH Workshop on Thrombosis and Hemostasis. International Society on Thrombosis and Haemostasis, Bangkok, Thailand (2017).
22.
Biere-Rafi S, Baarslag MA, Peters M et al. Cardiovascular risk assessment in haemophilia patients. Thromb. Haemost. 105(02), 274–278 (2011).
23.
Šrámek A, Kriek M, Rosendaal FR. Decreased mortality of ischaemic heart disease among carriers of haemophilia. Lancet 362(9381), 351–354 (2003).
24.
Faghmous I, Flores C, Sarouei K et al. Estimating the risk of myocardial infarction in persons with hemophilia A using a machine-learning approach with US claims data. 61st ASH (American Society of Hematology) Annual Meeting & Exposition. https://www.cpg-medicaleducation.de/media/faghmous_ash_2019_mi_haemophilia_a_1.pdf
25.
Meyfroidt G, Güiza F, Ramon J, Bruynooghe M. Machine learning techniques to examine large patient databases. Best Pract. Res. Clin. Anaesthesiol. 23(1), 127–143 (2009).
26.
Lyons J, Desai V, Xu Y et al. Development and validation of an algorithm for identifying patients with hemophilia A in an administrative claims database. Value Health 21(9), 1098–1103 (2018).
27.
Previtali E, Bucciarelli P, Passamonti SM, Martinelli I. Risk factors for venous and arterial thrombosis. Blood Transfus. 9(2), 120–138 (2011).
• Summarizes risk factors for thrombosis in the general population: hyperlipidemia, smoking, diabetes, hypertension and obesity for arterial TEs; trauma or fractures, surgery, hormonal therapy, pregnancy, hypercoagulability and age for venous TEs.
28.
Ewenstein BM, Valentino LA, Journeycake JM et al. Consensus recommendations for use of central venous access devices in haemophilia. Haemophilia 10(5), 629–648 (2004).
29.
Valentino LA, Ewenstein B, Navickis RJ, Wilkes MM. Central venous access devices in haemophilia. Haemophilia 10(2), 134–146 (2004).
•• This systematic review and meta-analysis of complications associated with central venous access devices summarized their risk of thrombosis, due to the combination of the thrombogenic potential of the central venous access device with regular administration of clotting factor concentrates, which predisposes the site around the tip of the catheter to thrombus formation.
30.
Jaffray J, Witmer C, O'Brien SH et al. Peripherally inserted central catheters lead to a high risk of venous thromboembolism in children. Blood 135(3), 220–226 (2020).
31.
Buttigieg J, Asciak R, Azzopardi CM. Pacemaker lead-associated thrombosis in cardiac resynchronisation therapy. BMJ Case Rep. 2015, (2015).
32.
Chang TR, Albright KC, Boehme AK et al. Factor VIII in the setting of acute ischemic stroke among patients with suspected hypercoagulable state. Clin. App. Thromb. Hemost. 20(2), 124–128 (2014).
•• Demonstrates that high factor VIII (FVIII) levels are a risk factor for both ischemic stroke; in some settings, such as surgery, replacement therapies lead to elevated levels of FVIII in PwHA and could therefore increase risk of TEs.
33.
Kyrle PA, Minar E, Hirschl M et al. High plasma levels of factor VIII and the risk of recurrent venous thromboembolism. N. Engl. J. Med. 343(7), 457–462 (2000).
34.
Hazendonk HCAM, van Moort I, Mathôt RAA et al. Setting the stage for individualized therapy in hemophilia: what role can pharmacokinetics play? Blood Rev. 32(4), 265–271 (2018).
35.
Timmer MA, Pisters MF, de Kleijn P, de Bie RA, Schutgens REG, Veenhof C. Movement behaviour in adults with haemophilia compared to healthy adults. Haemophillia 24(3), 445–451 (2018).
36.
Janczar S, Fogtman A, Koblowska M et al. Novel severe hemophilia A and moyamoya (SHAM) syndrome caused by Xq28 deletions encompassing F8 and BRCC3 genes. Blood 123(25), 4002–4004 (2014).
37.
Miskinyte S, Butler MG, Hervé D et al. Loss of BRCC3 deubiquitinating enzyme leads to abnormal angiogenesis and is associated with syndromic moyamoya. Am. J. Hum. Genet. 88(6), 718–728 (2011).
38.
Roh D, Roth W, Al-Mufti F et al. The utility of factor VIII infusion in a rare case of SHAM Syndrome (P4.343). Neurology 86(Suppl. 16), P4.343 (2016).
39.
Martin K, Key NS. How I treat patients with inherited bleeding disorders who need anticoagulant therapy. Blood 128(2), 178–184 (2016).
40.
Makris M, Iorio A, Lenting PJ. Emicizumab and thrombosis: the story so far. J. Thromb. Haemost. 17(8), 1269–1272 (2019).
41.
Tyree PT, Lind BK, Lafferty WE. Challenges of using medical insurance claims data for utilization analysis. Am. J. Med. Qual. 21(4), 269–275 (2006).
42.
Kurian AK, Cardarelli KM. Racial and ethnic differences in cardiovascular disease risk factors: a systematic review. Ethn. Dis. 17(1), 143–152 (2007).
43.
White RH, Keenan CR. Effects of race and ethnicity on the incidence of venous thromboembolism. Thromb. Res. 123(Suppl. 4), S11–S17 (2009).
Information & Authors
Information
Published In
Pages: 1323 - 1336
PubMed: 34676773
Copyright
© 2021 F. Hoffmann-La Roche Ltd. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 21 May 2021
Accepted: 30 September 2021
Published online: 22 October 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Estimating the risk of thrombotic events in people with congenital hemophilia A using US claims data. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0120
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Massimo Franchini, Matteo Zani, Daniele Focosi, Human Evolution: Between Hemorrhage and Thrombosis, Seminars in Thrombosis and Hemostasis, 10.1055/a-2905-4308, (2026).
- Guy Young, Kaan Kavakli, Robert Klamroth, Tadashi Matsushita, Flora Peyvandi, Steven W. Pipe, Savita Rangarajan, Ming-Ching Shen, Alok Srivastava, Jing Sun, Huyen Tran, Chur-Woo You, Bülent Zülfikar, Laurel A. Menapace, Chuanwu Zhang, Yuqian Shen, Marja Puurunen, Marek Demissie, Gili Kenet, Teh-Liane Khoo, Scott Dunkley, Stephanie P'ng, Dominic Pepperell, Stephanie Lam, Elizabeth Steinepreis, Jacques Malherbe, Tulene Kendrick, Marcus Lombard, Huyen Tran, Jessie Zhao, Hannah Stevens, Caroline Dix, James McFadyen, Jean St-Louis, Jeannine Kassis, Georges Rivard, Jing Sun, Xiaofang Li, Huiping Li, Jieyu Ye, Xuan Zhou, Dong Du, Xuefeng Wang, Jing Dai, Quilan Ding, Wenman Wu, Yiyi Lu, Runhui Wu, Guoqing Liu, Wanru Yao, Yan Wang, Yunyun Wei, Weiqun Xu, Yu Du, Liyao Xu, Di Wang, Chan Liao, Hongwei Zhang, Ziqiang Yu, Hong Tian, Haibo Wang, Jie Yin, Tienan Zhu, Huacong Cai, Juan Xiao, Shujie Wang, Shufen Liu, Kaini Shen, Yun Chen, Yali Chang, Tan Sang, Jun Zhao, Yawei Zhou, Liya Zhai, Xiadong Qiu, Yulei He, Hui Li, Yi Xia, Min Zhou, Feng Gao, Shipin Feng, Xiaoli Luo, Dan Li, Zhongguang Cui, Chunzhu Zhao, Hong Xu, Lingjie Sun, Xue Shi, Xiaojing Zeng, Lu Qi, Shuyun Cao, Zeping Zhou, Fuhou Zhang, Lingmei Yin, Hongli Mu, Hui Bi, Zhengchao Li, Yaping Miu, Yaming Xi, Mingfeng Jia, Long Zhao, Xielan Zhao, Yaochun Li, Jie Peng, Chia-Yau Chang, Yen-Lin Liu, Ming-Ching Shen, Cheng-Wei Huang, Shih-Chung Wang, Hsuan-Yu Lin, Ching-Yeh Lin, Sheng-Chieh Chou, Ming-Kai Chuang, Szu-Chun Hsu, Jiaan-Der Wang, Ming-Yang Shih, Liang-Tsai Hsiao, Giun-Yi Hung, Hsiu-Ju Yen, Po-Shen Ko, Hung Chang, Shih-Hsaing Chen, Te-Fu Weng, Yu-Hua Chao, Sherig-Wei Zeng, Peter Kampmann, Eva Funding, Yesim Dargaud, Claude Negrier, Stéphanie Desag, Laurent Frenzel, Guillemette Fouquet, Cécile Bally, Robert Klamroth, Ana-Marija Orlovic, Christian Pfrepper, Michael Metze, Rima Chakaroun, Maria Weise, László Nemes, Agnes Ronatas, Cecil Ross, Seetharam Anandram, Vandana Bharadwaj, Sonali Salvi, Sunil Lohande, Alok Srivastava, Aby Abraham, Fouzia Aboobacker, Shailendra Verma, Gaurav Datta, Savita Rangarajan, Shweta Bansal, Shashikant Apte, Kannan Subramanian, Beatrice Nolan, Saad Ahmed, Niamh O’Connell, James O’Donnell, Kevin Ryan, Michelle Lavin, Gili Kenet, Omri Cohen, Mudi Misgav, Assaf Barg, Sarina Levy Mendelovich, Flora Peyvandi, Roberta Gualtierotti, Ezio Zanon, Luca Spiezia, Chiara Simion, Tadashi Matsushita, Shuichi Okamoto, Nobuaki Suzuki, Takeshi Kanematsu, Naruko Suzuki, Yuka Kawaguchi, Satoshi Higasa, Tazuko Tokugawa, Akihiro Sawada, Rie Shirayama, Masaru Kawamura, Hiroshi Asai, Koichi Oshida, Tetsuji Sato, Takuma Ito, Katsuyoshi Koh, Yoshitaka Mizushima, Takahiro Ishikawa, Hirohito Kubota, Ryota Kaneko, Tomoya Irikura, Mamoru Honda, Katsuaki Taira, Yuki Arakawa, Makiko Mori, Kohei Fukoka, Koichi Oshima, Yuichi Mitani, Yoshiaki Ogawa, Kiyoshi Ando, Rikio Suzuki, Ryujiro Hara, Yasuyuki Aoyama, Masako Toyosaki, Daisuke Ogiya, Shinichiro Machida, Hiroshi Kawada, Yukari Shirasugi, Makoto Onizuka, Ken Omachi, Kagehiro Amano, Tomoko Yamaguchi, Ei Kinai, Takeshi Hagiwara, Mihoko Yotsumoto, Ryoko Sekiya, Masato Bingo, Yushi Chikasawa, Akito Ichiki, Yoshiko Kamikubo, Ryui Miyashita, Takashi Muramatsu, Ho-Jin Shin, DoYoung Kim, Chur-Woo You, Ju Young Kim, Seung Min Hahn, Chuhl Joo Lyu, Jung Woo Han, Young Shil Park, Ja Hyang Cho, Azizan Shariq, Soo Min Lim, Lily Wong, Heng Chang Choo, Gilbert Wilfred, Mohd Tarmizi Ahmad Zakhi, Yin Man Lim, Khaiteri Raghunathan, Jameela Sathar, Syazarin Fidhora Nasution, Yee Yee Yap, Veena Selvaratnam, Daniel Malan, Zelda Erika Punt, Ali Bulent Antmen, Ilgen Sasmaz, Utku Aygunes, Kaan Kavakli, Nihal Karadas, Deniz Karapinar, Alphan Kupesiz, Mine Erkan, Kupesiz Funda Tayfun, Elif Guler, Bulent Zulfikar, Basak Koc, Vahap Okan, Sahin Handan Haydaroglu, Canan Albayrak, Ibrahim Kartal, Ebru Yilmaz, Musa Karakukcu, Ekrem Unal, Alper Ozcan, Fahri Sahin, Betul Tuzun, Guray Saydam, Ievgenii Averianov, Oksana Kovtunenko, Oleksandra Stasyshyn, Maksym Semerak, Orest Tushnytskyy, Kateryna Vilchevska, Iryna Bakhchyvandzhy, Nataliya Romanyuk, Stanislav Nikulin, Alina Kobets, Jayanthi Alamelu MRCPCH, Samah Babiker, Catherine Bagot, James Tyan Rodgers, Lisa Boggio, Mindy Simpson, Erin Cockrell, Candance DeBerry, Dana Obzut, John Fargo, Jeffrey Hord, Stephanie Savelli, Joseph Lasky, Jennifer Buitrago, Waseem Alhushki, Cynthia Gauger, Darren Klawinski, Eric Sandler, Scott Bradfield, Paul Pitel, Michael Joyce, Howard Katzenstein, Manisha Bansal, Allison Bechtel, Christine Knoll, Esteban Gomez, Shanna White, Sanjay Shah, Joanna Gendreau, Lori Wagner, Maa-Ohui Quarmyne, Larissa Bornikova, Colleen Cleary CNP, Pamela G. Hodges, Alexandra Mossali, Rachel Rosovsky, Victoria Turbini, Valerie Wood, Hanny Al-Samkari, Steven Pipe, Angela Weyand, Jordan Shavit, Amit Soni, Diane Nugent, Nina Hwang, Vanessa Salinas, Guy Young, Tom Hofstra, Jennifer Donkin, Jacquelyn Keegan, Zaheer Sibgha, Wendy Leung, Julie Jaffray, Safety and efficacy of a fitusiran antithrombin-based dose regimen in people with hemophilia A or B: the ATLAS-OLE study, Blood, 10.1182/blood.2024027008, 145, 25, (2966-2977), (2025).
- Massimo Franchini, Daniele Focosi, Pier Mannuccio Mannucci, Thrombotic Complications in Hemophilia: An Intricate Conundrum, Seminars in Thrombosis and Hemostasis, 10.1055/a-2603-0344, 52, 02, (164-173), (2025).
- Hideo Wada, Katsuya Shiraki, Takeshi Matsumoto, Hideto Shimpo, Yumi Sakano, Hiroko Nishii, Shigehisa Tamaki, Kei Suzuki, Isao Tawara, Yoshiki Yamashita, Motomu Shimaoka, Evaluating Factor VIII Concentrates Using Clot Waveform Analysis, Journal of Clinical Medicine, 10.3390/jcm13133857, 13, 13, (3857), (2024).
- Takeshi Matsumoto, Hideo Wada, Katsuya Shiraki, Kei Suzuki, Yoshiki Yamashita, Isao Tawara, Hideto Shimpo, Motomu Shimaoka, The Evaluation of Clot Waveform Analyses for Assessing Hypercoagulability in Patients Treated with Factor VIII Concentrate, Journal of Clinical Medicine, 10.3390/jcm12196320, 12, 19, (6320), (2023).
- Pier Mannuccio Mannucci, Pasquale Agosti, Maddalena Lettino, Guidance for the antithrombotic management of persons with haemophilia and cardiovascular disease, Haemophilia, 10.1111/hae.14874, 29, 6, (1390-1393), (2023).
- Armando Tripodi, Pier Mannuccio Mannucci, Flora Peyvandi, Hemophilia patients: are they naturally anticoagulated?, Internal and Emergency Medicine, 10.1007/s11739-023-03331-7, 18, 5, (1251-1254), (2023).
- Christina Schnohr, Ola Ekholm, Lone Hvitfeldt Poulsen, Lars Lehrmann, Terkel Andersen, Eva Funding, Karen Binger Holm, Jakob Bue Bjorner, Health and quality of life of patients with haemophilia: A national study of 124 Danish men, Haemophilia, 10.1111/hae.14751, 29, 2, (538-544), (2023).
- Amy D. Shapiro, Brandon M. Hardesty, Flora Peyvandi, Alfonso Iorio, Prevalence of selected bleeding and thrombotic events in persons with hemophilia versus the general population: A scoping review, Research and Practice in Thrombosis and Haemostasis, 10.1016/j.rpth.2022.100007, 7, 1, (100007), (2023).