A real world cost-minimization analysis comparing the use of different endoscopic staplers in video-assisted thoracic surgery lobectomy procedures
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: China’s cost-containment measures increasingly focus solely on the prices of consumable medical supplies without taking a broader perspective on differences in features and overall costs. This study compared two types of endoscopic staplers in video-assisted thoracoscopic surgery (VATS) lobectomy. Materials & methods: Electronic medical records for video-assisted thoracoscopic surgery from 2016 to 2017 were collected from a hospital in Anhui province. Two cohorts were retroactively defined based on stapler type. Total costs were compared using a cost-minimization analysis model. Probabilistic sensitivity analysis was performed. Results: In the base case, the group using more expensive staplers achieved overall cost savings of about $300 per procedure. Sensitivity analysis confirmed this result in 86.5% of cases. Conclusion: A price-only supply selection strategy may have unintended cost consequences.
Lobectomy is the standard treatment option for a variety of severe lung diseases, including resectable lung carcinomas. Thoracoscopy is a widely used, minimally invasive approach to lobectomy that is performed without the trauma of open surgical incisions. As of 2014, the proportion of video-assisted thoracoscopic surgery (VATS) for lobectomy reached 58–88% in some of the larger hospitals in Shanghai, China [1].
The development of endoscopic stapler technology was critical for enabling the advancement of minimally invasive surgery [2]. Staplers give surgeons greater control and provide safer procedures for patients [3]. The US FDA recently raised the quality standard of staplers for internal use and recommended reclassifying these medical devices from Class I to Class II [4]. Endoscopic staplers represent a substantial proportion of the total cost of VATS lobectomy procedures.
Both branded and generic staplers are available in China. Branded staplers are normally priced higher than their generic counterparts. As public hospitals in China are increasingly pressured to contain costs, suitable criteria for procurement decision-making warrant investigation.
Improving the efficiency of healthcare resource utilization is a key priority as China deals with the challenges of its rapid growth in healthcare spending in the last decade. Multiple policy initiatives have been implemented or piloted to decelerate healthcare expenditure growth [5,6]. Public hospitals, as the dominant healthcare delivery channel in China, are responsible for implementing most of these cost-containment measures [5,6].
One of the key cost control initiatives focuses on cutting consumable medical supply spending. Public hospitals are not allowed any markup on consumable supplies, effective as of late 2019 [7]. In addition, the performance of public hospitals is measured by the ratio of disposable medical supply expenditure to total revenue. The National Healthcare Security Administration is piloting several prospective payment systems, including global hospital budget, per capita capitation and diagnostic-related groups [8]. These initiatives simultaneously create a strong incentive for hospital management to avoid branded consumable medical supplies and switch to cheaper generic alternatives.
From the perspective of a value-based healthcare delivery system, economic evaluations of consumable supplies should cover the entire episode of care rather than just the acquisition cost of any individual consumable medical supply. We hypothesized that some high-cost consumable medical supply may generate sufficient savings within the treatment pathway to offset their higher initial acquisition costs. Comprehensive economic evaluations of medical supplies are still rare in China.
This study used a cost-minimization analysis (CMA) model to compare the episodic cost of branded and generic endoscopic staplers in VATS lobectomy. The cost parameters for the branded and generic endoscopic staplers were derived from real-world retrospective cost data from an academic medical center in China.
Materials & methods
Cost data
The electronic medical record (EMR) data used in this study were obtained from a tertiary (Level III) Class A general hospital (the top rating in China’s public hospital ranking system) in Anhui province. The hospital was equipped with over 5000 hospital beds and carried out over 100,000 surgeries in 2018.
The hospital primarily used staplers from two manufacturers for VATS lobectomy, which are referred to as Type A and Type B in this study. Type A staplers are priced relatively low and are supplied by a generic domestic medical device manufacturer. Type B staplers are branded with a higher price and are manufactured by a global medical device company. Technical characteristics of the two staplers are described in Table 1.
| Type | Description |
|---|---|
| A | An endoscopic cutter for cutting and/or stapling tissue. Indicated for tissue resection in open or endoscopic surgeries, such as resection of the lungs, stomach or intestines. Holds six rows of staples and allows one-handed operation. Has lock-out feature to prevent refiring of a used reload. After each firing, the surgeon activates a retraction button to return the firing member to its starting position, in order for the stapler to be fired again. |
| B | An endoscopic linear cutter for cutting and/or stapling tissue. Indicated for use in open and/or minimally invasive surgeries, including general, gynecologic, urologic, thoracic and pediatric surgeries. Holds six staggered rows of staples. The articulated shaft can rotate in both directions. Has lock-out feature to prevent refiring of a used reload. Allows one-handed operation. After each firing, the firing member is automatically returned to its starting position and manual operation is not needed for retraction. |
VATS lobectomy EMR data from 2016 to 2017 were used to calculate the inputs needed for the CMA model from the hospital EMR database (Figure 1). VATS patients were selected from all lung resection surgeries (n = 6283) during this period. For patients with multiple VATS lobectomy surgeries, only the first surgery was included in the analysis to ensure a meaningful comparison. Surgery durations were used to identify outliers based on Tukey’s 1.5 interquartile range rule [9]. Records with unusually high or low operation times were flagged and excluded from the calculation. A small number of the procedures using cartridge/stapler combinations from different manufacturers were also excluded. The remaining patients were then grouped into Type A or Type B cohorts retrospectively based on the endoscopic stapler used (Figure 1).

Baseline characteristics for Type A and Type B cohorts were evaluated to check for any significant differences. In the case of imbalances between groups, propensity score matching was conducted.
The EMR database provided comprehensive records for each VATS lobectomy operation including item name, cost, quantity used and cost category. The cost categories and subcategories related to healthcare services used in EMR were defined by the National Standard of Billable Healthcare Services [10]. Their definitions are presented in Supplementary Table 1. Itemized costs were converted to USD using the average exchange rate in 2018, which was 6.616 RMB to 1 USD [11].
Stapler and cartridge costs were calculated separately from other medical supplies because they were the stratifying variable defining the two patient cohorts. The unit costs of staplers and cartridges were treated as constants in the calculation, as their prices were fixed by a centralized procurement process in the study period. The model assumed one stapler per procedure, consistent with real clinical practice. Multiple cartridges may be used in any given surgery. Medical supplies other than staplers and cartridges were assigned to a new cost category called other medical supply (OMS) cost. All costs under each category were summed to obtain the total cost of each category using the OMS cost category instead of the original medical supply cost category. The total costs of each cost category were used as cost components in the CMA model input, which are summarized in Table 2. Two-sided Welch’s t-test was used to compare cost components other than stapler and cartridge unit price, as cost distributions were skewed and equal variances were not assumed [12–15].
| Cost category | Description | Ref. |
|---|---|---|
| Native cost categories | ||
| Consumable medical supplies | Costs for consumable medical supplies; replaced by the other medical supply cost category in the analysis | |
| Pharmacy | Costs of drugs during inpatient stay | |
| Cost categories of healthcare services (defined by the National Standard of Billable Healthcare Services) | [10] | |
| – Bed | Costs of inpatient stay | |
| – Nursing | Costs of nursing services | |
| – Laboratory | Costs of laboratory tests | |
| – Imaging | Costs of medical imaging | |
| – Anesthesia | Costs of anesthesia services | |
| – Surgery | Costs of surgery operation (surgeon fee) | |
| – Consultation | Costs of physician consultation | |
| – Nonsurgery treatment | Costs of inpatient nonsurgery treatments | |
| Miscellaneous | Costs outside previous categories | |
| Custom cost categories | ||
| – Stapler costs | Assumed to be the cost of one stapler | |
| – Cartridge costs | Calculated by multiplying cartridge number by its unit cost | |
| – Other medical supply | Costs for consumable medical supplies, excluding staplers and cartridges; replaces the original medical supply costs category in the analysis | |
Model
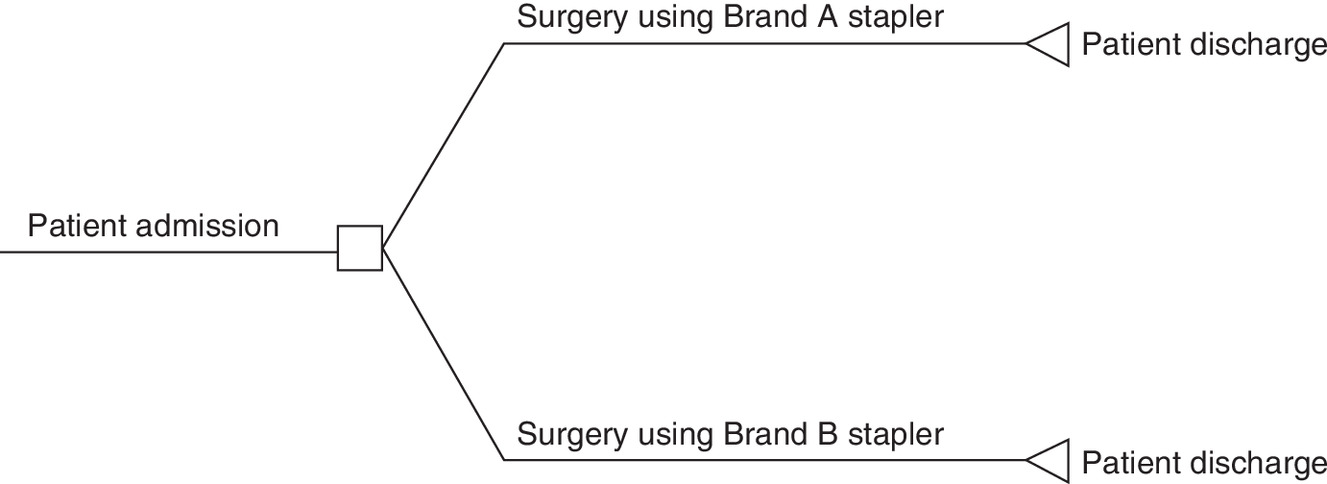
The CMA decision tree was constructed in Microsoft Excel (2016), as shown in Figure 2. Patients entered the model upon admission to the hospital for VATS lobectomy. They were stratified retrospectively into two different cohorts (Type A and Type B) based on the type of stapler/cartridges used in lobectomy. The average episodic cost of VATS lobectomy care was calculated as the sum of average inpatient category costs incurred along each treatment pathway. The episodic cost differential (ECD) between the two treatment pathways was estimated as the difference of average episodic costs between Type A and Type B cohorts.
The cost-minimization decision rule is formulated based on the value of ECD as follows:
Sensitivity analysis
A probabilistic sensitivity analysis with 10,000 simulations was performed on this model. Stapler price and cartridge price were held constant, as explained above. Cartridge count along with other cost categories were simulated as gamma distributions in which the distribution parameters were estimated based on real-world means and standard deviations. These distributions were assumed to be independently distributed with no underlying correlation structure.
Results
Patient baseline characteristics
Our analysis showed that Type A cohort (n = 64) and Type B cohort (n = 578) were similar in age distribution, gender distribution, types of health insurance, diagnosis (e.g., lung cancer and lung bullae), comorbidities (i.e., diabetes and hypertension) and area of resection, which are shown in Supplementary Table 2. Therefore, no matching was conducted.
Base case analysis
The average costs by category calculated from EMR for Type A and Type B cohorts are shown in Table 3. Except for stapler unit cost, OMS costs and imaging test costs, the Type B cohort had lower costs across all other categories. Even though the Type B cartridge unit costs were higher, fewer cartridges were used in Type B cohorts compared with Type A, resulting in lower spending on cartridges. The average inpatient episodic cost per VATS lobectomy was $7,485.41 and $7,169.05 for the Type A and Type B cohorts, respectively. The net saving associated with Type B stapler use was $316.36 per VATS lobectomy surgery episode.
| Cost component (costs in USD) | Type A cohort (n = 64) | Type B cohort (n = 578) | p-value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard deviation | Gamma distribution | Mean | Standard deviation | Gamma distribution | ||||
| α | β | α | β | ||||||
| Stapler unit price | 298.46 | – | – | – | 562.37 | – | – | – | – |
| Cartridge unit price | 286.12 | – | – | – | 354.93 | – | – | – | – |
| Cartridge count (n) | 8.25 | 4.45 | 216.54 | 0.04 | 6.64 | 2.74 | 3388.53 | <0.01 | 0.006 |
| Other medical supply cost | 549.73 | 1505.55 | 8.40 | 433.01 | 462.71 | 1181.62 | 88.48 | 34.60 | 0.588 |
| Imaging | 1066.73 | 562.5 | 226.57 | 31.15 | 1197.72 | 609.66 | 2226.97 | 3.56 | 0.101 |
| Pharmacy | 1014.39 | 603.43 | 178.03 | 37.70 | 748.95 | 601.98 | 893.12 | 5.55 | 0.001 |
| Surgery | 915.88 | 410.38 | 313.80 | 19.31 | 828.35 | 207.10 | 9230.72 | 0.59 | 0.005 |
| Nonsurgery treatment | 335.26 | 209.86 | 160.78 | 13.80 | 274.57 | 163.39 | 1629.29 | 1.11 | 0.006 |
| Anesthesia | 298.93 | 120.71 | 386.35 | 5.12 | 236.83 | 62.51 | 8283.47 | 0.19 | <0.001 |
| Laboratory | 254.38 | 145.98 | 191.31 | 8.80 | 185.37 | 139.02 | 1025.83 | 1.20 | <0.001 |
| Bed | 137.08 | 99.56 | 119.43 | 7.59 | 109.07 | 94.25 | 772.68 | 0.93 | 0.025 |
| Miscellaneous | 110.10 | 88.95 | 96.53 | 7.55 | 86.02 | 71.39 | 837.77 | 0.68 | 0.013 |
| Nursing | 93.14 | 52.4 | 199.02 | 3.10 | 76.36 | 38.48 | 2271.88 | 0.22 | 0.002 |
| Consultation | 50.82 | 28.07 | 206.53 | 1.63 | 44.03 | 22.50 | 2210.27 | 0.13 | 0.026 |
| Total cost | 7485.41 | – | – | – | 7169.05 | – | – | – | – |
Sensitivity analysis
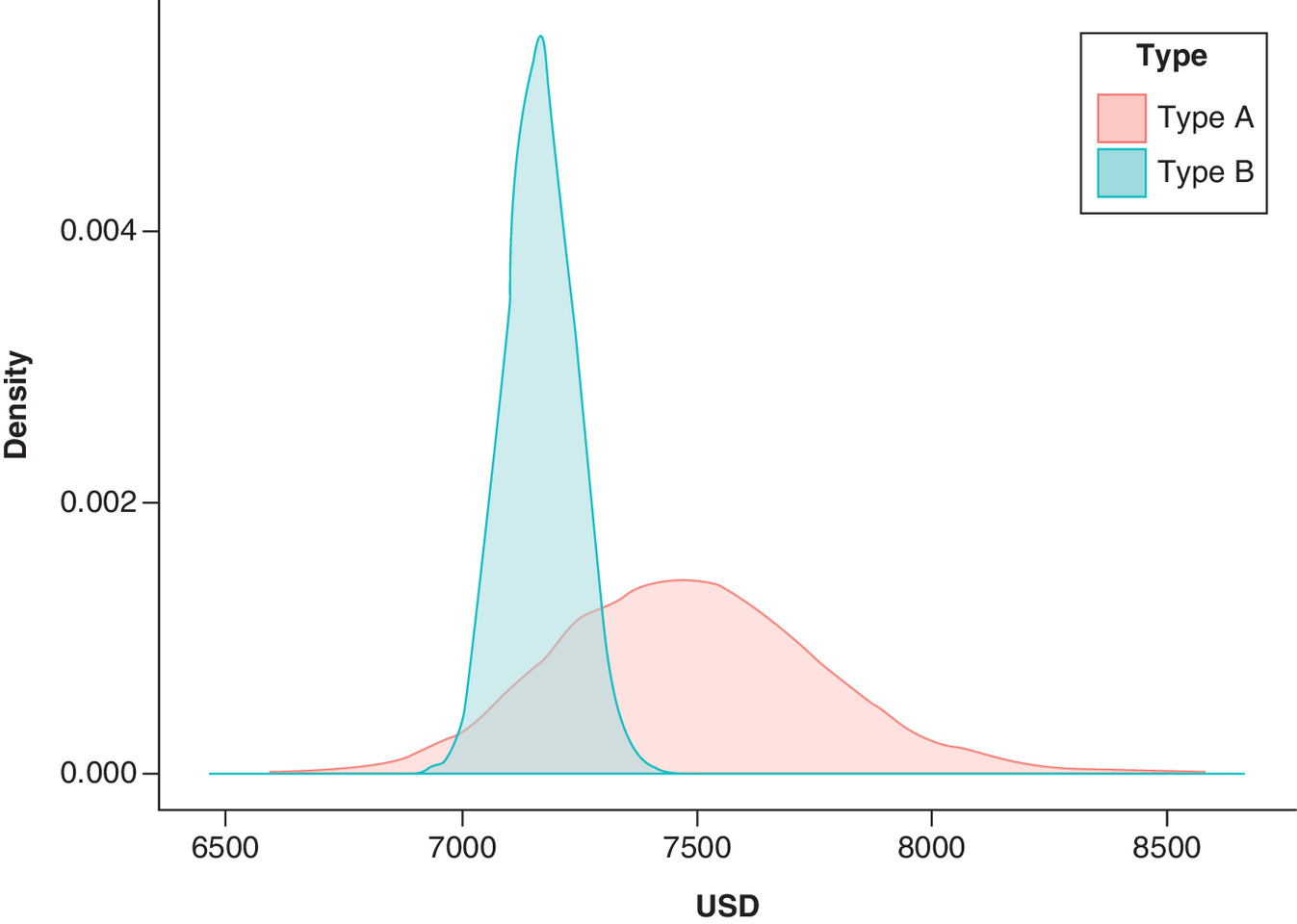
Distributions applied to all variable cost components are shown in Table 3. Ten thousand simulations were conducted. The probability distribution of total inpatient costs for an episode of VATS lobectomy using Type A and Type B staplers is shown in Figure 3.
The histogram of cost differentials from the simulation is shown in Figure 4. The vertical dashed line represents the decision boundary (ECD = 0). In 86.5% of cases, the ECD was negative, meaning that cases using Type B staplers were associated with a lower average episodic cost of VATS lobectomy.
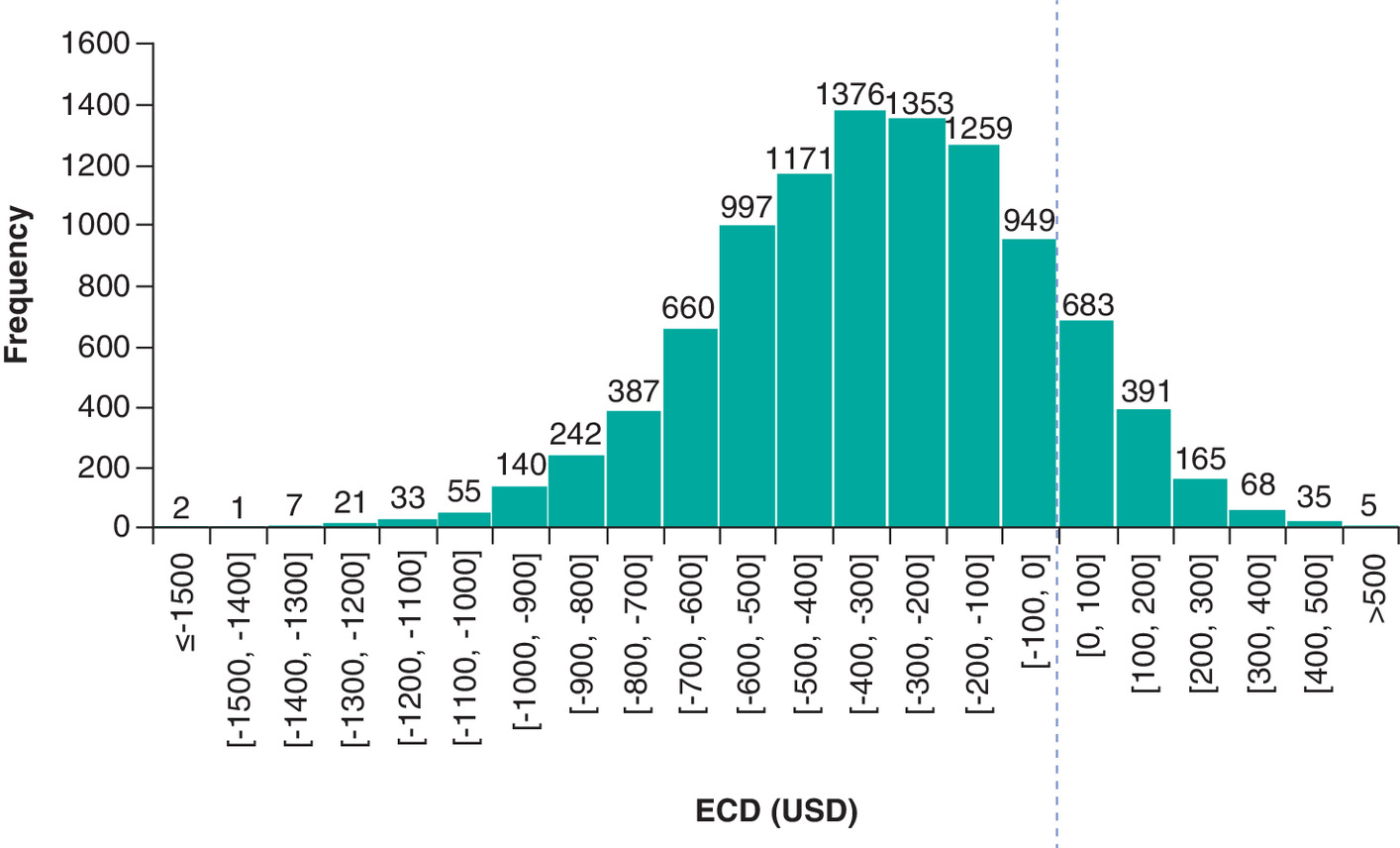
Figure 4. ECD distribution from 10,000 simulation runs.
ECD: Episodic cost differential.
Discussion
This analysis of real-world data demonstrated that low-cost medical supplies may be associated with an increase in other costs and a net increase in overall expenditure. This result is aligned with the findings of several previous studies that analyzed the financial consequences of utilizing new medical devices or devices with new features, assuming equivalent efficacy compared with conventional methods [16–19]. Although the new treatment methods incurred higher acquisition costs upfront, the overall expenditure decreased due to savings in other aspects of the treatment pathway [16–19].
The strength of this study is its combination of real-world data analysis with economic modeling, although the economic assessment of medical supplies is challenging [20]. The clinical outcomes of medical supplies, such as staplers, depend on multiple factors besides the intrinsic properties of the medical device. External factors, such as physician technique and preoperative and postoperative care can influence final clinical performance [20–23]. In this study, a large number of real-world VATS lobectomy cases were used to gain insights for an ‘average’ scenario. To limit the potential bias from presurgery conditions, we compared patient baseline characteristics between the two cohorts. The two sample groups were reasonably similar, with no statistically significant differences in all baseline characteristics except the proportion of hypertension patients. Extreme cases based on operation time were eliminated to reduce the impact of outliers.
Real-world data indicated that in cases using Type B staplers, which were more expensive, the cost per procedure was reduced by $300. An inspection of average categorical costs incurred in VATS lobectomy showed that the Type B cohort had lower expenditure in almost all other categories except for stapler unit price, OMS and imaging. The savings from the reduction in pharmacy costs and surgery were more than enough to offset the difference in stapler price. The Type B cohort also used fewer cartridges.
Our findings indicate that medical supply selection based on price alone may introduce biases in cost estimation for health systems that are attempting to reduce costs while maintaining quality standards. In the case of endoscopic operations, staplers are one of the most important assistive tools for surgeons. Video-assisted manual suturing is a challenging technique. Endoscopic staplers are user friendly, allowing easy access to the target site. The performance of endoscopic staplers is critical to minimizing wound-related complications and ensuring patient safety [2,3]. High-quality staplers can ensure the completeness of the staple line and stapler cut, avoid immediate staple line leakage or bleeding and avoid further surgical intervention such as prolonged air leakage [2,3].
In this study, Type B staplers automatically retract the firing member, as described in Table 1. However, when using Type A staplers, surgeons need to operate the retraction button between firings. This process may shift the position of the stapler and impact stability during firing, potentially resulting in malformed staples. In order to secure the staple site, more stapling attempts or manual suturing may be required. This would lead to additional cartridge use or longer operating time. Furthermore, malformed staples may increase the risk of postoperative infections and necessitate the use of antibiotics.
These technical differences may contribute to the reductions in pharmacy and surgery costs identified in our study, as well as cartridge use. This suggests that a broader perspective is needed in procurement decision making. The total episodic cost is a more comprehensive indicator of value compared with stapler or cartridge price alone.
Public hospital management teams in China face mounting pressure from escalating healthcare costs. Basing procurement decisions on acquisition price is one of the most direct methods of controlling costs. However, this study shows that focusing on acquisition price alone is not an ideal solution.
Previous experience with cost-containment policies in China have also demonstrated unintended consequences similar to our findings. China’s policy prohibited public hospitals from charging any markup on drugs, as drug sales previously accounted for almost half of hospital revenue [24]. However, in the long term, this policy had difficulty containing the growth of overall expenditure due to increase in other costs [25–28].
Regarding hospital procurement policy, in order to contain costs without sacrificing the quality of care, it is important to evaluate the costs from the wider perspective of the health system. A comprehensive economic evaluation of the whole episode of care would be a more suitable decision criterion.
Limitations
This study is subject to several limitations common to real-world data analysis and health economics modeling. Several assumptions were necessary to make the CMA feasible without significant deviation from real-world clinical practice: the analysis assumed patients in both cohorts achieved the same clinical outcome at discharge; a single stapler was used per procedure; and surgeons’ skills and experiences were similar between the two cohorts. It should be noted that the assumption of one stapler used per procedure is slightly biased in favor of the generic stapler (Type A) cohort. The real-world data collected in this study showed that among patients who had stapler count records available, 1.37 Type A staplers were used per procedure, while for Type B staplers, 1.13 were used per procedure.
Further, only access to administrative claim records was provided for this analysis. We were unable to access patient-level clinical information to investigate the clinical performance parameters.
In addition, the EMR data came from a single research hospital in Anhui province. The sample size of Type A cases is relatively small, leading to higher uncertainty in parameter estimation. This resulted in a large variation in costs associated with Type A stapler use in probabilistic sensitivity analysis. Finally, this analysis only covered the two types of staplers that are most commonly used in this hospital. The conclusions of this analysis may have limited representativeness for other hospitals in China, or other types of staplers.
Conclusion
The cost-minimization study demonstrated that the cohort treated with Type B staplers achieved lower average total expenditure per episode of VATS lobectomy. Comprehensive economic evaluation is more suitable in designing medical supply management strategies than focusing solely on individual supply prices.
•
Price negotiation and group procurement have been increasingly used to control consumable medical supply expenditure in China; thereby, controlling overall healthcare cost growth.
•
However, managing consumable medical supplies solely based on price may not be an adequate solution due to differences among features across products in the same category.
•
Electronic medical records of video-assisted thoracoscopic surgery cases with cost data from 2016 to 2017 from one of the largest research hospitals in Anhui province were retrospectively analyzed.
•
A cost-minimization analysis model showed that the patient group using a more expensive type of stapler achieved lower overall costs by about $300 per procedure.
•
Sensitivity analysis further demonstrated that in 86.5% of cases, the cohort treated with higher-cost branded staplers achieved lower total treatment costs.
•
This study demonstrated that the selection of medical supplies can affect overall healthcare costs in complex ways, beyond simple changes in acquisition cost of staplers alone.
•
A price-only supply selection strategy may be associated with unexpected increases in total healthcare expenditures.
•
Comprehensive value assessments based on real-world data can help hospitals evaluate the total impact of consumable medical supply management strategies.
Author contributions
W Gu, T Wang, G Tong and W Wang contributed to data acquisition and interpretation, and research conception. S Wu and Y Han contributed to model design and validation, and manuscript preparation. All authors read and approved the final manuscript.
Acknowledgments
The authors would like to thank L Shi for revising this manuscript and providing recommendations.
Financial & competing interests disclosure
The study was funded by Johnson & Johnson Medical Company, Shanghai, PR China. The funder provided information on the technical aspects of staplers. S Wu is an employee of VMLY&Rx, which received funding for this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate Institutional Review Board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (suppl_file.docx)
- Download
- 18.34 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Zhang X. Current status analysis of development of thoracic surgery in China. Zhongguo Fei Ai Za Zhi. 17(7), 518–522 (2014).
2.
Kuthe A, Haemmerle A, Ludwig K et al. Multicenter prospective evaluation of a new articulating 5-mm endoscopic linear stapler. Surg. Endosc. 30(5), 1883–1893 (2016).
3.
Akil A, Semik M, Freermann S et al. Use of a powered stapling system for minimally invasive lung volume reduction surgery: results of a prospective double-blind single-center randomized trial. Thorac. Cardiovasc. Surg. 67(3), 216–221 (2019).
4.
U.S. Food & Drug Administration. Surgical stapler and staples (2019). www.fda.gov/medical-devices/general-hospital-devices-and-supplies/surgical-staplers-and-staples
5.
Li L, Fu H. China’s health care system reform: progress and prospects. Int. J. Health Plann. Manage. 32(3), 240–253 (2017).
6.
Liu GG, Vortherms SA, Hong X. China’s health reform update. Annu. Rev. Public Health 38, 431–448 (2017).
• Gives a comprehensive review of policies implemented during China’s health reform. The three major areas of reform were health insurance, drug pricing and public hospitals. Several key tasks of public hospital reform aim to promote rational utilization of healthcare resources and control costs.
7.
Beijing: Central Government of the People's Republic of China. State Council notice regarding reform plan for regulation of high-cost medical consumable supplies (2019). www.gov.cn/zhengce/content/2019-07/31/content_5417518.htm
8.
Beijing: National Healthcare Security Administration. Regarding application for national pilot program of diagnostic related groups (2018). www.nhsa.gov.cn/art/2018/12/10/art_37_851.html
9.
Tukey JW. Chapter 2 Schematic Summaries, section 2D Fences, and outside values. In: Exploratory Data Analysis. Addison-Wesley Pub. Co, MA, USA (1970).
10.
Beijing: National Development and Reform Commission. Regarding standardization of healthcare service pricing and related issues (2012). www.ndrc.gov.cn/fzgggz/jggl/zcfg/201205/t20120510_478629.html
11.
Paris: Organization for Economic Cooperation and Development. Exchange rates (2019). https://data.oecd.org/conversion/exchange-rates.htm
12.
Welch, B. L. The generalization of Student’s problem when several different population variances are involved. Biometrika 34 28–35, (1947).
13.
Best DJ, Rayner JCW. Welch's Approximate Solution for the Behrens–Fisher Problem. Technometrics 29(2), 205–210 (1987).
14.
Ruxton GD. The unequal variance t-test is an underused alternative to Student’s t-test and the Mann–Whitney U test. Behav. Ecol. 17(4), 688–690 (2006).
15.
Fagerland MW, Sandvik L. Performance of five two-sample location tests for skewed distributions with unequal variances. Contemp. Clin. Trials 30(5), 490–496 (2009).
16.
Larmené-Beld KHM, Spronk JT-, Luttjeboer J, Taxis K, Postma MJ. A cost minimization analysis of ready-to-administer prefilled sterilized syringes in a Dutch hospital. Clin. Ther. 41(6), 1139–1150 (2019).
• This cost-minimization analysis compared the total costs of conventional syringe preparation and of using prefilled syringes. Despite additional equipment costs, the use of prefilled syringes yielded cost savings due to reduced risk of errors and contamination.
17.
Resnic FS, Arora N, Matheny M, Reynolds MR. A cost-minimization analysis of the angio-seal vascular closure device following percutaneous coronary intervention. Am. J. Cardiol. 99(6), 766–770 (2007).
18.
Hong JC, Yang GK, Delarmente BA et al. Cost-minimization study of the percutaneous approach to endovascular aortic aneurysm repair. J. Vasc. Surg. 71(2), 444–449 (2020).
• This cost-minimization study used a decision tree to compare payer perspective costs of percutaneous versus surgical access for endovascular aortic aneurysm repair. Although the percutaneous uses costly vascular closure devices, it was a cost-saving strategy compared with the surgical approach.
19.
Akazawa M, Konomura K, Shiroiwa T. Cost-minimization analysis of deep-brain stimulation using national database of Japanese health insurance claims. Neuromodulation 21(6), 548–552 (2018).
• This cost-minimization study compared rechargeable deep-brain stimulators with conventional devices, which require replacement surgery every 2–5 years. Although the rechargeable devices were more expensive, they incurred lower costs in the long run.
20.
Tarricone R, Torbica A, Drummond M. Challenges in the assessment of medical devices: the MedtecHTA Project. Health Econ. 26(Suppl. 1), 5–12 (2017).
21.
Drummond M, Griffin A, Tarricone R. Economic evaluation for devices and drugs–same or different? Value Health 12(4), 402–404 (2009).
22.
Ergina PL, Cook JA, Blazeby JM et al. Challenges in evaluating surgical innovation. Lancet 374(9695), 1097–1104 (2009).
23.
Boriani G, Biffi M, Martignani C et al. Expenditure and value for money: the challenge of implantable cardioverter defibrillators. QJM 102(5), 349–356 (2009).
24.
Beijing: Chinese Ministry of Health. 2010 Chinese health statistical digest (2011). www.moh.gov.cn/publicfiles//business/htmlfiles/zwgkzt/ptjty/digest2010/index.htm1
25.
He Y, Dou G, Huang Q et al. Does the leading pharmaceutical reform in China really solve the issue of overly expensive healthcare services? Evidence from an empirical study. PLoS ONE 13(1), e0190320 (2018).
26.
Yang C, Shen Q, Cai W et al. Impact of the zero-markup drug policy on hospitalisation expenditure in western rural China: an interrupted time series analysis. Trop. Med. Int. Health 22(2), 180–186 (2017).
27.
Yi H, Miller G, Zhang L, Li S, Rozelle S. Intended and unintended consequences of China's zero markup drug policy. Health Aff. (Millwood) 34(8), 1391–1398 (2015).
•• This article found that China’s zero markup drug policy reduced drug revenue in township health centers, but doubled inpatient care, which seemed to be driven by supply.
28.
Fu H, Li L, Yip W. Intended and unintended impacts of price changes for drugs and medical services: evidence from China. Soc. Sci. Med. 211, 114–122 (2018).
•• This article found that China’s zero markup drug policy led to a reduction in drug expenditures, but also a rise in expenditures for medical services, ultimately resulting in no measurable change in total health expenditures.
Information & Authors
Information
Published In
Pages: 1079 - 1088
PubMed: 34523357
Copyright
© 2021 Future Medicine Ltd.
History
Received: 21 December 2020
Accepted: 25 July 2021
Published online: 15 September 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A real world cost-minimization analysis comparing the use of different endoscopic staplers in video-assisted thoracic surgery lobectomy procedures. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0287
Export citation
Select the citation format you wish to export for this article or chapter.