The lateral and medial approach in total arthroplasty for valgus knee: a meta-analysis of current literature
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the lateral and medial approaches of total knee arthroplasty (TKA) in the valgus knee. Materials & methods: An electronic search from the PubMed, Embase, Web of Science and Cochrane library was performed according to ‘TKA’, ‘valgus’, ‘knee’ and ‘approach’. Subsequently, manual search was conducted from the reference lists in the identified studies. Results: Four randomized controlled trials and five cohorts were included. Better knee society score and function was noticed in patients after lateral approach. Similar postoperative valgus deformity, operative time, blood loss, Western Ontario and McMaster Universities Osteoarthritis Index, range of motion, pain and total complications in both groups. Conclusion: Compared with the medial approach for TKA in valgus knee, current data shows superior results after TKA by the lateral approach.
In the past few decades, practitioners have accepted the total knee arthroplasty (TKA) as an effective procedure to manage advanced knee arthritis. Among patients who need primary TKA, approximately 10–15% of patients show valgus deformity [1], which presents a unique challenge to the operating surgeon [2]. For joint surgeons, especially the junior doctors, the special pathological deformity in valgus knee needs more skills to gain the perfect component position and to restore soft-tissue balance. Initially, the conventional medial parapatellar capsulotomy was used to treat the valgus knee. However, there are controversies regarding this approach in the published literature. Through the standard medial approach, one study found that the anatomical axis was accurately restored in only 22–30% of valgus knees [3]. Additional studies also report poor results for TKA in the valgus knee using the medial approach [4–6]. In contrast, the minimally invasive medial approach can achieve similar range of motion (ROM) and knee society scores [7]. With enough soft tissue release, the medial approach exhibited an overall 15-year rate of 90.52% for implant survival [8].
To gain a good result, the flexion contracture deformity of the lateral side in severe valgus knee should be explored and released to obtain a balanced knee. Keblish et al. introduced the lateral approach and reported excellent results in valgus knees [9]. Modified methods of the lateral approach, such as Z-plasty of the articular capsule [10] and the pie-crusting technique [11], show good outcomes. Niki et al. reported that the lateral approach, when compared with the medial approach, showed comparable or superior postoperative knee scores, radiographic features and complication rates [12]. Another study reported improved patellar tilt control following total arthroplasty in the valgus osteoarthritic knee, with 3.1 degrees using the lateral approach compared with 18 degrees using the medial approach [13].
Although previous studies have reported promising results, small size of sample and different tests made it difficult to compare their results. Superiority of the medial or lateral approach remains controversial. The aim of this meta-analysis was to compare and analyze the clinical and radiological outcomes of the two approaches.
Methods
No specific approval was required from our hospital for this study because it was conducted based on data from published literatures. This paper was prepared in the guidelines of the prioritized reported items for systematic review and meta-analysis.
Study search & inclusion criteria
An extensive electronic search of the literature until 1 May 2019 was performed for the following database: PubMed, Embase, Web of Science and Cochrane library. To identify eligible studies, we used the following search terms: ‘valgus’ AND ‘knee’ in title AND ‘approach’ through the text. A further search of the references of the initially identified studies for other relevant articles missed by our search was also completed. No restrictions were made with regard to language. Eligible studies were selected by reviewing the abstract or title. If the abstract or title was inadequate, we reviewed the entire article to reach a final eligibility decision.
Studies comparing the effects of surgical approach were identified including randomized controlled trials (RCT), prospective or retrospective studies. Studies were excluded according to the following criteria: no comparison of the lateral and medial approach, studies with low methodological quality, unavailable data from full text.
Methodological assessment
All eligible studies were independently evaluated by two reviewers (Zhijun Li and Guijun Xu). According to the Cochrane handbook for systematic review of intervention, quality evaluation of the included RCTs was conducted. For the compared cohort studies, methodological quality was assessed using the methodological index for nonrandomized studiesform. Consensus was reached by discussion for any disagreements between the two researchers.
Data extraction
Data extraction was independently performed by two researchers (Zhijun Li and Guijun Xu) including the following information: authors, country, study design, publication year, age and gender, size of sample, BMI, diagnosis, extent of knee valgus, description of approach and time of follow-up. The following clinical outcomes in the analysis included: knee function, pain, ROM, operation time and blood loss. The radiological information included the degree of the valgus knee angle, fixed deformity and deformity of patella. Complications reported in the eligible studies were also included.
Data analysis & statistical methods
The meta-analyses were performed using RevMan 5.1 (The Cochrane Collaboration, Oxford, UK). The effects of the extracted clinical characteristics and radiological features were calculated as mean difference (MD) or odds ratio with a 95% CI for continuous or dichotomous variables. The data initially presented as a median and range were converted into mean and standard deviation according to the formulation in a previous study [14]. The heterogeneity for each outcome was evaluated using the standard χ2 test. I2 < 50% and p > 0.05 was defined as no significant heterogeneity and the fixed-effect model was adopted. Otherwise, the random-effect model was selected if I2 > 50% and p < 0.05.
Results
Search results
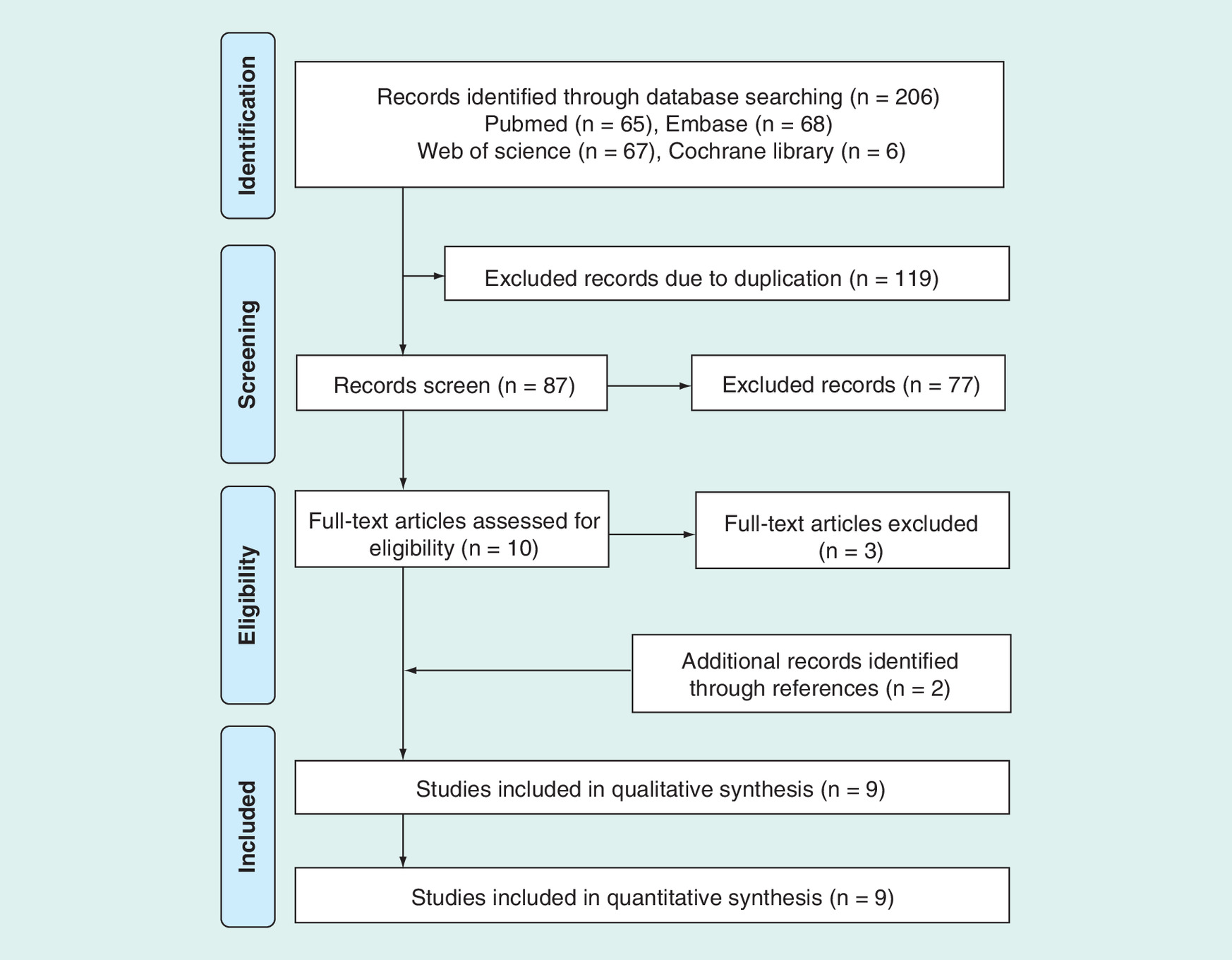
Figure 1 illustrates the search process. The electronic search initially identified 206 items, of which 119 studies were excluded because they were duplicate titles. After scanning the titles and abstracts, 77 records were excluded according to predefined criteria. Three studies were excluded after review of the full-text article. Another two studies were abstracted from the bibliographies of identified papers. In total, four RCTs [13,15–17] and five cohort studies [12,18–21] reporting the results of the lateral and medial approaches were included for further analyses.
Study characteristics
Table 1 summarizes the detailed demographic characteristics of the included studies. The identified studies were conducted in eight countries and published from 2011 to 2018. The sample sizes of the studies ranged from 21 cases in the study by Tonelli et al. [13] to 532 cases by Langen et al. [20]. In the study by Gunst et al. [19], an initial 315 cases in lateral group and 109 cases in the medial group was narrowed down to 238 and 89 patients in the two groups at the final follow-up, respectively. The sample size of all other studies was less than 50 cases. The diagnosis of knee disease included both osteoarthritis and rheumatoid arthritis in three studies, only osteoarthritis in three studies, only rheumatoid arthritis in one study and no clear description of disease in the other two studies. In the lateral approach group, the tibial tubercle osteotomy (TTO) was also performed in three studies [15,19,20]. The extent of valgus deformity of included patients is shown in Table 1. In the study by Langen et al., Ranawat grade II and III (>10 degrees) and neutral leg alignment were allocated in the lateral and medial group, respectively [20]. In Guo et al., the degree of valgus deformity in the medial group was 15–30 degrees while >30 degrees in the lateral group [21].
| Study (years) | Country | Design | Group | Size (M/F) | Age (year) | BMI (kg/m2) | Diagnosis | Valgus deformity (degree) | Surgical technique | Follow-up | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Nikolopoulos et al. (2011 [1995–2002]) | Greece | RCT | lateral | 22 (9/13) | 76.5 (59–81) | NA | OA: 16; RA: 6 | Ranawat grade II and III (15–36) | lateral parapatellar capsulotomy + TTO | All >7 years | [15] |
| medial | 22 (7/15) | 73 (57–80) | NA | OA: 19; RA: 3 | medial parapatellar approach | 76% > 7 years | |||||
| Niki et al. (2011 [2006–2009]) | Japan | Prospective | lateral | 26 (5/21) | 68.9 (39–84) | 23.9 | OA: 16; RA: 10 | Krackow type I and II | lateral parapatellar capsulotomy | 3 months | [12] |
| medial | 26 (5/21) | 67.2 (48–81) | 24.0 | OA: 16; RA: 10 | medial parapatellar approach | 3 months | |||||
| Sekiya et al. (2014 [NA]) | Japan | RCT | lateral | 24 (0/24) | 63 ± 6.6 | NA | RA: 24 | 6–24 | lateral parapatellar capsulotomy | 43.3 ± 14.2 months | [16] |
| medial | 24 (0/24) | 66 ± 6.7 | NA | RA: 24 | medial parapatellar approach | 43.2 ± 8.4 months | |||||
| Kornilov et al. (2015 [2008–2012]) | Russia | RCT | lateral | 25 (NA) | 62 ± 10 | 29 ± 2.7 | OA:25 | Krackow type II and III | lateral parapatellar capsulotomy | 23 ± 5 months | [17] |
| medial | 17 (NA) | 63.5 ± 12 | 28 ± 4.1 | OA:17 | medial parapatellar approach | 23 ± 5 months | |||||
| Rawal et al. (2015 [2004–2011]) | UK | Retrospective | lateral | 32 (NA) | 73.7 | 31.7 | NA | 18.5 (11–34) | lateral parapatellar capsulotomy | NA | [18] |
| medial | 17 (NA) | 70.1 | 29.9 | NA | medial parapatellar approach | NA | |||||
| Gunst et al. (2016 [1993–2011]) | USA | Prospective | lateral | 315 (60/255) | 70.9 ± 9.4 | 27.6 ± 4.3 | OA: 315 | 3–10 | lateral parapatellar capsulotomy + TTO (20.8%) | 2.8 ± 3.4 years | [19] |
| medial | 109 (24/85) | 68.1 ± 11.2 | 26.4 ± 5.2 | OA: 109 | medial parapatellar approach | 5.1 ± 4.2 years | |||||
| Langen et al. (2016 [2006–2013]) | Switzerland | Retrospective | lateral | 58 (13/45) | 71.0 ± 7.5 | 28.0 ± 5.0 | NA | Ranawat grade II and III (>10) | lateral parapatellar capsulotomy + TTO | 12 months | [20] |
| medial | 474 (205/196) | 68.3 ± 9.5 | 29.6 ± 5.4 | NA | Neutral leg alignment | medial parapatellar approach | 12 months | ||||
| Tonelli Filho et al. (2016 [NA]) | Brazil | RCT | lateral | 10 (1/9) | 62.9 ± 9.1 | 29 ± 3.9 | OA: 7, RA: 3 | Krackow type I and II | lateral parapatellar capsulotomy | 12 months | [13] |
| medial | 11 (1/10) | 62.6 ± 10.6 | 30.1 ± 3.9 | OA: 6, RA: 5 | medial parapatellar approach | 12 months | |||||
| Guo et al. (2018 [2011–2014]) | China | Retrospective | lateral | 13 (1/12) | 68 | NA | OA: 13 | >30 in 13 cases | lateral parapatellar capsulotomy | 6–12 months | [21] |
| medial | 18 (1/17) | 65 | NA | OA: 18 | <15 in 10 cases; 15–30 in 8 cases | medial parapatellar approach | 6–12 months |
BMI: Body mass index; M/F: Male/female; NA: Not available; OA: Osteoarthritis; RA: Rheumatoid arthritis; RCT: Randomized controlled trial; TTO: Tibial tubercle osteotomy.
Methodological assessment
A detailed analysis of the methodological quality of the RCTs is illustrated in the Figure 2. The study by Sekiya et al. did not report the generation of random sequence, allocation concealment, nor blinding of the participants or outcome assessment [16]. No description of random sequence generation was revealed in study by Kornilov et al. [17]. For the compared cohorts, the total methodological index for nonrandomized studie scores of compared cohorts ranged from 16 to 23 (Table 2). The main weaknesses of the retrospective studies were a lack of prospective data collection, no prospective calculation of sample size and a biased assessment of the study end points.

Figure 2. The risk of bias summary for randomized control trials.
There is low risk for circle with green ‘+’, high risk for circle with red ‘-‘ and unclear risk for circle with yellow ‘?’.
Outcomes of meta-analysis
The surgery-related outcomes mainly included the operative time and blood loss. Kornilov et al. reported longer operative time for patients undergoing the medial approach [17]. Longer operative time in the other studies ranged from 1.2 to 18.8 additional minutes in the lateral group. The pooled result from six studies showed similar operative time in both groups (MD = 2.49, 95% CI: -0.17 to 5.16, p = 0.07; I2 = 44%, p = 0.11; Figure 3). Two studies reported the volume of blood loss while one study reported the change of hemoglobin. The blood loss from the two studies was comparable in two groups (MD = 4.72, 95% CI: -2.34 to 11.79, p = 0.19; I2 = 0, p = 0.51).
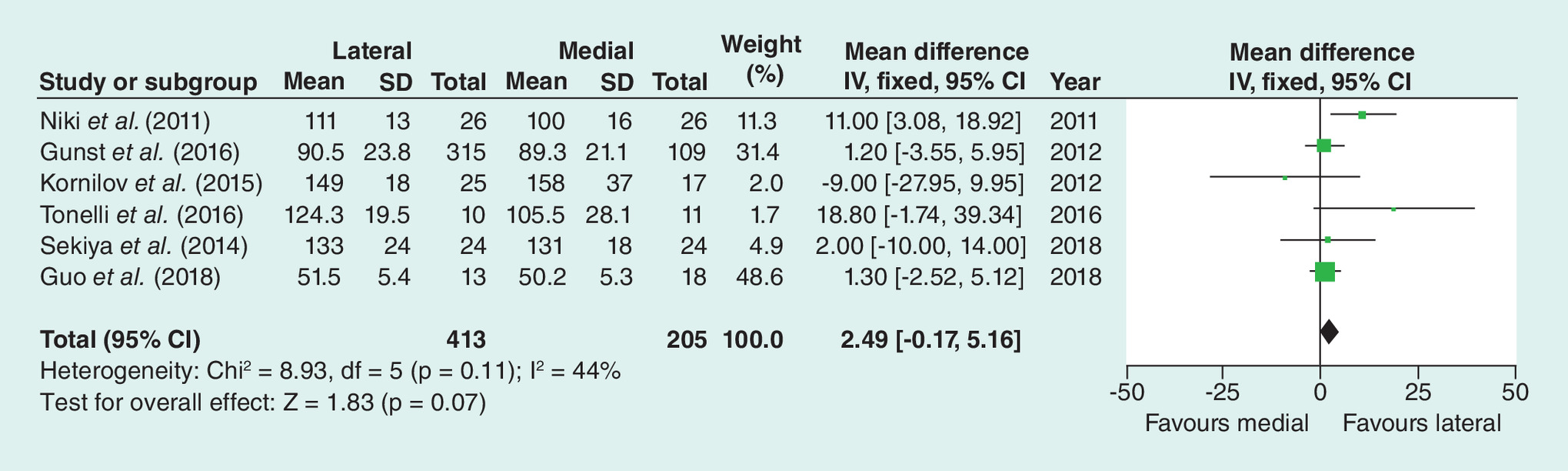
Figure 3. The pooled result of operative time between lateral and medial groups.
SD: Standard deviation.
For evaluation of the post-operative knee, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), International Knee Society System Score (IKSS), Hospital for Special Surgery (HSS) and Knee Society Score (KSS) were reported in different studies. Of these, KSS was the most adopted tool. The pooled data from six studies showed better result in patients with the lateral approach (MD = 2.49, 95% CI: 0.60–4.37, p = 0.01; I2 = 66%; p = 0.01; Figure 4). Significant heterogeneity was noticed and further analysis was performed by excluding the studies by Langen et al. and Guo et al. due to different valgus deformity in two groups. Excluding these two studies from analysis, the heterogeneity significantly decreased and a better KSS was confirmed in patients undergoing the lateral approach (MD = 2.14, 95% CI: 0.42–3.87; p = 0.01; I2 = 0; p = 0.89). Patients in the lateral group also displayed better result in the specific KSS-function (MD = 1.24, 95% CI: 0.57–1.90, p < 0.001; I2 = 0; p = 0.95). Comparable performance between two groups was found in the WOMAC (data from two studies; MD = -1.86, 95% CI: -5.29 to 1.56, p = 0.29; I2 = 92%; p < 0.001), ROM (data from four studies; MD = 2.32, 95% CI: -01.95 to 6.60, p = 0.29; I2 = 83%; p = 0.95) and pain (data from two studies; MD = 0.80, 95% CI: -2.12 to 3.73, p = 0.59; I2 = 0; p = 0.46).
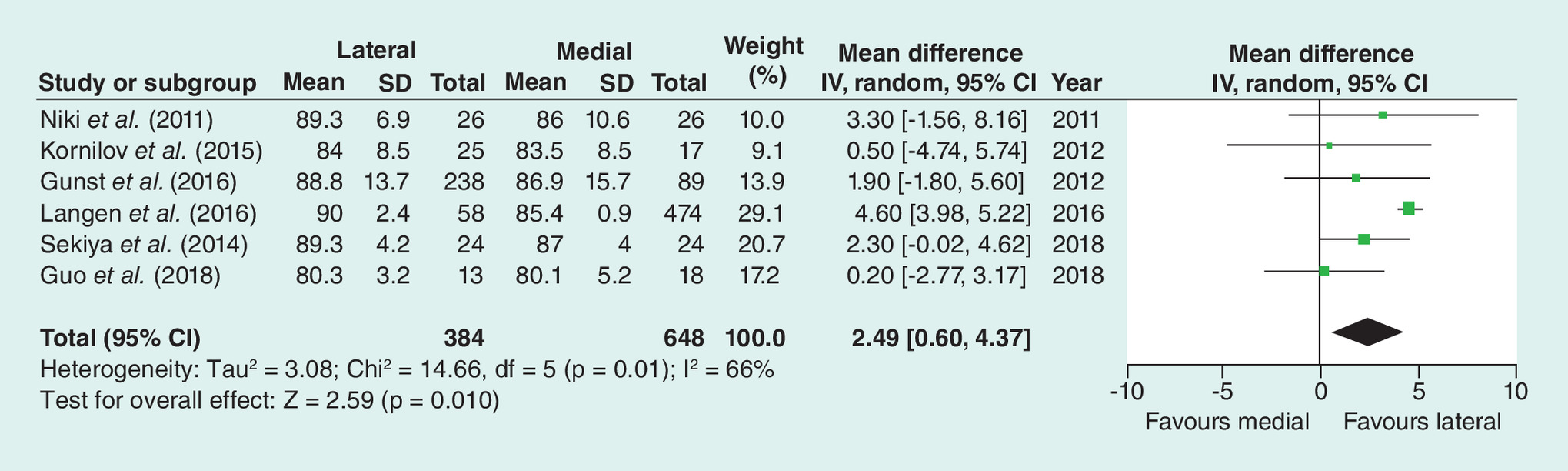
Figure 4. The pooled result of knee society score between lateral and medial groups.
SD: Standard deviation.
The postoperative valgus deformity was reported in eight studies. Four studies evaluated the valgus by the femoral and tibial anatomical axis (FTA) while mechanical axis (FTM) was used in the other four studies. In all patients and two subgroups, the pooled result showed no significant difference in postoperative valgus deformity between the lateral and medial approach group (MD = -0.10, 95% CI: -0.58 to 0.38, p = 0.68; I2 = 53%, p = 0.04; Figure 5).
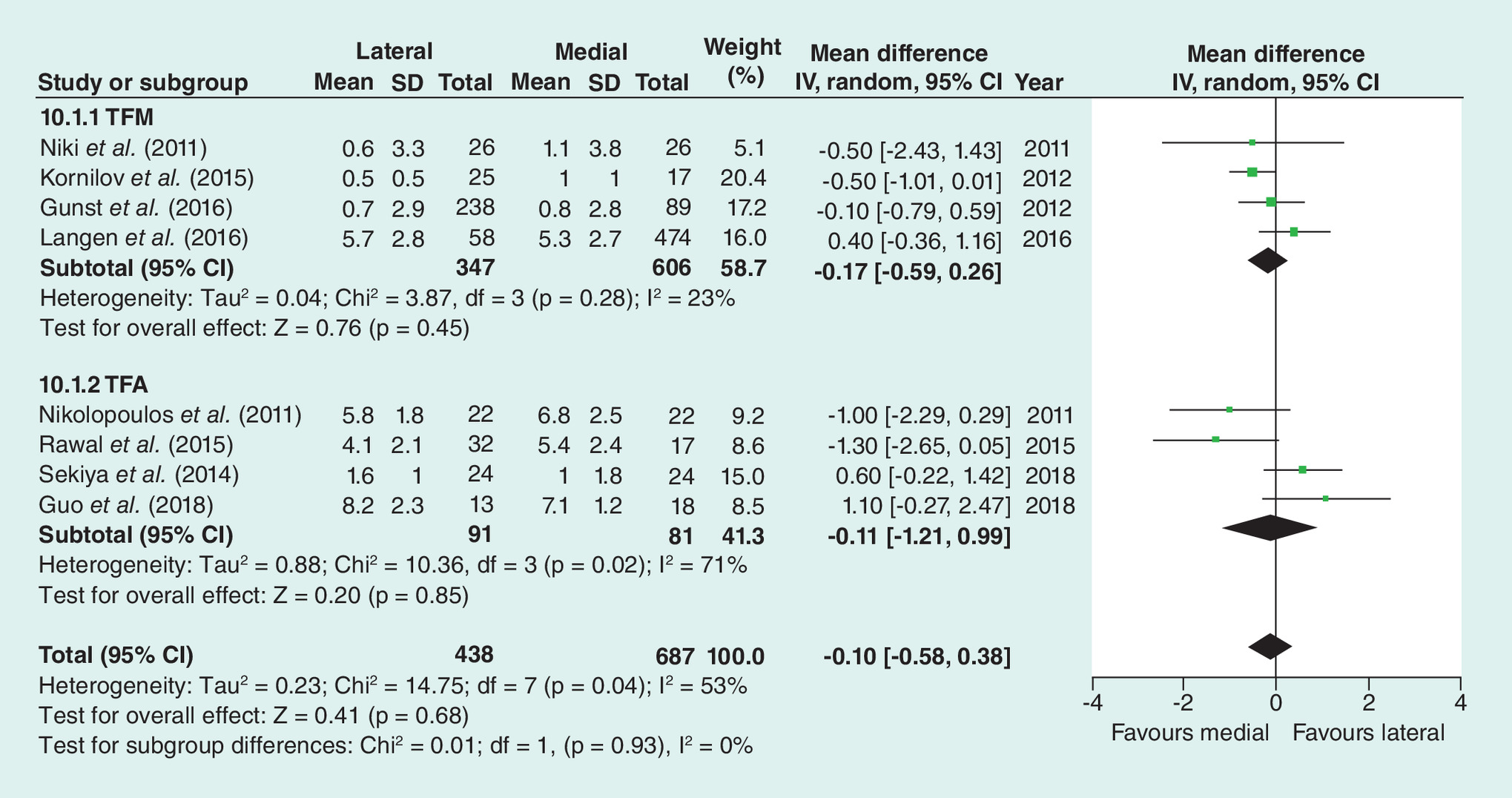
Figure 5. The pooled result of valgus deformity after operation between lateral and medial groups.
SD: Standard deviation; TFA: Tibial and femoral anatomical; TFM: Tibial and femoral mechanical.
The complications reported in six studies included the migration of tibial tuberosity, venous thrombosis, infection, hematoma, necrosis, nerve palsy and fracture of the tibial tuberosity. Based on the total number of complications from five studies, the pooled data found no significant difference between the lateral and medial groups (odds ratio = 0.86, 95% CI: 0.47–1.56, p = 0.62; I2 = 42, p = 0.14; Figure 6).
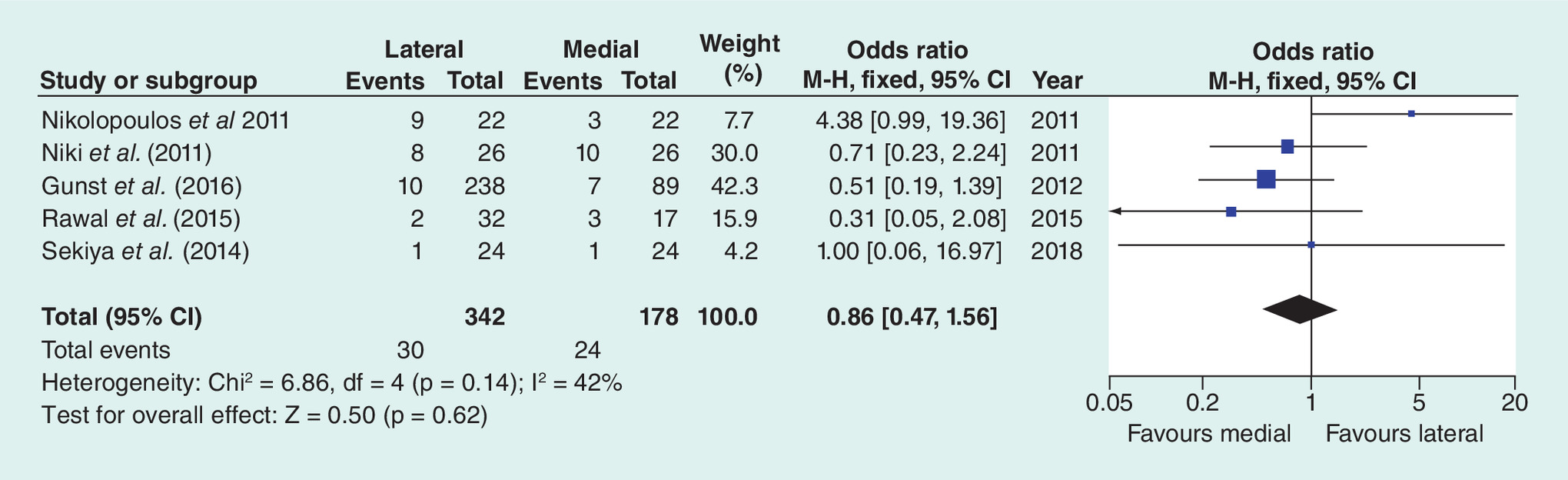
Figure 6. The pooled result of complications between lateral and medial groups.
M-H: Mantel-Haenszel.
| Quality assessment for nonrandomized trials | Niki et al. (2011) [15] | Rawal et al. (2015) [18] | Gunst et al. (2016) [19] | Langen et al. (2016) [20] | Guo et al. (2018) [21] |
|---|---|---|---|---|---|
| Clearly stated aim | 2 | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 1 | 1 | 2 | 2 | 1 |
| Prospective data collection | 2 | 0 | 2 | 0 | 0 |
| End points appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study end point | 2 | 0 | 0 | 2 | 0 |
| Follow-up period appropriate to the aims of study | 2 | 1 | 2 | 2 | 2 |
| Less than 5 % loss to follow-up | 2 | 2 | 0 | 2 | 2 |
| Prospective calculation of the sample size | 2 | 0 | 0 | 1 | 0 |
| Adequate control group | 2 | 2 | 2 | 2 | 2 |
| Contemporary groups | 2 | 2 | 2 | 2 | 2 |
| Baseline equivalence of groups | 2 | 2 | 2 | 1 | 1 |
| Adequate statistical analyses | 2 | 2 | 2 | 2 | 2 |
| Total score | 23 | 16 | 18 | 20 | 16 |
Discussion
In the current study, we searched the literature comparing the outcomes of the lateral and medial approach in TKA for the valgus knee. Pooled data showed superior knee score and KSS-function in patients using the lateral approach and comparable ROM, pain, valgus deformity and complications between the two approaches.
Balance of soft tissue is an important factor in the function after TKA, especially in the severely valgus knee. Initially, results of the treatment of the valgus knee by the medial approach were not as good as expected [3]. However, several papers reported excellent results in patients with severe valgus knee deformity after release of the lateral tissues by the medial parapatellar approach [8,22]. More recent studies have promoted the lateral approach an effective method of TKA for the valgus knee [23,24]. With the improvement of surgical procedures in medial and lateral approaches, both methods can guarantee the good knee function and pain control if the surgeons get well trained. Comparable blood loss and marginal differences in operative time also indicated the improvement of surgical technique.
The restoration of the anatomical axis after TKA is a critical factor for long-term success [25]. An inaccurate axis may impair the postoperative knee function [26]. It was previously reported that many valgus knee patients cannot achieve restoration of the anatomical axis through the medial approach [3]. In the current study, patients undergoing the lateral and medial approach exhibited comparable postoperative valgus deformity. Similar correction of the valgus deformity was the foundation of a comparable knee function. In addition, the patellofemoral instability was a factor in reported pain and need for surgical revision in some cases [27]. The lateral approach allows more control of the patellar tilt in the valgus knee. Niki et al. reported the tilt angle of the patella without further description and analysis [12]. Tonelli et al. found better control of the lateral tilt of the patella in the lateral approach group [13]. Accordingly, they suggested the use of the lateral approach for treatment of the valgus knee. Due to limited data, we cannot draw a definitive conclusion about the effect of approach on patella tilt. Additional data are required to evaluate the effects of these approaches on patella tilt.
Theoretically, the lateral approach may decrease complications due to the direct exposure and release of lateral constructions. Additionally, this approach may reduce the possibility of necrosis of the patella by avoiding damage to vascular structures that are encountered through the medial approach [28]. The included studies did not report any incidence of patellar necrosis with either of the medial or lateral approaches. However, the related fracture at the area of osteotomy or tibial plateau using the lateral approach was reported in the previously studies [5,29]. Langen et al. reported four cases of TTO-related complications out of 106 patients, of which three required additional fixations to manage operative fracture [20]. Fracture and migration were also reported in other studies. Excluding the TTO-related complications did not significantly change the trend in the two groups. Peroneal nerve palsy was reported to in 1–3% patients after TKA for valgus deformity [1,30]. However, only one included study reported two cases of transient peroneal nerve palsy in the lateral approach [18].
Some limitations must be mentioned in order to better understand the results. High-quality studies are the base to draw a solid conclusion in meta-analysis. However, only four RCTs were included and the total methodological quality in the current study was not promising. The radiological parameters were not thoroughly evaluated, and the patellar tracking should be further assessed to provide more evidence. Different techniques of release of the lateral soft tissue and the computer assisted surgery used in some studies also may have confounded our results. Future studies should have a standard design and with well-defined study parameters.
Conclusion
Current data show better KSS and KSS-function after arthroplasty with the lateral approach in patients with valgus knee. The lateral and medial approach performed similarly in terms of operative time, blood loss, WOMAC, ROM, pain, valgus control and total complications.
•
Total knee arthroplasty (TKA) is a challenge in patients with a valgus deformed knee.
•
There is no consensus in the results after medial or lateral approach for valgus knee.
•
An electronic search was performed in PubMed, Embase, Web of Science and Cochrane library. The following search terms were used: ‘total knee arthroplasty’ AND ‘valgus’ AND ‘knee’ limited in title AND ‘approach’ throughout the text. Manual search was conducted in the reference lists of initially identified studies.
•
Clinical characteristics and radiological features were extracted for analysis.
•
Mean difference (MD) or odds ratio with 95% CI was calculated for continuous or dichotomous variables. Fixed-effect model was used when I2 < 50% and p > 0.05. Otherwise, the random-effect model was selected.
•
Lateral approach leaded to better knee society score (MD = 2.49, 95% CI: 0.60–4.37, p = 0.01; I2 = 66%; p = 0.01) and function (MD = 1.24, 95% CI: 0.57–1.90, p < 0.001; I2 = 0; p = 0.95).
•
The two groups showed similar postoperative valgus deformity, operative time, blood loss, Western Ontario and McMaster Universities Osteoarthritis Index, range of motion, pain and total complications.
•
Compared with the medial approach for TKA in valgus knee, current data show superior results after TKA by the lateral approach.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
1.
Ranawat AS, Ranawat CS, Elkus M, Rasquinha VJ, Rossi R, Babhulkar S. Total knee arthroplasty for severe valgus deformity. J. Bone Joint Surg. Am. 87(Suppl. 1 [Pt 2]), 271–284 (2005).
2.
Apostolopoulos AP, Nikolopoulos DD, Polyzois I et al. Total knee arthroplasty in severe valgus deformity: interest of combining a lateral approach with a tibial tubercle osteotomy. Orthop. Traumatol. Surg. Res. 96(7), 777–784 (2010).
3.
Karachalios T, Sarangi PP, Newman JH. Severe varus and valgus deformities treated by total knee arthroplasty. J. Bone Joint Surg. Br. 76(6), 938–942 (1994).
4.
Gonzalez MH, Mekhail AO. The failed total knee arthroplasty: evaluation and etiology. J. Am. Acad. Orthop. Surg. 12(6), 436–446 (2004).
5.
Zonnenberg CB, Lisowski LA, van den Bekerom MP, Nolte PA. Tuberositas osteotomy for total knee arthroplasty: a review of the literature. J. Knee Surg. 23(3), 121–129 (2010).
6.
Hirschmann MT, Hoffmann M, Krause R, Jenabzadeh RA, Arnold MP, Friederich NF. Anterolateral approach with tibial tubercle osteotomy versus standard medial approach for primary total knee arthroplasty: does it matter? BMC Musculoskelet. Disord. 11, 167 (2010).
7.
Hamahashi K, Mitani G, Takagaki T et al. Clinical outcomes of patients with valgus deformity undergoing minimally invasive total knee arthroplasty through the medial approach. Open Orthop. J. 10, 717–724 (2016).
8.
Rajgopal A, Wakde O, Panda I. Long term outcomes of total knee arthroplasty in valgus knees – a fifteen year follow-up. Semin. Arthrop. 29(3), 214–222 (2018).
9.
Keblish PA. The lateral approach to the valgus knee. Surgical technique and analysis of 53 cases with over two-year follow-up evaluation. Clin. Orthop. Relat. Res. 271, 52–62 (1991).
10.
Stehlik J, Musil D, Held M, Starek M. Z-plasty for valgus deformity in total knee arthroplasty. Acta Chir. Orthop. Traumatol. Cech. 73(3), 169–175 (2006).
11.
Aglietti P, Lup D, Cuomo P, Baldini A, De Luca L. Total knee arthroplasty using a pie-crusting technique for valgus deformity. Clin. Orthop. Relat. Res. 464, 73–77 (2007).
12.
Niki Y, Matsumoto H, Hakozaki A, Kanagawa H, Toyama Y, Suda Y. Clinical and radiographic outcomes of minimally invasive total knee arthroplasty through a lateral approach. Knee Surg. Sports Traumatol. Arthrosc. 19(6), 973–979 (2011).
13.
Tonelli FJ, Passarelli MC, Brito JA, Campos GC, Zorzi AR, Miranda JB. Keblish's lateral surgical approach enhances patellar tilt in valgus knee arthroplasty. Rev. Bras. Ortop. 51(6), 680–686 (2016).
14.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 5, 13 (2005).
15.
Nikolopoulos DD, Polyzois I, Apostolopoulos AP, Rossas C, Moutsios-Rentzos A, Michos IV. Total knee arthroplasty in severe valgus knee deformity: comparison of a standard medial parapatellar approach combined with tibial tubercle osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 19(11), 1834–1842 (2011).
16.
Sekiya H, Takatoku K, Takada H, Sugimoto N, Hoshino Y. Lateral approach is advantageous in total knee arthroplasty for valgus deformed knee. Eur. J. Orthop. Surg. Traumatol. 24(1), 111–115 (2014).
17.
Kornilov N, Kulyaba T, Petukhov A, Ignatenko V, Thienpont E. Computer navigation helps achieving appropriate gap balancing and restoration of alignment in total knee arthroplasty for fixed valgus knee osteoarthritis irrespective of the surgical approach. Acta Orthop. Belg. 81(4), 673–681 (2015).
18.
Rawal J, Devany AJ, Jeffery JA. Arthroplasty in the valgus knee: comparison and discussion of lateral vs medial parapatellar approaches and implant selection. Open Orthop. J. 9, 94–97 (2015).
19.
Gunst S, Villa V, Magnussen R, Servien E, Lustig S, Neyret P. Equivalent results of medial and lateral parapatellar approach for total knee arthroplasty in mild valgus deformities. Int. Orthop. 40(5), 945–951 (2016).
20.
Langen S, Gaber S, Zdravkovic V, Giesinger K, Jost B, Behrend H. Lateral subvastus approach with tibial tubercle osteotomy for primary total knee arthroplasty: clinical outcome and complications compared to medial parapatellar approach. Eur. J. Orthop. Surg. Traumatol. 26(2), 215–222 (2016).
21.
Guo CJ, Liu J, Niu DS et al. Clinical application of different operative approach of total knee replacement in knee valgus patients. Retrospective cohort study. Int. J. Surg. 49, 80–83 (2018).
22.
Qiu S, Zhang M, Jia T. Total knee arthroplasty for severe valgus knee deformity. Int. J. Clin. Exp. Med. 9(5), 8725–8730 (2016).
23.
Chalidis BE, Ye K, Sachinis NP, Hawdon G, McMahon S. Lateral parapatellar approach with tibial tubercle osteotomy for the treatment of non-correctable valgus knee osteoarthritis. A retrospective clinical study. Knee 21(1), 204–208 (2014).
24.
Aurich M, Lenz M, Best N. A modified lateral approach for total knee replacement in type 2 valgus deformity. Orthopedics 40(5), 313–316 (2017).
25.
Favorito PJ, Mihalko WM, Krackow KA. Total knee arthroplasty in the valgus knee. J. Am. Acad. Orthop. Surg. 10(1), 16–24 (2002).
26.
Ritter MA, Faris PM, Keating EM, Meding JB. Postoperative alignment of total knee replacement. Its effect on survival. Clin. Orthop. Relat. Res. Feb(299), 153–156 (1994).
27.
Malo M, Vince KG. The unstable patella after total knee arthroplasty: etiology, prevention, and management. J. Am. Acad. Orthop. Surg. 11(5), 364–371 (2003).
28.
Young CF, Bourne RB, Rorabeck CH. Tibial tubercle osteotomy in total knee arthroplasty surgery. J. Arthroplasty 23(3), 371–375 (2008).
29.
Piedade SR, Pinaroli A, Servien E, Neyret P. Tibial tubercle osteotomy in primary total knee arthroplasty: a safe procedure or not? Knee 15(6), 439–446 (2008).
30.
Keblish PA. The lateral approach to the valgus knee. Surgical technique and analysis of 53 cases with over two-year follow-up evaluation. Clin. Orthop. Relat. Res. Oct(271), 52–62 (1991).
Information & Authors
Information
Published In
Pages: 35 - 44
PubMed: 31777265
Copyright
© 2019 Future Medicine Ltd.
History
Received: 4 August 2019
Accepted: 28 October 2019
Published online: 28 November 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The lateral and medial approach in total arthroplasty for valgus knee: a meta-analysis of current literature. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0111
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Vrajesh Shah, Rajiv Paradkar, Tanmay Jaysingani, Chintan Parmar, Sachin Patel, Nandlal Bharwani, Does Surgical Approach Actually Affect the Functional Outcomes of Total Knee Arthroplasty Patients?, Journal of Orthopaedic Diseases and Traumatology, 10.4103/jodp.jodp_32_25, 8, 1, (65-68), (2026).
- Xinhua Yang, Haokang Zhang, Guishi Li, Microscopic Anatomical Study of the Choke Zone in Valgus Knee Arthroplasty Incisions and its Clinical Implications, Indian Journal of Orthopaedics, 10.1007/s43465-025-01652-7, 60, 6, (1347-1354), (2025).
- Bin Yang, Christos Koutserimpas, Bin Sun, Cécile Batailler, Elvire Servien, Sébastien Lustig, Lateral approach for total knee arthroplasty in patients with valgus deformity: A step-by-step surgical technique, SICOT-J, 10.1051/sicotj/2025047, 11, (51), (2025).
- Emeline Chapron, Rémy Coulomb, Aymeric Weiss, Philippe Marchand, Pascal Kouyoumdjian, Robot-assisted surgery and knee arthroplasty in genu valgum: impact of the surgical approach, Orthopaedics & Traumatology: Surgery & Research, 10.1016/j.otsr.2025.104226, 111, 4, (104226), (2025).
- Luca Andriollo, Pietro Gregori, Christos Koutserimpas, Elvire Servien, Cécile Batailler, Pascal Kouyoumdjian, Sébastien Lustig, Lateral approach in robotic total knee arthroplasty for valgus knees: A step-by-step technique, SICOT-J, 10.1051/sicotj/2025017, 11, (20), (2025).
- Maamoun Alsalloum, Assil‐Ramin Alimy, Jan Hubert, Tim Rolvien, Bernd Fink, The lateral approach for total knee arthroplasty in valgus osteoarthritis provides similar clinical and radiological results compared with the medial approach, Knee Surgery, Sports Traumatology, Arthroscopy, 10.1002/ksa.12526, 33, 4, (1378-1386), (2024).
- Rajesh Kumar Rajnish, Amit Srivastava, Sandeep Kumar Yadav, Abhay Elhence, Nitesh Gahlot, Prasoon Kumar, Saurabh Gupta, Sameer Aggarwal, Comparative Analysis of Outcomes of Lateral Versus Medial Approach in the Total Knee Arthroplasty for Valgus Deformity: A Systematic Review and Meta-analysis, Indian Journal of Orthopaedics, 10.1007/s43465-024-01211-6, 58, 10, (1323-1338), (2024).
- Luca ANDRIOLLO, Stefano M. ROSSI, Rudy SANGALETTI, Alberto POLIZZI, Alice MONTAGNA, Luca MATASCIOLI, Loris PERTICARINI, Francesco BENAZZO, Total arthroplasty in valgus knee: an update in the robotics era, Minerva Orthopedics, 10.23736/S2784-8469.24.04429-8, 75, 3, (2024).
- Satoshi Miyamoto, Shin Sasaki, Hiroyuki Kojin, Ken Okazaki, Total knee arthroplasty for knee osteoarthritis associated with abnormal patellar tendon deformity: a case report, Journal of Surgical Case Reports, 10.1093/jscr/rjae102, 2024, 3, (2024).
- Michele Mercurio, Giorgio Gasparini, Olimpio Galasso, Filippo Familiari, Erminia Cofano, Valentina Sanzo, Gianluca Ciolli, Katia Corona, Simone Cerciello, Lateral versus medial approach for total knee arthroplasty for valgus knee deformity shows comparable functional outcomes, hip–knee–ankle angle values, and complication rates: a meta-analysis of comparative studies, Archives of Orthopaedic and Trauma Surgery, 10.1007/s00402-023-05088-2, 144, 2, (869-878), (2023).