A randomized controlled clinical trial of a hypothermically stored amniotic membrane for use in diabetic foot ulcers
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Determine the effectiveness of hypothermically stored amniotic membrane (HSAM) versus standard of care (SOC) in diabetic foot ulcers (DFUs). Methods: A randomized controlled trial was conducted on 76 DFUs analyzed digitally. Results: Cox wound closure for HSAM (38 wounds) was significantly greater (p = 0.04) at weeks 12 (60 vs 38%), and 16 (63 vs 38%). The probability of wound closure increased by 75% (Hazard Ratio = 1.75; 95% CI: 1.16–2.70). HSAM showed >60% reductions in area (82 vs 58%; p = 0.02) and depth (65 vs 39%; p = 0.04) versus SOC. Conclusion: HSAM increased frequency and probability of wound closure in DFUs versus SOC.
Over a million individuals suffer from nonhealing diabetic foot ulcers (DFUs) each year in the USA and it has been estimated that 15% of diabetics will develop a chronic ulcer at some point in their lives [1,2]. Once a patient develops a DFU and a wound care treatment is initiated, assessments of wound status at 4 weeks compared with baseline have been shown to be indicators of long-term clinical outcomes. Reductions in wound size at 4 weeks from baseline have been shown to be strong surrogates for DFU healing that may help guide clinicians' plans for DFU management. Using databases of over 40,000 DFUs, it has been demonstrated that size reductions of >50% and >60% were highly sensitive and specific surrogate end points for long-term healing [3–5]. The average ulcer can take 6 months to 1 year to heal completely and over 50% of subjects will have nonhealed ulcers that extend beyond 1 year [6–8]. It has been reported that within 5 years after achieving wound closure, between 70 and 100% of these healed ulcers will re-open and require additional ulcer management treatments [9]. DFUs substantially reduce patients' quality of life, are often painful, and adversely affect mobility and sleep [10–13]. Furthermore, ulcers are significantly correlated with time lost from work, job loss and high rates of adverse effects and serious adverse events [14,15]. It has been estimated that nonhealing ulcers of various etiologies cause the loss of over 2 million working days per year in the USA [16]. Costs to healthcare payers in the USA are estimated to exceed $20 billion per year considering only direct costs associated with medical resource utilization and treatment costs [17–19].
Contamination of the ulcer bed, colonization with bacteria and infection are associated with a localized inflammatory response in the ulcer bed with high levels of proteolytic enzymes, matrix metalloproteases and specific collagenases that degrade the extracellular matrix (ECM). These enzymes, if present in high concentrations in the initial inflammatory stages of wound closure interrupt the normal sequence of events that result in wound closure. If the ulcer is not modulated by the patient's own immune system or wound care techniques that down regulate the activity of proteolytic enzymes, it fails to proceed through the normal phases of wound closure. Chronic ulcers stall in the inflammatory stage of wound healing and thereby fail to progress through the normal phases of the wound closure cascade leading to full epithelialization. It has been reported that the incidence of developing a foot infection in patients diagnosed with diabetes is 9% and the most common complication is osteomyelitis [20,21]. The overall chance of a DFU becoming infected every 6 months was reported as 40% in a 2-year study of a representative population of patients presenting with uninfected DFUs. A high proportion of these DFUs developed an infection prior to healing, regardless of their ulcer type. DFUs that had healed in <3 months, between 3 and 12 months, and not healed by 12 months demonstrated infection rates of 32, 59 and 40% respectively [20]. Further, DFU infections have been shown to be a major cause of hospitalization and contribute to over 90% of nontraumatic lower limb amputations [22]. It has consistently been demonstrated that early detection and intervention for ulcers that exhibit delayed wound closure are essential to reduce the risk of serious, clinical outcomes [18,23].
Clinical studies have demonstrated the efficacy of cellular or tissue-based products such as placental-derived allografts in accelerating healing of chronic wounds [24–28]. The proposed mechanism of action is the delivery of growth factors and the reduction in proteases [29,30]. Novel processing technologies and hypothermic storage conditions of amniotic membranes that more completely preserve amnion and/or chorion components maintain viable differentiated cell populations, stem cells, growth factors, cytokines and ECM proteins. Preservation of these components may improve chronic wound management outcomes. To date, clinical trials have evaluated only dehydrated and cryopreserved grafts. This trial is the first to examine hypothermically stored amniotic membrane (HSAM).
Materials & methods
Study design
A multicenter, prospective, randomized, controlled, clinical trial was conducted across 14 centers to assess clinical outcomes associated with the use of HSAM plus standard of care (SOC) compared with SOC alone.
For HSAM, the investigational treatment, manufacturing, recovery and processing of donated tissues were performed in accordance with all federal, state and local regulations, including the US FDA regulations 21 CFR 1270 and 1271. Serological testing for bacterial, viral and infectious diseases were performed on blood specimens from each donor and exceeded the requirements of FDA and the American Association of Tissue Banks (AATB). Viral testing included antibodies to HIV-1, HIV-2, HTLV-1, HTLV-2, Hepatitis B Core, Hepatitis C and CMV total. Tests for HIV-1 nucleic acid, Hepatitis B Surface Antigen and other adventitious viruses and pathogens were also conducted.
In this trial, HSAM plus SOC treatment was compared with SOC treatment alone. SOC consisted of debridement, infection elimination, use of dressings and offloading by total contact casting (TCC). Study SOC followed guideline treatment that addressed debridement/devitalized tissue, infection or inflammation, moisture balance and wound edge preparation/wound depth (the DIME paradigm) [31]. HSAM-treated ulcers were compared with SOC-treated ulcers by analyses that determined frequency of wound closure. Also evaluated were time to wound closure, the number of subjects showing >60% reduction in baseline ulcer area, the number of subjects showing >60% reduction in baseline ulcer depth, the number of subjects showing >75% reduction in baseline ulcer volume. Measurements of ulcer area, depth and volume were obtained at each subject visit to determine mean percent changes from baseline.
The purpose of this randomized controlled trial (RCT) was to investigate the comparative effectiveness of HSAM and SOC versus SOC alone in the treatment of DFUs over a 16 week study period (12-week treatment phase and a 4 week follow-up phase). A 2 week screening phase of the study was required to determine if patients met all protocol inclusion and exclusion criteria. When all inclusion and exclusion criteria were met, and prior to receiving study treatment, patients were randomized 1:1 to either the HSAM plus SOC group (HSAM group), or the SOC alone (SOC) group. These analyses evaluated 76 randomized subjects. The primary analyses were frequency of and time to wound closure by 16 weeks (12 weeks in the treatment phase of the study, 4 weeks in the follow-up phase). Ulcer area (cm2), depth (mm) and volume (cm3) were measured using digital planimetry (Silhouette®, Aranz Medical, Christchurch, New Zealand). The Aranz laser-assisted wound measurement device has been demonstrated to provide accurate and valid measurements for wound area, depth and volume [32,33]. The percentage difference in measurements of all three parameters were computed at each study visit from baseline for each wound. The final visit denoting DFU wound closure was not always recorded; thus, wound closure was defined as an ulcer achieving an area between 0 and 0.1 cm2. The wound closure end point used in this study was consistent with Aranz Silhouette® imaging validation data [32–34]. The length of time that subjects were followed in the study was a maximum of 16 weeks. Treatment and evaluation visits occurred weekly. Assessments of frequency of and median time to wound closure were determined by ulcer area measurements at weekly subject visits. The incidence of ulcers that demonstrated >60% reduction in ulcer area and depth and the incidence of ulcers that demonstrated >75% reduction in ulcer volume from baseline were evaluated for HSAM versus SOC treatment groups. Mean percent changes from baseline in area, depth and volume were also calculated for HSAM and SOC treatment groups.
Subjects
This study was conducted in accordance with the specifications of the protocol and in accordance with principles consistent with Good Clinical Practice, 21 CFR 312, ICH E6, HIPAA regulations in 45 CFR Part 164. Western Institutional Review Board (WIRB; WA, USA) acted as the central institutional review board for the study. Subjects read and understood an institutional review board (IRB) approved informed consent prior to undergoing study activities. Treatment records included subject ID (including ulcer care center of treatment) and study treatment; subject baseline age and sex; and ulcer area, depth and volume at all study visits. The study population was comprised of subjects with Type I or II diabetes with a DFU of greater than or equal to 4-weeks duration at presentation that was unresponsive to SOC. All included subjects presented with a DFU located below the medial aspect of the malleolus extending at least through the epidermis into dermis, subcutaneous tissue, muscle, or tendon but not into bone. Subjects had well controlled glucose levels with HbA1c <12% and an ulcer between 1 and 25 cm2. Other key inclusion criteria included: minimum age of 18 years, adequate lower extremity perfusion as evidenced by transcutaneous oxygen measurement (TCOM) or a skin perfusion pressure (SPP) measurement of ≥30 mmHg, or an ankle-brachial index (ABI) between 0.7 and ≤1.3 or toe-brachial index (TBI) of ≥0.6 within 3 months of the first Screening Visit, no evidence of unresolved gross soft-tissue infection or osteomyelitis as ruled out by x-rays, CAT scan or MRI, no evidence of underlying comorbid conditions that would adversely affect wound closure (cancer, Raynaud's Syndrome, severe venous insufficiency or uncorrected arterial insufficiency), and abstaining from concomitant medications that would compromise wound closure (cytotoxic drugs or chemotherapeutics). Exclusion criteria included: evidence of skin cancer within or adjacent to the ulcer site, symptoms of osteomyelitis, ulcers of the calcaneus, renal impairment (creatinine >2.5 mg/dl), hepatic impairment (≥2 x ULN), hematologic disorders, cellulitis, ulcers with sinus tracts, active deep vein thrombosis, uncontrolled diabetes and severely immune compromised subjects. During the 2-week run-in period, the ulcers were debrided and off-loaded using TCC. During the 2-week run-in period, the ulcers were debrided and off-loaded using TCC. Ulcers that healed 20% or more were excluded from the trial. In both study groups the ulcers were prepared using standard methods that included sharp debridement (by curette or scalpel) to ensure that the ulcer area was free of debris and necrotic tissue. Ulcer beds and peri-ulcer areas were cleansed with normal, sterile saline solution. HSAM was applied directly with the stromal side in contact with the wound per manufacturer specifications on the open ulcer bed at weekly intervals or until healed. This was followed by application of outer dressings. Off-loading was achieved by means of TCC for plantar ulcers, and fixed ankle walker boots (in the case of infection), or other appropriate means at the discretion of the investigator for nonplantar ulcers.
Data collection
The data were collected via the Aranz digital data collection system and provided to the SerenaGroups® by Investigators. Accurate records of the clinical data generated from this study were maintained according to Good Clinical Practices requirements. Investigators were responsible for collecting and accurately recording the clinical data generated for this study in a timely manner.
Statistical methods
The study subjects who met protocol inclusion and exclusion were randomized 1:1 to either the HSAM or SOC group. PASS 15 was used to generate the random allocation sequence for each site, which was composed of a random sequence of block sizes of 4 interspersed with single asymmetric sequences, but still designed to achieve a balanced design. The number of study subjects in each group was computed to show sufficient statistical power for the primary end point. The sample size calculation was based on the assumption that there is a difference of 30% between the two treatment groups in the percentage of subjects who attain wound closure. The proportion in group one (HSAM) was assumed to be 0.30 under the null hypothesis and 0.60 under the alternative hypothesis. The proportion in group two (SOC) was 0.30. The test statistic used was the two-sided Z test with pooled variance. Under the above assumptions, 38 subjects per treatment group were required to meet the α level of statistical significance (p-value) of 0.05 and 80% power for a total of 76 subjects in the study.
Descriptive statistical methods were used to summarize the data with hypothesis testing performed for the primary and other selected efficacy end points. Statistical analyses were conducted using SAS 9.4 programs (SAS Institute, NC, USA). All testing for end points was performed using two-sided methods with alpha set at a level of <0.05 for significance. Baseline patient, wound and treatment characteristics were compared between treatment groups in the following manner: normal theory variables used the two-sample t test, other continuous variables used the Mann-Whitney-Wilcoxon test, and categorical variables used the χ2 test. All analyses were performed on the intent to treat (ITT) population of subjects randomized in the trial. Frequency of wound closure and a series of secondary analyses were also performed on data obtained by or on 16 weeks.
The frequency or proportions of wound closure (computed as number of wounds closed/number of wounds treated) were compared for HSAM and SOC by 12 and 16 weeks. χ2 tests were performed to determine statistical differences between all proportions. The incidence of ulcers achieving >60% reductions from baseline in ulcer area and depth, and >75% reduction from baseline in ulcer volume were calculated as the number of ulcers achieving the end point divided by the number of ulcers treated. These end points were summarized by counts and proportions. Mean percent changes from baseline were summarized for ulcer areas, depths and volumes.
Wound closure rates as a function of time (weeks) were determined (SAS 9.4) and tested for significance by log–rank tests, two-sided. The time to wound closure was evaluated using the Kaplan–Meier (K–M) method. The total duration of the trial was 16 weeks (12 weeks in the treatment phase of the study, 4 weeks in the follow-up phase). The median event time along with the percentage of subjects achieving wound closure at select time points were computed along with log–rank tests, two-sided.
A forward selection Cox proportional hazards regression model that adjusted for treatment, age, sex, BMI, area, depth, volume and age of the ulcer at baseline, was performed to compute the hazard ratio (HR; 95% CI) or probability of attaining wound closure over the entire course of the study (day 0 through to study week 16). Cox adjusted survival data for wound closure also was used to analyze the estimated frequency of wound closure at every timepoint that subjects were evaluated. Statistical significance was tested using the log–rank test, two-sided.
Data from all subjects randomized in the study (n = 76) were included in the ITT analysis (Figures 1–3).
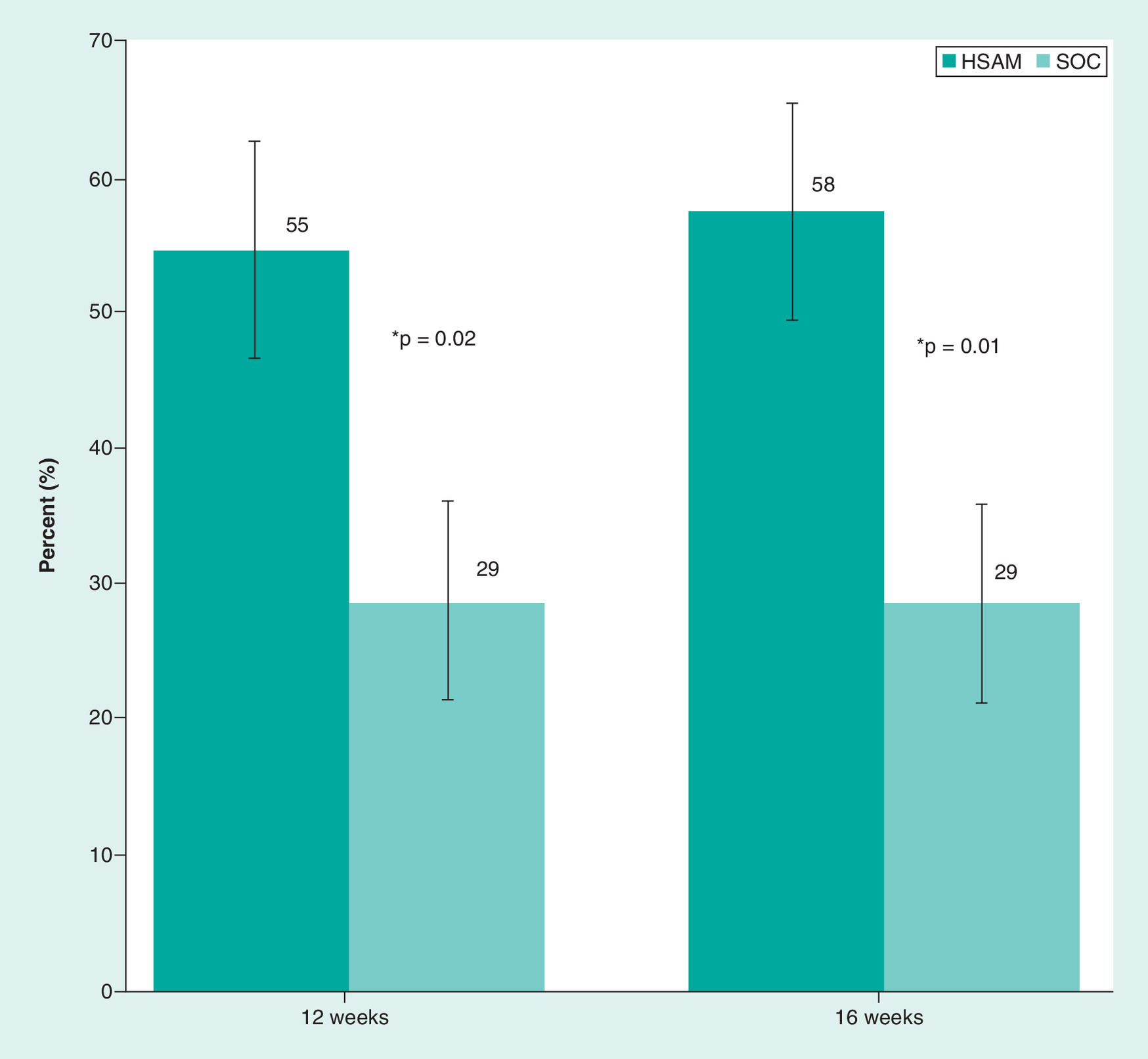
Figure 1. Incidence of wound closure at 12 weeks and 16 weeks.
*p-values at 12 and 16 weeks: χ2 tests.
HSAM: Hypothermically stored amniotic membrane; SOC: Standard of care.
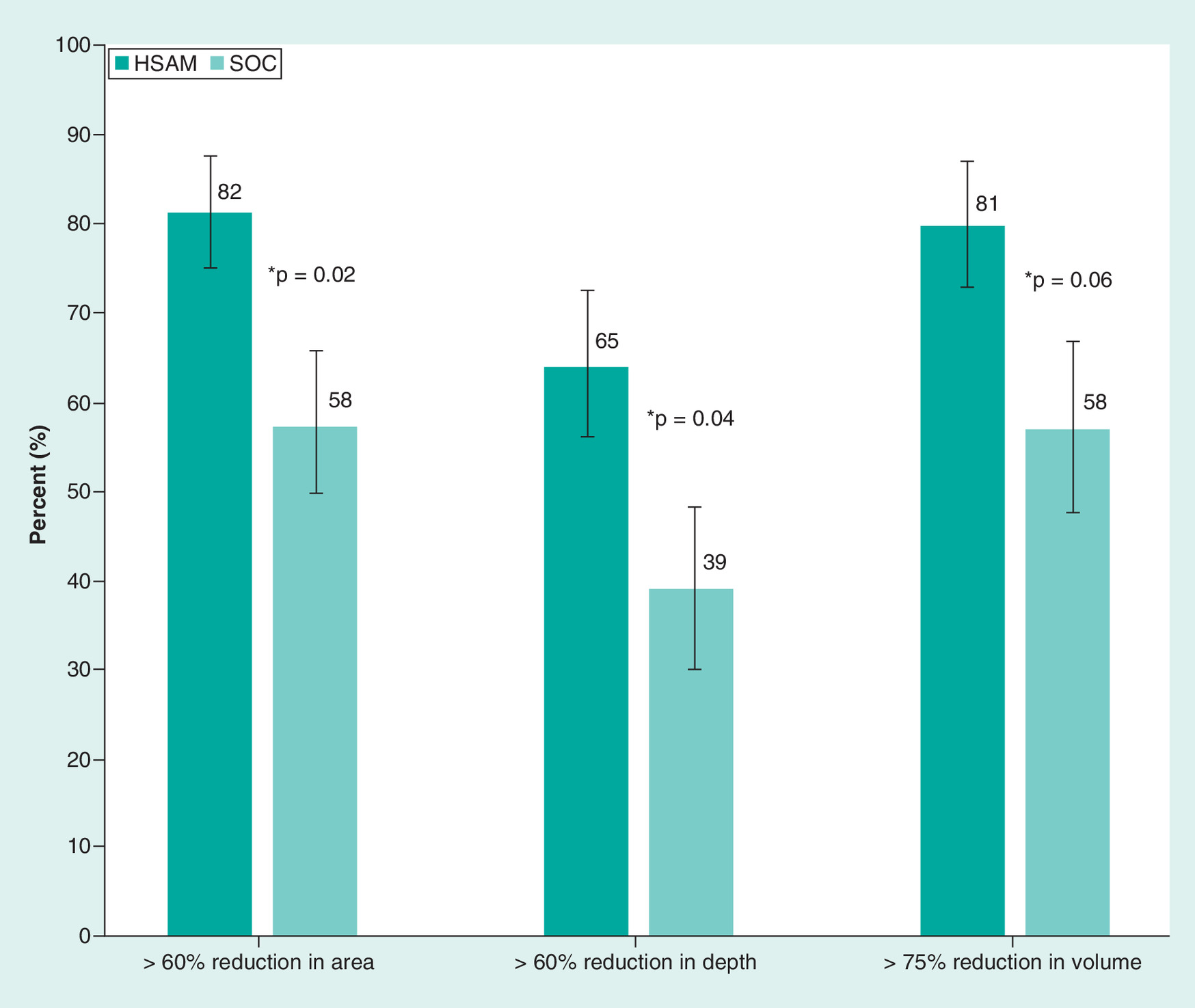
Figure 2. Incidence of reduction from baseline in ulcer area, depth, and volume.
*p-values: χ2 tests.
HSAM: Hypothermically stored amniotic membrane; SOC: Standard of care.
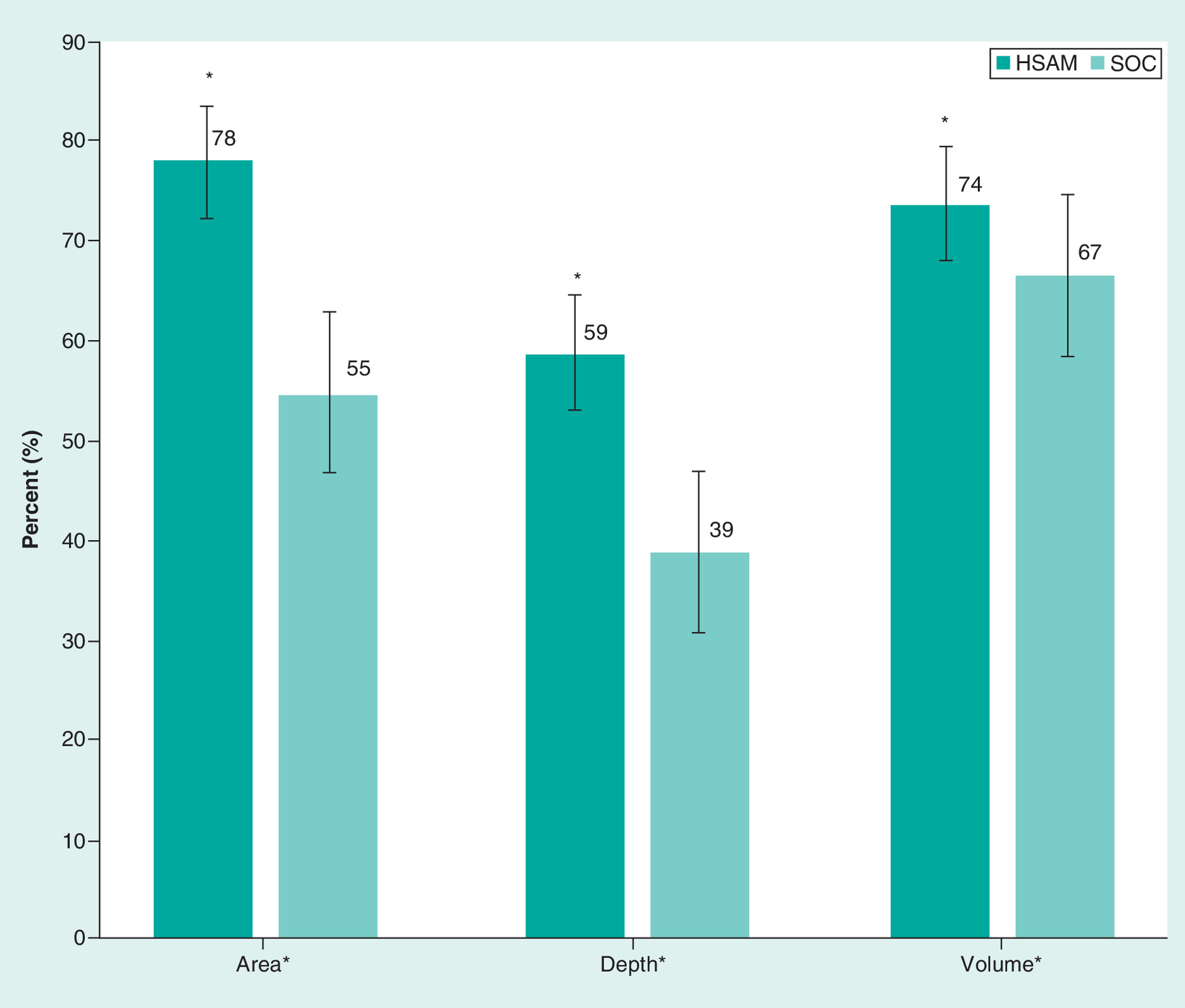
Figure 3. Treatment group mean percent reductions in ulcer area, depth, and volume.
HSAM: Hypothermically stored amniotic membrane; SOC: Standard of care.
Results
Each subject had one ulcer identified as the index ulcer for treatment in the study (n = 76: 38 HSAM [14 Wagner 1, 24 Wagner 2]; 38 SOC [15 Wagner 1, 23 Wagner 2]). There were no significant differences in baseline patient demographics or ulcer characteristics between the two treatment groups (Table 1). The majority of patients were males (77.6%) and the median age was 59 years. At the first treatment application, the mean ulcer area was 3.12 cm2 in the HSAM group and 3.33 cm2 in the SOC group. Ulcers in the HSAM and SOC groups had mean ulcer depths of 2.5 versus 3.0 mm and mean ulcer volumes of 0.33 versus 0.21 cm3 respectively (Table 1).
| Patient and ulcer characteristic | HSAM (n = 38) | SOC (n = 38) | p-value* |
|---|---|---|---|
| Age (years) | |||
| Mean ± SD | 59.2 ± 7.61 | 59.6 ± 10.72 | 0.801 |
| Median | 59.5 | 58.5 | |
| Sex, n (%) | 38 | 38 | |
| Female | 8 (21.1) | 9 (23.7) | 0.783 |
| Male | 30 (78.9) | 29 (76.3) | |
| Number of ulcers treated per patient | 38 | 38 | |
| Mean ± SD | 1.0 ± 0.00 | 1.0 ± 0.0 | 1 |
| Median | 1.0 | 1.0 | |
| Ulcer area (cm2) | 38 | 38 | |
| Mean ± SD | 3.12 ± 3.86 | 3.33 ± 4.62 | 0.763 |
| Median | 1.65 | 1.7 | |
| Ulcer depth (mm) | 34 | 28 | |
| Mean ± SD | 2.47 ± 3.28 | 2.99 ± 2.59 | 0.345 |
| Median | 2 | 3 | |
| Ulcer volume (cm3) | 31 | 26 | |
| Mean ± SD | 0.33 ± 0.61 | 0.21 ± 0.33 | 0.242 |
| Median | 0.10 | 0.10 |
*For continuous variables, the p-value is from a two-sided, two sample t test, testing for a difference in means between treatments. For categorical variables, the p-value is from a two-sided Fisher's exact test testing for a difference in proportions between treatments.
HSAM: Hypothermically stored amniotic membrane; SD: Standard deviation; SOC: Standard of care.
The primary unadjusted end point of wound closure for HSAM-treated ulcers was significantly greater than SOC by 12 weeks (55 vs 29%; p = 0.02) and 16 weeks (58 vs 29%; p = 0.01) respectively (Figure 1). The K–M median time to wound closure for HSAM-treated ulcers was 11 weeks. For SOC-treated ulcers, the K–M median time to wound closure was not attained by 16 weeks (i.e., 50% of patients in the SOC group failed to demonstrate wound closure by the end of study, 16 weeks). A forward selection Cox proportional hazards regression model that adjusted for treatment, age, sex, BMI, area, depth, volume and age of the ulcer at baseline, was performed to compute the hazard ratio (HR) or probability of attaining wound closure over the entire course of the study (study day 0 through to study week 16). The Cox regression hazard ratio (HR = 1.75 [1.16–2.70]) showed a 75% greater weekly probability of wound closure in favor of the HSAM group. Cox adjusted survival data for wound closure showed that HSAM was superior to SOC at 4 weeks (11% vs 3%), 8 weeks (36% vs 23%), 12 weeks (60% vs 38%) and 16 weeks (63% vs 38%); p = 0.04.
DFUs treated in the study showed an incidence of achieving greater than a 60% reduction in baseline area (82 vs 58%; p = 0.02) and depth (65 vs 39%; p = 0.04) for the HSAM-treated and the SOC-treated wounds respectively (Figure 2). In addition, the incidence of ulcers demonstrating greater than a 75% reduction in baseline volume was greater in the HSAM-treated subjects compared with the SOC-treated subjects (81 vs 58%; p = 0.06; Figure 2). Group comparisons showed that the HSAM-treated group demonstrated greater mean percent decreases at the end of study from baseline in ulcer area (78 vs 55%), depth (59 vs 39%) and volume (74 vs 67%) compared with the SOC group (Figure 3).
Discussion
The data show that the use of HSAM plus SOC was effective in managing DFUs. Results demonstrated favorable clinical outcomes in a diverse patient population with ulcers refractive to healing with routine wound care treatments. HSAM-treated subjects in this trial showed statistically significant, greater frequencies of wound closure compared with SOC-treated subjects. Improvement in the median time to wound closure was also shown for HSAM-treated ulcers. Additionally, significant reductions in baseline ulcer area and depth compared with SOC were demonstrated. Using one clinically meaningful example, when DFU improvement is defined as wound closure of >60%, 31 of 38 (82%) of HSAM-treated subjects improved compared with 22 of 38 (58%) of SOC-treated subjects (p = 0.02). The literature strongly supports the use of surrogate end points in predicting long-term healing of DFUs. In particular, robust surrogate end points for healing have been ulcer area reductions of >50% and >60% from baseline [3–5]. In this trial, we used a strict cut-off of >60% area reduction as an end point for ulcer improvement and as a surrogate for long-term healing. Greater than 70% sensitivity and specificity have been demonstrated when the >60% wound closure surrogate was used to predict healing [4]. One retrospective cohort study (39,918 neuropathic wounds on 20,213 individuals) showed correct classification of healed or not healed by 20 weeks of 70% [4]. The ulcer area reduction data reported in this study are intended to provide clinically meaningful information that may help guide treatment decisions for the management of DFUs. In addition, we showed reductions in ulcer depth and volume. These end points demonstrated remarkable similarities to area reduction data and suggest general responsiveness to HSAM treatment as well as overall clinical improvement. By all assessment metrics in this trial, HSAM wound management resulted in improved clinical outcomes that would be associated with beneficial effects on patients' quality of life, activities of daily living and ability to work.
It was notable in this study that the incidence of >60% reduction in ulcer area and depth, and the incidence of >75% reduction in ulcer volume correlated well with the mean percent decreases from baseline in area, depth and volume. On the one hand, for >60% reductions in area and depth, and >75% reduction in volume, only individuals meeting or exceeding the established thresholds are counted and positively contribute to the reported incidence. On the other hand, the entire population of HSAM-treated and SOC-treated subjects contribute data to the mean percent changes in area, depth and volume where no thresholds apply, and any single ulcer may show increases or decreases in the measured parameter. Concordance of the incidence data and the mean percent change data show that consistent, favorable clinical outcomes extended to over 80% of the HSAM-treated group.
Both frequency of and time to wound closure in this trial compared favorably to other published data on adjunctive ulcer care treatments categorized as skin substitutes by CMS (Centers for Medicare and Medicaid). The pivotal study for FDA approval of a bilayered living cellular construct (BLCC; Apligraf®, Organogenesis Inc., MA, USA) for the treatment of DFUs showed a frequency of wound closure of 56% and a median time to wound closure of 9 weeks [35]. HSAM showed similar results in this RCT with a frequency of wound closure of 55% at 12 weeks and a median time to wound closure of 11 weeks. In recent CERs of cell and tissue products for the treatment of chronic ulcers, median times to wound closure have been variously reported as: 26 weeks for dehydrated human amnion chorion membrane (dHACM; Epifix®, MiMedx, Integra LifeSciences, GA, USA), 30 weeks for fetal bovine collagen dressing (FBCD; PriMatrix®, Integra LifeSciences, MA, USA), and 43 weeks for acellular porcine small intestinal submucosa collagen dressing (SIS; Oasis®, Smith & Nephew, FL, USA) [36–38].
In this DFU study, clinical outcomes showed generalized improvement with HSAM DFU management when compared with SOC DFU management (sharp debridement, moist primary wound contact dressings, and aggressive offloading using TCC). These clinical benefits are likely due to HSAM's composition characterized by intact amniotic membrane. The manufacturing of HSAM occurs without modification to the native amnion structure, and refrigerator storage maintains membrane cell viability. This is in direct contrast to other human amniotic membrane products that are variously manipulated in manufacturing, dehydrated, or cryopreserved. Preclinical investigations have shown that HSAM preserves unmodified ECM, growth factors, viable differentiated cells and nondifferentiated cells. HSAM-treated DFUs in this study overcame the significant barriers to wound closure that exist in chronic ulcers treated with routine therapies, thus indicating that the HSAM applied positively supports the wound healing process [39,40].
The rigorous standards of data collection employed in this study are fundamental to the strength of the results. Many clinical trials report on subjective assessments of wound healing. In this study, we relied exclusively on wound measurements obtained from a validated wound imaging system used by all 14 participating sites. Determinations of wound closure, areas, depths and volumes used in the assessments of primary and secondary efficacy outcomes were consistently applied not only within and between treatment groups, but also within and between treatment centers. Much of the variability in wound evaluations that commonly confound study results was minimized or eliminated by the accurate data capture systems used in this trial. One uniformly applied measurement technique for index ulcers as well as validated, standardized methods of statistical analyses lend to the integrity of the study. Additionally, all measurements at all time points were used in a true ITT analysis where all randomized subjects contributed data to the final results. Clinical outcomes were reliably reported (Figures 1–3), and clinically meaningful conclusions were able to be drawn.
These HSAM effectiveness data are consistent with RCT data reviewed in meta-analyses that suggested potentially favorable healthcare economic outcomes with the use of amniotic membrane allografts in chronic wound management [26,41]. Positive healthcare economics associated with skin substitutes has been shown to be significant [17,42]. Findings suggest that use of living cell-based skin substitutes for treatment of DFU may lower overall medical costs through reduced utilization of costly healthcare services [43]. In recent analyses from large databases (US Ulcer Registry) from electronic health records (EHR) of subjects that mirror the population of subjects in the current HSAM study, over 7000 ulcers in more than 5000 subjects were tracked for clinical outcomes and costs of ulcer care [43]. Of the total number of subjects with nonwound closure ulcers analyzed, subjects with pressure ulcers made up 25% of the population, followed by 20% with surgical ulcers, 14% with DFUs, 13% with trauma ulcers, radiation ulcers and ulcers of various etiologies combined, with the remainder classified as being of mixed etiology. The subjects were followed for up to 5 years and were shown to accrue total direct costs to the medical system of over US$29,249,500 for ulcer management alone. The costs of unhealed ulcers were reported to increase substantially over time from US$4000 per patient at 6 months to US$18,000 at 2 years and beyond [43,44]. All subjects that entered this trial had longstanding, nonhealing ulcers that were refractive to routine treatments. It would be consistent with previously published literature that a skin substitute that demonstrates higher wound closure rates may offer a cost-effective DFU wound management approach. Importantly, HSAM-treated DFUs closed at a median time of 11 weeks (2.8 months), and the median time to closure was not achieved in SOC-treated DFUs by the end of the 4 month trial showing that the median time to wound closure for the SOC group was greater than 4 months.
Limitations of this trial included the lack of blinding in using a skin substitute compared with standard bandages as the primary wound contact material. While both investigators and patients in the trial were aware of treatment group assignment, digital imaging, transfer of de-identified patient wound measurement data generated by Aranz computer algorithms, and analyses of all wound data by a blinded independent group of assessors mitigated many of the potential biases associated with open-label trials. We also recognize that this study, like all RCTs, was intended to demonstrate efficacy and as such was conducted under carefully controlled conditions. This trial had high ‘internal validity’ because of randomization, careful selection of participants and standardized treatment protocols, and the objective of the study was to maximize the possibility of observing a treatment effect, if it existed [38,45,46]. While RCTs are considered level 1 evidence in determining if a product can actually work, there are limitations in the generalizability or ‘external validity’ of the clinical data generated [47]. Because this RCT of HSAM versus SOC required compliance to defined criteria for patient inclusion and exclusion, rigorous monitoring and adherence to the treatment protocol, clinical evaluations in ordinary settings and in broader populations are recommended.
Better informed clinical practice decisions rely on evidence from additional RCTs and CERs. Comprehensive data on clinically important DFU subgroups including patient demographics, wound characteristics and treatment characteristics have yet to be generated. The current HSAM trial results, however, show valid information that may help to further inform wound treatment algorithms regarding the use of skin substitutes. HSAM is currently in use in the US (HSAM is marketed in the US as an HCT) not only for DFUs, but also for dehisced wounds, pressure ulcers, venous leg ulcers and other wounds with exposed bone and tendon. What remains to be pursued by clinicians and clinical researchers is the systematic collection of clinical data for various wounds types, patient populations and clinical practice settings.
Though this was the first RCT of HSAM and the study was properly powered for expected treatment effect size based on real-life use of the product, further prospective effectiveness and cost-effectiveness studies, including studies analyzing patient reported outcomes and recurrence rates are warranted. Comparative effectiveness research studies in a real-world setting that include larger numbers of patients and centers, as well as longer follow-up times hold promise to better define the effectiveness of HSAM compared with other amniotic membrane allografts.
In conclusion, this RCT showed that HSAM significantly increased the frequency of wound closure compared with SOC and showed a shorter time to wound closure in a population of subjects with nonhealing DFUs. When used as an adjunct to SOC, HSAM significantly reduced baseline ulcer area, depth and volume.
•
This was the first prospective, comparative effectiveness research randomized control trial that compares efficacy of a fresh hypothermically stored amniotic membrane (HSAM) to an active control standard of care (SOC) for the treatment of diabetic foot ulcers (DFUs).
•
Treatment with HSAM significantly improved the incidence and time to DFU wound closure.
•
Cox adjusted survival data for wound closure showed that HSAM was superior to SOC at 4 weeks (11 vs 3%), 8 weeks (36 vs 23%), 12 weeks (60 vs 38%) and 16 weeks (63 vs 38%); p = 0.04.
•
HSAM shows a 75% greater probability of wound closure on a weekly basis for the entire 16 week study period compared with SOC-treated ulcers; Hazard ratio = 1.75 (95% CI: 1.16–2.70).
•
The unadjusted frequency of wound closure for HSAM-treated ulcers was significantly greater than SOC by 12 weeks (55 vs 29%; p = 0.02) and 16 weeks (58 vs 29%; p = 0.01).
•
HSAM showed a higher incidence of >60 percent reductions in area (82 vs 58%; p = 0.02) and depth (65 vs 39%; p = 0.04).
•
Improvements in the probability, wound closure rate and frequency of wound closure support use of HSAM plus SOC for DFU wound management.
•
Comparative Effectiveness Research studies of real-world data comparing HSAM to other amniotic membrane allografts for the management DFUs are warranted.
Author contributions
All authors (from institutions 1 – 7): (a) made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND (b) drafted the work or revised it critically for important intellectual content; AND (c) gave final approval of the version to be published; AND (d) agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. No ghostwriters were used to write this article.
Acknowledgments
The authors wish to acknowledge Virtu Stat, Ltd. (North Wales, PA) for statistical support.
Financial & competing interests disclosure
This study was funded by Organogenesis, Inc. TE Serena., R Yaakov, S Moore and R Hamil serve as SerenaGroup® consultants to Organogenesis, Inc. ML Sabolinski serves as a consultant for AOBiome, Neumedicines, Organogenesis Inc. and Allergan. S Wendling is an employee of Organogenesis. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human investigations. In addition, for all subjects participating in this prospective RCT, informed consent has been obtained prior to any study procedures being performed.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Data sharing statement
The manuscript reports original clinical research from a randomized controlled trial. Individual subject's data will be shared upon request post-completion of the trial and publication of the subject's data. All wound measurements will be available to participants. ICFs, IRB approvals, the study protocol will be shared as requested. Subjects must sign a data access request for their personal data and access to these data will be available for up to three years after publication study results.
References
1.
American Diabetes Association AD. Economic costs of diabetes in the U.S. in 2012. Diabetes Care 36(4), 1033–1046 (2013).
2.
Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA 293(2), 217 (2005).
3.
Sheehan P, Jones P, Caselli A, Giurini JM, Veves A. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes care. 26(6), 1879– 1882 (2003).
4.
Margolis DJ, Gelfand JM, Hoffstad O, Berlin JA. Surrogate end points for the treatment of diabetic neuropathic foot ulcers. Diabetes Care 26(6), 1696–1700 (2003).
5.
Snyder RJ, Cardinal M, Dauphinée DM, Stavosky J. A post-hoc analysis of reduction in diabetic foot ulcer size at 4 weeks as a predictor of healing by 12 weeks. Ostomy. Wound. Manage. 56(3), 44–50 (2010).
6.
Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv. Wound Care 4(9), 560–582 (2015).
7.
Driver VR, Fabbi M, Lavery LA, Gibbons G. The costs of diabetic foot: the economic case for the limb salvage team. J. Vasc. Surg. 52(3), 17S–22S (2010).
8.
Al-Musa HM. Prevalence of diabetic foot and the associated risk factors at primary health care level in southwestern Saudi Arabia Int. J. Current Research & Rev. 5(13), 58 (2013).
9.
Nunan R, Harding KG, Martin P. Clinical challenges of chronic wounds: searching for an optimal animal model to recapitulate their complexity. Dis. Model. Mech. 7(11), 1205–1213 (2014).
10.
Wang C, Mai L, Yang C et al. Reducing major lower extremity amputations after the introduction of a multidisciplinary team in patient with diabetes foot ulcer. BMC Endocr. Disord. 16(1), 38 (2016).
11.
Serena T, Yaakov R, Aslam S, Aslam R. Preventing, minimizing, and managing pain in patients with chronic wounds: challenges and solutions. Chronic Wound Care Manag. Res. 3, 85–90 (2016).
12.
Bradbury S, Price P. The impact of diabetic foot ulcer pain on patient quality of life. Wounds UK 7(4), (2011).
13.
Sheahan H, Canning K, Refausse N et al. Differences in the daily activity of patients with diabetic foot ulcers compared to controls in their free-living environments. Int. Wound J. 14(6), 1175–1182 (2017).
14.
Sumpio BE. Contemporary evaluation and management of the diabetic foot. Scientifica. 2012, 435487 (2012).
15.
Allen L, Powell-Cope G, Mbah A, Bulat T, Njoh E. A retrospective review of adverse events related to diabetic foot ulcers. Ostomy. Wound. Manage. 63(6), 30–33 (2017).
16.
Jung K, Covington S, Sen CK et al. Rapid identification of slow healing wounds. Wound Repair Regen. 24(1), 181–188 (2016).
17.
Rice JB, Desai U, Cummings AKG, Birnbaum HG, Skornicki M, Parsons NB. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care 37(3), 651–658 (2014).
18.
Rice JB, Desai U, Ristovska L et al. Economic outcomes among Medicare patients receiving bioengineered cellular technologies for treatment of diabetic foot ulcers. J. Med. Econ. 18(8), 586–595 (2015).
19.
Nussbaum SR, Carter MJ, Fife CE et al. An economic evaluation of the impact, cost, and Medicare policy implications of chronic nonhealing wounds. Value Health 21(1), 27–32 (2018).
20.
Jia L, Parker CN, Parker TJ et al. Incidence and risk factors for developing infection in patients presenting with uninfected diabetic foot ulcers. PLoS ONE 12(5), e0177916 (2017).
21.
Giurato L, Meloni M, Izzo V, Uccioli L. Osteomyelitis in diabetic foot: a comprehensive overview. World J. Diabetes 8(4), 135 (2017).
22.
Rodrigues BT, Vangaveti VN, Malabu UH. Prevalence and risk factors for diabetic lower limb amputation: a clinic-based case control study. J. Diabetes Res. 2016, 5941957 (2016).
23.
Hankin CS, Knispel J, Lopes M, Bronstone A, Maus E. Clinical and cost efficacy of advanced wound care matrices for venous ulcers. J. Manag. Care Pharm. 18(5), 375–384 (2012).
24.
Kirsner RS, Sabolinski ML, Parsons NB, Skornicki M, Marston WA. Comparative effectiveness of a bioengineered living cellular construct vs. a dehydrated human amniotic membrane allograft for the treatment of diabetic foot ulcers in a real world setting. Wound Repair Regen. 23(5), 737–744 (2015).
25.
Lavery LA, Fulmer J, Shebetka KA et al. The efficacy and safety of Grafix® for the treatment of chronic diabetic foot ulcers: results of a multi-centre, controlled, randomised, blinded, clinical trial. Int. Wound J. 11(5), 554–560 (2014).
26.
Laurent I, Astère M, Wang KR, Cheng Q, Li QF. Efficacy and time sensitivity of amniotic membrane treatment in patients with diabetic foot ulcers: a systematic review and meta-analysis. Diabetes Ther. 8(5), 967–979 (2017).
27.
Mohajeri-Tehrani MR, Variji Z, Mohseni S et al. Comparison of a bioimplant dressing with a wet dressing for the treatment of diabetic foot ulcers: a randomized, controlled clinical trial. Wounds 28(7), 248–254 (2016).
28.
Raspovic KM, Wukich DK, Naiman DQ et al. Effectiveness of viable cryopreserved placental membranes for management of diabetic foot ulcers in a real world setting. Wound Repair Regen. 26(2), 213–220 (2018).
29.
McQuilling JP, Vines JB, Mowry KC. In vitro assessment of a novel, hypothermically stored amniotic membrane for use in a chronic wound environment. Int. Wound J. 14(6), 993–1005 (2017).
30.
Koob TJ, Lim JJ, Zabek N, Massee M. Cytokines in single layer amnion allografts compared to multilayer amnion/chorion allografts for wound healing. J. Biomed. Mater. Res. Part B Appl. Biomater. 103(5), 1133–1140 (2015).
31.
Snyder RJ, Fife C, Moore Z. Components and quality measures of DIME (devitalized tissue, infection/inflammation, moisture balance, and edge preparation) in wound care. Adv. Skin Wound Care 29(5), 205–215 (2016).
32.
Constantine RS, Bills JD, Lavery LA, Davis KE. Validation of a laser-assisted wound measurement device in a wound healing model. Int. Wound J. 13(5), 614–618 (2016).
33.
ARANZ Medical. ARANZ medical resources (2019). www.aranzmedical.com/aranz-medical-resources/.
34.
Davis KE, Constantine FC, MacAslan EC, Bills JD, Noble DL, Lavery LA. Validation of a laser-assisted wound measurement device for measuring wound volume. J. Diabetes Sci. Technol. 7(5), 1161–1166 (2013).
35.
Veves A, Falanga V, Armstrong DG, Sabolinski ML. Graftskin, a human skin equivalent, is effective in the management of noninfected neuropathic diabetic foot ulcers: a prospective randomized multicenter clinical trial. Diabetes Care. 24(2), 290–295 (2001).
36.
Kirsner RS, Sabolinski ML, Parsons NB, Skornicki M, Marston WA. Comparative effectiveness of a bioengineered living cellular construct vs. a dehydrated human amniotic membrane allograft for the treatment of diabetic foot ulcers in a real world setting. Wound Repair Regen. 23(5), 737–744 (2015).
37.
Sabolinski ML, Gibbons G. Comparative effectiveness of a bilayered living cellular construct and an acellular fetal bovine collagen dressing in the treatment of venous leg ulcers. J. Comp. Eff. Res. 7(8), 797–805 (2018).
38.
Marston WA, Sabolinski ML, Parsons NB, Kirsner RS. Comparative effectiveness of a bilayered living cellular construct and a porcine collagen wound dressing in the treatment of venous leg ulcers. Wound Repair Regen. 22(3), 334–340 (2014).
39.
Carpenter S, Davis S, Fitzgerald R et al. Expert recommendations for optimizing outcomes in the management of biofilm to promote healing of chronic wounds. Wounds 28(Suppl. 6), 1–20 (2016).
40.
Wolcott RD, Rhoads DD, Bennett ME et al. Chronic wounds and the medical biofilm paradigm. J. Wound Care 19(2), 45–53 (2010).
41.
Haugh AM, Witt JG, Hauch A et al. Amnion membrane in diabetic foot wounds. Plast. Reconstr. Surg. Glob. Open 5(4), e1302 (2017).
42.
Rice JB, Desai U, Ristovska L et al. Economic outcomes among Medicare patients receiving bioengineered cellular technologies for treatment of diabetic foot ulcers. J. Med. Econ. 18(8), 586–595 (2015).
43.
Fife CE, Carter MJ, Walker D, Thomson B. Wound care outcomes and associated cost among patients treated in US outpatient wound centers: data from the US Wound Registry. Wounds 24(1), 10 (2012).
44.
Nussbaum SR, Carter MJ, Fife CE et al. An economic evaluation of the impact, cost, and medicare policy implications of chronic nonhealing wounds. Value Health 21(1), 27–32 (2018).
45.
Eaglstein WH, Kirsner RS. Expectations for comparative effectiveness and efficacy research: with welcomed questions may come unwelcome answers. JAMA Dermatol. 149(1), 18–199 (2013).
46.
van Staa T-P, Leufkens HG, Zhang B, Smeeth L. A comparison of cost effectiveness using data from randomized trials or actual clinical practice: selective cox-2 inhibitors as an example. PLoS Med. 6(12), e1000194 (2009).
47.
Concato J. When to randomize, or ‘evidence-based medicine needs medicine-based evidence’. Pharmacoepidemiol. Drug Saf. 21(Suppl. 2), 6–12 (2012).
Information & Authors
Information
Published In
Pages: 23 - 34
PubMed: 31691579
Copyright
© 2019 Michael L Sabolinski. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 23 September 2019
Accepted: 21 October 2019
Published online: 6 November 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A randomized controlled clinical trial of a hypothermically stored amniotic membrane for use in diabetic foot ulcers. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0142
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Stephanie M. Mueller, Hannah D. Shi, Aditi Kaveti, Amy Du, Devin J. Clegg, Romi Wagner, Dennis P. Orgill, Comparative Certainty of Evidence for Diabetic Foot Ulcer Therapies: A Narrative Synthesis, Diabetology, 10.3390/diabetology7070131, 7, 7, (131), (2026).
- Dean Vayser, Alexander Reyzelman, Alisha Oropallo, Michael L Sabolinski, Kelly A Kimmerling, Maribel Riesco, Hypothermically stored amniotic membrane compared to standard of care for complex venous leg ulcers: a randomised controlled clinical trial, Journal of Wound Care, 10.12968/jowc.2026.0204, 35, Sup7a, (2026).
- Jia Teng, Fuyang Lin, Ling Wang, Mingjun Jiang, Zhiqiao Li, Guanchi Yan, Jia Mi, Systematic review of the efficacy and safety of biologically and tissue-derived therapies for the treatment of diabetic foot, Frontiers in Endocrinology, 10.3389/fendo.2026.1800592, 17, (2026).
- Daniel Kapp, Angelina Ferguson, T Kent Denmark, Jonathan Johnson, Shawn Naqvi, Shaun Carpenter, Jordan Morrison, Efficacy of a dual-layer pre-hydrated amniotic membrane allograft in the treatment of hard-to-heal wounds, Journal of Wound Care, 10.12968/jowc.2025.0604, 35, 2, (150-161), (2026).
- Chengcheng Zheng, Weiwei Tang, Xingwu Ran, Efficacy and Safety of Human Amniotic Membrane for Chronic Wounds: A Systematic Review and Meta-Analysis of Clinical Trials, Advances in Wound Care, 10.1177/21621918251411808, (2026).
- Joseph Caporusso, Travis Motley, John C. Lantis, Stephen Heisler, Adam Hicks, Stephanie C. Wu, Alexander Reyzelman, A Multi‐Centre, Randomised, Controlled Clinical Trial Assessing Cryopreserved Ultra‐Thick Human Amniotic Membrane in the Treatment of Complex Diabetic Foot Ulcers, Wound Repair and Regeneration, 10.1111/wrr.70110, 33, 6, (2025).
- Kirk Mitchell, Application of a full-thickness placental allograft in complex wound management: a case series across diverse aetiologies, Journal of Wound Care, 10.12968/jowc.2025.0459, 34, S11a, (S15-S24), (2025).
- Brock A Liden, Kelly A Kimmerling, Katie C Mowry, Hypothermically stored amniotic membrane in the management of hard-to-heal wounds of the lower extremities: a retrospective case series, Journal of Wound Care, 10.12968/jowc.2025.0194, 34, 10, (782-788), (2025).
- Eddie Soong, Brad Marcinek, Cristin Taylor, Christopher Michaelis, Real-World Use of a Decellularized Porcine Placental Extracellular Matrix in Hard-to-Heal Wounds: A Retrospective, Single-Center Study, Journal of Clinical Medicine, 10.3390/jcm14196823, 14, 19, (6823), (2025).
- Xuyang Hu, Huixin Meng, Jiaru Liang, Hang An, Jiaqi Zhou, Yuling Gao, Chong You, Zhenni Zhang, Xiaoyang Gong, Yong Liu, Comparison of the efficacy of 12 interventions in the treatment of diabetic foot ulcers: a network meta-analysis, PeerJ, 10.7717/peerj.19809, 13, (e19809), (2025).
- See more