Comparative effectiveness of pulmonary arterial hypertension drugs in treatment-naive patients: a network meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: No network meta-analysis has been conducted to study efficacy of drug therapies specific for treatment of pulmonary arterial hypertension in treatment-naive patients only. Methods: Randomized controlled trials on pulmonary arterial hypertension-specific drug therapies were searched and a Bayesian network meta-analysis was performed. The 6-min walking distance (6MWD) and all-cause mortality were efficacy outcomes, whereas discontinuation due to adverse events was a safety-related outcome. Results: Analysis included 3.713 patients from 21 trials. Combination of ambrisentan and tadalafil showed the greatest impact on 6MWD, followed by epoprostenol and intravenous treprostinil (high dose). The latter two demonstrated marked effect size on mortality, although not statistically significant. Conclusion: According to 6MWD, ambrisentan/tadalafil combination was considered as most effective among all comparisons.
Prospero ID: CRD42019110832.
Pulmonary arterial hypertension (PAH) is classified as a group 1 pulmonary hypertension (PH) and is defined by mean pulmonary artery pressure ≥25 mmHg, pulmonary artery wedge pressure ≤15 mmHg and pulmonary vascular resistance >3 Wood units, in the absence of other causes of precapillary PH (such as lung disease, chronic thromboembolic disease and other rare diseases). For a definitive diagnosis of PAH, a hemodynamic assessment by right heart catheterization is required [1]. The most widely used exercise test in PH centers remains to be 6-min walking test, since an improvement of the measured 6-min walking distance (6MWD) is a valuable goal in patients with PAH for its prognostic features of increased survival [1]. According to the REVEAL registry study (Registry to Evaluate Early and Long-Term PAH Disease Management) several parameters were independently associated with 1-year survival and among these an increased mortality was associated with higher functional classes, and absolute values of 6MWD less than 165 m [2]. In the last decade, a significant progress has been made in the treatment of PH. Particularly, certain types of PAH are now being treated with recently authorized drugs, and nearly all have been approved for use based on a change in 6MWD as a clinically relevant endpoint [3,4]. Currently, there are three main pathways to which different drug classes interfere with purpose of treatment of PAH: prostacyclin pathway (epoprostenol and prostacyclin analogs; prostacyclin receptor agonists), nitric oxide pathway (phosphodiesterase-5 inhibitors [PDE-5i] and cyclic guanylate cyclase stimulators) and endothelin pathway (selective and dual endothelin receptor antagonists [ERAs]). All drug agents belonging to afore mentioned drug classes have been shown to improve dyspnea, 6MWD, pulmonary hemodynamics and functional class [5]. Several meta-analyses were published recently and have compared directly or indirectly the efficacy and/or safety of two or more drug agents within the same class or between classes, with focus on oral medications, or compared monotherapy versus combination (background) therapy, either in all patients from selected randomized controlled trials, or groups with a specific subtype of PAH. None of these have focused on PAH-specific drug therapies in treatment-naive patients [6–11].
Our objective was to conduct a systematic review of randomized controlled trials (RCTs) and to develop a Bayesian network meta-analysis model to assess the comparative efficacy of drug therapies specific for PAH in treatment-naive patients, based on 6MWD, mortality and discontinuation due to adverse events.
Methods
The protocol for the systematic review has been registered within international prospective register of systematic reviews database (PROSPERO). The registration number is CRD42019110832.
Study identification
We have conducted a systematic literature search for published data in electronic databases PubMed, Embase, Cochrane Library and ClinicalTrials.gov. Following subject terms were used in our searches: (‘pah’ OR ‘pulmonary arterial hypertension’) AND (‘epoprostenol’ OR ‘treprostinil’ OR ‘iloprost’ OR ‘ambrisentan’ OR ‘bosentan’ OR ‘beraprost’ OR ‘macitentan’ OR ‘sildenafil’ OR ‘tadalafil’ OR ‘riociguat’ OR ‘selexipag’). The titles and abstracts of all references were screened one by one to check their qualifications. The literature search was last updated in December 2018.
Eligibility criteria
All search hits were first filtered to hits available in English language, refined by deleting duplicates and limited to studies of a ‘RCT’ design. After reading the title and abstract, search hit was excluded, if the article: described a study on patients from other WHO PH groups or no data for PH group 1 was available. Articles unrelated to PAH, case reports or articles on studies with irrelevant interventions (either diagnostic or medical or pharmacological using vardenafil or sitaxentan or conventional therapy not specific to PAH – calcium channel blockers, anticoagulants, diuretics and other heart failure therapy) or design (cross-over, retrospective studies, observational) were also excluded.
After reading full-text articles, studies were considered as applicable, if recognized as RCTs, where comparator was either another PAH-specific drug, placebo or conventional therapy; reported the efficacy outcomes which are commonly adopted in clinical trials of PAH, namely: 6MWD and mortality; evaluated patients with PAH were primarily adults (although allowing patients under 18 years if most of the participants were adults); the minimal follow-up period was 8 weeks; evaluated an intervention with a PAH-specific therapy (administered alone or in a combination). At last, studies that included patients on PAH-specific background therapy were excluded, with exception of those where the percent of included patients on PAH-specific background therapy was less than 50%.
Data extraction & outcome measures
Database search was performed by two reviewers (M Petrovič & I Locatelli) who independently extracted following information from selected studies: first author, publication year, treatment and comparator arms, study design and duration, number of randomized participants, number of participants in each study arm, changes in 6MWD at 2–9 months, death (all-cause mortality), discontinuation due to adverse events, baseline 6MWD and classification of patients at baseline according to the WHO functional class (WHO FC). Additionally, for each study, the WHO FC factor was calculated by multiplication of the functional class number (I to IV) and proportion of the patients belonging to the respective WHO FC at baseline. Studies with the WHO FC factor calculated at 3 or above were classified as evaluating severe PAH patients, while studies with WHO FC factor below 3 were considered as evaluating PAH patients with low risk status.
For continuous outcome measure 6MWD, differences in the mean change from baseline (mean change) separately for treatment and comparator arm and their standard errors were extracted or calculated [12]. For dichotomous outcomes, the total number of patients (N) and the number of patients with events (n) were extracted or calculated for each treatment.
Quality assessment
The quality of included trials was assessed by using the Cochrane Risk of Bias assessment tool. The risk of bias tool covers six domains of bias: selections bias, performance bias, detection bias, attrition bias, reporting bias and other bias [12].
Network meta-analysis
A network meta-analysis (NMA) methodology allows for the combination of direct and indirect evidence for comparison among several treatments. This approach is widely accepted by decision makers in the context of health technology assessment [13,14]. The NMA was conducted by using a Bayesian framework in Openbugs version 3.2.3. Random effect models, adjusted to allow comparison of RCTs with more than two arms, were utilized for this analysis and the parameter estimation was performed using noninformative prior distributions [15]. Moreover, Bayesian technique enables rank ordering of each treatment included in the NMA. The rank order was calculated for each treatment with respect to the considered outcome (6MWD, mortality and discontinuation due to adverse events). For the continuous outcome (i.e., mean change in 6MWD), a regression model with a normal likelihood distribution and identity link was used, while a binomial distribution and logit link were used for dichotomous outcomes (i.e., mortality, and discontinuation due to adverse events) [15]. For continuous outcome, mean difference in change from baseline over study follow-up period was reported along with the 95% credible interval (CrI). CrIs are the Bayesian equivalent of CIs. For dichotomous outcomes, median values of the odds ratio (OR) and 95% CrI were reported. Results were considered statistically significant if the 95% CrI did not include zero for continuous outcome variables or one for dichotomous outcome variables.
Models were evaluated using the deviance information criterion (DIC), a measure which combines model fit and complexity of the model. The goodness-of-fit was measured using the overall residual deviance (Dres) and the degree of heterogeneity, defined as between-trial precision and between-trial standard deviation (for continuous outcome) or coefficient of variation (for dichotomous outcomes). Models with the lowest DIC or Dres value in relation to the number of data points were selected [16,17]. All the outcomes were assessed using random effects models. The initial 10,000 iterations of models were discarded as ‘burn-ins’, and models were run for 100,000 iterations to ensure convergence.
For evaluation of inconsistency, a node-splitting analysis was used to assess whether direct and indirect evidence on a specific node (the split node of a closed loop in the network) are united [18]. Triangular loops were identified in two networks (two for 6MWD network and one for the all-cause mortality network).
Sensitivity analysis
To examine the influence of studies having a high or unclear risk of bias on NMA results, a sensitivity analysis was performed separately for all three outcomes by including only studies with low risk of bias. In addition, a network meta-regression analysis with a subgroup indicator covariate (dichotomized WHO FC factor) was performed to examine differences in efficacy of treatments between patients with severe PAH and patients with low risk status. In this analysis, a common covariate effect across comparisons was assumed for the 6MWD outcome [15].
Results
Included studies
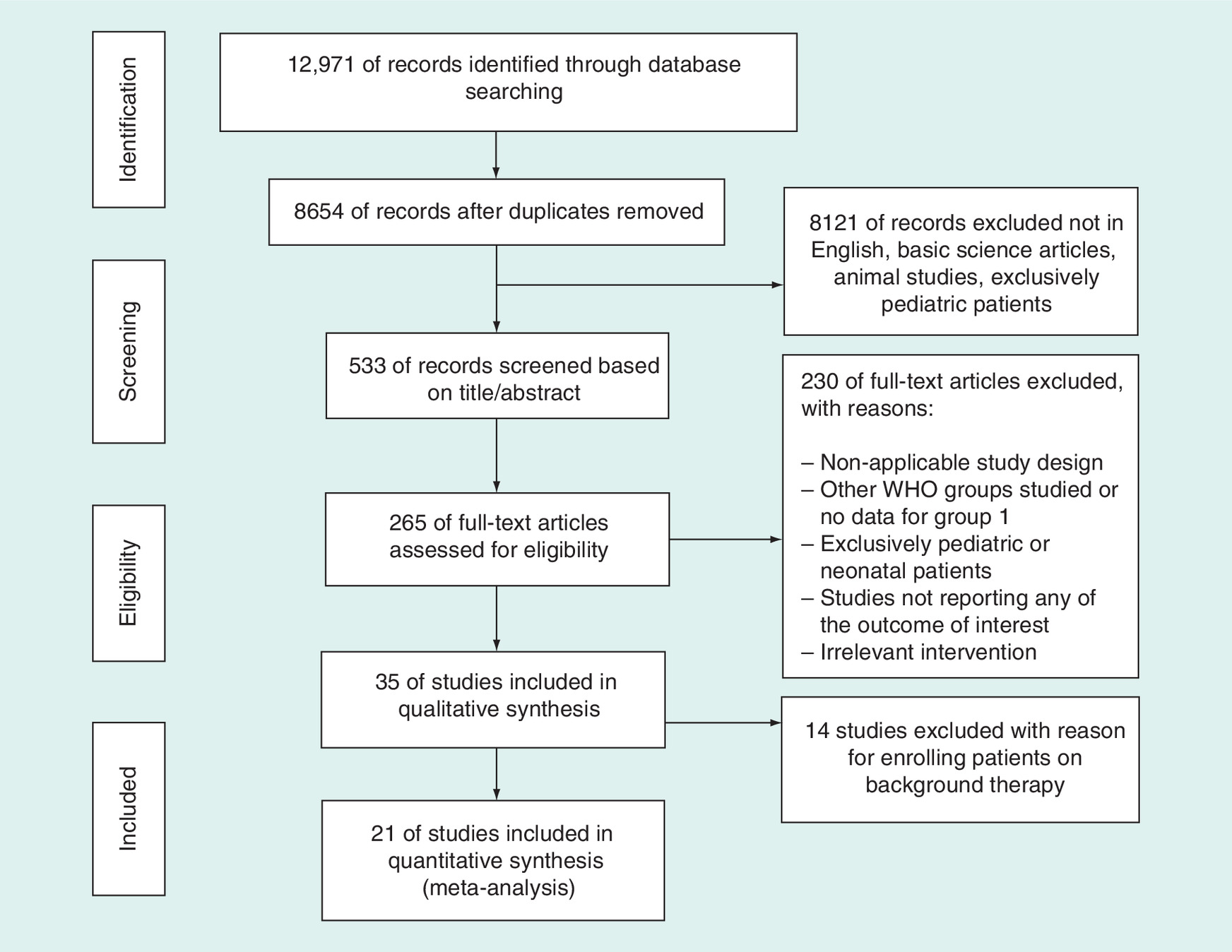
A total of 12.971 potentially relevant publications were identified by literature. After removing duplicates, and reviewing 533 articles, further 265 articles were excluded due to irrelevant titles and abstracts. After full text review of articles, 230 articles were removed for various reasons (as described in Figure 1). At last, 21 RCTs met the inclusion criteria and were retrieved for data extraction [4,19–37].
Characteristics & quality of included studies
Table 1 lists main characteristics of selected studies including first author, publication year, trial acronym (if existing), study design, description of PAH therapy in the treatment and comparator arms and number of belonging patients, route of administration, baseline value of 6MWD and proportion of patients distributed per FC. A total of 3.713 patients were included in the analysis. Nineteen studies compared at least one dose of PAH-specific drug therapy with placebo. Two studies directly compared two or more PAH-specific drug therapies without placebo [19,27]. A single study evaluated combination of two different PAH-specific drug therapies [19]. Five studies compared different doses of the same PAH-specific drug against placebo, namely ambrisentan [24], bosentan [31], sildenafil [26] and tadalafil [23]. The latter study was mainly performed on patients using bosentan as a background therapy, however, only results of subgroup analysis on treatment-naive patients were included. The same approach was taken for the study with riociguat [4]. Figure 2 shows three network diagrams of treatments, which were evaluated in studies separately for outcomes 6MWD, all-cause mortality and discontinuation due to adverse event.
| First author (year), trial name | Study design | Treatment(s), daily doses† | Comparator, daily doses† | Evaluated outcomes | Outcome assessment time | Baseline value of 6MWD, mean (SD) in metres | Proportion of patients per WHO FC at baseline (%) | WHO FC category | [Ref.] | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 6MWD | Mortality | AE | Treatment | Comparator | FC I | FC II | FC III | FC IV | |||||||
| Galieet al. (2015), AMBITION | MC, DB | Ambrisentan 10 mg + tadalafil 40 mg (n = 302) | Ambrisentan 10 mg (n = 152) | Yes | Yes | No | 24 w | 354 (88) | 354 (92) | 0 | 31 | 69 | 0 | Low-risk patients | [19] |
| Tadalafil 40 mg (n = 151) | 354 (88) | ||||||||||||||
| Ghofrani et al. (2013)## PATENT-1 | MC, DB | Riociguat 2.5 mg TID (n = 123) | Placebo (n = 66) | Yes | No | No | 12 w | 361 (68) | 368 (75) | 2 | 45 | 52 | 1 | Low-risk patients | [4] |
| Jing et al. (2013), FREEDOM-M | MC, DB | Treprostinil 12 mg BID (n = 233) | Placebo (n = 116) | Yes | Yes | Yes | 12 w | 332 (72) | 325 (77) | 0 | 37 | 63 | 0 | Severe patients | [13] |
| Hiremath et al. (2010), TRUST-1 | MC, DB | iv. Treprostinil‡ (n = 30) | Placebo (n = 14) | Yes | Yes | Yes | 12 w | 259 (12) | 231 (20) | 0 | 0 | 96 | 4 | Severe patients | [20] |
| Galie et al. (2008), EARLY¶¶ | MC, DB | Bosentan 125 mg BID (n = 93) | Placebo (n = 92) | Yes | Yes | Yes | 26 w | 438 (86) | 431 (91) | 0 | 100 | 0 | 0 | Low-risk patients | [21] |
| Galie et al. (2009)## PHIRST | MC, DB | Tadalafil 2.5 mg (n = 38) | Placebo (n = 35)## | Yes | No | No | 16 w | 347 (71) | 343 (84) | 2 | 31 | 66 | 1 | Low-risk patients | [22] |
| Tadalafil 10 mg (n = 39) | 338 (75) | ||||||||||||||
| Tadalafil 20 mg (n = 37) | 338 (74) | ||||||||||||||
| Tadalafil 40 mg (n = 37) | 352 (78) | ||||||||||||||
| Galie et al. (2008), ARIES-1 | MC, DB | Ambrisentan 5 mg (n = 67) | Placebo (n = 67) | Yes | Yes | Yes | 12 w | 340 (77) | 342 (73) | 3 | 33 | 57 | 7 | Low-risk patients | [23] |
| Ambrisentan 10 mg (n = 68) | 341 (78) | ||||||||||||||
| Galie et al. (2008), ARIES-2 | MC, DB | Ambrisentan 2.5 mg (n = 64) | Placebo (n = 65) | Yes | Yes | Yes | 12 w | 347 (84) | 343 (86) | 2 | 45 | 51 | 2 | Low-risk patients | [23] |
| Ambrisentan 5 mg (n = 63) | 355 (84) | ||||||||||||||
| Galie et al. (2006), BREATHE-5 | MC, DB | Bosentan 125 mg BID (n = 37) | Placebo (n = 17) | Yes | No | Yes | 16 w | 331 (82) | 366 (67) | 0 | 0 | 100 | 0 | Severe patients | [24] |
| Wilkins et al. (2005), SERAPH | SC, DB | Sildenafil 50 mg TID (n = 14) | Bosentan 125 mg BID (n = 12) | Yes | Yes | No | 16 w | 290 (89) | 305 (74) | 0 | 0 | 100 | 0 | Severe patients | [26] |
| Galie et al. (2005), SUPER | MC, DB | Sildenafil 20 mg TID (n = 69) | Placebo (n = 70) | Yes | Yes | No | 12 w | 347 (90) | 344 (79) | 0 | 39 | 58 | 3 | Low-risk patients | [25] |
| Sildenafil 40 mg TID (n = 67) | 345 (77) | ||||||||||||||
| Sildenafil 80 mg TID (n = 71) | 339 (79) | ||||||||||||||
| Barst et al. (2003) | MC, DB | Beraprost 20 μg QID (n = 60) | Placebo (n = 56) | Yes | Yes | Yes | 36 w | 433 (11) | 445 (10) | 0 | 53 | 47 | 0 | Low-risk patients | [28] |
| McLaughlin et al. (2003) | MC, DB | sc. Treprostinil§ (n = 17) | Placebo (n = 9) | Yes | No | Yes | 8 w | 373 (25) | 384 (27) | 0 | 0 | 96 | 4 | Severe patients | [29] |
| Galie et al. (2002), (ALPHABET) | MC, DB | Beraprost 20 μg QID (n = 65) | Placebo (n = 65) | Yes | Yes | No | 12 w | 362 (94) | 383 (93) | 0 | 49 | 51 | 0 | Low-risk patients | [30] |
| Rubin et al. (2002), BREATHE-1 | MC, DB | Bosentan 125 mg BID (n = 74) | Placebo (n = 70) | Yes | Yes | Yes | 16 w | 326 (73) | 344 (76) | 0 | 0 | 92 | 8 | Severe patients | [31] |
| Bosentan 250 mg BID (n = 70) | 333 (75) | ||||||||||||||
| Olschewski et al. (2002), AIR | MC, DB | inh. Iloprost¶ (n = 101) | Placebo (n = 102) | Yes | Yes | Yes | 12 w | 332 (93) | 315 (96) | 0 | 0 | 59 | 41 | Severe patients | [32] |
| Simonneau et al. (2002) | MC, DB | sc. Treprostinil# (n = 233) | Placebo (n = 236) | Yes | Yes | Yes | 12 w | 326 (5) | 327 (6) | 0 | 11 | 82 | 7 | Severe patients | [33] |
| Channick et al. (2001) | MC, DB | Bosentan 125 mg BID (n = 21) | Placebo (n = 11) | Yes | No | No | 16 w | 360 (86) | 355 (82) | 0 | 0 | 100 | 0 | Severe patients | [34] |
| Badesch et al. (2000) | MC, OL | iv. Epoprostenol†† (n = 56) | Placebo (n = 55) | Yes | Yes | No | 12 w | 271 | 240 | 0 | 5 | 78 | 17 | Severe patients | [35] |
| Barst et al. (1996) | MC, OL | iv. Epoprostenol‡‡ (n = 41) | Placebo (n = 40) | Yes | Yes | Yes | 12 w | 316 (18) | 272 (23) | 0 | 0 | 74 | 26 | Severe patients | [36] |
| Rubin et al. (1990) | MC, OL | iv. Epoprostenol§§ (n = 10) | Placebo (n = 9) | Yes | Yes | No | 8 w | 246 | 205 | 0 | 10 | 69 | 21 | Severe patients | [37] |
†
Oral administration, except where noted otherwise.
‡
Doses titrated from 4 ng/kg/min up to a maximum of 100 ng/kg/min weekly.
§
Daily doses titrated from 2.5 ng/kg/min up to a maximum of 20 ng/kg/min.
¶
Doses titrated from 2.5 μg up to a maximum of 5.0 μg; 6- to 9-times per day.
#
Daily doses titrated from 1.25 ng/kg/min up to a maximum of 22.5 ng/kg/min.
††
Daily doses titrated from ≤2 ng/kg/min up to a mean of 11.2 ng/kg/min.
‡‡
Daily doses titrated from 4 ng/kg/min up to a mean of 9.2 ng/kg/min.
§§
Daily doses titrated from 1 ng/kg/min up to a mean of 7.1 ng/kg/min.
¶¶
15% (treatment arm) and 16% (comparator arm) of enrolled patients were on a background therapy (sildenafil).
##
Only data on treatment-naive subgroups of patients are presented here, since these were considered for the NMA.
6MWD: 6-min walking distance; AE: Discontinuation due to adverse event; BID: Two times daily; DB: Double-blind design; iv.: Intravenous; inh.: Inhalation; MC: Multicentre; Mortality: All-cause mortality; NMA: Network meta-analysis; OL: Open label; QID: Four-times daily; sc.: Subcutaneous; SC: Single centre; SD: Standard deviation; TID: Three-times daily; w: Week; WHO FC: WHO functional class.
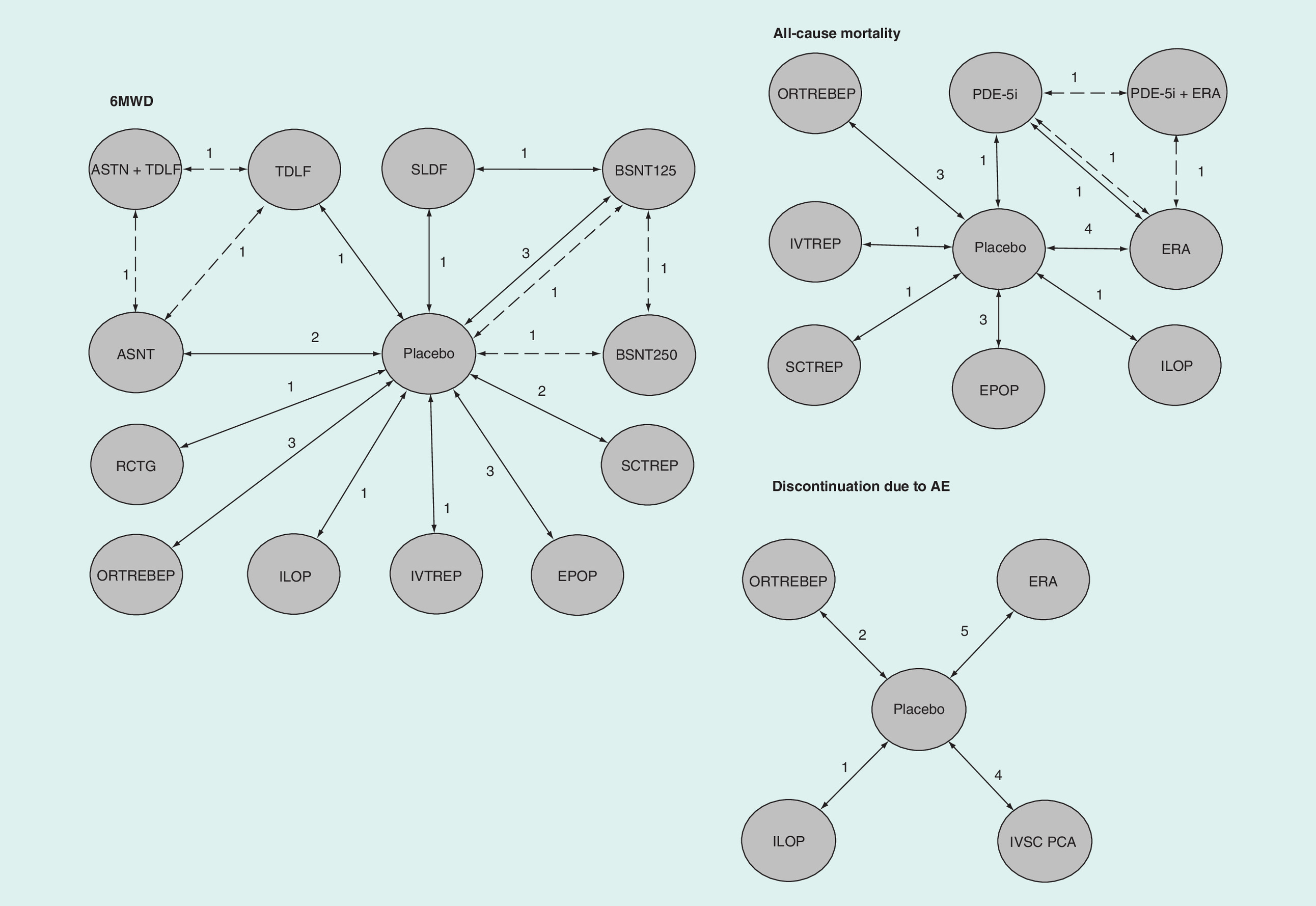
Figure 2. Graphic display of the network for all three outcomes: 6-min walking distance, all-cause mortality and discontinuation due to adverse event.
6MWD: 6-min walking distance; AE: Adverse event; ASNT: Ambrisentan; BSNT125: Bosentan 125 mg dose; BSNT250: Bosentan 250 mg dose; EPOP: Epoprostenol; ERA: Endothelin receptor antagonists ambrisentan 5 mg dose, ambrisentan 10 mg dose, bosentan 125 mg dose or bosentan 250 mg dose; ILOP: Iloprost; IVTREP: Treprostinil, administered iv.; ORTREBEP: Treprostinil or beraprost administered per os; PDE5i: Sildenafil; RCGT: Riociguat; SLDF: Sildenafil; TDLF: Tadalafil 40 mg dose.
Majority of studies reported adequate randomization and allocation concealment. For six RCTs, high risk of bias was evaluated for blinding of participants and personnel or outcome assessment, whereas two RCTs were evaluated as having an unclear risk of bias with respect to blinding of outcome assessment, two studies were exposed to other bias [21,23,28–30,32,35–37]. Three of these RCTs had an open label design (all studies with epoprostenol). Overall, most studies had a low to moderate risk of bias. Summary risk of bias and overall risk of bias are presented in Supplementary Material 1 & 2.
Efficacy outcome 6MWD
The outcome was reported in 21 RCTs with 43 comparisons and nine different PAH-specific drugs with one combination treatment. Initially, different dose or administration of the same drug was considered as a separate intervention. This resulted in 22 different treatments (with placebo), which were analyzed in the full NMA model. Results of this NMA model are presented in the Supplementary Material 3.
The full NMA model was then reduced in terms of number of interventions (treatments) as follows. The lowest dose of ambrisentan (2.5 mg) from the ARIES-2 study did not show statistically significantly better effect than placebo (22.0 m; 95% CrI: -7, 48) and was excluded from further analysis. Additionally, the other ambrisentan study arms (5 and 10 mg doses) were combined into a single ambrisentan treatment as the effect sizes were similar and were not statistically significantly different. Similarly, the sildenafil study arms (20, 40, 50 and 80 mg) were combined into a single sildenafil treatment. However, for tadalafil study arms (2.5, 10, 20 and 40 mg), only the 40 mg study arm was included in further analysis, the other three study arms were excluded. Furthermore, 250 mg dose of bosentan from the BREATHE-1 study showed a better effect than the 125 mg dose of bosentan (48 m; 95% CrI: 24, 72; versus 28 m; 95% CrI: 13, 42, respectively); therefore, these two interventions were analyzed as separate treatments (BSNT125 and BSNT250). Oral formulations of treprostinil and beraprost performed better than placebo. Since effects were very similar (26 m; 95% CrI: 12, 40; and 26 m; 95% CrI: 7.2, 45, respectively) these two drugs were combined into a single intervention (ORTREBEP). Additionally, in the study with intravenous (iv.) treprostinil (or ‘high dose’ treprostinil) an eightfold higher doses of treprostinil at the time of the outcome assessment were used compared with two studies with subcutaneous (sc.) treprostinil (mean dose for iv. treprostinil 72 ng/kg/min compared with 13 and 9 ng/kg/min for sc. treprostinil) [21,29,33]. Consequently, as the bioavailability of iv. and sc. treprostinil is similar, these treatments remained separated.
Following reductions in the number of analyzed treatments as described above, 25 direct comparisons were achieved, incorporating 12 PAH treatments in the final NMA model. Results of the final model are presented in Table 2. Furthermore, the final model presented with lower DIC value and better Dres value compared with the full model, indicating better model fit. The treatment with the lowest mean rank in the final model, in other words, value of 1.9, was a combination of tadalafil and ambrisentan, implicating the highest efficacy, while the treatment with the highest mean rank of 11.9 was sc. treprostinil, implicating the lowest efficacy among PAH treatments. Individual rankings for remaining ten PAH treatments and the results of all mutual comparisons are presented in the Table 2.
| Mean rank (Q1, Q3) | Treatment | Placebo | SCTREP | BSNT125 | ORTREBEP | ILOP | RCGT | TDLF | ASNT | SLDF | BSNT250 | EPOP | IVTREP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1.9 (1, 2) | TDLF + ASNT | 68 (50, 87) | 58 (38, 78) | 43 (19, 65) | 42 (21, 63) | 32 (3.0, 62) | 31 (-0.9, 62) | 26 (12, 39) | 22 (6.7, 37) | 22 (-0.6, 45) | 20 (-8.3, 48) | 11 (-21, 44) | -3.7 (-85, 75) |
| 3.6 (1, 6) | IVTREP | 72 (-2.8, 151) | 62 (-14, 140) | 47 (-28, 128) | 46 (-31, 124) | 36 (-44, 120) | 35 (-44, 116) | 30 (-47, 110) | 26 (-51, 107) | 26 (-50, 105) | 24 (-56, 106) | 15 (-64, 100) | |
| 3.6 (2, 5) | EPOP | 57 (31, 82) | 47 (20, 73) | 32 (1.8, 62) | 31 (2.8, 58) | 21 (-14, 56) | 20 (-17, 57) | 15 (-16, 44) | 11 (-19, 40) | 11 (-18, 39) | 9.0 (-26, 44) | ||
| 5.1 (3, 7) | BSNT250 | 48 (26, 70) | 38 (14, 61) | 23 (0.5, 44) | 22 (-2.6, 47) | 12 (-21, 44) | 11 (-23, 44) | 5.7 (-21, 32) | 1.8 (-25, 28) | 1.8 (-24, 27) | |||
| 5.4 (4, 7) | SLDF | 46 (34, 59) | 36 (22, 51) | 21 (1.8, 40) | 20 (3.2, 37) | 10 (-16, 38) | 9.1 (-18, 38) | 3.9 (-16, 24) | 0.03 (-19, 20) | ||||
| 5.4 (4, 7) | ASNT | 46 (32, 61) | 36 (20, 52) | 21 (-0.1, 42) | 20 (1.9, 38) | 10 (-17, 38) | 9.1 (-20, 38) | 3.9 (-10, 18) | |||||
| 6.4 (5, 8) | TDLF | 43 (28, 58) | 32 (16, 49) | 17 (-3.5, 37) | 16 (-2.0, 35) | 6.4 (-21, 34) | 5.2 (-24, 34) | ||||||
| 7.4 (6, 9) | RCGT | 37 (12, 62) | 27 (0.8, 53) | 12 (-17, 41) | 11 (-16, 38) | 1.2 (-33, 37) | |||||||
| 7.6 (6, 9) | ILOP | 36 (13, 59) | 26 (1.3, 50) | 11 (-17, 38) | 10 (-16, 35) | ||||||||
| 9.8 (9, 11) | ORTREBEP | 26 (15, 37) | 16 (2.5, 29) | 0.7 (-18, 19) | |||||||||
| 9.9 (9, 11) | BSNT125 | 26 (11, 40) | 15 (-1.2, 31) | ||||||||||
| 11.9 (12, 12) | SCTREP | 10 (3.1, 18) |
Treatments in rows are ranked from the best (lowest rank) to the worst. Numbers in bold represent statistically significant differences.
DIC: 355.6; Dres = 43.3; N = 44; tau: 0.19 [0.01, 23]; SD: 2.3 m [0.2, 8.8].
ASNT: Ambrisentan; BSNT125: Bosentan 125 mg dose; BSNT250: Bosentan 250 mg dose; CrI: Credible interval; DIC: Deviance information criterion; Dres: Overall residual deviance; EPOP: Epoprostenol; iv.: Intravenous; ILOP: Iloprost; IVTREP: Treprostinil, administered iv.; ORTREBEP: Treprostinil or beraprost administered per os; N: Number of data points; Q1: First quartile; Q3: Third quartile; RCGT: Riociguat; sc.: Subcutaneous; SCTREP: Treprostinil, administered sc.; SD: Between-trial standard deviation; SLDF: Sildenafil; tau: Between-trial precision (median with 95% CrI); TDLF: Tadalafil 40 mg dose.
All PAH treatments in the final NMA model performed statistically significantly better than placebo except for iv. treprostinil. Similarly, better improvement of the 6MWD mean difference was evident for majority of PAH treatments compared with sc. treprostinil. In addition, combination of tadalafil and ambrisentan performed statistically significantly better than 125 mg bosentan (43 m, 95% CrI: 19, 65), oral treprostinil or beraprost (42 m, 95% CrI: 21, 63), iloprost (32 m, 95% CrI: 3, 62), 40 mg tadalafil (26 m, 95% CrI: 12, 39) and ambrisentan (22 m, 95% CrI: 7, 37). The placebo compared effect size of i.v treprostinil (high dose) is the greatest (72 m, 95% CrI: -3, 151), however, due to a large variability in the estimate (small sample size of TRUST-1 study) the effect is not statistically significant. On the other hand, the mean ranks of epoprostenol and iv. treprostinil were comparable. Epoprostenol performed statistically significantly better than sc. teprostinil (47 m, 95% CrI: 20, 73), 125 mg bosentan (32 m, 95% CrI: 2, 62) and oral treprostinil or beraprost (31 m, 95% CrI: 3, 58). Bosentan 250 mg showed statistically significantly better effect also when compared with 125 mg bosentan (23 m; 95% CrI: 1, 44). The mean ranks and placebo compared effect sizes of 250 mg bosentan, ambrisentan, sildenafil and 40 mg tadalafil were very similar. Based on the final NMA model for 6MWD PAH treatments can be rank ordered as follows: tadalafil and ambrisentan combined > epoprostenol = iv. treprostinil (high dose) >250 mg bosentan = ambrisentan = sildenafil = 40 mg tadalafil > riociguat = iloprost > oral treprostinil or beraprost = 125 mg bosentan > sc. treprostinil (for the eightfold lower dose compared with iv. route of administration).
The network meta-regression model with WHO FC factor as a covariate had lower DIC value (353.3) and lower Dres value (40.3) at 44 data points, which indicates slightly better model fit. The effect of WHO FC factor was estimated at 29 m (95% CrI: 1, 57) for higher FC factor (severe patients) compared with lower WHO FC factor (low-risk patients), indicating that studies with severe patients obtained higher effect size of the PAH treatment over placebo than studies with low-risk patients. Based on network meta-regression model PAH treatments can be rank ordered as follows: tadalafil and ambrisentan combined > ambrisentan = sildenafil = iv. treprostinil (high dose) >40 mg tadalafil = riociguat > epoprostenol = 250 mg bosentan > oral treprostinil or beraprost >125 mg bosentan > iloprost > sc. treprostinil (detailed results not shown).
Efficacy outcome all-cause mortality
The outcome was reported in 16 RCTs that included eight different PAH treatments (no data for riociguat study was obtained). The starting model included the same distribution of PAH treatments as in the final model for the 6MWD outcome. However, in order to achieve the convergence of the NMA model, ambrisentan and bosentan (125 and 250 mg) were combined into a single treatment (ERA), similarly, sildenafil and 40 mg tadalafil were combined into a PDE-5i treatment. In the end, the NMA model included 9 treatments and 18 comparisons (Figure 2). None of the eight PAH treatments showed statistically significant reduction in mortality compared with placebo, however, the marked effect sizes for epoprostenol, ERA, iv. treprostinil (high dose) and iloprost were observed with ORs between 0.21 and 0.26. These four treatments also have similar mean ranks. Besides, the OR for epoprostenol and ERA were borderline significant due to smaller variability of the estimate. Based on NMA model for all-cause mortality, PAH treatments can be rank ordered as follows: epoprostenol = ERA = iv. treprostinil (high dose) = iloprost > PDE-5i and ERA combined = sc. treprostinil = PDE-5i > oral treprostinil or beraprost. Detailed results are presented in Table 3.
| Mean rank (Q1, Q3) | Treatment | Placebo | ORTREBEP | PDE5i | SCTREP | PDE5i + ERA | ILOP | IVTREP | ERA |
|---|---|---|---|---|---|---|---|---|---|
| 2.8 (2, 4) | EPOP | 0.21 (0.03, 1.1) | 0.08 (0.01, 0.9) | 0.17 (0.007, 2.5) | 0.18 (0.007, 3.2) | 0.25 (0.007, 6.0) | 0.8 (0.02, 64) | 0.8 (0.02, 20) | 0.8 (0.06, 8.8) |
| 3.0 (2, 4) | ERA | 0.25 (0.04, 1.2) | 0.10 (0.01, 1.1) | 0.21 (0.019, 1.5) | 0.22 (0.01, 3.8) | 0.31 (0.02, 3.6) | 1.04 (0.03, 71) | 0.97 (0.03, 24) | |
| 3.5 (2, 5) | IVTREP | 0.26 (0.02, 4.4) | 0.10 (0.004, 3.2) | 0.22 (0.005, 7.4) | 0.22 (0.005, 10) | 0.32 (0.006, 17) | 1.1 (0.01, 138) | ||
| 3.5 (1, 5) | ILOP | 0.25 (0.005, 6) | 0.096 (0.001, 4.2) | 0.19 (0.002, 9.4) | 0.21 (0.002, 12) | 0.28 (0.002, 21) | |||
| 5.6 (4, 8) | PDE5i + ERA | 0.8 (0.05, 15) | 0.33 (0.01, 10) | 0.7 (0.1, 6.8) | 0.71 (0.02, 31) | ||||
| 6.3 (5, 8) | SCTREP | 1.16 (0.096, 14) | 0.46 (0.02, 11) | 0.95 (0.03, 25) | |||||
| 6.5 (5, 8) | PDE5i | 1.20 (0.14, 14) | 0.49 (0.03, 11) | ||||||
| 7.8 (7, 9) | ORTREBEP | 2.5 (0.4, 16) |
Treatments in rows are ranked from the best (lowest rank) to the worst. The odds ratios below 1 favor the row-defining treatment. Numbers in bold represent statistically significant differences.
DIC: 143.7; Dres = 34.1; N = 33; tau: 1.1(0.01, 3.6); CV: 0.94 (0.52, 12.6).
CrI: Credible interval; CV: Between-trial coefficient of variation (median with 95% CrI); DIC: Deviance information criterion; Dres: Overall residual deviance; EPOP: Epoprostenol; ERA: Endothelin receptor antagonists ambrisentan 5 mg dose, ambrisentan 10 mg dose, bosentan 125 mg dose or bosentan 250 mg dose; iv.: Intravenous; ILOP: Iloprost; IVTREP: Treprostinil, administered iv.; N: Number of data points; ORTREBEP: Treprostinil or beraprost administered per os; PDE5i: Sildenafil; PDE5i + ERA: Tadalafil 40 mg and ambrisentan 10 mg; Q1: First quartile; Q3: Third quartile; sc.: Subcutaneous; SCTREP: Treprostinil, administered s.c; tau: Between-trial precision (median with 95% CrI).
Discontinuation due to adverse event
The outcome was reported in 12 RCTs with 12 comparisons. For the NMA model, sc. and iv. treprostinil were combined with epoprostenol to parenteral prostacyclin analogs (IV SC PCA), while ambrisentan and bosentan were combined to ERA (Figure 2). As a result, four PAH treatments were compared, namely; parenteral prostacyclin analogs, iloprost, ERA and oral treprostinil or beraprost. None of these results proved to be statistically significant when compared with placebo. Moreover, parenteral prostacyclin analogs as well as oral treprostinil or beraprost showed higher likelihood for treatment discontinuation due to adverse events when compared with placebo. However, iloprost and ERA presented statistically significant lower likelihood for discontinuation due to adverse events when compared with i.v or sc. prostacyclin analogs (median OR for iloprost: 0.05; 95% CrI: 0.003, 0.9; and median OR for ERA: 0.11; 95% CrI: 0.01, 0.8). According to the NMA model, the likelihood for treatment discontinuation due to adverse event can be rank ordered as follows: iloprost = ambrisentan or bosentan < oral treprostinil or beraprost < parenteral prostacyclin analogs. Detailed results are presented in Table 4.
| Mean rank (Q1, Q3) | Treatment | Placebo | IV SC PCA | ERA | ORTREBEP |
|---|---|---|---|---|---|
| 1.5 (1, 2) | ILOP | 0.38 (0.04, 3.6) | 0.05 (0.003, 0.9) | 0.09 (0.004, 1.2) | 0.48 (0.04, 6.0) |
| 2.1 (2, 3) | ERA | 0.80 (0.25, 2.4) | 0.11 (0.01, 0.8) | 0.18 (0.02, 1.1) | |
| 4.3 (4, 5) | ORTREBEP | 4.3 (1.1, 25) | 0.62 (0.07, 7.1) | ||
| 4.6 (4, 5) | IV SC PCA | 7.0 (1.4, 43) |
Treatments in rows are ranked from the best (lowest rank) to the worst. The odds ratios below 1 favor the row-defining treatment. No statistically significant differences were observed.
DIC: 109.9; Dres = 25.8; N = 24; tau: 2.95 (0.001, 3.3); CV: 0.58 (0.55, 32).
Cr: Credible interval; CV: Between-trial coefficient of variation (median with 95% CrI); DIC: Deviance information criterion; Dres: Overall residual deviance; ERA: Endothelin receptor antagonists ambrisentan or bosentan; iv.: Intravenous; ILOP: Iloprost; IV SC PCA: Prostacyclin analogs epoprostenol or treprostinil administered sc. or iv.; N: Number of data points; ORTREBEP: Treprostinil or beraprost administered per os; Q1: First quartile; Q3: Third quartile; sc.: Subcutaneous; tau: Between-trial precision (median with 95% CrI).
Sensitivity analysis on studies with low risk of bias
In total, nine studies with high or unclear risk of bias were excluded [21,23,28–30,32,35–37]. Compared with the final model for 6MWD, three treatments (epoprostenol, iloprost and iv. treprostinil) were omitted and one treatment modified (as studies with beraprost were excluded, ORTREBEP includes oral treprostinil only). The reduced model had a lower value of DIC (200.9), and Dres value of 27.3 at 26 data points which indicates poorer model fit. Based on the reduced model PAH treatments can be rank ordered as follows: tadalafil and ambrisentan combined >250 mg bosentan = sildenafil = ambrisentan >40 mg tadalafil = riociguat > oral treprostinil = 125 mg bosentan > sc. treprostinil. Compared with the final NMA model the reduced model presented similar rankings and effect on mean differences was negligible (detailed results not shown).
Same approach was taken for the outcome mortality. Following the exclusion of four PAH treatments (iv. treprostinil, iloprost, epoprostenol and beraprost), only nine studies with six treatments (ERA, PDE-5i, combination of PDE-5i and ERA, sc. treprostinil, oral treprostinil and placebo) were considered for the analysis. This led to reduced heterogeneity (0.45; 95% CrI: 0.0008, 3.5), and reduced values of DIC (81.3) and Dres (18.5 at 19 data points), indicating better model fit. Similarly, as for the outcome 6MWD, the reduced model for the outcome mortality presented comparable rankings and effect size as in original NMA but with fewer treatment options (detailed results not shown).
For the outcome discontinuation due to adverse events, the original NMA was modified by reducing the number of studies (from 12 to 6). After exclusion of PAH treatments such as are iloprost, beraprost and iv. treprostinil, three PAH treatments were considered for the NMA model: sc. treprostinil, oral treprostinil and ERA (ambrisentan or bosentan). The NMA model could not generate successful convergence of parameters for the full 100,000 iterations.
Study consistency & heterogeneity
Treatment estimates from direct and indirect evidence on 6MWD did not show loop-specific inconsistency. A 95% CI for the inconsistency estimate on 6MWD overlapped with 0 value suggested that there was no statistically significant evidence of different direct and indirect treatment effects. Similarly, was suggested for the inconsistency estimate on all-cause mortality. Nonetheless, wide CIs were indicative of lower power to observe evidence of heterogeneity. Data are presented in Supplementary Material 4 & 5.
The network for 6MWD indicated the presence of low heterogeneity standard deviation for between trial effect size was only 2.3 m, whereas networks for discontinuation due to adverse event and all-cause mortality showed moderate to high heterogeneity, in other words, coefficient of variation for between trial effect size was 0.58 and 0.94, respectively.
Discussion
Recently published meta-analyses have compared directly or indirectly the efficacy and/or safety of two or more drug agents within the same class or between classes, or compared monotherapy versus combination (background) therapy, but none of these have focused solely on patients who have never undergone a PAH-specific drug therapy [6–11,38]. In addition, we have evaluated the influence of different doses of PAH specific drugs and WHO FC classifications on treatment comparisons, which was not addressed in other meta-analyses. Based on prior research of direct and indirect evidence, this NMA compared PAH-specific drug therapies for efficacy and safety in 21 RCTs with 3.713 enrolled treatment-naive patients. We obtained ranking probabilities for nine drug agents of different strengths and formulations (beraprost, epoprostenol, treprostinil, iloprost, ambrisentan, bosentan, sildenafil, tadalafil and riociguat) for outcomes 6MWD, all-cause mortality and discontinuation due to adverse event. These results suggested that combination of tadalafil (40 mg) and ambrisentan (10 mg) proved to have a greater impact on the outcome of 6MWD over compared treatments, followed by epoprostenol and iv. treprostinil (high dose) although the estimate of effect size of treprostinil was very uncertain. In view of the predefined increase of ≥33 meters in 6MWD from baseline characterizing a minimal clinically important difference, associated with lower mortality and improved functional status, combination of tadalafil and ambrisentan, epoprostenol, treprostinil (high dose), bosentan (250 mg dose), sildenafil, ambrisentan, tadalafil, riociguat and iloprost have demonstrated such improvement of 6MWD when compared with placebo [39]. However, differences between these treatments cannot be considered as clinically significant.
With the availability of therapies that target multiple pathogenic pathways, and by considering patient's level of risk, combination therapy should be offered to all PAH patients [1,40]. However, with exception of the AMBITION trial, data on direct comparisons of combination therapy and monotherapy, initiated in newly diagnosed patients is lacking. For this reason, presented NMAs give a limited insight into comparison of the combination therapy against monotherapies in newly diagnosed patients. Even though real-world data also support initiation of therapy with combination of ERA and a PDE-5i proving to be associated with significant improvements in WHO FC, exercise capacity and hemodynamics; such fact raises a question whether and to what extent an initiation of a monotherapy is still substantial [40]. Initiation of monotherapy may be suitable for patients in the low risk category (treatment-naive patients with WHO FC II symptoms), particularly if the use of an ERA or a PDE-5i/soluble guanylate cyclase stimulator is contraindicated or is not tolerated [5,41]. Regardless of these facts, epoprostenol is the only therapy with class I recommendation and highest evidence level for patients in WHO FC IV; but the prostacyclin pathway may also be targeted with other oral prostacyclin analogs in patients with WHO FC II and III [1].
Other prostacyclin analogs included in our NMA were beraprost and treprostinil, and oral formulations of both were considered as equivalent in terms of effect size in relation to 6MWD. Because of up to eightfold difference (72 ng/kg/min vs 13 or 9 ng/kg/min) between mean doses at the time of outcome assessment in the RCTs, two separate treatments of parenteral formulation of treprostinil (per sc. or iv. route of administration) were considered in the conducted NMAs. This approach was not applied for epoprostenol, since differences of the mean doses from the applicable RCTs were minor (11, 9.2 and 7.1 ng/kg/min) [35–37]. However, among these parenteral PAH-specific drugs, iv. treprostinil demonstrated the greatest effect size on the 6MWD, however, this estimate was not proved to be statistically significant from placebo due to a small sample size. On the contrary, RCTs evaluating sc. treprostinil enrolled a greater sample of severely ill patients, but the effect on the 6MWD proved to be smallest, which is most likely associated with higher average baseline values of 6MWD in treatment arms (326 and 373 m) and lower mean doses of treprostinil administered via sc. route compared with iv. route [29,33]. In addition, RCTs evaluating efficacy of iv. treprostinil or epoprostenol also enrolled severely ill treatment-naive patients categorized to WHO FC III or IV, who have demonstrated the mean baseline values of 6MWD from approximately 250 m up to 316 m, and thus allowing a greater improvement of walked distance [21,36]. This is also supported by our meta-regression NMA, which indicates that studies with severe patients obtained higher effect size of the PAH treatment over placebo than studies with low-risk patients. Consequently, as the study with 250 mg bosentan included severe patients, the significant difference in the effect size of 250 mg dose versus 125 mg bosentan dose was diminished in results from the meta-regression NMA. Similarly, the estimate of effect size of epoprostenol, assessed on studies with severe patients only, was smaller in the meta-regression NMA.
Our NMA demonstrated that epoprostenol, ERA, iv. treprostinil (high dose) and iloprost having favorable and comparable effect size on outcome mortality in newly diagnosed patients, but statistically nonsignificant. Similar findings were reported in recent NMAs by Gao et al. and Jain et al., who did not observe significant differences in mortality between prostanoids, ERAs or PDE-5is, its combination and placebo regardless of drug dosage forms and existing PAH-specific drug therapy at the time of enrollment [9,10].
Higher risk of withdrawal with prostacyclin analogs when compared with ERA and placebo was observed by Lin et al., but these differences were not statistically significant [38]. Similar is demonstrated by the NMA, where IVSC PCA (epoprostenol or treprostinil, administered iv. or sc.) indicated higher likelihood for the outcome discontinuation due to adverse event. Nonetheless, data on frequency of events as are death and discontinuation due to adverse events are available from RCTs of PAH-specific drugs on a small population sample of patients, who were observed for a short period of time. Hence, the appropriate estimation of drug effect on disease progression or death is not plausible.
Clinical trials in PAH have historically implemented the 6MWD as the primary outcome measure and a surrogate endpoint representing the true response to targeted drug therapies in patients with PAH, particularly pivotal trials of an older date [26,31,33,35–37]. Although baseline 6MWD has a good selective capacity to prognosticate patients at the time of diagnosis, its utility as a primary end point has been challenged in recent years, since it has not proved to be a suitable indicator of long-term prognosis with treatment [42]. Pharmacological approach of disease management temporary improves clinical signs, delays disease progression, but eventually a great number of patients suffer from right heart failure and death [43]. Beforetime patient’s health-related quality of life is already affected by possible adverse reactions caused by PAH-specific drug therapy, especially if the patient is administered drugs via parenteral route [44]. Among other goals are improvement of functional class and 6MWD to more than 440 m, PAH treatment goals include preventing disease progression, increasing patient survival and improving health-related quality of life [1,45]. Gabler et al., and the outcomes of ten RCTs revealed that significant threshold effect in decreasing the incidence of clinical events is 41.8 m [46]. This NMA demonstrates that ambrisentan in combination with tadalafil, or monotherapies with bosentan 250 mg, or sildenafil or ambrisentan could affect treatment-naive patients in such manner.
Study limitations
Our findings are limited, because data on direct comparisons of combination therapy and monotherapy, initiated in newly diagnosed patients is lacking. Second, the scope of studies from 20 years ago was less complex with respect to studied endpoints. We have therefore chosen the most common endpoints with aim to include the maximum number of RCTs into the NMA. Third, the lack of reporting on mortality and treatment discontinuation outcomes from RCTs included in our NMAs led to insufficient dataset, affecting comparisons of all doses and treatments studied in the selected RTCs. Moreover, for this reason we failed to show statistically significant results of otherwise large effect sizes of tested treatments compared with placebo. In addition, patient sample sizes from included RTCs differentiated across treatment and comparator arms, resulting in comparisons of different proportions and leading to increased uncertainty of the effect sizes. While meta-analysis assumes that included RCTs were sufficiently similar in most respects other than the treatments under this NMA, statistical assessment of this assumption was limited by low power, although little evidence of network inconsistency was found. In addition, study designs, patients’ etiology, demographics and follow-up duration remained unclarified in our NMA. Furthermore, RCTs from 20 years ago included patients classified as WHO FC III or IV, whereas studies of a more recent date included patients where a vast majority of them was classified as WHO FC II or III. However, this was partly addressed using network meta-regression model. At last, to expand our NMA with data on use of macitentan and selexipag in treatment-naive patients, and to confirm our results, particularly regarding the influence of the dose, treatment administration and WHO FC classification on the treatment comparisons, a meta-analysis from a patient-level would be of a great value.
Conclusion & relevance
A Bayesian NMA on efficacy of PAH-specific drug therapies for use in treatment-naive patients demonstrated that the combination of ambrisentan and tadalafil had the greatest improvement of 6MWD, followed by epoprostenol and high doses of parenteral treprostinil. None of treatment comparisons demonstrated significant difference on mortality or discontinuation due to adverse event. Furthermore, among PAH-specific oral drug monotherapies evaluated in this NMA, bosentan (250 mg dose), ambrisentan, sildenafil and tadalafil (40 mg dose) had the greatest effect on the 6MWD, followed by riociguat. Our findings are limited, because data on direct comparisons of combination therapy and monotherapy is lacking and further studies in this field are warranted.
•
No meta-analysis for direct and indirect comparisons has been conducted to study efficacy of drug-therapies specific for treatment of pulmonary arterial hypertension (PAH) in newly diagnosed patients only. In addition, we have evaluated the influence of different doses of PAH-specific drugs and WHO functional class classifications on treatment comparisons.
•
For the purpose of this systematic review of randomized controlled trials (RCT), a Bayesian network meta-analysis model was developed to assess the comparative efficacy of drug therapies specific for PAH in treatment-naive patients.
•
The 6-min walking distance and all-cause mortality were efficacy outcomes whereas discontinuation due to adverse events was a safety-related outcome.
•
This report describes 21 RCTs which were retrieved for data extraction with 3.713 treatment-naive patients included in the analysis.
•
Combination of ambrisentan and tadalafil demonstrated greatest improvement of 6-min walking distance among other treatment comparisons, followed by epoprostenol and intravenous treprostinil (high dose).
•
None of treatment comparisons showed significant association with outcomes mortality or discontinuation due to adverse events.
•
Data on direct head-to-head comparisons of monotherapies and combination therapies in newly diagnosed patients is limited, requiring further comparative efficacy trials.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Financial & competing interests disclosure
M Petrovič is an employee of Krka, d.d., Novo mesto, Slovenia, and is a PhD student at the University of Ljubljana, Faculty of Pharmacy. I Locatelli is an employee of University of Ljubljana, Faculty of Pharmacy, the Department of Social Pharmacy, where acting as university teacher. I Locatelli reports personal fees from Astra Zeneca, personal fees from Forum of International Research and Development Pharmaceutical Companies, EIG, Slovenia, outside the submitted work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_file.docx)
- Download
- 445.47 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Galie N, Humbert M, Vachiery JL et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 37(1), 67–119 (2016).
•• Guidelines summarize and evaluate all available evidence on pulmonary hypertension, with the aim of assisting health professionals in selecting the best management strategies for an individual patient with pulmonary hypertension. Guidelines represent the official position of the European Society of Cardiology.
2.
Benza RL, Miller DP, Gomberg-Maitland M et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation 122(2), 164–172 (2010).
3.
Sitbon O, Channick R, Chin KM et al. Selexipag for the treatment of pulmonary arterial hypertension. N. Engl. J. Med. 373(26), 2522–2533 (2015).
4.
Ghofrani HA, Galie N, Grimminger F et al. Riociguat for the treatment of pulmonary arterial hypertension. N. Engl. J. Med. 369(4), 330–340 (2013).
5.
Taichman DB, Ornelas J, Chung L et al. Pharmacologic therapy for pulmonary arterial hypertension in adults: CHEST guideline and expert panel report. Chest 146(2), 449–475 (2014).
•• The guideline was supported by American College of Chest Physicians and provides clinicians advice regarding pharmacology therapy for adult patients with pulmonary arterial hypertension (PAH) according to available evidence.
6.
Coeytaux RR, Schmit KM, Kraft BD et al. Comparative effectiveness and safety of drug therapy for pulmonary arterial hypertension: a systematic review and meta-analysis. Chest 145(5), 1055–1063 (2014).
7.
Duo-Ji MM, Long ZW. Comparative efficacy and acceptability of endothelin receptor antagonists for pulmonary arterial hypertension: a network meta-analysis. Int. J. Cardiol. 234, 90–98 (2017).
8.
Fox BD, Shtraichman O, Langleben D, Shimony A, Kramer MR. Combination therapy for pulmonary arterial hypertension: a systematic review and meta-analysis. Can. J. Cardiol. 32(12), 1520–1530 (2016).
9.
Gao XF, Zhang JJ, Jiang XM et al. Targeted drugs for pulmonary arterial hypertension: a network meta-analysis of 32 randomized clinical trials. Patient Prefer. Adherence 11, 871–885 (2017).
10.
Jain S, Khera R, Girotra S et al. Comparative effectiveness of pharmacologic interventions for pulmonary arterial hypertension: a systematic review and network meta-analysis. Chest 151(1), 90–105 (2017).
• A recent and extensive network meta-analysis evaluating comparative efficacy and safety PAH-specific therapies in patients with PAH.
11.
Lajoie AC, Lauziere G, Lega JC et al. Combination therapy versus monotherapy for pulmonary arterial hypertension: a meta-analysis. Lancet Respir. Med. 4(4), 291–305 (2016).
• Compares efficacy of combination of PAH-specific therapies with monotherapies using the Mantel–Haenszel method.
12.
Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011] (2008). https://training.cochrane.org/handbook/archive/v5.1/
13.
Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 23(20), 3105–3124 (2004).
• Addresses issues and assumptions underlying modeling of mixed treatment comparisons, and the role of Bayesian deviance analysis.
14.
Sutton A, Ades AE, Cooper N, Abrams K. Use of indirect and mixed treatment comparisons for technology assessment. Pharmacoeconomics 26(9), 753–767 (2008).
• Reviews pair-wise meta-analysis and indirect and mixed treatment comparison approaches to synthesis, clearly outlining the assumptions involved in each approach.
15.
Jonas DE, Wilkins TM, Bangdiwala S et al. Findings of Bayesian Mixed Treatment Comparison Meta-Analyses: Comparison and Exploration Using Real-World Trial Data and Simulation. MD, USA (2013). www.effectivehealthcare.ahrq.gov/reports/final.cfm
16.
Spiegelhalter DJ, Best NG, Carlin BP, Van Der Linde A. Bayesian measures of model complexity and fit. J. R. Stat. Soc. Series B Stat. Methodol. 64(4), 583–639 (2002).
17.
Jansen JP, Cope S. Meta-regression models to address heterogeneity and inconsistency in network meta-analysis of survival outcomes. BMC Med. Res. Methodol. 12, 152 (2012).
18.
Dias S, Welton NJ, Caldwell DM, Ades AE. Checking consistency in mixed treatment comparison meta-analysis. Stat. Med. 29(7–8), 932–944 (2010).
19.
Galie N, Barbera JA, Frost AE et al. Initial use of ambrisentan plus tadalafil in pulmonary arterial hypertension. N. Engl. J. Med. 373(9), 834–844 (2015).
20.
Jing ZC, Parikh K, Pulido T et al. Efficacy and safety of oral treprostinil monotherapy for the treatment of pulmonary arterial hypertension: a randomized, controlled trial. Circulation 127(5), 624–633 (2013).
21.
Hiremath J, Thanikachalam S, Parikh K et al. Exercise improvement and plasma biomarker changes with intravenous treprostinil therapy for pulmonary arterial hypertension: a placebo-controlled trial. J. Heart Lung Transpl. 29(2), 137–149 (2010).
22.
Galie N, Rubin L, Hoeper M et al. Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet 371(9630), 2093–2100 (2008).
23.
Galie N, Brundage BH, Ghofrani HA et al. Tadalafil therapy for pulmonary arterial hypertension. Circulation 119(22), 2894–2903 (2009).
24.
Galie N, Olschewski H, Oudiz RJ et al. Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation 117(23), 3010–3019 (2008).
25.
Galie N, Beghetti M, Gatzoulis MA et al. Bosentan therapy in patients with Eisenmenger syndrome: a multicenter, double-blind, randomized, placebo-controlled study. Circulation 114(1), 48–54 (2006).
26.
Galie N, Ghofrani HA, Torbicki A et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N. Engl. J. Med. 353(20), 2148–2157 (2005).
27.
Wilkins MR, Paul GA, Strange JW et al. Sildenafil versus endothelin receptor antagonist for pulmonary hypertension (SERAPH) study. Am. J. Respir. Crit. Care Med. 171(11), 1292–1297 (2005).
28.
Barst RJ, Mcgoon M, Mclaughlin V et al. Beraprost therapy for pulmonary arterial hypertension. J. Am. Coll. Cardiol. 41(12), 2119–2125 (2003).
29.
Mclaughlin VV, Gaine SP, Barst RJ et al. Efficacy and safety of treprostinil: an epoprostenol analog for primary pulmonary hypertension. J. Cardiovasc. Pharmacol. 41(2), 293–299 (2003).
30.
Galie N, Humbert M, Vachiery JL et al. Effects of beraprost sodium, an oral prostacyclin analogue, in patients with pulmonary arterial hypertension: a randomized, double-blind, placebo-controlled trial. J. Am. Coll. Cardiol. 39(9), 1496–1502 (2002).
31.
Rubin LJ, Badesch DB, Barst RJ et al. Bosentan therapy for pulmonary arterial hypertension. N. Engl. J. Med. 346(12), 896–903 (2002).
32.
Olschewski H, Simonneau G, Galie N et al. Inhaled iloprost for severe pulmonary hypertension. N. Engl. J. Med. 347(5), 322–329 (2002).
33.
Simonneau G, Barst RJ, Galie N et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am. J. Respir. Crit. Care Med. 165(6), 800–804 (2002).
34.
Channick RN, Simonneau G, Sitbon O et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 358(9288), 1119–1123 (2001).
35.
Badesch DB, Tapson VF, Mcgoon MD et al. Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Ann. Intern. Med. 132(6), 425–434 (2000).
36.
Barst RJ, Rubin LJ, Long WA et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N. Engl. J. Med. 334(5), 296–301 (1996).
37.
Rubin LJ, Mendoza J, Hood M et al. Treatment of primary pulmonary hypertension with continuous intravenous prostacyclin (epoprostenol). Results of a randomized trial. Ann. Intern. Med. 112(7), 485–491 (1990).
38.
Lin H, Wang M, Yu Y et al. Efficacy and tolerability of pharmacological interventions for pulmonary arterial hypertension: a network meta-analysis. Pulmon. Pharmacol. Ther. 50, 1–10 (2018).
39.
Mathai SC, Puhan MA, Lam D, Wise RA. The minimal important difference in the 6-minute walk test for patients with pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 186(5), 428–433 (2012).
40.
Sitbon O, Gaine S. Beyond a single pathway: combination therapy in pulmonary arterial hypertension. Eur. Respir. Rev. 25(142), 408–417 (2016).
41.
Gaine S, Mclaughlin V. Pulmonary arterial hypertension: tailoring treatment to risk in the current era. Eur. Respir. Rev. 26(146), 170095 (2017).
42.
Savarese G, Paolillo S, Costanzo P et al. Do changes of 6-minute walk distance predict clinical events in patients with pulmonary arterial hypertension?: A meta-analysis of 22 randomized trials. J. Am. Coll. Cardiol. 60(13), 1192–1201 (2012).
43.
Tonelli AR, Arelli V, Minai OA et al. Causes and circumstances of death in pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 188(3), 365–369 (2013).
44.
Rival G, Lacasse Y, Martin S, Bonnet S, Provencher S. Effect of pulmonary arterial hypertension-specific therapies on health-related quality of life: a systematic review. Chest 146(3), 686–708 (2014).
45.
Mclaughlin VV, Archer SL, Badesch DB et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J. Am. Coll. Cardiol. 53(17), 1573–1619 (2009).
46.
Gabler NB, French B, Strom BL et al. Validation of 6-minute walk distance as a surrogate end point in pulmonary arterial hypertension trials. Circulation 126(3), 349–356 (2012).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 16 July 2019
Accepted: 15 October 2019
Published online: 17 December 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of pulmonary arterial hypertension drugs in treatment-naive patients: a network meta-analysis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0037
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hongmei Li, Xiaojun He, Cui Chen, Qiao Ni, Linghao Ni, Jiawei Zhou, Bin Peng, Causal Inference of Adverse Drug Events in Pulmonary Arterial Hypertension: A Pharmacovigilance Study, Pharmaceuticals, 10.3390/ph18081084, 18, 8, (1084), (2025).
- Cheng-Yu Tsai, Chuan-Wei Shen, Hsuan-Lin Lai, Chung-Yu Chen, Adherence and treatment patterns of disease-specific drugs among patients with pulmonary arterial hypertension: A nationwide, new-user cohort study, Frontiers in Pharmacology, 10.3389/fphar.2022.1030693, 13, (2023).
- Ralf Ewert, Dirk Habedank, Michael Halank, Beate Stubbe, Christian F. Opitz, Strategies for optimizing intravenous prostacyclin-analog therapy in patients with pulmonary arterial hypertension, Expert Review of Respiratory Medicine, 10.1080/17476348.2022.2011220, 16, 1, (57-66), (2021).
- Wenhai Fu, Wenjun He, Yuexin Li, Yangxiao Chen, Jingyi Liang, Hui Lei, Lin Fu, Yanghang Chen, Ni Ren, Qian Jiang, Yi Shen, Ran Ma, Tao Wang, Xinni Wang, Nuofu Zhang, Dakai Xiao, Chunli Liu, Efficacy and safety of novel-targeted drugs in the treatment of pulmonary arterial hypertension: a Bayesian network meta-analysis, Drug Delivery, 10.1080/10717544.2021.1927243, 28, 1, (1007-1019), (2021).
- Max Schlueter, Amélie Beaudet, Evan Davies, Binu Gurung, Andreas Karabis, Evidence synthesis in pulmonary arterial hypertension: a systematic review and critical appraisal, BMC Pulmonary Medicine, 10.1186/s12890-020-01241-4, 20, 1, (2020).
- Laura Dormer, Introducing Volume 9 of the Journal of Comparative Effectiveness Research , Journal of Comparative Effectiveness Research, 10.2217/cer-2019-0160, 9, 1, (1-5), (2019).