Minimally invasive surgery for degenerative spondylolisthesis: transforaminal or oblique lumbar interbody fusion
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the outcomes of minimally invasive surgery (MIS) for degenerative spondylolisthesis transforaminal lumbar interbody fusion (TLIF) and oblique lumbar interbody fusion (OLIF). Materials & methods: The clinical and surgical characteristics and outcomes of 38 patients with MIS–OLIF and 55 with MIS–TLIF were retrospectively evaluated. Results: Procedures and hospital stay were shorter and blood loss was less, with MIS–OLIF than with MIS–OLIF. The clinical and radiographic outcomes were similar. Postoperative changes in disk height and foraminal dimension were greater and patient satisfaction was better with MIS–OLIF than with MIS–TLIF. Conclusion: The clinical findings associated with the two procedures were similar; but patients preferred MIS–OLIF, which is less invasive, to MIS–TLIF. Clinical trial registration number: ChiCTR1800019443.
The prevalence of degenerative spondylolisthesis (DSL) in the general population has been estimated at 5–7% [1]. It leads to failure of the stabilizing system of the functional spinal unit [2]. The treatment options include nonpharmacological conservative treatment, pharmacotherapy and surgery. The choice of surgical treatment may be complicated by having to choose among the available intersomatic arthrodesis procedures [3–6]. Minimally invasive transforaminal lumbar interbody fusion (TLIF), anterior lumbar interbody fusion (ALIF), transpsoas lateral lumbar interbody fusion and oblique lumbar interbody fusion (OLIF) are available and widely used for the treatment of DSL [5,7–20]. Each of the four procedures have advantages. Previous studies have compared the clinical and radiographic outcomes of minimally invasive surgery (MIS)–OLIF and MIS–ALIF [21–23], MIS–TLIF and MIS–ALIF [24,25]. Few studies in addition to this one have compared the clinical and radiographic outcomes of MIS–TLIF and MIS–OLIF for the treatment of DSL and evaluated the comparative effectiveness.
Methods
A total of 202 patients with DSL and treated between October 2014 and July 2018 were enrolled and evaluated retrospectively. Four senior chief physicians performed the surgical treatment. Sixty-eight patients were treated with MIS–OLIF (OLIF with posterior bilateral percutaneous pedicle screws) and 134 were treated with MIS–TLIF. The inclusion criteria were DSL at L1–L5, at least 18 years of age, presentation with symptomatic Grade I or II DSL at one or two contiguous lumbar levels, and 12-months follow-up. Baseline data collection included demographics and diagnosis. Patients with previous lumbar fusion surgery, spinal metastases or active spinal tumor malignancy, rheumatoid arthritis or other autoimmune disease, or incomplete follow-up were excluded. Treatment data included the procedure performed, procedure time (including repositioning time), estimated blood loss and length of postoperative hospital stay. Activity levels were collected by patient-completed questionnaires administered preoperatively and postoperatively at 6, 12 and 24 weeks, and 12 months. Patient-reported outcomes were collected at baseline and at each postoperative visit and included the Oswestry Disability Index (ODI), visual analog score (VAS) and patient satisfaction with their outcome. Very satisfied and partially satisfied patients were considered satisfied; very dissatisfied and partially dissatisfied patients were considered dissatisfied. Patients were asked of their willingness to repeat the same surgery with advance knowledge of the clinical outcome. Totally or partially willing patients were considered willing. Totally or partially unwilling patients were considered unwilling [24]. Neurological assessment of motor and sensory function was performed preoperatively and at each postoperative evaluation using a modified American Spinal Injury Association scale. Evidence of restoration, alignment and indirect decompression was collected by radiographs and magnetic resonance imaging at 24 weeks postoperatively (Figure 1). Each measurement was repeated three-times by two independent observers; the mean values were recorded. To reduce error in the estimated size of the intervertebral foramen, differences of the preoperative and postoperative radiographic measurements were divided by the preoperative value (as measurement data).

Figure 1. Representative radiographs and magnetic resonance images.
(A) Dis angle; (B) dis height; (C) L1-S1 lordosis; (D) foraminal dimension, area; (E) foraminal dimension, height.
Statistical analysis
Statistical analysis was performed with SPSS 20.0. Descriptive statistics were calculated and comparative analysis of the MIS–OLIF and MIS–TLIF outcomes was performed using Fisher’s exact test and analysis of variance. Paired testing was used to compare the preoperative and postoperative values of the patient variables in the two treatment groups. Statistical significance was defined as p < 0.05.
Results
The patient characteristics and treatment outcomes are shown in Table 1. A total of 44 MIS–OLIF levels were treated in the 38 enrolled patients; 32 were single-level and six were two-level cases. Fifty-nine MIS–TLIF levels were treated in 55 patients; 51 were single-level and four were two-level cases. All the patients had DSL with one or more forms of stenosis. Cage height in the MIS–TLIF procedures was 10–12 mm; the width was 25–30 mm. Cage height and width in the MIS–OLIF procedures were 12–14 and 45–55 mm. All cages were from Medtronic Sofamor. There the proportions of patients diagnosed with central, foraminal, of subarticular stenoses in the MIS–OLIF and MIS–TLIF groups were not significantly different. Blood loss, procedure time and hospital stay were all significantly less in the MIS–OLIF than in the MIS–TLIF group (p < 0.001). Although the 9-min difference in procedure time was statistically significant, it was not clinically relevant. Procedure-related adverse events included postoperative hip flexion weakness, distal weakness and sensory deficit, and the occurrence was similar in the MIS–OLIF and MIS–TLIF groups. Two patients in the OLIF group experienced hip flexion weakness and one patient experienced sensory deficit that fully resolved by 24 weeks postoperatively. Two patients in the MIS–TLIF group, experienced hip flexion weakness, one experienced distal weakness and two experienced sensory deficit. All the adverse events resolved by 12 months postoperatively. All clinical symptoms, (e.g., back pain, leg pain and OD) were significantly improved in both treatment groups at 12 months after surgery (p < 0.05) and the between-group differences were not significant (Figure 2). The radiographic outcomes are shown in Table 2. The mean operative level disk height and foraminal dimension were greater in the MIS–OLIF than in the MIS–group. The disk angle and lumbar lordosis (L1–S1 angle) were in the two groups were similar. At 6 weeks after surgery, the patient satisfaction and willingness to undergo the same procedure differed significantly, with patients preferring MIS–OLIF to MIS–TLIF.
| Treatment characteristics | OLIF (38) | MIS–TLIF (55) | t | p-value |
|---|---|---|---|---|
| Age (years) | 65.29 ± 8.88 | 60.62 ± 12.37 | 2.12 | 0.037 |
| Female | 78% | 54% | 6.866 | 0.006 |
| N levels treated | 2 level:6 | 2 level:4 | 0.307 | 0.168 |
| 1 levels:32 | 1 levels:51 | |||
| Mean procedure time (min) | 90.79 ± 7.93 | 100.2 ± 14.95 | 3.935 | 0.000 |
| Mean hospital stay (day) | 5.21 ± 1.26 | 7.22 ± 1.58 | 6.523 | 0.000 |
| Blood loss (ml) | 63.95 ± 23.31 | 186.36 ± 80.19 | 10.686 | 0.000 |
| Diagnoses | ||||
| Central stenosis | 22 | 17 | 2.561 | 0.278 |
| Foraminal stenosis | 12 | 20 | ||
| Subarticular stenosis | 10 | 12 | ||
| Hip flexion weakness | 1 | 2 | 1.000 | 0.637 |
| Distal motor weakness | 0 | 1 | 1.000 | 0.591 |
| Sensory deficit (neural) | 1 | 2 | 1.000 | 0.637 |
| Patient satisfaction | 38 | 38 | 14.373 | 0.000 |
| Willingness to repeat | 38 | 34 | 18.741 | 0.000 |
MIS: Minimally invasive surgery; OLIF: Oblique lumbar interbody fusion; TLIF: transforaminal lumbar interbody fusion.
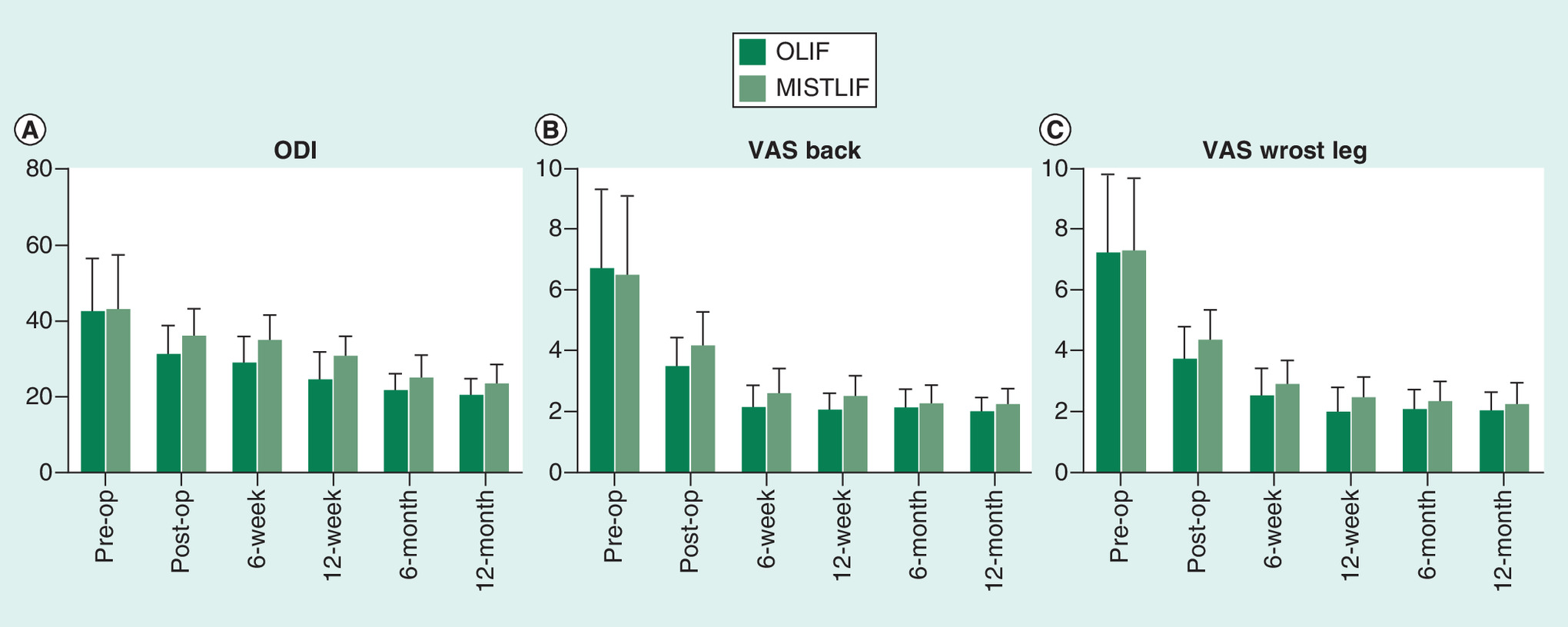
Figure 2. Graphs showing changes over time between the minimally invasive surgery–transforaminal lumbar interbody fusion and OLIF groups.
Both groups experienced significant improvements (p < 0.05) from baseline to last follow-up and there were no statistically significant differences between the groups (p > 0.05).
MIS: Minimally invasive surgery; ODI: Oswestry disability index; OLIF: Oblique lumbar interbody fusion; TLIF: transforaminal lumbar interbody fusion; VAS: Visual analog score.
| Radiographic measures | MIS–TLIF (32) | OLIF (20) | t | p-value |
|---|---|---|---|---|
| Dis angle | 0.93 ± 1.59 | 1.55 ± 3.44 | 0.877 | 0.385 |
| L1-S1 lordosis | 0.05 ± 0.19 | 0.05 ± 0.21 | 0.148 | 0.883 |
| Foraminal dimensions height | 0.06 ± 0.25 | 0.16 ± 0.21 | 3.763 | 0.00 |
| Foraminal dimensions area | 0.33 ± 0.23 | 0.59 ± 0.37 | 2.866 | 0.007 |
| Dis height | 0.13 ± 0.27 | 0.31 ± 0.57 | 2.939 | 0.009* |
MIS: Minimally invasive surgery; OLIF: Oblique lumbar interbody fusion; TLIF: transforaminal lumbar interbody fusion.
Discussion
Previous studies have found that lumbar arthrodesis for the treatment of spondylolisthesis was associated with increased complication rates and that nerve root injury and postoperative nerve adhesions could not be completely prevented [4,26]. OLIF, which involves an oblique channel between the prevertebral venous structures and the psoas muscle was first reported in 2012 [27,28]. In this study, the mean operative blood loss during OLIF was 64 ml, which was similar to that reported by Silvestre [27]. Consistent with previous studies, the mean operative blood loss in MIS–OLIF was less that reported in MIS–TLIF, and can be attributed to indirect decompression and not entering the spinal canal [10,20,29]. Hospital stay was shorter in OLIF than in MIS–TLIF patients because complete resection of the paraspinal and psoas muscles can be achieved in OLIF without disturbing the articular process and allowing more rapid resumption of activity [13]. Restoring sagittal balance and correcting lumbar lordosis are essential for the treatment of lumbar fusion and depend on recovery disk height and angle lumbar lordosis [22,30]. Some studies reported that MIS–TLIF was not effective for the correction of lumbar lordosis, others found that the effect of TLIF on lordosis depended on the degree of shortening of the posterior column [11,12,22,31]. In this study, both MIS–OLIF and MIS–TLIF corrected lumbar lordosis and disk angle because of the large cage that was used with posterior fixation [12,31]. In addition, most patients had single-stage spondylolisthesis. Larger cages were used with MIS–OLIF (width up to 55 mm and height up to 14 mm) than with MIS–TLIF (width of 25–30 mm and height up to 10–12 mm). The wide cage was mounted on the hard epiphyseal ring around the vertebral body rather than the relatively weak area of bone cortex in the central depression of the endplate. Consequently, the disk height, foraminal dimension and area change were all larger in MIS–OLIF than in MIS–TLIF. Disability (ODI) scores and back and leg pain in both MIS–OLIF and MIS–TLIF patients improved significantly from baseline to 24 weeks postoperatively. MIS–OLIF patients experienced 71% improvements in leg and in back pain and 55% improvement in ODI. MIS–TLIF patients experienced 65, 62 and 52% improvements in leg and back pain and ODI, respectively. The study results are consistent with those of Ohtori et al., who reported that MIS–OLIF significantly reduced leg pain from a preoperative VAS of 8.2 ± 2.7 to a postoperative VAS of 1.5 ± 0.80 (p = 0.005) and back pain from 9.5 ± 3.5 to 2.3 ± 1.7 (p = 0.005) at 1 year.
Hip flexor and distal motor weakness result from psoas muscle function and sensory deficit results from retraction of the associated sensory nerves [23]. In this study, the incidence of hip flexion weakness was 2%, distal motor weakness was not reported and sensory deficit occurred in 2% of MIS–OLIF patients. Hynes reported thigh numbness in 16% and weakness of the hips and quadriceps in 6.5% of patients [32]. Silvestre et al. reported lower-extremity sympathetic chain disruption symptoms in 1.7% [27]. Fujibayashi et al. reported transient leg weakness in 7.1% and transient numbness in 21.4%, which can be attributed to the small sample size [33]. At present, significant attention has been focused on the surgical experience of the patients, as good surgical experiences provide excellent postoperative clinical results [34–36]. The patients MIS–OLIF patients had 100% satisfaction, significantly better than the MIS–TLIF patients, and were willing to undergo a repeat procedure.
The study limitations included its retrospective single-center design and radiographic follow-up at 24 weeks only. In addition, some radiographic evaluations such as spondylolisthesis, flexion/extension and translation and fusion were not included.
Conclusion
The disk height and foraminal dimension change of the MIS–OLIF group were better than that of the MIS–TLIF group. Disk angle and lumbar lordosis were similar between the two groups. Despite similar clinical findings, the MIS–OLIF group had less blood loss and hospital stay than the MIS–TLIF group. These results suggest that both MIS–OLIF and MIS–TLIF are effective approaches for the treatment of lumbar DSL with stenosis. However, the patients preferred MIS–OLIF (more minimally invasive) to MIS–TLIF.
Future perspective
MIS–OLIF and MIS–TLIF are effective approaches for the treatment of lumbar DSL with stenosis. However, MIS–OLIF (more minimally invasive) will be more popular.
•
Few studies have compared the clinical and radiographic outcomes of minimally invasive surgery (MIS)–transforaminal lumbar interbody fusion (TLIF) and MIS–oblique lumbar interbody fusion (OLIF) for treatment of degenerative spondylolisthesis.
•
This study compared the clinical and radiographic outcomes of and the effectiveness of MIS–TLIF and MIS–OLIF for treatment of degenerative spondylolisthesis.
•
Patient and treatment characteristics, patient-reported outcomes, and radiographic outcomes were compared.
•
This was a retrospective study.
•
Procedure time, blood loss and length of hospital stay were significantly reduced in MIS–OLIF compared with MIS–TLIF patients. Patient-reported outcomes were similar.
•
Changes in disc height and foraminal dimension were greater in MIS–OLIF than in the MIS–TLIF patients.
•
Patient satisfaction was greater in MIS–OLIF than in MIS–TLIF patients.
•
The clinical findings in the two treatment groups were similar, but patients preferred MIS–OLIF (less invasive) to MIS–TLIF.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. All data are provided in the manuscript.
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Jacobsen S, Sonne-Holm S, Rovsing H, Monrad H, Gebuhr P. Degenerative lumbar spondylolisthesis: an epidemiological perspective: the Copenhagen Osteoarthritis Study. Spine 32, 120–125 (2007).
2.
Modic MT, Ross JS. Lumbar degenerative disk disease. Radiology 245, 43–61 (2007).
3.
Parker SL, Adogwa O, Bydon A, Cheng J, McGirt MJ. Cost-effectiveness of minimally invasive versus open transforaminal lumbar interbody fusion for degenerative spondylolisthesis associated low-back and leg pain over two years. World Neurosurg. 78, 178–184 (2012).
4.
Rodgers WB, Gerber EJ, Rodgers JA. Lumbar fusion in octogenarians: the promise of minimally invasive surgery. Spine 35, S355–S360 (2010).
5.
Brau SA. Mini-open approach to the spine for anterior lumbar interbody fusion: description of the procedure, results and complications. Spine J. 2, 216–223 (2002).
6.
Lucio JC, Vanconia RB, Deluzio KJ et al. Economics of less invasive spinal surgery: an analysis of hospital cost differences between open and minimally invasive instrumented spinal fusion procedures during the perioperative period. Risk Manag. Healthc. Policy 5, 65–74 (2012).
7.
Brodano GB, Martikos K, Lolli F et al. Transforaminal lumbar interbody fusion in degenerative disk disease and spondylolisthesis grade i: minimally invasive versus open surgery. J. Spinal Disord. Tech. 28, E559–E564 (2015).
8.
Parker SL, Mendenhall SK, Shau DN et al. Minimally invasive versus open transforaminal lumbar interbody fusion for degenerative spondylolisthesis: comparative effectiveness and cost-utility analysis. World Neurosurg. 82, 230–238 (2014).
9.
Orr RD. In patients with one-level lumbar degenerative spondylolisthesis, a posterior approach with transforaminal lateral interbody fusion improved radiographic but not clinical outcomes. J. Bone Joint Surg. Am. 100, 345 (2018).
•• Article on a similar topic.
10.
Sakeb N, Ahsan K. Comparison of the early results of transforaminal lumbar interbody fusion and posterior lumbar interbody fusion in symptomatic lumbar instability. Indian J. Orthop. 47, 255–263 (2013).
11.
Hsieh PC, Koski TR, O’Shaughnessy BA et al. Anterior lumbar interbody fusion in comparison with transforaminal lumbar interbody fusion: implications for the restoration of foraminal height, local disc angle, lumbar lordosis, and sagittal balance. J. Neurosurg. Spine 7, 379–386 (2007).
•• Article on a similar topic.
12.
Phan K, Thayaparan GK, Mobbs RJ. Anterior lumbar interbody fusion versus transforaminal lumbar interbody fusion-systematic review and meta-analysis. Br. J. Neurosurg. 29, 705–711 (2015).
13.
Miscusi M, Ramieri A, Forcato S et al. Comparison of pure lateral and oblique lateral inter-body fusion for treatment of lumbar degenerative disk disease: a multicentric cohort study. Eur. Spine J. 27, 222–228 (2018).
•• Article on a similar topic.
14.
Ozgur BM, Aryan HE, Pimenta L, Taylor WR. Extreme lateral interbody fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J. 6, 435–443 (2006).
15.
Sharma AK, Kepler CK, Girardi FP, Cammisa FP, Huang RC, Sama AA. Lateral lumbar interbody fusion: clinical and radiographic outcomes at 1 year: a preliminary report. J. Spinal Disord. Tech. 24, 242–250 (2011).
16.
Arnold PM, Anderson KK, McGuire RA Jr. The lateral transpsoas approach to the lumbar and thoracic spine: a review. Surg. Neurol. Int. 3, S198–S215 (2012).
17.
Mayer HM. A new microsurgical technique for minimally invasive anterior lumbar interbody fusion. Spine 22, 691–699, discussion 700 (1997).
18.
Mehren C, Mayer HM, Zandanell C, Siepe CJ, Korge A. The oblique anterolateral approach to the lumbar spine provides access to the lumbar spine with few early complications. Clin. Orthop. Relat. Res. 474, 2020–2027 (2016).
19.
Shimer AL. CORR Insights([R]): the oblique anterolateral approach to the lumbar spine provides access to the lumbar spine with few early complications. Clin. Orthop. Relat. Res. 474, 2028–2029 (2016).
20.
Abbasi H, Murphy CM. Economic performance of oblique lateral lumbar interbody fusion (OLLIF) with a focus on hospital throughput efficiency. Cureus 7, e292 (2015).
21.
Khajavi K, Shen AY. Two-year radiographic and clinical outcomes of a minimally invasive, lateral, transpsoas approach for anterior lumbar interbody fusion in the treatment of adult degenerative scoliosis. Eur. Spine J. 23, 1215–1223 (2014).
22.
Watkins RG 4th, Hanna R, Chang D, Watkins RG 3rd. Sagittal alignment after lumbar interbody fusion: comparing anterior, lateral, and transforaminal approaches. J. Spinal Disord. Tech. 27, 253–256 (2014).
23.
Xu DS, Walker CT, Godzik J, Turner JD, Smith W, Uribe JS. Minimally invasive anterior, lateral, and oblique lumbar interbody fusion: a literature review. Ann. Transl. Med. 6, 104 (2018).
24.
Sembrano JN, Tohmeh A, Isaacs R, Group SDS. Two-year comparative outcomes of MIS lateral and MIS transforaminal interbody fusion in the treatment of degenerative spondylolisthesis: part I: clinical findings. Spine 41(Suppl. 8), S123–S132 (2016).
25.
Isaacs RE, Sembrano JN, Tohmeh AG, Group SDS. Two-year comparative outcomes of MIS lateral and MIS transforaminal interbody fusion in the treatment of degenerative spondylolisthesis: Part II: Radiographic findings. Spine 41(Suppl. 8), S133–S144 (2016).
26.
Carreon LY, Puno RM, Dimar JR 2nd, Glassman SD, Johnson JR. Perioperative complications of posterior lumbar decompression and arthrodesis in older adults. J. Bone Joint Surg. Am. 85-A, 2089–2092 (2003).
27.
Silvestre C, Mac-Thiong JM, Hilmi R, Roussouly P. Complications and morbidities of mini-open anterior retroperitoneal lumbar interbody fusion: oblique lumbar interbody fusion in 179 patients. Asian Spine J. 6, 89–97 (2012).
28.
Jin J, Ryu KS, Hur JW, Seong JH, Kim JS, Cho HJ. Comparative study of the difference of perioperative complication and radiologic results: MIS-DLIF (minimally invasive direct lateral lumbar interbody fusion) versus MIS-OLIF (minimally invasive oblique lateral lumbar interbody fusion). Clin. Spine Surg. 31, 31–36 (2018).
29.
Youssef JA, McAfee PC, Patty CA et al. Minimally invasive surgery: lateral approach interbody fusion: results and review. Spine 35, S302–S311 (2010).
30.
Glassman SD, Berven S, Bridwell K, Horton W, Dimar JR. Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine 30, 682–688 (2005).
31.
Jagannathan J, Sansur CA, Oskouian RJ Jr, Fu KM, Shaffrey CI. Radiographic restoration of lumbar alignment after transforaminal lumbar interbody fusion. Neurosurgery 64, 955–963, (2009).
32.
Hynes RA. Oblique lateral interbody fusion (OLIF) technique and complications in 457 levels L1 to S1. Presented at: International Society for the Advancement of Spine Surgery Conference. FL, USA, 30 April–2 May (2014).
33.
Fujibayashi S, Hynes RA, Otsuki B, Kimura H, Takemoto M, Matsuda S. Effect of indirect neural decompression through oblique lateral interbody fusion for degenerative lumbar disease. Spine 40, E175–E182 (2015).
34.
Mancuso CA, Duculan R, Stal M, Girardi FP. Patients’ expectations of lumbar spine surgery. Eur. Spine J. 24, 2362–2369 (2015).
35.
Toyone T, Tanaka T, Kato D, Kaneyama R, Otsuka M. Patients’ expectations and satisfaction in lumbar spine surgery. Spine 30, 2689–2694 (2005).
36.
Mancuso CA, Duculan R, Cammisa FP et al. Fulfillment of patients’ expectations of lumbar and cervical spine surgery. Spine J. 16, 1167–1174 (2016).
Information & Authors
Information
Published In
Pages: 45 - 51
PubMed: 31838875
Copyright
© 2019 Future Medicine Ltd.
History
Received: 4 May 2019
Accepted: 28 October 2019
Published online: 16 December 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Minimally invasive surgery for degenerative spondylolisthesis: transforaminal or oblique lumbar interbody fusion. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0055
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lantao Liu, Chicheng Ma, Lianghai Jiang, Longwei Chen, Xinpeng Zhou, Dechun Wang, Early radiological adjacent segment changes following L4/5 fusion: a retrospective comparative study of oblique lateral interbody fusion and minimally invasive transforaminal lumbar interbody fusion, PeerJ, 10.7717/peerj.19918, 13, (e19918), (2025).
- Po-Hsin Chou, Jing-Jie Chen, Chen-Sheng Chen, Shih-Tien Wang, Chien-Lin Liu, Shih-Liang Shih, Changing rod stiffness to moderate stress of adjacent disc in oblique lumbar interbody fusion - a finite element analysis, BMC Musculoskeletal Disorders, 10.1186/s12891-025-08504-3, 26, 1, (2025).
- Jian Tong, Daoyu Chen, Jin Li, Tao Yu, Haobo Chen, Qingquan Kong, Evaluating the efficacy and suggesting technical optimizations for endoscopic lumbar interbody fusion across different lumbar spondylolisthesis types, Heliyon, 10.1016/j.heliyon.2024.e32576, 10, 11, (e32576), (2024).
- Xun Xiao, Heng Duan, Xin Pan, Hua Zhao, Fusion rate and complications of oblique lumbar interbody fusion and transforaminal lumbar interbody fusion in the treatment of lumbar degenerative diseases: a meta-analysis, Frontiers in Surgery, 10.3389/fsurg.2024.1374134, 11, (2024).
- Yuanhu Lei, Juemiao Chen, Zhixuan Liu, Mingjiang Luo, Yuxin Yang, Can Liang, Zhihong Xiao, Effect of Lateral Surgery Compared with Posterior Surgery on Lumbar Degenerative Disease: A Meta-Analysis of 41 Cohort Studies, World Neurosurgery, 10.1016/j.wneu.2024.01.142, 184, (e417-e448), (2024).
- Zhengquan Xu, Qingcong Zheng, Liqun Zhang, Rongsheng Chen, Zhechen Li, Weihong Xu, Biomechanical evaluation of different oblique lumbar interbody fusion constructs: a finite element analysis, BMC Musculoskeletal Disorders, 10.1186/s12891-024-07204-8, 25, 1, (2024).
- 晋德 王, Comparison of Early Clinical Effect between OLIF Combined with Posterior Per-cutaneous Pedicle Screw Fixation Technique and Conventional TLIF in the Treatment of Lumbar Spondylolisthesis, Advances in Clinical Medicine, 10.12677/ACM.2024.141170, 14, 01, (1173-1181), (2024).
- Xiangyu Li, Xiaolong Chen, Yu Wang, Ashish D. Diwan, Shibao Lu, Early outcomes of oblique lateral interbody fusion with posterior fixation versus posterior interbody fusion with fixation for treating adult degenerative scoliosis, Journal of Orthopaedic Surgery and Research, 10.1186/s13018-023-04363-7, 18, 1, (2023).
- Auroshish Sahoo, Mantu Jain, Suprava Naik, Gurudip Das, Pankaj Kumar, Sujit Kumar Tripathy, Harish V. K. Ratna, Mathan Kumar Ramasubbu, Does indirect decompression by oblique lateral interbody fusion produce similar clinical and radiological outcomes to direct decompression by open transforaminal lumbar interbody fusion, Journal of Neurosciences in Rural Practice, 10.25259/JNRP_322_2023, 15, (53-61), (2023).
- Art Eleanore, Susan R. Christopher, Zoher Ghogawala, Randomized controlled trials and degenerative grade I spondylolisthesis, Seminars in Spine Surgery, 10.1016/j.semss.2023.101042, 35, 3, (101042), (2023).