Cost–effectiveness of elagolix versus leuprolide acetate for treating moderate-to-severe endometriosis pain in the USA
Abstract
Aim: To assess the cost–effectiveness of elagolix versus leuprolide acetate in women with moderate to severe endometriosis pain. Methods: A Markov model was developed. The efficacy of leuprolide acetate was derived from statistical prediction models using elagolix trial data. Model inputs were extracted from Phase III clinical trials and published literature. Results: Compared with leuprolide acetate, elagolix generated positive net monetary benefit (NMB) assuming a payer's willingness-to-pay threshold of US$100,000 per quality-adjusted life year over a 1-year time horizon: US$5660 for elagolix 150 mg and US$6443 for elagolix 200 mg. The 2-year NMBs were also positive. Conclusion: Elagolix was cost effective versus leuprolide acetate in the management of moderate to severe endometriosis pain over 1- and 2-year time horizons. Results were robust in sensitivity analyses.
Endometriosis is a chronic gynecological condition defined by the presence of endometrial glands and stroma outside the uterus [1]. The estimated prevalence of endometriosis ranges between 4 and 10% among women in their reproductive years [2–4]. Endometriosis manifests with pain symptoms – including nonmenstrual pelvic pain (NMPP), dysmenorrhea (DYS; painful menstruation) and dyspareunia (painful intercourse) [5] – that are often severe enough to result in decrements in quality-of-life and productivity in the workplace and at home [6–8]. Due to the nonspecific nature of pain, patients are often diagnosed about 7 years after symptom onset, at which time they typically would have accrued a substantial burden of disease [9–12]. A retrospective analysis of women with endometriosis using a commercial database between 2010 and 2014 found that they incurred US$10,002 and US$2132 in direct and indirect healthcare costs per year, respectively, more than matched women without endometriosis [13]. Efforts are ongoing to improve the awareness and diagnosis of endometriosis, including the standardization of transvaginal ultrasonography terminologies by the International Deep Endometriosis Analysis (IDEA) group [14].
Pain management is the cornerstone of endometriosis treatment and for patients with moderate to severe pain, it often involves repeated courses of medical therapy, surgery or both [15]. In the absence of contraindications, nonsteroidal anti-inflammatory drugs, cyclical combined oral contraceptives and progestins are common first-line medical therapies for endometriosis [15,16]. If pain persists, a switch to continuous combined oral contraceptives or a levonorgestrel intrauterine system may be warranted. If these approaches are not effective, gonadotropin-releasing hormone (GnRH) agonist therapy, for example, with leuprolide acetate [17], can be appropriate per clinical guidelines [5,15]. However, while GnRH agonist therapy is effective in controlling pain, it also has considerable side effects due to the induced hypoestrogenic state. This may lead to bone loss of up to 13% over a period of 6 months, requiring progestogen add-back therapy from 6 months to a maximum of 1-year treatment as per US FDA approval [17,18]. Surgical approaches – including laparoscopy, hysterectomy and laparotomy – can be used as first-line therapy or after failed medical therapies [5,15,19]. However, in addition to its invasiveness, surgery often does not resolve endometriosis pain and is associated with recurrence of pain requiring additional therapy (in 30–60% of patients) within 6 to 12 months post-surgery [15]. There is thus an unmet need for more effective, better tolerated and safer treatment for moderate to severe endometriosis pain.
In July 2018, the FDA approved elagolix (ORILISSA™), an oral GnRH antagonist specifically developed for women with moderate to severe pain associated with endometriosis [20,21]. Patients initiate treatment with elagolix 150 mg once daily (QD) for a maximum of 24 months or 200 mg twice daily (BID) for a maximum of 6 months [21]. The FDA approval of elagolix was based on data from two multinational, double-blind, placebo-controlled Phase III trials – Elaris Endometriosis I and II (EM-I and EM-II) [22] – involving almost 1700 premenopausal women with moderate to severe pain associated with endometriosis; the coprimary end points were the proportion of patients whose DYS or NMPP responded to treatment at month 3. The trials revealed that, compared with placebo, patients treated with elagolix 150 mg QD and 200 mg BID had significantly reduced DYS and NMPP pain. The 200 mg BID dosage also led to a significant reduction of dyspareunia. Most common adverse reactions (>5%) in trials included hot flushes and night sweats, headache, nausea, insomnia, amenorrhea, anxiety, arthralgia, depression-related adverse reactions and mood changes [21,22].
Elagolix has not yet been assessed for its cost–effectiveness relative to current medical treatments for moderate to severe endometriosis pain. Although the Institute for Clinical and Economic Review (ICER) recently completed a review of elagolix for moderate to severe endometriosis pain, it was relative to placebo or no active treatment [23]. The objective of the present study was to estimate the cost–effectiveness of elagolix relative to the GnRH agonist leuprolide acetate, the most commonly used second-line medical treatment for endometriosis according to an internal analysis of Truven health insurance claims in 2016 (see Supplementary Material B). The analysis was conducted from the perspective of a US managed care organization that only considered direct medical care costs. Specifically, a cost–effectiveness model (CEM) was developed to assess the 1- and 2-year cost–effectiveness of 24-month treatment with elagolix 150 mg QD and 6-month treatment with elagolix 200 mg BID, each relative to 12-month treatment with leuprolide acetate plus 6-month add-back therapy, in a hypothetical population of women with moderate to severe endometriosis pain. The duration of each treatment was determined by the treatment's label [17,21].
Methods
A summary table of model assumptions is presented in Supplementary Material A.
Model structure
Developed as a health-state (Markov) transition model, the CEM included twelve (12) health states: three on-treatment symptom severity states (no/mild symptoms; moderate symptoms; severe symptoms), two off-treatment symptom severity states (off-treatment with no/mild symptoms; other medical treatment with moderate/severe symptoms), six surgery and post-surgery states (first laparoscopy; post-first laparoscopy; second laparoscopy; post-second laparoscopy; hysterectomy; post-hysterectomy) and one absorbing mortality state. Permissible transitions between these health states, depicted as arrows in Figure 1, were assumed to take place at the beginning of each 3-month Markov cycle.
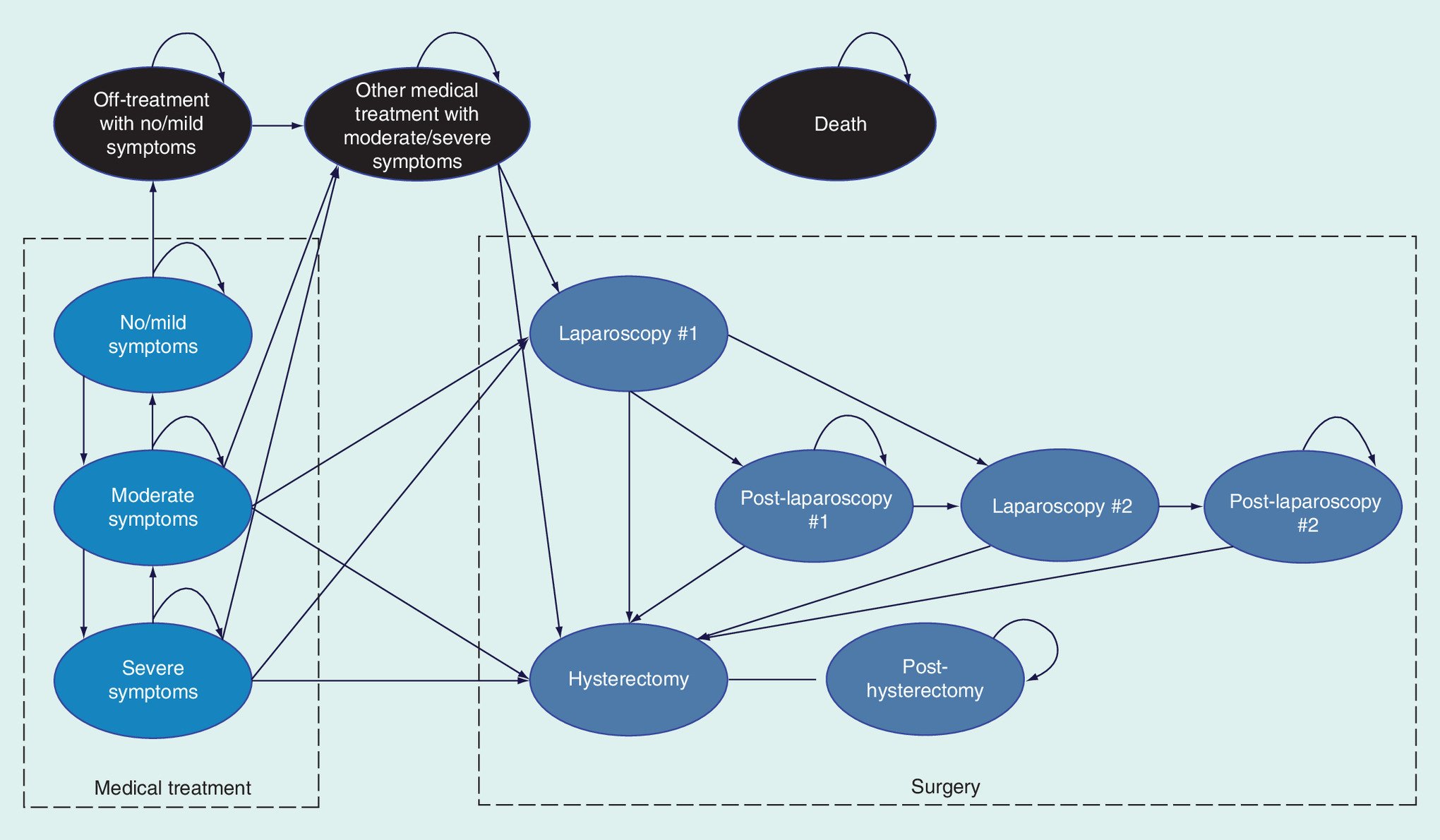
Figure 1. Cost–effectiveness model structure.
Health states are depicted by ellipses, while arrows represent permissible transitions between health states. Transition to all-cause death is possible from all states. Transition to operative death is possible from states: ‘laparoscopy #1’, ‘laparoscopy #2’ and ‘hysterectomy’.
Patients entered the CEM through its three on-treatment symptom severity states for two endometriosis symptoms: DYS and NMPP. The severity of each symptom was defined by the Endometriosis Daily Pain Impact Diary (EDPID) score: 0/1 = no/mild, 2 = moderate and 3 = severe [24]. From their initial state, patients transitioned from a worse severity state to a better severity state per treatment-specific symptom response rates. To combine the two symptoms, equal weights were assigned to each symptom (varied in sensitivity analysis from 0 to 100% DYS). The resulting weighted averages were used for all symptom-related model inputs.
Two off-treatment states captured treatment discontinuation (unplanned) or completion (planned) with elagolix or leuprolide acetate. Upon treatment discontinuation or completion, patients with no/mild symptoms transitioned to ‘off-treatment with no/mild symptoms’ while patients with moderate/severe symptoms transitioned to ‘other medical treatment with moderate/severe symptoms’. For cycles before the treatment-specific model duration of treatment (DOT), treatment-specific premature discontinuation rates were estimated from the treatments’ Phase III trials. All remaining patients transitioned to their respective off-treatment state upon reaching the treatment-specific model DOT. Patients in the ‘off-treatment with no/mild symptoms’ state could experience symptom recurrence and transition to ‘other medical treatment with moderate/severe symptoms’. Patients in states with moderate/severe symptoms could receive up to two laparoscopies; those not wanting to preserve their fertility could also receive hysterectomy. A proportion of patients in the post-surgery states were assumed to still experience symptoms and therefore, received other medical treatments. Finally, patients could transition to all-cause death from any state based on the natural death rate; patients undergoing surgery faced additional risk of operative death.
The model was constructed in Microsoft Excel 2016 (Microsoft Corporation, WA, USA).
Study population
The study population comprised 1686 patients enrolled in the Phase III trials of elagolix, namely, premenopausal women between the ages of 18 and 49 years who had received a surgical diagnosis of endometriosis in the previous 10 years and who had moderate or severe endometriosis-associated pain. It was assumed that patients were evenly distributed between moderate and severe pain, faced an all-cause death rate associated with a baseline age of 32 years and were all eligible to receive hysterectomy. Baseline patient characteristics in the model are summarized in Table 1.
| Characteristic | Base | Low | High | DSA Info: low and high source | PSA info: SE used; assumed distribution | Source/note |
|---|---|---|---|---|---|---|
| Symptom severity distribution: | ||||||
| – Moderate | 50.0% | 40.0% | 60.0% | Assumed | Calculated†; β | Assumed |
| – Severe | 50.0% | 60.0% | 40.0% | Assumed | 100% – moderate | Assumed |
| Age (years) | 32 | Not varied | Not varied | Weighted average age across all patients in Elaris EM-I and EM-II [22] | ||
| Proportion preserving fertility | 0.0% | 0.0% | 10.0% | Assumed | Calculated after adding 1%†; β | Assumed; patients preserving fertility were not eligible to receive hysterectomy |
| Proportion of DYS vs NMPP in combined inputs | 50.0% | 0.0% | 100.0% | ±20% | Calculated†; β | Assumed |
†SE calculated as ([base-low] + [high-base])/(2 × 1.96).
DSA: Deterministic sensitivity analysis; DYS: Dysmenorrhea; NMPP: Nonmenstrual pelvic pain; PSA: Probabilistic sensitivity analysis; SE: Standard error.
Intervention & comparator
The model comparator was 12-month treatment with leuprolide acetate plus 6-month add-back with norethindrone acetate (NA) in the latter half of treatment. Leuprolide acetate was administered as an intramuscular injection of 11.25 mg every 3 months for a maximum of four injections. Add-back was administered as 5 mg NA tablets per day for 6 months [17]. For the intervention, both FDA-approved regimens of elagolix were assessed relative to the comparator.
Model inputs
Treatment efficacy
The efficacy of elagolix and leuprolide acetate at eliciting clinical response with respect to moderate to severe DYS and NMPP was each assessed in Phase III trials: elagolix in EM-I and EM-II [22] and leuprolide acetate in Schlaff et al. [25] and Crosignani et al. [26]. However, the treatments’ trials used different definitions for response: elagolix's trials used response rates calculated from self-administered daily EDPID scores and a receiver operating characteristics (ROC)-determined threshold [22] while leuprolide acetate's trials used response rates calculated from clinician-administered monthly Biberoglu and Behrman (B&B) scores and a 1-point threshold [27]. Although the B&B scale is the most commonly used instrument for assessing endometriosis symptoms in a clinical setting, compared with EDPID scores, there is potential recall bias (monthly vs daily reference point) and rater bias (including inter- and intra-rater variability) arising from being clinician- versus self-administered [28].
To reconcile the differences in DYS and NMPP response measurement methodologies, patient-level data from EM-I and EM-II were used to develop statistical prediction models that mapped patient characteristics to 6-month DYS and NMPP response probabilities calculated from daily EDPID scores and the ROC-determined threshold. Predictions of DYS and NMPP response for leuprolide acetate were then generated as the cross-product of the mean predictor values from the leuprolide acetate trials [25,26] and their corresponding fitted coefficients. The technical details of this prediction are described in Supplementary Material D. All model inputs related to treatment efficacy are described in Table 2.
| 3-month transition probabilities | Base | Low | High | DSA info: low and high source | PSA info: SE used; assumed distribution | Source/note |
|---|---|---|---|---|---|---|
| Elagolix 150 mg QD: | ||||||
| – Premature discontinuation | 11.3% | 9.0% | 13.5% | ±20% | Calculated†; β | Taylor et al. [22] |
| – DYS response | 22.2% | 17.8% | 26.6% | ±20% | Calculated†; β | Phase III elagolix data for treatment completers (see Supplementary Material D) |
| – NMPP response | 26.2% | 21.0% | 31.5% | ±20% | Calculated†; β | Phase III elagolix data for treatment completers (see Supplementary Material D) |
| Elagolix 200 mg BID: | ||||||
| – Premature discontinuation | 12.3% | 9.8% | 14.7% | ±20% | Calculated†; β | Taylor et al. [22] |
| – DYS response | 41.5% | 33.2% | 49.8% | ±20% | Calculated†; β | Phase III elagolix data for treatment completers (see Supplementary Material D) |
| – NMPP response | 33.1% | 26.5% | 39.7% | ±20% | Calculated†; β | Phase III elagolix data for treatment completers (see Supplementary Material D) |
| Leuprolide acetate (±NA): | ||||||
| – Premature discontinuation | 8.5% | 6.8% | 10.1% | ±20% | Calculated†; β | Schlaff et al. [25]; Crosignani et al. [26] |
| – DYS response | 38.5% | 30.8% | 46.2% | ±20% | Calculated†; β | Phase III elagolix data for treatment completers (see Supplementary Material D); Schlaff et al. [25]; Crosignani et al. [26] |
| – NMPP response | 36.1% | 28.9% | 43.3% | ±20% | Calculated†; β | Phase III elagolix data for treatment completers (see Supplementary Material D); Schlaff et al [25]; Crosignani et al. [26] |
†SE calculated as ([base-low] + [high-base])/(2 × 1.96).
BID: Twice a day; DOT: Duration of treatment; DSA: Deterministic sensitivity analysis; DYS: Dysmenorrhea; NA: Norethindrone acetate; NMPP: Nonmenstrual pelvic pain; PSA: Probabilistic sensitivity analysis; QD: Once a day; SE: Standard error.
Natural history transition probabilities
Transition probabilities not specific to treatment were either obtained from published literature or assumed, including probabilities for symptom recurrence, surgery and death. Calculated 3-month transition probabilities (or proportions) that did not differ by treatment are summarized in Table 3 [29].
| 3-month transition probabilities (unless specified otherwise) | Base | Low | High | DSA info: low and high source | PSA info: SE used; assumed distribution | Source/note |
|---|---|---|---|---|---|---|
| Symptom recurrence: | ||||||
| – On-treatment: proportion that worsen (vs remain the same) | 2.50% | 2.00% | 3.00% | ±20% | Calculated†; β | Assumed |
| – Off-treatment: from ‘off-treatment with no/mild symptoms’ to ‘other medical treatment with moderate/severe symptoms’ | 4.84% | 3.87% | 5.81% | ±20% | Calculated†; β | Cheewadhanaraks [30]‡ |
| Surgery with moderate/severe symptoms: | ||||||
| – To ‘laparoscopy #1’ from: ‘moderate symptoms’; ‘severe symptoms’; or ‘other medical treatment with moderate/severe symptoms’ | 1.08% | 0.86% | 1.29% | ±20% | Calculated†; β | Soliman et al. [31]§ |
| – To ‘hysterectomy’ from: ‘moderate symptoms’; ‘severe symptoms’; or ‘other medical treatment with moderate/severe symptoms’ | 3.05% | 2.44% | 3.66% | ±20% | Calculated†; β | Soliman et al. [31]§ |
| After laparoscopy: | ||||||
| – To ‘laparoscopy #2’ from: ‘laparoscopy #1’ or ‘post-laparoscopy #1’ | 0.82% | 0.65% | 0.98% | ±20% | Calculated†; β | Soliman et al. [32]¶ |
| – To ‘hysterectomy’ from: ‘laparoscopy #1 or #2’ or ‘post-laparoscopy #1 or #2’ | 1.43% | 1.15% | 1.72% | ±20% | Calculated†; β | Soliman et al. [32]# |
| – Other medical treatments (proportion) | 19.6% | 15.7% | 23.6% | ±20% | Calculated†; β | Surrey et al. [33]†† |
| – Operative death | 0.003% | 0.003% | 0.038% | Low: -20%; hysterectomy high value | Calculated†; β | Chapron et al. [34]‡‡ |
| After hysterectomy: | ||||||
| – Other medical treatments (proportion) | 1.9% | 1.5% | 2.3% | ±20% | Calculated†; β | Surrey et al. [33]†† |
| – Operative death | 0.04% | 0.03% | 0.05% | ±20% | Calculated†; β | Maresh et al. [35]§§ |
†SE calculated as ([base-low] + [high-base])/(2 × 1.96).
‡Cumulative recurrence rate of pain after DMPA treatment (12- adjusted to 3-month).
§Usage of surgical procedures following leuprolide acetate initiation for women with endometriosis (12- adjusted to 3-month).
¶Endometriosis-related laparoscopy (after 14 days of the first laparoscopy) occurring within 1 year of the first endometriosis-related laparoscopy (12- adjusted to 3-month).
#Endometriosis-related hysterectomy occurring within 1 year of the first endometriosis-related laparoscopy (12- adjusted to 3-month).
††Medical treatment (gonadotropin-releasing hormone agonists, progestin and danazol) within 3 months of endometriosis-related laparoscopy or hysterectomy.
‡‡Death from all types of laparoscopy (e.g., diagnostic, minor, major and advanced).
§§Death within 6-week post-operative.
DSA: Deterministic sensitivity analysis; PSA: Probabilistic sensitivity analysis; SE: Standard error.
For patients who did not discontinue treatment, experience symptom response or undergo surgery, a small proportion (2.5%) was assumed to transition from a better on-treatment symptom severity state to a worse one, while the rest (97.5%) remained in their current state. After treatment discontinuation, the probability of symptom recurrence was derived from a study on the cumulative recurrence rates of pain after depot medroxyprogesterone acetate (DMPA) treatment, which was 18% at 12 months [30].
Probabilities of initial surgery (laparoscopy or hysterectomy) were derived from a retrospective claims analysis of the usage of surgical procedures following leuprolide acetate initiation among women with endometriosis. In their first year after leuprolide acetate initiation, 4.2% (11.7%) of women underwent laparoscopy (hysterectomy) [31]. After the first laparoscopy, probabilities for another laparoscopy or hysterectomy were derived from another claims database analysis on retreatment rates among endometriosis patients with laparoscopy: 3.2% (5.6%) experienced another laparoscopy (hysterectomy) within 1 year of their index laparoscopy [32]. In the post-surgery states, the proportions of patients experiencing moderate to severe pain and receiving other medical treatments were derived from a claims data analysis that found 19.6% (1.9%) of the patients with laparoscopy (hysterectomy) received second-line therapy (i.e., GnRH agonists, progestin and danazol) by 3 months [33].
Adverse events
In the model, only patients in on-treatment states were at risk of experiencing treatment-related adverse events (AEs), including breast pain, depression, headache, hot flushes, libido decrease, nausea and weight gain. It was assumed that AEs negatively impact health state costs (increase) and utilities (decrease). Treatment-related AE rates of any severity were obtained from the AE occurrence data collected in EM-I and EM-II [37] and leuprolide acetate's prescribing information [17]. Weighted average 6-month AE rates were adjusted to 3-month rates and presented in Table 4. The AE rates for ‘other medical treatments’ were assumed to be the averages of all treatments’ rates.
| 3-month event rates | Base | Low | High | DSA info: low and high source | PSA info: SE used; assumed distribution | Source/note |
|---|---|---|---|---|---|---|
| Elagolix 150 mg QD (weighted average rates from Elaris EM-I and EM-II trial data): [37] | ||||||
| – Breast pain | 0.2% | 0.2% | 0.3% | ±20% | Calculated†; β | Include breast swelling/enlargement and tenderness |
| – Depression | 1.3% | 1.0% | 1.5% | ±20% | Calculated†; β | Include depressed mood, depressive symptoms, emotional disorder |
| – Headache | 6.8% | 5.4% | 8.1% | ±20% | Calculated†; β | Include migraines |
| – Hot flushes | 12.8% | 10.3% | 15.4% | ±20% | Calculated†; β | Include night sweats |
| – Libido decrease | 1.4% | 1.1% | 1.7% | ±20% | Calculated†; β | Include libido increased, loss of libido |
| – Nausea | 5.4% | 4.3% | 6.5% | ±20% | Calculated†; β | Include vomiting |
| – Weight gain | 1.2% | 0.9% | 1.4% | ±20% | Calculated†; β | Include weight decreased |
| Elagolix 200 mg BID (weighted average rates from Elaris EM-I and EM-II trial data): [37] | ||||||
| – Breast pain | 0.3% | 0.3% | 0.4% | ±20% | Calculated†; β | Include breast swelling/enlargement and tenderness |
| – Depression | 2.8% | 2.2% | 3.3% | ±20% | Calculated†; β | Include depressed mood, depressive symptoms, emotional disorder |
| – Headache | 9.0% | 7.2% | 10.8% | ±20% | Calculated†; β | Include migraines |
| – Hot flushes | 27.7% | 22.2% | 33.3% | ±20% | Calculated†; β | Include night sweats |
| – Libido decrease | 2.8% | 2.2% | 3.3% | ±20% | Calculated†; β | Include libido increased, loss of libido |
| – Nausea | 6.7% | 5.4% | 8.1% | ±20% | Calculated†; β | Include vomiting |
| – Weight gain | 1.2% | 0.9% | 1.4% | ±20% | Calculated†; β | Include weight decreased |
| Leuprolide acetate monotherapy (weighted average rates from leuprolide acetate PI): [17] | ||||||
| – Breast pain | 3.0% | 2.4% | 3.6% | ±20% | Calculated†; β | Include breast changes/tenderness |
| – Depression | 12.8% | 10.2% | 15.4% | ±20% | Calculated†; β | Include emotional lability |
| – Headache | 22.3% | 17.8% | 26.8% | ±20% | Calculated†; β | |
| – Hot flushes | 64.1% | 51.3% | 76.9% | ±20% | Calculated†; β | Include hot sweats |
| – Libido decrease | 5.7% | 4.6% | 6.8% | ±20% | Calculated†; β | |
| – Nausea | 8.2% | 6.5% | 9.8% | ±20% | Calculated†; β | Include vomiting |
| – Weight gain | 6.7% | 5.3% | 8.0% | ±20% | Calculated†; β | Include weight loss |
| Leuprolide acetate+NA (weighted average rates from leuprolide acetate PI): [17] | ||||||
| – Breast pain | 4.8% | 3.9% | 5.8% | ±20% | Calculated†; β | Include breast changes/tenderness |
| – Depression | 17.5% | 14.0% | 21.0% | ±20% | Calculated†; β | Include emotional lability |
| – Headache | 27.6% | 22.1% | 33.2% | ±20% | Calculated†; β | Include migraine |
| – Hot flushes | 41.7% | 33.3% | 50.0% | ±20% | Calculated†; β | Include hot sweats |
| – Libido decrease | 3.2% | 2.6% | 3.8% | ±20% | Calculated†; β | Include libido increase (changes) |
| – Nausea | 9.0% | 7.2% | 10.9% | ±20% | Calculated†; β | Include vomiting |
| – Weight gain | 3.5% | 2.8% | 4.2% | ±20% | Calculated†; β | Include weight loss |
| Surgical complications: | ||||||
| – Laparoscopy | 13.7% | 10.9% | 16.4% | ±20% | Calculated†; β | 3-month results from Surrey et al. [33] |
| – Hysterectomy | 25.1% | 20.1% | 30.1% | ±20% | Calculated†; β | 3-month results from Surrey et al. [33] |
†SE calculated as ([base-low] + [high-base])/(2 × 1.96).
BID: Twice a day; DSA: Deterministic sensitivity analysis; NA: Norethindrone acetate; PI: Prescribing information; PSA: Probabilistic sensitivity analysis; QD: Once a day; SE: Standard error.
Patients in surgical states were at risk of surgery-related complications. Rates of surgery-related complications were obtained from the 3-month results of a published retrospective claims analysis of endometriosis patients, where 13.7% (25.1%) of endometriosis patients with laparoscopy (hysterectomy) developed complications within 3 months of surgery (36.4% [46.0%] within 12 months of surgery as published) [33].
Of note, although bone mineral density (BMD) loss is a known AE of medical endometriosis treatments, modeling BMD loss in terms of fracture risk was excluded given its expected negligible impact on model results. Specifically, the fracture risk estimated by the FRAX score (US Caucasian) for a woman who might have been in EM-I or EM-II was only 0.1% over 10 years (0.01% over 1 year) [38,39] (we estimated the 10-year risk of hip fracture risk for a representative woman included in the EM-I and EM-II trials assuming: body mass index [BMI] = 27, no previous fractures, no parent fractured hip, no current smoking, no glucocorticoids, no rheumatoid arthritis, no secondary osteoporosis, no alcohol 3 or more units/day, with a femoral neck BMD t-score of -1). In addition, as the weighted average age in EM-I and EM-II was 32 years (Table 1), 8 years younger than the minimum 40 years of age assumed for the FRAX score, the 10-year risk estimate of 0.1% was likely an overestimate. Combined with the facts that 1) neither treatments resulted in large incremental relative changes in BMD over 6 months (at most 5–6% decline for leuprolide acetate) [17,21,22,25,26]; 2) changes in BMD predominantly occurred while on treatment with partial recovery observed in the post-treatment follow-up studies [21,22,40]; and 3) model time horizon was only a maximum of 2 years, the impact of including versus excluding fractures on model results would likely be negligible.
Utilities
To estimate quality-adjusted life years (QALYs), utilities for the on- and off-treatment health states were derived from an analysis of patients’ EQ-5D-5L data collected in EM-II at baseline, month 3 and month 6 (see Supplementary Material C). Utilities for the surgery states were derived using a similar approach as Roberts et al. [41]. Specifically, it was assumed that patients had zero utility for the first 3 days after a laparoscopy and the first seven days after a hysterectomy. Utilities for post-surgery states were assumed to be weighted averages of the utility for ‘other medical treatment with moderate/severe symptoms’ for the proportion of patients still experiencing symptoms and the utility for ‘off-treatment with no/mild symptoms’ for the remaining proportion of ‘cured’ patients after each type of surgery. Health state utilities in the model are summarized in Table 5 [41–43]. The AE- and surgical complication-related disutilities were either derived from published literature or assumed and summarized in Table 6 [41,44–48].
| Health state utility | Base | Low | High | DSA info: low and high source | PSA info: SE used; assumed distribution | Source/note |
|---|---|---|---|---|---|---|
| Off-treatment with no/mild symptoms | 0.842 | 0.674 | 1.000 | ±20% | Calculated†; β | EQ-5D-5L data collected in elagolix Phase III trial Elaris EM-II (see Supplementary Material C)§ |
| No/mild symptoms | 0.874 | 0.699 | 1.000 | ±20% | Calculated†; β | EQ-5D-5L data collected in elagolix Phase III trial Elaris EM-II (see Supplementary Material C)§ |
| Moderate symptoms | 0.777 | 0.622 | 0.933 | ±20% | Calculated‡; Log-normal | EQ-5D-5L data collected in elagolix Phase III trial Elaris EM-II (see Supplementary Material C)§ |
| Severe symptoms | 0.649 | 0.520 | 0.779 | ±20% | Calculated‡; Log-normal | EQ-5D-5L data collected in elagolix Phase III trial Elaris EM-II (see Supplementary Material C)§ |
| Other medical treatment with moderate/severe symptoms | 0.741 | 0.593 | 0.889 | ±20% | Calculated‡; Log-normal | EQ-5D-5L data collected in elagolix Phase III trial Elaris EM-II (see Supplementary Material C)§ |
| Laparoscopy #1 and #2 | 0.689 | 0.551 | 0.827 | ±20% | Calculated‡; Log-normal | Abbott et al. [42]¶ |
| Post-laparoscopy #1 and #2 | 0.822 | 0.658 | 0.987 | ±20% | Calculated‡; Log-normal | Assumed# |
| Hysterectomy | 0.654 | 0.523 | 0.784 | ±20% | Calculated‡; Log-normal | Roberts et al. [41]¶ |
| Post-hysterectomy | 0.840 | 0.672 | 1.000 | ±20% | Calculated‡; Log-normal | Assumed# |
†SE calculated as ([base-low] + [high-base])/(2 × 1.96).
‡The relative difference (delta or ratio) in utility between these states and ‘no/mild symptoms’ were sampled from the log-normal distribution which was applied to obtain health utilities in these states at each simulation.
§Health state utilities were estimated using fractional logit GEE models.
¶For the hysterectomy and laparoscopy states, weighted average utilities of zero (0) utility for 7 and 3 days (assumed) followed by disutilities of 12.5% and 15.4% relative to the ‘off-treatment with no/mild symptoms’ state for ∼84 and ∼88 days, respectively, are assumed.
#Assumed to be weighted average of the utility of ‘other medical treatment with moderate/severe symptoms’ for the proportion of patients receiving other medical treatments and the utility of ‘off-treatment with no/mild symptoms’ for the remaining proportion of ‘cured’ patients after each surgery type.
DSA: Deterministic sensitivity analysis; GEE: Generalized estimating equation; PSA: Probabilistic sensitivity analysis; SE: Standard error.
| Adverse event disutility | Base | Low | High | DSA Info: low and high source | PSA info: SE used; assumed distribution | Source |
|---|---|---|---|---|---|---|
| Breast pain | -0.003 | -0.002 | -0.003 | ±20% | Calculated†; β | Sullivan et al. [46]‡ |
| Depression | -0.120 | -0.096 | -0.144 | ±20% | Calculated†; β | Sapin et al. [45]§ |
| Headache | -0.027 | -0.022 | -0.033 | ±20% | Calculated†; β | Sullivan et al. [46]¶ |
| Hot flushes | -0.011 | -0.009 | -0.014 | ±20% | Calculated†; β | Lux et al. [44]# |
| Libido decrease | -0.049 | -0.039 | -0.059 | ±20% | Calculated†; β | Maniadakis et al. [47]†† |
| Nausea | -0.040 | -0.032 | -0.048 | ±20% | Calculated†; β | Matza et al. [48]‡‡ |
| Weight gain | -0.040 | -0.032 | -0.048 | ±20% | Calculated†; β | Matza et al. [48]§§ |
| Laparoscopy complication | -0.070 | -0.056 | -0.084 | ±20% | Calculated†; β | Assumed same disutility as hysterectomy complication |
| Hysterectomy complication | -0.070 | -0.056 | -0.084 | ±20% | Calculated†; β | Roberts et al. [41]¶¶ |
†SE calculated as ([base-low] + [high-base])/(2 × 1.96).
‡Based on utility of nonmalignant breast conditions.
§Based on utility of mild depression.
¶Based on utility of headache including migraine.
#Based on the relative change in utility between no event versus weight gain, hot flushes, vaginal discharge.
††Based on disutility of sexual dysfunction.
‡‡Based on basic health state with nausea.
§§Based on basic health state with 3% higher weight.
¶¶Difference between hysterectomy (0.56) and severe complications after hysterectomy (0.49).
DSA: Deterministic sensitivity analysis; PSA: Probabilistic sensitivity analysis; SE: Standard error.
Resource identification & costs
Each patient who spent a model cycle in the three on-treatment states incurred 3-month cost of acquiring and administering elagolix or leuprolide acetate (±NA). Likewise, in every model cycle, each patient in the ‘other medical treatments with moderate/severe symptoms’ state and 19.6% (1.9%) of patients in the post-laparoscopy (post-hysterectomy) states incurred 3-month cost of acquiring and administering other medical treatments [33]. The 3-month cost of other medical treatments was assumed to be made up of progestin (62.8%; assumed to be DMPA), followed by GnRH agonists (36.6%; assumed to be equally distributed between goserelin and nafarelin acetate), and danazol (0.5%) [33].
Drug acquisition costs were calculated based on the drugs’ Wholesale Acquisition Cost prices and their [expected] indicated dose/frequency for endometriosis [49]. For elagolix, a price of US$844.87 per 28-day was assumed for both doses. Administration costs were included for treatments administered intramuscularly (leuprolide acetate) and subcutaneously (DMPA and goserelin acetate) [50]. The unit costs behind their calculations are described in Table 7. Costs of managing treatment-related AEs, summarized in Table 8, were obtained from either the 2014 Medical Expenditure Panel Survey [51] or US-based published literature [52–55].
| Resource unit | Base## (2018 US$) | Source/note |
|---|---|---|
| Elagolix (150 mg QD) – per mg | 0.20 | Red Book® Online [49]† |
| Elagolix (200 mg BID) – per mg | 0.08 | Red Book® Online [49]‡ |
| Leuprolide acetate (11.25 mg/3-month IM injection) – per mg | 326.52 | Red Book® Online [49]§ |
| NA (5 mg QD) – per mg | 0.38 | Red Book® Online [49]¶ |
| DMPA (104 mg/3-month SC injection) – per injection | 233.46 | Red Book® Online [49]# |
| Danazol (300 mg BID) – per 200+100 mg capsule pair | 10.02 | Red Book® Online [49]†† |
| Goserelin acetate (3.6 mg/month SC injection) – per injection | 605.00 | Red Book® Online [49]‡‡ |
| Nafarelin acetate (0.2 mg nasal spray BID) – per nasal spray | 35.46 | Red Book® Online [49]§§ |
| IM injection administration | 31.32 | CPT code: 96402 [50]¶¶ |
| SC injection administration | 20.88 | CPT code: 96372 [50]¶¶ |
†Identifier(s): 00074-0038-28.
‡Identifier(s): 00074-0039-56.
§Identifier(s): 00074-3663-03.
¶Identifier(s): 65162-0475-09, 65162-0475-05, 65862-0715-50, 42291-0650-90, 50268-0602-15, 68462-0304-50, 00555-0211-10.
#Identifier(s): 00009-4709-13.
††Identifier(s): 42291-0243-01, 00527-1369-01, 00527-1369-06, 00527-1368-01, 00555-0635-02, 00555-0635-09, 00555-0634-02.
‡‡Identifier(s): 00310-0950-36.
§§Identifier(s): 00025-0166-08.
¶¶National non-facility.
##The unit costs of treatment acquisition and administration were not varied in the DSA and PSA.
BID: Twice a day; DMPA: Depot medroxyprogesterone acetate; DSA: Deterministic sensitivity analysis; IM: Intramuscular; NA: Norethindrone acetate; PSA: Probabilistic sensitivity analysis; QD: Once a day; SC: Subcutaneous; SE: Standard error.
| Adverse event | Base (2018 US$) | Low (2018 US$) | High (2018 US$) | DSA info: low and high source | PSA info: SE used; assumed distribution | Source/note |
|---|---|---|---|---|---|---|
| Breast pain | 394 | 316 | 473 | ±20% | Calculated†; γ | MEPS (2014) [51]‡ |
| Depression | 611 | 489 | 734 | ±20% | Calculated†; γ | MEPS (2014) [51]§ |
| Headache | 251 | 200 | 301 | ±20% | Calculated†; γ | MEPS (2014) [51]¶ |
| Hot flushes | 363 | 290 | 436 | ±20% | Calculated†; γ | Sarrel et al. [53] |
| Libido decrease | 279 | 223 | 334 | ±20% | Calculated†; γ | Foley et al. [52]# |
| Nausea | 110 | 88 | 132 | ±20% | Calculated†; γ | Piwko et al. [54]†† |
| Weight gain | 526 | 421 | 631 | ±20% | Calculated†; γ | Kim et al. [55]‡‡ |
†SE calculated as ([base-low] + [high-base])/(2 × 1.96).
‡MEPS mean expenses per person with care (any service) for non-malignant breast disease.
§MEPS mean expenses per person with care (any service) for mental disorders.
¶MEPS mean expenses per person with care (any service) for headache.
#Increase in 12-month total costs between women diagnosed with sexual dysfunction and matched controls.
††Direct cost per woman treated for moderate nausea and vomiting of pregnancy (assume 3-month costs).
‡‡Annual medical spending attributable to an obese individual in 2014 US$.
DSA: Deterministic sensitivity analysis; MEPS: Medical Expenditure Panel Survey; PSA: Probabilistic sensitivity analysis; SE: Standard error.
For non-surgery health states, direct medical costs were calculated as the sum product of the expected number of consultation and office visits with their unit costs [50,56]. For surgery states, direct medical costs of the surgery and 3-month post-surgical healthcare were obtained from the 3-month results of a US claims database study on the cost burden of endometriosis surgeries [57]. The 3-month post-surgical healthcare costs covered amounts paid for inpatient admissions, emergency room, outpatient visits and outpatient pharmacy. Finally, patients in the operative death state incurred a one-time cost, assumed to be the same as the average hospitalization cost for uterine endometriosis [58]. These direct medical costs and utilization are presented in Table 9.
Unit costs of resources were inflated to 2018 US$ using the medical component of the consumer price index [59] and adjusted to 3-month costs [29]. Unit costs of resources obtained from published cost databases were not varied in sensitivity analysis; only cost estimates from statistical analyses were varied.
Discounting
Both costs and benefits were discounted at a rate of 3% per year (equivalent to a 3-month rate of 0.74%), which was varied from 0 to 7% per annum in sensitivity analyses [60].
Sensitivity analyses
Deterministic sensitivity analysis (DSA) was conducted by varying model parameters by their low and high values (presented in Tables 1–9) to assess their impact on model outputs. DSA results are presented in the form of tornado diagrams for a given payer's willingness-to-pay (WTP) for a QALY (assumed to be US$100,000/QALY). Probabilistic sensitivity analysis (PSA) was conducted by considering the uncertainty in all model parameters simultaneously. Results are presented as cost–effectiveness acceptability curves (CEAC; i.e., probability of each treatment option being cost–effectiveness for a given WTP threshold).
| Cost component | Base | Low | High | DSA info: low and high source | PSA info: SE used; assumed distribution | Source/note |
|---|---|---|---|---|---|---|
| Unit costs of outpatient visits (2018 US$): | ||||||
| – Consultation visit for a new patient | 150 | Not varied | Not varied | CPT code: 99204 [50] | ||
| – Office visit for an established patient | 63 | Not varied | Not varied | CPT code: 99213 [50] | ||
| Non-surgery health states: Number of consultation visit(s) per 3-month: | ||||||
| – Off-treatment with no/mild symptoms | 0.0 | 0.00 | 1.00 | ±1 (min 0) | Calculated†; γ | Assumed |
| – No/mild symptoms | 0.5 | 0.00 | 1.50 | ±1 (min 0) | Calculated†; γ | On-treatment states; assumed 0.5 initial visit per quarter based on Winkel et al. [56] |
| – Moderate symptoms | 0.5 | 0.00 | 1.50 | ±1 (min 0) | Calculated†; γ | On-treatment states; assumed 0.5 initial visit per quarter based on Winkel et al. [56] |
| – Severe symptoms | 0.5 | 0.00 | 1.50 | ±1 (min 0) | Calculated†; γ | On-treatment states; assumed 0.5 initial visit per quarter based on Winkel et al. [56] |
| – Other medical treatment with moderate/severe symptoms | 0.5 | 0.00 | 1.50 | ±1 (min 0) | Calculated†; γ | On-treatment states; assumed 0.5 initial visit per quarter based on Winkel et al. [56] |
| – Post-laparoscopy #1 and #2 | 0.0 | 0.00 | 1.00 | ±1 (min 0) | Calculated†; γ | Post-surgical states; assumed |
| – Post-hysterectomy | 0.0 | 0.00 | 1.00 | ±1 (min 0) | Calculated†; γ | Post-surgical states; assumed |
| Non-surgery health states: number of office visit(s) per 3-month: | ||||||
| – Off-treatment with no/mild symptoms | 0.0 | 0.00 | 1.00 | ±1 (min 0) | Calculated†; γ | Assumed |
| – No/mild symptoms | 1.5 | 0.50 | 2.50 | ±1 (min 0) | Calculated†; γ | On-treatment states; assumed 1.5 return visit per quarter based on Winkel et al. [56] |
| – Moderate symptoms | 1.5 | 0.50 | 2.50 | ±1 (min 0) | Calculated†; γ | On-treatment states; assumed 1.5 return visit per quarter based on Winkel et al. [56] |
| – Severe symptoms | 1.5 | 0.50 | 2.50 | ±1 (min 0) | Calculated†; γ | On-treatment states; assumed 1.5 return visit per quarter based on Winkel et al. [56] |
| – Other medical treatment with moderate/severe symptoms | 1.5 | 0.50 | 2.50 | ±1 (min 0) | Calculated†; γ | On-treatment states; assumed 1.5 return visit per quarter based on Winkel et al. [56] |
| – Post-laparoscopy #1 and #2 | 1.0 | 0.00 | 2.00 | ±1 (min 0) | Calculated†; γ | Post-surgical states; assumed |
| – Post-hysterectomy | 0.0 | 0.00 | 1.00 | ±1 (min 0) | Calculated†; γ | Post-surgical states; assumed |
| Surgery health states: surgery and 3-month post-surgical healthcare costs (2018 US$): | ||||||
| – Laparoscopy | 11,765 | 11,677 | 11,852 | Published ±1.96 × SE = US$45 | γ | 3-month results from Soliman et al. [57] |
| – Hysterectomy | 16,155 | 16,044 | 16,267 | Published ±1.96 × SE US$57 | γ | 3-month results from Soliman et al. [57] |
| – Operative death (one-time cost) | 10,563 | 10,056 | 11,070 | Published ±1.96 × SE US$259 | γ | HCUPnet [58]‡ |
†SE calculated as ([base-low] + [high-base])/(2 × 1.96).
‡Average hospitalization cost for uterine endometriosis (International Classification of Diseases, 9th Revision, code 617.0).
DSA: Deterministic sensitivity analysis; PSA: Probabilistic sensitivity analysis; SE: Standard error.
Results
Base case results of the model are presented in Table 10 for the 1- and 2-year time horizons. Over the 1-year time horizon, both doses of elagolix dominated leuprolide acetate, in other words, elagolix generated more QALYs for less costs. Compared with leuprolide acetate, both doses of elagolix generated positive net monetary benefit (NMB) based on a payer WTP of US$100,000/QALY over the 1-year time horizon: US$5660 for 24-month elagolix 150 mg QD and US$6443 for 6-month elagolix 200 mg BID. Similarly, over the 2-year time horizon, both doses of elagolix were associated with positive NMBs relative to leuprolide acetate: US$2374 for 24-month elagolix 150 mg QD and US$1342 for 6-month elagolix 200 mg BID.
| Treatment | Total costs (2018 US$) | ΔCosts vs LA (2018 US$) | Total QALYs | ΔQALY vs LA | ICER vs LA (2018 US$) | NMB vs LA (2018 US$)† |
|---|---|---|---|---|---|---|
| 1-year time horizon results | ||||||
| Elagolix (150 mg QD) for 24 months | 12,202 | -4482 | 0.7414 | 0.0118 | Elagolix dominant | 5660 |
| Elagolix (200 mg BID) for 6 months | 10,551 | -6132 | 0.7327 | 0.0031 | Elagolix dominant | 6443 |
| LA (+NA) for 12 months | 16,683 | – | 0.7296 | – | – | – |
| 2-year time horizon results | ||||||
| Elagolix (150 mg QD) for 24 months | 21,017 | -591 | 1.5005 | 0.0178 | Elagolix dominant | 2374 |
| Elagolix (200 mg BID) for 6 months | 17,833 | -3775 | 1.4583 | -0.0243 | 155,145 (for LA) | 1342 |
| LA (+NA) for 12 months | 21,607 | – | 1.4827 | – | – | – |
†NMB determined based on a payer WTP of US$100,000 per QALY.
BID: Twice daily; ICER: Incremental cost–effectiveness ratio; LA: Leuprolide acetate; NMB: Net monetary benefit; QALY: Quality-adjusted life year; QD: Once a day; WTP: Willingness-to-pay.
Figures 2 and 3 present the results of the DSA showing the ten most influential model parameters. Over the 1-year time horizon, the model was most sensitive to the non-surgery health state utilities, the treatment-specific response rates for NMPP and DYS, as well as the AE-related disutilities. In all the DSA runs, both 24-month elagolix 150 mg QD and 6-month elagolix 200 mg BID remained cost-effective versus leuprolide acetate based on a WTP of US$100,000/QALY, indicating robust 1-year model outcomes. Over the 2-year time horizon, the model was likewise most sensitive to the non-surgery health state utilities and the treatment-specific response rates for NMPP and DYS. The comparison of 24-month elagolix 150 mg QD versus leuprolide acetate revealed that elagolix was strictly cost-effective versus leuprolide acetate in eight of the ten most influential parameters at a WTP of US$100,000/QALY (Figure 3A). This fell to five out of ten influential parameters for 6-month elagolix 200 mg BID versus leuprolide acetate (Figure 3B).
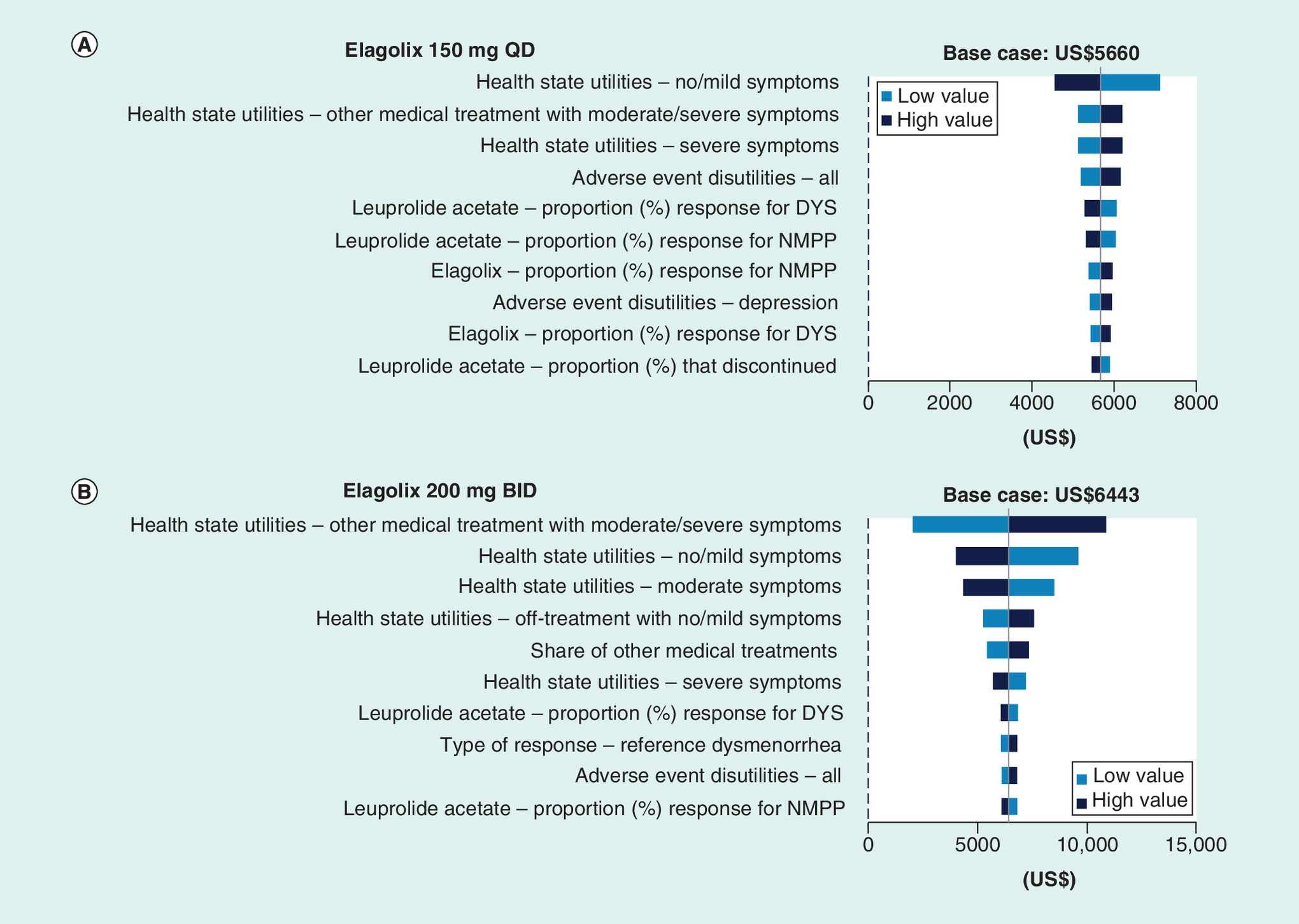
Figure 2. Deterministic sensitivity analysis results showing the ten most influential model parameters comparing elagolix 150 mg once a day and elagolix 200 mg twice a day to leuprolide acetate: 1-year net monetary benefit (willingness-to-pay = US$100,000/quality-adjusted life year).
A dotted vertical line indicating an net monetary benefit of zero based on a willingness-to-pay of US$100,000/quality-adjusted life year is displayed. Hence, bars strictly to the right of this line indicate sensitivity analyses where elagolix is cost-effective against leuprolide acetate.
BID: Twice a day; DYS: Dysmenorrhea; NMPP: Nonmenstrual pelvic pain; QD: Once a day.
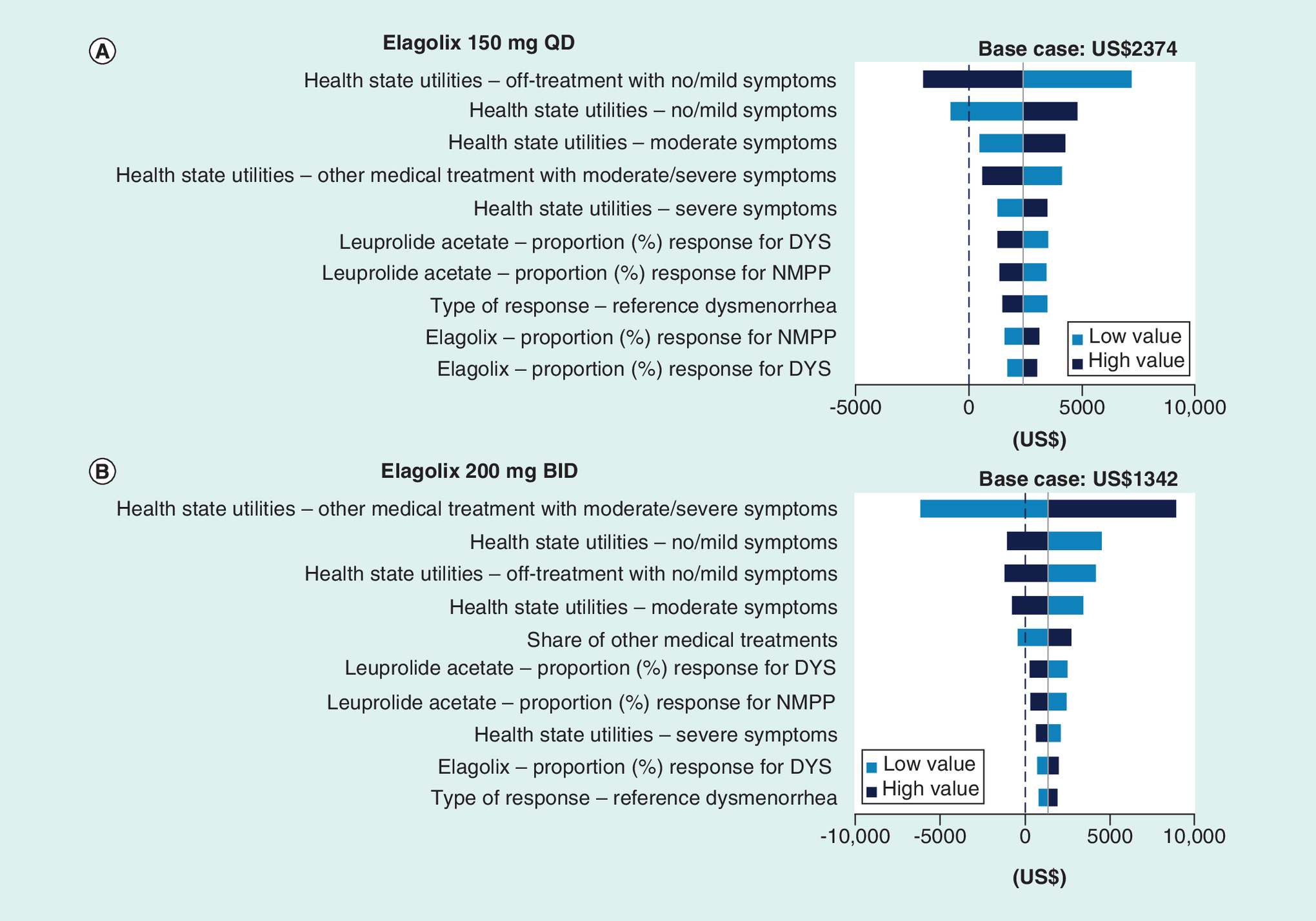
Figure 3. Deterministic sensitivity analysis results showing the ten most influential model parameters comparing elagolix 150 mg once a day and elagolix 200 mg twice a day to leuprolide acetate: 2-year net monetary benefit (willingness-to-pay. = US$100,000/adjusted life year).
A dotted vertical line indicating a net monetary benefit of zero based on a willingness-to-pay of US$100,000/quality-adjusted life year is displayed. Hence, bars strictly to the right of this line indicate sensitivity analyses where elagolix is cost-effective against leuprolide acetate.
BID: Twice a day; DYS: Dysmenorrhea; NMPP: Nonmenstrual pelvic pain; QD: Once a day.
Figure 4 (A–D) present the CEACs of the 500 PSA simulations. Over the 1-year time horizon, both 24-month elagolix 150 mg QD (A) and 6-month elagolix 200 mg BID (B) were the cost-effective option versus leuprolide acetate in 100% of the PSA simulations, for any WTP up to US$100,000/QALY. When the time horizon was extended to 2 years, the probabilities of 24-month elagolix 150 mg QD (C) and 6-month elagolix 200 mg BID (D) being cost-effective versus leuprolide acetate were 80.2 and 78.4%, respectively, for a WTP threshold of US$100,000/QALY.
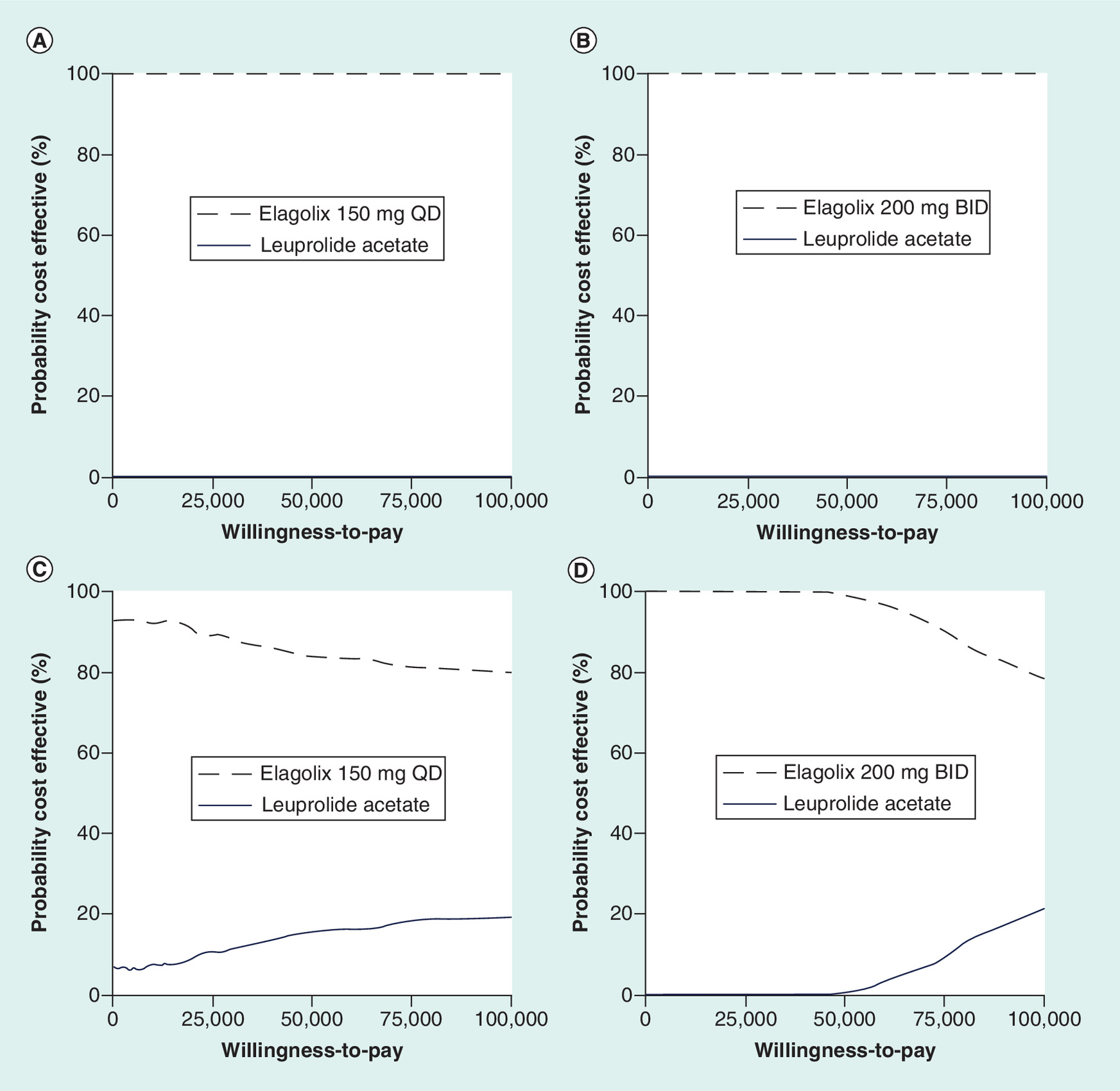
Figure 4. Probabilistic sensitivity analysis; results, cost–effectiveness acceptability curve.
(A) Elagolix 150 mg once a day and leuprolide acetate: 1-year; (B) elagolix 200 mg twice a day and leuprolide acetate: 1-year; (C) elagolix 150 mg once a day and leuprolide acetate: 2-year; (D) elagolix 200 mg BID and leuprolide acetate: 2-year.
BID: Twice a day; QD: Once a day.
Discussion
The CEM showed that both elagolix regimens (i.e., 24-month 150 mg QD and 6-month 200 mg BID) were cost-effective versus leuprolide acetate over the 1-year time horizon, generating positive NMBs versus leuprolide acetate at a WTP of US$100,000/QALY. In fact, base case results showed that both elagolix regimens dominated leuprolide acetate, generating more benefits (i.e., QALYs) for less costs. These results were robust to extensive sensitivity analyses. Specifically, the DSA showed that positive NMB was maintained for both elagolix regimens despite wide ranges (mostly ±20%) in model inputs. Likewise, the PSA revealed that the dominance of 24-month 150 mg QD over leuprolide acetate was robust, occurring in 99.6% of 500 simulations. The dominance of 6-month 200 mg BID over leuprolide acetate was less robust, occurring in 64.0% of 500 simulations, due to greater variability in elagolix's ability to generate more QALYs than leuprolide acetate.
The cost–effectiveness of elagolix versus leuprolide acetate was maintained when extending the time horizon from 1 to 2 years, albeit at reduced magnitudes. Over the 2-year time horizon, the 24-month 150 mg QD regimen generated a positive NMB, indicating that it continued to be cost-effective versus leuprolide acetate but at a more marginal NMB (US$2374). Similarly, the 6-month 200 mg BID regimen generated a smaller NMB (US$1342). These base case results appeared to be highly sensitive: the DSA showed that wide range (mostly ±20%) changes in key model inputs such as non-surgery health state utilities would switch the NMB of both elagolix regimens from positive to negative or vice versa. The highly sensitive nature of the 2-year model results was also supported by the scatterplots and CEACs of the PSA.
The 1-year model results were more appropriate indicators of elagolix's value in the current context where the treatment duration in EM-I and EM-II trials was for 6 months, treatments had unequal model DOTs (i.e., 6-month elagolix 200 mg BID vs 12-month leuprolide acetate), and there were no expected benefits and harms of therapy once discontinued. As such, the shorter time horizon minimized the reliance on extrapolated trial results, reduced the impact of unequal model DOTs and simplified the model to capture differential benefits and harms of treatments only when present, respectively. Longer time horizons would have been more appropriate if there were a persistent differential in mortality or morbidity from two or more treatments for a disease, which is not the expectation for endometriosis.
The cost–effectiveness of treatments for endometriosis pain symptoms has been studied earlier by the NIH and Care Excellence (NICE) in the UK [61], Wu et al. [62], Sanghera et al. [63], as well as the previously mentioned ICER review of elagolix [23]. However, none of these previous studies are relevant to the present study. The NICE review used a Markov decision analytic model to access the cost–effectiveness of various combinations of diagnostic and treatment strategies over a lifetime [61]. As such, a ‘population of healthy women’ entered the NICE model, while a population of women with surgically-diagnosed endometriosis entered the current model. Wu et al. [62] and Sanghera et al. [63] are likewise irrelevant as both studies are economic evaluations of different strategies to prevent endometriosis recurrence following conservative surgery. This means that all patients entered their models without endometriosis symptoms, which is in direct contrast to the moderate to severe endometriosis pain experienced by patients entering the current model.
One scenario not considered owing to lack of data was that the model did not incorporate formulation preferences and their effect on quality-of-life, such as the preference women with endometriosis have for daily oral dosing over monthly injections [64]. Another scenario not included due to negligible impact on model results was the treatments’ effect on BMD loss. Though statistically significant losses in BMD were observed in both treatments’ clinical trials [17,21,22,25,26,40], owing to the low-risk study population (by average age) and short model time horizons (1- and 2-year), these losses did not translate into meaningful absolute and incremental fracture risks. The risk of cardiovascular symptoms (such as palpitations, syncope and tachycardia) in women with endometriosis treated with Lupron was observed in less than 5% of subjects in the Lupron trials [17]. Both favorable changes (i.e., increase in high-density lipoprotein cholesterol [HDL-C]) and unfavorable changes (i.e., increase in low density lipoprotein cholesterol [LDL-C]) in lipid profile were observed in patients treated with elagolix [21,22]. However, it is unclear whether these changes in lipid profile would affect long-term cardiovascular risk in this otherwise low-risk population [22]. Like BMD, cardiovascular risk was not included in the model, owing to the short time horizon of the analysis. Moreover, the lower rates of its occurrence also meant that its absolute and incremental impact would be negligible.
The CEM was subject to several other key limitations. First, no head-to-head trial compared the two therapies. Second, the elagolix and leuprolide acetate trials included different end points for assessing efficacy. As such, the efficacy of the comparator leuprolide acetate in the model needed to be predicted using elagolix Phase III data instead of taken as observed. Third, the model was based on clinical trial results for efficacy and AE rates, but real-world outcomes would be more appropriate to estimate effects; at this time, there are no real-world outcomes for elagolix-treated patients. Fourth, AE data may not be reported similarly across the elagolix and leuprolide acetate trials, and health utilities and cost estimates came from AEs measured in other studies. Health utility was not measured frequently enough in the elagolix studies to validly identify AE disutilities in an endometriosis patient population. Finally, the model evaluated average effects for all indicated patients; subgroup analysis was not conducted owing to lack of data, but effects could be different across patient subgroups.
Conclusion
The base case and sensitivity results of the CEM showed that the two recently FDA-approved doses of elagolix for the management of moderate to severe pain associated with endometriosis – namely 24-month 150 mg QD and 6-month 200 mg BID – were both cost-effective versus leuprolide acetate over a time horizon of 1 to 2 years. Our results were robust to sensitivity analyses. Moreover, treatment with elagolix is an oral medication, which may be favorable to surgery or intramuscular injection treatment alternatives. Last, given that the burden of endometriosis in the US is significant, elagolix seems to offer a good value for money treatment option for payers.
Endometriosis is a chronic gynecological condition with an estimated prevalence ranging from 4 to 10% among women in their reproductive years.
Endometriosis manifests with pain symptoms that are often severe enough to result in decrements in quality-of-life and productivity in the workplace and at home.
In July 2018, elagolix (ORILISSA™) became the first and only US FDA-approved oral gonadotropin-releasing hormone (GnRH) antagonist for treating moderate to severe endometriosis pain. There are two approved regimens of elagolix: 150 mg once daily (QD) for 24 months or 200 mg twice daily (BID) for 6 months.
This study assessed the 1- and 2-year cost–effectiveness of both elagolix regimens, relative to 12-month leuprolide acetate plus 6-month add-back, for moderate to severe endometriosis pain from a US payer perspective.
A de novo Markov state transition model was developed that tracked and quality-adjusted the time spent in treatment, off treatment, surgery, post-surgery and death by a hypothetical cohort of endometriosis patients in 3-month increments.
Model inputs were obtained from Phase III trials data and published literature.
Due to efficacy measurement differences across treatments, the efficacy of leuprolide acetate was mapped from its trial patient characteristics using statistical prediction models estimated from the elagolix patient-level Phase III data.
Model results showed that elagolix was cost-effective versus leuprolide acetate in the management of moderate to severe endometriosis pain over 1- and 2-year time horizons, generating positive net monetary benefits at a willingness-to-pay of US$100,000/quality-adjust life year.
Model results were robust to both deterministic and probabilistic sensitivity analyses.
Elagolix may be considered a cost-effective treatment option in women with moderate to severe endometriosis pain from a US healthcare payer perspective.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
AM Soliman, SK Agarwal, SJ Johnson, S-T Wang and D Mitchell were involved in the conception and design of the analysis; S-T Wang and D Mitchell were involved in the analysis and interpretation of the data; all authors were involved in revising it critically for intellectual content; and the final approval of the version to be published. All authors agree to be accountable for all aspects of the work.
Financial & competing interests disclosure
S-T Wang and SJ Johnson are employees of Medicus Economics LLC, a consulting company that conducts economic evaluations in a variety of therapeutic areas for pharmaceutical companies, which received payment from AbbVie, the study sponsor. D Mitchell is a contractor to Medicus Economics. AM Soliman and JB Vora are employees of AbbVie Inc. and may own AbbVie stock. AbbVie is the manufacturer of elagolix and Lupron Depot (leuprolide acetate). SK Agarwal has served in a consulting role on research for AbbVie Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors acknowledge the technical writing assistance of S Virabhak, an employee of Medicus Economics, in the preparation of this manuscript. Medicus Economics LLC has received funding from AbbVie Inc. for technical writing assistance.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt. The source of these data is: NCT01620528 and NCT01931670.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementaryappendix.docx)
- Download
- 105.80 KB
References
Papers of special note have been highlighted as: • of interest
1.
Parasar P, Ozcan P, Terry KL. Endometriosis: epidemiology, diagnosis and clinical management. Curr. Obstet. Gynecol. Rep. 6(1), 34–41 (2017).
2.
Fuldeore MJ, Soliman AM. Prevalence and symptomatic burden of diagnosed endometriosis in the United States: national estimates from a cross-sectional survey of 59,411 women. Gynecol. Obst. Invest. 82(5), 453–461 (2017).
3.
Ferrero S, Arena E, Morando A, Remorgida V. Prevalence of newly diagnosed endometriosis in women attending the general practitioner. Int. J. Gynecol. Obstet. 110(3), 203–207 (2010).
4.
Eskenazi B, Warner ML. Epidemiology of endometriosis. Obstet. Gynecol. Clin. North Am. 24(2), 235–258 (1997).
5.
Practice bulletin no. 114: management of endometriosis. Obstet. Gynecol. 116(1), 223–236 (2010).
6.
Nnoaham KE, Hummelshoj L, Webster P et al. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil. Steril. 96(2), 366–373.e368 (2011).
7.
Kvaskoff M, Mu F, Terry KL et al. Endometriosis: a high-risk population for major chronic diseases? Hum. Reprod. Update 21(4), 500–516 (2015).
8.
Soliman AM, Coyne KS, Gries KS, Castelli-Haley J, Snabes MC, Surrey ES. The effect of endometriosis symptoms on absenteeism and presenteeism in the workplace and at home. J. Manag. Care Specialty Pharm. 23(7), 745–754 (2017).
• This US claims data study assessed the burden of endometriosis pain symptoms on productivity loss both in the workplace (presenteeism and absenteeism) and at home.
9.
Soliman AM, Yang H, Du EX, Kelley C, Winkel C. The direct and indirect costs associated with endometriosis: a systematic literature review. Hum. Reprod. 31(4), 712–722 (2016).
10.
Simoens S, Dunselman G, Dirksen C et al. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum. Reprod. 27(5), 1292–1299 (2012).
11.
Mirkin D, Murphy-Barron C, Iwasaki K. Actuarial analysis of private payer administrative claims data for women with endometriosis. J. Manag. Care Pharm. 13(3), 262–272 (2007).
12.
Fuldeore M, Yang H, Du EX, Soliman AM, Wu EQ, Winkel C. Healthcare utilization and costs in women diagnosed with endometriosis before and after diagnosis: a longitudinal analysis of claims databases. Fertil. Steril. 103(1), 163–171 (2015).
13.
Soliman AM, Surrey E, Bonafede M, Nelson JK, Castelli-Haley J. Real-world evaluation of direct and indirect economic burden among endometriosis patients in the United States. Adv. Ther. 35(3), 408–423 (2018).
14.
Guerriero S, Condous G, Van Den Bosch T et al. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: a consensus opinion from the International Deep Endometriosis Analysis (IDEA) group. Ultrasound Obstet. Gynecol. 48(3), 318–332 (2016).
15.
Giudice LC. Clinical practice. Endometriosis. N. Engl. J. Med. 362(25), 2389–2398 (2010).
16.
Ferrero S, Barra F, Leone Roberti Maggiore U. Current and emerging therapeutics for the management of endometriosis. Drugs 78(10), 995–1012 (2018).
17.
Abbvie. Lupron Depot: highlights of prescribing information (2018). www.accessdata.fda.gov/drugsatfda_docs/label/2018/020708s035lbl.pdf.
18.
Hornstein MD, Surrey ES, Weisberg GW, Casino LA. Leuprolide acetate depot and hormonal add-back in endometriosis: a 12-month study. Lupron Add-Back Study Group. Obstet. Gynecol. 91(1), 16–24 (1998).
• This is the pivotal Phase III leuprolide acetate (Lupron) trial comparing leuprolide acetate alone and leuprolide acetate with three hormonal add-back regimens.
19.
Collinet P, Fritel X, Revel-Delhom C et al. Management of endometriosis: CNGOF/HAS clinical practice guidelines – short version. J. Gynecol. Obstet. Hum. Reprod. 47(7), 265–274 (2018).
20.
US FDA. Novel drug approvals for 2018 (2018). www.fda.gov/Drugs/DevelopmentApprovalProcess/DrugInnovation/ucm592464.htm.
21.
Abbvie. Orilissa (elagolix): highlights of prescribing information (2018). www.accessdata.fda.gov/drugsatfda_docs/label/2018/210450s000lbl.pdf.
22.
Taylor HS, Giudice LC, Lessey BA et al. Treatment of endometriosis-associated pain with elagolix, an oral GnRH antagonist. N. Engl. J. Med. 377(1), 28–40 (2017).
• This is the pivotal elagolix Phase III trials comparing elagolix to placebo in women with moderate to severe pain symptoms.
23.
Institute for Clinical and Economic Review, New England Comparative Effectiveness Public Advisory Council. Endometriosis: final evidence report (2018). https://icer-review.org/material/endo-final-evidence-report/.
24.
Wyrwich KW, O'Brien CF, Soliman AM, Chwalisz K. Development and validation of the endometriosis daily pain impact diary items to assess dysmenorrhea and nonmenstrual pelvic pain. Reprod. Sci. 25(11), 1567–1576 (2018).
25.
Schlaff WD, Carson SA, Luciano A, Ross D, Bergqvist A. Subcutaneous injection of depot medroxyprogesterone acetate compared with leuprolide acetate in the treatment of endometriosis-associated pain. Fertil. Steril. 85(2), 314–325 (2006).
• This is one of two Phase III trials comparing depot medroxyprogesterone acetate to leuprolide acetate (Lupron) in women with moderate to severe pain symptoms.
26.
Crosignani PG, Luciano A, Ray A, Bergqvist A. Subcutaneous depot medroxyprogesterone acetate versus leuprolide acetate in the treatment of endometriosis-associated pain. Hum. Reprod. 21(1), 248–256 (2006).
• This is one of two Phase III trials comparing depot medroxyprogesterone acetate to leuprolide acetate (Lupron) in women with moderate to severe pain symptoms.
27.
Biberoglu KO, Behrman SJ. Dosage aspects of danazol therapy in endometriosis: short-term and long-term effectiveness. Am. J. Obstet. Gynecol. 139(6), 645–654 (1981).
28.
Deal LS, Dibenedetti DB, Williams VS, Fehnel SE. The development and validation of the daily electronic Endometriosis Pain and Bleeding Diary. Health Qual. Life Outcomes 8, 64 (2010).
29.
Fleurence RL, Hollenbeak CS. Rates and probabilities in economic modelling: transformation, translation and appropriate application. PharmacoEconomics 25(1), 3–6 (2007).
30.
Cheewadhanaraks S. Cumulative recurrence rates of endometriosis-associated pain after long-term intramuscular depot medroxyprogesterone acetate therapy. J. Med. Assoc. Thai. 96(2), 140–143 (2013).
31.
Soliman AM, Bonafede M, Farr AM, Castelli-Haley J, Winkel C. Analysis of adherence, persistence, and surgery among endometriosis patients treated with leuprolide acetate plus norethindrone acetate add-back therapy. J. Manag. Care Specialty Pharm. 22(5), 573–587 (2016).
32.
Soliman AM, Du EX, Yang H, Wu EQ, Haley JC. Retreatment rates among endometriosis patients undergoing hysterectomy or laparoscopy. J. Women's Health 26(6), 644–654 (2017).
33.
Surrey ES, Soliman AM, Yang H, Du EX, Su B. Treatment patterns, complications, and health care utilization among endometriosis patients undergoing a laparoscopy or a hysterectomy: a retrospective claims analysis. Adv. Ther. 34(11), 2436–2451 (2017).
34.
Chapron C, Querleu D, Bruhat MA et al. Surgical complications of diagnostic and operative gynaecological laparoscopy: a series of 29,966 cases. Hum. Reprod. 13(4), 867–872 (1998).
35.
Maresh MJ, Metcalfe MA, Mcpherson K et al. The VALUE national hysterectomy study: description of the patients and their surgery. BJOG 109(3), 302–312 (2002).
36.
Arias E, Heron M, Xu J. United States life tables, 2014. Natl. Vital Stat. Rep. 66(4), (2017).
37.
Abbvie. Data on file: H18.DoF.030 (2018).
38.
Looker AC, Sarafrazi Isfahani N, Fan B, Shepherd JA. FRAX-based estimates of 10-year probability of hip and major osteoporotic fracture among adults aged 40 and over: United States, 2013 and 2014. Natl Health Stat. Rep. 103, 1–16 (2017).
39.
FRAX: Fracture Risk Assessment Tool – Calculation Tool (2018). www.sheffield.ac.uk/FRAX/tool.aspx?country=9.
40.
Surrey E, Taylor HS, Giudice L et al. Long-term outcomes of elagolix in women with endometriosis: results from two extension studies. Obstet. Gynecol. 132(1), 147–160 (2018).
• This paper presented the long-term results of the two pivotal elagolix Phase III trials’ 6-month extension studies, after 12 months of total continuous treatment.
41.
Roberts TE, Tsourapas A, Middleton LJ et al. Hysterectomy, endometrial ablation, and levonorgestrel releasing intrauterine system (Mirena) for treatment of heavy menstrual bleeding: cost–effectiveness analysis. BMJ 342, d2202 (2011).
42.
Abbott J, Hawe J, Hunter D, Holmes M, Finn P, Garry R. Laparoscopic excision of endometriosis: a randomized, placebo-controlled trial. Fertil. Steril. 82(4), 878–884 (2004).
43.
Abbvie. Data on file: H18.DoF.034 (2018).
44.
Lux MP, Reichelt C, Karnon J et al. Cost–benefit analysis of endocrine therapy in the adjuvant setting for postmenopausal patients with hormone receptor-positive breast cancer, based on survival data and future prices for generic drugs in the context of the german health care system. Breast Care (Basel, Switzerland) 6(5), 381–389 (2011).
45.
Sapin C, Fantino B, Nowicki M-L, Kind P. Usefulness of EQ-5D in assessing health status in primary care patients with major depressive disorder. Health Qual. Life Outcomes 2, 20–20 (2004).
46.
Sullivan PW, Lawrence WF, Ghushchyan V. A national catalog of preference-based scores for chronic conditions in the United States. Med. Care 43(7), 736–749 (2005).
47.
Maniadakis N, Kourlaba G, Mougiakos T, Chatzimanolis I, Jonsson L. Economic evaluation of agomelatine relative to other antidepressants for treatment of major depressive disorders in Greece. BMC Health Serv. Res. 13, 173 (2013).
48.
Matza LS, Boye KS, Yurgin N et al. Utilities and disutilities for type 2 diabetes treatment-related attributes. Qual. Life Res. 16(7), 1251–1265 (2007).
49.
Truven Health Analytics. Micromedex Red Book Online Search. (2018).
50.
American Medical Association. CPT/Medicare Payment Search. www.ama-assn.org/practice-management/cpt-current-procedural-terminology.
51.
Medical Expenditure Panel Survey (2014).
52.
Foley K, Foley D, Johnson BH. Healthcare resource utilization and expenditures of women diagnosed with hypoactive sexual desire disorder. J. Med. Econ. 13(4), 583–590 (2010).
53.
Sarrel P, Portman D, Lefebvre P et al. Incremental direct and indirect costs of untreated vasomotor symptoms. Menopause 22(3), 260–266 (2015).
54.
Piwko C, Koren G, Babashov V, Vicente C, Einarson TR. Economic burden of nausea and vomiting of pregnancy in the USA. J. Pop. Therapeut. Clin. Pharmacol. 20(2), e149–e160 (2013).
55.
Kim DD, Basu A. Estimating the medical care costs of obesity in the United States: systematic review, meta-analysis, and empirical analysis. Value Health 19(5), 602–613 (2016).
56.
Winkel CA. Modeling of medical and surgical treatment costs of chronic pelvic pain: new paradigms for making clinical decisions. Am. J. Manag. Care 5(5 Suppl.), S276–S290 (1999).
57.
Soliman AM, Taylor H, Bonafede M, Nelson JK, Castelli-Haley J. Incremental direct and indirect cost burden attributed to endometriosis surgeries in the United States. Fertil. Steril. 107(5), 1181–1190.e1182 (2017).
• This retrospective cohort study quantified the incremental direct (healthcare) and indirect (absenteeism and short-/long-term disability) cost burden of endometriosis surgeries in the US.
58.
Agency for Healthcare Research and Quality. Healthcare cost and utilization project (2015). http://hcupnet.ahrq.gov.
59.
Consumer Price Index for All Urban Consumers (2017).
60.
Lipscomb J, Weinstein MC, Torrance GW, United States Public Health Service Panel on cost–effectiveness in health and medicine. Time preference. In: Cost–Effectiveness In Health and Medicine. Gold MR, Siegel JE, Russell LB, Weinstein MC (Eds). Oxford University Press, USA, 214–246 (1996).
61.
National Institute for Health and Care Excellence. Endometriosis: diagnosis and management. NICE Guideline [NG73] (2017).
62.
Wu B, Yang Z, Tobe RG, Wang Y. Medical therapy for preventing recurrent endometriosis after conservative surgery: a cost–effectiveness analysis. BJOG 125(4), 469–477 (2018).
63.
Sanghera S, Barton P, Bhattacharya S, Horne AW, Roberts TE. Pharmaceutical treatments to prevent recurrence of endometriosis following surgery: a model-based economic evaluation. BMJ Open 6(4), (2016).
64.
Poulos C, Soliman AM, Renz C, Posner J, Agarwal SK. A discrete-choice experiment study of patient preferences for treatments for endometriosis-associated pain. Presented at: American Society for Reproductive Medicine 2018 Scientific Congress & Expo. AL, USA, 26–10 October (2018).
Information & Authors
Information
Published In
Copyright
© 2019 Medicus Economics, LLC.
History
Received: 14 November 2018
Accepted: 8 January 2019
Published online: 6 February 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of elagolix versus leuprolide acetate for treating moderate-to-severe endometriosis pain in the USA. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0124
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Magdalena Gniadek, Alina Porubenska, Karolina Pełka, Zuzanna Rzepkowska, Jerzy Florjański, Endometriosis-Associated Infertility: A Review of Pathophysiological Mechanisms and Current Treatment Strategies, Journal of Clinical Medicine, 10.3390/jcm15114297, 15, 11, (4297), (2026).
- Sunita Tandulwadkar, Basab Mukherjee, Chaitanya Ganpule, Madhuri Patel, Subash Mallya, P.M. Gopinath, Brajbala Tiwari, Expert opinion by Federation of Obstetric and Gynaecological Societies of India on elagolix − Redefining the endometriosis therapy landscape, European Journal of Obstetrics & Gynecology and Reproductive Biology, 10.1016/j.ejogrb.2026.115115, 322, (115115), (2026).
- Yihan Xu, Carley Prentice, Sergio Torres-Rueda, András Meczner, Jan Multmeier, Aidan Wickham, Laura Kelly, Anna Klepchukova, Heorhi Stsefanovich, Liudmila Zhaunova, Economic evaluation of a digital symptom checker for endometriosis using a Markov decision process model, npj Digital Medicine, 10.1038/s41746-025-02332-4, 9, 1, (2026).
- Lan Luo, Yonglin Zhang, Li Zhang, Senguo Yang, Tian Zhou, Ke Luo, Shu Liu, Ovarian escape in premenopausal breast cancer: Challenges and strategies for optimizing hormone suppression, Cancer Treatment Reviews, 10.1016/j.ctrv.2025.102970, 139, (102970), (2025).
- Madhuri Patel, Recent Trends in Medical Management of Endometriosis, The Journal of Obstetrics and Gynecology of India, 10.1007/s13224-024-02097-y, 74, 6, (479-483), (2024).
- Jessica Ottolina, Roberta Villanacci, Sara D’Alessandro, Xuemin He, Giorgia Grisafi, Stefano Maria Ferrari, Massimo Candiani, Endometriosis and Adenomyosis: Modern Concepts of Their Clinical Outcomes, Treatment, and Management, Journal of Clinical Medicine, 10.3390/jcm13143996, 13, 14, (3996), (2024).
- Mong‐Jen Chen, Patrick Marroum, Yi‐Lin Chiu, Melina Neenan, Nael M. Mostafa, Mohamad Shebley, Bioequivalence of Elagolix/Estradiol/Norethindrone Acetate Fixed‐Dose Combination Product: Phase 1 Results in Healthy Pre‐ and Postmenopausal Women, Clinical Pharmacology in Drug Development, 10.1002/cpdd.1399, 13, 6, (601-610), (2024).
- Essam Othman, Ayman Al-Hendy, Radwa Mostafa, Cornelis Lambalk, Velja Mijatovic, Oral GnRH Antagonists in Combination with Estradiol and Norethindrone Acetate for Pain Relief Associated with Endometriosis: A Review of Evidence of a Novel Class of Hormonal Agents, International Journal of Women's Health, 10.2147/IJWH.S442357, Volume 16, (309-321), (2024).
- Josep Darbà, Alicia Marsà, Economic Implications of Endometriosis: A Review, PharmacoEconomics, 10.1007/s40273-022-01211-0, 40, 12, (1143-1158), (2022).
- Jacques Donnez, Marie-Madeleine Dolmans, GnRH Antagonists with or without Add-Back Therapy: A New Alternative in the Management of Endometriosis?, International Journal of Molecular Sciences, 10.3390/ijms222111342, 22, 21, (11342), (2021).