A 90-day episode-of-care cost analysis of robotic-arm assisted total knee arthroplasty
Abstract
Aim: To evaluate 90-day episode-of-care (EOC) costs associated with robotic-arm assisted total knee arthroplasty (rTKA) versus manual TKA (mTKA). Patients & methods: TKA procedures were identified in Medicare 100% data. Accounting for baseline differences, propensity score matching was performed 1:5. 90-day EOC and index costs, lengths-of-stay, discharge disposition and readmission rates were assessed. Results: A total of 519 rTKA and 2595 mTKA were included. Overall 90-day EOC costs were US$2391 less for rTKA (p < 0.0001). Over 90% of patients in both cohorts utilized post-acute services, with rTKA accruing fewer costs than mTKA. Post-acute savings can be attributed to discharge destination. Conclusion: rTKA incurred an overall lower 90-day EOC cost versus mTKA. Savings were driven by fewer readmissions and an economically beneficial discharge destinations.
Knee osteoarthritis (OA) affects approximately 14 million individuals in the USA [1]. Its prevalence has roughly doubled since the middle of the 20th century and is expected to continue to grow as a result of the aging population and their increasing desire to maintain active lifestyles [1–4]. Although a number of nonsurgical and surgical management modalities exist, total knee arthroplasty (TKA) has been considered the gold standard procedure for end-stage knee OA [7–11]. For most patients, this surgery is highly successful, resulting in substantial improvements in quality of life and function [12]. Additionally, some studies have shown that TKA is a highly cost-effective procedure [13]. For these reasons and more, the volume of primary TKAs is estimated to increase from roughly 700,000 procedures in 2008 to nearly three million procedures in 2030 [2]. Despite the number of clinical and economic benefits of TKAs, due to its high demand and volume, the associated overall healthcare costs present a substantial financial burden on payers.
One way to potentially help contain healthcare costs is the utilization of technological advances in the operating room [3]. Robotic-arm assisted technology was introduced in orthopedics in efforts to help enhance clinical, radiographic and patient-reported outcomes [4]. Robotic-arm assisted total knee arthroplasty (rTKA) systems aim to build on previous systems and to provide surgeons with enhanced preoperative planning abilities, as well as real-time, intraoperative data, allowing for continuous assessments of ligamentous tensions and ranges-of-motion [5]. Additionally, haptically controlled saw blades can provide the surgeon with immediate, pulsatile feedback while making bone cuts [6,7]. This haptic feedback helps ensure that bone cuts are performed in the desired location in three-dimensions, which has been shown to help protect the surrounding soft-tissues and ligaments [6,7].
Robotic-arm assisted technology has also demonstrated improved bone cut accuracy and precision to plan, component alignment and soft-tissue balancing [7,8]. Furthermore, it has been associated with a short learning curve, high ability to predict implant sizes, improved patient satisfaction scores and reduced early post-operative pain [5,9–11]. These advances have the potential to enhance surgical outcomes and may also reduce episode-of-care (EOC) costs for patients, payers and hospitals. Additionally, total joint arthroplasty has been a target of value-based reimbursement platforms such as Comprehensive Care for Joint Replacement (CJR) and the Bundled Payment Care Initiative (BPCI), which most believe are the future of value-based models. Therefore, demonstrating the need for further understanding of the economic outcomes associated with robotic-arm assisted arthroplasties is critical moving forward. To this end, the purpose of this study was to perform a cost analysis between robotic-arm assisted TKA and manual TKA (mTKA) techniques. Specifically, we compared: 90-day EOC costs, as well as several variables within the episode, including index costs; index lengths-of-stay (LOS); discharge dispositions; and readmission rates. Given the published evidence demonstrating rTKA's clinical benefits as compared with mTKA, this study hypothesized that the rTKA cohort would experience a reduction in resource utilization and associated payments connected with the 90-day EOC.
Methods
Study design & data sources
This analysis was designed to evaluate post-index 90-day EOC costs to Medicare and utilization for Medicare patients undergoing rTKA and mTKA procedures from the payer perspective. Data were obtained from the Medicare 100% Standard Analytic Files (SAF), compiled by the Center for Medicare and Medicaid Services (CMS) and is representative of medical services provided to nearly 37 million Medicare Fee-for-Service beneficiaries. A retrospective claims analysis was conducted to provide longitudinal assessments of Medicare Fee-for-Service beneficiaries who underwent rTKA and mTKA procedures performed between 1 January 2016 and 31 March 2017 (referred to as the index period), and included the following post-index services: Inpatient, Outpatient, Skilled Nursing (SNF) and Home Health Agency (HHA). Costs (dollars) were defined as total payments made to providers.
Study population selection
Medicare beneficiaries who received a primary TKA (referred to as the index procedure) during the index period were considered for inclusion into the study. Cases were identified by the presence of International Classification of Diseases, Tenth Version (ICD-10) billing codes (0SRD0J9, 0SRD0JA, 0SRD0JZ, 0SRC0J9, 0SRC0JA and 0SRC0JZ), in addition to a diagnosis related group (DRG) assignment of 461, 462, 469 or 470. Only TKAs were included with unicompartmental procedures excluded. A more detailed description of the coding is presented in Appendix A.
Following the identification of TKA claims, two study cohorts were created: robotic-arm assisted TKA (rTKA) and manual TKA (mTKA). Cases in the rTKA cohort were defined by the presence of the following criteria: a pre-operative computed tomography (CT)-scan (CPT 73700, 73701 or 73702) that occurred within 60 days prior to the rTKA procedure, and an ICD-10 code indicative of a robotic assisted procedure present (8E0Y0CZ). Cases in the mTKA cohort included the remaining claims identified with the absence of a CT-scan in addition to the absence of the ICD-10 robotic assisted procedure code. This case identification methodology was designed to identify cases performed with the Mako System (Stryker, Mahwah, NJ, USA) as the pre-operative CT-scan is required to create the pre-operative 3D plan for the Mako System. Hospitals included in the analysis were also reviewed against a list of Mako System locations as an added verification step.
Following the identification of TKA claims, two study cohorts were created: robotic-arm assisted TKA (rTKA) and manual TKA (mTKA). Cases in the rTKA cohort were defined by the presence of the following criteria: a pre-operative computed tomography (CT)-scan (CPT 73700, 73701 or 73702) that occurred within 60 days prior to the rTKA procedure, and an ICD-10 code indicative of a robotic assisted procedure present (8E0Y0CZ). Cases in the mTKA cohort included the remaining claims identified with the absence of a CT-scan in addition to the absence of the ICD-10 robotic assisted procedure code. This case identification methodology was designed to identify cases performed with the Mako System (Stryker, Mahwah, NJ, USA) as the pre-operative CT-scan is required to create the pre-operative 3D plan for the Mako System. Hospitals included in the analysis were also reviewed against a list of Mako System locations as an added verification step.
Claims were excluded from the analysis if they met any of the following criteria:
Payments associated with the index procedure considered erroneous (claims missing payment information);
Patient had a hip or staged bilateral knee arthroplasty within 90 days of the index procedure (pre or post) identified by the assignment of a DRG indicating major joint replacement or reattachment of lower extremity with major complications or comorbidities (DRG 469) or without major complications or comorbidities (DRG470);
Patient who experienced in-hospital mortality during study duration.
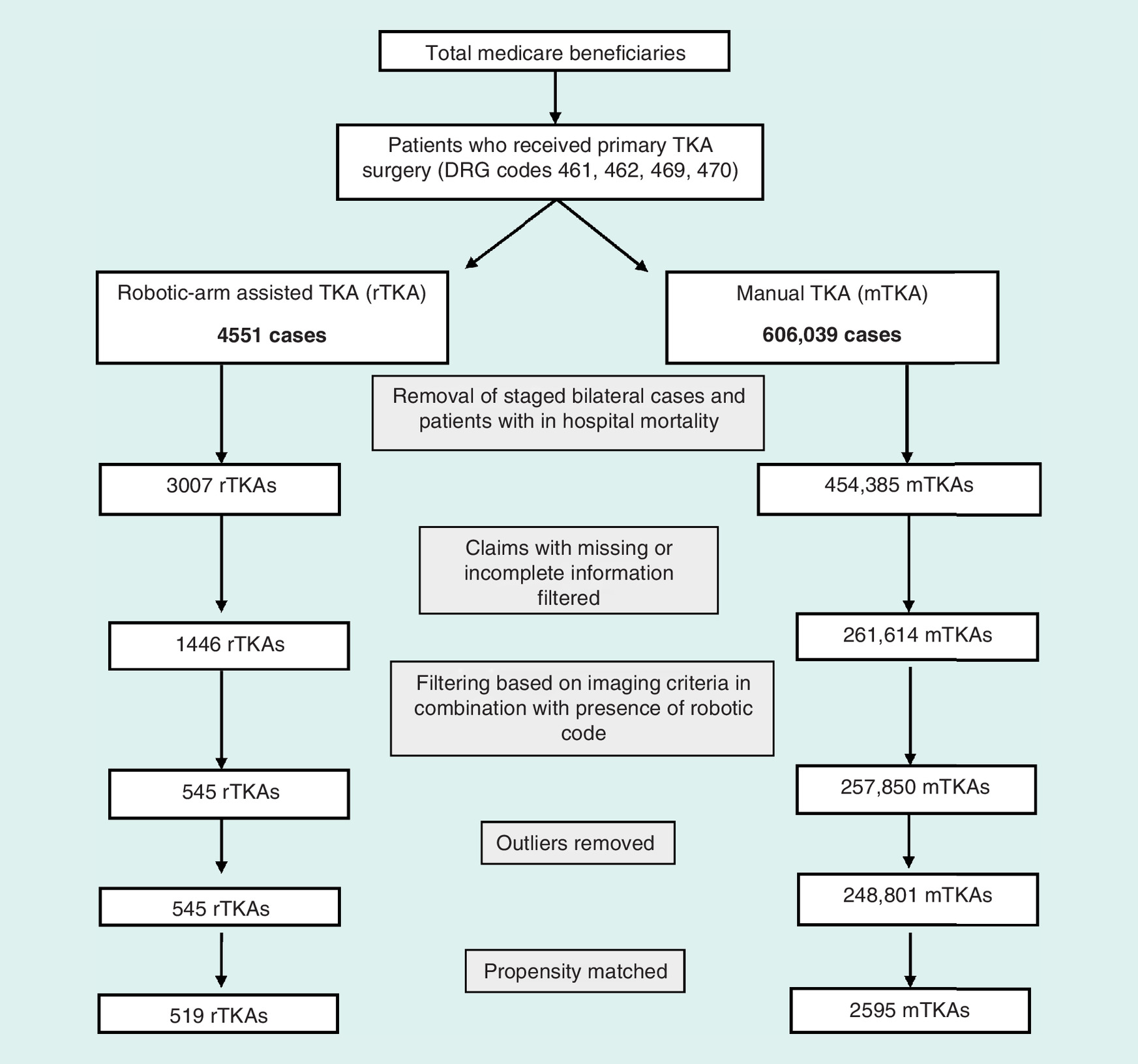
The initial search based on DRG codes 461, 462, 469 and 470 yielded 4551 rTKA and 606,039 mTKAs. Removing staged bilateral cases and patients with in-hospital mortality resulted in 3007 rTKA and 454,385 mTKAs. After filtering based on the presence of a CT-scan in combination with presence of a robotic code, 545 rTKAs and 257,850 mTKAs were identified. After outliers were removed from both cohorts (using an exponential [Gamma] distribution with a cut-off value of Zk = 0.001), 519 rTKAs and 248,801 mTKAs were identified prior to propensity score matching and further review or analysis of the data.
Propensity score matching
To account for potential baseline differences, propensity score matching was performed using the Fisher's Scoring methodology. Patients were matched rTKA to mTKA in a 1-to-5 ratio. Matching was based on the following criteria: age, sex, race (as defined by CMS), geographic division (based on US Census Bureau divisions) and high-cost comorbidities (including chronic obstructive pulmonary disease [COPD], hypertension, diabetes, coronary artery disease [CAD], smoking, pneumonia, cancer, and obesity). After propensity score matching, 519 rTKA and 2595 mTKA were identified and included for analysis. A detailed flowchart of the case selection methodology is illustrated in Figure 1.
90-day EOC
The overall 90-day EOC costs, including the index procedures (facility and physician costs), LOS, discharge dispositions and readmissions were calculated. EOC costs to Medicare were identified through the presence of claims billed representing services rendered in an inpatient, outpatient, emergency room, SNF or HHA setting during the index or the 90-day post-index period. This identification of EOC costs are consistent with methods used by Medicare in their bundled payment programs for arthroplasty bundles. Discharge disposition was assessed for the index procedure (including discharge to Home Health with Health Aid, Home with Self-Care, SNF and Inpatient Rehabilitation). For patients who experienced an in-hospital readmission during the 90-day period immediately following their index procedure (known as the 90-day post-index period), readmission rates and inpatient costs were evaluated (no calculations and/or modeling occurred). LOS were collected at index, as well as in the 90-day post-index period for SNF and inpatient settings.
Data analysis
A Generalized Linear Model was selected to test for statistical significance due to the data not being normally distributed. Statistical comparisons were made of EOC costs in the 90-day post-index period. A two-part model was created to conduct statistical analyses of the probability of having utilization as well as the associated costs in each postoperative cost setting. A binomial regression with a log-link was used to test the probability of having costs or utilization in the 90-day post-index period in the first part of the model. A gamma distribution with a log-link function was used to analyze cost distributions among members who had costs in the second part of the model. Utilization distributions among members who had utilization were tested using negative binomial distribution with a log-link function when the variance exceeded the mean; otherwise, a Poisson distribution with a log-link was utilized. Test differences among dichotomous and categorical variables were analyzed using Pearson's χ2 test and those among continuous variables were analyzed using the Mann–Whitney U test. These analyses were performed using SAS Enterprise Guide 7.1 software (SAS Institute Inc., Cary, NC, USA).
Results
Population demographics
No statistical differences were observed between the two cohorts in age, sex, race, geographical location or high-cost comorbidities. However, both cohorts had equally high rates of white members (according to CMS classification) (92 rTKA vs 93% mTKA), as well as equally high rates of members from the New England and South Atlantic regions (27 and 25% in both cohorts, respectively). Hypertension and diabetes were also quite common among both cohorts (64 and 18% in both cohorts, respectively). Table 1 highlights the demographic and comorbidity profile of the matched study cohorts.
| Characteristics | rTKA (n = 519) (%) | mTKA (n = 2595) (%) | Difference (%) | p-value |
|---|---|---|---|---|
| Age | ||||
| – 65–69 | 37.19 | 36.99 | 0.19 | 0.9339 |
| – 70–74 | 29.48 | 29.36 | 0.12 | 0.9579 |
| – 75–79 | 21.20 | 21.16 | 0.04 | 0.9843 |
| – 80–84 | 7.13 | 7.36 | -0.23 | 0.8536 |
| – ≥84 | 5.01 | 5.13 | -0.12 | 0.9130 |
| Sex | ||||
| – Male | 42.78 | 41.77 | 1.00 | 0.6728 |
| Race | ||||
| – Asian | 0.77 | 0.69 | 0.08 | 0.8482 |
| – Black | 1.73 | 1.93 | -0.19 | 0.7688 |
| – Hispanic | 0.19 | 0.08 | 0.12 | 0.4384 |
| – North American Native | 0.58 | 0.50 | 0.08 | 0.8226 |
| – Other | 1.54 | 1.62 | -0.08 | 0.8985 |
| – Unknown | 2.89 | 2.51 | 0.39 | 0.6125 |
| – White | 92.29 | 92.68 | -0.39 | 0.7593 |
| Division | ||||
| – East North Central | 5.97 | 5.82 | 0.15 | 0.8913 |
| – East South Central | 2.31 | 2.20 | 0.12 | 0.8703 |
| – Mid-Atlantic | 14.07 | 14.03 | 0.04 | 0.9816 |
| – Mountain | 4.62 | 4.78 | -0.15 | 0.8802 |
| – New England | 27.17 | 27.17 | 0.00 | 1.0000 |
| – Pacific | 6.94 | 6.90 | 0.04 | 0.9748 |
| – South Atlantic | 25.05 | 24.86 | 0.19 | 0.9262 |
| – West North Central | 0.96 | 0.96 | 0.00 | 1.0000 |
| – West South Central | 12.91 | 13.30 | -0.39 | 0.8130 |
| High-cost comorbidities | ||||
| – COPD | 5.78 | 5.97 | -0.19 | 0.8654 |
| – Smoking | 2.51 | 2.81 | -0.31 | 0.6956 |
| – Hypertension | 64.16 | 64.12 | 0.04 | 0.9867 |
| – Diabetes | 17.92 | 17.53 | 0.38 | 0.8333 |
| – CAD | 13.30 | 12.99 | 0.31 | 0.8490 |
| – Cancer | 0.19 | 0.15 | 0.04 | 0.8414 |
| – Obesity | 13.49 | 13.06 | 0.42 | 0.7941 |
CAD: Coronary artery disease; COPD: Chronic obstructive pulmonary disease; mTKA: Manual assisted total knee arthroplasty; rTKA: Robotic-arm assisted total knee arthroplasty.
EOC costs
Overall 90-day EOC costs for rTKA patients were found to be significantly less than that for mTKA patients (US$18,568 vs US$20,960). These amounts showed that rTKA patients had an 11% (US$2391) lower average cost associated with their 90-day post-index period of care (p < 0.0001) (Table 2). Although this analysis was examining payments from Medicare over the 90-day EOC (from index plus the 90-day post-index period), a CT-scan is required for the rTKA technology. Average hospital outpatient reimbursement for a CT was US$209 (including facility and physician payments); if included, we would still find overall savings of greater than US$2150.
| rTKA | mTKA | Difference | p-value | |
|---|---|---|---|---|
| Index facility costs | ||||
| – Index Costs | US$12,384 | US$13,024 | -US$640 | 0.0001† |
| Post 90-day costs by setting | ||||
| – Inpatient | US$12,075 | US$13,267 | -US$1192 | 0.4904 |
| – Outpatient | US$699 | US$839 | -US$141 | 0.0019† |
| – Emergency room | US$614 | US$736 | -US$122 | 0.1600 |
| – Skilled nursing facility | US$7201 | US$7947 | -US$746 | 0.0230† |
| – Home health | US$3045 | US$3536 | -US$491 | <0.0001† |
| Total post 90 days | US$5234 | US$6978 | -US$1744 | <0.0001† |
| Total EOC costs (index + 90-day post index) | US$18,568 | US$20,960 | -US$2391 | <0.0001† |
†Indicates statistically significant p-values.
‡This table only includes data for those who have costs in the expense category of interest.
EOC: Episode-of-care; mTKA: Manual assisted total knee arthroplasty; rTKA: Robotic-arm assisted total knee arthroplasty.
Index facility costs and length of stay
Overall index facility costs to the payer for rTKA patients were found to be significantly less than those for mTKA patients (US$12,384 vs US$13,024; p = 0.0001). These amounts for rTKA patients showed a 5% (US$640) lower cost associated with their index facility costs (Table 2). The index facility cost varied between hospitals, as DRG payments for the same procedure varies by hospital based on several factors including geographic wage index differences. In addition to the index facility cost findings, rTKA patients also experienced a significantly lower index LOS than the mTKA patients (1.84 vs 2.53 days; p < 0.0001).
Discharge disposition
Over 90% of patients in both cohorts utilized post-acute services, with rTKA accruing $1744 (25%) less costs than mTKA (US$5234 vs US$6978; p < 0.0001). Post-acute savings can be potentially attributed to rTKA patients being discharged to home health aid (56.65 vs 46.67%; p < 0.0001) or home with self-care (27.55% vs 23.62%; p = 0.0566) more frequently, and SNF less frequently (12.52% vs 21.70%; p < 0.0001). Table 3 presents a distribution of discharge status per cohort.
| Discharge code | Discharge disposition description | rTKA (%) | mTKA (%) | p-value |
|---|---|---|---|---|
| 06 | Home Health Aid (%) | 56.65 | 46.67 | <0.0001† |
| 01 | Home with Self-Care (%) | 27.55 | 23.62 | 0.0566 |
| 03 | Skilled Nursing Facility (%) | 12.52 | 21.70 | <0.0001† |
| 62 | Inpatient Rehabilitation (%) | 2.70 | 6.55 | 0.0007† |
†Indicates statistically significant p-values.
mTKA: Manual assisted total knee arthroplasty; rTKA: Robotic-arm assisted total knee arthroplasty.
Post-acute services
While over 90% of members in both cohorts utilized post-acute services (91.33 vs 93.6%; p = 0.0654), rTKA members utilized fewer post-acute services. Differences in utilization were most notable in the SNF and ER settings. The rTKA members were 47% less likely to have a SNF admission and 16% less likely to utilize ER services in the 90-day post-index period (13.68 vs 25.78%; p < 0.0001 and 11.18 vs 13.29%; p = 0.1726, respectively).
Among those members utilizing post-acute services, rTKA members experienced decreased post-index LOS and fewer visits. Most notably, rTKA members utilized fewer days in inpatient and SNF care (3.82 vs 6.93; p < 0.0001 and 14.8 vs 15.5; p = 0.0642), respectively. Aside from inpatient services, rTKA members also utilized fewer outpatient and HHA visits, with rTKA members having 17% fewer outpatient visits (3.00 vs 3.59; p = 0.0004), 13% fewer ER visits (1.09 vs 1.25; p = 0.3545) and 16% fewer HHA visits compared with mTKA (11.94 vs 14.28; p < 0.0001).
The aforementioned reductions in healthcare utilization resulted in decreased costs for the rTKA cohort. As previously noted, members in the rTKA cohort averaged US$1744 (25%) fewer costs overall than those in the mTKA cohort (US$5234 vs US$6978; p < 0.0001). In addition to statistically significant savings in the outpatient (US$699 vs US$839; p = 0.0019), SNF (US$7201 vs US$7947; p = 0.0230) and HHA settings (US$3045 vs US$3536; p < 0.0001), savings were also realized in the inpatient and ER settings. The rTKA members were also less likely to have costs for SNF admissions and ER visits when compared with mTKA (13.49 vs 25.55%; p < 0.0001 and 11.18 vs 13.26%; p = 0.1802, respectively). Table 2 presents the average costs by expense category among members of each cohort during the 90-day post-index period.
Readmissions
The rTKA patients had a significant 90-day readmission reduction of 33% (p = 0.0423), when compared with mTKA patients. Table 4 presents the findings for members who experienced an inpatient readmission during the 90-day post-index period.
| Cohort | Patients | Visits | Average LOS† | Readmission rate‡ | Average costs† |
|---|---|---|---|---|---|
| rTKA | 27 | 35 | 4.14 | 5.20% | US$10,570 |
| mTKA | 201 | 246 | 4.07 | 7.75% | US$9,696 |
| Difference | 0.07 | -2.54% | US$874 |
†Average LOS and average costs are at the patient level. LOS and costs were summed for patients that had more than one visit during the 90-day post-index period and averaged at the patient level.
‡p = 0.0423 for the difference in readmission rates between the two cohorts.
LOS: Length of stay; mTKA: Manual assisted total knee arthroplasty; rTKA: Robotic-arm assisted total knee arthroplasty.
Discussion
Although rTKA has been shown to have a number of advantages, one key element that has been missing from its evaluation to date is a comprehensive real-world cost analysis with actual cost data specifically related to EOC. Therefore, this study utilized a large Medicare database to compare the following outcomes between rTKA and mTKA patients: 90-day EOC costs; as well as several variables within the episode, including index costs; index LOS; discharge dispositions; and readmission rates. Our results indicate that rTKA patients had statistically significantly lower 90-day EOC costs. Contributions to these lower EOC costs were lower facility index costs, shorter LOS, higher likelihood that rTKA patients were discharged home (less likely to be discharged to SNF), as well as having lower readmission rates. Examination of post-acute services utilization showed that while more than 90% of members in both cohorts utilized post-acute services, rTKA members utilized fewer days in inpatient and SNF care as well as fewer outpatient and HHA visits, leading to decreased post-acute costs. Additional analysis of the index facility savings for rTKA revealed the savings was due to reduced DRG payments to Medicare for short-stay visits.
LOS and discharge location have been indicated in the peer-reviewed literature as predictors of post-discharge care and the associated costs [14]. Following TKA, Rossman et al. found that emergency department events were significantly less frequent among patients who were discharged earlier as well as those who were discharged home, while Keswani et al. found that patients discharged to a SNF or inpatient rehabilitation facility were significantly more likely to have unplanned readmissions or severe adverse events [15,16]. Additionally, others have found that patients discharged to SNF had higher odds of hospital readmission within 90 days of the index TKA compared with those discharged home (OR = 1.6; 95% CI: 1.1–2.4; p = 0.01).
These findings build on existing clinical literature on the use of rTKA. For example, one study of robotic-arm assisted versus mTKAs found that in-hospital, rTKA patients had less postoperative pain, fewer physiotherapy sessions and decreased hospital stay when compared with manual [11]. Our study also found a decreased length of stay as well as a reduction in overall utilization and an associated decreased in costs. Further, Kayani and colleagues evaluated soft tissue protection in the clinical setting between the two cohorts and found reduced bone and periarticular soft tissue injury in robotic-arm assisted patients compared with manual, which also may have contributed to the post-acute care and reduced costs [20]. Many of these advantages may be attributed to the enhanced pre-operative planning facilitated by the CT-scan based, 3D joint renderings that are necessary for the robotic-arm assisted TKA [5].
One of the potential cost-related concerns associated with robotic-arm assisted technology is the need for pre-operative CT-scans. Although the uses and advantages of the CT-scan for pre-operative planning and intra-operative surgeon feedback has been reported, there are still perceived cost concerns, as CT-scans are less commonly used for mTKA. However, CT-scans have been found to be significantly more sensitive (93 and 100%; p < 0.004) and accurate (95 and 99%; p < 0.001) in detecting bony deformities when compared with fixed flexion radiographs [17]. Additionally, CT-scan based pre-operative plans have been shown to increase accuracy and placement of implants [18], which are essential for successful outcomes [19]. Even when taking into consideration the added costs of a CT-scan, this study showed that the 90-day EOC to be significantly lower for rTKA patients, indicating that this enhanced imaging modality did not contribute to net higher overall healthcare costs to patients and payers in this setting.
This study is not without limitations. As a large administrative claims database study, it is difficult to precisely identify the desired study population of interest as well as their clinical progressions. Specific to our study, identifying patients who underwent rTKA based on coding for a CT-scan performed 60 days prior to TKA at an outpatient setting substantially reduced the number of patients who could be included for analysis. The sample size was also limited, as the study time period was early in the adoption for rTKA in the US and the Medicare SAF data had a significant lag between the provision of services and the availability of the data. Additionally, it is possible that some of the cases identified had been incorrectly coded, although the literature tells us this would only be likely in a small minority of cases [21]. In addition, other clinical factors, such as the type and duration of anesthesia, the anticoagulation prescribed, and other risk factors were not assessed. However, we performed a propensity score match in order to account for age, sex, race, geographic region and high-cost comorbidities with the goal of minimizing confounding factors between study cohorts. This study evaluated all-cause readmissions, consistent with Medicare's definition in their Bundled Payment Programs. Future studies could analyze individual causes for readmission or more specific complications (e.g., pin-site infections, periprosthetic fractures, etc.). Unfortunately, the dataset in our analysis does not provide the level of granularity needed to facilitate a specific evaluation of pin-site complications, however existing literature shows the incidence with similar fixation types to be as low as 0.065 to 0.64% [22,23]. Finally, this analysis examined the economic impact of rTKA to a payer and did not account for capital equipment investment(s) or the pre-operative CT-scan. Aside from these limitations, this study is still valuable for patients and payers as it is a large, properly powered study with strict inclusion criteria and compares 90-day EOC, as well as potentially contributing cost-related factors between rTKA and mTKA patients.
Conclusion
In conclusion, the results from this study show rTKA to be associated with significantly lower 90-day EOC costs. These lower rTKA patient costs are likely attributable to the significantly lower index costs, increased likelihood of being discharged to home shorter LOS and decreased readmission rates, when compared with mTKA patient costs. Additional contributing factors may include a number of robotic-arm assisted clinical, radiographic and patient outcome advantages. Future studies should build on these findings by performing hospital and surgeon-specific cost analyses as well as an analysis from the provider perspective. Additionally, these data can stimulate further discussions regarding healthcare cost-containment with operating-room technology utilization. Based on our results, robotic-arm assisted surgery appears to be cost-effective and provide added value for payers. As a result of these findings, robotic-arm assisted surgery can be an effective tool in managing existing value-based care programs while also offering value given its potential to promote efficiencies through the EOC journey.
Future perspective
Robotic surgery, in its more primitive forms, has been around for over two decades. Historically, many people questioned the future of such technology, much as they questioned the future of automation in factories and the value of autopilot in aircraft. However, robotics has demonstrated an ability to improve consistency and decrease variability in various industries. As robotics is growing as a valuable adjunct to the surgeon in optimizing patient-specific arthroplasty, we suspect that its role will continue to expand as the benefit to value-based care continues to develop. Robotics, coupled with 3-dimensional patient specific imaging, has the potential to bring widespread change to joint replacement, reducing component placement errors, reducing soft tissue damage and by catalyzing further innovations in implant design and development. Alongside this, we also see a growing population of joint replacement candidates, an expanding self-insured employer market, and the need to contain costs, produce efficiencies and improvements in care, quality of life, and outcomes. Robotics is well-positioned as a tool to help achieve these goals. It is difficult to predict the array of technological innovations that will be used to transform robotic assisted arthroplasty and additional research is required to fully define the costs, possible capabilities, and benefits of surgical robotics. Considering the clinical and economic advancements we are seeing with robotic surgery today, in a time where there is increasing focus on reducing healthcare costs while improving patient experience, satisfaction and outcomes, it is clear that robotic surgery is here to stay.
The prevalence of knee osteoarthritis (OA) has roughly doubled since the middle of the 20th century, driving the growing demand and volume for total knee arthroplasty (TKA), the gold standard procedure for end-stage knee OA.
As a result, the overall costs associated with TKA contribute substantial financial burdens on payers.
Robotic-arm assisted TKA (rTKA), a technological advancement, has been introduced as an alternative to manual TKA (mTKA) to help enhance clinical, radiographic and patient-reported outcomes.
Clinical evidence for rTKA compared with mTKA has demonstrated accuracy, precision to plan and assistance in soft-tissue protection, which can largely be attributed to the enhanced pre-operative planning and haptic guidance required for rTKA procedures.
TKA has already been shown to be cost-effective for patients, but the potential value added from an rTKA device has yet to be determined.
This study is the first of its kind to conduct a comprehensive economic analysis between rTKA and mTKA.
This economic analysis showed that use of rTKA yielded statistically significantly lower costs in the overall 90-day episode-of-care period.
Post-acute savings for rTKA were driven by rTKA experiencing fewer readmissions and an economically beneficial discharge destination.
rTKA utilized fewer post-index services overall than mTKA, ultimately reducing the costs for the rTKA in the 90-day episode.
Study results presented herein can assist managed care decision-makers to identify a cost-sparing way to manage patients who need to undergo TKA.
Acknowledgments
The authors would like to thank D Gregory, K Needham and L Stradford for their assistance with study conceptualization and data analysis.
Financial & competing interests disclosure
Funding for this study was provided by Stryker Orthopaedics (Mahwah, NJ), which develops and manufactures orthopedic products, and provided input on the study design, data collection, analysis and interpretation. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementaryappendix.xlsx)
- Download
- 16.65 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Deshpande BR, Katz JN, Solomon DH et al. The number of persons with symptomatic knee osteoarthritis in the United States: impact of race/ethnicity, age, sex, and obesity. Arthritis Care Res. 68, 1743–1750 (2016).
2.
Sloan M, Premkumar A, Sheth NP. Projected volume of primary total joint arthroplasty in the US, 2014 to 2030. JBJS 100(17), 1455–1460 (2018).
3.
Mont MA, Khlopas A, Chughtai M, Newman JM, Deren M, Sultan AA. Value proposition of robotic total knee arthroplasty: what can robotic technology deliver in 2018 and beyond? Expert Rev. Med. Dev. 15(9), 619–630 (2018).
4.
Khlopas A, Sodhi N, Sultan AA, Chughtai M, Molloy RM, Mont MA. Robotic arm-assisted total knee arthroplasty. J. Arthroplasty 33(7), 2002–2006 (2018).
5.
Marchand RC, Sodhi N, Bhowmik-Stoker M et al. Does the robotic arm and preoperative ct planning help with 3D intraoperative total knee arthroplasty planning? J. Knee Surg. (2018).
•• The use of robotic arm-assisted (rTKA) and preoperative computerized tomography (CT) planning provides substantial assistance with intraoperative planning and accurate prediction of implant sizes, demonstrating 95% of femoral and 99% of tibial prostheses sizes to be accurately predicted within one size of what was implanted.
6.
Khlopas A, Chughtai M, Hampp EL et al. Robotic-arm assisted total knee arthroplasty demonstrated soft tissue protection. Surg. Technol. Int. 30, 441–446 (2017).
7.
Hampp EL, Chughtai M, Scholl LY et al. Robotic-arm assisted total knee arthroplasty demonstrated greater accuracy and precision to plan compared with manual techniques. J. Knee Surg. (2018).
8.
Sultan AA, Piuzzi N, Khlopas A, Chughtai M, Sodhi N, Mont MA. Utilization of robotic- arm assisted total knee arthroplasty for soft tissue protection. Expert Rev. Med. Dev. 14(12), 925–927 (2017).
9.
Sodhi N, Khlopas A, Piuzzi NS et al. Erratum to: the learning curve associated with robotic total knee arthroplasty. J. Knee Surg. 31(04), 370 (2018).
10.
Marchand RC, Sodhi N, Khlopas A et al. Patient satisfaction outcomes after robotic arm-assisted total knee arthroplasty: a short-term evaluation. J. Knee Surg. 30(09), 849–853 (2017).
•• Short-term patient satisfaction outcomes collected at 6 months postoperatively between rTKA and mTKA patients demonstrate that rTKA patients were found to have significantly better WOMAC total and pain scores (p < 0.05), highlighting the potential of rTKA to improve total satisfaction scores, alongside pain and physical function.
11.
Kayani B, Konan S, Tahmassebi J, Pietrzak JRT, Haddad FS. Robotic-arm assisted total knee arthroplasty is associated with improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based total knee arthroplasty. Bone Joint J. 100(7), 930–937 (2018).
• A prospective cohort study comparing early postoperative functional outcomes and time to hospital discharge between conventional TKA and rTKA, highlighting that rTKA is associated with decreased pain, improved early functional recovery and reduced time to hospital discharge.
12.
Morgan L. US healthcare annual spending estimated to rise by 5.8% on average through 2024. Am. Health Drug Benefits 8(5), 272 (2015).
13.
Waimann CA, Fernandez-Mazarambroz RJ et al. Cost–effectiveness of total knee replacement: a prospective cohort study. Arth. Care Res. 66(4), 592–599 (2014).
14.
Tarity TD, Swall MM. Current trends in discharge disposition and post-discharge care after total joint arthroplasty. Curr. Rev. Musculoskelet. Med. 10(3), 397–403 (2017).
15.
Rossman SR, Reb CW, Danowski RM, Maltenfort MG, Mariani JK, Lonner JH. Selective early hospital discharge does not increase readmission but unnecessary return to the emergency department is excessive across groups after primary total knee arthroplasty. J. Arthroplast. 31, 1175–1178 (2016).
16.
Keswani A, Tasi MC, Fields A, Lovy AJ, Moucha CS, Bozic KJ. Discharge destination after total joint arthroplasty: an analysis of postdischarge outcomes, placement risk factors, and recent trends. J. Arthroplast. 31, 1155–1162 (2016).
17.
Segal NA, Nevitt MC, Lynch JA, Niu J, Torner JC, Guermazi A. Diagnostic performance of 3D standing CT imaging for detection of knee osteoarthritis features. Phys. Sportsmed. 43(3), 213–220 (2015).
•• This analysis was a prospective study that observed 20 patients and compared standing computerized tomography (SCT) to magnetic resonance imaging (MRI) as the reference standard. The results indicate that SCT has greater sensitivity and accuracy in detecting bony deformities when compared with fixed flexion radiographs.
18.
Hampp EL, Scholl LY, Prieto M et al. Robotic-arm assisted total knee arthroplasty demonstrated greater accuracy to plan compared to manual technique. Orthopaed. Proc. 99-B(Suppl. 20), 44 (2017).
• This study, which observed 12 cadaver knees, exhibited that when compared with manual TKA, robotic-assisted TKA demonstrated more accurate and precise bone cuts and implant positioning to plan.
19.
Abdel MP, Parratte S, Budhiparama NC. The patella in total knee arthroplasty: to resurface or not is the question. Curr. Rev. Musculoskelet. Med. 7(2), 117–124 (2014).
20.
Kayani B, Konan S, Pietrzak JRT, Haddad FS. Iatrogenic bone and soft tissue trauma in robotic-arm assisted total knee arthroplasty compared with conventional jig-based total knee arthroplasty: a prospective cohort study and validation of a new classification system. J. Arthroplasty 33(8), 2496–2501 (2018).
21.
Gologorsky Y1, Knightly JJ, Lu Y, Chi JH, Groff MW. Improving discharge data fidelity for use in large administrative databases. Neurosurg. Focus. 36(6), E2 (2014).
22.
Brown MJ, Matthews JR, Bayers-Thering MT, Phillips MJ, Krackow KA. Low incidence of postoperative complications with navigated total knee arthroplasty. J. Arthroplasty 32(7), 2120–2126 (2017).
23.
Kamara E, Berliner Z, Hepinstall M, Cooper H. Pin site complications associated with computer-assisted navigation in hip and knee arthroplasty. J. Arthroplasty 32(9), 2842–2846 (2017).
Information & Authors
Information
Published In
Copyright
© 2019 Baker Tilly.
History
Received: 28 November 2018
Accepted: 10 January 2019
Published online: 28 January 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A 90-day episode-of-care cost analysis of robotic-arm assisted total knee arthroplasty. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0136
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Warran Wignadasan, Andreas Fontalis, Abdulellah Alsheddi, Jenni Tahmassebi, Nishma Patel, Elena Pizzo, Fares S. Haddad, Cost-utility analysis of robotic and conventional total knee arthroplasty: A 200-patient micro-costing study in a public sector institution, Journal of Robotic Surgery, 10.1007/s11701-026-03658-1, 20, 1, (2026).
- Adam M. Gordon, Chase W. Smitterberg, David Jacofsky, Michael A. Mont, Robotic-assisted total knee arthroplasty associated with lower odds of vascular injury: A retrospective cohort analysis, Journal of Clinical Orthopaedics and Trauma, 10.1016/j.jcot.2026.103452, 77, (103452), (2026).
- Lars‐Rene Tuecking, Marco Ezechieli, Christoph Barkhausen, Christian Hendrich, Lea Charlotte Wienholt, Christoph Pross, Rüdiger von Eisenhart‐Rothe, Henning Windhagen, Reduced length of stay and improved perioperative outcomes in robotic‐arm‐assisted TKA: A real‐world evidence study of 63,931 cases from German hospitals, Knee Surgery, Sports Traumatology, Arthroscopy, 10.1002/ksa.70437, (2026).
- David Maman, Yaniv Steinfeld, Yaron Berkovich, In-hospital outcomes and hospital charges after robotic-assisted versus conventional total knee arthroplasty: A 2016–2022 Nationwide Inpatient Sample study, PLOS One, 10.1371/journal.pone.0346031, 21, 4, (e0346031), (2026).
- Amir Ghafarian, Muaaz Wajahath, Noah Hodson, Jawad Saad, Ali Mehaidli, Clinical and mechanical outcomes of robotic-assisted versus conventional total knee arthroplasty: a retrospective propensity-matched analysis of 163,516 patients, Journal of Orthopaedic Surgery and Research, 10.1186/s13018-026-06770-y, 21, 1, (2026).
- Steve Nishiyama, John Walsh, Imageless Robotic-Assisted Total Knee Arthroplasty – Review of Current Technologies and Techniques, Innovations in Knee Surgery - Contemporary Approaches to Arthroplasty, Preservation, and Sports Medicine [Working Title], 10.5772/intechopen.1014777, (2026).
- Zheng Liu, Dongyang Chen, Weijun Wang, Jin Dai, Xiaofeng Zhang, Jianghui Qin, Kai Song, Xinhua Li, Jing Han, Qing Chang, Miaofeng Zhang, Chenxi Xue, Huanyu Zhang, Jun Lu, Lidong Wu, Yunfeng Yao, Lan Li, Zhihong Xu, Qing Jiang, The LANCET robotic system improves radiographic alignment and prosthesis positioning in TKA: a multicenter, prospective controlled clinical trial, Advanced Orthopaedics, 10.1016/j.advop.2026.02.001, (2026).
- Zenat A. Khired, Manal Mohamed Elhassan Taha, Mapping the integration of artificial intelligence in knee replacement surgery: a data-driven bibliometric analysis with emphasis on robotic innovation, Journal of Robotic Surgery, 10.1007/s11701-025-03103-9, 20, 1, (2026).
- Yasushi Oshima, Tokifumi Majima, Robotic-Assisted Total Knee Arthroplasty With Metal Block Augmentation for Severe Varus Knee With Tibial Defect, Arthroplasty Today, 10.1016/j.artd.2025.101915, 36, (101915), (2025).
- Christopher Katchis, Bryan Ang, Emil Haikal, Kisan Patel, Renaud Lafage, Virginie Lafage, James Slover, Impact of robotic assistance on hospital stay direct costs of total knee arthroplasty, Journal of Robotic Surgery, 10.1007/s11701-025-02828-x, 19, 1, (2025).
- See more