Using flowable gelatin in anterior cervical spine surgery in real-world practice: a retrospective cohort study
Abstract
Aim: To assess the clinical and economic impact of flowable gelatin hemostatic matrix (FGHM) in anterior cervical spine surgery (ACSS). Patients & methods: A total of 451 patients with performed ACSS were included to compare FGHM with conventional hemostatic methods for clinical and cost outcomes using propensity score matching method. Results: The comparisons of the matched 125 pairs observed that FGHM was associated with significantly lower blood transfusion volume (11.2 vs 36.3 ml; p = 0.039), shorter postsurgery hospital stay length (3.7 vs 4.7 days; p = 0.002), shorter operation time (103.5 vs 117.7 min; p = 0.004), lower drainage placement rate (51.2 vs 89.6%; p < 0.001) and also lower total hospital costs (median ¥64,717 vs ¥65,064; p = 0.035). Conclusion: Use of FGHM in ACSS improved perioperative outcomes without increasing hospital costs.
Anterior approach is the most common cervical spine surgery technique [1]. One of the difficulties during anterior cervical spine surgery (ACSS) is to stop the epidural venous oozing. If hemostasis is not achieved promptly, the reduced surgical visual field could result in higher risk of iatrogenic injury on nerve and longer operation time [2]. Also, studies have demonstrated that massive blood loss is associated with mortality and utilizing more health resource [3,4]. Therefore, many hemostatic measures have been implemented to control bleeding of epidural venous plexus. Adjunctive absorbable hemostatic agents, such as oxidized regenerated cellulose, gelatin sponge and collagen sponge have been used in ACSS for many years [4–6]. However, these products are difficult to position in the deep, narrow and suboptimally visualized bleeding sites during ACSS procedures [7].
The absorbable and flowable gelatin hemostatic matrix (FGHM) SURGIFLO® was approved by the China Food and Drug Administration in 2011. It stops bleeding by accelerating blood clot formation with the gelatin matrix and is able to reach difficult-to-access bleeding sites due to its flowable property. Many studies [8–10] have investigated the efficacy on hemostasis in various surgeries using FGHM preloaded with thrombin, including few clinical reports regarding the use of FGHM in spinal surgery [11,12]. A randomized clinical trial showed that the hemostasis efficacy of flowable gelatin matrix in posterior spinal fusion for idiopathic scoliosis decreased intraoperative blood loss by 30% [11]. A multicenter prospective clinical trial demonstrated that the efficacy of flowable gelatin matrix (Proceed) on hemostasis for different bleeding sites during spine surgery [12]. However, the literature lacks research on FGHM in ACSS and regarding related economic outcomes. Additionally, the real-world evidence clarifying the hemostatic effects of FGHM in Chinese patients with ACSS was lacking and using health economic evidence from western countries to support reimbursement decision making in China has become challengeable. Thus, we conducted this study to assess the impact of FGHM hemostatic matrix (SURGIFLO) in ACSS on the perioperative clinical outcomes associated with hemostasis and direct hospital costs in a Chinese tertiary hospital.
Patients & methods
This was a retrospective study including patients who underwent ACSS for cervical degenerative disease at a single institution from January 2014 to December 2016. The research proposal of this study was reviewed and approved by the research ethics board in the study institution.
Data source & extraction
The medical and billing records were exported from the hospital electronic database. The hospital database contains information on patient demographics, socioeconomic status, first and final diagnosis as well as comorbidities. The laboratory test records were used for screening patient's baseline of coagulation function one day before operation. The surgical records provided information on operation time, type of procedure, operation site, volume of blood loss as well as autologous and allogeneic blood transfusion during surgery. The medical notes included records of operation-related complications. The postoperative length of stay (LOS) was calculated as the date difference between surgery and discharge. The exported billing records were summed to provide total direct cost. To allow further analysis, all charge details were clustered into 15 cost categories: topical absorbable hemostatic (TAH) agent, implanted devices for fixation, medicine, disposable supplies, blood transfusion, hospital bed, medical image, laboratory tests, anesthesia, operation, other therapy, nursing service, personal care, in-hospital dining and others.
Patient selection
Generally, FGHM is applied to the bleeding that cannot be adequately controlled by traditional hemostatic agents, which leads to the higher risk of bleeding associated with utilization of FGHM. This clinical practice could confound the hemostatic effects of FGHM compared with traditional hemostatic agents after the introduction of FGHM (January 2015). Thus, this study included patients who underwent ACSS in 2014 to create the historical control group (HC), whereas the FGHM group was created by including patients who underwent ACSS with the utilization of FGHM in 2015 and 2016. This study identified patients using the following two inclusion criteria: operation position was between C2 and C6; operation procedure was anterior cervical corpectomy with fusion or anterior cervical discectomy with fusion. Additionally, this study used the following exclusion criteria to control potential bias: applied thrombin prior to or during operation; history of spinal surgery; operation for nondegenerative diseases, such as trauma, tumor, or infection; other irrelevant operations during the same hospital episode for ACSS; multiple surgical sites unrelated to ACSS; insufficient information for analysis.
Statistical analysis
Individuals usually differ in various baseline characteristics, such as type of procedures and number of fusion cages, which could directly affect postoperative outcomes, resulting in biased estimation on effect. To manage this bias, propensity score matching was applied. The confounders were identified by the unadjusted baseline comparison between groups using Student's t-test (for continuous variables) and Fisher exact test (for categorical variables). The 1:1 matched groups for FGHM versus HC were created by using greedy approach with criteria of propensity score difference less than 0.001. After the matching, all nonmatched cases from the database were discarded and the matched cases were used for further statistical analysis.
The matched groups were compared with the surgical outcomes and distribution of hospital costs using a paired t-test for continuous outcomes, McNemar test for dichotomous outcomes and Wilcoxon signed rank test for the distribution of hospital costs. Additionally, conventional regression analyses with adjustment for patient baseline characteristics were conducted to confirm the adjusted comparisons of measured outcomes related to blood transfusion and hospital costs. These regression analyses included logistic regression analysis for risk of blood transfusion, linear regression analysis for blood transfusion volume and generalized linear regression for hospital costs. Statistical software SAS 9.2 was used to conduct the data analysis described above and the statistical significance was defined as the two-sided p-value less than 0.05.
Results
The hospital (ward II and III, Department of Orthopedics) identified 425 patients in 2014 and 930 patients in 2015 and 2016, who had the diagnosis of cervical spondylopathy and were treated by surgery. According to the inclusion and exclusion criteria, 186 patients were included in the HC group and 265 patients were included in the FGHM group. The details of patient inclusion and exclusion are illustrated in Figure 1.
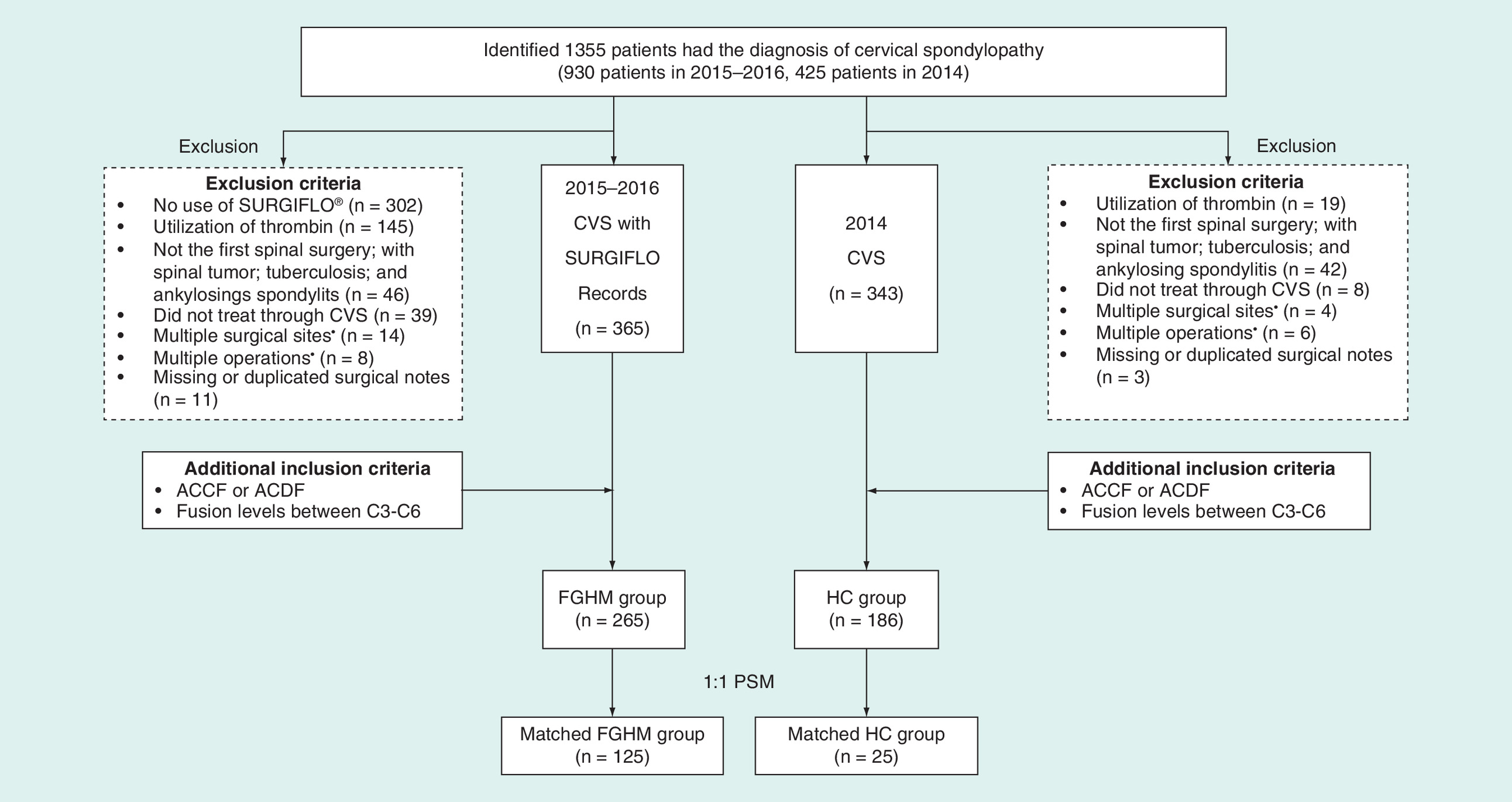
Figure 1. The patient flow of the study.
ACCF: Anterior cervical corpectomy fusion; ACDF: Anterior cervical discectomy fusion; CVS: FGHM: Flowable gelatin hemostatic matrix HC: Historical control.
Baseline comparison before propensity score matching
The patient baseline characteristics associated with FGHM and HC before and after propensity score matching are summarized in Table 1. The direct comparisons of patient baseline characteristics of two created groups (FGHM vs HC) observed significant differences in the distributions of gender (male: 59.2 vs 72.0%; p = 0.005), employment status (full-time employment: 27.9 vs 54.3%; p < 0.001; unemployed: 35.1 vs 14.0%; p < 0.001), normal international normalized ratio (93.5 vs 97.8%; p = 0.040) and the distribution of surgery procedures (ACCF: 15.8 vs 31.2%; p < 0.001; anterior cervical discectomy with fusion: 84.2 vs 68.8%; p < 0.001). Additionally, the two groups were different in the distribution of the utilization of fusion cages (two cages: 42.6 vs 27.4%; p = 0.001; more than two cages: 9.1 vs 2.7%; p = 0.006) and titanium mesh (1.5 vs 14.5%; p < 0.001). These characteristics were included to develop propensity score calculation formula and then to identify 125 propensity score-matched pairs with well-balanced patient baseline characteristics for FGHM versus HC.
| Variable | Mean ± SD/% | p-value | Mean ± SD/% | p-value | ||
|---|---|---|---|---|---|---|
| FGHM group (n = 265) | HC group (n = 186) | Matched FGHM group (n = 125) | Matched HC group (n = 125) | |||
| Patient characteristics | ||||||
| Gender (males) | 59.2 | 72 | 0.005 | 67.2 | 67.2 | 1.000 |
| Age (years) | 52.9 ± 10.0 | 52.1 ± 10.1 | 0.384 | 52.0 ± 9.5 | 51.3 ± 10.3 | 0.594 |
| BMI (kg/m2) | 25.3 ± 3.6 | 26.6 ± 10.7 | 0.087 | 25.7 ± 3.9 | 26.9 ± 12.8 | 0.273 |
| Full-time employment | 27.9 | 54.3 | <0.001 | 47.2 | 45.6 | 0.480 |
| Unemployed | 35.1 | 14.0 | <0.001 | 23.2 | 17.6 | 0.296 |
| Local public health insurance | 17.4 | 14.0 | 0.363 | 12.8 | 12.8 | 1.000 |
| Out-of-pocket costs for medical expenses | 81.9 | 84.9 | 0.444 | 86.4 | 86.4 | 1.000 |
| Drinking | 9.1 | 11.3 | 0.524 | 10.4 | 12.8 | 0.700 |
| Smoking | 23.0 | 26.9 | 0.375 | 23.2 | 24.8 | 0.877 |
| Normal INR | 93.5 | 97.8 | 0.040 | 98.4 | 98.4 | 1.000 |
| Normal hemoglobin | 86.8 | 90.0 | 0.231 | 84.0 | 92.0 | 0.089 |
| Normal erythrocytes | 96.2 | 98.4 | 0.255 | 94.4 | 98.4 | 0.182 |
| Cardiovascular comorbidity | 11.7 | 17.7 | 0.076 | 11.2 | 17.6 | 0.230 |
| Cerebral infarction comorbidity | 1.1 | 3.8 | 0.100 | 0.0 | 5.6 | 0.265 |
| Previous antiplatelet/coagulants agents | 1.9 | 1.6 | 1.000 | 2.4 | 0.8 | 0.617 |
| Treatment | ||||||
| ACCF | 15.8 | 31.2 | <0.001 | 16.8 | 17.6 | 1.000 |
| ACDF | 84.2 | 68.8 | <0.001 | 83.2 | 82.4 | 1.000 |
| Number of operated vertebral levels | 2.8 ± 0.7 | 2.7 ± 0.7 | 0.372 | 2.7 ± 0.7 | 2.7 ± 0.7 | 0.914 |
| C4/C5 | 5.7 | 5.9 | 1.000 | 7.2 | 8.8 | 0.823 |
| C5/C6 | 24.5 | 28 | 0.446 | 31.2 | 26.4 | 0.417 |
| C6/C7 | 6.8 | 7.5 | 0.853 | 7.2 | 10.4 | 0.502 |
| C3/C4/C5 | 4.2 | 6.5 | 0.285 | 4.0 | 4.8 | 1.000 |
| C4/C5/C6 | 26.0 | 21.5 | 0.315 | 22.4 | 20.0 | 0.728 |
| C5/C6/C7 | 16.2 | 16.1 | 1.000 | 16.0 | 17.6 | 0.850 |
| C3/C4/C5/C6 | 8.3 | 4.8 | 0.187 | 6.4 | 4.8 | 0.773 |
| C4/C5/C6/C7 | 7.5 | 8.6 | 0.726 | 4.8 | 5.6 | 1.000 |
| C3/C4/C5/C6/C7 | 0.8 | 1.1 | 1.000 | 0.8 | 1.6 | 1.000 |
| Number of cages = 0 | 0.4 | 12.9 | <0.001 | 0.0 | 3.2 | 0.502 |
| Number of cages = 1 | 47.9 | 57.0 | 0.069 | 59.2 | 57.6 | 0.803 |
| Number of cages = 2 | 42.6 | 27.4 | 0.001 | 36.8 | 36.0 | 1.000 |
| Number of cages >2 | 9.1 | 2.7 | 0.006 | 4.0 | 3.2 | 1.000 |
| Number of implanted cages | 1.6 ± 0.7 | 1.2 ± 0.7 | <0.001 | 1.4 ± 0.6 | 1.4 ± 0.6 | 0.145 |
| Utilization of titanium mesh | 1.5 | 14.5 | <0.001 | 2.4 | 2.4 | 1.000 |
ACCF: Anterior cervical corpectomy fusion; ACDF: Anterior cervical discectomy fusion; BMI: Body mass index; FG: Flowable gelatin; HC: Historical control; INR: International normalized ratio; SD: Standard deviation.
Adjusted comparisons of FGHM versus HC for perioperative outcomes
All matched patients used gelatin sponges for hemostasis during operation. However, the utilization of gelatin sponges was significantly less in matched FGHM patients (3.0 ± 1.3 vs 4.0 ± 1.1 bags; p < 0.001). The average use of FGHM in the matched patients was 1.0 unit (SD 0.1). The comparisons of the measured outcomes for matched FGHM versus matched HC observed lower blood transfusion volume (11.2 ± 62.5 vs 36.3 ± 115.4 ml; p = 0.039), shorter operation time (103.5 ± 35.0 vs 117.7 ± 39.6 min; p = 0.002), shorter postsurgery LOS (3.7 ± 1.9 vs 4.7 ± 3.1 days; p = 0.004), and lower rate of drainage tube placement (51.2 vs 89.6%; p < 0.001), slight but nonsignificant decrease in intraoperative transfusion risk (3.2 vs 9.6%; p = 0.080). The results of the comparisons of surgical outcomes are summarized in Table 2. Multiple regression analysis with the adjustment for surgery procedure (anterior cervical corpectomy with fusion), operation site (C5 + C6), comorbidities and utilization of titanium mesh observed statistical significance for lower intraoperative blood transfusion risk (odds ratio 0.428; p = 0.032) but not for lower intraoperative blood transfusion volume (coefficient -18.319; p = 0.137) in patients with the utilization of FGHM (Figure 2).
| Variable | Mean ± SD/% | p-value | |
|---|---|---|---|
| Matched FGHM group (n = 125) | Matched HC group (n = 125) | ||
| TAH agents | |||
| SURGIFLO (units) | 1.0 ± 0.1 | – | |
| Gelatin sponges (bags) | 3.0 ± 1.3 | 4.0 ± 1.1 | <0.001 |
| Operation time (min) | 103.5 ± 35.0 | 117.7 ± 39.6 | 0.002 |
| Hospital stay length (days) | 6.9 ± 2.6 | 9.0 ± 3.7 | <0.001 |
| Postoperative LOS (days) | 3.7 ± 1.9 | 4.7 ± 3.1 | 0.004 |
| Intraoperative blood loss and transfusion | |||
| Blood loss (ml) | 61.0 ± 59.9 | 71.6 ± 55.2 | 0.157 |
| Blood transfusion rate | 3.2 | 9.6 | 0.080 |
| Blood transfusion volume (ml) | 11.2 ± 62.5 | 36.3 ± 115.4 | 0.039 |
| Drain output | |||
| Drainage tube placement rate | 51.2 | 89.6 | <0.001 |
| Duration of placed drainage tube (days) | 1.6 ± 1.8 | 1.3 ± 0.7 | 0.455 |
| Total drain output (ml) | 93.4 ± 428.5 | 33.2 ± 83.7 | 0.374 |
| Perioperative complication | 0.8 | 0.0 | 1.000 |
Transfusion: refers the total volume of autologous blood, allogeneic red blood cell, platelet, plasma and whole blood. Transfusion threshold stays the same during year 2014–2016.
FGHM: Flowable gelatin hemostatic matrix; HC: Historical control; LOS: Length of stay; SD: Standard deviation; TAH: Topical absorbable hemostatic agent.
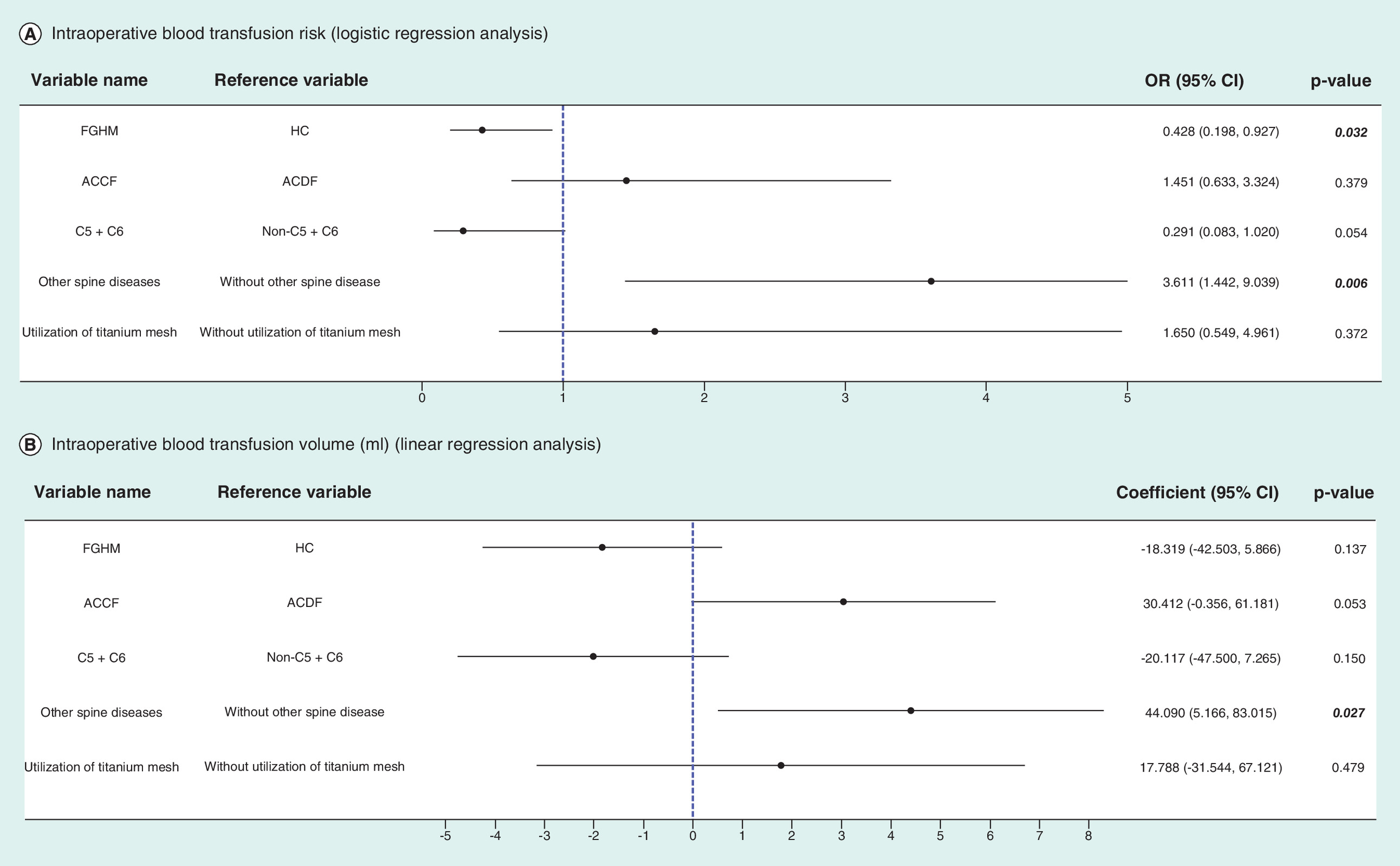
Figure 2. Risk factors of intraoperative transfusion by regression analysis.
ACCF: Anterior cervical corpectomy fusion; ACDF: Anterior cervical discectomy fusion; CI: Confidence interval; FGHM: Flowable gelatin hemostatic matrix HC: Historical control; OR: Odds ratio.
Adjusted comparisons of the distribution of hospital costs for matched groups
The allocation of costs for two matched groups is summarized in Table 3. The utilization of FGHM significantly increased the costs of TAH agents (median ¥3105 vs ¥60; p < 0.001; average currency exchange during 2014 to 2016: US$1=¥6.3378) for the matched patients. However, in the matched FGHM group, significantly lower other categories of hospital costs were observed, including disposable medical consumables (median ¥5353 vs ¥7325; p < 0.001), nursing (median ¥420 vs ¥876; p < 0.001), laboratory tests (median ¥2070 vs ¥2225; p = 0.021), and hospital bed (median ¥342 vs ¥482; p < 0.001). Therefore, the total reduced medical costs except TAH and implanted fixation in the matched FGHM patients was ¥2906 (median). The total hospital costs associated with the matched FGHM patients was lower than that in the matched HC patients with statistical significance (median ¥64,717 vs ¥65,064; p = 0.035). The results from generalized linear regression with adjustment for demographics, social economic status, lifestyle, type of procedure, operation site, utilization of fusion cage and titanium mesh and comorbidities were consistent with propensity score matching results: significantly lower total hospital costs subtracted cost of TAH and of implanted fixation (coefficient -0.050; p = 0.022) (Figure 3).
| Variables | Matched FGHM group (n = 125) | Matched HC group (n = 125) | p-value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Q1 | Q3 | SD | Mean | Median | Q1 | Q3 | SD | ||
| TAH | 3155 | 3105 | 3095 | 3120 | 382 | 60 | 60 | 45 | 60 | 17 | <0.001 |
| Gelatin sponge | 61 | 50 | 50 | 75 | 29 | 60 | 60 | 45 | 60 | 17 | 0.944 |
| SURGIFLO® | 3094 | 3045 | 3045 | 3045 | 384 | 0 | 0 | 0 | 0 | 0 | <0.001 |
| Implanted fixation | 46,877 | 43,127 | 37,617 | 53,291 | 12,296 | 44,369 | 43,226 | 36,567 | 50,821 | 11,070 | 0.008 |
| Disposable supplies | 5368 | 5353 | 3365 | 6323 | 2236 | 7443 | 7325 | 5880 | 9391 | 2616 | <0.001 |
| Nursing | 467 | 420 | 182 | 629 | 337 | 777 | 876 | 526 | 980 | 382 | <0.001 |
| Laboratory tests | 2254 | 2070 | 1702 | 2481 | 927 | 2397 | 2225 | 1921 | 2674 | 752 | 0.021 |
| Hospital bed | 420 | 342 | 258 | 538 | 251 | 560 | 482 | 314 | 678 | 359 | <0.001 |
| Operation | 3049 | 3061 | 2797 | 3097 | 310 | 3258 | 3153 | 2975 | 3396 | 552 | <0.001 |
| In-hospital dining | 139 | 131 | 58 | 184 | 116 | 183 | 166 | 103 | 247 | 114 | <0.001 |
| Other therapy | 129 | 114 | 97 | 142 | 62 | 191 | 140 | 122 | 174 | 401 | <0.001 |
| Personal care | 12 | 3 | 2 | 18 | 16 | 18 | 9 | 3 | 29 | 21 | 0.009 |
| Blood transfusion | 30 | 0 | 0 | 0 | 175 | 49 | 0 | 0 | 67 | 108 | <0.001 |
| Medical image | 1529 | 1331 | 984 | 2023 | 824 | 1155 | 1021 | 850 | 1451 | 606 | <0.001 |
| Anesthesia | 545 | 558 | 531 | 586 | 69 | 524 | 558 | 503 | 586 | 106 | 0.341 |
| Medicine | 6043 | 5481 | 4543 | 6620 | 3864 | 5670 | 5286 | 4485 | 6959 | 1808 | 0.769 |
| Others | 17 | 4 | 4 | 4 | 25 | 26 | 4 | 4 | 49 | 53 | 0.087 |
| Hospital costs, except TAH and implant fixation | 20,002 | 19,214 | 17,115 | 21,616 | 6070 | 22,251 | 22,120 | 18,394 | 25,418 | 5033 | <0.001 |
| Hospitalization cost, except implant fixation | 23,157 | 22,345 | 20,205 | 24,743 | 6134 | 22,311 | 22,165 | 18,454 | 25,463 | 5035 | 0.452 |
| Total hospital costs | 70,034 | 64,717 | 58,767 | 78,034 | 14,779 | 66,680 | 65,064 | 57,573 | 74,510 | 13,402 | 0.035 |
Average currency exchange during 2014 to 2016: US$1 ≈ ¥6.3378.
p-value: Wilcoxon test.
FGHM: Flowable gelatin hemostatic matrix; HC: Historical control; SD: Standard deviation; TAH: Topical absorbable hemostatic agent.
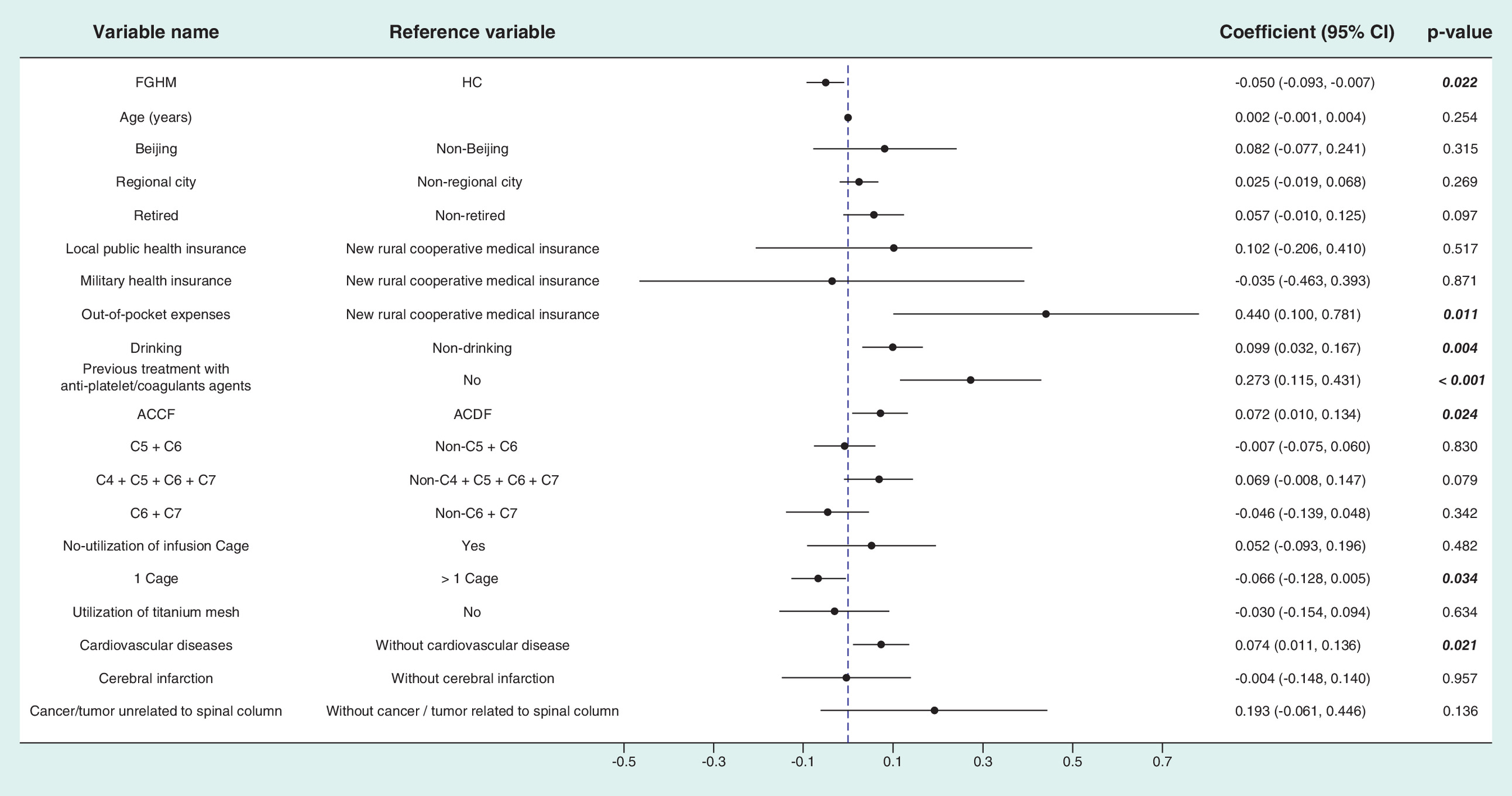
Figure 3. The impact of flowable gelatin hemostatic matrix on the hospital costs after the subtraction of the costs of hemostatic agents and implanted fixation in the included patients (n = 451).
ACCF: Anterior cervical corpectomy fusion; ACDF: Anterior cervical discectomy fusion; CVS: Cervical vertebrae surgery; FGHM: Flowable gelatin hemostatic matrix; HC: Historical control.
Discussion
The large volume of real-world cases of ACSS using FGHM (SURGIFLO) from 2015 to 2016 in our site allowed us to create sufficient propensity-score matched pairs and demonstrate the clinical and economic benefits associated with hemostasis. This is the first known study that assessed the impact of FGHM on cervical–spine perioperative benefits associated with hemostasis and hospital cost by using hospital medical records.
Every patient in the matched FGHM group received gelatin sponge but in significantly lower amounts compared with patients in matched HC group. According to the surgeons of the included patients, the gelatin sponge was usually used first for bleeding control in the FGHM group. Gelatin sponge can soak blood and provide a matrix for clot formation [13,14]. The spongey physical property renders it effective at stopping continuous oozing of visualized and even sites. However, it could be challenging when applying cauterization and high-swell TAH agents to stop bleeding of epidural veins, because these veins are a plexus of vessels surrounding the spinal cord and spinal nerves. Gelatin sponge is a mass-occupying agent and could considerably swell up once saturated with blood, which may potentially lead to neurological compression [15]. Flowable gelatin provides an environment for platelets to adhere and has a distinctly smaller swelling factor compared with gelatin sponge [7]. Also, flowable gelatin better conforms to irregular and deep surgical surface than performed nonflowable TAH agents [12,16]. These characteristics bring advantages to flowable gelatin for stopping venous bleeding from the spinal epidural space in ACSS when the conventional hemostatic agents did not work well in the first line setting. The lower amount of gelatin sponge in the matched FGHM group reflected that the improved hemostasis brought by FGHM reduced the needs of traditional hemostatic agents and offset some costs for gelatin sponge. Thus, the generated clinical evidence in our study confirmed that previously reported superior hemostasis effects of FGHM [17–20] could also occur in the Chinese setting.
Unlike a prospective study, patients in this observational study were not randomly assigned for treatment in clinical pathway. This limitation of retrospective studies necessitates other methods to minimize confounders on hemostatic agents and outcomes [21]. Therefore, this study applied propensity score matching to manage the treatment-selection bias. The low intraoperative blood transfusion rate and volume may be a result of the characteristics of ACSS. Compared with posterior lumbar spinal surgery, there is often less resection of the posterior longitudinal ligament in ACSS, causing less damage to tissue and blood vessel. Thus, the bleeding volume in ACSS was much less compared with the average 600 ml blood loss in lumbar spinal surgery [22]. The improved hemostasis effect of FGHM can also be supported by the statistical significance for the reduced operation time. When the anterior approach is used in cervical spinal discectomy, the operative field is narrow: mild intraoperative bleeding can reduce visibility, degrading accuracy and safety of the surgical technique. In other words, surgeons tend to conduct each step in the surgical procedure followed by prompt hemostasis, though it is time consuming. The prompt hemostasis achieved by FGHM could improve the flow and duration of procedure execution, which may bring better perioperative outcomes including shorter postsurgery LOS and lower risk of drainage tube placement. The operation time could have an impact on other outcomes, such as infection [23] and complications after hospital discharge [24], but these indicators were not measured in our study.
The cost of implanted fixation devices was separated mainly for two reasons: these devices in China are notably more expensive than other medical resources, and their prices vary from brand to brand. Cost of implanted fixation devices could be a confounder if the total medical cost is directly used for comparisons. Therefore, ‘hospital costs, except cost of TAH and implanted fixation’ was used to measure the economic impact associated with FGHM. This study showed that the cost savings associated with improved hemostasis by FGHM could offset the increased acquisition costs of FGHM (SURGIFLO). The comparisons of the cost distribution between matched groups showed that the reduction of medical costs in the matched FGHM group was driven primarily by the decreased cost of disposable medical consumables, which are mainly charged during blood transfusion and postsurgery care. For example, the lower requirement on intraoperative transfusion could result in less frequent usage of disposable blood-transfusion sets; the decreased risk for drainage could save the cost on disposable drainage tubes. Additionally, the economic impacts associated with the shortened postsurgery LOS was reflected through a lower cost of hospital bed, nursing service as well as laboratory tests that were used for postoperative infection and complications monitoring. Thus, this study could be a good example to demonstrate the economic impact associated with improved hemostasis. Though a significant reduction of blood transfusion in matched FGHM was observed, cost savings on blood transfusion were not observed, likely due to the already low blood transfusion rate/volume in ACSS and relatively low price of packed red blood cell (¥210/200 ml) in China. It also should be noted that the economic impact of reduced operation time associated with FGHM could be minimal because of the low service fee for operation rooms in China. This study also observed the costs of clinically relevant outcomes, including reduced blood transfusion, operation time, drainage tube placement and postsurgery LOS. Cost comparison results demonstrated that the increased cost for FGHM could be completely offset by the savings for other medical resources.
This study has limitations that could compound the generalizability of the results. First, this study was conducted in a single tertiary care hospital. Clinical outcomes associated with FGHM should be further explored in other medical settings. Second, due to the retrospective nature of this study, direct clinical measures, such as accurate bleeding volume to assess the hemostatic effects of FGHM, were not possible. Thus, future studies are needed to confirm the findings herein. Finally, our study excluded patients who received thrombin in surgery in order to minimize the potential confounding effects associated with thrombin in the control of bleeding. In real clinical practices, thrombin could be mixed with FGHM to further improve the hemostatic effects. Because the cost of thrombin is relatively low, future studies should further evaluate the hemostatic effects associated with FGHM mixed with thrombin that could gain more clinical and economic benefits.
In summary, this observational study identified a large number of propensity score-matched patients to demonstrate the favorable impact of FGHM on outcomes related to hemostasis in ACSS. Moreover, medical resources savings related to improved surgical outcomes could completely offset the acquisition costs of FGHM. These findings suggest that the adoption of FGHM beyond basic gelatin sponge would bring more favorable outcomes than gelatin sponge alone for hemostasis in ACSS. Future studies using direct outcome measures are warranted to confirm cost-effectiveness dominance of FGHM in ACSS.
Controlling epidural venous oozing during anterior cervical spine surgery is critical for the success of operation.
Many studies have proven the efficacy of flowable gelatin hemostatic matrix (FGHM) in spinal surgery, but the economic impact of FGHM remains unclarified.
The utilization of FGHM in anterior cervical spine surgery improved perioperative clinical outcomes.
The use of FGHM did not increase overall hospital costs associated with anterior cervical spine surgery.
The observed clinical and economic benefits associated with FGHM for anterior cervical spinal surgery support the introduction of FGHM for hemostasis in spine surgery.
Author contributions
Z Wang formulated the research idea and worked with Yunchang Wu; Yiqing Wu, G Gangoli, A Bourcet, W Danker III and W Chen drafted the study protocol, which was verified by Z Wang. Yunchang Wu and Q Gong coordinated the data acquisition. W Chen and H Zhan structured the collected data into the database, developed the data analysis plan, and conducted data analysis. Yunchang Wu and Z Wang interpreted the results from clinical perspective. Z Wang, Yunchang Wu, Yiqing Wu, G Gangoli, A Bourcet, W Danker III and W Chen were fully involved with the development of this manuscript. All authors critically reviewed the manuscript and approved the submission of this manuscript.
Financial & competing interests disclosure
This study was funded by Johnson & Johnson Medical Devices Companies, Somerville, NJ, USA. Yiqing Wu, A Bourcet, G Gangoli and W Danker are employees of Johnson & Johnson Medical Devices Companies. Q Gong, H Zhan and W Chen are the employees of Normin Health, a consulting firm receiving industry to conduct health outcomes and economics research.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval for this work.
References
1.
Laratta JL, Shillingford JN, Saifi C et al. Cervical disc arthroplasty: a comprehensive review of single-level, multilevel, and hybrid procedures. Global Spine J. 8(1), 78–83 (2018).
2.
Szpalski M, Gunzburg R, Sztern B. An overview of blood-sparing techniques used in spine surgery during the perioperative period. Eur. Spine J. 13(Suppl. 1), s18–s27 (2004).
3.
Shander A. Financial and clinical outcomes associated with surgical bleeding complications. Surgery 142(4S), S20–S26 (2007).
4.
Corral M, Ferko N, Hollmann S et al. Health and economic outcomes associated with uncontrolled surgical bleeding: a retrospective analysis of the Premier Perspectives Database. Clinicoecon. Outcomes Res. 7, 409–421 (2015).
5.
Emilia M, Luca S, Francesca B et al. Topical hemostatic agents in surgical practice. Transfus. Apher. Sci. 45(3), 305–311 (2011).
6.
Sewlikar S, Rillai R, Mahajan N, Desai A. Bleeding scenarios in spine surgeries: role for tropical hemostatic agents. J. Spinal Surg. 2(1), 13–16 (2015).
7.
Gazzeri R, De Bonis C, Galarza M. Use of a thrombin–gelatin hemostatic matrix (SURGIFLO®) in spinal surgery. Surg. Technol. Int. 25, 280–285 (2014).
8.
Comadoll JL, Comadoll S, Hutchcraft A et al. Comparison of hemostatic matrix and standard hemostasis in patients undergoing primary TKA. Orthopedics 35(6), e785–e793 (2012).
9.
Tackett SM, Sugarman R, Kreuwel HT et al. Hospital economic impact from hemostatic matrix usage in cardiac surgery. J. Med. Econ. 17(9), 670–676 (2014).
10.
Echave M, Oyagüez I, Casado MA. Use of Floseal®, a human gelatine–thrombin matrix sealant, in surgery: a systematic review. BMC Surg. 14(1), 111 (2014).
11.
Helenius I, Keskinen H, Syvanen J et al. Gelatine matrix with human thrombin decreases blood loss in adolescents undergoing posterior spinal fusion for idiopathic scoliosis. Bone Joint J. 98(3), 395–401 (2016).
12.
Renkens KL Jr, Payner TD, Leipzig TJ et al. A multicenter, prospective, randomized trial evaluating a new hemostatic agent for spinal surgery. Spine 26(15), 1645–1650 (2001).
13.
Sileshi B, Achneck HE, Lawson JH. Management of surgical hemostasis: topical agents. Vascular 16(1 Suppl.), 22–28 (2008).
14.
Schonauer C, Tessitore E, Barbagallo G et al. The use of local agents: bone wax, gelatin, collagen, oxidized cellulose. Eur. Spine J. 13(Suppl. 1), S89–S96 (2004).
15.
Alander DH, Stauffer ES. Gelfoam-induced acute quadriparesis after cervical decompression and fusion. Spine 20(8), 970–971 (1995).
16.
Cappabianca P, Esposito F, Esposito I et al. Use of a thrombin–gelatin haemostatic matrix in endoscopic endonasal extended approaches: technical note. Acat. Neurochir. 151, 69–77 (2009).
17.
Gazzeri R, Galarza M, Alfier A. Safety biocompatibility of gelatin hemostatic matrix (Floseal and SURGIFLO®) in neurosurgical procedures. Surg. Tech. Int. 22, 49–54 (2012).
18.
Gazzeri R, Galarza M, Neroni M, Alfieri A, Giordano M. Hemostatic matrix sealant in neurosurgery: a clinical and imaging study. Acta Neurochir. 153(1), 148–155 (2011).
19.
Landi A, Gregori F, Marotta N, Delfini R. Efficacy, security, and manageability of gelified hemostatic matrix in bleeding control during thoracic and lumbar spine surgery: FloSeal versus Surgiflo. J. Neurol. Surg. A Cent. Eur. Neurosurg. 77(2), 139–143 (2016).
20.
Price JS, Tackett S, Patel V. Observational evaluation of outcomes and resource utilization from hemostatic matrices in spine surgery. J. Med. Economics 18(10), 777–786 (2015).
21.
Despotis GJ, Joist JH, Goodnough LT. Monitoring of hemostasis in cardiac surgical patients: impact of point-of-care testing on blood loss and transfusion outcomes. Clin. Chem. 43(9), 1684–1696 (1997).
22.
Seraph V, Lerch C, Walochnik N et al. Comparison of conventional versus minimally invasive extraperitoneal approach for anterior lumbar interbody fusion. Eur. Spine J. 13, 425–431 (2004).
23.
Eva YW, Cheung WY, Ng KF et al. Reducing perioperative blood loss and allogeneic blood transfusion in patients undergoing major spine surgery. JBJS 93(13), 1268–1277 (2011).
24.
Wimmer C, Gluch H, Franzreb M et al. Predisposing factors for infection in spine surgery: a survey of 850 spinal procedures. Clin. Spine Surg. 11(2), 124–128 (1998).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 30 October 2018
Accepted: 7 January 2019
Published online: 25 January 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Using flowable gelatin in anterior cervical spine surgery in real-world practice: a retrospective cohort study. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0121
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Abdulrahim Saleh Alrasheed, Ameena Manzoor, Abdulaziz S. Almuhaisen, Óscar L. Alves, Saleh S. Baeesa, Safety and Efficacy of Flowable Gelatin Hemostatic Matrix Sealants in Spine Surgery: A Systematic Review and Meta-Analysis, Spine Open, 10.1097/bn9.0000000000000093, 2, 3, (2026).
- Chengyi Huang, Zhu Chen, Hao Liu, Junbo He, Yiwei Shen, Tingkui Wu, Beiyu Wang, The Effect of Thrombin-gelatin Matrix Compared With Absorbable Gelatin Sponge on Intraoperative Hemostasis in Unilateral Open-door Laminoplasty, Spine, 10.1097/BRS.0000000000005107, (2024).
- So Kato, Junya Miyahara, Yoshitaka Matsubayashi, Yuki Taniguchi, Toru Doi, Hiroyasu Kodama, Akiro Higashikawa, Yujiro Takeshita, Masayoshi Fukushima, Takashi Ono, Nobuhiro Hara, Seiichi Azuma, Hiroki Iwai, Masahito Oshina, Shurei Sugita, Shima Hirai, Kazuhiro Masuda, Sakae Tanaka, Yasushi Oshima, Predictors for hemostatic thrombin-gelatin matrix usage in spine surgery: a multicenter observational study, BMC Musculoskeletal Disorders, 10.1186/s12891-023-06408-8, 24, 1, (2023).
- Zhengyu Liu, Qingming Zhang, Juyong Wang, Shibao Lu, Intelligent Three-Dimensional Reconstruction Algorithm-Based X-Ray Film for Analysis of the Changes in Sagittal Parameters and Curative Effect of Anterior Cervical Surgery, Scientific Programming, 10.1155/2021/5194613, 2021, (1-8), (2021).