Willingness to pay for medical treatments in chronic diseases: a multicountry survey of patients and physicians
Abstract
Aim: The objective was to investigate factors influencing patients’ willingness to pay (WTP) and physician’s views on the cost of therapy for two contrasted chronic diseases, chronic heart failure and psoriasis. Methods: A cross-sectional survey was conducted in ten developing countries, using a stated WTP contingent valuation method. Multivariate analyses were performed by linear regression. Results: Independent factors influencing patient WTP were income (+0.04 $PPP [purchasing power parity] in WTP per $PPP in monthly income; p < 0.001) and purchase of branded treatment for chronic heart failure therapy, and income, out-of-pocket treatment costs but also education level higher than secondary school (+115 $PPP in WTP comparatively to patients with none/primary school level; p = 0.008) for psoriasis therapy, suggesting the influence of sociopsychological factors in this disease. Conclusion: Disease-specific factors may affect WTP for treatment that should be accounted for to support effective public health programs in developing countries.
Predicting client response to the price of therapeutics in developed countries has become critical for effective public health program management and new drug development. In setting prices, drug or service providers – be they pharmaceutical firms, nongovernmental organizations or public sector programs – must strike a balance between a cost that is sufficiently high to enable a sustainable supply of the therapy and to fund R&D activities for new therapies and one that is sufficiently low to allow broad access and to achieve coverage goals. Although pricing could be determined experimentally under real market conditions by lowering or raising prices and observing changes in client volume, the ability to predict client behavior without the need for such manipulations would provide managers a more straightforward approach.
In the last decades, willingness to pay (WTP) techniques have increasingly been applied to inform policy decisions in healthcare [1]. Such techniques are based on either observed actual consumer behavior (revealed WTP approach) or hypothetical consumer behavior expressed in a survey (stated WTP approach) [2]. Contingent valuation is a stated-preference approach that uses survey methods to ascertain the maximum amount individuals would be willing to pay for products or services presented in the context of hypothetical scenarios. Due to its practical advantages and demonstrated reliability, contingent valuation has been extensively used in studies of demand for a variety of healthcare goods and services [3–5].
Identification of the most relevant factors associated with WTP is a key goal for WTP studies. In chronic disease management, these factors may include disease-related factors (e.g., symptom severity, risk of morbidity or mortality) and socio-economic factors (e.g., personal income, education level), but also other potentially relevant but less studied factors including physician-specific factors (e.g., physician perception of reasonable product price based on cost–effectiveness evidence), health system factors (e.g., presence of reimbursement mechanism) and psychocultural factors (e.g., patients personal expectations and perceived stigma related to a particular condition). Yet few studies have evaluated patients’ WTP across multiple chronic disease areas while also accounting for the interactions between factors influencing chronic disease management.
In this regard, chronic heart failure (CHF) and psoriasis are two chronic diseases that both are very common and yet have significantly different impacts on health, the former being a potentially life-threatening condition marked by severe morbimortality [6], the latter being characterized by generally less pronounced physical manifestations but psychological burden and social stigma [7]. Consequently, exploring which common or unique factors could affect WTP in those two conditions could provide a potentially useful model for gaining insight into additional factors that impact WTP. Guideline recommendations for the management of patients with CHF and New York Heart Association (NYHA) Class II symptoms include angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers and β-blockers, with the key aim of relieving symptoms and prolonging survival [8]. Although drug therapy for CHF may be substantially cheaper than cancer drugs, the cost of several new CHF treatments, such as implantable and cardiac resynchronization therapy devices, have higher costs. In contrast, psoriasis is a chronic skin condition that has a major impact on health-related quality of life (QoL) but is not associated with significant morbidity or mortality. WTP has been assessed in various dermatological disorders to measure patient-defined utilities and identify the relative severity of a variety of QoL domains [9], showing that physical comfort, social comfort and emotional health were the domains of health most affected by psoriasis.
We hypothesized that a variety of intricate factors may impact patients’ WTP, including individual socio-economic features, characteristics of the disease, patients’ and society’s expectations of health, and cross-cultural aspects relating to health and health expenses. Using a survey performed in ten developing countries, the aim of the present study was to demonstrate the use of a stated WTP contingent valuation method (CVM) to investigate and compare patients’ WTP for medications and physician’s views onthe cost of therapy for heart failure and psoriasis, two chronic diseases characterized by contrasting determinants and outcomes.
Materials & methods
Study population
A cross-sectional design, using a convenience sample, was used to identify the participants’ WTP. Patients eligibility criteria were chosen to be aligned with the indications of the products being studied for CHF and psoriasis. Inclusion criteria for psoriasis stakeholders were as follows: patients had to be at least 18 years of age and referred by a physician having been diagnosed with moderate to severe psoriasis; physicians had to be dermatologists with at least 5 years of postspecialization practice and regularly involved in the treatment of patients with moderate to severe psoriasis. Inclusion criteria for CHF stakeholders were as follows: patients had to be at least 40 years of age and referred by a physician has having been diagnosed with CHF with a reduced ejection fraction (HF-REF); physicians had to be cardiologists, internists or general practitioners with at least 5 years of postspecialization practice and regularly involved in the treatment of patients with CHF. For the CHF sample, physicians were divided equally between cardiologists and other practitioners (internists and general practitioners).
Exclusion criteria for all psoriasis and CHF stakeholders were a lack of proficiency in English or a local language and unwillingness or inability to provide an informed and signed consent.
For both the psoriasis and CHF samples, stakeholder groups were drawn from the public and private sectors so as to reflect the general distribution of public and private treatment patterns in the general population. For example, if, in a given country, 70% of the population was generally treated in the public sector and 30% was treated in the private sector, then the target sample for each stakeholder group comprised 70% of participants from the public sector and 30% from the private sector. With respect to sample selection by geographic area, the target sample for all stakeholder groups represented the two most populous cities in each country or the largest city and a city known to have the second-largest commercial center. Within each country, the number of stakeholders enrolled by city was proportional to the population in each city.
The selection of stakeholders for all groups was made using the existing Axios in-country networks, and the final groups were convenience samples that adhered as closely as possible to the criteria outlined above. Patients with moderate to severe psoriasis or CHF were identified through their treating physicians and approached for study participation immediately following a physician consultation (exit interview conducted on the premises of the institution where consultation took place). Physicians were identified through the Axios in-country networks and were initially approached for participation through an introductory letter, followed by a phone call. Physician interviews were conducted in their respective offices. The survey was conducted by Axios International in the framework of the establishment of a tracing strategy for two new products of a pharmaceutical company, using a slightly different selection of targeted countries depending on the product. The company had no role in the study design, analyses or drafting of the manuscript.
Questionnaires
For both psoriasis and CHF medications, the patient questionnaire was organized based on several relevant domains identified from the literature as potential factors influencing WTP, including: socio-economic factors, in other words, household income, education/socio-economic status, insurance coverage (assessed through questions about the availability of any help from the government or an insurance company to pay for the treatment of the disease of interest and what percentage of the total cost was on average covered by this insurance); severity of the disease (assessed through the existence of lesions in sensible areas, namely the palms of hands, the soles of feet, the face or the genital region in patients with psoriasis, and the overall number of emergency room [ER] visits and the NYHA Class in patients with CHF) and current health status; and level of concern of disease health effects. The questionnaires were translated into the languages of the surveyed countries and pretested for comprehensibility and average duration of administration by staff speaking the local language and a selection of patients. The patient questionnaire was designed to solicit direct patient input on their own WTP for a new therapy, while the physician questionnaire captured physician perspectives on what they thought would be a reasonable price that their patients, not the physicians themselves, would pay.
Willingness to pay methodology
The CVM has previously been described [10,11]. Briefly, the CVM was initially developed as a survey approach to assess the value of goods and services provided directly to the public without a consumer-based market and to determine how this valuation impacted price and demand for these goods and services. The approach has also shown utility in evaluating goods and services, including those related to health and medicine, for which a market exists but is regulated by the public sector and not based on free market economics. WTP is included as a component of both cost–effectiveness and cost-benefit analyses, and in the latter, can provide insight into how effectively goods and services are allocated.
Statistical analysis
Descriptive results are given as means ( ± standard deviation) for quantitative data and numbers (%) for categorical data. Unadjusted and multivariate analyses were conducted to identify independent determinants of the prices stated by patients and physicians. For unadjusted analyses, unpaired t-tests or Mann–Whitney tests (two groups) and ANOVA or Kruskal–Wallis tests (three and more groups) were performed to compare mean prices across categories, depending on the normality of variable distributions. Multivariate analysis was conducted using linear regression models led on all observations, since no patients declared a zero-valued WTP. A stepwise backward approach was used for sequentially removing variables not significant at the p < 0.05 level until reaching the final model.
Price values were assessed as international dollars using the World Bank’s gross domestic product purchasing power parity (PPP) conversion factor. A sensitivity analysis was also conducted based on nominal dollars to assess the robustness of the results. Similar results were yielded using this latter approach with respect to the independent predictors of patient’s WTP identified in multivariate analyses so that only results from the main analysis by $PPP are shown.
Finally, supportive descriptive results based on an in-house proprietary mathematical model (‘affordability model’) were computed in order to provide quantitative global numbers summarizing drug access and ability to pay of patients within a given country. Briefly, the model uses a three-step methodology, by determining the income distribution curve across population segments based on available data from international agencies (World Bank, IMF); estimating household healthcare expenditure, overall and specifically allocated for the treatment of interest; and finally limiting the patient pool based on all expected barriers that might impede the diagnosis, treatment and follow-up of patients apart from the ability to pay for medication, including ease of disease diagnosis, availability of sites to diagnose the disease and the rural rate. Results from the affordability model are shown as curves plotting the number or the proportion of diagnosed and treated patients expected to be able to access and buy a product against a range of hypothetical prices.
All analyses were stratified by chronic condition (psoriasis or CHF) and performed using Stata v14.1 (StataCorp, TX, USA).
Results
Study population
The study was conducted in eight developing countries for CHF (Egypt, India, Indonesia, Mexico, Nigeria, Romania, Russia and Venezuela) and five developing countries for psoriasis (Egypt, India, Indonesia, Philippines and Thailand), and comprised a total of 167 CHF patients, 155 CHF physicians (102 cardiologists, 24 internists, 28 general practitioners and one other physician type), 85 psoriasis patients and 64 psoriasis physicians (dermatologists). One patient with CHF with too much missing information (including the primary end point) was excluded from the present analysis, yielding 166 CHF patients.
As summarized in Table 1, psoriasis and CHF patients had a mean patient age of 47 years and 62 years, respectively, with a higher education level in 51 and 40% of patients. Mean and median income values varied by country and by disease category. Overall, median monthly income (USD) and median monthly income ($PPP) were $560 and $1865 for psoriasis patients and $477 and $1031 for CHF patients. Median monthly income (USD) ranged from $210 (Egypt) to $1120 (Philippines) for psoriasis patients and $279 (Egypt) to $1272 (Venezuela) for CHF patients. Median monthly income ($PPP) ranged from $699 (Egypt) to $2801 (Venezuela) for psoriasis patients and $773 (Russia) to $3253 (India).
| Characteristics | Psoriasis sample n = 85 | Chronic heart failure sample n = 166 | |
|---|---|---|---|
| Age (years), mean (SD) | 47.2 (±14.5) | 62.0 (±11.0) | |
| Education level, n (%) | None/primary | 25 (29.4) | 46 (27.7) |
| Secondary | 17 (20.0) | 54 (32.5) | |
| Higher | 43 (50.6) | 66 (39.8) | |
| Per country patient and income distribution | Overall, n (%) | 85 (100) | 166 (100) |
| Monthly income (USD), median (IQR) | 560.2 (279.7; 907.9) | 476.8 (279.3; 813.2) | |
| Monthly income (PPP), median (IQR) | 1864.7 (808.3; 2797.0) | 1031.2 (644.5; 1804.6) | |
| Egypt, n (%) | 20 (23.5) | 16 (9.6) | |
| Monthly income (USD), median (IQR) | 209.8 (104.9; 419.6) | 279.3 (153.6; 419.0) | |
| Monthly income (PPP), median (IQR) | 699.3 (349.6; 1398.5) | 931.1 (512.1; 1396.6) | |
| India, n (%) | 20 (23.5) | 15 (9.0) | |
| Monthly income (USD), median (IQR) | 646.7 (485.0; 1293.3) | 975.9 (650.6; 1301.2) | |
| Monthly income (PPP), median (IQR) | 2155.5 (1616.6; 4311.1) | 3252.9 (2168.6; 4337.2) | |
| Indonesia, n (%) | 15 (17.6) | 31 (18.7) | |
| Monthly income (USD), median (IQR) | 322.9 (161.4; 565.0) | 410.9 (205.5; 657.5) | |
| Monthly income (PPP), median (IQR) | 1076.2 (538.1; 1883.4) | 1369.8 (684.9; 2191.7) | |
| Mexico, n (%) | – | 15 (9.0) | |
| Monthly income (USD), median (IQR) | 592.0 (370.0; 888.0) | ||
| Monthly income (PPP), median (IQR) | 986.7 (616.7; 1480.0) | ||
| Nigeria, n (%) | – | 30 (18.1) | |
| Monthly income (USD), median (IQR) | 447.0 (238.4; 595.9) | ||
| Monthly income (PPP), median (IQR) | 893.9 (476.8; 1191.9) | ||
| Philippines, n (%) | 15 (17.6) | – | |
| Monthly income (USD), median (IQR) | 1120.4 (560.2; 1568.6) | ||
| Monthly income (PPP), median (IQR) | 2801.1 (1400.5; 3921.5) | ||
| Romania, n (%) | – | 15 (9.0) | |
| Monthly income (USD), median (IQR) | 563.9 (282.0; 676.7) | ||
| Monthly income (PPP), median (IQR) | 1127.8 (563.9; 1353.4) | ||
| Russia, n (%) | – | 29 (17.5) | |
| Monthly income (USD), median (IQR) | 464.0 (340.3; 618.7) | ||
| Monthly income (PPP), median (IQR) | 773.4 (567.2; 1031.2) | ||
| Thailand, n (%) | 15 (17.6) | – | |
| Monthly income (USD), median (IQR) | 907.9 (756.5; 1513.1) | ||
| Monthly income (PPP), median (IQR) | 2269.6 (1891.4; 3782.7) | ||
| Venezuela, n (%) | – | 15 (9.0) | |
| Monthly income (USD), median (IQR) | 1272.3 (1033.8; 1590.4) | ||
| Monthly income (PPP), median (IQR) | 1817.6 (1476.8; 2272.0) | ||
IQR: Interquartile range; PPP: Purchasing power parity; USD: US dollars; SD: Standard deviation
Descriptive results
Figure 1 depicts the WTP for one CHF treatment and one psoriasis treatment according to education level (panels A and B), patients, physicians and affordability model (panels C and D) and country (panels E and F). The graphs represent the percentage of respondents who were willing to pay for a treatment (y-axis) according to the price for the treatment (x-axis). The curves revealed a clear association between higher WTP for expensive products and higher education level in both conditions, with an apparent more marked and graded relationship found in psoriasis patients (panels A and B). Patients’ WTP was found consistently higher than the cumulative percentages obtained from physicians and the mathematical ‘affordability’ model (panels C and D), indicating a gap between actual expectations and demands from patients and an external estimation of the price deemed reasonable by physicians or the patient’s financial capacity calculated by simulation. Finally, WTP varied strongly between countries and medications, with the highest WTP percentages found in Indonesia, Venezuela, Egypt and India for CHF and Thailand and Philippines for psoriasis (panels E and F).
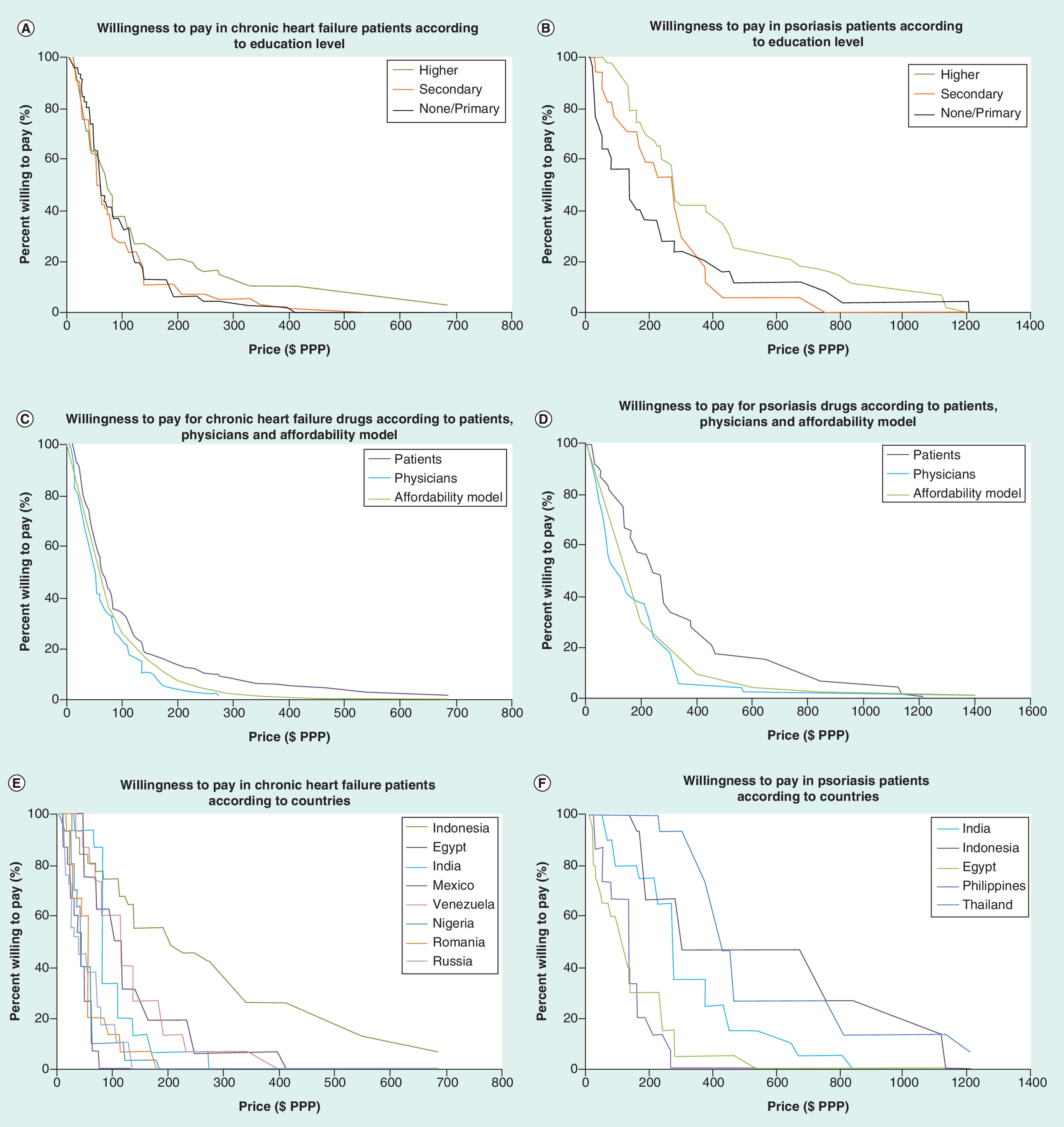
Figure 1. Willingness to pay in chronic heart failure and psoriasis patients.
• Panels A and B: Willingness to pay in chronic heart failure (A) and psoriasis (B) patients according to education level
• Panels C and D: Willingness to pay for chronic heart failure (C) and psoriasis (D) drugs according to patients, physicians and affordability model
• Panels E and F: Willingness to pay in chronic heart failure (E) and psoriasis (F) patients according to countries
Factors independently associated with patients’ willingness to pay & physicians’ recommendation for payment
CHF
Factors independently associated with a $PPP price considered reasonable by patients for CHF medication are summarized in Table 2. Significant factors identified in univariate analysis with increased price were: country (p < 0.001) with higher prices reported by patients from Indonesia, Venezuela and Egypt, increasing number of emergency room visits (p = 0.016, with, e.g., +65 $PPP in patients with ≥2 visits when compared with those with 0 as the reference), government or health insurance support in paying for CHF treatment (p = 0.003; +54 $PPP), recent purchase of branded angiotensin receptor blocker (p < 0.0001; +131 $PPP) or branded diuretic as a negatively associated factor (p = 0.043; -41 $PPP), increasing age (p = 0.005), increasing monthly income by USD (p = 0.002) or by purchasing power parity ($PPP; p < 0.001), increasing percentage of insurance coverage for CHF drugs (p < 0.001; +0.81 $PPP per % insurance coverage) and increasing monthly out-of-pocket costs for other long-term treatments by $PPP (p = 0.036). In multivariate analysis, three factors remained significantly associated with patient WTP ($PPP) for CHF therapy: country (p < 0.001; from -86 $PPP for India to +107 $PPP for Indonesia when compared with Egypt taken as reference), recent purchase of branded angiotensin receptor blocker (p = 0.002; +54 $PPP) and an increasing monthly income by $PPP (p < 0.001; +0.04 $PPP in WTP per $PPP in monthly income).
| Patients' results¶ (n = 166) | n | Univariate analysis | Multivariate analysis§ | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Unadjusted coefficient† (95% CI) | p-value | Adjusted coefficient† (95% CI) | p-value | |||
| Country | Egypt | 16 | 125 ± 93.06 | 0 (ref) | <0.001 | 0 (ref) | <0.001 |
| India | 15 | 102 ± 55.47 | -23 (-91 to 46) | -86 (-152 to -19) | |||
| Indonesia | 31 | 242 ± 191.54 | 117 (58 to 175) | 107 (53 to 162) | |||
| Mexico | 15 | 40 ± 19.48 | -85 (-153 to -16) | -62 (-123 to -1) | |||
| Nigeria | 30 | 51 ± 34.63 | -74 (-133 to -15) | -39 (-93 to 14) | |||
| Romania | 15 | 58 ± 39.84 | -67 (-136 to 1) | -30 (-91 to 31) | |||
| Russia | 29 | 51 ± 38.82 | -74 (-133 to -15) | -31 (-84 to 23) | |||
| Venezuela | 15 | 127 ± 80.47 | 2 (-66 to 71) | -8 (-69 to 54) | |||
| Education level | None/primary | 46 | 88 ± 74.32 | 0 (ref) | 0.057 | ||
| Secondary | 54 | 86 ± 84.04 | -2 (-49 to 45) | ||||
| Higher | 66 | 132 ± 158.30 | 44 (-1 to 88) | ||||
| NYHA class | 1 | 9 | 68 ± 51.21 | 0 (ref) | 0.075 | ||
| 2 | 49 | 140 ± 154.31 | 72 (-12 to 156) | ||||
| 3 | 78 | 87 ± 95.34 | 19 (-63 to 101) | ||||
| 4 | 30 | 106 ± 113.19 | 38 (-50 to 126) | ||||
| Number of ER visits | 0 | 39 | 58 ± 43.00 | 0(ref) | 0.016 | ||
| 1 | 46 | 112 ± 117.39 | 54 (4 to 104) | ||||
| 2 and more | 81 | 123 ± 138.12 | 65 (20 to 110) | ||||
| Government or insurance help to pay HF treatment | No | 72 | 74 ( ± 68.84) | 0 (ref) | 0.003 | ||
| Yes | 94 | 128 ( ± 142.05) | 54 (18 to 90) | ||||
| Branded angiotensin-converting enzyme inhibitors recently purchased | No | 104 | 95 ± 106.18 | 0 (ref) | 0.180 | ||
| Yes | 62 | 121 ± 137.04 | 26 (-12 to 63) | ||||
| Branded angiotensin receptor blockers recently purchased | No | 131 | 77 ± 63.94 | 0 (ref) | <0.001 | 0 (ref) | 0.002 |
| Yes | 35 | 209 ± 197.39 | 131 (91 to 171) | 54 (19 to 89) | |||
| Branded β-blockers recently purchased | No | 105 | 114 ± 130.63 | 0 (ref) | 0.218 | ||
| Yes | 61 | 90 ± 94.51 | -24 (-61 to 14) | ||||
| Branded mineralocorticoid receptor antagonists recently purchased | No | 129 | 112 ± 127.66 | 0 (ref) | 0.162 | ||
| Yes | 37 | 81 ± 77.93 | -31 (-75 to 13) | ||||
| Branded diuretics recently purchased | No | 118 | 117 ± 124.20 | 0 (ref) | 0.043 | ||
| Yes | 48 | 76 ± 99.95 | -41 (-81 to -1) | ||||
| Age (years) | 166 | -0.22‡ | -2.35 (-3.98 to -0.73) | 0.005 | |||
| Monthly income (USD) | 163 | 0.25‡ | 0.05 (0.02 to 0.08) | 0.002 | |||
| Monthly income (PPP) | 163 | 0.41‡ | 0.03 (0.02 to 0.05) | <0.001 | 0.04 (0.02 to 0.05) | <0.001 | |
| % insurance coverage for HF drugs | 164 | 0.30‡ | 0.81 (0.41 to 1.20) | <0.001 | |||
| Monthly cost paid out-of-pocket for HF treatment ($PPP) | 156 | -0.001‡ | 0.00 (-0.18 to 0.18) | 0.988 | |||
| Monthly cost paid out-of-pocket for other long term treatments ($PPP) | 153 | 0.17‡ | 0.18 (0.01 to 0.35) | 0.036 | |||
†Results are β-regression coefficients yielded from univariate and multivariate linear regression modeling, respectively, directly conveying the effect of a 1-unit increase of a given predictor on the price considered reasonable.
‡Pearson correlation coefficients.
§Applying a stepwise backward approach by sequentially removing variables not-significant at the p < 0.05 level until reaching the final model.
¶Original question: ‘If your physician recommended this new medication to you, what would be a reasonable price to pay for it per month?’ (expressed in US dollars).
Bolded p-values are statistically significant at the 0.05 level.
ER: Emergency room; HF: Heart failure; NYHA: New York Heart Association; PPP: Purchasing power parity; SD: Standard deviation.
Factors independently associated with an increased $PPP price considered reasonable by physicians for CHF medication are summarized in Table 3. Significant factors identified in multivariate analysis were: country (p < 0.001) with higher prices reported by physicians from Venezuela, Egypt, India and Indonesia, and physician sector (p = 0.017) with higher prices from physicians from the private sector (+24 $PPP when compared with public sector as the reference).
| Physicians' results¶ (n = 155) | Univariate analysis | Multivariate analysis§ | |||||
|---|---|---|---|---|---|---|---|
| n | Mean ± SD | Unadjusted coefficient† (95% CI) | p-values | Adjusted coefficient† (95% CI) | p-value | ||
| Country | Egypt | 10 | 83 ± 62 | 0 (ref) | <0.001 | 0 (ref) | <0.001 |
| India | 40 | 94 ± 55 | 12 (-18 to 41) | 7 (-23 to 36) | |||
| Indonesia | 25 | 82 ± 55 | -1 (-33 to 30) | -6 (-37 to 25) | |||
| Mexico | 14 | 58 ± 20 | -25 (-59 to10) | -23 (-57 to 11) | |||
| Nigeria | 25 | 26 ± 28 | -57 (-88 to -25) | -54 (-85 to -23) | |||
| Romania | 9 | 38 ± 13 | -45 (-84 to -6) | -38 (-76 to 0) | |||
| Russia | 25 | 18 ± 12 | -65 (-97 to -34) | -62 (-93 to -31) | |||
| Venezuela | 7 | 141 ± 46 | 58 (17 to 100) | 57 (16 to 97) | |||
| Physician specialty | Cardiologist | 102 | 63 ± 56 | 0 (ref) | 0.914 | ||
| Internist | 24 | 63 ± 36 | 0 (-24 to 25) | ||||
| General practitioner | 28 | 67 ± 62 | 3 (-20 to 26) | ||||
| Other | 1 | 28 | -35 (-144 to 73) | ||||
| Physician sector | Public | 53 | 45 ± 38 | 0 (ref) | <0.001 | 0 (ref) | 0.017 |
| Private | 53 | 90 ± 62 | 45 (25 to 64) | 24 (7 to 41) | |||
| Public & private | 49 | 56 ± 50 | 11 (-9 to 31) | 6 (-10 to 23) | |||
| Most important unmet needs in current therapy | Improved tolerability/symptoms/QoL | 92 | 54 ± 46 | 0 (ref) | 0.003 | ||
| Improved renal preservation/hospitalization rate/mortality | 61 | 80 ± 62 | 26 (9 to 44) | ||||
| Considers patient ability to pay when prescribing | No | 17 | 85 ± 60 | 0 (ref) | 0.089 | ||
| Yes | 138 | 61 ± 53 | -24 (-51 to 4) | ||||
| Factors influencing prescription willingness apart safety/efficacy | Brand | 34 | 84 ± 52 | 0 (ref) | 0.071 | ||
| Local availability | 52 | 59 ± 59 | -25 (-49 to -2) | ||||
| Delivery method | 2 | 50 ± 60 | -33 (-110 to 43) | ||||
| P&R status | 59 | 57 ± 49 | -27 (-50 to -5) | ||||
| Other | 4 | 104 ± 46 | 20 (-35 to 76) | ||||
| Number of years practicing | 155 | 0.24‡ | 1.42 (0.51 to 2.33) | 0.003 | |||
| Average NYHA Class in HF patients treated | 125 | -0.01‡ | -0.65 (-20.71 to 19.42) | 0.949 | |||
†Results are β-regression coefficients yielded from univariate and multivariate linear regression modeling, respectively, directly conveying the effect of a 1-unit increase of a given predictor on the price considered reasonable.
‡Pearson correlation coefficients.
§Applying a stepwise backward approach by sequentially removing variables not significant at the p < 0.05 level until reaching the final model.
¶Original question: ‘What would be a reasonable price for your HF-REF patients to pay for this new medication per month’ (expressed in US dollars).
Bolded p-values are statistically significant at the 0.05 level.
HF-RFF: Heart failure with reduced ejection fraction; NHYA: New York Heart Association; QoL: Quality of life; SD: Standard deviation.
Psoriasis
Factors independently associated with a $PPP price considered reasonable by patients for psoriasis medication are summarized in Table 4. Significant factors identified in multivariate analysis were: country (p < 0.001) with higher prices reported by patients from Thailand and Philippines (+202 $PPP and +246 $PPP, respectively, when compared with Egypt taken as reference), education level (p = 0.008; with, e.g., +115 $PPP in patients with education level higher than secondary school comparatively to those with none/primary school as the reference), monthly $PPP income (p < 0.001; +0.03 $PPP in WTP per $PPP in monthly income), and monthly $PPP out-of-pocket costs for psoriasis treatment (p = 0.003; +0.18 $PPP in WTP per $PPP in monthly costs).
| Patients' results¶ (n = 85) | n | Univariate analysis | Multivariate analysis§ | |||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Unadjusted coefficient† (95% CI) | p-values | Adjusted coefficient† (95% CI) | p-value | ||||
| Country | Egypt | 20 | 132 ± 120 | 0 (ref) | <0.001 | 0 (ref) | <0.001 | |
| India | 20 | 304 ± 197 | 172 (29 to 316) | -8 (-134 to118) | ||||
| Indonesia | 15 | 129 ± 72 | -3 (-158 to 152) | -13 (-125 to 98) | ||||
| Philippines | 15 | 506 ± 359 | 374 (219 to 529) | 246 (125 to 367) | ||||
| Thailand | 15 | 525 ± 303 | 392 (237 to 548) | 202 (76 to 329) | ||||
| Education level | None/primary | 25 | 226 ± 286 | 0 (ref) | 0.038 | 0 (ref) | 0.008 | |
| Secondary | 17 | 234 ± 160 | 8 (-162 to 178) | -4 (-118 to 110) | ||||
| Higher | 43 | 383 ± 296 | 157 (21 to 294) | 115 (27 to 203) | ||||
| Government or insurance help to pay psoriasis treatment | No | 60 | 322 ± 290 | 0 (ref) | 0.470 | |||
| Yes | 25 | 273 ± 254 | -48 (-181 to 84) | |||||
| Lesions in sensible areas | No | 20 | 280 ± 229 | 0 (ref) | 0.615 | |||
| Yes | 65 | 316 ± 294 | 36 (-107 to 179) | |||||
| Current treatments | Phototherapy | No | 32 | 205 ± 242 | 0 (ref) | 0.008 | ||
| Yes | 53 | 369 ± 285 | 165 (45 to 285) | |||||
| Methotrexate | No | 35 | 289 ± 208 | 0 (ref) | 0.606 | |||
| Yes | 50 | 321 ± 322 | 32 (-91 to 155) | |||||
| Ciclosporin | No | 75 | 305 ± 290 | 0 (ref) | 0.822 | |||
| Yes | 10 | 326 ± 189 | 21 (-167 to 210) | |||||
| Retinoids | No | 65 | 331 ± 298 | 0 (ref) | 0.162 | |||
| Yes | 20 | 231 ± 198 | -100 (-242 to 41) | |||||
| Others | No | 27 | 195 ± 172 | 0(ref) | 0.011 | |||
| Yes | 58 | 360 ± 305 | 164 (39 to 290) | |||||
| Overall satisfaction regarding efficacy (1 to 5) | Highly dissatisfied | 3 | 418 ± 220 | 0 (ref) | 0.431 | |||
| Dissatisfied | 13 | 292 ± 322 | -126 (-483 to 231) | |||||
| Neither | 25 | 231 ± 194 | -187 (-527 to 153) | |||||
| Satisfied | 35 | 331 ± 295 | -87 (-422 to 248) | |||||
| Highly satisfied | 9 | 411 ± 366 | -7 (-378 to 364) | |||||
| Age (years) | 85 | -0.08‡ | 0.36 (-3.84 to 4.56) | 0.866 | ||||
| Monthly income (USD) | 85 | 0.87‡ | 0.13 (0.10 to 0.16) | <0.001 | ||||
| Monthly income (PPP) | 85 | 0.84‡ | 0.05 (0.04 to 0.06) | <0.001 | 0.03 (0.02 to 0.04) | <0.001 | ||
| % insurance coverage for psoriasis drugs | 85 | -0.11‡ | -0.83 (-2.34 to 0.68) | 0.280 | ||||
| Treatment duration (weeks) | 85 | 0.13‡ | -0.19 (-0.46 to 0.09) | 0.176 | ||||
| Monthly cost paid out-of-pocket for psoriasis treatment (PPP) | 85 | 0.69‡ | 0.42 (0.30 to 0.54) | <0.001 | 0.18 (0.07 to 0.30) | 0.003 | ||
| Monthly cost paid out-of-pocket for other long term treatments (PPP) | 85 | 0.16‡ | 0.22 (-0.11 to 0.54) | 0.185 | ||||
†Results are β-regression coefficients yielded from univariate and multivariate linear regression modeling, respectively, directly conveying the effect of a 1-unit increase of a given predictor on the price considered reasonable
‡Pearson correlation coefficients
§Applying a stepwise backward approach by sequentially removing variables not-significant at the p < 0.05 level until reaching the final model
¶Original question: ‘If your physician recommended this new medication to you, what would be a reasonable price to pay for it per month?’ (expressed in US dollars)
Bolded p-values are statistically significant at the 0.05 level.
PPP: Purchasing power parity; SD: Standard deviation.
Factors independently associated with a $PPP price considered reasonable by physicians for psoriasis medication are summarized in Table 5. Average treatment duration of patients currently treated (p < 0.001) was the only remaining significant predictor in multivariate analysis.
| Physicians' results¶ (n = 64) | n | Univariate analysis | Multivariate analysis§ | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Unadjusted coefficient† (95% CI) | p-values | Adjusted coefficient† (95% CI) | p-value | |||
| Country | Egypt | 16 | 524 ± 1125 | 0 (ref) | 0.606 | ||
| India | 18 | 557 ± 476 | 33 (-410 to 476) | ||||
| Indonesia | 10 | 198 ± 65 | -326 (-846 to 193) | ||||
| Philippines | 10 | 616 ± 318 | 92 (-428 to 612) | ||||
| Thailand | 10 | 545 ± 283 | 21 (-499 to 540) | ||||
| Physician specialty | Dermatologist | 64 | 500 ± 638 | – | – | ||
| Physician sector | Public | 20 | 203 ± 147 | 0 (ref) | 0.028 | ||
| Private | 21 | 553 ± 505 | 350 (-32 to 732) | ||||
| Public & private | 23 | 710 ± 886 | 507 (134 to 881) | ||||
| Considers patient ability to pay when prescribing | Yes | 64 | 500 ± 638 | – | – | ||
| Awareness of funding programs to assist patients in payment for psoriasis treatment | No | 43 | 471 ± 712 | 0 (ref) | 0.612 | ||
| Yes | 21 | 558 ± 461 | 87 (-254 to 429) | ||||
| Factors influencing prescription willingness apart from safety/efficacy | Brand | 4 | 936 ± 687 | 0(ref) | 0.285 | ||
| Local availability | 10 | 251 ± 182 | -685 (-1435 to 64) | ||||
| Delivery method | 4 | 320 ± 192 | -616 (-1512 to 280) | ||||
| P&R status | 46 | 532 ± 703 | -404 (-1065 to 256) | ||||
| Number of patients treated in clinic in the past year | 64 | 0.04‡ | 0.03 (-0.17 to 0.24) | 0.746 | |||
| Number of patients personally treated in the past year | 64 | 0.21‡ | 0.46 (-0.08 to 1.00) | 0.092 | |||
| Average treatment duration of patients currently treated (weeks) | 58 | 0.47‡ | 28 (14 to 42) | <0.001 | 28 (14 to 42) | <0.001 | |
| % Adult patients with moderate/severe psoriasis eligible for biologic treatments | 64 | -0.01‡ | -16 (-720 to 688) | 0.964 | |||
†Results are β-regression coefficients yielded from univariate and multivariate linear regression modeling, respectively, directly conveying the effect of a 1-unit increase of a given predictor on the price considered reasonable.
‡Pearson correlation coefficients.
§Applying a stepwise backward approach by sequentially removing variables not-significant at the p < 0.05 level until reaching the final model.
¶Original question: ‘What would be a reasonable price for your patients with moderate to severe psoriasis to pay for this new medication per month?’ (expressed in US dollars).
Bolded p-values are statistically significant at the 0.05 level.
SD: Standard deviation.
Discussion
Main findings
This paper presents the results of a study on consumers’ willingness and ability to pay for new drugs developed for two different chronic conditions, CHF and psoriasis, in eight and five developing countries, respectively, using the CVM. The results from multivariate analysis indicate that country, recent angiotensin receptor blocker purchase and $PPP monthly income were significant factors impacting patients’ WTP for CHF treatment, while country, education level, monthly $PPP income and monthly $PPP out-of-pocket expenses for psoriasis treatment were significant factors for patients’ WTP for psoriasis treatment. For physicians, treatment sector was a significant factor in reasonable price for both CHF and psoriasis treatment, while country was a factor for CHF treatment and average treatment duration for patients currently treated was a factor in WTP for psoriasis treatment.
Individual economic factors
Previous studies have shown that stated inability to pay for treatment is a common reason for un-WTP for treatment [1]. In the current study, monthly $PPP income was a significant factor in patients’ WTP for both CHF and psoriasis treatment. This suggests that individual economic resources are a key determinant independent of the morbidity and mortality risk associated with a given disease. It is important to consider this economic factor when establishing pricing models, especially for diseases with higher long-term health risks that could ultimately results in higher patient care costs overtime. For example, while a patient who forgoes psoriasis treatment due to economic constraints is less likely to require more expensive care in the future, patients who forgo relatively cost-effective oral medication for CHF may require costly interventions or life-saving treatments in the future. Pricing models for diseases with significant morbidity and mortality should be designed to encourage early use of less costly therapies even among those patients with limited financial ability to pay in order to reduce or minimize the need for more costly care in the future [12,13].
Sociopsychological factors
In this study, the association between education level and WTP was significant only for psoriasis patients (persisting in multivariate analysis) but not for CHF patients, suggesting the influence of psychological factors related to social interactions and aesthetic concerns on WTP. This is consistent with a previous study demonstrating that dermatological diseases have a negative impact on health-related QoL even in the absence of serious physical limitations or discomfort [14]. Patients with higher education levels may be engaged in work-related activities in which their physical appearance may impact their ability to succeed or achieve career advancement, leading to an association between education level and a disease with aesthetic effects. Similarly, more educated patients may have higher aspirations for social status than their less-educated peers, increasing the value of personal appearance among the more educated patients. In contrast, no correlation was observed between education level and patient WTP for CHF treatment. This may be due to patients at all educational levels understanding the serious nature of CHF.
Comparisons patients/physicians
Price recommendations from physicians appear lower than WTP stated by patients across the factors assessed in this study. This discrepancy appears even more markedly in psoriasis patients, which is consistent with previous reports indicating that physicians tend to be more willing to prescribe more expensive therapies if they address diseases that are life-threatening rather than conditions that impact QoL but do not affect survival [15]. That patients with psoriasis are willing to pay more for treatment than their physicians recommend underscores a possible disconnect between the consumer and medical communities with respect to the negative effects that dermatologic diseases impose on patients’ day-to-day lives [14] and the related benefits they might expect from new therapy, to be compared with the physicians’ point of view who have a broad experience seeing how these treatments actually work in larger populations and real life settings.
Implications of results on price decisions
Previous results suggest that WTP surveys are reliable and valid, and improve a program manager’s ability to predict client responses to price changes [11]. Our findings provide insight into factors that impact patients’ and physicians’ WTP for chronic disease therapies and may help guide the development of both pricing models and educational programs that align the actual and perceived physical and psychosocial benefits of different therapies. We identified patient financial ability to pay for therapy as a significant factor in WTP for both CHF and psoriasis treatment. From a price model perspective, models that provide additional subsidies for those patients with fewer financial resources may help increase use of cost-effective therapies earlier in the disease process, delaying or avoiding the need for most costly treatments in the future. This would be beneficial to both patients and countries’ health systems. For diseases with high risks of morbidity, mortality and increased costs of future care, educating patients about the benefits that specific treatments can provide may help increase the perceived value of these therapies and drive a similar increase in patient WTP.
The finding that educated psoriasis patients have a higher WTP for treatment than their physicians again suggests that there is a disconnect between how these two groups view the effects of the disease on daily life. Educational programs designed to help physicians understand the psychosocial impacts of psoriasis may be important for ensuring that they effectively address their patients’ needs.
Limitations
Our study has several limitations. First, the sample size per country was limited and cross-country comparisons should thus be interpreted with caution, considering the multiplicity of factors possibly involved, including economic (gross domestic product), health insurance (out-of-pockets payments) and cultural elements and/or access to generic medications. Some potential relationships may also have been overlooked due to insufficient statistical power. However, despite the relatively low number of respondents, we were able to identify important factors that impact patients’ WTP and physician perception of a reasonable price to be paid by their patients for chronic disease treatments. Our findings also appear consistent with previous reports on the topic and are likely to be reproducible in other comparable settings and/or in larger surveys. Regarding the method used, we did not observe any ‘protest zeros’, which may occur when respondents reject some aspect of the contingent valuation (CV) market scenario by reporting a zero value even though they place a positive value on the amenity being valued, and thus may affect the reliability [16]. Second, considering the CVM used in the present study, a hypothetical bias cannot be ruled out, referring to the discrepancy between the hypothetical WTP stated by respondents in laboratory or field experiments and the actual (revealed) amount they would pay. It has been well documented in systematic reviews that hypothetical WTP values systematically overestimate the actual payments [17]. Despite this limitation which probably affected the accuracy of our estimates of absolute WTP values, it is noteworthy that the main objective of our work was focused on the identification of the factors associated with WTP, thus most likely preserving the relevance of our results. Finally, the study population was sampled from the two most populous cities from each country, thus precluding direct generalization to the whole population.
Conclusion
The results of this study demonstrate how a CVM can be used to identify factors that impact patient and physician WTP for treatments that address chronic diseases that have different morbidity, mortality and psychosocial impact profiles. Information gleaned from surveys similar to those used in this study may provide important insight that can support the development of pricing models that achieve an optimum balance between program sustainability and patient access to quality care.
Predicting patient response to the price of therapeutics in developed countries has become critical for effective public health program management and new drug development.
Willingness to pay (WTP) techniques such as the contingent valuation approach are increasingly been applied to inform policy decisions in healthcare.
Factors associated with WTP in chronic disease management include disease-related and socio-economic factors, but also other potentially relevant but less-studied factors including physician-specific, health system and psychocultural factors.
Yet, few studies have evaluated patients’ WTP across multiple chronic disease areas while also accounting for the interactions between factors influencing chronic disease management.
Chronic heart failure and psoriasis are two chronic diseases both very common, the former being marked by severe morbimortality, the latter by generally less pronounced physical manifestations but psychological burden and social stigma, thus provide a potentially useful model for gaining insight into the factors that impact WTP.
In this survey performed in ten developing countries, we used a stated WTP contingent valuation method to investigate and compare patients’ WTP for medications and physician’s views on the cost of therapy for heart failure and psoriasis.
Independent factors influencing patient WTP were income and purchase of branded treatment for chronic heart failure therapy, and income, out-of-pocket treatment costs but also higher education level for psoriasis therapy, suggesting the influence of sociopsychological factors in this disease.
Disease-specific factors may affect WTP for treatment that should be accounted for to support effective public health programs in developing countries.
Author contributions
E Audureau contributed to the conception of the work, data analysis and interpretation, and to drafting the manuscript. B Davis contributed to the conception of the work, data acquisition and interpretation of the results, and to revising critically the manuscript. MH Besson, J Saba and J Ladner contributed to the conception of the work, interpretation of the results and to revising critically the manuscript. All authors gave their final approval of the manuscript and agreed to be accountable for all aspects of the work.
Financial & competing interests disclosure
No conflict of interest and no specific funding for the present analysis. The present work was conducted by Axios International in the framework of the establishment of a tracing strategy for two new products of a pharmaceutical company in low to middle income countries. The company had no role in the study design, analyses or drafting of the manuscript. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance has been used for the creation of the manuscript and funded by Axios International.
Ethical conduct
An informed and signed consent has been obtained from all participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Tambor M, Pavlova M, Rechel B, Golinowska S, Sowada C, Groot W. Willingness to pay for publicly financed health care services in Central and Eastern Europe: evidence from six countries based on a contingent valuation method. Soc. Sci. Med. 116, 193–201 (2014).
2.
Breidert C, Hahsler M, Reutterer T. A review of methods for measuring willingness-to-pay. Innov. Market. 2(4), 8–32 (2006).
• Provides key background on mehods for measuring willingness to pay.
3.
Whitty JA, Lancsar E, Rixon K, Golenko X, Ratcliffe J. A systematic review of stated preference studies reporting public preferences for healthcare priority setting. Patient 7(4), 365–386 (2014).
4.
Lin PJ, Cangelosi MJ, Lee DW, Neumann PJ. Willingness to pay for diagnostic technologies: a review of the contingent valuation literature. Value Health 16(5), 797–805 (2013).
5.
Deogaonkar R, Hutubessy R, Van Der Putten I, Evers S, Jit M. Systematic review of studies evaluating the broader economic impact of vaccination in low and middle income countries. BMC Public Health 12, 878 (2012).
6.
Whitty JA, Stewart S, Carrington MJ et al. Patient preferences and willingness-to-pay for a home or clinic based program of chronic heart failure management: findings from the Which? trial. PLoS ONE 8(3), e58347 (2013).
7.
Delfino M, Jr., Holt EW, Taylor CR, Wittenberg E, Qureshi AA. Willingness-to-pay stated preferences for 8 health-related quality-of-life domains in psoriasis: a pilot study. J. Am. Acad. Derm. 59(3), 439–447 (2008).
• Provides key information on quality of life and preferences of patients with psoriasis.
8.
Ademi Z, Pasupathi K, Liew D. Cost–effectiveness of eplerenone compared to usual care in patients with chronic heart failure and NYHA class II symptoms, an Australian perspective. Medicine 95(18), e3531 (2016).
9.
Beikert FC, Langenbruch AK, Radtke MA, Kornek T, Purwins S, Augustin M. Willingness to pay and quality of life in patients with atopic dermatitis. Arch. Dermatolog. Res. 306(3), 279–286 (2014).
10.
Bridges JF. Stated preference methods in health care evaluation: an emerging methodological paradigm in health economics. Ap. Health Econ. Health Pol. 2(4), 213–224 (2003).
• Other overview of stated preference techniques in health economics.
11.
Foreit JR, Foreit KG. The reliability and validity of willingness to pay surveys for reproductive health pricing decisions in developing countries. Health Policy 63(1), 37–47 (2003).
12.
Fendrick AM, Chernew ME. Value-based insurance design: aligning incentives to bridge the divide between quality improvement and cost containment. Am. J. Manag. Care 12(Spec no.), SP5–SP10 (2006).
13.
Braithwaite R, Rosen AB. Linking cost sharing to value: an unrivaled yet unrealized public health opportunity. Ann. Intern. Med. 146(8), 602–605 (2007).
14.
Radtke MA, Schafer I, Gajur A, Langenbruch A, Augustin M. Willingness-to-pay and quality of life in patients with vitiligo. Brit. J. Dermatol. 161(1), 134–139 (2009).
15.
Greenberg D, Hammerman A, Vinker S, Shani A, Yermiahu Y, Neumann PJ. Which is more valuable, longer survival or better quality of life? Israeli oncologists' and family physicians’ attitudes toward the relative value of new cancer and congestive heart failure interventions. Value Health 16(5), 842–847 (2013).
• Provides key information on quality of life and preferences of patients with chronic health failure.
16.
Fonta WM, Ichoku HE, Kabubo-Mariara J. The effect of protest zeros on estimates of willingness to pay in healthcare contingent valuation analysis. Ap. Health Econ. Health Pol. 8(4), 225–237 (2010).
17.
Murphy JJ, Allen PG, Stevens TH, Weatherhead D. A Meta-analysis of hypothetical bias in stated preference valuation. Environ. Resource Econ. 30(3), 313–325 (2005).
Information & Authors
Information
Published In
Copyright
© 2019 Axios International.
History
Received: 8 October 2018
Accepted: 21 December 2018
Published online: 16 January 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Willingness to pay for medical treatments in chronic diseases: a multicountry survey of patients and physicians. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0106
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Maryam Karandish, Sulmaz Ghahramani, Fatemeh Mohammadi, Mohammad Sayari, Seyyed Hossein Owji, Najmeh Moradi, Willingness to Pay for a Service Package Solving the Problems of Patients With Cleft Lip and Palate Referred to the Cleft Lip and Palate Center, International Journal of Paediatric Dentistry, 10.1111/ipd.70059, (2025).
- Hien Thi Bich Tran, Viet Nhu Nguyen, Phuong Nhat Le, Trung Quang Vo, Hiep Thanh Nguyen, Due The Ong, Van Nu Hanh Pham, Thao Ho Dieu Nguyen, Nhi Pham Yen Le, Setting cost-effectiveness thresholds for health technologies in Vietnam: A WTP/QALY approach, Health Policy and Technology, 10.1016/j.hlpt.2024.100972, 14, 3, (100972), (2025).
- Alexander H. Gunn, Haider J. Warraich, Robert J. Mentz, Costs of care and financial hardship among patients with heart failure, American Heart Journal, 10.1016/j.ahj.2023.12.001, 269, (94-107), (2024).
- I. S. van Maurik, E. D. Bakker, A. A. J. M. van Unnik, H. M. Broulikova, M. D. Zwan, E. van de Giessen, J. Berkhof, F. H. Bouwman, J. E. Bosmans, W. M. van der Flier, How healthy participants value additional diagnostic testing with amyloid-PET in patients diagnosed with mild cognitive impairment — a bidding game experiment, Alzheimer's Research & Therapy, 10.1186/s13195-023-01346-y, 15, 1, (2023).
- Nurin Haniah Asmuni, Adina Najwa Kamarudin, Norazliani Md Lazam, Hafizah Besar Sa'aid, Willingness to pay for heart disease insurance: A case study of a university hospital in Malaysia, The 5TH ISM INTERNATIONAL STATISTICAL CONFERENCE 2021 (ISM-V): Statistics in the Spotlight: Navigating the New Norm, 10.1063/5.0110694, (020018), (2023).
- Caroline Steigenberger, Magdalena Flatscher-Thoeni, Uwe Siebert, Andrea M. Leiter, Determinants of willingness to pay for health services: a systematic review of contingent valuation studies, The European Journal of Health Economics, 10.1007/s10198-022-01437-x, 23, 9, (1455-1482), (2022).
- Theodoros V. Giannouchos, Benjamin Ukert, Athanassios Vozikis, Evangelia Steletou, Kyriakos Souliotis, Informal out-of-pocket payments experience and individuals’ willingness-to-pay for healthcare services in Greece, Health Policy, 10.1016/j.healthpol.2021.04.001, 125, 6, (693-700), (2021).
- N. Poudel, B. Banjara, S. Kamau, N. Frost, S. Ngorsuraches, Factors influencing patients’ willingness-to-pay for disease-modifying therapies for multiple sclerosis, Multiple Sclerosis and Related Disorders, 10.1016/j.msard.2020.102720, 48, (102720), (2021).
- V. Boima, K. Agyabeng, V. Ganu, D. Dey, E. Yorke, M. B. Amissah-Arthur, A. A. Wilson, A. E. Yawson, C. C. Mate-Kole, J. Nonvignon, Willingness to pay for kidney transplantation among chronic kidney disease patients in Ghana, PLOS ONE, 10.1371/journal.pone.0244437, 15, 12, (e0244437), (2020).