Impact of selective serotonin reuptake inhibitors in the veteran population: 10-year risk outcomes
Abstract
Aim: To evaluate the comparative risk of hip fracture or osteoporosis among US Veterans based on selective serotonin reuptake inhibitor (SSRI) exposure. Patients & methods: A retrospective cohort study of eligible US Veterans Health Administration patients enrolled in 2003–2004 was performed to examine SSRIs’ 2-, 5- and 10-year impact on bone health using multiple logistic regression. Results: Veterans on SSRIs were found to be 56.7% more likely over a 10-year period to suffer a hip fracture (risk ratio: 1.567; 95% CI: 1.464–1.676) and 34.6% more likely to develop osteoporosis (risk ratio: 1.346; 95% CI: 1.319–1.374) when compared with those who were SSRI naive. Conclusion: SSRI usage was associated with greater risk of hip fracture and osteoporosis over a 10-year period in the veteran population, with similar effect sizes to smaller studies.
Military service is associated with an increased risk of anxiety, depression and post-traumatic stress disorder (PTSD). One study found 0.6% of all new military recruits had anxiety or depression prior to joining the military [1]. In another study of junior enlisted army soldiers (E-4 and below) who spent at least 7 months in a combat zone, 6.4% met the clinical criteria for anxiety or depression [2]. Further, another study of all recently discharged Operation Iraqi Freedom, Operation Enduring Freedom (OIF/OEF) veterans seen at United States Department of Veterans Affairs (VA) healthcare facilities found 25% had at least one mental health diagnosis, with PTSD (13%), anxiety (6%) and depression (5%) being some of the most common [3].
A common treatment for anxiety, depression and PTSD is selective serotonin-reuptake inhibitor (SSRI) therapy, which is generally considered safe, is well-tolerated and indicated for a wide range of conditions. SSRIs are indicated in the VA-DoD clinical practice guidelines for all severities of major depressive disorder [4] and PTSD [5].
While for single-episode treatment there is a recommendation to discontinue after 1 year [6], if there is a relapse a clinician may be reluctant to discontinue SSRI therapy due to the increased likelihood of recurrence. Therefore, SSRI therapy could be quite lengthy. A young veteran recently released from active duty after 4 years of service can be as young as 21 and potentially placed on SSRIs for decades to help manage the symptoms of anxiety, depression or PTSD – raising questions of long-term effects of this class of medications.
SSRIs are believed to have an overall negative serotonergic effect on bone regulation [7]. SSRIs have been found to inhibit the formation and function of osteoclasts and osteoblasts in humans [8]. Further, serotonin transporters have been identified in bone [8–10], suggesting that SSRIs could affect bone metabolism and increase the risk of osteoporosis.
Numerous studies have looked at the effect of SSRIs on bone health. One small study (n = 51) found a correlation between SSRI usage and calcaneal bone mineral density in young adults, aged 18–25 [11]. A registry study of Norwegians aged 60 and older (n = 906,422) over a 5-year period found a higher incidence of hip fracture among SSRI users [12]. One meta-analysis of 34 studies (n = 1,217,464 people) found an increased risk of any fracture among SSRI and tricyclic antidepressant users, odds ratio (OR) was 1.39 (95% CI: 1.32–1.47) and for hip fracture: OR = 1.47 (95% CI: 1.36–1.58) [13]. However, studies are limited in their lack of ethnic diversity [12], sample size [11,14], limited patient age range or by using solely perimenopausal women [15].
This study was designed to examine the impact of SSRIs on bone health, using hip fracture or initial diagnosis of osteoporosis as outcomes in a large sample, among Veterans Health Administration (VHA) patients over one decade. It is our hypothesis that veterans exposed to SSRIs have higher risk of hip fracture and being diagnosed with osteoporosis than veterans who are SSRI naive.
Materials & methods
To compare the rate of hip fracture or being diagnosed with osteoporosis among those who are on SSRIs versus those who are SSRI naive, this study used a retrospective longitudinal cohort design where VHA patients who were receiving care at any VA medical center in the index period (2003–2004) were identified and assessed for eligibility criteria. Eligible patients were followed for 10 years, or until they left the VA system to answer the research questions. All analyses were performed using SAS version 9.4 (NC, USA). Statistical significance was defined a priori at α = 0.05. The minimal clinically important difference in risk for hip fracture was defined as 20% [16]. This study was reviewed and approved by the Institutional Review Board at the Medical University of South Carolina.
Dataset construction
All veteran patients of 18–75 years of age who were continuously enrolled for healthcare at the VA during the years of 2003–2004 were identified from the VHA's corporate data warehouse. This warehouse contains the full treatment records of each patient – including inpatient and outpatient treatment, medication dispensing and demographic information. Patients were excluded if they were diagnosed with osteoporosis (International Classification of Diseases-9th Revision-Clinical Modifications [ICD-9-CM] of 733.00-.03 and 733.09), hip fracture (820.X), or failure to thrive (783.41 or 783.7) prior to enrollment (Figure 1). Patients on calcitonin nasal spray [17] or bisphosphonates [18] during the baseline period were also excluded as they are common treatments for corticosteroid-induced osteoporosis, as were patients on hormone replacement therapy (estrogens or progestins). Patients had to be actively enrolled at the VA for at least 24 months, the entire fiscal years 2003 and 2004.
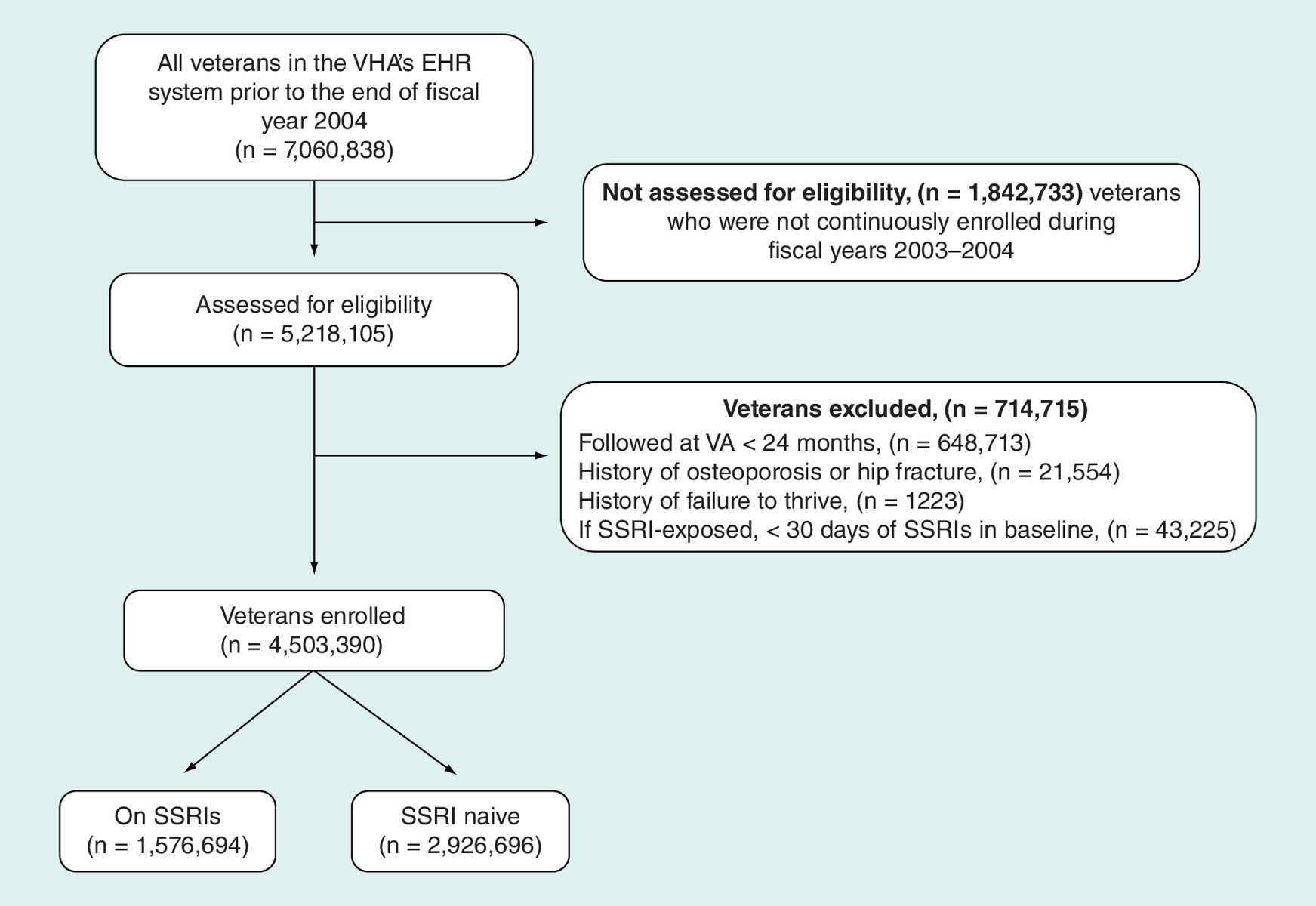
Figure 1. Patient flow diagram.
EHR: Electronic health record; SSRI: Selective serotonin-reuptake inhibitor; VA: United States Department of Veterans Affairs; VHA: Veterans Health Administration.
Patients were stratified into cohorts according to SSRI usage. The list of SSRIs included: citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine and sertraline. Patients in the SSRI cohort had to have at least 30 days of SSRI medication filled in the baseline period (2003–2004). Patients in the control group had to be naive of SSRI medication throughout the baseline period.
The primary outcome of hip fracture was defined through an inpatient or outpatient primary ICD-9-CM diagnosis of 820.X. As hip fracture is an emergent event, the initial treatment may not have occurred at a VHA facility, although the follow-up care, including rehabilitation, would have been through the VHA. Therefore all inpatient and outpatient records were reviewed for a diagnosis of hip fracture. The secondary outcome of osteoporosis was defined as 733.00–03 or 733.09. Comorbidity was assessed using the Deyo update to the Charlson comorbidity index [19], which is a validated measure to adjust for a patient's 1-year risk of mortality [20]. Diagnoses recorded during the enrollment period were used to construct the Charlson comorbidity index for each patient.
Statistical analysis
Descriptive statistics were used to compare the characteristics of the two cohorts. Means and standard deviations were calculated to describe continuous data. Frequencies and percentages were calculated to describe categorical data. Univariate statistical tests to compare the two cohorts were not conducted, due to large sample sizes – which would inflate type-I error.
Multiple logistic regression models were used for the outcome variables, to compare the rate of hip fracture or initial diagnosis of osteoporosis between the two cohorts at 2, 5 and 10 years post study enrollment. The main independent variable in these regressions was a binary indicator of SSRI utilization. Variables investigated to control for potential confounding differences between these cohorts were age, sex, race, marital status, presence of secondary healthcare insurance, catastrophic disability [21], being a combat veteran, alcohol dependence, tobacco use disorder and body mass index category (confer [c.f.] Table 1 for ICD-9-CM codes). Manual backward regression model fitting was used. Potential covariates not found to significantly contribute to the model were removed one at a time, and the models were then refit using standard model fitting methods [22]. Covariates were assessed for collinearity using Pearson correlation coefficients; no collinearity was found in these data (all p > 0.25). All multiple logistic regression models were then re-ran using a modified Poisson regression model with a robust error variance to yield adjusted relative risk (RR) and corresponding 95% CIs, as these outcomes are relatively rare events and RR yields better estimates of effect size than ORs [23].
| Outcomes | |
|---|---|
| – Hip fracture – Osteoporosis | – 820.X – 733.00, 733.01, 733.02, 733.03, 733.09 |
| Exclusions | |
| – Failure to thrive – Hip fracture – Osteoporosis | – 783.41, 783.7 – 820.X – 733.00, 733.01, 733.02, 733.03, 733.09 |
| Comorbidities | |
| – Alcohol dependence – Anxiety – Calcium metabolism disorder – Dysthymia – Major depressive disorder – Morbid obesity – Obese – Overweight – PTSD – Tobacco use disorder | – 303.90, 303.91, 303.92 – 300.00, 300.01, 300.02, 300.09 – 275.4X – 300.4 – 296.2X, 296.3X – 278.01 – 278.00 – 278.02 – 309.81 – 305.1, F17.210 |
PTSD: Post-traumatic stress disorder.
Results
After applying exclusion and inclusion criteria, 4,503,390 veterans were enrolled; 1,576,694 (35%) were in the SSRI cohort, 2,926,696 (65%) were in the SSRI-naive cohort (Figure 1). Because of large sample size, p-values are not given because all differences in baseline characteristics were significant. However, qualitatively the two cohorts do not appear to differ significantly with respect to most baseline demographics (Table 2). The groups were 95.3% male for the SSRI-naive cohort and 91.2% male in the SSRI cohort. Secondary insurance was common (73.3 vs 70.9%). The rate of catastrophic disability was rare (0.7 vs 1.0%). The groups seemed to differ with respect to Charlson score (77.4% had a score of zero vs 70.5%), age (56.8 vs 52.4 years), race (60.0% Caucasian vs 64.5%), combat veteran status (12.3 vs 19.7%) and prevalence of diagnoses for which SSRIs are prescribed (e.g., anxiety, depression and PTSD). The average duration of study enrollment was 8 years, 5 months for the SSRI-naive cohort and 9 years for the SSRI cohort; however, 2,916,463 (64.8%) of veterans were followed for the full 10 years (Table 3).
| Overall | SSRI naive | On SSRIs | |
|---|---|---|---|
| Characteristic | n = 4,503,390 | n = 2,926,696 | n = 1,576,694 |
| Age (years) | 55.2 ± 13.0 | 56.8 ± 13.1 | 52.4 ± 12.4 |
| Sex: | |||
| – Males | 4,227,241 (93.9) | 2,788,993 (95.3) | 1,438,248 (91.2) |
| – Females | 276,149 (6.1) | 137,703 (4.7) | 138,446 (8.8) |
| Secondary insurance: | 3,261,976 (72.4) | 2,144,608 (73.3) | 1,117,368 (70.9) |
| – Medicaid | 116,846 (2.6) | 60,512 (2.1) | 56,334 (3.6) |
| Catastrophically disabled | 37,829 (0.8) | 21,562 (0.7) | 16,267 (1.0) |
| Race: | |||
| – Black | 652,623 (14.5) | 400,474 (13.7) | 252,149 (16.0) |
| – White | 2,773,710 (61.6) | 1,755,979 (60.0) | 1,017,731 (64.5) |
| – Other/missing | 1,077,057 (23.9) | 770,243 (26.3) | 306,814 (19.5) |
| Married | 2,463,627 (54.7) | 1,692,877 (57.8) | 770,750 (48.9) |
| Combat veteran | 669,286 (14.9) | 358,522 (12.3) | 310,764 (19.7) |
| Charlson score: | |||
| – 0 | 3,377,438 (75.0) | 2,265,707 (77.4) | 1,111,731 (70.5) |
| – 1 | 606,777 (16.5) | 346,491 (11.8) | 260,286 (16.5) |
| – 2+ | 519,175 (13.0) | 314,498 (11.5) | 204,677 (13.0) |
| Months in study | 103 ± 28 | 101 ± 29 | 108 ± 25 |
| Diagnoses:† | |||
| – Alcohol dependence | 159,520 (3.5) | 56,495 (1.9) | 103,025 (6.5) |
| – Anxiety | 154,741 (3.4) | 36,602 (1.3) | 118,139 (7.5) |
| – Calcium metabolism disorder | 4352 (0.1) | 2553 (0.1) | 1799 (0.1) |
| – Dysthymia | 147,505 (3.3) | 19,339 (0.7) | 128,166 (8.1) |
| – Major depressive disorder | 242,531 (5.4) | 27,719 (0.9) | 214,812 (13.6) |
| – Post-traumatic stress disorder | 332,815 (7.4) | 59,733 (2.0) | 273,082 (17.3) |
| – Tobacco use disorder | 448,806 (10.0) | 231,953 (7.9) | 216,853 (13.8) |
| Weight category:‡ | |||
| – Normal/overweight | 4,147,862 (92.1) | 2,717,531 (92.9) | 1,430,331 (90.7) |
| – Obese | 323,995 (7.2) | 191,858 (6.6) | 132,137 (8.4) |
| – Morbidly obese | 31,533 (0.7) | 17,307 (0.6) | 14,226 (0.9) |
All values are mean ± standard deviation, n (%), or as otherwise indicated.
†See Table 6 for a list of ICD-9-CM diagnoses.
‡Weight category as reported by diagnosed conditions during the baseline period. Subjects without a diagnosis of being overweight/obese/morbidly obese were considered to be of normal weight. Due to undercoding, overweight subjects were grouped with normal weight subjects.
ICD-9-CM: International Classification of Diseases-9th Revision-Clinical Modification; SSRI: Selective serotonin reuptake inhibitor.
| Number of patients | ||||
|---|---|---|---|---|
| Overall | SSRI naive | On SSRIs | ||
| Total patients: | – Year 2 | 4,503,390 | 2,926,696 | 1,576,694 |
| – Year 5 | 3,929,779 | 2,492,451 | 1,437,328 | |
| – Year 10 | 2,916,463 | 1,782,961 | 1,133,502 | |
| Hip fractures: | – Year 2 | 1190 | 524 | 666 |
| – Year 5 | 3105 | 1507 | 1598 | |
| – Year 10 | 7229 | 3536 | 3693 | |
| Osteoporosis: | – Year 2 | 18,112 | 6887 | 11,225 |
| – Year 5 | 38,666 | 15,634 | 23,032 | |
| – Year 10 | 64,681 | 27,192 | 37,489 | |
SSRI: Selective serotonin-reuptake inhibitor.
Of those who were on SSRIs during the 10-year study period, the most common prescriptions were for citalopram (32.9%), sertraline (32.7%) and fluoxetine (19.8%) (Table 4). However, when examining the dosages of these medications – using defined daily dose (DDD) – fluvoxamine is prescribed in the highest doses, totaling 8.7 billion DDD, followed by sertraline at 1.3 billion DDD (Table 4).
| SSRIs | Prescriptions | Defined daily doses | ||
|---|---|---|---|---|
| Count | Percentage of total | Count | Percentage of total | |
| Citalopram | 12,725,362 | 32.9% | 977,521,126 | 8.1% |
| Escitalopram | 500,548 | 1.3% | 36,138,623 | 0.3% |
| Fluoxetine | 7,671,672 | 19.8% | 626,554,261 | 5.2% |
| Fluvoxamine | 124,292 | 0.3% | 8,720,136,250 | 72.2% |
| Paroxetine | 5,002,514 | 12.9% | 366,832,111 | 3.0% |
| Sertraline | 12,636,554 | 32.7% | 1,343,740,022 | 11.1% |
| Total | 38,660,942 | 12,070,922,393 | ||
The defined daily dose for selective serotonin-reuptake inhibitors is defined as the dose for moderately severe symptoms. One defined daily dose is defined as follows: citalopram (20 mg), escitalopram (10 mg), fluoxetine (20 mg), fluvoxamine (0.1 g), paroxetine (20 mg) and sertraline (50 mg) [24].
The crude rate per 10,000 people who experienced a hip fracture by year 10 differed between the two groups (19.83 for the SSRI-naive cohort vs 32.58 for the SSRI-exposed cohort; Table 5). The crude rate per 10,000 people who were diagnosed with osteoporosis by year 10 also differed between the two groups (152.51 for the SSRI-naive cohort vs 330.74 for the SSRI-exposed cohort).
| Crude rates (Per 10,000 people) | ||||
|---|---|---|---|---|
| SSRI naive | On SSRIs | Rate difference | ||
| Hip fracture: | – Year 2 | 1.79 | 4.22 | 135.9% |
| – Year 5 | 6.05 | 11.12 | 83.9% | |
| – Year 10 | 19.83 | 32.58 | 64.3% | |
| Osteoporosis: | – Year 2 | 23.53 | 71.19 | 202.5% |
| – Year 5 | 62.73 | 160.24 | 155.5% | |
| – Year 10 | 152.51 | 330.74 | 116.9% | |
SSRI: Selective serotonin-reuptake inhibitor.
The final adjusted logistic regression models used the following covariates to control for potential confounding differences in the cohorts: age category (18–29, 30–39, 40–49, 50–59, 60–69, 70–89), sex, race (Black, White, other/missing), marital status, Charlson score, catastrophic disability, weight category (normal/overweight, obese, morbidly obese), alcohol dependence and tobacco use disorder. These models showed that subjects on SSRIs were 42.7% more likely to suffer a hip fracture by year 2 (RR: 1.427; CI: 1.261–1.615; p < 0.0001), 66.8% more likely by year 5 (RR: 1.668; CI: 1.525–1.824; p < 0.0001), and 56.7% more likely by year 10 (RR: 1.567; CI: 1.464–1.676; p < 0.0001) than those who were SSRI naive (Table 6). At year 2, being married showed a slight protective effect (RR: 0.512; CI: 0.454–0.579), as did being of Black vs White race (RR: 0.677, CI: 0.551–0.831), whereas having a catastrophic disability was shown to be a hazard (RR: 2.545; CI: 1.796–3.606), as was alcohol dependence (RR: 1.863; CI: 1.488–2.334), and tobacco use disorder (RR: 1.229; CI: 1.039–1.454).
| Adjusted relative risk | Adjusted ORs | ||||
|---|---|---|---|---|---|
| RR | 95% CI | OR | 95% CI | ||
| Hip fracture: | – Year 2 | 1.427 | (1.261–1.615) | 1.440 | (1.261–1.615) |
| – Year 5 | 1.668 | (1.525–1.824) | 1.670 | (1.525 –1.824) | |
| – Year 10 | 1.567 | (1.464–1.676) | 1.568 | (1.464–1.676) | |
| Osteoporosis: | – Year 2 | 1.280 | (1.240–1.321) | 1.365 | (1.240–1.321) |
| – Year 5 | 1.356 | (1.325–1.388) | 1.346 | (1.325–1.388) | |
| – Year 10 | 1.346 | (1.319–1.374) | 1.359 | (1.319–1.374) | |
The point estimates for the RR and ORs of suffering a hip fracture or being diagnosed with osteoporosis, along with 95% CIs. RR should be used for interpretation; ORs are given for comparison of effect size with prior studies.
Variables used to control for potential confounding differences between these cohorts included: Age category (18–29, 30–39, 40–49, 50–59, 60–69, 70–89), sex, race (Black, White, other), marital status, Charlson score, weight category (normal/overweight, obese, morbidly obese), catastrophic disability, alcohol dependence and tobacco use disorder.
OR: Odds ratio; RR: Relative risk.
The final adjusted logistic regression models showed that subjects on SSRIs were 28.0% more likely to be diagnosed with osteoporosis by year 2 (RR: 1.280; CI: 1.240–1.321; p < 0.0001), 35.6% more likely by year 5 (RR: 1.356; CI: 1.325–1.388; p < 0.0001) and 34.6% more likely by year 10 (RR: 1.346; CI: 1.319–1.374; p < 0.0001) than those who were SSRI naive (Table 6 & Figure 2). Similar to the findings for the hip fracture outcomes, being of Black versus White race showed a slight protective effect (RR: 0.436, CI: 0.408–0.466), whereas having a catastrophic disability was shown to be a hazard (RR: 1.359; CI: 1.208–1.528), as was alcohol dependence (RR: 1.223; CI: 1.125–1.328), and tobacco use disorder (RR: 1.271; CI: 1.214–1.329). Interestingly, being married did not yield a protective effect in any of the osteoporosis outcomes, as it did with the hip fracture outcomes (Supplementary Table 1).
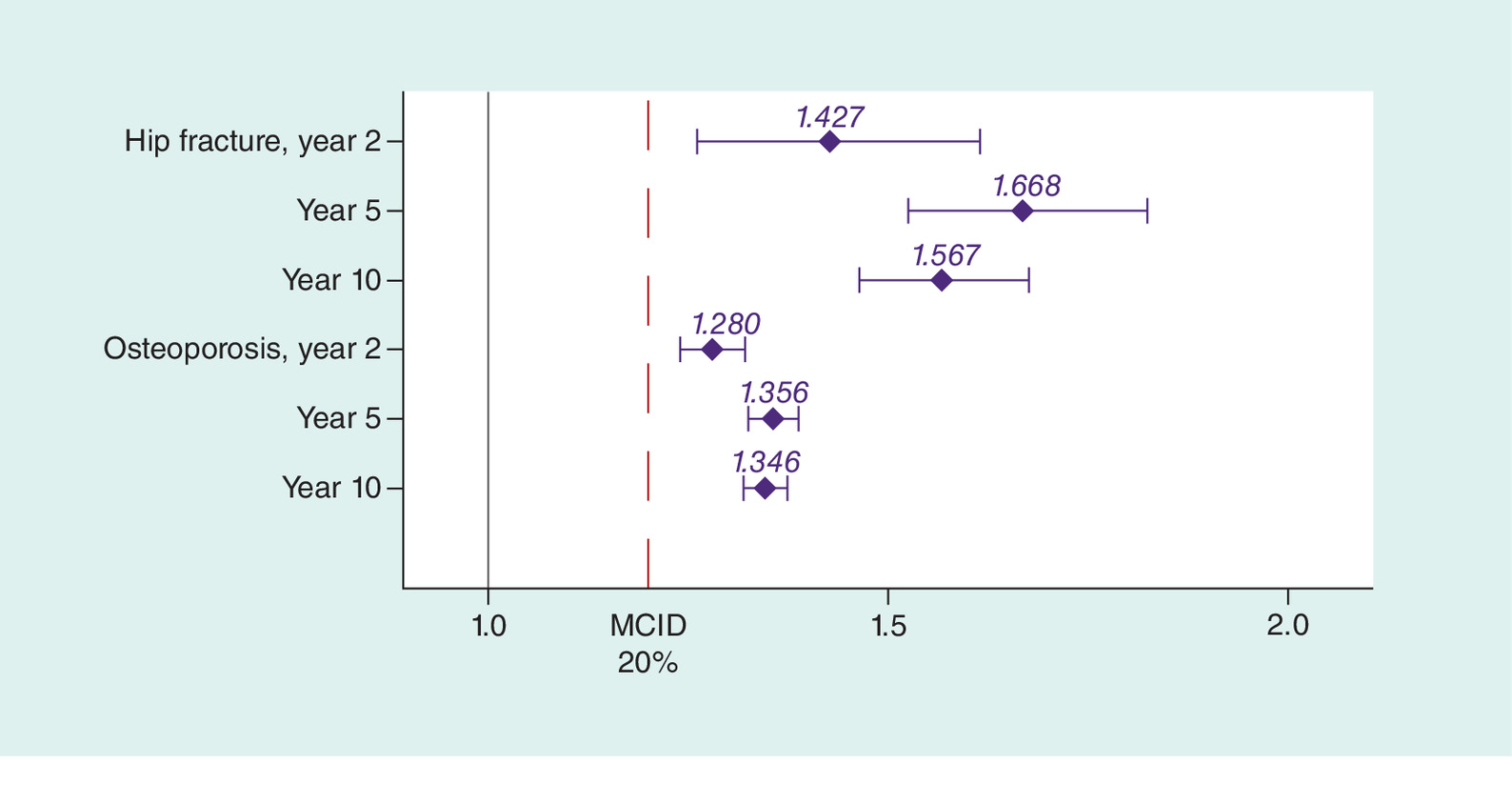
Figure 2. Adjusted risk ratios for hip fracture or osteoporosis for those on selective serotonin reuptake inhibitors compared with those who are selective serotonin reuptake-inhibitor naive.
The point estimates for the relative risk ratios of suffering a hip fracture or being diagnosed with osteoporosis, along with 95% confidence intervals. Variables used to control for potential confounding differences between these cohorts included: age (18–29, 30–39, 40–49, 50–59, 60–69, 70–89), sex, race (Black, White, other), marital status, Charlson score, weight category (normal/overweight, obese, morbidly obese), catastrophic disability, alcohol dependence, and tobacco use disorder.
MCID: Minimal clinically important difference.
To examine sensitivity of findings to a change in greater exposure to SSRIs among those in the SSRI group, a sensitivity analysis was conducted. We included only those in the SSRI-exposed group who had at least 6 months of SSRI usage during the baseline period of fiscal years 2003–2004 (n = 1,171,73) comparing results to those who were SSRI naive (n = 2,926,696). The results of this sensitivity analysis showed a negligibly small increase in effect size for all outcomes and time periods (Supplementary Table 1), demonstrating stability of this study's findings to a change in SSRI-exposure requirements.
Discussion
This study investigated the association between SSRI utilization and its effect on bone health – specifically the risk of hip fracture or developing osteoporosis. Adjusted logistic regression models found that those on SSRIs were 56.7% more likely to suffer a hip fracture over 10 years, 56.7% more likely by year 10 (RR: 1.567; CI: 1.464–1.676; ORs are given in Table 6) than those who were SSRI naive. Similarly, those same individuals were 34.6% more likely to develop osteoporosis over 10 years (RR: 1.346; CI: 1.319–1.374) than those who were SSRI naive. These findings are more conservative than a previous meta-analysis, which found that those on SSRIs had twice the odds of hip fracture (OR: 2.06; 95% CI: 1.84–2.30) [25]. A prior study suggested that a 20% change in risk of fracture was clinically important, [16] underscoring the importance of these findings.
For the provider who is treating a patient with long-term SSRI therapy, the results of this study combined with prior research raise questions about the effects of these medications on bone health over time. Given the amount of research pointing toward an association between SSRI usage and bone degradation, evidence-based osteoporosis prophylaxis may be considered for concomitant therapy. Possible options include encouraging exercise, [26] as well as possible medications known to improve bone health – such as bisphosphonates, [18] calcitonin [17] and calcium with vitamin D [27].
The incorporation of SSRI use as a possible candidate clinical risk factor in predictive tools such as the FRAX® tool should be considered, which predicts a person's 10-year risk of major osteoporotic fracture [28]. However, FRAX does not take into account SSRIs as a potential risk factor – considering only glucocorticoid medications, which are associated with corticosteroid-induced osteoporosis.
Consideration to baseline and periodic dual-energy x-ray absorptiometry (DXA; bone densitometry) measurements for patients who are likely to be initiating long-term SSRI therapy may be considered. However, limitations on reimbursement of DXA scans by insurance providers, particularly CMS in the USA, make this difficult. Further, the United States Preventive Services Taskforce's 2011 recommendations on screening for osteoporosis states the usage of DXA monitoring is beneficial in patients whose risk is greater than 9.3% using the FRAX tool [24], highlighting the need to recalibrate this instrument.
This study has several strengths. This is a population-based study, with a large study size (n = 4,503,390). The next largest study of its kind was a much smaller (n = 456,866) study of a more racially-homogeneous study of Danish subjects [29]. Further, the period of this study – 10 years – allows for sufficient follow-up to ascertain a long-term treatment effect. This study also utilized VHA records, which are extensive medical and administrative patient records going back to September, 1999. Moreover, the VHA is an integrated delivery system, benefitting from thorough patient treatment records – allowing patients to be followed longitudinally across the USA. Finally, a sensitivity analysis conducted revealed the findings were stable to a more stringent SSRI exposure requirement.
This study also has several limitations. This is a veteran-only study, comprised of predominantly male (93.9%) subjects, limiting generalizability. Further, this study utilized prescription dispensing records from VA pharmacies as an imperfect measure of medication utilization. Also, not all patients take their medications – in spite of having received their medication. Not all covariates can be accurately measured using clinical and administrative data, raising the possibility of unmeasured confounders. This study could not account for modifiable risk factors associated with an increased risk for osteoporotic fracture, such as smoking [30], excessive alcohol intake [31], nor lack of physical exercise [32,33] – all of which are more common among those with depression [34,35] and PTSD [36]. While this study controlled for tobacco use disorder and alcohol dependence diagnoses, these are likely undercoded in the records. The present study is also limited as it did not investigate the dose–response relationship of SSRIs on bone health. This study represents a first look at risk in a large group of patients. Future studies should investigate this risk in a propensity score-matched study to control for confounding – examining the dose–response relationship, and the magnitude to which known treatments that are protective of bone health can mitigate the effects of SSRIs on the risk of bone degradation.
This study has shown exposure to SSRIs is associated with increased risk of hip fracture and osteoporosis in the veteran population. The increased risk of a hip fracture or development of osteoporosis that was found through this study is of similar effect size to other studies that studied this effect in smaller sample sizes and different populations. Given these findings of similar effect size to other studies, providers may want to consider patients’ other risk factors for bone degradation prior to initiating potentially long-term SSRI therapy. Further, recalibration of existing instruments that are used to predict major osteoporotic fractures should consider incorporating SSRI usage. Future research should investigate the excess cost of fractures potentially attributable to long-term SSRI therapy, which could inform healthcare policy when considering alternatives to SSRIs and reimbursement of more aggressive bone density monitoring.
A common treatment for anxiety, depression and post-traumatic stress disorder is selective serotonin-reuptake inhibitor (SSRI) therapy. However, prior studies show a strong association between SSRI usage and risk of fractures.
The present study used a retrospective longitudinal cohort study design and US Veterans Health Administration data from 2003 to 2014 to compare the risk of hip fractures or development of osteoporosis among those who are on SSRIs and those who are not.
The findings from this study reveal differential risk of hip fracture and osteoporosis between the two groups at 2-, 5- and 10-years postindex, with those on SSRIs having a greater risk than those who were not on SSRIs.
The findings in this present study of increased risk of hip fracture or osteoporosis were of similar effect size to other studies in different populations. Resultantly, providers may want to consider patients’ other risk factors for bone degradation prior to initiating potentially long-term SSRI therapy.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2018-0085
Author contributions
DL Brinton, AC LaRue and AN Simpson did the study conception and design. DL Brinton did the acquisition of data. DL Brinton did the analysis of data. DL Brinton, CE Fominaya, AC LaRue and AN Simpson did the interpretation of data. DL Brinton, CE Fominaya and AC LaRue and AN Simpson drafted the manuscript. DL Brinton, CE Fominaya, AC LaRue and AN Simpson did the critical revision.
Financial & competing interests disclosure
Biomedical Laboratory Research and Development Program of the Department of Veterans Affairs (Merit Award BX000333). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct
The authors attest that this study was reviewed and approved by the Institutional Review Board at the Medical University of South Carolina as an expedited review study.
Supplementary Material
File (suppl_file.docx)
- Download
- 43.94 KB
References
1.
Office of The Surgeon General, United States Army Medical Command, and Office of the Command Surgeon Headquarters, US Army Central Command (USCENTCOM), and Office of the Command Surgeon US Forces Afghanistan (USFOR-A). Mental Health Advisory Team 9 (MHAT 9) Operation Enduring Freedom (OEF) Afghanistan (2013). www.hsdl.org/?abstract&did=750301.
2.
Monahan P, Hu Z, Rohrbeck P. Mental disorders and mental health problems among recruit trainees, U.S. Armed Forces, 2000–2012. MSMR 20(7), 13–18; discussion 16–18 (2013).
3.
Seal KH, Bertenthal D, Miner CR, Sen S, Marmar C. Bringing the war back home: mental health disorders among 103 788 US Veterans returning from Iraq and Afghanistan seen at Department of Veterans Affairs Facilities. Arch. Intern. Med. 167(5), 476–482 (2007).
4.
The Management of Major Depressive Disorder Working Group. VA/DoD Clinical Practice Guideline for the Management of Major Depressive Disorder, Version 3.0. 173 (2016).
5.
The Management of Post-Traumatic Stress Working Group. VA/DoD Clinical Practice Guideline for Management of Post-Traumatic Stress, Version 2.0. 198 (2010).
6.
World Health Organization. mhGAP Intervention Guide: for Mental, Neurological and Substance Use Disorders in Nonspecialized Health Settings. 174 (2016).
7.
Sansone RA, Sansone LA. SSR Is: bad to the bone? Innov. Clin. Neurosci. 9(7–8), 42–47 (2012).
8.
Hodge JM, Wang Y, Berk M et al. Selective serotonin-reuptake inhibitors inhibit human osteoclast and osteoblast formation and function. Biol. Psychiatry 74(1), 32–39 (2013).
9.
Battaglino R, Fu J, Spate U et al. Serotonin regulates osteoclast differentiation through its transporter. J. Bone Miner. Res. 19(9), 1420–1431 (2004).
10.
Bliziotes M, Eshleman A, Burt-Pichat B et al. Serotonin transporter and receptor expression in osteocytic MLO-Y4 cells. Bone 39(6), 1313–1321 (2006).
11.
Seifert CF, Wiltrout TR. Calcaneal bone mineral density in young adults prescribed selective serotonin reuptake inhibitors. Clin. Ther. 35(9), 1412–1417 (2013).
12.
Bakken MS, Engeland A, Engesaeter LB, Ranhoff AH, Hunskaar S, Ruths S. Increased risk of hip fracture among older people using antidepressant drugs: data from the Norwegian Prescription Database and the Norwegian Hip Fracture Registry. Age Ageing 42(4), 514–520 (2013).
13.
Rabenda V, Nicolet D, Beaudart C, Bruyere O, Reginster JY. Relationship between use of antidepressants and risk of fractures: a meta-analysis. Osteoporosis Int. 24(1), 121–137 (2013).
14.
Feuer AJ, Demmer RT, Thai A, Vogiatzi MG. Use of selective serotonin-reuptake inhibitors and bone mass in adolescents: an NHANES study. Bone 78, 28–33 (2015).
15.
Sheu YH, Lanteigne A, Sturmer T, Pate V, Azrael D, Miller M. SSRI use and risk of fractures among perimenopausal women without mental disorders. Inj. Prev. 21(6), 397–403 (2015).
16.
Ettinger B, Black DM, Mitlak BH et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple outcomes of raloxifene evaluation (MORE) investigators. JAMA 282(7), 637–645 (1999).
17.
Cranney A, Welch V, Adachi JD et al. Calcitonin for the treatment and prevention of corticosteroid-induced osteoporosis. Cochrane Database Syst. Rev. Cd001983 (2000).
18.
Homik J, Cranney A, Shea B et al. Bisphosphonates for steroid induced osteoporosis. Cochrane Database Syst. Rev. Cd001347 (2000).
19.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45(6), 613–619 (1992).
20.
Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40(5), 373–383 (1987).
21.
United States Code of Federal Regulations. 38 CFR § 17.36 – Enrollment – provision of hospital and outpatient care to veterans. 17.36(E) C. 38. www.law.cornell.edu/cfr/text/38/17.36.
22.
Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression (Third Edition). John Wiley & Sons, Inc., NJ, USA (2013).
23.
Zou G. A modified Poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 159(7), 702–706 (2004).
24.
U.S. Preventive Services Task Force. Screening for osteoporosis: US preventive services task force recommendation statement. Ann. Intern. Med. 154(5), 356–364 (2011).
25.
Eom C-S, Lee H-K, Ye S, Park SM, Cho K-H. Use of selective serotonin-reuptake inhibitors and risk of fracture: a systematic review and meta-analysis. J. Bone Miner. Res. 27(5), 1186–1195 (2012).
26.
Howe TE, Shea B, Dawson LJ et al. Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane Database Syst. Rev. Cd000333 (2011).
27.
Weaver CM, Alexander DD, Boushey CJ et al. Calcium plus vitamin D supplementation and risk of fractures: an updated meta-analysis from the National Osteoporosis Foundation. Osteoporosis Int. 27(1), 367–376 (2016).
28.
Kanis JA, Johnell O, Oden A, Johansson H, Mccloskey E. FRAX and the assessment of fracture probability in men and women from the UK. Osteoporosis Int. 19(4), 385–397 (2008).
29.
Vestergaard P, Rejnmark L, Mosekilde L. Selective serotonin-reuptake inhibitors and other antidepressants and risk of fracture. Calcif. Tissue Int. 82(2), 92–101 (2008).
30.
Law MR, Hackshaw AK. A meta-analysis of cigarette smoking, bone mineral density and risk of hip fracture: recognition of a major effect. BMJ 315(7112), 841–846 (1997).
31.
Berg KM, Kunins HV, Jackson JL et al. Association between alcohol consumption and both osteoporotic fracture and bone density. Am. J. Med. 121(5), 406–418 (2008).
32.
Chastin SF, Mandrichenko O, Helbostadt J, Skelton DA. Associations between objectively-measured sedentary behavior and physical activity with bone mineral density in adults and older adults, the NHANES study. Bone 64, 254–262 (2014).
33.
Tremblay MS, Colley RC, Saunders TJ, Healy GN, Owen N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 35(6), 725–740 (2010).
34.
Boden JM, Fergusson DM. Alcohol and depression. Addiction 106(5), 906–914 (2011).
35.
Roshanaei-Moghaddam B, Katon WJ, Russo J. The longitudinal effects of depression on physical activity. Gen. Hosp. Psychiatry 31(4), 306–315 (2009).
36.
Jakupcak M, Tull MT, Mcdermott MJ, Kaysen D, Hunt S, Simpson T. PTSD symptom clusters in relationship to alcohol misuse among Iraq and Afghanistan war veterans seeking postdeployment VA healthcare. Addict. Behav. 35(9), 840–843 (2010).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 21 August 2018
Accepted: 14 January 2019
Published online: 11 March 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact of selective serotonin reuptake inhibitors in the veteran population: 10-year risk outcomes. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0085
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Wenbin Tan, Ting He, Jia Li, Research progress of drug-induced osteoporosis, Osteoporosis International, 10.1007/s00198-026-07941-7, (2026).
- Mengjia Guo, Silu Tao, Yi Xiong, Meijun Dong, Zhangrong Yan, Zixiang Ye, Dongmei Wu, Comparative analysis of psychiatric medications and their association with falls and fractures: A systematic review and network meta-analysis, Psychiatry Research, 10.1016/j.psychres.2024.115974, 338, (115974), (2024).
- Sara J. Sidles, Ryan R. Kelly, Kirsten D. Kelly, Jessica D. Hathaway-Schrader, Stephanie K. Khoo, Jeffrey A. Jones, James J. Cray, Amanda C. LaRue, Inescapable foot shock induces a PTSD-like phenotype and negatively impacts adult murine bone, Disease Models & Mechanisms, 10.1242/dmm.050044, 17, 1, (2024).
- Mark A. Boyce, Emily L. Durham, Sharon Kuo, Jane M. Taylor, Rajiv Kishinchand, Amanda C. LaRue, James J. Cray, In utero exposure to selective serotonin re‐uptake inhibitor affects murine mandibular development, Orthodontics & Craniofacial Research, 10.1111/ocr.12624, 26, 3, (415-424), (2022).
- Zhen Zhang, Zhichao Hao, Caihong Xian, Yifen Fang, Bin Cheng, Jun Wu, Juan Xia, Neuro-bone tissue engineering: Multiple potential translational strategies between nerve and bone, Acta Biomaterialia, 10.1016/j.actbio.2022.09.023, 153, (1-12), (2022).
- I.G. Litovka, INFLUENCE OF SEROTONIN ON THE METABOLISM OF BONE TISSUE, Fiziolohichnyĭ zhurnal, 10.15407/fz68.05.079, 68, 5, (79-88), (2022).
- Renato de Filippis, Michele Mercurio, Giovanna Spina, Pasquale De Fazio, Cristina Segura-Garcia, Filippo Familiari, Giorgio Gasparini, Olimpio Galasso, Antidepressants and Vertebral and Hip Risk Fracture: An Updated Systematic Review and Meta-Analysis, Healthcare, 10.3390/healthcare10050803, 10, 5, (803), (2022).
- Ryan R. Kelly, Sara J. Sidles, Amanda C. LaRue, Effects of Neurological Disorders on Bone Health, Frontiers in Psychology, 10.3389/fpsyg.2020.612366, 11, (2020).
- Yuko Fujita, Kenji Hashimoto, Decreased bone mineral density in ovariectomized mice is ameliorated after subsequent repeated intermittent administration of ( R )‐ketamine, but not ( S )‐ketamine , Neuropsychopharmacology Reports, 10.1002/npr2.12132, 40, 4, (401-406), (2020).
- Emily Durham, Yuhua Zhang, Amanda LaRue, Amy Bradshaw, James Cray, Selective serotonin reuptake inhibitors (SSRI) affect murine bone lineage cells, Life Sciences, 10.1016/j.lfs.2020.117827, 255, (117827), (2020).