Comparison between oral and intravenous application of tranexamic acid for total hip arthroplasty: a meta-analysis
Abstract
Aim: We conducted a meta-analysis to compare the efficacy and safety of oral and intravenous applications of tranexamic acid (TXA) in total hip arthroplasty (THA). Materials & methods: Electronic databases, including PubMed, Cochrane CENTRAL, ScienceDirect and Embase, were searched to identify the studies comparing the efficacy and safety of oral and intravenous applications of TXA in THA. Relevant journals and conference proceedings were manually searched. The pooled data were analyzed using RevMan 5.1. Results: Four randomized control trials and one retrospective study were identified. A meta-analysis showed no significant differences in hemoglobin reduction, total blood loss and transfusion requirements. Conclusion: Oral applications of TXA are comparable to intravenous applications of TXA in primary unilateral THA for blood conservation and cost-saving measures.
Total hip arthroplasty (THA) is an effective surgical procedure for the treatment of terminal stage diseases of the hip joint, such as osteoarthritis, femoral head necrosis and hip fractures [1]. However, significant blood loss in THA (700–2000 ml, as has been previously reported) is a substantial problem, especially for elderly patients. Subsequent blood transfusions may lead to several complications, such as infection and allergic reaction, which can lead to increasing medical costs [2].
Tranexamic acid (TXA) is a synthetic derivative of the amino acid lysine. It can inhibit fibrinolysis by blocking the lysine binding sites on plasminogen. To date, the intravenous administration of TXA in THA has been well established in the literature [3]. Recently, the oral administration of TXA was reported to be cost-effective in total knee arthroplasty (TKA) and could be a safe alternative to the intravenous or topical forms of TXA [4,5]. A recent published meta-analysis supported this new method of TXA administration in TKA [6]. Recently, several published studies have reported on the oral application of TXA in THA [7–9]. However, their results are not consistent. Moreover, some limitations exist in these previous studies, such as small sample sizes, inconclusive results and inaccurate evaluations. Therefore, we conducted a meta-analysis on the pooled results of randomized controlled trials (RCTs) and non-RCTs, in order to compare the efficacy and safety of oral administrations of TXA in patients undergoing THA.
Materials & methods
Literature & search strategy
Electronic databases, including PubMed, Cochrane CENTRAL, ScienceDirect and Embase, were searched, in order to identify the studies comparing oral or intravenous TXA administrations on blood conservation in unilateral primary THA; the databases were searched with a range from the origination of the electronic databases to July 2018. Structured search strategies were used in combination, according to Boolean logic: ‘tranexamic acid or TXA,’ ‘hip arthroplasty or replacement,’ ‘oral’ and ‘intravenous’. In addition, a manual search of reference lists was conducted for other trials that could potentially be included. The meta-analysis was based on the acknowledged guidelines of the prioritized reported items for systematic review and meta-analysis.
Inclusion criteria
Articles were included in the further meta-analysis when they met the following criteria: the patients were treated with THA; the intervention used oral versus intravenous applications of TXA; the outcomes included blood loss, blood transfusions, hemoglobin reductions, transfusion rates, hospitalizations, complications and medical costs; and the study was a published comparative trial (RCTs or non-RCTs).
Exclusive criteria
We excluded articles that were: repeat published articles or articles having the same content and result; case report, theoretical research, conference report, systematic review, meta-analysis, expert comment and economic analysis; the outcomes were not relevant.
Data extraction & outcome measures
Two of the reviewers independently reviewed and extracted information from the identified studies by including the first author name, the publication year, the sample size, the study design and outcomes. The main outcomes were a decrease in hemoglobin, blood loss and transfusion requirements. Postoperative thromboembolic events and lengths of hospitalization were secondary outcomes to be reported.
Quality assessment
The methodological index for nonrandomized studies was used to evaluate the quality of the nonrandomized studies. The quality assessment of the randomized trial was conducted by using the Cochrane Collaboration. The literature quality was evaluated separately by two reviewers. If there was a divergence, a consensus was reached via consultation.
Data analysis & statistical methods
The RevMan 5.1 (The Cochrane Collaboration, Oxford, UK) was used for the analysis of the pooled data. Heterogeneity was estimated by the p-value and I2, based on the standard χ2 test. If there was significant heterogeneity (I2 > 50%, p < 0.1), a random-effects model was used for the data analysis. When no significant heterogeneity was found (I2 < 50%, p > 0.1), a fixed-effects model was used for the data analysis. In cases of significant heterogeneity, a subgroup analysis was performed, in order to investigate the sources. The mean differences (MDs) and 95% CIs were determined for the continuous outcomes. The dichotomous data were calculated by the use of the odds ratio (OR) and the 95% CIs.
Results
Search results
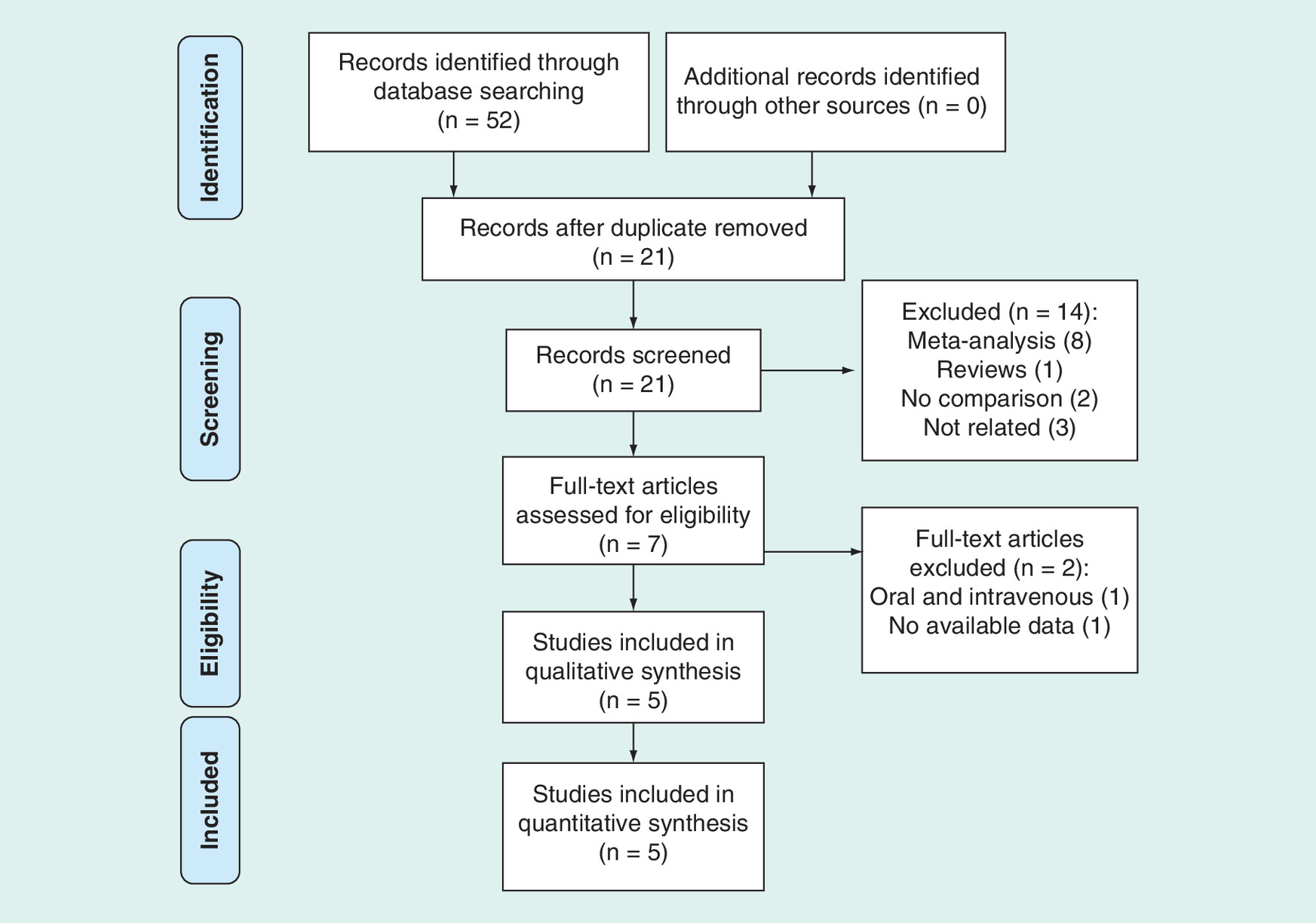
The searching process is illustrated in Figure 1; the original database search yielded 52 records, of which 45 trials were excluded by their titles and abstracts. In a study by Irwin et al. [7], data were reported together from TKA and THA, and no available data were able to be used for further meta-analysis. Another study compared oral versus intravenous administrations of TXA; however, intravenous TXA was offered to all of the patients before the incisions, even though TXA was postoperatively applied either orally or intravenously [10]. Both of these studies were excluded. Finally, a total of five articles were included in the current study, among which four of the studies were randomized trials [9,11–13] and one was a retrospective study by Gortemoller et al. [14].
Study characteristics
The demographic characteristics and details concerning the included studies are summarized in Table 1. The study by Gortemoller et al. included both THA and TKA patients, and we only pooled the data of patients who received THA [14]. All of these studies that were included in the meta-analysis were published in the past 2 years and included 229 patients who were treated by oral TXA and 222 patients who were treated by intravenous TXA. The smallest sample size was 29, whereas the largest sample size was 60. All of the patients received a unilateral primary THA for hip osteoarthritis or femoral head necrosis. No drains were used, and the total blood loss was calculated based on the method that was presented in the previous study [15]. Different TXA protocols were applied in the four studies. Oral TXA administration of 2 g for 2 h prior to the incision was used in three of the studies, whereas an administration of 20 mg/kg at 2 h before and 3 h after THA was used in the study by Zhao et al. [12]. For the intravenous TXA administration, 1 g of TXA administered immediately prior to the incision was applied in two of the studies, and 20 mg/kg of TXA administered prior to the incision was applied in the study by Luo et al. [11]; alternatively, 15 mg/kg of TXA administered 10 min before and 3 h after THA was applied in the study by Zhao et al. [12]. Furthermore, one dose of 1 g TXA before the incision and two times after the operation was adopted by Wu et al. [13].
| Study (year) | Type | Country | Oral TXA group/intravenous group | Approach | TXA protocol | |||
|---|---|---|---|---|---|---|---|---|
| Patients | Females | Ages (year) | Oral | Intravenous | ||||
| Gortemoller et al. (2018) | Retrospective | USA | 39/29 | NM | NM | NM | 1950 mg† | 1000 mg‡ |
| Kayupav et al. (2017) | RCT | USA | 40/43 | 20/21 | 60 ± 10/55 ± 12 | Posterior | 1950 mg† | 1000 mg‡ |
| Luo et al. (2018) | RCT | China | 60/60 | 32/33 | 67.6 ± 10.4/67 ± 8.6 | Posterolateral | 2000 mg† | 20 mg/kg‡ |
| Wu et al. (2018) | RCT | China | 50/50 | 29/30 | 66.5/65.1 | Posterolateral | 1000 mg§ | 1000 mg¶ |
| Zhao et al. (2018) | RCT | China | 40/40 | 18/17 | 60.5 ± 10.4/60.5 ± 10.4 | Direct anterior | 20 mg/kg†† | 15 mg/kg‡‡ |
†2 h prior to incision.
‡Immediately prior to incision.
§2 h before and 3 and 6 h after THA.
¶10 min before and 3 and 6 h after THA.
††2 h before and 3 h after THA.
‡‡10 min before and 3 h after THA.
NM: Not mentioned; RCT: Randomized controlled trial; THA: Total hip arthroplasty; TXA: Tranexamic acid.
Methodological quality assessment
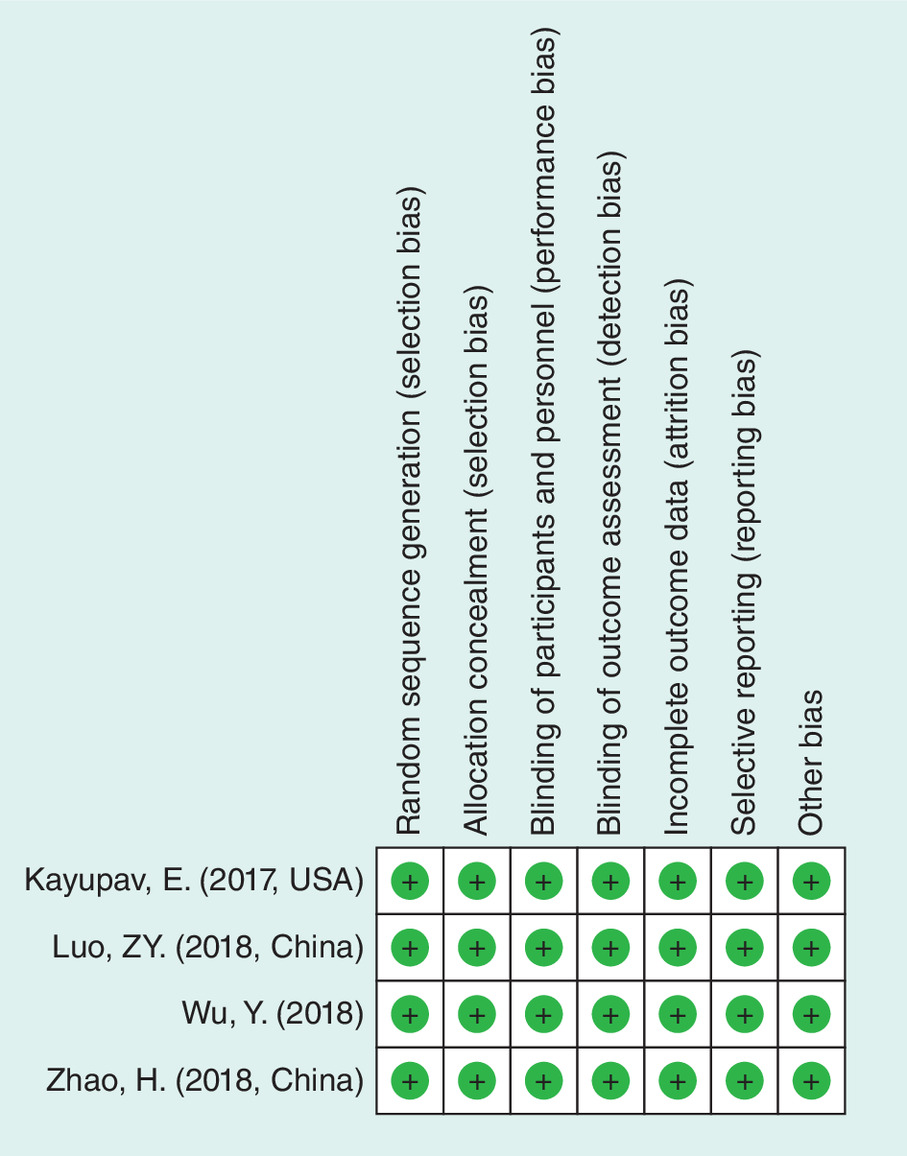
The methodological quality score of the retrospective study was 18, based on the methodological index for nonrandomized studies score (Table 2). The data from this study were not prospectively collected, and the patients of the oral TXA group were measured from January 2015 to August 2015, whereas the patients of the intravenous group were measured from the same time period of 2016. The other four randomized trials were well designed and conducted (Figure 2).
| Quality assessment for nonrandomized trials | Gortemoller |
|---|---|
| A clearly stated aim | 2 |
| Inclusion of consecutive patients | 2 |
| Prospective data collection | 0 |
| End points appropriate to the aim of the study | 2 |
| Unbiased assessment of the study end point | 2 |
| A follow-up period appropriate to the aims of study | 2 |
| Less than 5% loss to follow-up | 2 |
| Prospective calculation of the sample size | 2 |
| An adequate control group | 2 |
| Contemporary groups | 0 |
| Baseline equivalence of groups | 2 |
| Adequate statistical analyses | 2 |
| Total score | 18 |
Outcomes of meta-analysis
The hemoglobin levels were tested in all of the studies, and hemoglobin reductions were not significantly different between the two groups (I2 = 0, p = 0.59; MD = -0.06, 95% CI: -0.22–0.10, p = 0.45; Figure 3). Total blood loss and transfusion rates were reported in the three randomized trails. No additional blood loss was reported from the drain. Total blood loss was similar in both of the groups, according to the modification of the Gross formula (I2 = 0, p = 0.92; MD = -6.33, 95% CI: -55.81–43.14, p = 0.80; Figure 4). Hemoglobin levels that were less than 7 g/dl without significant clinical symptoms or higher hemoglobin levels with cardiac problems or symptoms were set as transfusion criteria. Six patients in the oral TXA group and five patients in the intravenous TXA group needed transfusions for total arthroplasty without separate hip replacements in the study by Gortemoller et al. [14]. Based on the number of patients from the four RCTs, the transfusion rates were calculated, and the pooled data showed similar transfusion rates in both of the groups (I2 = 0%, p = 0.61; OR = 0.91, 95% CI: 0.36–2.29, p = 0.84; Figure 5).
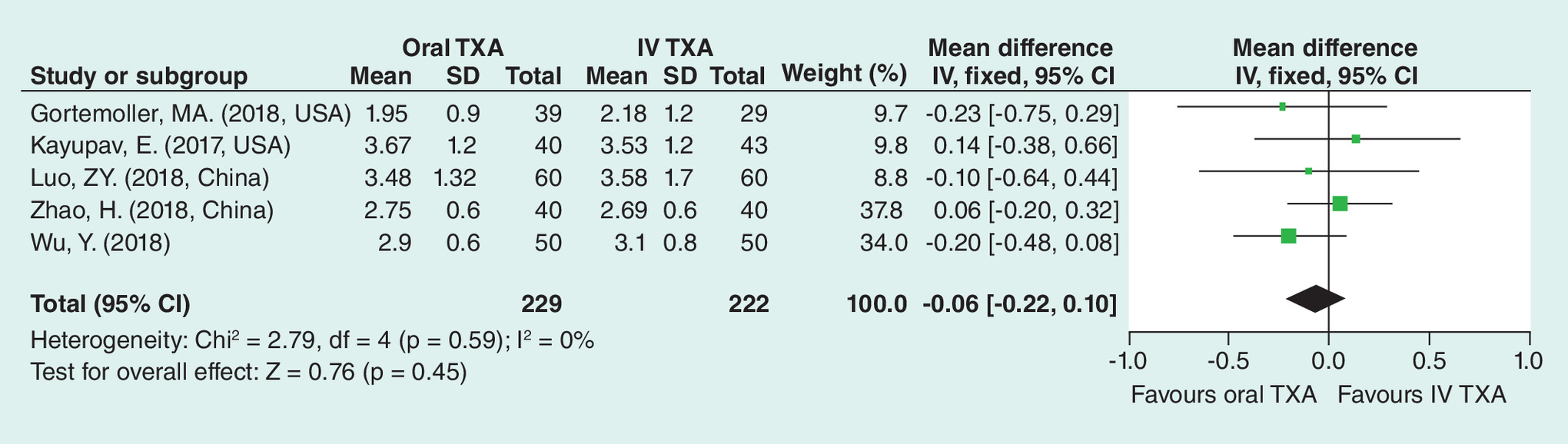
Figure 3. Forest plot showing hemoglobin reduction.
SD: Standard deviation; TXA: Tranexamic acid.
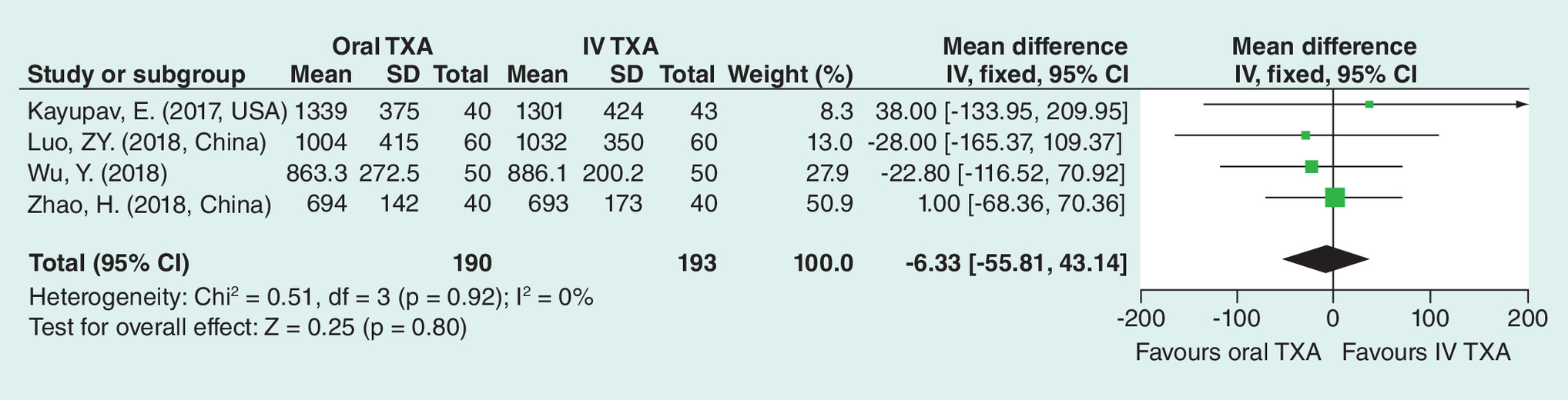
Figure 4. Forest plot showing total blood loss.
SD: Standard deviation; TXA: Tranexamic acid.
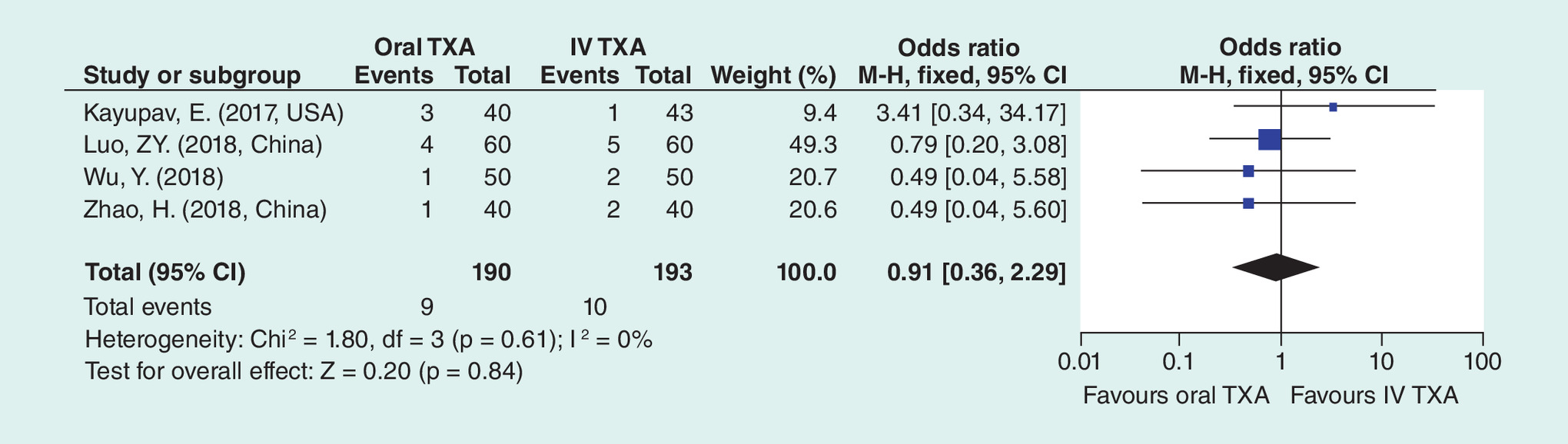
Figure 5. Forest plot showing transfusion requirements.
SD: Standard deviation; TXA: Tranexamic acid.
Four randomized studies reported the time that patients spent in the hospital. No significant differences were observed. Intramuscular venous thrombosis was reported in the study by Zhao et al. [12], including three patients in the oral TXA group and four patients in the intravenous TXA group. Three patients in the oral TXA group and five patients in the intravenous TXA group, in the study by Wu et al., suffered calf muscular vein thrombosis [13]. The pooled data showed no significant difference between the groups (I2 = 64%, p = 0.1; OR = 0.02, 95% CI: -0.10–0.14, p = 0.73). No deep venous thrombosis or pulmonary embolisms were noticed in any of the four studies. One wound problem was also reported by Luo et al. [11]. One venous thromboembolism was reported in the oral TXA group, without a clear explanation, from knee or hip replacement by Gortemoller et al. [14].
Discussion
The intravenous application of TXA has been confirmed as effectively decreasing blood loss and transfusion rates in THA patients. The oral application of TXA has a similar mechanism of action to the intravenous application of TXA, and several studies have assessed the efficacy of the oral application of TXA in THA. However, it is controversial as to whether the oral application of TXA is effective in blood conservation in THA. To our knowledge, the present study is the first quantitative meta-analysis to compare the efficacy and safety of oral TXA administration with intravenous TXA administration in patients undergoing THA. The present meta-analysis showed that an oral application of TXA is comparable to an intravenous application of TXA in primary unilateral THA for blood conservation and cost-saving measures.
Studies have shown that the total calculated blood loss ranged from 1000 to 2000 ml in primary THA [16]. The use of pharmaceutical interventions in THA is a common strategy that is attractive to surgeons. The effectiveness of TXA for decreasing perioperative blood loss during THA has been widely reported [8,17]. The pooled results indicated that the total blood loss and hemoglobin reductions in the oral TXA group were similar to those in the intravenous TXA group.
Previous studies have shown that 10–38% of patients need transfusions to correct anemia. There is a risk of transfusion-associated complications, such as inductions of infectious diseases, hemolysis and anaphylactic reactions, as well as the fact that blood transfusions may also increase the economic burden [18]. The indications for blood transfusions were based on the postoperative hemoglobin levels and the clinical symptoms of anemia. Although the triggers for the transfusions varied among the included studies, the present meta-analysis showed that the blood transfusion rates exhibited no significant difference between the oral and intravenous TXA groups.
TXA dose was a major factor in affecting the therapeutic effects. For oral TXA administration, a single dose of 2 g TXA was applied at 2 h prior to the incision in three studies. Zhao et al. applied 20 mg/kg TXA at 2 h before and 3 h after THA. Given that the average bodyweight of the patients was 60 kg, the dose of TXA was 2.4 g, which was a bit higher than that in the other three studies. For the intravenous administration of TXA, 1 g was used in two studies, 20 mg/kg was used in the study by Luo [11] and two doses of 15 mg/kg were used in Zhao's study [12], in which the dose was equal to or more than 1 g. The doses of TXA were relatively similar with little difference, which was another important factor that contributed to lower heterogeneity. A bolus dose of 2 g that was orally administered at 2h preoperative THA was an effective method in controlling blood loss.
Previous studies have indicated that the oral application of TXA was associated with lower mean total direct hospital costs after primary THA. However, only a limited amount of data could be extracted for the meta-analysis. Kayupov et al. reported that the oral TXA dosage cost $14 per dose, compared with $47–108 per intravenous dose of TXA [9]. Luo et al. reported a lower cost of TXA in the oral group than in the intravenous TXA group ($70.56 vs $489.40) [11]. In another study by Zhao et al., the total cost was 546 RMB for the patients in the oral TXA group versus a total cost of 4573.2 RMB for the patients in the intravenous TXA group. Oral TXA administration is more economical than intravenous TXA administration and has a similar efficacy. Therefore, there is an advantage for patients undergoing THA in using an oral application of TXA. This was further confirmed in the study by Cao et al., in which four boluses of 2 g of oral TXA were preoperatively used at 2 h and were postoperatively used at 4, 10 and 16 h [19].
Several potential limitations should be noted: only four studies were included, with all of the studies having a relatively small sample size; methodological weaknesses existed in the studies, and some of the outcome parameters were not fully described, which led to these studies not being included in the meta-analysis; and a subgroup analysis was not performed because of the limited number of included studies, and we could not determine the source of the heterogeneity.
Conclusion
The oral application of TXA is comparable to the intravenous application of TXA in primary unilateral THA for blood conservation and cost-saving measures.
Total hip arthroplasty (THA) is an effective surgical procedure to treat terminal stage diseases of the hip. However, THA is associated with significant blood loss.
Intravenous administration of tranexamic acid (TXA) in THA has been well established in the literature.
Recently, several published studies have reported on the oral application of TXA in THA.
A meta-analysis was conducted to compare the efficacy and safety of oral administrations of TXA in patients undergoing THA.
PubMed, Cochrane CENTRAL, ScienceDirect and Embase searches (January 1966 to July 2018) yielded 52 results; five studies were included for review.
Meta-analyses were conducted using fixed-effects or random model that reported odds ratio or mean differences and 95% credible intervals.
There were no significant differences in hemoglobin reduction, total blood loss and transfusion requirements.
Oral applications of TXA are comparable to intravenous applications of TXA in primary unilateral THA for blood conservation and cost-saving measures.
Acknowledgments
We thank the authors of all of the included studies.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
1.
Kurtz SM, Ong KL, Lau E, Bozic KJ. Impact of the economic downturn on total joint replacement demand in the United States: updated projections to 2021. J. Bone Joint Surg. Am. 96(8), 624–630 (2014).
2.
Kim JL, Park JH, Han SB, Cho IY, Jang KM. Allogeneic blood transfusion is a significant risk factor for surgical-site infection following total hip and knee arthroplasty: a meta-analysis. J. Arthroplasty 32(1), 320–325 (2017).
3.
Ho KM, Ismail H. Use of intravenous tranexamic acid to reduce allogeneic blood transfusion in total hip and knee arthroplasty: a meta-analysis. Anaesth. Intensive Care 31(5), 529–537 (2003).
4.
Yuan X, Li B, Wang Q, Zhang X. Comparison of 3 routes of administration of tranexamic acid on primary unilateral total knee arthroplasty: a prospective, randomized, controlled study. J. Arthroplasty 32(9), 2738–2743 (2017).
5.
Lee QJ, Ching WY, Wong YC. Blood sparing efficacy of oral tranexamic acid in primary total knee arthroplasty: a randomized controlled trial. Knee Surg. Relat. Res. 29(1), 57–62 (2017).
6.
Zhang LK, Ma JX, Kuang MJ et al. The efficacy of tranexamic acid using oral administration in total knee arthroplasty: a systematic review and meta-analysis. J. Orthop. Surg. Res. 12(1), 159 (2017).
7.
Irwin A, Khan SK, Jameson SS, Tate RC, Copeland C, Reed MR. Oral versus intravenous tranexamic acid in enhanced-recovery primary total hip and knee replacement: results of 3000 procedures. Bone Joint J. 95-B(11), 1556–1561 (2013).
8.
Lee QJ, Chang WY, Wong YC. Blood-sparing efficacy of oral tranexamic acid in primary total hip arthroplasty. J. Arthroplasty 32(1), 139–142 (2017).
9.
Kayupov E, Fillingham YA, Okroj K et al. Oral and intravenous tranexamic acid are equivalent at reducing blood loss following total hip arthroplasty: a randomized controlled trial. J. Bone Joint Surg. Am. 99(5), 373–378 (2017).
10.
Cao G, Huang Z, Xie J et al. The effect of oral versus intravenous tranexamic acid in reducing blood loss after primary total hip arthroplasty: a randomized clinical trial. Thromb. Res. 164, 48–53 (2018).
11.
Luo ZY, Wang HY, Wang D, Zhou K, Pei FX, Zhou ZK. Oral vs intravenous vs topical tranexamic acid in primary hip arthroplasty: a prospective, randomized, double-blind, controlled study. J. Arthroplasty 33(3), 786–793 (2018).
12.
Zhao H, Xiang M, Xia Y, Shi X, Pei FX, Kang P. Efficacy of oral tranexamic acid on blood loss in primary total hip arthroplasty using a direct anterior approach: a prospective randomized controlled trial. Int. Orthop. 42(11), 2535–2542 (2018).
13.
Wu Y, Zeng Y, Hu Q et al. Blood loss and cost–effectiveness of oral vs intravenous tranexamic acid in primary total hip arthroplasty: a randomized clinical trial. Thromb. Res. 171, 143–148 (2018).
14.
Gortemoller MA, Allen B, Forsyth R, Theiss K, Cunningham K, Tucker C. Comparison of oral and intravenous tranexamic acid for prevention of perioperative blood loss in total knee and total hip arthroplasty. Ann. Pharmacother. 52(3), 246–250 (2018).
15.
Gross JB. Estimating allowable blood loss: corrected for dilution. Anesthesiology 58(3), 277–280 (1983).
16.
Toy PT, Kaplan EB, McVay PA, Lee SJ, Strauss RG, Stehling LC. Blood loss and replacement in total hip arthroplasty: a multicenter study. The Preoperative Autologous Blood Donation Study Group. Transfusion 32(1), 63–67 (1992).
17.
Li GL, Li YM. Oral tranexamic acid can reduce blood loss after total knee and hip arthroplasty: a meta-analysis. Int. J. Surg. 46, 27–36 (2017).
18.
Jans O, Kehlet H, Hussain Z, Johansson PI. Transfusion practice in hip arthroplasty – a nationwide study. Vox Sang. 100(4), 374–380 (2011).
19.
Cao G, Huang Q, Huang Z et al. The efficacy and safety of multiple-dose oral tranexamic acid on blood loss following total hip arthroplasty: a randomized controlled trial. Int. Orthop. (2018) (Epub ahead of print).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 29 October 2018
Accepted: 14 January 2019
Published online: 12 March 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparison between oral and intravenous application of tranexamic acid for total hip arthroplasty: a meta-analysis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0120
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Mohamed Aziz Daghmouri, Frederic Salmeron, Abdallah Amine Lahdheri, Adriano Carneira Da Costa, Mohamed Ali Chaouch, Efficacy and Safety of Oral versus Intravenous Administration of Tranexamic Acid in Elective Total Hip Arthroplasty: A Systematic Review and Meta-Analyses of Randomized Controlled Trials, The Journal of Arthroplasty, 10.1016/j.arth.2025.04.042, 41, 1, (265-273.e1), (2026).
- Sibylle Kietaibl, Aamer Ahmed, Arash Afshari, Pierre Albaladejo, Cesar Aldecoa, Giedrius Barauskas, Edoardo De Robertis, David Faraoni, Daniela C. Filipescu, Dietmar Fries, Anne Godier, Thorsten Haas, Matthias Jacob, Marcus D. Lancé, Juan V. Llau, Jens Meier, Zsolt Molnar, Lidia Mora, Niels Rahe-Meyer, Charles M. Samama, Ecaterina Scarlatescu, Christoph Schlimp, Anne J. Wikkelsø, Kai Zacharowski, Management of severe peri-operative bleeding: Guidelines from the European Society of Anaesthesiology and Intensive Care, European Journal of Anaesthesiology, 10.1097/EJA.0000000000001803, 40, 4, (226-304), (2023).
- Rodolfo Morales-Avalos, Tomas Ramos-Morales, Jesús A. García-Pedro, Ana M. Espinoza-Galindo, Carlos Acosta-Olivo, Michelle Morcos-Sandino, Héctor N.G. Silva-Ramos, Víctor M. Peña-Martínez, Raymundo A. Rodríguez-Torres, Félix Vilchez-Cavazos, Tranexamic acid versus aminocapróic acid in multiple doses via the oral route for the reduction of postoperative bleeding in total primary hip arthroplasty: a prospective, randomized, double-blind, controlled study, Blood Coagulation & Fibrinolysis, 10.1097/MBC.0000000000001005, 32, 2, (132-139), (2021).
- Xingming Xu, Jiang Jiang, Wei Liu, Xiaofeng Li, Huading Lu, Application of thromboelastography to evaluate the effect of different routes administration of tranexamic acid on coagulation function in total hip arthroplasty, Journal of Orthopaedic Surgery and Research, 10.1186/s13018-019-1497-y, 14, 1, (2019).