Importance of assessing and adjusting for cross-study heterogeneity in network meta-analysis: a case study of psoriasis
Abstract
Aim: The importance of adjusting for cross-study heterogeneity when conducting network meta-analyses (NMAs) was demonstrated using a case study of biologic therapies for moderate-to-severe plaque psoriasis. Methods: Bayesian NMAs were conducted for Psoriasis Area and Severity Index 90 response. Several covariates were considered to account for cross-trial differences: baseline risk (i.e., placebo response), prior biologic use, body weight, psoriasis duration, age, race and baseline Psoriasis Area and Severity Index score. Model fit was evaluated. Results: The baseline risk-adjusted NMA, which adjusts for multiple observed and unobserved effect modifiers, was associated with the best model fit. Lack of adjustment for cross-trial differences led to different clinical interpretations of findings. Conclusion: Failure to adjust for cross-trial differences in NMA can have important implications for clinical interpretations when studying the comparative efficacy of healthcare interventions.
A network meta-analysis (NMA) can be conducted to compare multiple treatments that may not have been compared directly in head-to-head clinical trials [1,2]. However, when undertaking an NMA, it is vital to assess the degree of heterogeneity between trials regarding patient characteristics and study design so as to determine the suitability of synthesizing the results of multiple trials in a unified analysis [3–5]. The appropriate use of NMAs can lead to enhanced decision-making in situations where head-to-head clinical trials do not exist; however, decision makers need to be aware of the potential challenges that can arise if NMAs are conducted that do not adequately adjust for cross-trial heterogeneity.
The presence of clinical heterogeneity across trials for treatments of interest may undermine the validity of NMAs [4,6,7]. Failure to account for these differences can lead to misleading comparisons of treatment effect [3,5]. For example, in an NMA where the severity of illness varies across studies and treatments, failure to adjust for these differences using meta-regression may result in misleading estimates of treatment effect comparisons between interventions. Past research has demonstrated how adjustments can play an important role in the validity of NMAs. For example, Salanti et al. [5] previously demonstrated in NMA-based comparisons of interventions to prevent dental caries that magnitudes of treatment effect, as well as the rank ordering of treatments, were altered when accounting for differences in clinically relevant covariates, such as baseline mean caries level. In a separate study, Thorlund et al. [8] reviewed methods and findings from a total of 13 published NMAs comparing biologic therapies for rheumatoid arthritis to establish the underlying reasons for discrepancies in their findings, and noted that both failure to analytically adjust for cross-trial differences, as well as inappropriate grouping of different patient sub-populations, were the apparent causes. Therefore, it is important to demonstrate the need for assessing systematic differences in treatment effect modifiers across comparisons when conducting an NMA for healthcare decision makers and researchers.
In this paper, we consider a case study assessing the comparative efficacy of treatments for moderate-to-severe psoriasis. Although a considerable number of systematic reviews have been performed in recent years looking at the effects of interventions for psoriasis, few have considered an NMA approach, and a smaller subset have considered analytic approaches that account for the presence of heterogeneity between studies [9–11]. Among them, inclusion of a comprehensive selection of interventions has been lacking. In the current study, we present graphical and analytic approaches that were used to explore and identify the degree of interstudy clinical heterogeneity present for a series of key clinical variables. We also present the findings from an unadjusted NMA and compare them with an NMA model that accounts for the effects of disparities in clinical covariates. Differences in clinical interpretation of these findings are discussed to highlight the potential implications that may arise when failing to account for important clinical heterogeneity and systematic differences in treatment effect modifiers between studies. We also present findings from an NMA on the risk difference scale, representing an alternative approach to dealing with the presence of variations in baseline risk between studies. In presenting this work, we aim to add to past works that have discussed the importance of investigating and accounting for cross-trial differences in NMA [5,8].
Methods
In the current study, we first present a clinical background for readers to provide an understanding of some of the key symptoms and signs experienced by patients diagnosed with plaque psoriasis, as well as to introduce the currently available biologic therapies for the management of this condition. A brief description of variations in findings from recent reviews that have assessed the benefits and harms of therapies in this area is also provided. Next, the reader is introduced to the methods that were employed in conducting our systematic review of induction therapies, collecting all necessary outcome and study data and pursuing subsequent investigations for cross-study heterogeneity, as well as implement unadjusted and adjusted NMAs. Next, findings from visual and quantitative evaluations of interstudy heterogeneity are presented, followed by a detailed comparison of findings from unadjusted NMA as well as NMAs that account for the presence of heterogeneity. Last, we discuss the importance of adjusting for cross-study heterogeneity in NMA, both generally and in the context of the network considered in this study.
Targeted therapies for moderate-to-severe plaque psoriasis
Psoriasis is a symptomatic, disfiguring and chronic dermatological condition characterized by autoimmune-mediated inflammation of the skin [12,13]. The most common form is plaque-type, which affects approximately 80–90% of patients with psoriasis [14]. Several targeted treatments are currently available for moderate-to-severe plaque psoriasis, with their objective being to achieve a high level of skin clearance. These include biological therapies such as TNF-α inhibitors (adalimumab 40 mg; infliximab 5 mg/kg; etanercept 50 mg twice weekly [BIW], 50 mg once weekly [QW] and 25 mg BIW), IL-17 (ixekizumab 80 mg every 2 weeks [Q2W]; secukinumab 150 and 300 mg) and IL-17 receptor (brodalumab 140 and 210 mg) inhibitors, an IL-12/23 inhibitor (ustekinumab 45, 45/90 and 90 mg) and an IL-23 inhibitor (guselkumab 100 mg), as well as a small molecule PDE4 inhibitor (apremilast). A considerable number of randomized controlled trials (RCTs) involving these therapies have been performed previously. Although an increasing number of head-to-head trials have directly compared active treatments, the majority of studies have involved comparisons against placebo only. The need to employ NMA methods to derive treatment comparisons between active therapies is apparent based upon the presence of multiple interventions of relevance to psoriasis and the need to be able to do comparisons among all of the biologics at the same time.
In recent years, several systematic reviews incorporating NMA methods have been reported [9–11,15–19]. However, the approaches used to account for clinical heterogeneity were different between the studies. Moderate-to-severe plaque psoriasis represents an excellent case study for illustrating the importance of systematically evaluating cross-study differences to identify the need for covariate adjustments in the context of NMA.
Systematic review: NMAs of targeted therapies for moderate-to-severe plaque psoriasis
The case study for this research is based upon a recently conducted systematic review of RCTs that evaluated induction treatment with targeted therapies for moderate-to-severe plaque psoriasis. Rigorous systematic review methodology was followed (see protocol registration in the PROSPERO database for details: CRD42017060190) to identify eligible RCTs, including a rigorous search of Medline, Embase and the Cochrane Register of Controlled Trials performed in February 2017. All details related to the exploration of clinical heterogeneity and the performance of NMAs using both unadjusted and adjusted models were prespecified and used established models recommended by the NICE (additional modeling details are described below) [3,20]. The process of study selection identified a total of 41 unique RCTs [21–58], some of which also had companion reports. Please see the Supplementary Material for more information. The current report is focused on the presentation of findings related to Psoriasis Area and Severity Index (PASI) 90 response, a widely used endpoint across recent RCTs that captures the proportion of patients who achieved ≥ 90% improvement in disease severity from baseline. Analyses were focused upon the induction period of treatment, which corresponds to the time frame for which most trials employ placebo treatment as a control regimen. PASI 90 response has been used as a primary efficacy outcome in recent studies due to its clinical significance and high level of importance to patients [59]. PASI 90 response data were available from 40 of the 41 included trials (n = 23,916 patients). The trial [19] comparing etanercept and biosimilar etanercept (Erelzi®, Sandoz, Holzkirchen, Germany) lacked PASI 90 data and was excluded from the NMA. The associated network diagram summarizing the available evidence base is presented in Figure 1. All treatments were assessed in at least one study that included a placebo group while several head-to-head trials between therapies were also identified.

Figure 1. Network of available randomized controlled trials in moderate-to-severe plaque psoriasis for Psoriasis Area and Severity Index 90 response.
Treatment nodes and edges are sized to proportionately reflect (A) the respective numbers of patients randomized to each treatment and (B) the numbers of studies underlying each comparison.
ADA: Adalimumab; APR: Apremilast; BIW: Twice weekly; BRO: Brodalumab; ENT: Etanercept; GUS: Guselkumab; IFX: Infliximab; IXE: Ixekizumab; PBO: Placebo; QW: Once weekly; Q2W: Every two weeks; SEC: Secukinumab; UST: Ustekinumab.
Methods for unadjusted NMAs
Unadjusted Bayesian random effect (RE) and fixed effect NMAs were first performed using WinBUGS software (version 1.4.3, MRC Biostatistics Unit, Cambridge, UK) in accordance with recommendations and code made available by NICE that adjusts for correlation in multiarm trials [20]. Vague prior distributions for treatment effects (normal with mean 0 and precision 0.0001) in both models were used. Risk ratios (RRs) and corresponding 95% credible intervals (CrIs) were estimated to summarize pairwise comparisons between interventions. Surface Under the Cumulative Ranking (SUCRA) curve and the probability of each intervention being the best treatment (referred to from here onwards as ‘probability best’) were also estimated from the model. The RE model was found to be adequate and have a much-improved fit relative to the fixed effect model for PASI 90 response (based upon inspection of posterior residual deviance and DIC values in the Supplementary Material), and is the focus of all results described in the current report. NMAs were performed using three unique sets of starting values and were based on burn-in and sampling of 50,000 iterations or more. Model convergence was assessed by inspection of Gelman-Rubin plots, trace plots and Monte Carlo standard error of parameter estimates from the Markov Chain Monte Carlo analysis. All NMAs were performed using WinBUGS Software version 1.4.3 (MRC Biostatistics Unit, Cambridge University, UK) and R Software (version 3.3.4, The R Foundation for Statistical Computing).
Evaluating interstudy heterogeneity: variations in baseline risk
A prespecified selection of patient characteristics was assessed to evaluate the extent of clinical heterogeneity between study populations. Careful attention was paid to differences in baseline risk (i.e., placebo group response rates) across studies and interventions, as this measure has been known to reflect potentially important differences in measured and unmeasured confounders across study populations [3]. The bar plot in Figure 2 presents a visualization of these rates, with several evident notable differences between studies. It should be noted that even minor differences in placebo response rates between studies (and treatments in the network) can affect NMA results given that placebo response is a component of the denominator of relative risks and odds ratios (i.e., dividing by a smaller number can inflate relative effects). A similar assessment was performed for the following additional covariates: percentage of patients with prior exposure to biologic therapies, average baseline weight, average age, average duration of disease, average baseline PASI score, race distribution and study-specific duration of the induction period. The corresponding bar plots for these covariates are presented in the Supplementary Material, along with scatterplots assessing the relationship between these covariates. Notably, patients’ prior exposure to biologics, and, to a lesser degree, mean duration of psoriasis and mean weight, were found to have mild-to-moderate associations with placebo response. Past guidance regarding the performance of meta-regression analyses has noted the importance of having sufficient numbers of studies available [60,61]. Given that network meta-regression analyses are limited by the number of studies in a network (and consideration of multiple covariates simultaneously would be underpowered given the evidence structure), a baseline risk (or placebo-adjusted) NMA can serve as a statistically efficient meta-regression approach to adjust for multiple known and unknown cross-trial differences among RCTs. As baseline risk was also found to be the most influential adjustment factor (underlying statistical rationale are documented in subsequent sections below), the remainder of the current report will focus upon findings from this adjusted analysis.
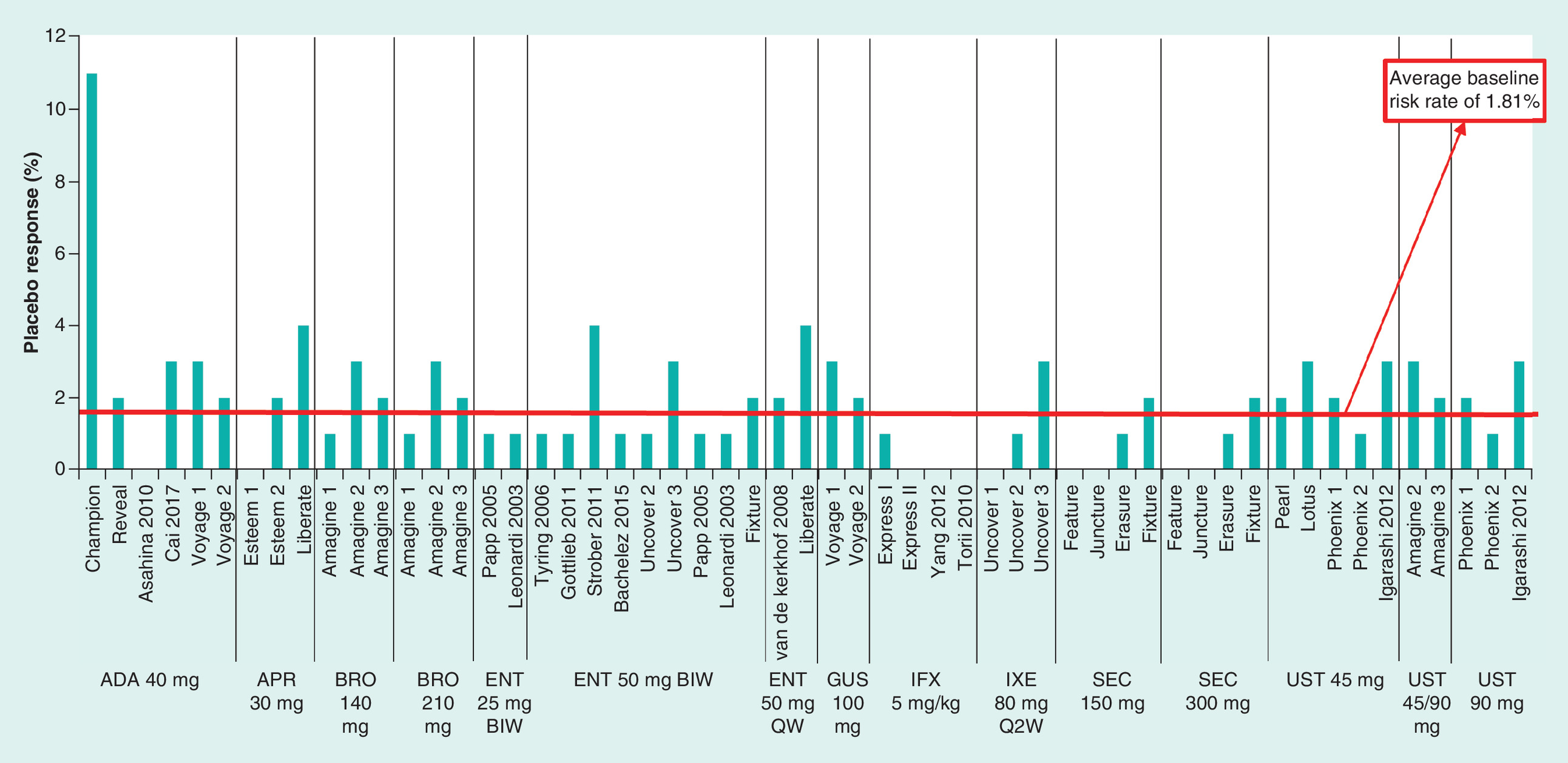
Figure 2. Placebo response rates for Psoriasis Area and Severity Index 90 response at the end of the induction period.
ADA: Adalimumab; APR: Apremilast; BIW: Biweekly; BRO: Brodalumab; ENT: Etanercept; GUS: Guselkumab; IFX: Infliximab; IXE: Ixekizumab; NA: Not applicable (no placebo group); NR: Not reported; QW: Once weekly; Q2W: Every two weeks; SEC: Secukinumab; UST: Ustekinumab.
Several observations regarding differences in placebo group PASI 90 response rates among included studies can be drawn from Figure 2. Relative to the overall average placebo response rate of 1.81%, certain studies of ixekizumab (UNCOVER 1 [25] and UNCOVER 2 [27]), infliximab (EXPRESS 2 [35]), ustekinumab (PHOENIX 2 [39]) and apremilast (ESTEEM 1 [38]) were found to be associated with lower placebo response rates. Conversely, certain studies of guselkumab (VOYAGE 1 [44], VOYAGE 2 [23]), adalimumab (CHAMPION [47]; Cai et al. [58]), etanercept (Strober et al. [48]; van de Kerkhof et al. [54]), ixekizumab (UNCOVER 3 [27]), brodalumab (AMAGINE 2 [32] and AMAGINE 3 [32]), ustekinumab (PHOENIX 1 [33], Igarashi et al. [30], PEARL [52], LOTUS [56]) and apremilast (LIBERATE [45]) were associated with higher than average rates. Figure 3 presents a scatterplot of each trial's estimated PASI 90 treatment effect (on the natural log scale) versus the associated placebo group response rate. The data pattern demonstrates the presence of a negative linear correlation between higher placebo response rates and smaller observed treatment effects. The coloring of individual cells in the league table presented in Figure 4 reflects the extent of statistical heterogeneity present in pairwise meta-analyses (conducted before NMAs, to assess variability amongst components of the network). High heterogeneity (I2) values (defined as ≥ 75%) were observed for meta-analyses of trials involving ixekizumab every 2 weeks (75.20%), while low (0–25%) or moderate (26–75%) I2 values were observed for all other meta-analyses. The I2 values and the related findings from pairwise meta-analyses are provided in the Supplementary Material.
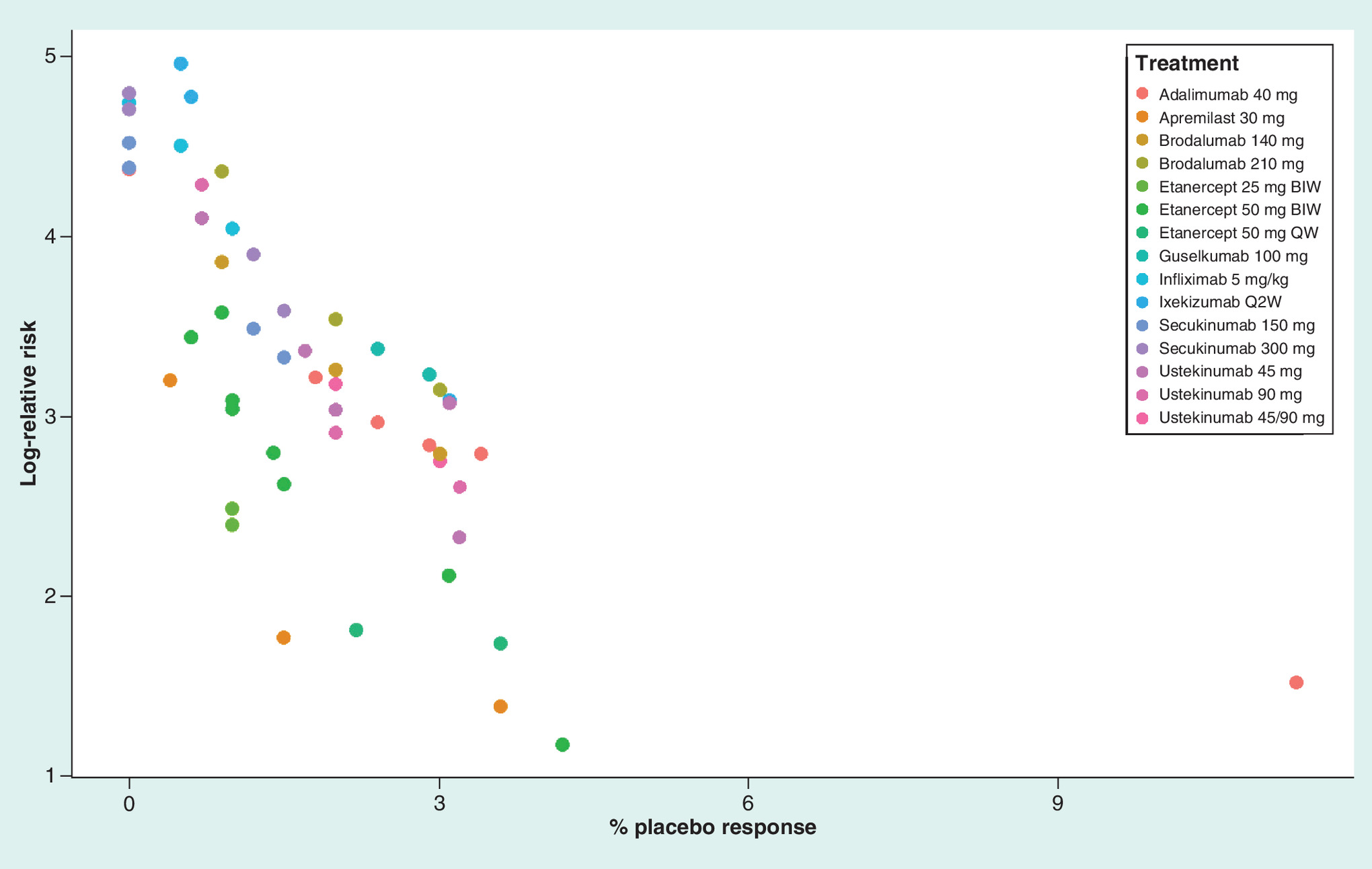
Figure 3. Scatterplot of placebo response rates versus log (risk ratio) for Psoriasis Area and Severity Index 90 response.
A scatterplot of the natural log of each study's treatment effect versus its corresponding placebo response rate. Points are color-coded by intervention. A clear relationship exists between percentage placebo response (i.e., control group risk) and treatment effect.
BIW; Biweekly; QW: Once weekly; Q2W: Every two weeks.

Figure 4. League table of unadjusted risk ratios for Psoriasis Area and Severity Index 90 response.
Results from the unadjusted random effects NMA are presented. Treatments are ordered from upper left to lower right in order of decreasing SUCRA value. The text within each cell presenting a pairwise comparison has been colored so as to reflect the degree of heterogeneity present in a traditional pairwise meta-analysis of the underlying studies (see legend for details). All comparisons wherein the 95% credible interval for the risk ratio excludes the null value of 1 are shown in bolded and underlined font.
BIW: Twice weekly; NMA: Network meta-analysis; Q2W: Every 2 weeks; QW: Once weekly; SUCRA: Surface Under the Cumulative Ranking.
Results
Unadjusted NMA on the risk ratio scale
The league table in Figure 4 summarizes findings from the unadjusted RE NMA. All targeted therapies were associated with an increased likelihood of PASI 90 response relative to placebo (RR range from 7.18 to 47.12). Ixekizumab 80 mg Q2W was associated with the most favorable results among treatments. Summary estimates also indicated the presence of clinically important differences in favour of ixekizumab compared with treatments within the same drug class, such as brodalumab 200 mg (RR: 1.15; 95% CrI: 1.001–1.34) and secukinumab 300 mg (RR: 1.18; 95% CrI: 1.04–1.36), as well as guselkumab 100 mg (RR: 1.29; 95% CrI: 1.07–1.60). However, as shown in Figure 4, ixekizumab 80 mg Q2W was also the treatment with the most statistical heterogeneity among pair-wise meta-analyses.
NMAs adjusting for variation in baseline risk
Box 1 provides context as to the importance of adjusting for differences in placebo rates among clinical trials using a simple indirect comparison within the NMA. As per Box 1, there appears to be heterogeneity within pair-wise meta-analysis estimates that can be partially explained by the presence of low placebo response rates in ixekizumab studies. Based on Box 1, two broader analytic strategies, meta-regression adjustment for placebo response on the relative scale and implementation of a risk difference on the absolute scale, were undertaken to account for differences in placebo responses. Meta-regression requires a sufficient number of studies and variation in covariates across studies.
Ixekizumab was identified as an intervention with high I2 values. Indeed, the I2 resulting from a meta-anlaysis of ixekizumab versus placebo was 75%, which represents substantial heterogeneity. It was also identified as an intervention whose underlying randomized controlled trials RCTs were associated with low placebo response rates compared with those from other studies, particularly the UNCOVER 1 and UNCOVER 2 trials. Two simple Bayesian anchored indirect comparisons between guselkumab and ixekizumab were performed using placebo as the common linking intervention, and using data from the guselkumab RCTs (VOYAGE 1 and VOYAGE 2) and the ixekizumab RCTs (UNCOVER 1, UNCOVER 2 and UNCOVER 3).
Forest plots displaying the outcome data from these trials (along with traditional pairwise meta-analyses thereof) are presented below. League tables summarizing the results of the two indirect comparisons are also presented. The first Bayesian indirect comparison was based on a random effects NMA model and incorporated data from all five studies; the analysis produced summary estimates that were comparable to those from the unadjusted NMA. However, 95% CrIs were wider (risk ratio 1.30; 95% CrI: 0.68–4.16). The second indirect comparison was based upon afixed effect NMA model (due to the presence of few studies per comparison remaining) and included data from only the UNCOVER 3 trial for ixekizumab and the VOYAGE 1 and 2 trials for guselkumab. This selection of studies was based on the identification of notably lower placebo group response rates in the UNCOVER 1 and UNCOVER 2 trials (0.5% and 0.6%, respectively) compared with those observed in the UNCOVER 3, VOYAGE 1 and VOYAGE 2 trials (3.1, 2.9 and 2.4%, respectively).
The objective of excluding studies was to improve the homogeneity and increase the validity of the indirect comparison. The direction of the risk ratio comparing guselkumab and ixekizumab switched, in favor of guselkumab (risk ratio: 1.10; 95% CrI: 0.80–1.61). The change in the direction of the indirect comparison suggests there may be differences among the guselkumab and ixekizumab trials. The different results from the two simple indirect comparisons (including vs excluding the dissimilar UNCOVER trials) provide further support for the importance of adjusting for placebo response in the NMAs Figure 5.
Traditional meta-analyses of ixekizumab versus placebo and guselkumab versus placebo to compare Psoriasis Area and Severity Index 90 response are shown in forest plots along with supporting trial data. Low placebo group response rates are visible for the UNCOVER 1 and UNCOVER 2 trials for ixekizumab while response rates in the treatment groups across trials are similar. A random effect NMA to compare ixekizumab and guselkumab using all five trials favored ixekizumab. A sensitivity analysis using a fixed effect NMA model (to account for the low number of studies per connection in the network) and excluding UNCOVER 1 and UNCOVER 2 due to low placebo-group response rates, favored guselkumab.
CRI: Credible interval; GUS: Guselkumab; IXE: Ixekizumab; NMA: Network meta-analysis ; PBO: Placebo; RCT: Randomized controlled trial.
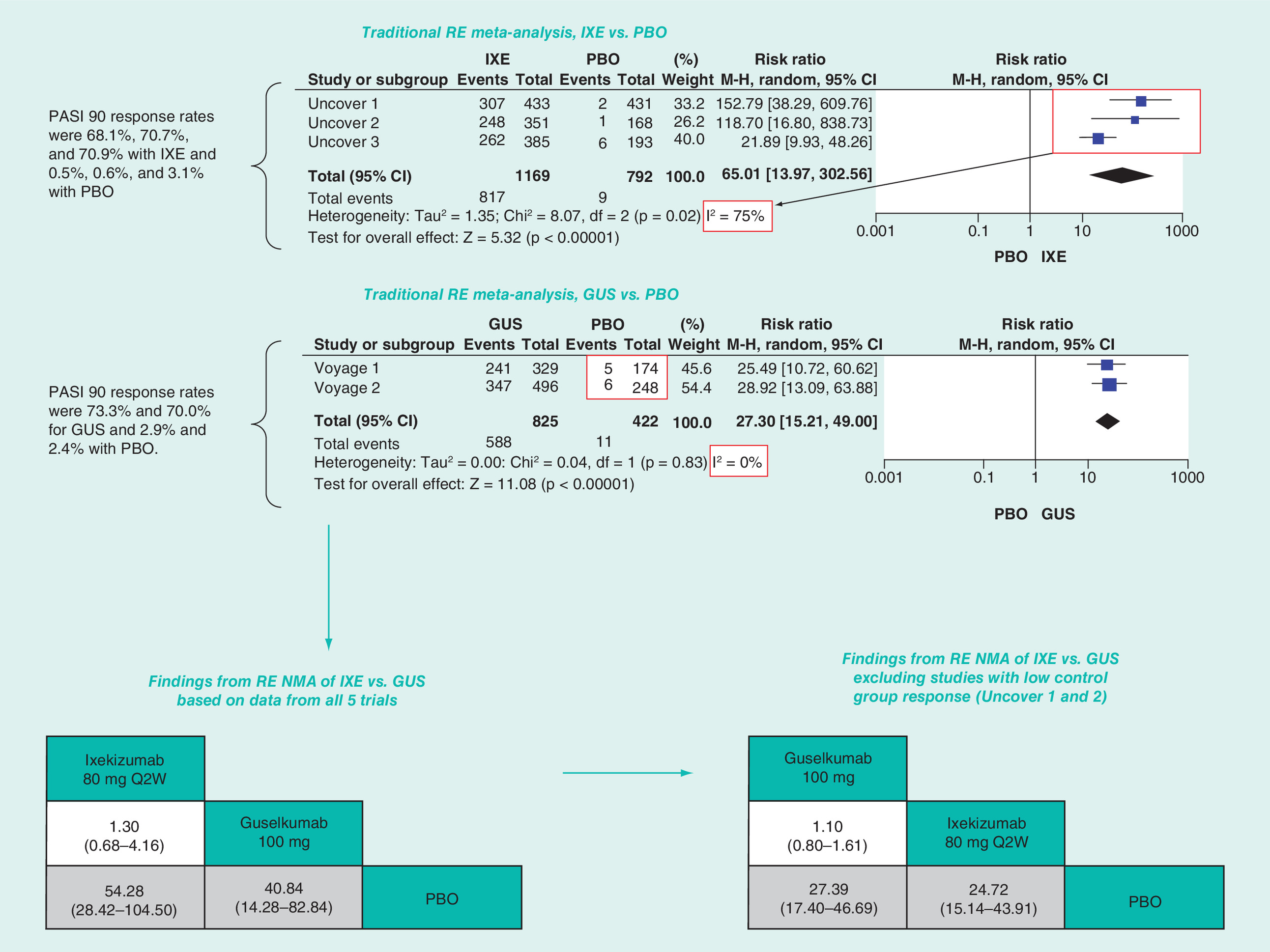
Figure 5. Indirect comparison of guselkumab and ixekizumab for Psoriasis Area and Severity Index 90 response.
GUS: Guselkumab; IXE: Ixekizumab; PBO: Placebo.
NMA meta-regression adjustment for placebo response on a relative scale
A meta-regression adjustment was introduced into the RE NMA using an established extension of the unadjusted model [5] mentioned earlier. In the analysis, a regression coefficient (β) was assigned a vague normal prior distribution with mean 0 and precision 0.0001, assuming a constant coefficient across interventions. Guidance from the NICE Decision Support Unit (DSU) Technical Support Documents (TSDs) [3] was followed to judge whether this model was a better fit than the unadjusted model, and thus more appropriate for establishing clinical interpretations. Specifically, we explored whether the regression coefficient was associated with a statistically significant difference in treatment effect (i.e., a 95% CrI which excluded 0) and whether the summary estimate for the between-study standard deviation (SD) parameter (and its 95% CrI) was reduced. We also assessed the deviance information criterion (DIC) and the posterior residual deviance. However, as noted in NICE DSU TSD 3 [3], the DIC is not a reliable criterion for deciding whether to include a covariate in RE models. Therefore, in accordance with best practice, adequacy of model fit was largely based on whether the regression coefficient was associated with a statistically significant effect on treatment effect (i.e., a 95% CrI which excluded 0), and whether the summary estimate for the between-study SD parameter (and its 95% CrI) was reduced. The WinBUGS code for the baseline risk meta-regression analysis is based on NICE TSD 3, where baseline risk meta-regression takes the ‘true’ baseline (as estimated by the model) as the covariate and takes the uncertainty in each log odds into account.
NMA performed on the risk difference scale
In addition to meta-regression adjustment of effects on the relative scale, use of an NMA on the risk difference scale represents a viable alternative approach to account for the presence of cross-study differences in placebo response rate. Rather than calculating relative effects which include division by varying magnitudes of placebo response rates (which may sometimes inflate relative effects), absolute probabilities of treatment response are subtracted across interventions. In particular, a risk difference NMA could be used as an alternative method when there are imbalances in the number of studies with low placebo response rates across pairwise contrasts in the network. The code for risk differences is also based on code outlined in NICE DSU TSD 2 [20] and Warn et al. [62].
Findings from NMAs adjusting for variation in baseline risk
Figure 6 presents a forest plot diagram of RRs for each treatment versus placebo and the 95% CrI from all three NMA approaches along with all ‘probability guselkumab is better’ values. A corresponding heat map of SUCRA values for all treatments is provided in the Supplementary Material.
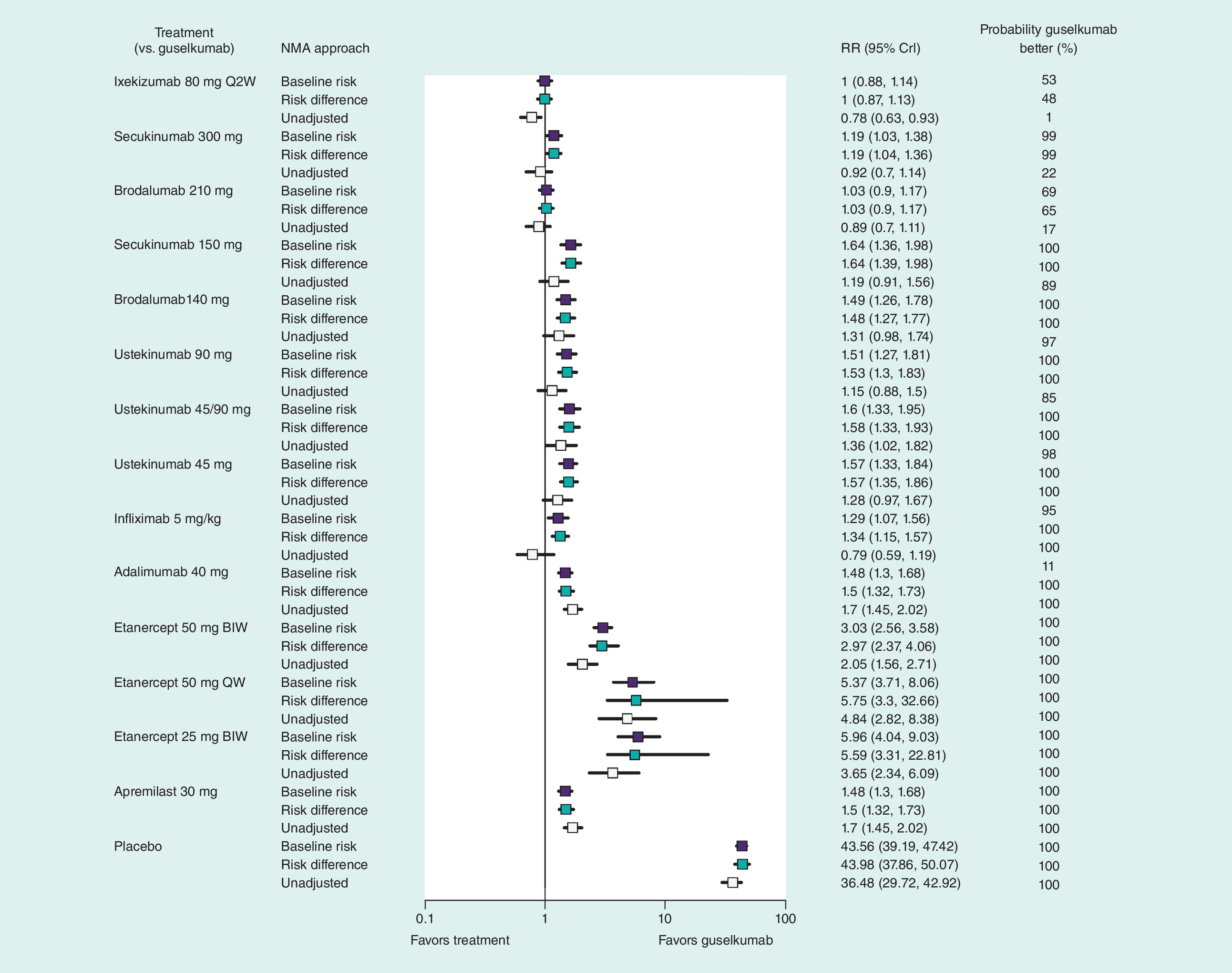
Figure 6. Forest plot of comparisons of guselkumab with other biologics across analytic approaches.
Risk ratios and risk differences estimated from the various RE NMAs are presented showing comparisons of guselkumab with other biologics and the probability of guselkumab being superior to each intervention included in the network. Values are reported with corresponding 95% credible intervals risk ratios and risk differences >0 favor guselkumab.
BIW: Twice weekly; CrI: Credible interval; NMA: Network meta-analysis; Q2W: Every 2 weeks; QW: Once weekly; RE: Random effect; RR: Risk ratio.
The baseline risk-adjusted model was associated with improved fit relative to the unadjusted model; the estimated regression coefficient β was -0.91 (95% CrI: -1.05 to -0.82), and the interstudy SD was reduced in magnitude from 0.12 (95% CrI: 0.01–0.29) to 0.11 (95% CrI: 0.04–0.20). Results from the baseline risk-adjusted NMA were associated with certain noteworthy changes in effect estimates and some important modifications in clinical interpretations. With regard to SUCRA, the ordering of the top five interventions changed compared with the unadjusted analysis, with guselkumab 100 mg (93%) and ixekizumab 80 mg Q2W (93%) ranking highest, followed by brodalumab 210 mg (87%), secukinumab 300 mg (80%) and infliximab 5 mg/kg (73%), with percentages reflecting the probability of being ranked highly (Supplement). Notably, in the baseline risk-adjusted analysis, guselkumab 100 mg was found to offer equivalent benefits compared with ixekizumab 80 mg Q2W (RR: 1.00; 95% CrI: 0.88–1.14); both interventions were found to offer clinically important increases in the likelihood of PASI 90 response compared with all other interventions in the network, with the exception of brodalumab 210 mg. This finding was supported by the ‘probability better’ values for guselkumab 100 mg which were greater than 99% or higher versus all interventions except for ixekizumab 80 mg Q2W (53%) and brodalumab 210 mg (69%) (Figure 6).
The results from the NMA using risk differences as the summary measure aligned closely with those from the baseline risk-adjusted NMA (Figure 6), underscoring the importance of adjusting for cross-trial differences and lending credibility to the approach of selecting the best fitting models when interpreting results on the relative scale. Lack of adjustment for cross-trial differences led to different clinical interpretations of the NMA results and tended to bias in favor of treatments that reported lower placebo response rates.
For completeness, all measures of model fit and related statistical details, as well as complete summaries of pairwise comparisons from all three approaches to analysis, and additional content, are provided in the Supplementary Material.
Discussion
As the annual number of NMAs published continues to rise [63], and the number of systematic reviewers pursuing this type of analysis expands, it is increasingly important to ensure awareness of appropriate approaches for modeling in the presence of interstudy variations [3]. Failure to investigate and, when present, to analytically account for cross-study heterogeneity in patient populations and methods may produce misleading estimates of comparative efficacy. This report seeks to add to past works that have presented focused efforts to address this issue [3,5,8].
The extent of clinical heterogeneity present within our case study suggested the need for a rigorous approach to minimize the bias among comparisons of comparative efficacy. An unadjusted NMA comparing targeted therapies identified ixekizumab 80 mg Q2W as the most efficacious intervention for the achievement of PASI 90 response. In the unadjusted analysis that did not account for cross-trial differences, ixekizumab 80 mg Q2W was associated with a ‘probability best’ value of 100% and corresponding relative risk measures that demonstrated clinically important advantages over almost all comparators. However, inspection of interstudy I2 values, bar charts and scatterplots of clinically important covariates identified important differences between studies, particularly concerning baseline risk (i.e., placebo response). As described earlier, variations in placebo response can serve as a proxy for differences in known and unknown confounders across trials. Small differences in placebo response can bias findings in favor of therapies with lower placebo group response rates. Accordingly, we conducted detailed analyses to adjust for cross-trial differences between studies. Based upon model fit statistics that were established a priori, a baseline risk-adjusted model accounting for differences in placebo group response was identified as having a better fit to the data than the model that did not adjust for cross-trial differences (i.e., the unadjusted NMA). Lack of adjustment for cross-trial differences led to different clinical interpretations of the NMA results and tended to bias in favor of treatments that reported lower placebo response rates. Indeed, ixekizumab 80 mg Q2W, which had high heterogeneity (I2 >75%) and lower placebo response rates in two of three evaluated RCTs, was associated with more favorable results in the unadjusted NMA. By contrast, guselkumab 100 mg, which had higher placebo response rates in the RCTs, was associated with either similar or more favorable results in the analyses that adjusted for cross-trial differences. Findings from a risk difference analysis aligned closely with those from the baseline risk-adjusted NMA, underscoring the importance of adjusting for cross-trial differences in NMAs related to moderate-to-severe plaque psoriasis.
We identified multiple meta-analyses and NMAs [9,10,15–19,64–69] of treatments for moderate-to-severe plaque psoriasis published over the past 5 years that have focused on treatment efficacy during induction (i.e., weeks 10–16 of therapy). The majority of NMAs included TNF-α inhibitors (etanercept, infliximab, adalimumab) and the IL-12/23 inhibitor ustekinumab as relevant comparators; only a small number included the more recently approved and clinically relevant IL-17 inhibitors (secukinumab, ixekizumab). Four recent NMAs by Sbidian et al. [19], Hartz et al. [66], Sawyer et al. [10] and Loos et al. [9] considered PASI outcomes; the latter two [9,10] explored adjustments for variations in baseline risk or placebo response while the former two [19,66] did not. All four reviews [9,10,19,66] reported that ixekizumab was associated with the most favorable benefits among the therapies compared. However, findings from the Sawyer et al. [10] and Loos et al. [9] reviews using meta-regression adjustment for baseline risk indicated ixekizumab's benefits were reduced relative to the unadjusted NMA analysis. An independent Evidence Review Group from NICE [70] considered the meta-regression adjustment for baseline risk to be more appropriate than the unadjusted NMA. The findings from Sawyer et al. [10] and Loos et al. [9] are in line with trends observed in the current methods paper. Our approach also aligns with that outlined in Signorovitch et al. [11], in which the authors also highlighted the importance of adjusting for baseline risk.
To minimize the risk of biased estimates of comparative efficacy, we encourage that future efforts to produce NMAs in psoriasis incorporate thorough assessments for the presence of heterogeneity between studies through careful inspection of tables and graphical displays [71]. In particular, several systematic reviews assessing the benefits and risks of targeted therapies for moderate-to-severe plaque psoriasis have been performed in past years [9–11,15–19,66]; some incorporated NMAs, but to our knowledge only three [9–11] have included any form of secondary analyses accounting for differences between studies regarding patients’ baseline demographics. As shown in this report, these represent potentially important effect modifiers which can influence findings generated from NMAs, and future evidence syntheses in this realm should prospectively plan to account for such differences in their analysis plans. When cross-trial differences remain unaddressed, the potential for suboptimal decision making is heightened. In our current study, accounting for cross-study variation of baseline risk was a vital component of the analysis and more accurately established the similarity of effects of guselkumab 100 mg and ixekizumab 80 mg Q2W.
This study has certain limitations that should be noted. Although there were several previously noted covariates of clinical relevance to be considered to be included in the adjusted analysis, implementation of multivariable adjustments in the NMA was not feasible. There were too few studies within connections in the evidence network to adjust for multiple covariates simultaneously. Fortunately, the baseline risk covariate is often used in NMAs because it can operate as a proxy measure, capturing the effects of several relevant known and unknown factors simultaneously. Thus, the baseline risk measure likely represents an important adjustment factor in cases when seeking to adjust for various cross-trial differences related to study populations.
Conclusion
In summary, when comparing results from multiple RCTs that have interstudy heterogeneous patient populations, unadjusted NMAs should not be conducted, as this may bias comparative efficacy estimates between treatments. The baseline risk-adjusted NMA, which accounts for multiple observed and unobserved effect modifiers, was associated with the best model fit among all prespecified analyses. Findings from the risk difference NMA aligned with the baseline-risk adjusted NMA, lending further credibility to analyses adjusting for heterogeneity. We have presented approaches to more clearly identify heterogeneity among RCTs and adjust for cross-trial differences using a case study in moderate-to-severe plaque psoriasis. Collectively, these approaches should result in more transparent and less biased comparative efficacy estimates when conducting NMAs.
Network meta-analysis has become a commonly used methodology for syntheses having the objective to compare multiple interventions for decision making.
When between-study heterogeneity in important characteristics exists, the guidance suggests that researchers should take careful steps to account for its presence in analyses.
For moderate-to-severe psoriasis, where multiple treatments exist, past systematic reviews have been varied regarding the treatments and studies considered, as well as the inclusion of efforts to account for variation in patient characteristics.
Meta-regression adjustments for baseline risk in NMA are appealing given their potential to account for differences in multiple patient characteristics simultaneously.
In this study, analyses for a comprehensive network of interventions for the Psoriasis Area and Severity Index 90 outcome were performed using unadjusted and adjusted approaches to consider potential implications for interpretations and decision making.
Model fit was improved in NMAs adjusting for variations in baseline risk. Clinically important changes in treatment effect estimates and ordering of treatments were observed. Risk difference NMA produced similar changes.
Future NMAs comparing interventions for plaque psoriasis should incorporate considerations for baseline risk in their analytic plan.
In general, knowledge synthesis researchers should note that adjustments for cross-trial differences in NMA can have important implications when studying the comparative efficacy of healthcare interventions.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2018-0065
Author's contributions
C Cameron, B Hutton, C Druchok, S McElligott, S Nair, A Schubert, A Situ, A Varu, and R Villacorta contributed to study concept and design. C Druchok performed the study selection and screened studies and extracted data. A Situ and A Varu performed the statistical analyses. C Cameron, B Hutton, C Druchok, S McElligott, S Nair, A Schubert, A Situ, A Varu, and R Villacorta reviewed the results and interpreted data. C Cameron, B Hutton, and A Situ prepared figures and wrote the first draft of the manuscript. All authors reviewed multiple versions of the manuscript and approved the final version of the manuscript.
Financial & competing interests disclosure
This study was funded by Janssen, Inc. Cornerstone received financial support from Janssen, Inc. for the conduct of this study. S McElligott, S Nair, A Schubert, and R Villacorta are employees of Janssen, Inc. C Cameron is an employee and shareholder of Cornerstone Research Group, Inc. B Hutton is an employee of the Ottawa Hospital Research Institute and provides methodological advice for Cornerstone Research Group, Inc. C Druchok, A Situ, and A Varu are employees of Cornerstone Research Group, Inc. This research was performed under a research contract between Cornerstone Research Group, Inc. and Janssen, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_material.docx)
- Download
- 1.02 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Caldwell DM, Ades AE, Higgins JP. Simultaneous comparison of multiple treatments: combining direct and indirect evidence. BMJ 331(7521), 897–900 (2005).
2.
Lu G, Ades A. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 23, 3105–3124 (2004).
3.
Dias S, Sutton A, Welton N, Ades A. NICE DSU Technical Support Document 3: heterogeneity: subgroups, meta-regression, bias and bias-adjustment (2012). www.nicedsu.org.uk.
•• Provides key background on implementing meta-regressions.
4.
Salanti G. Indirect and mixed-treatment comparison, network, or multipletreatments meta-analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Res. Synth. Methods 3(2), 80–97 (2012).
5.
Salanti G, Marinho V, Higgins J. A case study of multiple-treatments meta-analysis demonstrates that covariates should be considered. J. Clin. Epidemiol. 62(8), 857–864 (2009).
• Provides case study of the importance of meta-regression adjustments.
6.
Cameron C, Fireman B, Hutton B et al. Network meta-analysis incorporating randomized controlled trials and non-randomized comparative cohort studies for assessing the safety and effectiveness of medical treatments: challenges and opportunities. Syst. Rev. 4, 147 (2015).
7.
Donegan S, Williamson P, D'alessandro U, Tudur Smith C. Assessing key assumptions of network meta-analysis: a review of methods. Res. Synth. Methods 4(4), 291–323 (2013).
8.
Thorlund K, Druyts E, Aviña-Zubieta JA, Wu P, Mills EJ. Why the findings of published multiple treatment comparison meta-analyses of biologic treatments for rheumatoid arthritis are different: an overview of recurrent methodological shortcomings. Ann. Rheum. Dis. 72(9), 1524–1535 (2013).
9.
Loos AM, Liu S, Segel C, Ollendorf DA, Pearson SD, Linder JA. Comparative effectiveness of targeted immunomodulators for the treatment of moderate-to-severe plaque psoriasis: a systematic review and network meta-analysis. J. Am. Acad. Dermatol. 79(1), e7 (2018).
• Other key reviews in the area we cover that have considered network meta-analysis (NMA) with adjustments.
10.
Sawyer L, Fotheringham I, Wright E, Yasmeen N, Gibbons C, Holmen Moller A. The comparative efficacy of brodalumab in patients with moderate-to-severe psoriasis: a systematic literature review and network meta-analysis. J. Dermatolog. Treat., 1–12 (2018) (Epub ahead of print).
• Another key review in the area we cover that has considered NMA with adjustments.
11.
Signorovitch JE, Betts KA, Yan YS et al. Comparative efficacy of biological treatments for moderate-to-severe psoriasis: a network meta-analysis adjusting for cross-trial differences in reference arm response. Br. J. Dermatol. 172(2), 504–512 (2015).
• Other key reviews in the area we cover that have considered NMA with adjustments.
12.
Queiro R, Tejón P, Alonso S, Coto P. Age at disease onset: a key factor for understanding psoriatic disease. Rheumatology (Oxford) 53(7), 1178–1185 (2014).
13.
World Health Organization. Global Report on Psoriasis (2016). http://apps.who.int/iris/bitstream/10665/204417/1/9789241565189_eng.pdf.
14.
Di Meglio P, Villanova F, Nestle FO. Psoriasis. Cold Spring Harb. Perspect. Med. 4(8), pii: a015354 (2014).
15.
National Institute for Clinical Excellence in Health. Apremilast for treating moderate to severe psoriasis (2015). www.nice.org.uk/guidance/ta419/documents/committee-papers-2.
16.
National Institute for Clinical Excellence in Health. Ixekizumab for treating moderate to severe plaque psoriasis (2016). www.nice.org.uk/guidance/ta442/documents/committee-papers-3.
17.
National Institute for Clinical Excellence in Health. Secukinumab for the treatment of moderate to severe plaque psoriasis (2015). www.nice.org.uk/guidance/ta350/documents/secukinumab-for-treating-moderate-to-severe-plaque-psoriasis-committee-papers2.
18.
Jabbar-Lopez ZK, Yiu ZZN, Ward V et al. Quantitative evaluation of biologic therapy options for psoriasis: a systematic review and network meta-analysis. J. Invest. Dermatol. 137(8), 1646–1654 (2017).
19.
Sbidian E, Chaimani A, Garcia-Doval I et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst. Rev. 12, CD011535 (2017).
20.
Dias S, Welton N, Sutton A, Ades A. NICE DSU Technical Support Document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials (2011). http://www.nicedsu.org.uk.
21.
Asahina A, Nakagawa H, Etoh T, Ohtsuki M. Adalimumab M04-688 Study Group. Adalimumab in Japanese patients with moderate to severe chronic plaque psoriasis: efficacy and safety results from a Phase II/III randomized controlled study. J. Dermatol. 37(4), 299–310 (2010).
22.
Bachelez H, Van De Kerkhof PC, Strohal R et al. Tofacitinib versus etanercept or placebo in moderate-to-severe chronic plaque psoriasis: a Phase III randomised non-inferiority trial. Lancet 386(9993), 552–561 (2015).
23.
Blauvelt A, Papp KA, Griffiths CE et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the Phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J. Am. Acad. Dermatol. 76(3), 405–417 (2016).
24.
De Vries AC, Thio HB, De Kort WJ et al. A prospective randomised controlled trial comparing infliximab and etanercept in patients with moderate to severe chronic plaque type psoriasis: the psoriasis infliximab versus etanercept comparison evaluation, the PIECE study. Br. J. Dermatol. 176(3), 624–633 (2016).
25.
Gordon KB, Blauvelt A, Papp KA et al. Phase III trials of ixekizumab in moderate-to-severe plaque psoriasis. N. Engl. J. Med. 375(4), 345–356 (2016).
26.
Gottlieb AB, Leonardi C, Kerdel F, Mehlis S, Olds M, Williams DA. Efficacy and safety of briakinumab vs. etanercept and placebo in patients with moderate to severe chronic plaque psoriasis. Br. J. Dermatol. 165(3), 652–660 (2011).
27.
Griffiths CE, Reich K, Lebwohl M et al. Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis (UNCOVER-2 and UNCOVER-3): results from two Phase III randomised trials. Lancet 386(9993), 541–551 (2015).
28.
Griffiths CE, Strober BE, Van De Kerkhof P et al. Comparison of ustekinumab and etanercept for moderate-to-severe psoriasis. N. Engl. J. Med. 362(2), 118–128 (2010).
29.
Griffiths CE, Thaci D, Gerdes S et al. The EGALITY study: a confirmatory, randomised, double-blind study comparing the efficacy, safety and immunogenicity of GP2015, a proposed etanercept biosimilar, versus the originator product in patients with moderate to severe chronic plaque-type psoriasis. Br. J. Dermatol. 176(4), 928–938 (2016).
30.
Igarashi A, Kato T, Kato M, Song M, Nakagawa H, Japanese Ustekinumab Study Group. Efficacy and safety of ustekinumab in Japanese patients with moderate-to-severe plaque-type psoriasis: long-term results from a Phase II/III clinical trial. J. Dermatol. 39(3), 242–252 (2012).
31.
Langley RG, Elewski BE, Lebwohl M et al. Secukinumab in plaque psoriasis-results of two Phase III trials. N. Engl. J. Med. 371(4), 326–338 (2014).
32.
Lebwohl M, Strober B, Menter A et al. Phase III studies comparing brodalumab with ustekinumab in psoriasis. N. Engl. J. Med. 373(14), 1318–1328 (2015).
33.
Leonardi CL, Kimball AB, Papp KA et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 76-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 1). [Erratum appears in Lancet 371(9627), 1838 (2008)]. Lancet 371(9625), 1665–1674 (2008).
34.
Leonardi CL, Powers JL, Matheson RT et al. Etanercept as monotherapy in patients with psoriasis. N. Engl. J. Med. 349(21), 2014–2022 (2003).
35.
Menter A, Feldman SR, Weinstein GD et al. A randomized comparison of continuous vs. intermittent infliximab maintenance regimens over 1 year in the treatment of moderate-to-severe plaque psoriasis. J. Am. Acad. Dermatol. 56(1), e1 (2007).
36.
Menter A, Tyring SK, Gordon K et al. Adalimumab therapy for moderate to severe psoriasis: a randomized, controlled Phase III trial. J. Am. Acad. Dermatol. 58(1), 106–115 (2008).
37.
Mrowietz U, Leonardi CL, Girolomoni G et al. Secukinumab retreatment-as-needed versus fixed-interval maintenance regimen for moderate to severe plaque psoriasis: a randomized, double-blind, noninferiority trial (SCULPTURE). J. Am. Acad. Dermatol. 73(1), e1 (2015).
38.
Papp K, Reich K, Leonardi CL et al. Apremilast, an oral phosphodiesterase 4 (PDE4) inhibitor, in patients with moderate to severe plaque psoriasis: results of a Phase III, randomized, controlled trial (Efficacy and Safety Trial Evaluating the Effects of Apremilast in Psoriasis [ESTEEM] 1). J. Am. Acad. Dermatol. 73(1), 37–49 (2015).
39.
Papp KA, Langley RG, Lebwohl M et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 52-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 2). Lancet 371(9625), 1675–1684 (2008).
40.
Papp KA, Reich K, Paul C et al. A prospective Phase III, randomized, double-blind, placebo-controlled study of brodalumab in patients with moderate-to-severe plaque psoriasis. Br. J. Dermatol. 175(2), 273–286 (2016).
41.
Papp KA, Tyring S, Lahfa M et al. A global Phase III randomized controlled trial of etanercept in psoriasis: safety, efficacy, and effect of dose reduction. Br. J. Dermatol. 152(6), 1304–1312 (2005).
42.
Paul C, Cather J, Gooderham M et al. Efficacy and safety of apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate-to-severe plaque psoriasis over 52 weeks: a Phase III, randomized controlled trial (ESTEEM 2). Br. J. Dermatol. 173(6), 1387–1399 (2015).
43.
Paul C, Lacour JP, Tedremets L et al. Efficacy, safety and usability of secukinumab administration by autoinjector/pen in psoriasis: a randomized, controlled trial (JUNCTURE). J. Eur. Acad. Dermatol. Venereol. 29(6), 1082–1090 (2015).
44.
Reich K, Armstrong AW, Foley P et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: results from the Phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J. Am. Acad. Dermatol. 76(3), 418–431 (2016).
45.
Reich K, Gooderham M, Green L et al. The efficacy and safety of apremilast, etanercept and placebo in patients with moderate-to-severe plaque psoriasis: 52-week results from a Phase IIIb, randomized, placebo-controlled trial (LIBERATE). J. Eur. Acad. Dermatol. Venereol. 31(3), 507–517 (2016).
46.
Reich K, Nestle FO, Papp K et al. Infliximab induction and maintenance therapy for moderate-to-severe psoriasis: a Phase III, multicentre, double-blind trial. Lancet 366(9494), 1367–1374 (2005).
47.
Saurat JH, Stingl G, Dubertret L et al. Efficacy and safety results from the randomized controlled comparative study of adalimumab vs. methotrexate vs. placebo in patients with psoriasis (CHAMPION). Br. J. Dermatol. 158(3), 558–566 (2008).
48.
Strober BE, Crowley JJ, Yamauchi PS, Olds M, Williams DA. Efficacy and safety results from a Phase III, randomized controlled trial comparing the safety and efficacy of briakinumab with etanercept and placebo in patients with moderate to severe chronic plaque psoriasis. Br. J. Dermatol. 165(3), 661–668 (2011).
49.
Strohal R, Puig L, Chouela E et al. The efficacy and safety of etanercept when used with as-needed adjunctive topical therapy in a randomised, double-blind study in subjects with moderate-to-severe psoriasis (the PRISTINE trial). J. Dermatolog. Treat. 24(3), 169–178 (2013).
50.
Thaci D, Blauvelt A, Reich K et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate to severe plaque psoriasis: CLEAR, a randomized controlled trial. J. Am. Acad. Dermatol. 73(3), 400–409 (2015).
51.
Torii H, Nakagawa H, Japanese Infliximab Study investigators. Infliximab monotherapy in Japanese patients with moderate-to-severe plaque psoriasis and psoriatic arthritis. A randomized, double-blind, placebo-controlled multicenter trial. J. Dermatol. Sci. 59(1), 40–49 (2010).
52.
Tsai TF, Ho JC, Song M et al. Efficacy and safety of ustekinumab for the treatment of moderate-to-severe psoriasis: a Phase III, randomized, placebo-controlled trial in Taiwanese and Korean patients (PEARL). J. Dermatol. Sci. 63(3), 154–163 (2011).
53.
Tyring S, Gottlieb A, Papp K et al. Etanercept and clinical outcomes, fatigue, and depression in psoriasis: double-blind placebo-controlled randomised Phase III trial. Lancet 367(9504), 29–35 (2006).
54.
Van De Kerkhof PC, Segaert S, Lahfa M et al. Once weekly administration of etanercept 50 mg is efficacious and well tolerated in patients with moderate-to-severe plaque psoriasis: a randomized controlled trial with open-label extension. Br. J. Dermatol. 159(5), 1177–1185 (2008).
55.
Yang HZ, Wang K, Jin HZ et al. Infliximab monotherapy for Chinese patients with moderate to severe plaque psoriasis: a randomized, double-blind, placebo-controlled multicenter trial. Chin. Med. J. 125(11), 1845–1851 (2012).
56.
Zhu X, Zheng M, Song M et al. Efficacy and safety of ustekinumab in Chinese patients with moderate to severe plaque-type psoriasis: results from a Phase III clinical trial (LOTUS). J. Drugs Dermatol. 12(2), 166–174 (2013).
57.
Blauvelt A, Prinz JC, Gottlieb AB et al. Secukinumab administration by pre-filled syringe: efficacy, safety and usability results from a randomized controlled trial in psoriasis (FEATURE). Br. J. Dermatol. 172(2), 484–493 (2015).
58.
Cai L, Gu J, Zheng J et al. Efficacy and safety of adalimumab in Chinese patients with moderate-to-severe plaque psoriasis: results from a Phase III, randomized, placebo-controlled, double-blind study. J. Eur. Acad. Dermatol. Venereol. 31(1), 89–95 (2017).
59.
Torres T, Puig L. Treatment goals for psoriasis: Should PASI 90 become the standard of care? Acta Dermosifiliogr. 106(3), 155–157 (2015).
60.
Higgins JP, Thompson SG. Controlling the risk of spurious findings from meta-regression. Stat. Med. 23(11), 1663–1682 (2004).
61.
Thompson SG, Higgins JP. How should meta-regression analyses be undertaken and interpreted? Stat. Med. 21(11), 1559–1573 (2002).
62.
Warn DE, Thompson SG, Spiegelhalter DJ. Bayesian random effects meta-analysis of trials with binary outcomes: methods for the absolute risk difference and relative risk scales. Stat. Med. 21(11), 1601–1623 (2002).
63.
Nikolakopoulou A, Chaimani A, Veroniki AA, Vasiliadis HS, Schmid CH, Salanti G. Characteristics of networks of interventions: a description of a database of 186 published networks. PLoS ONE 9(1), e86754 (2014).
64.
Gómez-García F, Epstein D, Isla-Tejera B, Lorente A, Vélez García-Nieto A, Ruano J. Short-term efficacy and safety of new biological agents targeting the interleukin-23-T helper 17 pathway for moderate-to-severe plaque psoriasis: a systematic review and network meta-analysis. Br. J. Dermatol. 176(3), 594–603 (2017).
65.
Gupta S, Faughnan ME, Tomlinson GA, Bayoumi AM. A framework for applying unfamiliar trial designs in studies of rare diseases. J. Clin. Epidemiol. 64(10), 1085–1094 (2011).
66.
Hartz S. Network meta-analysis to evaluate the efficacy of ixekizumab in the treatment of moderate-to-severe psoriasis. ISPOR 19th Annual European Congress. Vienna, Austria, 29 October–2 November (2016).
67.
Lin VW, Ringold S, Devine EB. Comparison of ustekinumab with other biological agents for the treatment of moderate to severe plaque psoriasis: a Bayesian network meta-analysis. Arch. Dermatol. 148(12), 1403–1410 (2012).
68.
Odom D, Brogan A, Talbird SE, Schenkel B. A network meta-analysis of randomized, controlled trials of ustekinumab and adalimumab for moderate-to-severe psoriasis. Value Health 16, A112 (2013).
69.
Peruzzi M, Colombo D, De Falco E, Chimenti I, Abbate A et al. Biologic therapy for psoriatic arthritis or moderate to severe plaque psoriasis: systematic review with pairwise and network meta-analysis. Int. J. Stat. Med. Res. 3, 74–87 (2014).
70.
National Institute for Clinical Excellence in Health. Final appraisal determination. Brodalumab for treating moderate to severe plaque psoriasis (2018). www.nice.org.uk/guidance/gid-ta10220/documents/final-appraisal-determination-document.
71.
Batson S, Score R, Sutton AJ. Three-dimensional evidence network plot system: covariate imbalances and effects in network meta-analysis explored using a new software tool. J. Clin. Epidemiol. 86, 182–195 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Janssen Inc.
History
Received: 9 July 2018
Accepted: 17 August 2018
Published online: 2 October 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Importance of assessing and adjusting for cross-study heterogeneity in network meta-analysis: a case study of psoriasis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0065
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yuning Zhao, Guangxin Luo, Can Huang, Zhenyang Chen, Yu Wei, Qiaosen Chen, Fang Wang, Yong Gan, Xiaoxv Yin, Comparative effects of some pharmacological and non-pharmacological interventions on cognitive function in Alzheimer’s disease: A Bayesian network meta-analysis, The Journal of Prevention of Alzheimer's Disease, 10.1016/j.tjpad.2026.100564, 13, 6, (100564), (2026).
- Keya Joshi, Aaron Situ, Wei-Jhih Wang, Mihaela Georgieva, Nicolas van de Velde, Ekkehard Beck, Letter to the Editor: comparative effectiveness of omicron XBB 1.5-adapted COVID-19 vaccines: a systematic literature review and network meta-analysis, Expert Review of Vaccines, 10.1080/14760584.2025.2554689, 24, 1, (870-872), (2025).
- Mark G. Lebwohl, André Carvalho, Akihiko Asahina, Jianzhong Zhang, Mir Sohail Fazeli, Ellen Kasireddy, Paul Serafini, Thomas Ferro, Ranga Gogineni, Diamant Thaçi, Biologics for the Treatment of Moderate-to-Severe Plaque Psoriasis: A Systematic Review and Network Meta-analysis, Dermatology and Therapy, 10.1007/s13555-025-01423-0, 15, 7, (1633-1656), (2025).
- Nils Erik Gilhus, Saiju Jacob, Mahmoud Hashim, Suzy Van Sanden, Christopher Drudge, Anna Nero, Sumeet Singh, Kavita Gandhi, Brian Hutton, Network connectivity, between-study heterogeneity and timepoint challenges in generalized myasthenia gravis: a feasibility assessment of indirect treatment comparisons, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0009, 14, 6, (2025).
- Nicholas Riley, Christopher Drudge, Morag Nelson, Anja Haltner, Michael Barnett, Simon Broadley, Helmut Butzkueven, Pamela McCombe, Anneke Van der Walt, Erin O. Y. Wong, Martin Merschhemke, Nicholas Adlard, Rob Walker, Imtiaz A. Samjoo, Comparative efficacy of ofatumumab versus oral therapies for relapsing multiple sclerosis patients using propensity score analyses and simulated treatment comparisons , Therapeutic Advances in Neurological Disorders, 10.1177/17562864241239453, 17, (2024).
- Carole Lunny, Areti-angeliki Veroniki, Julian P. T. Higgins, Sofia Dias, Brian Hutton, James M. Wright, Ian R. White, Penny Whiting, Andrea C. Tricco, Methodological review of NMA bias concepts provides groundwork for the development of a list of concepts for potential inclusion in a new risk of bias tool for network meta-analysis (RoB NMA Tool), Systematic Reviews, 10.1186/s13643-023-02388-x, 13, 1, (2024).
- April W. Armstrong, Richard B. Warren, Yichen Zhong, Joe Zhuo, Allie Cichewicz, Ananth Kadambi, Daniela Junqueira, Tracy Westley, Renata Kisa, Carolin Daamen, Matthias Augustin, Short-, Mid-, and Long-Term Efficacy of Deucravacitinib Versus Biologics and Nonbiologics for Plaque Psoriasis: A Network Meta-Analysis, Dermatology and Therapy, 10.1007/s13555-023-01034-7, 13, 11, (2839-2857), (2023).
- Christopher Drudge, Imtiaz A Samjoo, Róisín Brennan, Lohit Badgujar, Vivek Khurana, Santosh Tiwari, Nicholas Adlard, Judit Banhazi, An overview of reviews with network meta-analyses comparing disease-modifying therapies for relapsing multiple sclerosis, Future Neurology, 10.2217/fnl-2023-0009, 18, 3, (2023).
- Herman Sehmbi, Susanne Retter, Ushma J. Shah, Derek Nguyen, Janet Martin, Vishal Uppal, Epidemiological, methodological, and statistical characteristics of network meta-analysis in anaesthesia: a systematic review, British Journal of Anaesthesia, 10.1016/j.bja.2022.08.042, 130, 3, (272-286), (2023).
- Dan Pettitt, Michael Plotnick, Joshua Gagne, Letter to the Editor Regarding Long-Term Benefit–Risk Profiles of Treatments for Moderate-to-Severe Plaque Psoriasis: A Network Meta-analysis, Dermatology and Therapy, 10.1007/s13555-022-00809-8, 12, 12, (2863-2866), (2022).