Daclatasvir combined with asunaprevir is a cost-effective and cost-saving treatment for hepatitis C infection in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate the cost–effectiveness of the novel all-oral direct-acting antiviral regimen daclatasvir + asunaprevir (DUAL), versus interferon-based regimens for the treatment of chronic hepatitis C virus genotype 1b infection. Methods: Inputs for a lifetime Markov model were sourced from clinical trials and published literature. Outputs include disease management costs, life expectancy, quality-adjusted life-years and cost–effectiveness. Sensitivity analyses assessed the drivers of cost–effectiveness and sustained virologic response thresholds at which DUAL is cost-saving. Results: DUAL was associated with discounted incremental quality-adjusted life-years of 1.29–3.85 and incremental life-years of 0.85–2.59 per patient, with discounted lifetime cost savings of USD$1415–8525. Associated sustained virologic response rates could fall to 45.1–84.8%, while remaining dominant. Conclusion: Treatment with DUAL provides significant clinical benefit, while accruing lower lifetime costs.
Hepatitis C is a liver disease caused by infection with the blood-borne hepatitis C virus (HCV). Untreated, chronic infection with HCV can lead to life-threatening end-stage liver disease (ESLD) complications, including DC and hepatocellular carcinoma (HCC) and death [1].
HCV infection is associated with a significant disease burden in China, where, as of 2015, approximately 9.8 million people were estimated to be chronically infected [2]. The majority of HCV cases in China are of genotype 1b infection (56.8%) [3]; however, the prevalence of specific HCV genotypes have been reported to vary significantly across provinces within China [4–6].
Standard of care for HCV treatment in China is evolving rapidly, with the majority of patients still treated with interferon-based regimens only, specifically pegylated interferon-alfa-2a + ribavirin (pegIFN/RBV) and interferon-alfa + ribavirin (IFN/RBV) [3,7]. However, these regimens offer suboptimal efficacy and safety profiles, and a considerable proportion of patients are contraindicated for therapy due to intolerance to or ineligibility for interferon [8–10]. In particular, treatment of genotype 1b HCV infection is known to be difficult, and the therapeutic response to interferon-based regimens in these patients have been reported to be lower compared with patients infected with genotypes 2 or 3 [3,11,12]. Furthermore, a large proportion of HCV patients in China present with severe or advanced disease due to poor public awareness and delays in seeking medical care; treatment options for these patients are notably limited [3]. Hence, there is a significant unmet need with respect to HCV disease management and public health.
The aim of treatment for chronic HCV infection is to achieve viral eradication via a sustained virologic response (SVR). SVR corresponds to cure (from a virologic standpoint) in 99% of patients, with studies demonstrating that undetectable levels of HCV RNA were maintained over long-term follow-up, and is associated with improved quality of life, regression of fibrosis and reduced risk of liver-related complications [13–15]. The development of novel, all-oral direct-acting antiviral (DAA) regimens have revolutionized HCV therapy; DAAs have the potential to address the unmet need of safe and effective HCV therapy by providing efficacious and well-tolerated treatment options. The DAA combination of daclatasvir + asunaprevir (DUAL) has demonstrated high efficacy for patients infected with HCV genotype 1b, and represents a treatment option for those for which interferon-based treatments are incompatible or whom would otherwise not be treated [16,17]. DUAL is the first DAA to receive regulatory approval in China [18]. As such, there is a requirement to assess the potential clinical and economic benefit associated with the introduction of DUAL in China versus current interferon-based regiments.
The objective of this study, therefore, was to demonstrate the relative clinical and economic value of DUAL versus current interferon-based regimens, via a conventional cost–effectiveness analysis for the treatment of genotype 1b HCV infection in China.
Methods
The analysis undertaken within this study aims to evaluate the cost–effectiveness of DUAL versus interferon-based regimens, in two key patient populations. The following comparisons have been undertaken:
–
Interferon-ineligible/intolerant
•
DUAL versus no treatment
–
Treatment-naive population
•
DUAL versus pegIFN/RBV
•
DUAL versus IFN/RBV
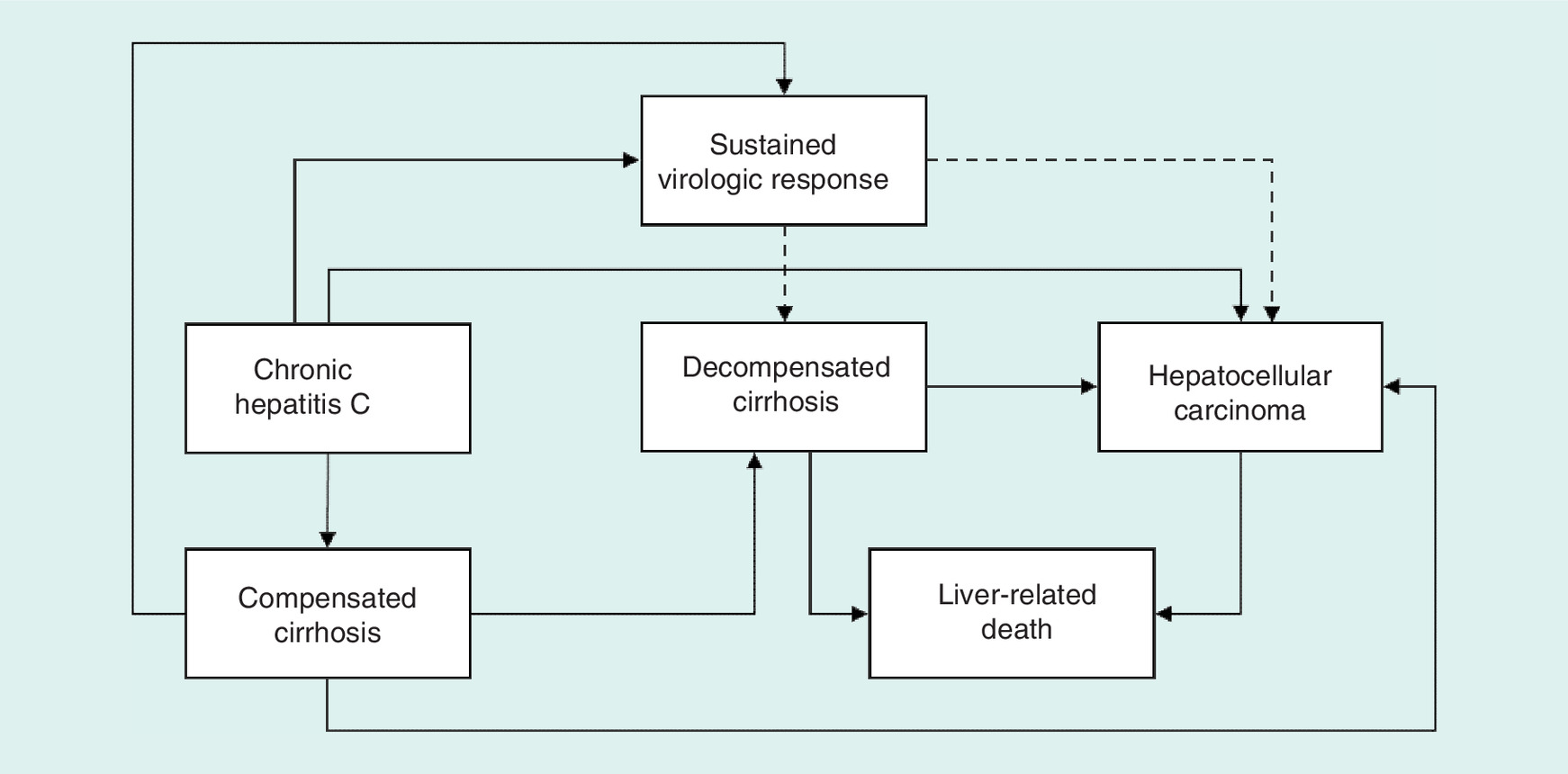
A previously published disease progression and cost–effectiveness model [19–28] was used to estimate the costs and benefits associated with 24 weeks of treatment with DUAL versus 48 weeks of treatment with pegIFN/RBV, 48 weeks of treatment with IFN/RBV or no treatment [29–34]. The model runs in annual cycles over a variable time horizon, up to patient lifetime (a maximum of 80 modeled years), with a half-cycle correction applied, and employs a treatment decision tree in the first modeled year to predict treatment-related outcomes and costs. Patients enter the model at the chronic hepatitis C without cirrhosis health state or the compensated cirrhosis (CC) health state (or they may be distributed across the two), and may subsequently progress to decompensated cirrhosis (DC), HCC or death (Figure 1). Simulation of the natural history of chronic hepatitis C is captured through the application of health state-specific disease transition rates, and the clinical and cost implications for each health state are informed by Chinese data (Table 1). Background rates of all-cause mortality for those in the chronic hepatitis C and CC health states were modelled in line with Chinese life tables; disease specific mortality rates were utilized for all other health states [35].
| Health states | Mean cost USD$ (SE)† | Source | Utility value (SE) | Source |
|---|---|---|---|---|
| Chronic hepatitis C | 900‡ (149) | Chen et al. 2016 [55] | 0.86 (0.02) | MHLW, 2013 [56] |
| Compensated cirrhosis | 2563 (844) | 0.77 (0.02) | MHLW, 2013 [56] | |
| Decompensated cirrhosis | 5708 (1143) | 0.64 (0.04) | MHLW, 2013 [56] | |
| HCC | 12,048 (1727) | 0.47 (0.05) | MHLW, 2013 [56] | |
| SVR from chronic hepatitis C§ | – | – | 0.93 | MHLW, 2013 [56] |
| SVR from compensated cirrhosis§ | 1817 (599) | Rate ratio of 0.709 applied to the cost of compensated cirrhosis, taken from Manos et al. 2013 [57] | 0.93 | MHLW, 2013 [56] |
†
‡
Applied in the first year only, based upon clinical expert opinion.
§
Assumed that no direct medical costs incurred by patients following SVR in chronic hepatitis C stage.
HCC: Hepatocellular carcinoma; SE: Standard error; SVR: Sustained virologic response.
A cohort of 1000 patients with mean age of 44.5 years, 52.1% male and 6.1% with CC was modeled until death (or until age 100, the maximum modeled age) and predicted total HCV-related costs (treatment and disease management), life-years and quality-adjusted life years (QALYs) were accrued [36]. A payer perspective has been adopted, with costs and benefits discounted at an annual rate of 5% [37].
Treatment is initiated during the first year of the modeled time horizon and a decision tree is used to determine whether treatment is successful, defined according to rates of SVR. If treatment is successful, patients move to the SVR health state. Based upon published probabilities and consistent with a previous study regarding the expected complication rates associated with the regimens of interest [32], it is assumed that patients who achieve SVR from the chronic hepatitis C state without cirrhosis remain in the SVR state for the duration of the simulation and do not incur further complications; however, a proportion of those who achieve SVR from the state of CC will progress to HCC. In those subjects that do not achieve SVR, disease progression continues from whichever state they were in at initiation of antiviral therapy (Table 2).
| Transition rates | Mean rate (SE) | Source |
|---|---|---|
| Chronic hepatitis C to compensated cirrhosis | 0.060 (0.007) | MHLW, 2013 [56] |
| Chronic hepatitis C to HCC | 0.007 (0.004) | MHLW, 2013 [56] |
| Compensated cirrhosis to decompensated cirrhosis | 0.041 (0.002) | MHLW, 2013 [56] |
| Compensated cirrhosis to HCC | 0.019 (0.002) | MHLW, 2013 [56] |
| Decompensated cirrhosis to HCC | 0.024 (0.004) | MHLW, 2013 [56] |
| Decompensated cirrhosis to death | 0.142 (0.011) | MHLW, 2013 [56] |
| HCC to death | 0.576 (0.036) | MHLW, 2013 [56] |
| Post SVR (compensated cirrhosis) to decompensated cirrhosis | 0 (0) | Assumption |
| Post SVR (compensated cirrhosis) to HCC | 0 (0) | Assumption |
HCC: Hepatocellular carcinoma; SE: Standard error; SVR: Sustained virologic response.
Efficacy data were sourced from four published Phase III trials [38–41] and analyses were stratified by the following patient populations: treatment-naive and interferon-ineligible/intolerant patients. Rates of SVR and discontinuation are presented in Table 3; discontinuation was applied in week 4 of the modeled horizon as data relating to the timing of discontinuation was unavailable. A treatment decision tree is used within the first modeled year to predict treatment-related outcomes and costs. Treatment-related adverse events were not incorporated due to the lack of consistent reporting of endpoints across studies; such an omission can be considered conservative due to the higher rate of adverse event incidence among interferon-based regimens [42,43]. Total treatment costs associated with 24 weeks of DUAL and 48 weeks of pegIFN/RBV and IFN/RBV were estimated at ¥57,810 ($8835), ¥48,432 ($7402) and ¥10,276 ($1571), respectively; all drug costs were taken from China-specific sources [44–46]. Costs associated with testing for baseline resistance associated substitutions (RAS), a resistance which can impact the efficacy of DAA therapies, was not explicitly incorporated within the analysis [47]. All costs have been inflated to 2017 values in line with China inflation factors [48,49].
| Population | Treatment regimen | SVR n/N (% [SE]) | Discontinuation n/N (% [SE]) ¶ | Author (Year) | Ref. |
|---|---|---|---|---|---|
| Intervention | |||||
| Treatment-naive# | DUAL | 110/119 (92.4 [2.4])† | 1/155 (0.6 [0.6])‡ | Wei et al. (2017) | [58] |
| Interferon ineligible-intolerant | DUAL | 116/127 (91.3 [2.5]) | 9/127 (7.1 [2.3])§ | Wei et al. (2016) | [41] |
| Comparator | |||||
| Treatment-naive# | PegIFN + RBV | 111/178 (62.4 [3.6]) | 7/178 (3.9 [1.5])# | Rao et al. (2016) | [59] |
| Treatment-naive# | IFN + RBV | (44.4 [3.0]) | (15.0 [2.4])# | Mao (2012) | [46] |
| Interferon ineligible-intolerant | No treatment | 0 | 0 | Assumption | – |
†
“Chinese” subgroup analysis of treatment-naive cohort.
‡
Whole treatment-naive cohort.
§
Did not complete treatment due to lack of efficacy, AE or death.
¶
As the timing of discontinuation is not available, all discontinuations are assumed to occur at week 4 (the earliest point of discontinuation that the model allows).
#
Patients who have not received prior treatment for hepatitis C virus infection.
DUAL: Daclatasvir + asunaprevir; pegIFN: Pegylated interferon-alfa; RBV: Ribavirin; SE: Standard error; SVR: Sustained virologic response.
Univariate sensitivity analysis was undertaken to assess the impact of individual model parameters upon cost–effectiveness outcomes. In addition, four specific scenarios were considered to assess alternative modelling assumptions:
–
DUAL retreatment: As DUAL was the only available DAA regimen at the time of this analysis, all patients failing to achieve SVR with DUAL were retreated with the same regimen; retreatment was assumed to take place in the first modelled year.
–
Midpoint treatment discontinuation: Due to the uncertainty in the timing of discontinuation, a scenario was undertaken where discontinuation was applied at the midpoint of the treatment schedule (12 weeks for DUAL, 24 weeks for IFN-based regimens).
–
Post-SVR CHC cost: In line with previous studies, in the base case analysis, no cost associated with post-SVR disease management in those achieving SVR from the chronic hepatitis C health state has been applied. As there remains some uncertainty as to the application of such a cost, a scenario analysis was undertaken in which a cost of $638.41 was applied to patients that achieved SVR from the chronic hepatitis C health state each year post SVR. This cost was derived by taking the ratio of SVR to non-SVR CC health state costs and multiplying the ratio by the chronic hepatitis C health state cost.
–
CHC cost in subsequent years: In line with previous studies, in the base case analysis, no cost associated with chronic hepatitis C disease management is applied in subsequent years. As there remains some uncertainty as to the application of such a cost, a scenario analysis was undertaken where the chronic hepatitis C health state cost associated with the initial year of management was also applied in all subsequent years.
Probabilistic sensitivity analysis was undertaken to assess the overall uncertainty in predicted economic outcomes arising from the joint uncertainty in model input parameters. The analysis utilized a conventional probabilistic analysis approach in which all model input parameters are simultaneously, and independently, sampled using appropriate statistical distributions. A Beta distribution was used to sample proportions, a Gamma distribution used to sample costs, while patient age was sampled from a Normal distribution.
Outcomes of the cost–effectiveness analyses were converted from RMB¥ to USD$ using a conversion rate of 1USD$:6.54312RMB¥ [50].
Results
DUAL was associated with significant reductions in HCV-related morbidity and mortality (Figure 2). Among a cohort of 1000 treatment-naive patients, it was estimated that the introduction of DUAL could result in 182 and 151 fewer patients developing DC and HCC over a lifetime, respectively, and 306 fewer liver-related deaths, compared with interferon-based regimens. Similar reductions, were observed in the interferon-ineligible/intolerant population, when DUAL was compared with no treatment (DC: 347; HCC: 288; liver-related mortality: 581). Consequently, DUAL was associated with a reduction in DC, HCC and liver-related mortality incidence of 79.8, 86.3 and 91.3%, when compared with pegIFN/RBV, IFN/RBV and no treatment, respectively.
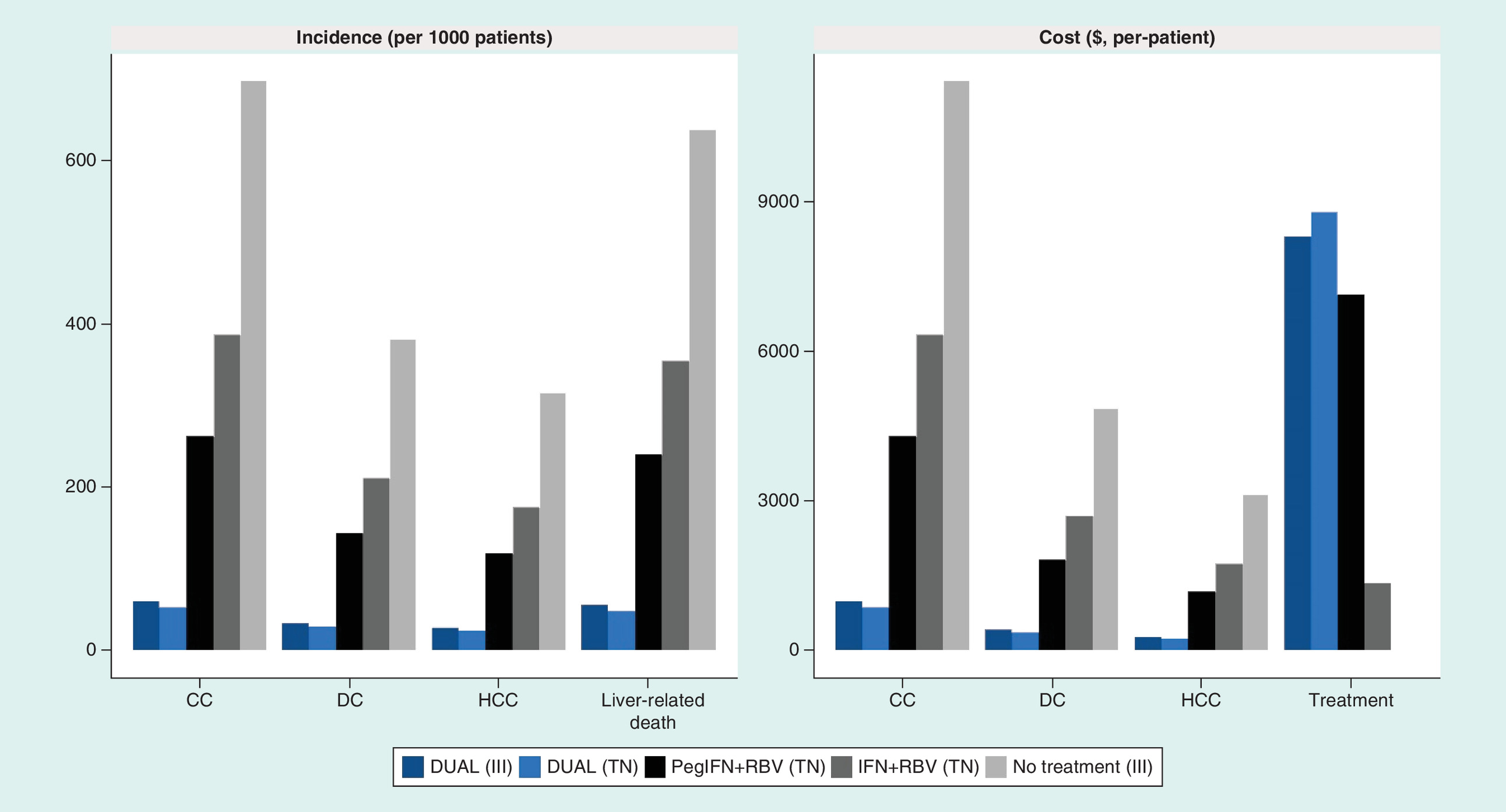
Figure 2. End stage liver disease and mortality incidence and cost.
III: Interferon-ineligible/intolerant; TN: Treatment-naive.
As a consequence of greater rates of efficacy and subsequently, lower rates of HCV-related morbidity and mortality, DUAL was associated with significant improvements in quality of life and life expectancy. Discounted lifetime QALY and life-year gains, compared with pegIFN/RBV, IFN/RBV and no treatment, were 1.29, 2.04 and 3.85 QALYs, and 0.85, 1.36 and 2.59 life-years, respectively (Table 4 & Figure 3).
| Population | Discounting | Treatment regimen | Total cost ($) | Total QALYs | Total life years | Incremental cost of DUAL ($) | Incremental QALYs associated with DUAL | Incremental life years associated with DUAL | ICER ($/QALY) | Lowest DUAL SVR at which DUAL remains dominant |
|---|---|---|---|---|---|---|---|---|---|---|
| Interferon-ineligible/ intolerant | Discounted | DUAL | 11,702 | 14.58 | 15.86 | – | – | – | – | – |
| No treatment | 20,227 | 10.73 | 13.27 | -8525 | 3.85 | 2.59 | -2213 (DUAL is dominant) | 45.1% | ||
| Undiscounted | DUAL | 15,471 | 29.51 | 32.06 | – | – | – | – | – | |
| No treatment | 44,056 | 18.80 | 23.66 | -28,585 | 10.71 | 8.41 | -2670 (DUAL is dominant) | 20.60% | ||
| Treatment-naive† | Discounted | DUAL | 11,978 | 14.63 | 15.89 | – | – | – | – | – |
| PegIFN + RBV | 15,857 | 13.34 | 15.04 | -3879 | 1.29 | 0.85 | -3013 (DUAL is dominant) | 74.10% | ||
| IFN + RBV | 13,393 | 12.58 | 14.53 | -1415 | 2.04 | 1.36 | -694 (DUAL is dominant) | 84.80% | ||
| Undiscounted | DUAL | 15,505 | 29.64 | 32.16 | – | – | – | – | – | |
| PegIFN + RBV | 25,975 | 26.10 | 29.40 | -10,470 | 3.54 | 2.76 | -2958 (DUAL is dominant | 66.50% | ||
| IFN + RBV | 27,467 | 23.99 | 27.74 | -11,962 | 5.64 | 4.42 | -2119 (DUAL is dominant) | 62.90% |
†
Patients who have not received prior treatment for hepatitis C virus infection
DUAL: Daclatasvir + asunaprevir; ICER: Incremental cost–effectiveness ratio; IFN: Interferon; PegIFN: Pegylated interferon-alfa; QALY: Quality-adjusted life year; RBV: Ribavirin.
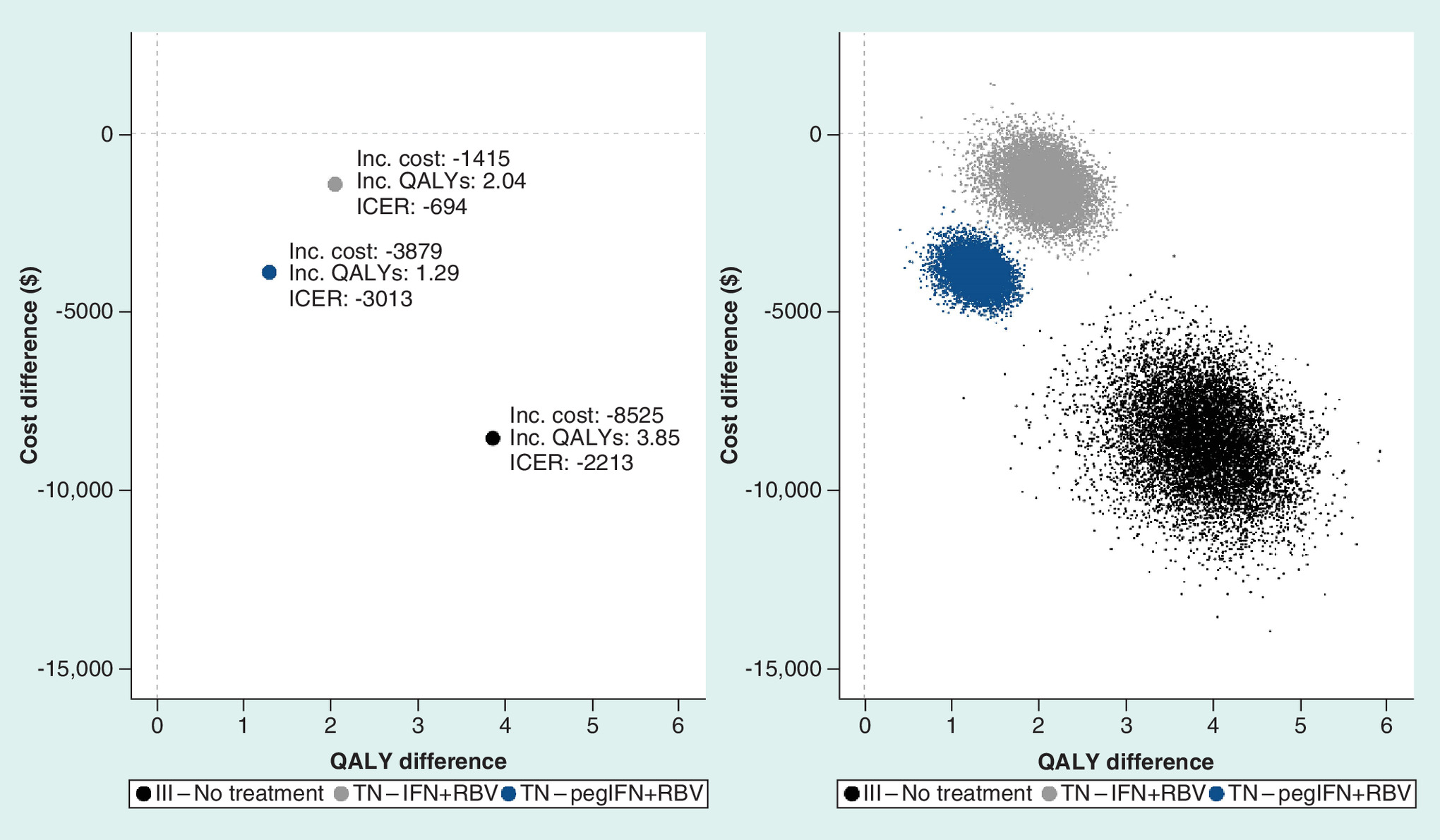
Figure 3. Cost–effectiveness plane and probabilistic sensitivity analysis scatter plot comparing cost–effectiveness of pegIFN/RBV, IFN/RBV and no treatment.
III: Interferon-ineligible/intolerant; TN: Treatment-naive.
Treatment with DUAL was associated with higher treatment costs compared with current interferon-based regimens (between $1654 and $8312 when discounting was applied) but a reduction in total lifetime costs, due to cost-offsets associated with reduced ESLD incidence and subsequent management (Figure 2). Discounted lifetime incremental costs ranged from -$8525 to -$1415, with the largest reduction observed in the interferon-ineligible/intolerant population (Table 4 & Figure 3).
In terms of cost–effectiveness, DUAL was predicted to dominate (more effective, less expensive) all comparators (pegIFN/RBV, IFN/RBV and no treatment), in both treatment-naive and interferon-ineligible/intolerant patient populations. These findings were robust across sensitivity analyses, including SVR threshold analyses that demonstrated DUAL would remain dominant even with significant reductions in the rate of SVR (Table 4). Univariate (deterministic) sensitivity analyses demonstrated that cost–effectiveness conclusions were relatively insensitive to alternative parameter assumptions and model input values (Figure 4). Estimated cost–effectiveness results were most sensitive to the simulated time horizon, starting health state, SVR rates and alternative cost assumptions; while baseline patient age and sex, rates of discounting and transition rates were the least influential. DUAL was estimated to have a 100% probability of being cost-effective across all comparisons in probabilistic analyses, assuming a willingness-to-pay threshold of $8123/QALY (1 × China GDP per capita) [51].
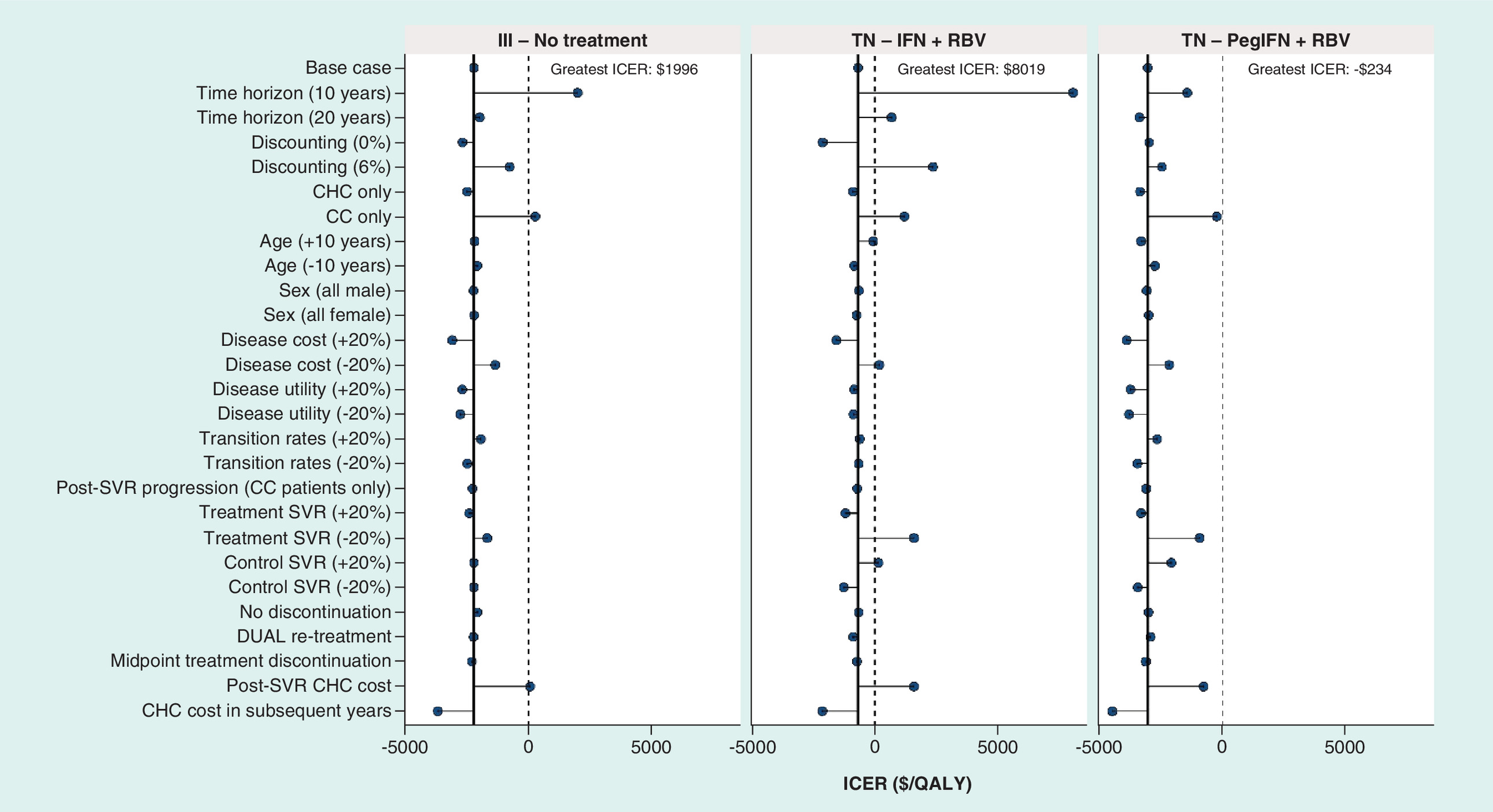
Figure 4. Univariate and sensitivity analyses (cost–effectiveness).
CC: Compensated cirrhosis; DUAL: Daclatasvir + asunaprevir; ICER: Incremental cost–effectiveness ratio; IFN: Interferon; III: Interferon-ineligible/intolerant; QALY: Quality-adjusted life year; RBV: Ribavirin; SVR: Sustained virological response; TN: Treatment-naive.
Discussion & conclusion
DUAL is the first all-oral DAA regimen approved as a treatment option for HCV in China. To understand the consequences associated with the introduction of DUAL to patients and the health system, an economic analysis was conducted to assess the clinical and economic implications of DUAL compared with current interferon-based regimens.
Treatment with DUAL was associated with reduced lifetime costs and greater life expectancy and quality-adjusted life expectancy, compared with current interferon-based regimens, due to a reduction in ESLD event incidence through significantly improved SVR rates. Results of this study demonstrate that DUAL dominates all comparators (pegIFN/RBV, IFN/RBV and no treatment) in terms of cost–effectiveness (more effective, less expensive). Consequently, from a payers perspective, and when considering lifetime outcomes, the introduction of DUAL is likely to benefit both patients (in terms of improved life expectancy and quality of life) and healthcare providers (in terms of reduced cost), with previous studies demonstrating that these benefits are maximized through early treatment [25].
These findings are particularly relevant given that interferon-based regimens, the historical standard of care for HCV infection in China, are not well-tolerated and have suboptimal rates of cure, with a significant proportion of patients either intolerant to, or ineligible for, interferon-based treatment. Therefore, there are a significant number of patients whose disease prognosis is particularly poor and that have no alternative, viable, treatment options. In this context, the introduction of DUAL and the ability to treat such patients is likely to offer significant benefit to patients, the healthcare system, and society in general, through reduced HCV-related morbidity and mortality and lost economic productivity.
There are several limitations related to the data and modeling assumptions required to generate estimates of cost–effectiveness that are relevant to the interpretation of these results. Uncertainty in the values of key model parameters, including SVR and disease progression, therapy acquisition cost and heterogeneity among patients, has been accounted for in extensive model sensitivity analysis. Results of sensitivity analyses confirm the robustness of cost–effectiveness inferences. While local (Chinese) data sources were used where available, alternative data sources from non-Chinese populations were sourced otherwise; these data sources were largely drawn from Asian populations, but the generalizability of these findings should be viewed in the context of potential differences in disease prognosis (i.e., patient phenotypes, disease progression, availability of liver transplant, etc.) observed in differing populations. The all-encompassing health state ‘chronic hepatitis C’ (as opposed to health states stratified by fibrosis stage F0–F3) have been utilized due to historical precedent and the availability of data in the literature. As this study focuses on a patient population representative of the general Chinese population and given that health state costs and utility associated with the disaggregated health states do not typically follow a pronounced nonlinear relationship and often observe similar inputs, this simplification is unlikely to significantly impact results [52].
Further, this analysis was restricted to current interferon-based regimens and DUAL as the first approved DAA in China; as further treatments and data (particularly real-world outcomes data) become available, further cost–effectiveness analysis should be undertaken to quantify the impact of these factors. One potential future consideration for the introduction of DUAL is the impact of RAS testing, both in terms of resource use and patient outcomes. Efficacy of DAAs is typically greater in patients without baseline RAS, and there has been much debate over the need to test for such resistance [53]. Costs associated with testing for baseline RAS, and the subsequent impact on SVR, were not explicitly incorporated within the analysis. Such an assumption was made as the cost of baseline RAS testing is not available in the Chinese setting and testing was not incorporated within the trial setting, with subsequent SVR rates reflective of both patients with and without baseline RAS. Further, it is unclear whether RAS testing will be undertaken in the Chinese setting. Given the significant improvement in efficacy associated with DUAL versus current interferon-based regimens and the relatively low expected cost of baseline RAS testing, it is unlikely that cost–effectiveness conclusions would change across subgroups of patients with and without baseline RAS.
DUAL is the first approved DAA treatment for genotype 1b HCV infection in China. It has rates of SVR approaching 100% and offers untreated, suboptimally treated and difficult-to-treat patients a significantly greater opportunity of cure. This is particularly relevant in the Chinese setting, where HCV disease transmission is predominantly driven by injection drug use. These difficult-to-treat patients are associated with poor treatment adherence and outcomes [54]. DUAL offers a simple, convenient and highly tolerable treatment option for these patients, and may offer further benefits not captured within this analysis, such as the potential for reduced disease transmission which would further improve the cost–effectiveness of DUAL in China [28]. The extent to which these benefits are realized in China reflects the heterogeneity in HCV prevalence, treatment uptake, and geographical variation in HCV genotypes; for example, while genotype 1b dominates the northern regions (58.0%), the majority of cases in southern regions are of genotype 2b (36.8%) and genotype 6a/6b (18.4%) [4]. Therefore, while this study offers a robust interpretation of results from a country-wide genotype 1b perspective, in order to fully realize the potential of DUAL and other emerging DAA regimens, the implementation of treatment must be tailored to the particular region of interest in order to optimize clinical outcomes and resource use.
In conclusion, results from this study demonstrate that the introduction of DUAL for the treatment of HCV genotype 1b infection in China is likely to provide significant benefit, in terms of improving quality of life and survival and reducing lifetime medical costs. Hence, DUAL may represent a well-tolerated, clinically efficacious and cost-effective treatment alternative for patients with chronic HCV infection and contribute to the reduction of the chronic HCV disease burden in China.
Future perspective
There is a pre-existing precedent in health economics to focus on the cost–effectiveness of treatments in an average population. The hepatitis C treatment horizon has evolved rapidly over recent years, with a large number of treatments, including DUAL, offering significantly reduced treatment durations and the very realistic achievement of cure, in even the most difficult-to-treat patients. As such, it is anticipated that over the coming years, the focus of cost–effectiveness analyses will be prioritized toward identifying the most appropriate treatment for individual patients, both from a clinical and economic perspective. With onward disease transmission predominantly driven by ‘risky’ behavior in patients with chaotic lifestyles, such prioritization will likely alleviate future clinical and economic burden through successful eradication of disease, and consequent reductions in disease transmission.
•
Hepatitis C virus (HCV) infection is a significant disease burden in China and historical standard of care (SOC) comprises interferon-based regimens only.
•
These regimens offer suboptimal efficacy and safety profiles and a considerable proportion of patients are contraindicated due to intolerance/ineligibility for interferon.
•
Daclatasvir + asunaprevir (DUAL) is the first direct-acting antiviral to receive regulatory approval in China and has demonstrated high efficacy for HCV genotype 1b patients, representing a treatment option for those unsuitable for interferon-based treatments.
•
The clinical and economic impact of the introduction of DUAL as a treatment for genotype 1b HCV infection in China has not previously been assessed.
•
This study aims to address the paucity of relative analyses via a conventional cost–effectiveness evaluation of DUAL versus current interferon-based regimens.
•
Results from this study demonstrate that the introduction of DUAL for the treatment of HCV genotype 1b infection in China is likely to provide significant benefit, in terms of improving quality of life and survival, and reducing lifetime medical costs.
•
DUAL may represent a well-tolerated, clinically efficacious and cost-effective treatment alternative for patients with chronic HCV infection and contribute to the reduction of the chronic HCV disease burden in China.
Author contributions
Each of the listed authors contributed to the development of the manuscript in the form of ( a) substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; and (b) drafting the work or revising it critically for important intellectual content; and (c) final approval of the version to be published; and (d) agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Financial & competing interests disclosure
G Wygant, P Wang and J Yan are employees of Bristol-Myers Squibb Pharmaceuticals Ltd. J Gordon, T Ward and MP Tan are employees of Health Economics and Outcomes Research Ltd, who received funding from Bristol-Myers Squibb for research and writing. W Chen is an employee of Fudan University, China, who received funding from Bristol-Myers Squibb for research. Publication of study results is not contingent on the sponsor’s approval or censorship of the manuscript. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance was utilized in the production of this manuscript. Funding for research and writing of this manuscript was provided by Bristol-Myers Squibb.
References
1.
Chen SL, Morgan TR. The natural history of hepatitis C virus (HCV) infection. Int. J. Med. Sci. 3(2), 47 (2006).
2.
TPOHCV Collaborators TPOH. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: a modelling study. Lancet Gastroenterol. Hepatol. 2(3), 161–176 (2017).
3.
Duan Z, Jia J-D, Hou J et al. Current challenges and the management of chronic hepatitis C in mainland China. J. Clin. Gastroenterol. 48(8), 679 (2014).
4.
Wei L, Lopez-Talavera JC, Rao H et al. Prevalence of HCV and host Il28b genotypes in China. Hepatology 54(4), A563–A564 (2011).
5.
Cui Y, Jia J. Update on epidemiology of hepatitis B and C in China. J. Gastroenterol. Hepatol. 28(S1), 7–10 (2013).
6.
Bennett H, Waser N, Johnston K et al. A review of the burden of hepatitis C virus infection in China, Japan, South Korea and Taiwan. Hepatol. Int. 9(3), 378–390 (2015).
7.
Han Q-Y, Liu Z-W. Current treatment of chronic hepatitis C in China: dilemma and potential problems. World J. Gastroenterol. 22(19), 4615 (2016).
8.
Hézode C, Fontaine H, Dorival C et al. Triple therapy in treatment-experienced patients with HCV-cirrhosis in a multicentre cohort of the French Early Access Programme (ANRS CO20-CUPIC)–NCT01514890. J. Hepatol. 59(3), 434–441 (2013).
9.
Backus L, Belperio P, Shahoumian T, Cheung R, Mole L. Comparative effectiveness of the hepatitis C virus protease inhibitors boceprevir and telaprevir in a large US cohort. Aliment. Pharmacol. Ther. 39(1), 93–103 (2014).
10.
Stedman CA. Current prospects for interferon‐free treatment of hepatitis C in 2012. J. Gastroenterol. Hepatol. 28(1), 38–45 (2013).
11.
Cartwright EJ, Miller L. Novel drugs in the management of difficult-to-treat hepatitis C genotypes. Hepat. Med. 5, 53 (2013).
12.
Welsch C, Jesudian A, Zeuzem S, Jacobson I. New direct-acting antiviral agents for the treatment of hepatitis C virus infection and perspectives. Gut 61(Suppl. 1), i36–i46 (2012).
13.
European Association for Study of Liver. EASL Clinical Practice Guidelines: management of hepatitis C virus infection. J. Hepatol. 60(2), 392 (2014).
14.
Smith-Palmer J, Cerri K, Valentine W. Achieving sustained virologic response in hepatitis C: a systematic review of the clinical, economic and quality of life benefits. BMC Infect. Dis. 15(1), 19 (2015).
15.
Swain MG, Lai MY, Shiffman ML et al. A sustained virologic response is durable in patients with chronic hepatitis C treated with peginterferon alfa-2a and ribavirin. Gastroenterology 139(5), 1593–1601 (2010).
16.
Kumada H, Suzuki Y, Ikeda K et al. Daclatasvir plus asunaprevir for chronic HCV genotype 1b infection. Hepatology 59(6), 2083–2091 (2014).
17.
McPhee F, Suzuki Y, Toyota J et al. Elderly and cirrhotic patients without baseline NS5A polymorphisms in HCV genotype 1b have very high sustained virologic responses to daclatasvir plus asunaprevir. Presented at: 24th Conference of the Asian Pacific Association for the Study of Liver. Istanbul, Turkey, 12–15 March 2014.
18.
Bristol-Myers Squibb. China FDA Approves Country’s First All-Oral Regimen for Chronic Hepatitis C, Daklinza® (daclatasvir) in Combination with Sunvepra® (asunaprevir). (2017). https://investors.bms.com/iframes/press-releases/press-release-details/2017/China-FDA-Approves-Countrys-First-All-Oral-Regimen-for-Chronic-Hepatitis-C-Daklinza-daclatasvir-in-Combination-with-Sunvepra-asunaprevir/default.aspx
19.
McEwan P, Webster S, Ward T et al. Estimating the cost-effectiveness of daclatasvir+ sofosbuvir versus sofosbuvir+ ribavirin for patients with genotype 3 hepatitis C virus. Cost Eff. Resour. Alloc. 15(1), 15 (2017).
20.
Ward T, Webster S, Mishina S et al. Assessing the budget impact and economic outcomes of the introduction of daclatasvir+ asunaprevir and sofosbuvir/ledipasvir for the treatment of chronic hepatitis C virus infection in Japan. Value Health Reg. Issues 12, 1–6 (2017).
21.
Han K-H, Jun B, Kim TH et al. Estimating the cost-effectiveness of one-time screening and treatment for hepatitis C in Korea. PLoS ONE 12(1), e0167770 (2017).
22.
Ward T, Gordon J, Bennett H et al. Tackling the burden of the hepatitis C virus in the UK: characterizing and assessing the clinical and economic consequences. Public Health 141, 42–51 (2016).
23.
McEwan P, Bennett H, Ward T et al. The cost-effectiveness of daclatasvir-based regimens for the treatment of hepatitis C virus genotypes 1 and 4 in the UK. Eur. J. Gastroenterol. Hepatol. 28(2), 173–180 (2016).
24.
Selvapatt N, Ward T, Harrison L et al. The cost impact of outreach testing and treatment for hepatitis C in an urban drug treatment unit. Liver Int. 37(3), 345–353 (2017).
25.
Ward T, Gordon J, Jones B et al. Value of sustained virologic response in patients with Hepatitis C as a function of time to progression of end-stage liver disease. Clin. Drug Invest. 37(1), 61–70 (2017).
26.
Bennett H, Gordon J, Jones B et al. Hepatitis C disease transmission and treatment uptake: impact on the cost-effectiveness of new direct-acting antiviral therapies. Eur. J. Health Econ. 18(8), 1001–1011 (2016).
27.
McEwan P, Selvapatt N, Brown A et al. A clinician’s guide to the cost and health benefits of hepatitis C cure assessed from the individual patient perspective. Eur. J. Gastroenterol. Hepatol. 29(2), 208–214 (2017).
28.
Bennett H, McEwan P, Sugrue D, Kalsekar A, Yuan Y. Assessing the long-term impact of treating hepatitis C virus (HCV)-infected people who inject drugs in the UK and the relationship between treatment uptake and efficacy on future infections. PLoS ONE 10(5), e0125846 (2015).
29.
McEwan P, Kim R, Yuan Y. Assessing the cost utility of response-guided therapy in patients with chronic hepatitis C genotype 1 in the UK using the MONARCH model. App. Health Econ. Health Pol. 11(1), 53–63 (2013).
30.
McEwan P, Ward T, Bennett H et al. Estimating the clinical and economic benefit associated with incremental improvements in sustained virologic response in chronic hepatitis C. PLoS ONE 10(1), e0117334 (2015).
31.
McEwan P, Ward T, Chen C-J et al. Estimating the Incidence and Prevalence of Chronic Hepatitis C Infection in Taiwan Using Back Projection. Value Health Reg. Issues 3(0), 5–11 (2014).
32.
McEwan P, Ward T, Webster S et al. Estimating the long-term clinical and economic outcomes of daclatasvir plus asunaprevir in difficult-to-treat Japanese patients chronically infected with hepatitis C genotype 1b. Value Health Reg. Issues 3, 136–145 (2014).
33.
McEwan P, Ward T, Webster S et al. Estimating the cost‐effectiveness of daclatasvir plus asunaprevir in difficult to treat Japanese patients chronically infected with hepatitis C genotype 1b. Hepatol. Res. 46(5), 423–433 (2016).
34.
McEwan P, Ward T, Yuan Y, Kim R, L'Italien G. The impact of timing and prioritization on the cost-effectiveness of birth cohort testing and treatment for hepatitis C virus in the United States. Hepatology 58(1), 54–64 (2013).
35.
World Health Organization. Life tables by country: China July 2016. http://apps.who.int/gho/data/?theme=main&vid=60340
36.
Rao H, Wei L, Lopez-Talavera JC et al. Distribution and clinical correlates of viral and host genotypes in Chinese patients with chronic hepatitis C virus infection. J. Gastroenterol. Hepatol. 29(3), 545–553 (2014).
37.
ISPOR. China Guidelines for Pharmacoeconomic Evaluations 2011 www.ispor.org/PEguidelines/countrydet.asp?c=28&t=4
38.
Clinical Trials Database: NCT01293279. https://clinicaltrials.gov/ct2/show/NCT01293279
39.
Poynard T, Marcellin P, Lee SS et al. Randomised trial of interferon α2b plus ribavirin for 48 weeks or for 24 weeks versus interferon α2b plus placebo for 48 weeks for treatment of chronic infection with hepatitis C virus. Lancet 352(9138), 1426–1432 (1998).
40.
Wei L, Wang F-S, Zhang M-X et al. Daclatasvir plus asunaprevir in treatment-naive patients with hepatitis C virus genotype 1b infection. World J. Gastroenterol. 24(12), 1361 (2018).
41.
Wei L, Zhang M, Xu M et al. A phase 3, open-label study of daclatasvir plus asunaprevir in Asian patients with chronic hepatitis C virus genotype 1b infection who are ineligible for or intolerant to interferon alfa therapies with or without ribavirin. J. Gastroenterol. Hepatol. 31(11), 1860–1867 (2016).
42.
Kumada H, Suzuki F, Suzuki Y et al. Randomized comparison of daclatasvir + asunaprevir versus telaprevir + peginterferon/ribavirin in Japanese hepatitis C virus patients. J. Gastroenterol. Hepatol. 31(1), 14–22 (2016).
43.
Signorovitch JE, Betts KA, Song Y et al. Comparative efficacy and safety of daclatasvir/asunaprevir versus IFN-based regimens in genotype 1b hepatitis C virus infection. J. Comp. Eff. Res. 4(6), 593–605 (2015).
44.
Bristol-Myers Squibb. BMS data on file (2017).
45.
GBI Health. Roche, Zhengda Tianqing and other three pharmaceutical companies take the initiative to apply for price cuts. http://source.gbihealth.com (2017).
46.
Mao W, Wei L. Cost-effectiveness analysis of peg-interferon alpha-2a plus ribavirin vs. conventional interferon plus ribavirin for the treatment of chronic hepatitis C in China. China J. Pharmaceut. Econ. 1, 6–14 (2012).
47.
Carrasco I, Arias A, Benitez-Gutierrez L et al. Baseline NS5A resistance associated substitutions may impair DAA response in real-world hepatitis C patients. J. Med. Virol. 90(3), 532–536 (2018).
48.
OECD. Exchange rates (indicator) July 2017. https://data.oecd.org/conversion/exchange-rates.htm
49.
OECD. Inflation (CPI) (indicator) July 2017. https://data.oecd.org/price/inflation-cpi.htm
50.
XE Currency Converter. XE: Convert USD/CNY. United States Dollar to China Yuan Renminbi. 14 September 2017. www.xe.com/currencyconverter/convert/?Amount=1&From=USD&To=CNY
51.
The World Bank Data. GDP per capita (current US$). 14 September 2017. https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=CN
52.
Townsend R, McEwan P, Kim R, Yuan Y. Structural frameworks and key model parameters in cost-effectiveness analyses for current and future treatments of chronic hepatitis C. Value Health 14(8), 1068–1077 (2011).
53.
Pérez AB, Chueca N, García F. Resistance testing for the treatment of chronic hepatitis C with direct acting antivirals: when and for how long? Germs 7(1), 40 (2017).
54.
Qin Q, Smith MK, Wang L et al. Hepatitis C virus infection in China: an emerging public health issue. J. Viral Hep. 22(3), 238–244 (2015).
55.
Chen GF, Wei L, Chen J et al. Will Sofosbuvir/Ledipasvir (Harvoni) be cost-effective and affordable for chinese patients infected with hepatitis Cvirus? An economic analysis using real-world data. PLoS ONE 11(6), e0155934 (2016).
56.
Ministry of Health Labour & Welfare. A Study on medical economic assessments of measures for viral liver diseases: Study report. (2013).
57.
Manos MM, Darbinian J, Rubin J et al. The effect of hepatitis C treatment response on medical costs: a longitudinal analysis in an integrated care setting. J. Manag. Care Pharm. 19(6), 438–447 (2013).
58.
Wei et al. Oral presentation LB005. Presented at: 26th Conference of the Asian Pacific Association for the Study of the Liver (APASL). Shanghai, China, 15–19 February 2017.
59.
Rao HY, Li H, Chen H et al. Real world treatment patterns and clinical outcomes of HCV treatment-naive patients in China: an interim analysis from the CCgenos study. J. Gastroenterol. Hepatol. 32(1), 244–252 (2017).
Information & Authors
Information
Published In
Pages: 785 - 795
PubMed: 29860879
Copyright
© 2018 Future Medicine Ltd.
History
Received: 8 January 2018
Accepted: 9 May 2018
Published online: 4 June 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Daclatasvir combined with asunaprevir is a cost-effective and cost-saving treatment for hepatitis C infection in China. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0005
Export citation
Select the citation format you wish to export for this article or chapter.