A decision framework for treating chronic immune thrombocytopenia with thrombopoietin receptor agonists
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Eltrombopag and romiplostim are comparable second-line therapies in chronic immune thrombocytopenia. Treatment decisions are made in different contexts. A framework was created to outline decision pathways for physicians and payers. Materials & methods: The costs of drugs, administration, routine care, bleeding, other adverse events and mortality were included in the year-long calculation of total costs from a US private payer perspective. Treatment parameters and outcome data were obtained from relevant clinical trials. Results: The total cost per year, per patient of eltrombopag was US$51,000 versus US$76,000 for romiplostim. Drug costs and costs associated with bleeding-related events were the main drivers of cost difference. Conclusion: This framework facilitates decision-making in the management of chronic immune thrombocytopenia with eltrombopag and romiplostim.
Immune thrombocytopenia (ITP) is a rare autoimmune disorder characterized by pathological platelet destruction and compromised production, resulting in impaired clotting and poor control of bleeding [1]. Both pediatric and adult patients are affected by ITP, although often the condition resolves naturally in children. An estimated 9.5 people are affected per 100,000, qualifying ITP as an orphan disease (<5 people per 10,000) [2–4].
Chronic ITP (cITP) is a debilitating condition in which patients experience a range of bleeding-related symptoms from mild bruising to potentially fatal intracranial hemorrhage [5,6]. In part due to their high risk of serious bleeding, patients’ quality of life is diminished [7–9]. Bleeding-related events can be unpredictable, and patients may experience anxiety that impinges on their day-to-day functioning. When severe bleeding does occur, patients are necessarily hospitalized, which can further significantly impact quality of life [7,10].
ITP patients with severe bleeding require blood transfusions, in addition to pharmacological therapy, and incur substantial costs [11]. Although hospitalizations and emergency room (ER) visits may be infrequent thus making the incidence of these events low, the treatment of bleeding and bruising is cost intensive and accounts for a large proportion of overall health expenditure in ITP patients. Hospitalizations related to ITP are longer and more expensive than average: US$2574/day over 6.4 days versus US$2091/day over 4.8 days [12]. Reducing the risk of bleeding and resulting events are primary treatment goals in cITP [13]. Therefore, the prevention of bleeding episodes through safe and effective treatments for cITP could result in significant healthcare savings [10]. Further, the success of a particular agent in reducing severe bleeding may be key to its value [10,14].
A typical first-line therapeutic regimen in cITP features corticosteroids and immunoglobulins [6]. These agents have broad immunosuppressive properties and are commonly used to treat autoimmune disorders. However, many cITP patients do not respond to these therapies, or their responses are insufficient [15,16]. First-line therapeutic alternatives include splenectomy and treatment with immune-modulatory agents such as the anti-CD20 monoclonal antibody rituximab [5,17]. More recently, thrombopoietin receptor agonists (TPO-RAs) have entered the therapeutic field of refractory cITP. Two TPO-RAs, eltrombopag (once-daily oral agent) and romiplostim (once-weekly subcutaneous injection) are both indicated for the treatment of adults with cITP who have had an insufficient response to corticosteroids or immunoglobulins. Thus TPO-RAs, which are generally safe and very effective, could potentially be beneficial in deferring nonreversible splenectomy or the use of rituximab as later line options.
TPO-R agonists are the only drugs in ITP appropriately studied with double-blind randomized controlled trials. The 2011 RAISE randomized Phase III study demonstrated that eltrombopag was effective for the management of cITP. Over a period of 6 months, eltrombopag maintained platelet counts, decreased the risk of bleeding and improved quality of life in cITP patients [18]. In two parallel 2008 randomized Phase III trials, romiplostim was also demonstrated to be an effective and well-tolerated treatment for cITP. Most romiplostim-treated patients achieved satisfactory platelet counts and were able to reduce or discontinue concurrent therapies [19]. Eltrombopag and romiplostim are both US FDA-approved and they are similarly indicated for the treatment of cITP patients who have had an insufficient response to corticosteroids, immunoglobulins or splenectomy; their value comparison is therefore pertinent.
The objectives of this article are: to describe the framework for the estimation of costs, including drugs and administration, routine care, adverse events and mortality, and consequences, in terms of the clinical event rate; and to calculate and compare the estimated total costs per patient on approved TPO-RAs, eltrombopag and romiplostim, in the USA.
Materials & methods
To understand the costs of treating ITP with TPO-RAs, a framework was developed incorporating clinical events and their associated costs. While clinical trial data supporting the use of TPO-RAs are robust, the total costs of the treatment pathways have yet to be fully evaluated. Furthermore, the overall costs of TPO-RA therapy have not been compared for different agents. This analysis yielded a cost estimator that provides an economic support framework for the treatment of cITP using the TPO-RAs eltrombopag and romiplostim.
Essential characteristics of the analysis
An Excel-based model was generated in which a user can supply data to best describe their unique drug utilization scenario. This analysis was performed to estimate the total costs of treatment for cITP with TPO-RAs from a US payer perspective. All costs are reported in 2017 US dollars and were adjusted for inflation where necessary, based on the inflation rate reported by the US Bureau of Labor Statistics Consumer Price Index [20]. The 12-month time horizon was chosen to reflect the typical budgetary interval for payers for hospitals and pharmacies.
Efficacy data for eltrombopag were obtained from the pivotal 24-week Phase III RAISE study. In RAISE, adults (n = 302) with cITP who had received prior therapy were enrolled. Patients were randomly allocated (in a 2:1 ratio) treatment with local standard of care plus 50 mg eltrombopag or matching placebo once daily for 6 months. For romiplostim, efficacy data were extracted from two Phase III trials reported by Kuter et al. (2008) [19,21]. The parallel, multicenter, double-blind, placebo-controlled trials were conducted in adult splenectomized (n = 63) and nonsplenectomized (n = 62) patients. Patients were randomized to receive romiplostim or placebo over a 24-week period, with dosages adjusted according to weekly platelet counts.
Overall, these studies that formed the basis of FDA approvals for the respective compounds were determined to be sufficiently comparable and indicative of clinical practice in the USA. Therefore, efficacy values from an indirect treatment comparison (ITC) that adjusted the romiplostim efficacy data to match that of eltrombopag (described elsewhere [22]) were used. Briefly, frequentist ITC was employed and 95% confidence intervals were calculated. Romiplostim results were pooled using random effects model (Mantel–Haenszel method), which generated odds ratios for romiplostim versus placebo, as placebo was the common ITC ‘anchor’ between the eltrombopag and romiplostim trials.
The total costs of each regimen were calculated by summing the costs of the drugs, administration (if nonoral), routine care, bleeding-related episodes, other adverse events and mortality over 1 year. The duration of therapy and the prevalence of adverse events and bleeding were dictated by the relevant clinical trials. Routine care utilization values were obtained from a federated network of electronic medical records, which provided therapy-specific values [23]. The conceptual framework is presented in Figure 1.
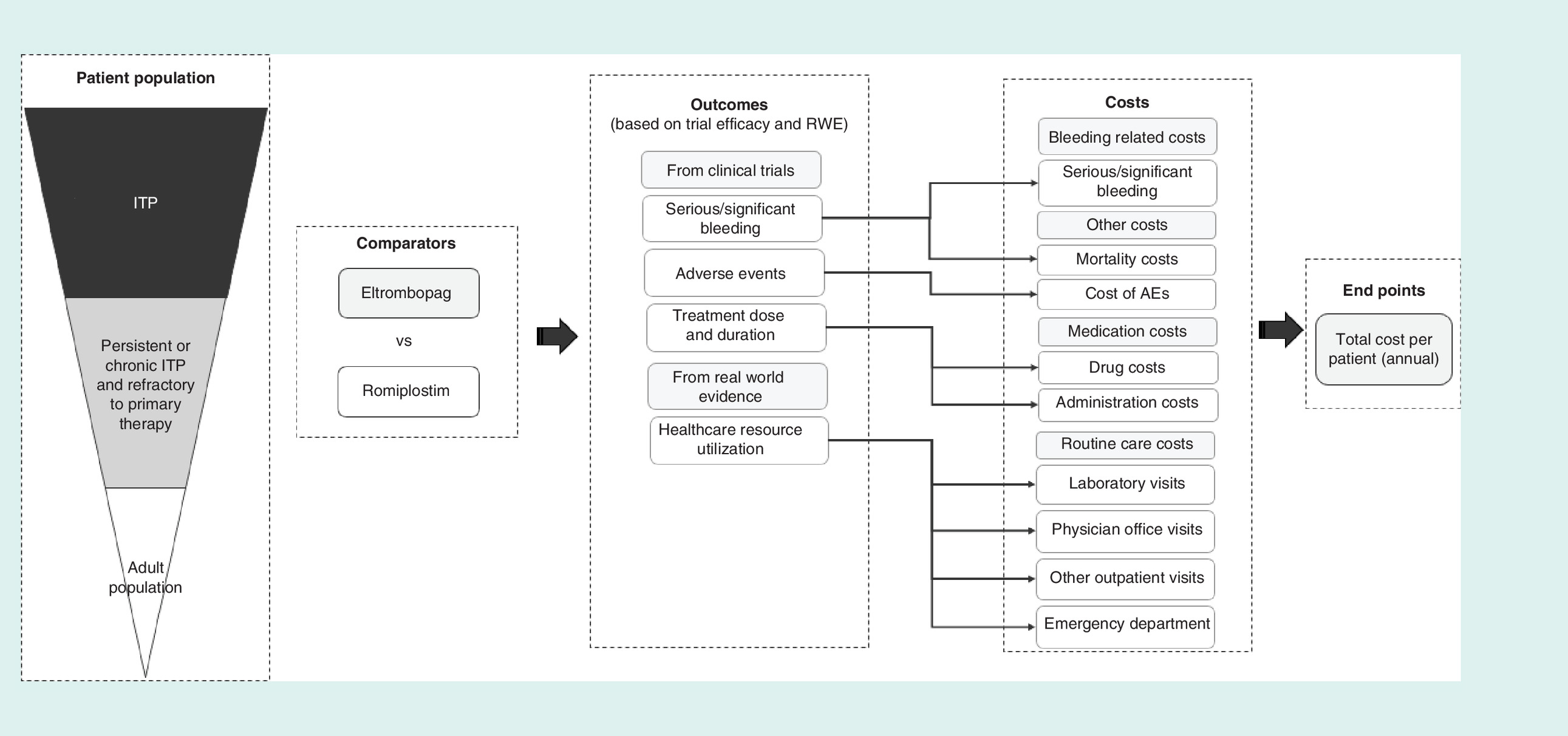
Figure 1. Conceptual model framework.
AE: Adverse event; ITP: Immune thrombocytopenia; RWE: Real-world evidence.
Drugs & administration
The cost-per-dose for drugs and administration was multiplied by number of doses required over the treatment’s duration. Average doses were based on the therapies’ respective health technology assessments, where 51.30 mg/day of eltrombopag and 307.49 μg/day of romiplostim were assumed to be the average doses received by patients [24,25]. Patients were assumed to adhere to all therapies over the entire duration of therapy with no skipped doses, dose escalation or de-escalation in order to conservatively estimate the greatest possible treatment costs. Based on their respective within-trial treatment durations, eltrombopag treatment and romiplostim treatment lasted 5.69 and 5.38 months, respectively. Following treatment discontinuation, it was assumed that patients did not receive secondary therapy for the remainder of the year.
The costs of eltrombopag and romiplostim were obtained from AnalySource (2017), which provided up-to-date pricing information based on the First Databank Drug Pricing Database [26]. A 30-unit (unit strength of 50) package of eltrombopag was US$8254.94 while a 4-unit package (unit strength 250) of romiplostim was US$6492.00. As eltrombopag is orally administered, its administration costs were assumed to be US$0. For the romiplostim, the cost of subcutaneous administration was also included and was estimated to be US$75.19 per weekly injection (per the Centers for Medicare and Medicaid Services Fee Schedule, 2017) [27].
The total number of doses for the duration of therapy was calculated for each drug using data from the respective clinical trials [18,19]. To account for wastage and provide conservative drug cost estimates, derived monthly doses were rounded up to the nearest pack sizes. For therapies administered by syringe, it was assumed no vial sharing took place based on the common practice in US medical care [28]. Per month, an average of 1.04 packages of eltrombopag (based on a mean trial dose of 51.30 mg/day with a package size of thirty 50 mg tabs) and 2.00 packages of romiplostim (based on a mean trial dose of 4.14 mg/kg, or 307.49 mg/day, with a package size of four 250 mg infusions) were administered after accounting for vial wastage.
Routine medical care
Routine care utilization was based on data obtained from a database of electronic medical records [23,29–32]. The database contained information (inpatient and outpatient services and procedures, diagnoses, prescriptions and labs) on over 84 million patient-lives from 29 US hospital institutions at the time of analysis. For the model, the search included patients diagnosed with primary ITP who had been treated with eltrombopag or romiplostim as second-line therapy. First, all patients with ITP were identified via ICD-10 codes (D69.3, D69.4 and D69.6) and then patients were matched on conditions implying secondary ITP to generate comparable, mutually exclusive cohorts with patients of primary ITP. The cohorts were matched on:
•
Prior steroid treatment
•
History of HBV/HCV/HIV
•
Malignancy
•
Severe aplastic anemia, myelodysplastic syndrome and myelofibrosis
•
Splenectomy
Costs were based on inflation-adjusted estimates from Healthcare Utilization Project (HCUPnet) for hospitalization costs and Saleh et al. (2009) for all other routine care costs [11,33]. The rates of routine care utilization were collected over 12 months following eltrombopag or romiplostim initiation. Unit costs were applied to the rates of routine care utilization to calculate the costs per patient per year for each resource use.
Bleeding-related events
Severe bleeding, ≥grade 3, is a medical emergency associated with high costs. As defined by the WHO, grade 3 bleeding describes a gross loss of blood requiring a transfusion of red blood cells while the grade 4 designation includes life-threatening and fatal bleeding [34,35]. Reducing the rates of bleeding events is the ultimate goal of treating ITP. This, in addition to the subsequent reduction in hospitalizations, would reduce the overall economic burden of ITP and as such, the prevention of severe bleeding was an important focus of this analysis [10].
Based on the respective clinical trials, while ITC eltrombopag had a severe bleeding rate of 2.20%, romiplostim had a severe bleeding rate of 3.68%. Monthly-adjusted rates of severe bleeding events in each trial were multiplied by the inflation-adjusted literature cost of a bleeding-related event (US$44,590.08) to account for costs specifically related to bleeding in this analysis [10,18,19].
Other adverse events
Adverse events corresponded to the drug labels, and included any adverse event with a prevalence >10% reported for either eltrombopag or romiplostim. Prevalence was based on clinical trial data and it is presented in Supplementary Table 1. In the RAISE trial (eltrombopag), 3.28% (38 out of 1160 total) adverse events reported were serious events. Based on this value, it was assumed that for both eltrombopag and romiplostim, 3.28% of adverse events would require inpatient care, for which inpatient care costs were applied in the analysis [18]. The remaining 96.72% of adverse events were assumed to require outpatient care, where separate outpatient costs were applied. Costs for inpatient and outpatient treatment of each adverse event, based on inflation-adjusted HCUPnet (2014) estimates for average ambulatory and inpatient event-specific costs, respectively, were proportionally summed [33]. To obtain cost per adverse event for each therapy, the adverse event prevalence for the treatment duration was multiplied by the average adverse event cost. Detailed adverse event cost calculations are presented in the Supplemental Information, Supplementary Table 1.
Mortality
For ITP, mortality rate of all hospital discharges in the USA (2.39%; from HCUPnet 2013 [33]) was multiplied by the cITP relative mortality ratio (1.5; based on the estimate by Danese et al. (2009) [12]) to estimate the mortality rate of ITP discharges in the USA (3.59%). To obtain the treatment-specific mortality rate, the yearly rate of severe bleeding events for each comparator was multiplied by this standard rate. The average yearly cost of a mortality event for each treatment was estimated by multiplying the cost of inpatient treatment for ITP (Lin et al. [2017]) by the derived treatment-specific yearly mortality rates [10].
Results
Drugs & administration
Total drug and administration costs associated with eltrombopag or romiplostim are presented in Table 1. Values incorporated during the calculation of these totals are also summarized.
Routine medical care
Based on the calculations described earlier, final routine care utilization and cost values are presented in Table 2.
| Resources | Mean resource use (yearly) | Unit cost (including inflation) | Final cost for 12 months | ||
|---|---|---|---|---|---|
| EPAG | ROMI | EPAG | ROMI | ||
| Office visits | 0.28 | 0.26 | 103.51 | 28.66 | 27.24 |
| Emergency department visits | 0.15 | 0.13 | 345.03 | 53.06 | 45.41 |
| Diagnostic tests† | 0.26 | 0.45 | 35.83 | 9.32 | 16.12 |
| Total | 91.04 | 88.77 | |||
Utilization source: electronic medical records (2017).
†
All diagnostic radiology tests included.
EPAG: Eltrombopag; ROMI: Romiplostim.
Bleeding-related events
Eltrombopag was associated with a 0.39% severe bleeding rate per month, amounting to monthly costs of US$172.35 (US$2068 per year). A severe bleeding rate of 0.68% per month was calculated for romiplostim at costs of US$305.03 per month (US$3660 per year).
Other adverse events
Calculated as described in detail in the Methods and Supplemental Information, Table 3 presents the prevalence and average cost of each adverse event.
| Adverse events | Eltrombopag | Romiplostim | ||
|---|---|---|---|---|
| Prevalence in trial (%) | Average cost (per patient, per year) | Prevalence in trial (%) | Average cost (per patient, per year) | |
| Arthralgia | 7 | 28.03 | 26 | 104.13 |
| Confusion | 1 | 3.95 | 25 | 98.75 |
| Diarrhea | 13 | 46.85 | 17 | 61.27 |
| Epistaxis | 5 | 22.83 | 32 | 146.11 |
| Fatigue | 10 | 31.24 | 33 | 103.09 |
| Headache | 30 | 90.22 | 35 | 105.26 |
| Infusion reactions | 0 | 0.00 | 0 | 0.00 |
| Pain in extremities | 7 | 25.48 | 13 | 47.33 |
| Petechiae | 0 | 0.00 | 17 | 57.62 |
| Upper respiratory tract infection | 10 | 43.98 | 17 | 74.76 |
Mortality
The average mortality rates for eltrombopag and romiplostim were 0.17 and 0.29% per year, respectively, resulting in an average mortality costs per patient treated with eltrombopag at US$91.85 and US$162.56 per patient treated with romiplostim.
Cost summary
Annual costs associated with eltrombopag and romiplostim treatment are presented in Table 4 & Figure 2. In each category and overall, the costs of romiplostim treatment were greater. The total cost per year, per patient of eltrombopag treatment was US$51,000 as compared with US$76,000 for romiplostim treatment. The pharmacy costs were 1.46-fold higher for romiplostim compared with eltrombopag (US$71,587 vs US$48,908, respectively), which was the main cost difference driver between the comparators. Bleeding-related costs were also lower in the eltrombopag-treated group compared with romiplostim-treated patients, where eltrombopag had US$2068 worth of costs, compared with US$3660 for romiplostim (a 1.77-fold difference). Both routine care and mortality costs were similar between comparators but were also numerically higher in the romiplostim-treated group compared with eltrombopag.
| Events and costs | Eltrombopag | Romiplostim |
|---|---|---|
| Event rates | ||
| Severe bleeding | 4.64% | 8.21% |
| Mortality | 0.17% | 0.29% |
| Costs (US$) | ||
| Drugs and administration | 48,908 | 71,587 |
| Routine care | 91.04 | 88.77 |
| Adverse events | 292.58 | 798.31 |
| Bleeding | 2068.24 | 3660.35 |
| Mortality | 91.85 | 162.56 |
| Total | 51,451.82 | 76,297.48 |
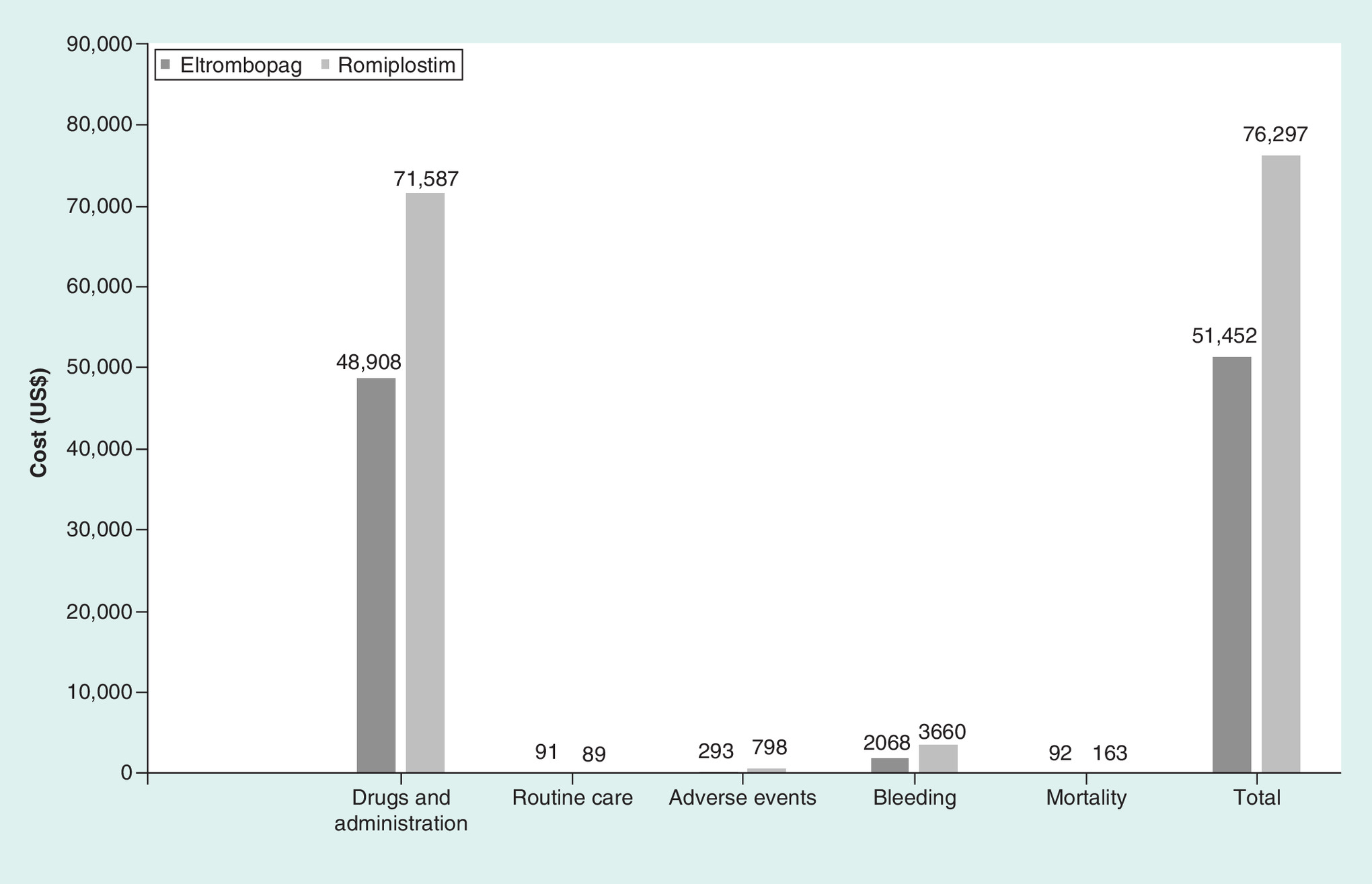
Figure 2. Total cost of treatment regimens.
Per patient, per year, US$.
Sensitivity analyses were performed to assess the impact of varied model assumptions. Namely, vial sharing for intravenous (iv.) therapies and use of naive (non-ITC adjusted severe bleeding rates) were included. The results are presented in Table 5.
| Events and costs | Base case | Vial sharing included | Naive severe bleeding trial data used | |||
|---|---|---|---|---|---|---|
| Eltrombopag | Romiplostim | Eltrombopag | Romiplostim | Eltrombopag | Romiplostim | |
| Event rates | ||||||
| Severe bleeding | 4.64% | 8.21% | 4.64% | 8.21% | 4.64% | 15.85% |
| Mortality | 0.17% | 0.29% | 0.17% | 0.29% | 0.17% | 0.57% |
| Costs (US$) | ||||||
| Drugs and administration | 48,908 | 71,587 | 48,908 | 48,440 | 48,908 | 71,587 |
| Routine care | 91.04 | 88.77 | 91.04 | 88.77 | 91.04 | 88.77 |
| Adverse events | 292.58 | 798.31 | 292.58 | 798.31 | 292.58 | 798.31 |
| Bleeding | 2068 | 3660 | 2068 | 3660 | 2068 | 7064 |
| Mortality | 91.85 | 162.56 | 91.85 | 162.56 | 91.85 | 313.72 |
| Total | 51,452 | 76,297 | 51,452 | 53,150 | 51,452 | 79,852 |
Discussion
This analysis serves as a framework for predicting the economic impact of approved TPO-RA therapies for cITP. We evaluated the key expenses associated with treating cITP, including a detailed breakdown of adverse events and their prevalence based on clinical trial data. Reducing the risk of bleeding is the primary treatment goal in cITP and, as such, costs related to bleeding were considered individually. Estimating the costs of each treatment per patient, per year demonstrated the lower costs of eltrombopag therapy: US$51,000 as compared with US$76,000 with romiplostim therapy. Pharmacy (drug and administration) costs and bleeding-related costs contributed most of the financial burden. In presenting costs along with clinical evidence, this comparison framework could help to define value and guide real-world decision-making in cITP for physicians and payers alike.
In each treatment scenario, routine care, adverse event and mortality costs were comparable while drug costs composed most of the total expenses. Eltrombopag medication costs were lower, and its oral administration imposed no additional costs. Extrapolating clinical trial data, eltrombopag was associated with reduced monthly rates of severe bleeding and therefore provides a solution to one of the most expensive aspects of ITP care [10,18]. Based on Health Technology Assessment (HTA) assessments, eltrombopag and romiplostim are considered equivalent in general, although a recent analysis agreed that eltrombopag may be associated with fewer bleeding-related events compared with romiplostim [22,37].
Some inherent limitations impact modeling studies such as this one. The model used clinical trial data, which reflected the expected clinical usage of the experimental agents. Though optimized in the trials, factors such as therapy duration and dosing schedules may vary in a real-world setting. In addition, the model assumes patient adherence to therapy over the course of the median duration of therapy, and dose modifications and interruptions resulting from toxicities are not included. However, using the median duration of therapy implicitly helps account for any potential impact of discontinuation. The mean dose assumed here for the two drugs was based on the respective technology appraisals/assessment reports, which may deviate from received doses in actuality (e.g., dose received by romiplostim patients may vary between 1 and 10 μg per kg/day). Thus, the drug-related costs may be skewed lower or higher, depending on the received dose.
Additionally, other than direct treatment effects, the higher bleeding rates seen in romiplostim may in part be due to the fact romiplostim required slow titration (particularly during early trials), which may result in increased bleeding risk, although there is no robust data on this to the knowledge of the authors at the time of writing. In relation to administration-borne outcomes, romiplostim has recently been approved for home-administration, which may reduce overall administration costs for this therapy (though exploratory analyses found the cost of romiplostim to still be higher than eltrombopag, even if administration costs were US$0 for subcutaneous therapy). Furthermore, certain general assumptions were necessary to ensure the simplicity and comprehensibility of the model. Clinical trial results were assumed to predict outcomes in real world practice. Additionally, secondary (post-eltrombopag or -romiplostim) therapies were not included even though cITP patients commonly receive salvage therapies if other treatments fall short. Salvage therapy typically consists of inexpensive steroids and, therefore, the associated costs are expected to be minimal and the inclusion of such costs would not be expected to have a notable impact on the results [5].
Conclusion
The present study represents the most comprehensive, transparent and detailed estimator of the annual cost burden of cITP in patients treated with recommended TPO-R agonists to date. It provides the framework, or analytical decision-making pathway, for further analyses and comparisons relevant to real world practice.
•
Immune thrombocytopenia (ITP) is an immune-mediated bleeding disorder characterized by low platelet count and impaired clotting; many patients do not achieve a sufficient response with first-line therapies and still experience bleeding episodes that impact their quality of life.
•
A framework was developed to compare the estimated total yearly costs per ITP patient treated with second-line thrombopoietin receptor agonists eltrombopag and romiplostim.
•
The costs of medications and their administration, costs resulting from bleeding episodes and other adverse events, costs associated with routine care and costs related to mortality were included in the calculation of total pharmacy and medical costs from a US private payer perspective.
•
The total cost per year, per patient of romiplostim treatment was US$76,000 as compared with US$51,000 for eltrombopag treatment.
•
The pharmacy costs were 1.46-fold higher for romiplostim compared with eltrombopag (US$71,600 vs US$48,900, respectively), which was the main driver for the cost difference between the comparators.
•
Bleeding related costs also impacted the results: US$3660 worth of costs were estimated for romiplostim, compared with US$2070 for eltrombopag (a 1.77-fold difference).
•
Routine care and mortality costs were similar between comparators, but were higher in the romiplostim-treated group.
•
This framework allows for the comprehensive estimation of the costs and consequences of managing ITP using US FDA-approved thrombopoietin receptor agonists, which are indicated for patients with limited therapeutic options, and provides a basis for further budget impact and cost–effectiveness analyses.
Author’s contributions
M Dolph made substantial contributions to the conception and design, analyzed and interpreted the data and critically revised the article. J Hearnden and CS Kwon acquired, analyzed and interpreted data, and contributed to the drafting and revision of the manuscript. A Roy, A Forsythe, M Bhor, G Tremblay and A Briggs made substantial contributions to conception and design, and critically revised the article for important intellectual content. All authors agree to be accountable for all aspects of the work.
Financial & competing interests disclosure
This study was sponsored by Novartis. A Roy and M Bhor are employees of Novartis. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (supplementaryinformation.docx)
- Download
- 36.12 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Rodeghiero F, Stasi R, Gernsheimer T et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood 113(11), 2386–2393 (2009).
2.
Segal JB, Powe NR. Prevalence of immune thrombocytopenia: analyses of administrative data. J. Thromb. Haemost. 4(11), 2377–2383 (2006).
3.
Landgren O, Gridley G, Fears TR, Caporaso N. Immune thrombocytopenic purpura does not exhibit a disparity in prevalence between African American and white veterans. Blood 108(3), 1111–1112 (2006).
4.
Medicines for rare diseases. European Medicines Agency, 2015. www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/orphans/2009/11/human_orphan_000191.jsp&mid=WC0b01ac058001d12b
5.
Provan D, Newland AC. Current management of primary immune thrombocytopenia. Adv. Ther. 32(10), 875–887 (2015).
6.
Stevens W, Koene H, Zwaginga JJ, Vreugdenhil G. Chronic idiopathic thrombocytopenic purpura: present strategy, guidelines and new insights. Neth. J. Med. 64(10), 356–363 (2006).
7.
Mathias SD, Gao SK, Miller KL et al. Impact of chronic immune thrombocytopenic purpura (ITP) on health-related quality of life: a conceptual model starting with the patient perspective. Health Qual. Life Outcomes 6, 13 (2008).
8.
Zhou Z, Yang L, Chen Z et al. Health-related quality of life measured by the Short Form 36 in immune thrombocytopenic purpura: a cross-sectional survey in China. Eur. J. Haematol. 78(6), 518–523 (2007).
9.
Michel M. Immune thrombocytopenic purpura: epidemiology and implications for patients. Eur. J. Haematol. Suppl. (71), 3–7 (2009)
10.
Lin J, Zhang X, Li X et al. Cost of bleeding-related episodes in adult patients with primary immune thrombocytopenia: a population-based retrospective cohort study of administrative claims data for commercial payers in the United States. Clin. Ther. 39(3), 603.e601–609.e601 (2017).
•• Reports on the high costs of hospitalization due to bleeding-related events in immune thrombocytopenia. Bleeding costs in this analysis were based on this study by Lin et al.
11.
Saleh MN, Fisher M, Grotzinger KM. Analysis of the impact and burden of illness of adult chronic ITP in the US. Curr. Med. Res. Opin. 25(12), 2961–2969 (2009).
• Estimates by Saleh et al. and Danese et al. informed routine care and mortality costs in this analysis.
12.
Danese MD, Lindquist K, Gleeson M, Deuson R, Mikhael J. Cost and mortality associated with hospitalizations in patients with immune thrombocytopenic purpura. Am. J. Hematol. 84(10), 631–635 (2009).
• Estimates by Saleh et al. and Danese et al. informed routine care and mortality costs in this analysis.
13.
Provan D, Newland AC. Guidelines for immune thrombocytopenia. N. Engl. J. Med. 364(6), 580–581 (2011).
14.
Li X, Sharma A, Zhang X et al. Cost per treatment success of thrombopoietin receptor agonists vs “watch and rescue” strategy for treating adult non-splenectomized patients with chronic immune thrombocytopenia: a US payer perspective. Blood 126(23), 4461–4461 (2015).
15.
Portielje JE, Westendorp RG, Kluin-Nelemans HC, Brand A. Morbidity and mortality in adults with idiopathic thrombocytopenic purpura. Blood 97(9), 2549–2554 (2001).
16.
George JN. Management of patients with refractory immune thrombocytopenic purpura. J. Thromb. Haemost. 4(8), 1664–1672 (2006).
17.
Moulis G, Sailler L, Sommet A, Lapeyre-Mestre M, Derumeaux H, Adoue D. Rituximab versus splenectomy in persistent or chronic adult primary immune thrombocytopenia: an adjusted comparison of mortality and morbidity. Am. J. Hematol. 89(1), 41–46 (2014).
18.
Cheng G, Saleh MN, Marcher C et al. Eltrombopag for management of chronic immune thrombocytopenia (RAISE): a 6-month, randomised, Phase 3 study. Lancet 377(9763), 393–402 (2011).
•• Cheng et al. and Kuter et al. provided data on the efficacy of eltrombopag and romiplostim, respectively.
19.
Kuter DJ, Bussel JB, Lyons RM et al. Efficacy of romiplostim in patients with chronic immune thrombocytopenic purpura: a double-blind randomised controlled trial. Lancet 371(9610), 395–403 (2008).
•• Cheng et al. and Kuter et al. provided data on the efficacy of eltrombopag and romiplostim, respectively.
20.
Consumer Price Index. United States Department of Labor: Bureau of Labor Statistics, 2017. www.bls.gov/cpi/data.htm
21.
Kuter DJ, Rummel M, Boccia R et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N. Engl. J. Med. 363(20), 1889–1899 (2010).
22.
Tremblay G DM, Bhor M, Elliott B. Cost consequence model comparing eltrombopag and romiplostim for adult patients with previously-treated chronic immune thrombocytopenia. Presented at: ISPOR 22nd Annual International Meeting. Boston, MA, USA, 20 May 2017.
23.
Electronic Medical Records. Federated network of large hospital institutions across the US. 2017.
24.
Cooper K, Matcham J, Helme K, Akehurst R. Update on romiplostim and eltrombopag indirect comparison. Int. J. Technol. Assess. Health Care 30(1), 129–130 (2014).
25.
Eltrombopag for treating chronic immune (idiopathic) thrombocytopenic purpura. In: Technology Appraisal Guidance [TA293]. National Institute for Health and Care Excellence (NICE), (2013). www.nice.org.uk/guidance/ta293
26.
First Databank Drug Pricing Database In: Analysource: Premier Drug Pricing Services. Analysource, Syracuse, NY, USA (2017). www.analysource.com/
27.
Centers for Medicare and Medicaid Services Fee Schedule, 2017. www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/
28.
Bach PB, Conti RM, Muller RJ, Schnorr GC, Saltz LB. Overspending driven by oversized single dose vials of cancer drugs. BMJ 352, i788 (2016).
29.
Forsythe A, Bhor M, Roy A, Portella MSO, Kwon C, Tremblay G. Economic burden of immune thrombocytopenia (ITP) in patients receiving eltrombopag (EPAG) and romiplostim (ROMI): real world evidence from 26 US institutions. Presented at: ISPOR 20th Annual European Congress. Glasgow, Scotland, 8 November 2017.
30.
Forsythe A, Roy A, Bhor M, Portella MSO. Bleeding-related episodes (BRE) in patients with immune thrombocytopenia (ITP) receiving eltrombopag (EPAG) or romiplostim (ROMI): real world evidence from 26 US institutions. Presented at: ISPOR 20th Annual European Congress. Glasgow, Scotland, 8 November 2017.
31.
Kwon C, Forsythe A, Roy A, Bhor M, Portella MSO, Tremblay G. Health care resource use (HCRU) due to bleeding related episodes (BRE) in patients with immune thrombocytopenic purpura (ITP) receiving eltrombopag (EPAG), romiplostim (ROMI), or rituximab (RITUX): real world evidence (RWE) from 27 US institutions. Presented at: ISPOR 20th Annual European Congress. Glasgow, Scotland, 8 November 2017.
32.
Forsythe A, Roy A, Bhor M et al. Benefit–risk comparison in patients with immune thrombocytopenia (ITP) receiving eltrombopag or romiplostim: real world evidence (RWE) from 26 hospital institutions. Presented at: ASH 59th Annual Meeting and Exposition. Atlanta, GA, USA, 6 December 2017.
33.
HCUPnet Healthcare Cost and Utilization Project. AHRQ Agency for Healthcare Research (2017). https://hcupnet.ahrq.gov/#setup
34.
Josephson CD, Granger S, Assmann SF et al. Bleeding risks are higher in children versus adults given prophylactic platelet transfusions for treatment-induced hypoproliferative thrombocytopenia. Blood 120(4), 748–760 (2012).
35.
WHO Handbook for Reporting the Results of Cancer Treatment. WHO, Geneva, Switzerland (1979). http://apps.who.int/iris/handle/10665/37200
36.
CHMP ASSESSMENT REPORT FOR Nplate, International Nonproprietary Name: Romiplostim. In: Procedure No. EMEA/H/C/942. European Medicines Agency Evaluation of Medicines for Human Use, London, UK (2015) www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/000942/WC500039475.pdf
37.
Allen R, Bryden P, Grotzinger KM, Stapelkamp C, Woods B. Cost–effectiveness of eltrombopag versus romiplostim for the treatment of chronic immune thrombocytopenia in England and Wales. Value Health 19(5), 614–622 (2016).
Information & Authors
Information
Published In
Pages: 775 - 784
PubMed: 29848048
Copyright
© 2018 Future Medicine Ltd.
History
Received: 19 April 2018
Accepted: 16 May 2018
Published online: 31 May 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A decision framework for treating chronic immune thrombocytopenia with thrombopoietin receptor agonists. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0034
Export citation
Select the citation format you wish to export for this article or chapter.