Comparative effectiveness of a bilayered living cellular construct and an acellular fetal bovine collagen dressing in the treatment of venous leg ulcers
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the effectiveness of bilayered living cellular construct (BLCC) and an acellular fetal bovine collagen dressing (FBCD) for the treatment of venous leg ulcers. Methods: Data from WoundExpert® (Net Health, PA, USA) was used to analyze 1021 refractory venous leg ulcers treated at 177 facilities. Results: Kaplan–Meier analyses showed that BLCC (893 wounds) was superior to FBCD (128 wounds), p = 0.01 for: wound closure by weeks 12 (31 vs 25%), 24 (55 vs 43%) and 36 (68 vs 53%); reduction in time to wound closure of 37%, (19 vs 30 weeks); and improvement in the probability of healing by 45%. Conclusion: BLC versus FBCD showed significant differences in both time to and frequency of healing suggesting that BLCC may provide significant cost savings compared with FBCD.
Venous leg ulcers (VLUs), also referred to as venous stasis ulcers, are the most common type of chronic leg wound. These often painful wounds represent the majority of leg ulcers [1–3]. VLUs have a prevalence estimated at 1% of adults [4,5], with rates even higher among the elderly (1.7% prevalence, annually) [6]. The annual direct financial cost to US payers for the treatment of chronic VLUs has been estimated to be US$15 billion [7].
The standard treatment for VLUs is compression therapy. However, with standard care alone, research has shown that up to 75% of patients fail to achieve healing with the use of standard compression therapy [8]. Up to 50% of VLUs remain unhealed at 6 months, 20% at 2 years and approximately 8% at 5 years [9]. Advanced treatment options, such as skin substitutes, have been demonstrated to show safety and effectiveness as adjunctive therapies to accelerate the wound healing process in nonhealing VLUs [10,11]. Treatment algorithms for initiating advanced therapies in VLUs have not been definitively established. Such therapies, however, may be appropriate to use as part of the initial treatment regimen in patients with poor prognostic indicators such as an ulcer size ≥10 cm2 and an ulcer that has been present ≥12 months [12]. Data also suggest that advanced therapies should be considered in VLUs that have not reduced in surface area by at least 40% following 4 weeks of good standard wound care with compression therapy [13].
A bilayered living cellular construct (BLCC; Apligraf, Organogenesis, Inc., MA, USA) is at present the only product that has undergone premarket review and is approved by the US FDA for the treatment of VLUs (premarket approval (PMA)-approved Class III medical device). BLCC is comprised of human neonatal keratinocytes and fibroblasts in an extracellular matrix (bovine collagen and other extracellular matrix proteins) and has been in clinical use for the treatment of VLUs since 1998. In order to gain FDA approval for the treatment of VLUs, BLCC was evaluated in a pivotal randomized controlled trial (RCT) with a sample size of 275 patients that showed, when used in conjunction with compression therapy, BLCC significantly increased the percentage of patients healed by 6 months and reduced the median time to complete wound closure when compared with an active control (standard compression therapy) [10].
Fetal bovine collagen dressing (FBCD; Primatrix; Integra, NJ, USA) has been cleared by FDA as a 510(k) Class II device for the management of VLUs and other skin wounds with the exception of third degree burns. FBCD is an animal-derived acellular collagen dressing that has been processed and treated to remove cellular elements, lipids, carbohydrates and noncollagenous proteins, resulting in a scaffold with physiological amounts of collagen but without viable cells. Retrospective comparison of diabetic foot ulcer and venous stasis ulcer healing outcomes (n = 40) between FBCD and BLCC showed that both treatments were highly effective; however, the FBCD-treated wounds healed faster than patients treated with BLCC [14]. FBCD in the published retrospective analysis [14] was demonstrated to be successfully incorporated into standard of care therapy as a primary wound covering for the treatment of VLUs.
BLCC has not been compared with FBCD in comparative effectiveness research (CER) studies in real-world treatment settings. Effective treatment, established in CER studies, is the extent to which an intervention produces its intended effect in routine care conditions (real-world situations). RCTs with positive results, on the other hand, provide evidence of efficacious treatment in controlled, highly constrained conditions that are optimal for obtaining favorable results [15]. Thus, it is important to determine if efficacy reported from the results of RCTs can be translated to everyday, routine practice settings (effectiveness) to support evidence-based practice.
The purpose of this study was to investigate the comparative effectiveness of BLCC to FBCD for the treatment of VLUs in real-world settings using data over a 2-year period from a large wound care-specific electronic medical record (EMR) database (WoundExpert®, Net Health, PA, USA) that is utilized by approximately 20,000 physicians in over 1000 wound care facilities across the USA.
Methods
Study design
This study is a retrospective analysis to compare the effectiveness of BLCC and FBCD for the treatment of VLUs using de-identified EMRs from wound care facilities across the USA in a 2-year period. The primary analyses were median time to and frequency of wound closure evaluated up to 36 months. Wound areas (cm2) were calculated from wound measurements of length and width. The final visit denoting VLU closure was not always recorded; thus, wound closure was defined as an ulcer achieving an area between 0 and 0.25 cm2.
Patients
Patients eligible for inclusion were those documented as receiving at least one treatment of either BLCC or FBCD on a partial or full thickness venous ulcer with the location coded as ankle, lower leg, shin, pretibial or calf. Included baseline wound areas were 1–40 cm2 with ulcer duration of longer than 1 month prior to first treatment with BLCC or FBCS. To ensure that analyses were restricted to refractory VLUs, no ulcers were included that achieved >40% closure within the 4 weeks prior to first treatment with BLCC or FBCD. Wounds without baseline or follow-up area measurements were excluded as well as those where the date of BLCC or FBCD treatment was unknown. Wounds were also excluded if they received skin substitute treatments (Apligraf, Primatrix, Dermagraft, Epifix, Theraskin, Grafix, Graftjacket) on or within 28 days of the first treatment with BLCC or FBCD. Censoring occurred for nonhealed wounds at their last visit with an area measurement. Patients were also censored at the visit where the alternate product was applied (either BLCC or FBCD). Wounds treated with the same product >183 days after the prior application were censored at the visit where the subsequent application occurred. Other concurrent treatments such as hyperbaric oxygen or negative pressure wound therapy were allowed as this was a real-world study of wound care clinical practice not governed by a standardized, single protocol as in RCTs.
Data collection
Data were obtained from the WoundExpert EMR, which was de-identified under the terms and conditions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Net Health provided all treatment records for any patient receiving at least one application of BLCC or FBCD from January 2015 to January 2017 from 177 centers with contracted agreements for the transfer of de-identified data for research purposes. Treatment records included patient baseline demographics including age (years, ≤89 per HIPAA), sex, race, wound size and duration, and wound-specific information recorded at each visit including area measurements and treatments.
Statistical analysis
Descriptive data are expressed as mean (standard deviation) and median for continuous variables and n (%) for categorical variables. The level of p < 0.05 was established for the purpose of defining statistical significance. Baseline characteristics were reported as observational data for both continuous and categorical variables. Missing covariates were imputed with the mean value of the treatment group. The primary analyses comparing incidence of and median time to wound closure were determined by Kaplan–Meier analysis with a two-tailed log-rank test. The last observation was carried forward for missing data. Cox proportional hazards regression analysis was used to estimate the percentage of VLUs with closure at weeks 12, 24 and 36. Median time to wound closure was determined by the Cox proportional hazards regression survivor function. The frequency of wounds closed at week 12, 24 and 36, and median time to wound closure, hazard ratio with 95% CI and p-value were estimated from the Cox model with terms for treatment, baseline wound area, baseline wound duration, baseline wound depth, sex, BMI and patient age at first treatment.
Results
All VLUs that received their first treatment with BLCC or FBCD from January 2015 and January 2017 at all participating Net Health centers were eligible for inclusion. A total of 927 patients with 1021 refractory wounds met the eligibility requirements for inclusion in the analysis. 893 wounds (805 patients) were treated with BLCC, and 128 wounds (122 patients) were treated with FBCD.
Baseline patient characteristics are shown in Table 1, and baseline wound and treatment characteristics are shown in Table 2. Treatment groups were similar with respect to age, sex, BMI and number of wounds per patient. The median age was 70 years old in both groups. Women represented a little more than half of the population in the BLCC group while men represented greater than half of the population in the FBCD group, and the median BMI was comparable between groups (31.5 kg/m2 in the BLCC group and 30.6 kg/m2 in the FBCD group). Groups were comparable for the percentage of patients presenting with a single wound (65.7 vs 71.3% for BLCC and FBCD, respectively) as well as patients presenting with multiple wounds at baseline (34.3 vs 28.7% for BLCC and FBCD, respectively). Though some nominal differences were observed, the BLCC and FBCD treated wounds were similar for baseline wound area, depth and duration (Table 2). At the first treatment application, the mean wound area was 10.1 cm2 in the BLCC group and 10.6 cm2 in the FBCD group. The mean wound durations in the BLCC and the FBCD groups were similar, both being >1 year (12.6 and 17.3 months in the BLCC and FBCD treatment groups, respectively).
| Patient characteristic | BLCC (n = 805) | FBCD (n = 122) | p-value† |
|---|---|---|---|
| Age (years), n: – Mean ± SD – Median | 803 69.0 ± 14.2 70.0 | 122 68.3 ± 14.9 70.0 | 0.80 |
| Sex, n (%): – Male – Female | 798 378 (47.4) 420 (52.6) | 120 65 (54.2) 55 (45.8) | 0.17 |
| BMI (kg/m2), n: – Mean ± SD – Median | 633 33.5 ± 10.7 31.5 | 95 32.9 ± 9.6 30.6 | 0.86 |
| Number of wounds per patient, n (%): – Single wound – Multiple wounds | 805 529 (65.7) 276 (34.3) | 122 87 (71.3) 35 (28.7) | 0.22 |
| Number of wounds per patient: – Mean ± SD – Median | 1.62 ± 1.13 1.0 | 1.48 ± 0.90 1.0 | 0.21 |
†
For BMI, the p-value is from the Wilcoxon rank-sum test, testing for a difference in distribution between treatments. For other categorical variables, the p-value is from a two-tailed Fisher’s exact test, testing for a difference in proportions between treatments. For continuous variables, the p-value is from a two-tailed, two-sample t-test, testing for a difference in means between treatments.
BLCC: Bilayered living cellular construct (Apligraf); FBCD: Fetal bovine collagen dressing (Primatrix); SD: Standard deviation.
| Wound and treatment characteristics | BLCC (n = 893) | FBCD (n = 128) | p-value† |
|---|---|---|---|
| Wound area (cm2), n: – Mean ± SD – Median | 893 10.1 ± 9.1 7.0 | 128 10.6 ± 9.2 7.4 | 0.22 |
| Wound duration (months)‡, n: – Mean ± SD – Median | 740 12.6 ± 32.4 4.8 | 100 17.3 ± 31.7 5.9 | 0.03 |
| Wound depth (mm), n: – Mean ± SD – Median | 883 1.8 ± 1.5 2.0 | 128 2.0 ± 1.1 2.0 | 0.01 |
| Number of treatment applications:– Mean ± SD – Median | 893 2.8 ± 1.6 2.0 | 128 2.1 ± 1.7 2.0 | <0.01 |
| Interval between application (days), n: – Mean ± SD – Median | 658 20.1 ± 22.8 14.0 | 68 25.2 ± 19.7 21.0 | <0.01 |
| Single/multiple applications, n (% patients): – Single – Multiple | 893 235 (26.3) 658 (73.7) | 128 60 (46.9) 68 (53.1) | <0.01 |
| Number of debridements at or within 28 days prior to day 0§, n (% patients): – 0 – 1 – 2 – 3 – 4 or more | 893 192 (21.5) 141 (15.8) 137 (15.3) 132 (14.8) 291 (32.5) | 128 25 (19.5) 17 (13.3) 18 (14.1) 25 (19.5) 43 (33.6) | 0.65 |
| Other treatments, n (% patients): – HBO2 – Day -28 to <day 0 – Day 0 to last follow-up visit – NPWT – Day -28 to <day 0 – Day 0 to last follow-up visit | 11 (1.4) 17 (2.1) 25 (3.1) 21 (2.6) | 2 (1.6) 6 (4.9) 5 (4.1) 7 (5.7) | 0.68 0.11 0.58 0.08 |
†
For categorical variables, the p-value is from a two-tailed Fisher’s exact test testing for a difference in proportions between treatments. For continuous variables, the p-value is from a two-tailed, two sample t-test, testing for a difference in means between treatments.
‡
Wound duration was reported in days and converted to months (30 days = 1 month).
§
Day 0 defined as first application visit.
BLCC: Bilayered living cellular construct (Apligraf); FBCD: Fetal bovine collagen dressing (Primatrix); HBO2: Hyperbaric oxygen; NPWT: Negative pressure wound therapy; SD: Standard deviation.
Treatment characteristics are also shown in Table 2. The median number of treatment applications received was comparable for BLCC and FBCD with a mean of 2.8 ± 1.6 for BLCC and 2.1 ± 1.6 for FBCD. FBCD was used as a single application 46.9% of the time. Multiple applications were used on 53.1% of FBCD-treated ulcers. The percentage of patients treated with a single application with BLCC was 26.3%, and 73.7% had multiple applications. For patients receiving multiple applications, the median interval between applications was longer with FBCD compared with BLCC (21.0 vs 14 days). Groups were similar with regard to the number of debridements at or within 28 days prior to or post the initial treatment application. Treatment with hyperbaric oxygen or negative pressure wound therapy prior to or concurrent with BLCC or FBCD treatment rarely occurred (<6% of wounds treated) and comparable between groups (Table 2).
After adjusting for treatment, treatment characteristics, baseline wound area, baseline wound duration, baseline wound depth, sex, BMI and patient age at first treatment application, Cox proportional hazards analysis showed that BLCC treatment significantly improved the median time to VLU wound closure by 37%, achieving the end point 11 weeks sooner than FBCD-treated patients (19 weeks for BLCC vs 30 weeks for FBCD; p = 0.01) (Figure 1). The estimated incidence of wound closure for BLCC compared with FBCD was significantly improved by week 12 (31.0 vs 25.0%), week 24 (55.0 vs 43%) and week 36 (68 vs 53%); p = 0.01 (Figure 2). BLCC treatment increased the probability of wound closure compared with FBCD by 45% showing a hazard ratio (HR) of 1.45 (95% CI: 1.08, 1.94), p = 0.01.
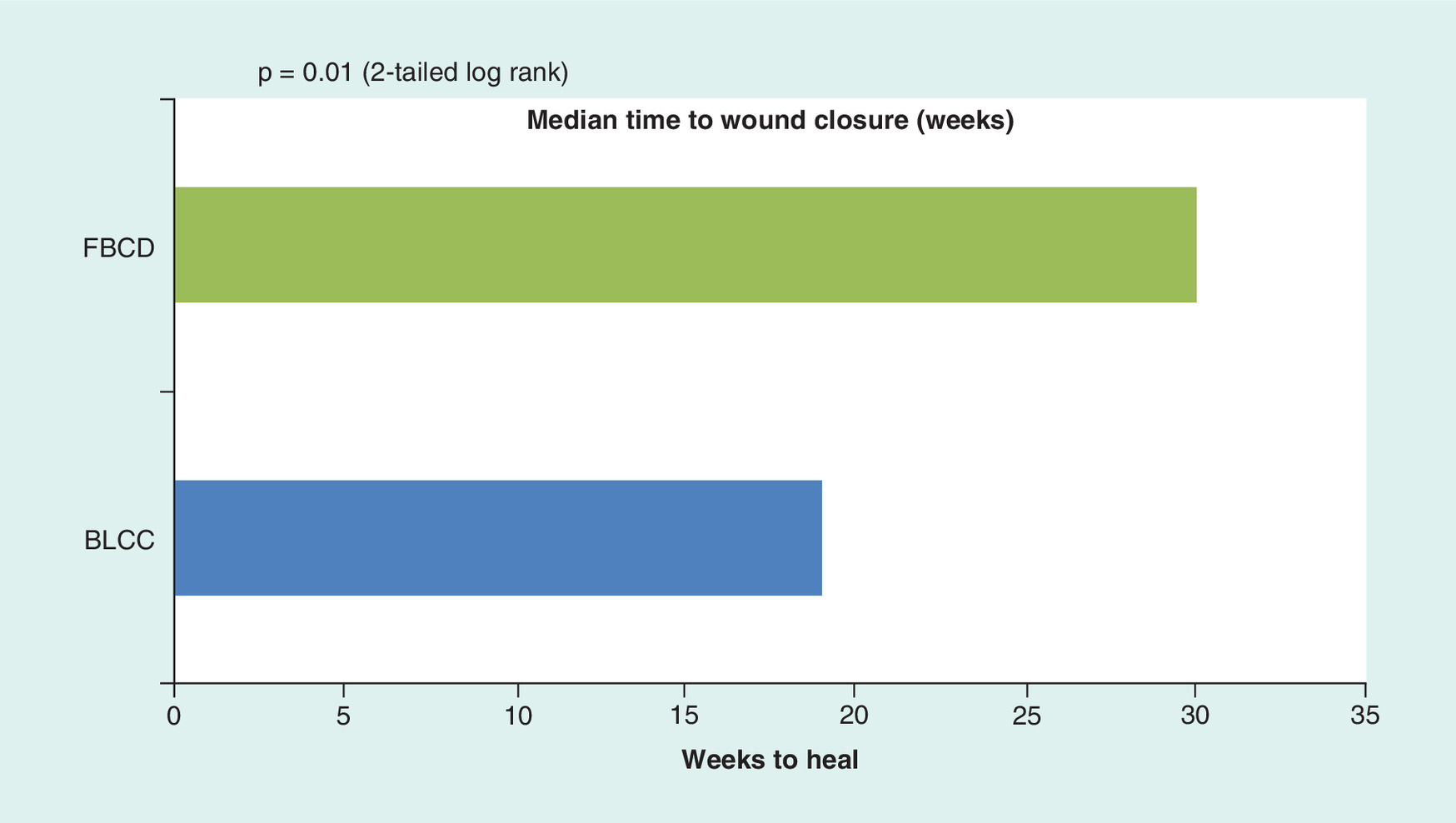
Figure 1. Median time to wound closure.
BLCC: Bilayered living cellular construct (Apligraf); FBCD: Fetal bovine collagen dressing (Primatrix).
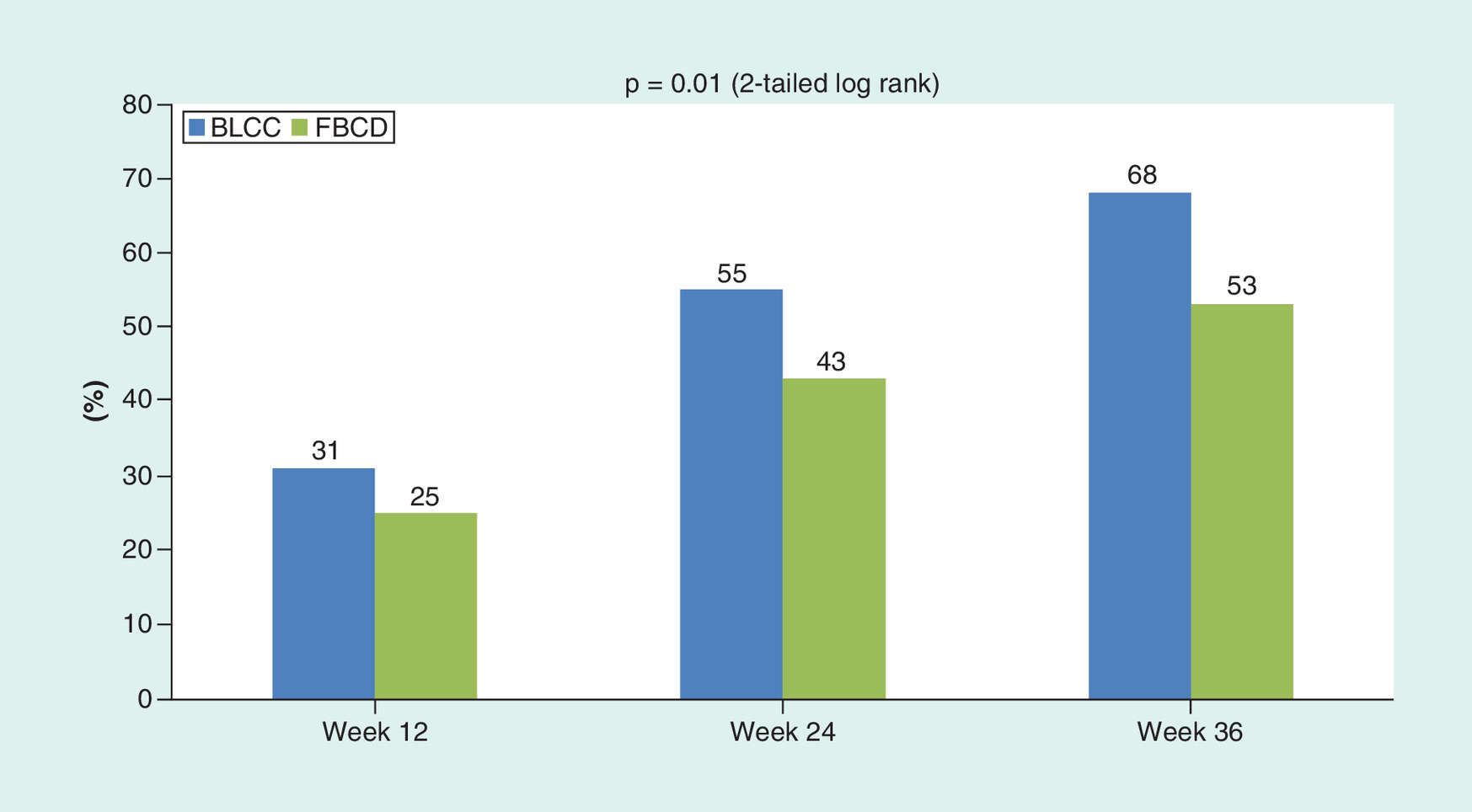
Figure 2. Percent wounds achieving wound closure.
BLCC: Bilayered living cellular construct (Apligraf); FBCD: Fetal bovine collagen dressing (Primatrix).
Discussion
This is the first comparative effectiveness study to evaluate BLCC and FDCD for the treatment of VLUs. The ulcers in the patient population evaluated were refractory or nonhealing with routine care. Ulcers in both study groups showed a duration of >1 year, failed to achieve ≥40% wound closure in 4 weeks prior to the first treatment application, and had a mean size of >10 cm2 at baseline, all negative risk factors for healing [11,13,16,17]. That the wounds in this analysis were required to have closed by <40% prior to treatment with either BLCC or FBCD is consistent with common, current clinical practice where the use of this prognostic indicator has become widely adopted to identify patients who may benefit from advanced wound care therapy, including skin substitutes. In this retrospective CER study analysis, BLCC demonstrated wound closure at significantly higher frequencies and in significantly less time compared with FBCD. BLCC increased the probability of wound closure by 45% over the 36 weeks of observation.
In order to address the potential impact of sex, age and BMI as individual patient characteristics on comparative clinical outcomes of BLCC and FBCD, three additional Cox analyses were performed. When treatment was adjusted for: sex as a categorical variable, HR = 1.42 (95% CI: 1.06, 1.91); p = 0.02; age as a continuous variable, HR = 1.44 (95% CI: 1.07, 1.93); p = 0.02; and BMI as a continuous variable, HR = 1.42 (95% CI: 1.06, 1.91); p = 0.02. These data are consistent with the outcomes reported in our primary Cox analysis when terms for treatment, treatment characteristics, baseline wound area, baseline wound duration, baseline wound depth, sex, BMI and patient age at first treatment are all included (HR = 1.45 [95% CI: 1.08, 1.94]; p = 0.01). These data would appear to indicate that the comparative effectiveness outcomes of BLCC and FBCD are minimally affected by sex, age and BMI when these patient characteristics are considered in isolation from multivariate wound and treatment characteristics.
Efficacy reflects the degree to which an intervention produces the expected result under the carefully controlled conditions of a clinical research protocol. RCTs provide the best method for establishing efficacy and are considered to have high ‘internal validity’ because of randomization, careful selection of participants and standardized treatment practices proscribed by the clinical protocol [18,19]. The conditions of an RCT are intended to maximize the probability of showing differences between treatment groups if they exist. RCTs act as the basis of FDA premarket review (New Drug Applications [NDAs], Biologics License Applications [BLAs], and PMAs) of clinical evidence for the approval of drugs, biologics and Class III devices. For guideline therapy, RCTs are generally considered level 1 evidence and the ‘gold standard’ in determining if a product can actually work. However, RCTs have limitations. The generalizability or ‘external validity’ of data generated may be problematic if RCT data alone are interpreted in the absence of real-world data [20]. The strict criteria for patient inclusion (which may exclude ‘higher risk’ patients), rigorous monitoring and adherence to treatment protocols may create an environment not reflective of clinical practice conditions in the community at large, and patients treated in RCTs may not truly represent typical patient populations treated where these products are utilized [21]. CER studies do not narrowly select patient populations but rather reflect interventions as typically used in practice without forced standardization. CER analyses may therefore be interpreted as more widely applicable and complementary to RCTs since CERs evaluate treatments in ordinary settings and in broader populations [22].
In effectiveness studies, performance is often reduced in less homogeneous populations treated outside of expert clinical research centers and in a less rigorous fashion. Thus, it is important to determine if efficacy can be translated to routine practice settings. Although strict comparisons between RCTs and the results presented here cannot be made because of differences in study design and patient populations, we found the incidence of complete wound closure for the 146 BLCC-treated patients in the pivotal RCT was 63% at week 24. These data correlated well with the wound closure rates of 55 and 68% at weeks 24 and 36, respectively in this CER analysis [10]. To date, there has not been a prospective RCT reporting the results of FBCD versus standard of care compression therapy in VLUs to allow for a comparison with the outcomes demonstrated in this CER study.
VLUs have been estimated to affect approximately 2.5 million patients in the USA [23,24]. The economic burden of VLUs on the US healthcare system in an analysis of 81,000 chronic VLU patients [7,25] was determined to be approximately US$18 billion annually in direct costs. Medicare VLU patients receiving skin substitutes analyzed over the same time period showed total healthcare costs were US$537 per week higher for patients who were still incurring VLU-related costs (‘nonhealed’ ulcers) compared with those no longer incurring VLU-related costs (‘healed’ ulcers). Of this amount, US$377 per week were for selected services considered directly related to VLU treatment [7]. Therefore the 11-week difference in median time to wound closure (19 weeks for BLCC vs 30 weeks for FBCD) in the current analysis could result in estimated cost savings of between US$4100 and US$5900 per patient based on the differences in median time of having an open ulcer. This estimate likely understates the overall economic burden of nonhealing VLUs as it does not include 20% of the total costs of care not covered by Medicare. Analyses of two deidentified insurance claims databases showed that VLU treatment costs were directly proportional to the frequency of and time to healing. Medicare patients with nonhealed VLUs had 78% more hospitalization days, 50% more emergency department visits, 27% more outpatient office visits and 60% more days of home healthcare [7]. Important indirect costs not factored in must also be taken into consideration. These indirect costs include those associated with quality of life and lost productivity because of patient and caregiver missed days of work. Further specifics on relative costs would require a database with more detailed information than was available for this analysis.
We recognize that this study design analyzing real-world data, like all retrospective analyses, introduces ‘noise’ into the study environment that typical prospective RCTs minimize. A limitation of this study is that EMR databases often are not developed for research purposes, and variability in recording practices of individual clinics exists. Even with the WoundExpert EMR data collection system, uniform data reporting is not monitored. Although certain fields within the WoundExpert EMR were reliably and consistently completed (such as wound measurements), information regarding the type of secondary dressings was found to be less consistently reported and often entered as ‘free text’ making reliable analyses problematic. Completion of some baseline patient information fields such as medical history, prior surgical interventions or concomitant medications, varied across centers. Additionally, the reporting of all safety-related outcomes, adverse events or ulcer recurrences were not possible as this information was not uniformly captured. Finally, given the lack of randomization, there is a possibility of bias in selection of patients for BLCC or FBCD at the centers involved in patient care. However, given the large number of wounds and centers providing information for the analysis, it is less likely that a uniform bias was present that affected the study results. Additionally, Cox analyses used to determine wound closure outcomes adjusted for multiple covariates and corrected for any imbalances between groups that might have arisen based on entry criteria.
There were also many advantages that the WoundExpert afforded. Because of the large sample sizes of the two treatment groups in the Net Health database, we were able to investigate outcomes in refractory, ‘hard-to-heal’ VLUs and excluded wounds that had reduced in size >40% in the 4 weeks prior to the first application of investigational treatment. It is notable that percent reduction in wound size of <40% at 4 weeks from baseline has been reported as the strongest negative predictor of nonhealing in VLUs (i.e., identifies VLUs that will not achieve wound closure in a timely fashion) [13]. This 4-week prognostic milestone has been selectively adopted across the field of wound care to identify patients who may benefit most from intervention with advanced therapies; however, few previous studies have employed criteria that apply this measurement for inclusion. These results may provide important data to help guide treatment decisions for patients with recalcitrant wounds.
Conclusion
These real-world data showed that BLCC, compared with FBCD, significantly improved the probability, speed, and the incidence of wound closure in VLUs.
•
This is the first comparative effectiveness research study that compares the clinical outcomes of a bilayer living cellular construct (BLCC) and an acellular fetal bovine collagen dressing (FBCD) for the treatment of venous leg ulcers (VLUs) in a real-world setting.
•
Treatment with BLCC significantly improves the incidence and speed of VLU wound closure compared with FBCD.
•
The effectiveness of BLCC in these analyses was supportive of the efficacy results from the pivotal BLCC trial in VLUs.
•
BLCC showed a 45% greater probability of wound closure when compared with FBCD.
•
BLCC demonstrated accelerated time to wound closure of 37%, an 11-week improvement compared with FBCD.
•
The incidence of wound closure was superior with BLCC versus FBCD at all time points in the study.
•
Improvements in the probability, speed and the incidence of wound closure in VLUs treated with BLCC suggest a greater clinical benefit as well as a potential cost savings benefit.
•
Electronic healthcare databases when used in Comparative Effectiveness Research studies offer the benefit of providing robust sources of data in large study populations over long observation periods.
Financial & competing interests disclosure
This study was funded by Organogenesis, Inc. ML Sabolinski, serves as managing member of Sabolinski LLC., Franklin, MA, USA. ML Sabolinski serves as a consultant for Organogenesis Inc., AOBiome, Neumedicines and Allergan. G Gibbons, serves as a consultant and speaker for Organogenesis, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
De-identified patient data released to Organogenesis, Inc. were consistent with the terms and conditions of Net Health’s client contracts and the requirements of the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Net Health was not involved in the analysis, interpretation or reporting of the data.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Valencia IC, Falabella A, Kirsner RS, Eaglstein WH. Chronic venous insufficiency and venous leg ulceration. J. Am. Acad. Dermatol. 44(3), 401–421 (2001).
2.
Sen CK, Gordillo GM, Roy S et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 17(6), 763–771 (2009).
3.
Fife C, Walker D, Thomson B, Carter M. Limitations of daily living activities in patients with venous stasis ulcers undergoing compression bandaging: problems with the concept of self-bandaging. Wounds 19(10), 255–257 (2007).
4.
Hankin CS, Knispel J, Lopes M, Bronstone A, Maus E. Clinical and cost efficacy of advanced wound care matrices for venous ulcers. J. Manag. Care Pharm. 18(5), 375–384 (2012).
5.
Fowkes FG, Evans CJ, Lee AJ. Prevalence and risk factors of chronic venous insufficiency. Angiology 52(Suppl. 1), S5–S15 (2001).
6.
Margolis DJ, Bilker W, Santanna J, Baumgarten M. Venous leg ulcer: incidence and prevalence in the elderly. J. Am. Acad. Dermatol. 46(3), 381–386 (2002).
7.
Rice JB, Desai U, Cummings AK, Birnbaum HG, Skornicki M, Parsons N. Medical, drug, and work-loss costs of venous leg ulcers. Value Heal. 16(3), A73 (2013).
8.
O’Meara S, Cullum NA, Nelson EA. Compression for venous leg ulcers. Cochrane Database Syst. Rev. 1, CD000265 (2009).
9.
Kurz X, Kahn SR, Abenhaim L et al. Chronic venous disorders of the leg: epidemiology, outcomes, diagnosis and management. Summary of an evidence-based report of the VEINES task force. Venous insufficiency epidemiologic and economic studies. Int. Angiol. 18(2), 83–102 (1999).
10.
Falanga V, Margolis D, Alvarez O et al. Rapid healing of venous ulcers and lack of clinical rejection with an allogeneic cultured human skin equivalent. Arch. Dermatol. 134(3), 293–300 (1998).
•• The landmark paper of the randomized controlled trial of bilayer living cellular construct for the treatment of venous leg ulcers when compared with an active control (compression therapy) that reports safety and efficacy.
11.
Falanga V, Sabolinski M. A bilayered living skin construct (APLIGRAF®) accelerates complete closure of hard-to-heal venous ulcers. Wound Repair Regen. 7(4), 201–207 (1999).
12.
Falanga V, Sabolinski ML. Prognostic factors for healing of venous and diabetic ulcers. Wounds 12(5 Suppl. A), A42–A46 (2000).
13.
Gelfand JM, Hoffstad O, Margolis DJ. Surrogate endpoints for the treatment of venous leg ulcers. J. Invest. Dermatol. 119(6), 1420–1425 (2002).
14.
Karr JC. Retrospective comparison of diabetic foot ulcer and venous stasis ulcer healing outcome between a dermal repair scaffold (PriMatrix) and a bilayered living cell therapy (Apligraf). Adv. Skin Wound Care 24(3), 119–125 (2011).
15.
Toh S, García Rodríguez LA, Hernán MA. Analyzing partially missing confounder information in comparative effectiveness and safety research of therapeutics. Pharmacoepidemiol. Drug Saf. 21(Suppl. 2), 13–20 (2012).
16.
Kerstein MD, Brem H, Giovino KB, Sabolinski M. Development of a severity scale for evaluating the need for Graftskin in nonhealing venous ulcers. Adv. Ski. Wound Care 15(2), 66–71 (2002).
17.
Margolis DJ, Allen-Taylor L, Hoffstad O, Berlin JA. The accuracy of venous leg ulcer prognostic models in a wound care system. Wound Repair Regen. 12(2), 163–168 (2004).
18.
Eaglstein WH, Kirsner RS. Expectations for comparative effectiveness and efficacy research. JAMA Dermatol. 149(1), 18 (2013).
• An important, general publication in the field of Comparative Effectiveness Research that explains the strengths and potential limitations inherent in Comparative Effectiveness Research studies.
19.
van Staa T-P, Leufkens HG, Zhang B, Smeeth L. A comparison of cost effectiveness using data from randomized trials or actual clinical practice: selective Cox-2 inhibitors as an example. PLoS Med. 6(12), e1000194 (2009).
20.
Concato J. When to randomize, or ‘evidence-based medicine needs medicine-based evidence’. Pharmacoepidemiol. Drug Saf. 21(Suppl. 2), 6–12 (2012).
21.
Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. National Academies Press, DC, USA (2009).
22.
Gandjour A. Prioritizing comparative effectiveness research: are drug and implementation trials equally worth funding? Pharmacoeconomics 29(7), 555–561 (2011).
23.
Gillespie DL, Kistner B et al. Writing Group III of the Pacific Vascular Symposium 6. Venous ulcer diagnosis, treatment, and prevention of recurrences. J. Vasc. Surg. 52(5 Suppl.), S8–S14 (2010).
24.
González-Consuegra RV, Verdú J. Quality of life in people with venous leg ulcers: an integrative review. J. Adv. Nurs. 67(5), 926–944 (2011).
25.
Rice JB, Desai U, Cummings AKG, Birnbaum HG, Skornicki M, Parsons N. Burden of venous leg ulcers in the United States. J. Med. Econ. 17(5), 347–356 (2014).
•• Provides a detailed analysis of the costs of treating open venous leg ulcers.
Information & Authors
Information
Published In
Pages: 797 - 805
PubMed: 29809059
Copyright
© 2018 Michael L Sabolinski.
History
Received: 6 April 2018
Accepted: 10 May 2018
Published online: 29 May 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of a bilayered living cellular construct and an acellular fetal bovine collagen dressing in the treatment of venous leg ulcers. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0031
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yunyao Bo, Zehui Zhou, Ruitong Dong, Li Sun, Chenxi Li, Lin Zhang, Yuan Yan, Silk fibroin nanofibers-GelMA hydrogel composite loaded with embryonic fibroblasts: A strategy for enhanced wound healing, Colloids and Surfaces B: Biointerfaces, 10.1016/j.colsurfb.2026.115581, 263, (115581), (2026).
- Oscar M Alvarez, Tad Archambault, Michael L Sabolinski, Comparative effectiveness study of a bilayer cellular construct and dehydrated human amnion/chorion membrane in the treatment of pressure injuries, Journal of Wound Care, 10.12968/jowc.2024.0070, 34, 8, (616-622), (2025).
- Shawn M Cazzell, Joseph Caporusso, Dean Vayser, R Daniel Davis, Oscar M Alvarez, Michael L Sabolinski, Dehydrated Amnion Chorion Membrane versus standard of care for diabetic foot ulcers: a randomised controlled trial, Journal of Wound Care, 10.12968/jowc.2024.0139, 33, Sup7, (S4-S14), (2024).
- Ali Esmaeili, Masoud Soleimani, Maryam Rouhani, Ghasem Noorkhajavi, Seyed Mohsen Aghaei-Zarch, Behnam Hasannejad-Asl, Saeid Bagheri-Mohammadi, Maryam Ebrahimi, Saeed Heidari Keshel, Xenograft-based skin substitutes: A critical review, Journal of Drug Delivery Science and Technology, 10.1016/j.jddst.2024.105613, 95, (105613), (2024).
- Nathaniel R. Primous, Peter T. Elvin, Kathleen V. Carter, Hagner L. Andrade, Javier La Fontaine, Naohiro Shibuya, Claudia C. Biguetti, Bioengineered Skin for Diabetic Foot Ulcers: A Scoping Review, Journal of Clinical Medicine, 10.3390/jcm13051221, 13, 5, (1221), (2024).
- Michael L Sabolinski, Tad Archambault, Real-world data analysis of bilayered living cellular construct and fetal bovine collagen dressing treatment for pressure injuries: a comparative effectiveness study, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0109, 13, 4, (2024).
- Maryam Kaviani, Bita Geramizadeh, Basic Aspects of Skin Tissue Engineering: Cells, Biomaterials, Scaffold Fabrication Techniques, and Signaling Factors, Journal of Medical and Biological Engineering, 10.1007/s40846-023-00822-y, 43, 5, (508-521), (2023).
- Prarthana Patil, Katherine A. Russo, Joshua T. McCune, Alonda C. Pollins, Matthew A. Cottam, Bryan R. Dollinger, Carlisle R. DeJulius, Mukesh K. Gupta, Richard D’Arcy, Juan M. Colazo, Fang Yu, Mariah G. Bezold, John R. Martin, Nancy L. Cardwell, Jeffrey M. Davidson, Callie M. Thompson, Adrian Barbul, Alyssa H. Hasty, Scott A. Guelcher, Craig L. Duvall, Reactive oxygen species–degradable polythioketal urethane foam dressings to promote porcine skin wound repair, Science Translational Medicine, 10.1126/scitranslmed.abm6586, 14, 641, (2022).
- Aubrey E Woodroof, Gail K Naughton, Fiona M Wood, Robert J Christy, Shanmugasundaram Natesan, William L Hickerson, Path to ‘One and Done’, Journal of Wound Care, 10.12968/jowc.2021.30.10.794, 30, 10, (794-802), (2021).
- Aseel Bin Sawad, Fatema Turkistani, Treatment of venous leg ulcers using bilayered living cellular construct, Journal of Comparative Effectiveness Research, 10.2217/cer-2020-0076, 9, 13, (907-918), (2020).