Treatment of venous leg ulcers using bilayered living cellular construct
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: Venous leg ulcers (VLUs) present a significant economic burden on the US healthcare system and payers (US$14.9 billion). Aim: To evaluate the quality of life (QoL) of patients with VLUs; to analyze the limitations of standard of care (SOC) for VLUs; and to explain how using bilayered living cellular construct (BLCC) with SOC for treatment of VLUs can help heal more VLUs faster (than using SOC alone) as well as help improve QoL and help reduce the burden on the US healthcare system and payers. Materials & methods: This is a review study. The search was conducted in February 2020 by way of electronic databases to find relevant articles that provided information related to QoL of patients with VLUs, limitations of SOC for VLUs and economic analyses of using BLCC for treatment of VLUs. Results: VLUs impact patients’ physical, functional and psychological status and reduce QoL. A total 75% of VLU patients who used SOC alone failed to achieve healing in a timely fashion, which led to increased healthcare costs and healthcare resource utilization. Although the upfront cost is high, the greater effectiveness of BLCC offsets the added cost of the product during the time period of the studies. Therefore, BLCC helps to improve the QoL of VLU patients. As an example, for every 100 VLU patients in a healthcare plan, the use of BLCC can create cost savings of US$1,349,829.51. Conclusion: Payers’ coverage of BLCC results in reduction of the overall medical cost for treating VLU patients.
Venous leg ulcers (VLUs) are the most common type of chronic lower extremity ulcer and accounts for 80% of these cases [1]. In the US, VLUs affect approximately 2.5 million patients per year [2]. Of the seven million people in the US with venous insufficiency about a million develop VLUs [3]. As the population of the elderly increases, the prevalence of VLUs can be expected to rise [4]. VLUs are more common among women than men [5–8]. The main risk factors of VLUs are increased age, female gender, obesity, previous leg injuries, deep venous thrombosis and phlebitis [3,5–8]. VLUs are usually recurrent and can persist from weeks to many years [4,9].
VLUs usually appear between the knee and ankle and are typically caused by venous valve incompetence [10–12]. Valvular incompetence may lead to distention of vessels due to increased retrograde blood flow, thereby resulting in venous hypertension [11]. Moreover, veins may be injured through surgery, trauma or deep vein thrombosis, which can result in a backflow of blood in the venous system at the point of injury. Other causes are multiple pregnancies, obesity, congenital vein abnormalities and varicose veins [11]. VLUs are defined by periods of exacerbation and remission and a long heal time [1,13,14], leading to increased resource utilization and healthcare costs [15] as well as a decreased quality of life (QoL) for patients [16]. VLUs present a significant annual economic burden on the US healthcare system and payers (US$14.9 billion) [15]. A previous study compared Medicare and privately insured patients with and without VLUs [15]. This study indicated that VLU patients utilize more healthcare resources (e.g., hospitalizations, outpatient/physician office visits, home health and emergency department) and incurred more healthcare costs compared with non-VLU patients [15]. For Medicare-insured beneficiaries, the annual healthcare costs per VLU patient (US$18,986) were higher than the costs per non-VLU patient (US$12,595) [15]. Moreover, for privately insured beneficiaries, the annual healthcare costs (including drug costs) per VLU patient (US$13,653) were double for a non-VLU patient (US$6623) [15].
Standard of care (SOC) for VLUs involves compression therapy [17–21]. An example of compression therapy is the application of a zinc oxide compression wrap from foot to knee (i.e., Unna’s boot procedure) [17–20]. Although compression therapy is supported by level 1 evidence (i.e., meta-analysis of multiple randomized clinical trials) [17,18], as being beneficial for VLUs, it has many limitations. With SOC, 75% of VLU patients failed to achieve healing in a timely fashion [22]. A randomized clinical trial (RCT) showed that VLUs healed within 6 months after using SOC [23]. Another study reported that 96% of VLUs healed in 1 year [24]. VLU healing is defined as complete wound closure (100% epithelialization) that has lasted for 2 weeks with and no drainage [23].
The objectives of this review article were: to evaluate the QoL of patients with VLUs; to analyze the limitations of SOC for VLUs; and to explain how the use of a bilayered living cellular construct (BLCC) can aid in healing VLUs sooner, can aid in improving QoL for VLU patients and can help reduce the burden on the healthcare system and payers.
Materials & methods
The focus of this review was on articles that provided information related to QoL of patients with VLUs, limitations of SOC for VLUs and economic analysis (cost analysis and cost–effectiveness) of using BLCC for treatment of VLUs. For the last objective (comparing BLCC plus SOC vs SOC alone), we focused on the studies that compared the two groups (i.e., one group includes BLCC plus SOC and the second group includes SOC alone) and we excluded single arm studies (i.e., SOC alone and not compared with BLCC plus SOC). The search was conducted in February 2020 on the following electronic databases:
•
PubMed (1946 through 25 February 2020);
•
EMBASE (1974 through 25 February 2020);
•
Cochrane Library (date of search: 25 February 2020); and
•
Google Scholar (date of search: 25 February 2020)
The following keywords were used in the literature search: venous leg ulcer, VLU, quality of life, QoL, standard of care, standard treatment, bilayered living cellular construct, (BLCC, Apligraf), economics, cost–effectiveness, cost, cost analysis. Articles in English language, from any originating country or geography, were retrieved. The bibliographies of all retrieved relevant articles were explored to further identify more relevant articles. After reviewing the literature, the costs were converted to 2019 US dollars using the US Consumer Price Index (CPI), US city average and medical care commodities.
Figure 1 shows the preferred reporting items for systematic reviews and meta-analyses. Figure 1 demonstrates the initial number of papers that were identified from databases and the final number of studies that were included in this review. These studies are focused on the cost saving and cost–effectiveness comparing BLCC plus SOC versus SOC alone for treatment of VLUs.
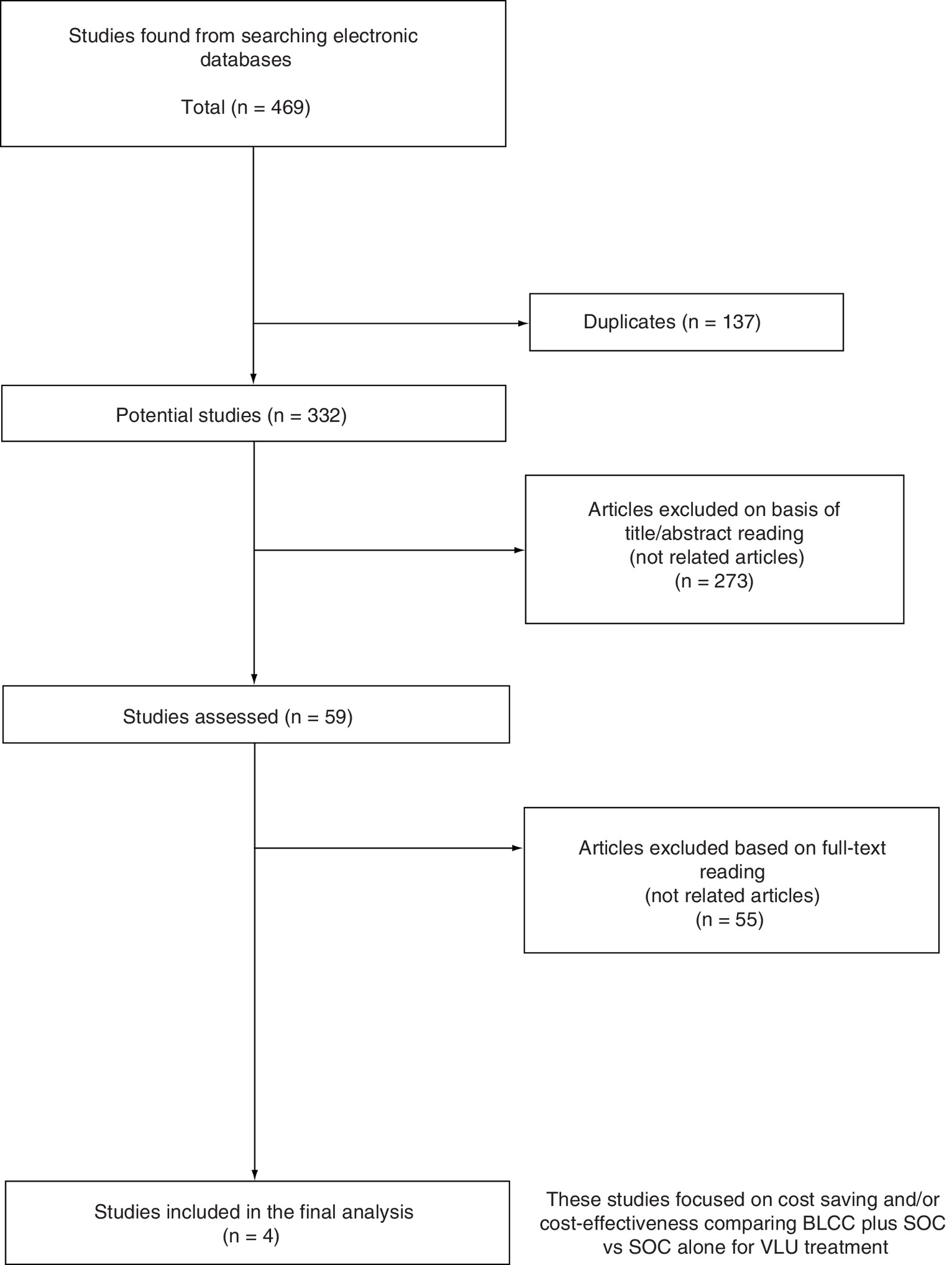
Figure 1. The preferred reporting items for systematic reviews and meta-analyses.
BLCC: Bilayered living cellular construct; SOC: Standard of care; VLU: Venous leg ulcers.
Results & discussion
QoL of patients with VLUs
Generally, chronic leg ulcers profoundly impact a patient’s physical, functional and psychological status [25–27]. Specifically, VLUs cause pain, exudate and foul odor, mobility restrictions and long-term continuous treatments, which when combined affect the daily activities of a patient and could even lead to several life changes [26,28,29]. Because the VLU recurrence rate is as high as 70% within 3 months of wound closure, the reappearance of VLUs can significantly disrupt the lives of patients [30].
The QoL among patients with VLUs is reduced not only from wound complications but also from SOC [31]. Pain is the most frequently reported symptom of VLUs [32] and usually worsens when dressings are changed and are typically difficult to manage. Additionally, studies have shown that pain-associated sleep disturbances play a significant role in lowering QoL in VLU patients [33–35]. Another important factor that reduces QoL among VLU patients is the restriction in mobility, largely, due to pain, swelling, leakage of exudate from the dressing and associated foul odor [27,29]. Swelling exacerbates pain and it is a major predictor of impaired mobility [26]. There are also patients who have difficulty finding adequate, comfortable footwear and clothing that would conceal their wounds [26,27,36–38].
VLUs and their treatment (e.g., prolonged dressings or compression therapy) interfere with lifestyle (e.g., clothing, mobility, socialization, etc.) and work (i.e., loss of workdays) [26,27,36–38]. Reduced QoL is also attributed to physical and psychological stress that adversely affects a patient’s functioning [16,29]. Many VLU patients demonstrate an unhealthy preoccupation with their VLU [29]. For example, exudate and foul odor may have adverse effects on VLU patients’ psychological state, leading to an emotional state of disgust, self-loathing and low self-esteem and, as a consequence, may shun social functions [39]. Avoidance of social functions may bring about emotional distress, which also negatively impacts QoL in VLU patients [40]. Further to this, VLU patients often have decreased work capacity, culminating in a loss in income [4].
SOC for VLUs & Limitations of SOC
SOC for VLUs
Considering the hardships associated with VLUs, guidelines that involve SOC have been developed and are explained below [17–21]. Examples of these guidelines include the Wound Healing Society guidelines, clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum and the guidelines published by the Association of Advanced Wound Care [17–21].
Compression therapy
Compression therapy is the mainstay in venous ulcer therapy [17–21] and can be categorized into high compression (i.e., pressure: 24–35 mmHg) and low compression (i.e., pressure: 14–17 mmHg) [41]. Because high compression achieves better healing rates than low compression, the first line of treatment for non-complicated VLUs is a Class 3 (most supportive), multilayered high-compression system with sufficient padding. An example of compression therapy is Unna’s boot procedure (i.e., a zinc oxide bandage applied to the lower leg that can be covered with an elastic dressing). Pentoxifylline is commonly used to improve blood circulation and is effective when combined with compression therapy [17–19,21].
Wound care
Venous leg ulcers should be cleansed with a neutral, nonirritating, nontoxic solution [17–19]. Sharp, enzymatic, mechanical, biological or autolytic debridement is required to remove all necrotic or devitalized tissue and excessive bioburden [17–19]. Cost factors of each type of debridement method are different. Payers pay attention to one-time use products versus several applications needed (e.g., enzymatic debridement may require several visits). In addition to debridement, evaluation and correction of the causes of tissue damage (e.g., systematic disease and medication, nutrition and tissue perfusion and oxygenation) should be conducted [17–19]. Table 1 shows example of tests and parameters that should be used for determining adequate tissue perfusion and range of values that would lead to proper healing of tissue wounds [42–45].
| Test/parameter | Notes | Ref. |
|---|---|---|
| ABI | • ABI = highest pressure in the leg/the highest pressure in the arm. • The lower ABI value indicates more severe disease. ○ Normal: ABI = 0.91–1.30 ○ Mild occlusion: ABI = 0.70–0.90 ○ Moderate occlusion: ABI = 0.40–0.69 ○ Severe occlusion: ABI <0.40 ○ Poorly compressible vessels: ABI >1.30 | [42–44] |
| TcPO2 | • TcPO2 is also known as transcutaneous oximetry. • Expectation of wound full healing potential when TcPO2 ≥30–40 mmHg. • TcPO2 <20 mmHg indicates sever deprivation of wound oxygenation and hence poor prognosis for wound healing. | [42,43] |
| Laser Doppler | • Laser Doppler is used to test the skin perfusion pressure. • A previous study showed that 90.80% wound healing rate was achieved when the laser Doppler values >30 mmHg compared with 50% wound healing rate when laser Doppler values <30 mmHg. | [42,43,45] |
ABI: Ankle-Brachial Index; TcPO2: Transcutaneous oxygen pressure.
Bacterial control & treatment of wound infection
Dressings (dressing technique should be clean to prevent cross-infection)
Dressings should maintain a moist wound-healing environment, facilitate continued moisture, manage the VLU exudate and protect the surrounding ulcer skin, be cost-effective and be appropriate to the setting and the healthcare provider (supported by level 1 evidence) [18,19,21]. The least expensive and cost-effective dressings are moist saline gauze. However, maintaining a gauze dressing continuously moist may pose a challenge for the clinicians’ time [18].
Surgery in selected patients
Patients with chronic VLU and superficial venous reflux are considered for surgery to promote ulcer healing and prevent recurrence of the ulcer [21]. Sclerotherapy is recommended for superficial varicosities as well as incompetent perforators surrounding the ulcer and may facilitate rapid healing [18,19,21]. The Early Venous Reflux Ablation trial evaluated the early endovenous treatment of superficial venous reflux as an adjunct to compression therapy in VLU patients. The Early Venous Reflux Ablation trial results showed that early endovenous ablation resulted in faster VLU healing and more time free from ulcers compared with deferred endovenous ablation [46].
Limitations of SOC for VLUs
Researchers have shown that VLUs of longer duration and larger size tend to have poor prognoses [47]. VLUs without appropriate treatment can progress to larger ulcers that would require more complex interventions, such as plastic surgery procedures for successful treatment [47]. Unsuccessful treatment of VLUs has been associated with increased rates of morbidity, which will have a significant reduction in patient QoL and a direct increase in costs.
A Cochrane Library systematic review shows that high level of compression with a multilayered bandage is effective for the treatment of VLU [48]. However, a high percentage of VLU patients (75%) failed to achieve healing in a timely fashion [22], which led to increased healthcare costs and healthcare resource utilization. Therefore, there was a significant economic burden on the US healthcare system and payers.
Ma, O'Donnell, Rosen and Iafrati followed VLU patients for a year from initial wound presentation to determine the total cost of treating VLUs. Ma et al. found that patients could be healed without VLU recurrence in a mean time of 122 days at a cost of US$10,563, but costs could reach up to US$50,967 [49]. At times, the total medical cost may reach up to US$132,730 without achieving healing of VLUs. Significant contributing factors to the costs of VLU treatment are outpatient facility fees (US$10,332) and visiting nurse services (US$11,365) [49]. Another important driver for increased costs was hospital admissions and related complications due to infection [49]. The cost could be as high as US$71,526 for those who experience complications (related to surgery) compared with those who had no complications (US$15,285; p < 0.001) [49].
Time to healing is the major contributing factor that influence VLU treatment costs [44]. Prolonged use of healthcare resources were found to triple the costs in nonhealed VLU patients (US$33,907) as compared with healed VLU patients (US$10,563; p < 0.05) [44]. The costs of a visiting nurse (US$11,636) and outpatient facility (wound care center; US$10,332) are the major drivers of significantly increasing costs in nonhealed VLU patients group [49].
Using BLCC for treatment of VLUs
Adding an additional VLU treatment modality to SOC could be of value to VLU patients (through improvement of healing time and QoL) and payers (through reduction of overall cost associated with treatment). BLCC is supplied as a living, bilayered skin substitute [50,51] and it consists of an epidermal layer (formed from human keratinocytes) and a dermal layer (composed of human fibroblasts in a bovine type I collagen matrix) [50,51]. It is void of any antigen-presenting cells and clinical trials have found no evidence of clinical rejection, while immunological tests indicated no humoral or cellular response to keratinocytes and fibroblasts of BLCC [50,51].
The key to BLCC’s healing process is that it accelerates VLU healing [50]. BLCC aids and stimulates healing by providing extracellular matrix components, cytokines and other regulatory cellular components necessary for healing. BLCC accelerates healing because of other multiple functions found in human skin [4]. These include the production of structural and regulatory substances (e.g., collagen, growth factors, cytokines) and interactions with the underlying tissue to promote more effective wound repair [4].
Many studies compared the effectiveness of BLCC versus other modalities for VLU treatment [52–55]. Nelson (2011) indicated that BLCC increases VLU healing in patients receiving compression [56]. A RCT compared the effectiveness of BLCC plus SOC versus compression therapy alone at 24 weeks [52]. The results showed a statistically significance difference in which 56.8% of VLUs were healed using BLCC plus SOC compared with 39.8% of VLUs that were healed using SOC alone [51,52]. Another RCT showed that BLCC plus SOC was superior (63% healing rate) compared with SOC alone (49% healing rate) [23,53]. In addition, the results of the comparative effectiveness study of a BLCC and a porcine collagen wound dressing in VLU treatment showed that BLCC reduced the median time to wound healing by 44%, achieving healing 19 weeks sooner than a porcine collagen wound dressing (24 vs 43 weeks, respectively) [54]. Another comparative effectiveness study compared a BLCC and an acellular fetal bovine collagen dressing for VLU treatment [55]. The results showed that BLCC significantly improved the median time to wound healing by 37%, achieving healing 11 weeks sooner than fetal bovine collagen dressing (19 vs 30 weeks, respectively) [55]. Furthermore, a pilot study assessed health-related QoL of VLU patients treated with BLCC plus SOC [57]. This study indicated that all patients reported improvement in their QoL after BLCC treatment [57].
Cost saving & cost–effectiveness comparing BLCC plus SOC versus SOC alone
It must be emphasized that VLU patients may contend with significant spending during the course of their wound care. These individuals have high utilization rates for home healthcare, prescription medications along with wound dressings supplies, aside from being frequently hospitalized [58]. A prospective multicenter RCT showed that BLCC plus SOC is associated with faster VLU healing than the SOC alone [23]. Another study reported that faster VLU healing associated with BLCC lead to cost savings [59].
Most payers use Medicare as a base for setting payment rate. From the payers’ payment perspective, the upfront cost of BLCC is higher than the upfront cost of SOC (e.g., Unna’s boot). The average 2019 Medicare payment rate for a BLCC procedure per visit is US$1548.96 while the cost for the application of an Unna’s boot per visit is US$250.47 (combined cost of Unna’s boot (US$134.62) and a clinic visit (US$115.85) given that both are typically billed together) [60]. However, the payers need to look at the overall cost and effectiveness of treating VLU patients over a period of time (i.e., a month or a year). Several studies reported that using BLCC and SOC for VLUs is cost-effective compared with SOC alone [58,59,61].
Schonfeld et al. assessed the total annual medical cost and cost–effectiveness of using BLCC and SOC compared with SOC and zinc-impregnated gauze (Unna’s boot) for the treatment of hard-to-heal VLUs over 1 year [59]. The total annual direct medical cost included the main therapeutic option (i.e., BLCC and SOC or Unna’s boot), additional compression dressing, clinician office visits, home health visits, diagnostic tests and procedures, inpatient admission (i.e., hospitalization) and management of adverse events. This economic assessment was from the perspective of a commercial health plan [59]. Based on this economic assessment [59] and by converting to 2019 US dollars (costs were converted using the CPI), the total annual direct medical cost of BLCC and SOC for treatment of a patient with a hard-to-heal VLU (US$36,301.57) is lower than that of Unna’s boot (US$49,799.87) [59]. Therefore, the payers who include BLCC in their healthcare plan coverage, have the opportunity to save US$13,498.30 per VLU patient per year. Based on this information, if we just estimate that a healthcare plan (that covers BLCC) has only 100 VLU patients and the physicians use BLCC for these patients, the cost-savings will be US$1,349,829.51. And if the number of the VLU patients is 10,000 patients, the cost savings can be more than US$134.5 million. Moreover, physicians’ use of BLCC and SOC led to three additional months in the healed state per VLU patient per year compared with Unna’s boot [59]. BLCC improved ulcer healing and therefore, required fewer months of treatment, which resulted in lower overall cost compared with Unna’s boot [59].
To illustrate to payers the cost-savings due to covering BLCC in their healthcare plans, the comparison between BLCC plus SOC versus SOC alone should be presented in addition to the breakdown of the VLU total direct medical cost (2019 US dollars) over a specific period of time (e.g., a month). Figure 2 shows the average monthly direct medical costs of treating one hard-to-heal VLU patient using BLCC and SOC versus Unna’s boot. It is critical for payers to consider the total cost of care given that treating patients living with VLUs involve utilizing healthcare resources (e.g., hospitalization, diagnostic tests and procedures, home health visits, etc.) beyond SOC or SOC plus BLCC. As depicted in Figure 2, BLCC initially costs more than Unna’s boot. However, for VLU patients treated with Unna's boot, the additional compression dressings costs (US$45.28) along with Unna’s boot costs (US$88.76) account for only 2.70% of the monthly direct medical costs, while hospitalization costs ($3725.98) represent 74.96%. Furthermore, when the cost of Unna’s boot is combined with other necessary healthcare costs (home health visits, diagnostic tests and procedures, hospitalization and management of adverse events, etc.), the overall cost of using Unna’s boot is higher compared with using BLCC plus SOC (Figure 2).
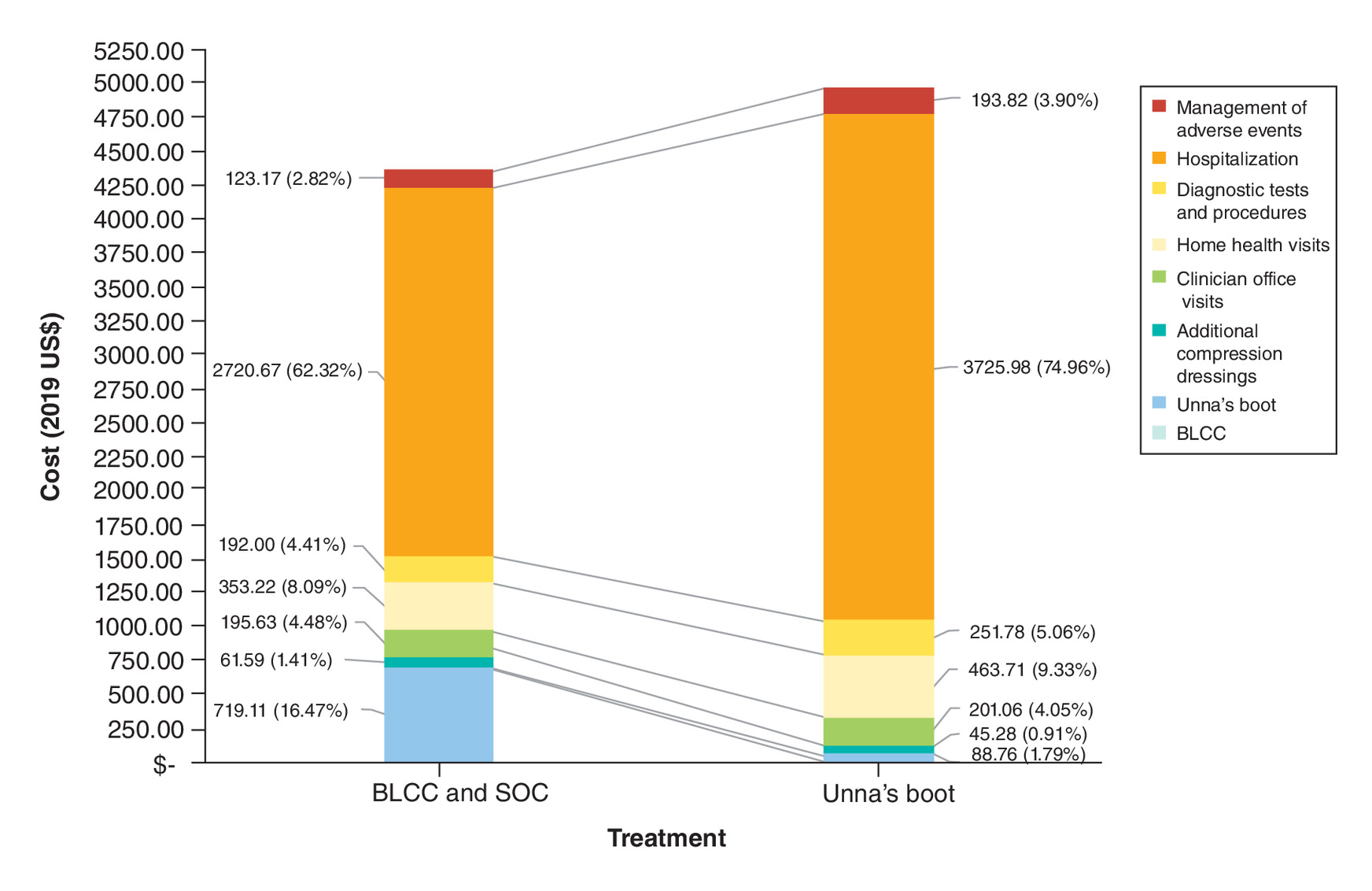
Figure 2. The average monthly direct medical costs of treating a hard-to-heal venous leg ulcer patient*.
*Based on Schonfeld et al. results, the costs were converted to 2019 US dollars using the US CPI, US city average, medical care commodities.
BLCC: Bilayered living cellular construct; CPI: Consumer Price Index; SOC: Standard of care.
While the Schonfeld et al. cost–effectiveness study results were derived from a model that was based on the clinical trial findings [59], it is critical to look at the real-world data and economic assessment of adding BLCC to SOC in the real-world clinical practice setting. Olin et al. described the distribution of the total direct medical cost across the medical services (related to VLU treatment) from the healthcare system perspective [62]. This previous study indicated that hospitalization and home healthcare accounted for 73% of the total VLU direct medical cost, while topical medications, prescription medications and home dressings represented only less than 23% [62].
In this review article, the medical costs were converted to 2019 US dollars, so a comparison of past costs reported in older published US studies can be made and reflected in 2019 US currency. For example, Schonfeld et al. reported that the average monthly direct medical costs were equal to US$4970.39 [59]. Because Schonfeld et al. focused on hard-to-heal VLUs, they reported average monthly direct medical costs that were higher compared with the costs reported by Olin et al. who focused on VLU patients compliant with scheduled office visits. Olin et al. indicated the average monthly direct medical costs are equal to US$4248.49 [62].
The Olin study et al. found that the total VLU direct medical cost was strongly related to duration of follow-up (1 year following the initial visit or until the ulcer healed, whichever occurred first; p < 0.0001) [62]. Therefore, minimizing the time to VLU healing would aid in reducing the overall VLU management cost [62]. According to the BLCC RCT results, the median time to complete wound closure for VLU patients treated with SOC alone is 181 days (i.e., around 6 months) while it is 61 days (around 2 months) for VLU patients treated with BLCC plus SOC [23]. It can be concluded from this study that the addition of BLCC to SOC reduced the time to complete wound closure by 4 months. Therefore, multiplying the reduced time to VLU healing (4 months) by the average monthly VLU direct medical costs (US$4248.49 based on Olin et al.) results in a total cost-saving for the healthcare plan that covers BLCC equal to US$16,993.96 per VLU patient treated with BLCC plus SOC. Also, payers should consider that the 1-year VLU (treated with SOC) recurrence rate is as high as 69% [63] and more than 50% of VLU patients experienced repeated VLUs at 3–5 years of follow-up [64]. Although there is no statistical difference in the VLU recurrence rate between VLU patients treated with BLCC plus SOC and those treated with SOC alone [4], the healthcare plan may have repeated cost-savings by allowing coverage of BLCC and SOC for treatment of VLUs. Furthermore, treating VLUs with BLCC plus SOC reduced the time to VLU healing and improve patients’ QoL.
Fivenson and Scherschun conducted a cost evaluation of BLCC based on VLU-related medical care costs (US dollars) in relation to ulcer size (cm2) changes over 3 months prior and 3 months following VLU treatment with BLCC [58]. The ulcer size measurements were derived from patients’ charts at the hospital while the medical care costs were derived from the billing records [58]. The medical care costs included costs that were directly related to VLU care (i.e., outpatient visits, medical procedures, prescriptions, dressing and supplies, professional fees) [58]. For the costs of BLCC post-treatment period in addition to the mentioned costs, the total medical care costs also include BLCC costs and procedural charges [58]. Fivenson and Scherschun reported that the physicians’ use of BLCC resulted in lower costs per change in ulcer size when comparing the 3 months following BLCC treatment (i.e., BLCC plus SOC) to the 3 months before VLU patients treatment with BLCC (i.e., SOC alone) [58]. Based on this real-world economic assessment [58] and converting to 2019 US dollars (costs were converted using the CPI), Figure 3 shows the comparison of the cost per change in ulcer size (US$/cm2) 3 months prior and 3 months following use of BLCC in each VLU patient. While this study included the available real-world data of only five VLU patients [58], the payers should consider high cost-savings if the BLCC is added to SOC for many patients enrolled in the healthcare plan. Future studies are needed to provide economic evaluation based on real-world databases.
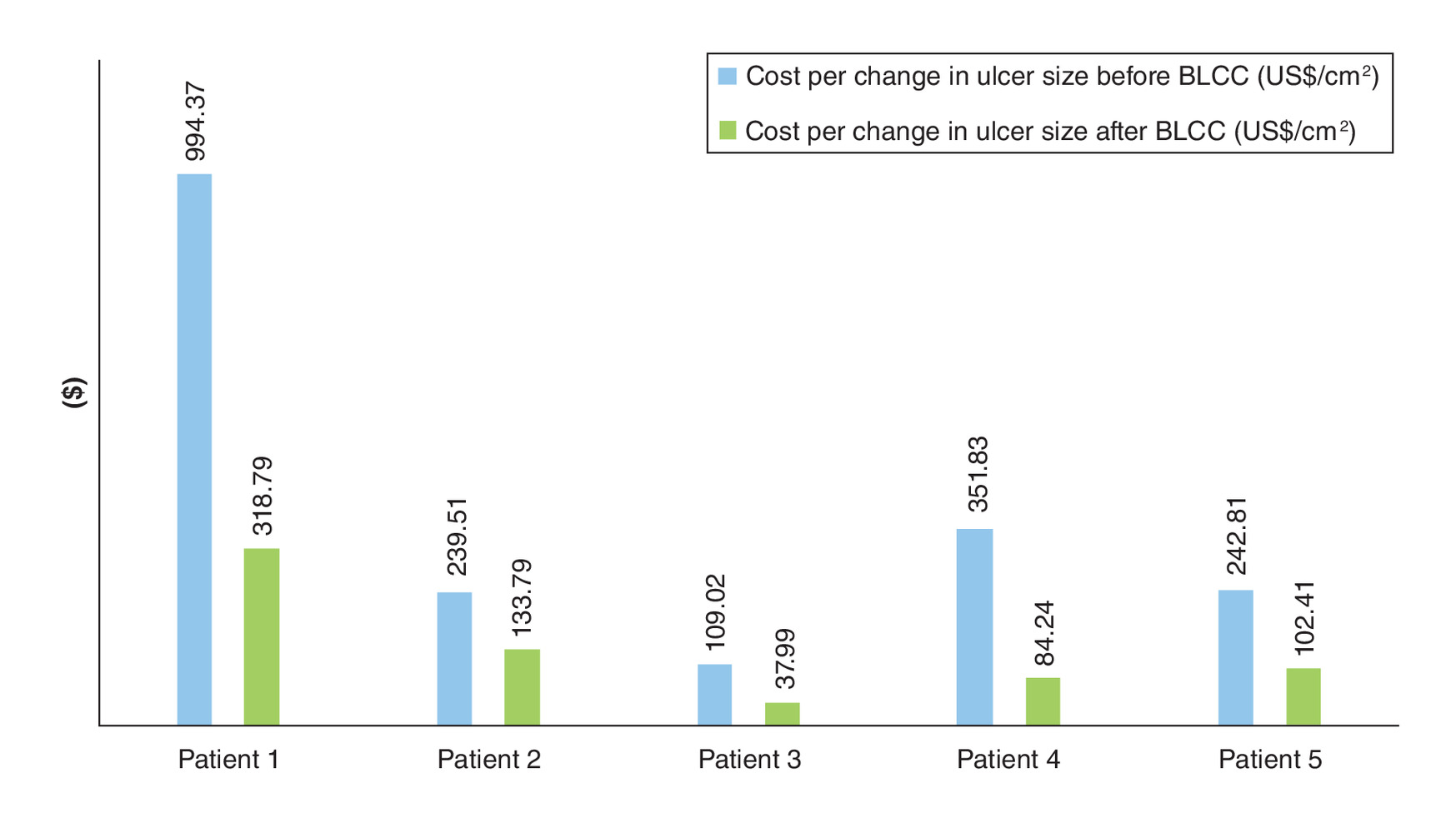
Figure 3. The cost per change in ulcer size 3 months before and 3 months after using bilayered living cellular construct*.
*Based on Fivenson and Scherschun results [58], the costs were converted to 2019 US dollars using the US CPI, US city average, medical care commodities.
BLCC: Bilayered living cellular construct; CPI: Consumer Price Index.
A Canadian study that was published in 2001, examined the cost effectiveness of adding BLCC to SOC [61]. In this study, researchers aimed to discern any justifications for the upfront high acquisition cost of BLCC. They evaluated the cost–effectiveness of treating VLU patients with one BLCC application plus a high compression four-layer bandage compared with a high compression four-layer bandage alone (over the course of three and 6 months) [61]. This study was from the healthcare and societal perspectives [61]. Although the total cost per VLU patient was higher for the BLCC plus four-layer bandage arm from both perspectives, BLCC plus four-layer bandage were more effective than the four-layer bandage alone [61]. The study data showed that using BLCC plus four-layer bandage over 3 months would have averted 22 days of treatment with an additional cost per patient of 316 Canadian dollars (CAD) (healthcare perspective) or 304 CAD (societal perspective) compared with a four-layer bandage [61]. So, over 3 months of treatment, the incremental cost for the course per ulcer per day averted was 14.36 CAD (healthcare provider perspective) or 13.82 CAD (societal perspective). Furthermore, using BLCC over 6 months would drop the incremental cost further to less than 5 CAD per ulcer per day [61]. Looking at the results of this Canadian study [61], by adding BLCC to SOC, the payers who cover BLCC may spend a few more dollars for each VLU patient per day to shorten the period of VLU treatment and, hence, avert treatment days given that more treatment days can cost more money because of increased healthcare resource utilization. An example would be treating infection and hospitalization if BLCC is not covered in the healthcare plan and if the VLU patients were treated with SOC alone. On the other hand, this study assumed only one BLCC application plus SOC for treating VLU patients in three or 6 months [61]. However, RCTs reported using more than one BLCC for treating VLU [4,23]. Future cost–effectiveness studies with different assumptions (e.g., using more than one BLCC application) and long-term time horizons (e.g., more than 6 months) are needed.
The results of our study are reproducible. We relied on peer-reviewed published studies that provided information related to QoL of patients with VLUs, limitations of SOC for VLUs and economic analyses of using BLCC as a treatment of VLUs. The medical costs were converted to 2019 US dollars using the CPI, so a comparison of past costs reported in older published US studies can be made and reflected in 2019 US currency. However, the increase in costs could exceed the CPI [65]. It is likely our study may have underestimated medical costs and hence, the cost-savings for payers could be more than the calculated value in this article. Systematic review is required to provide more comprehensive information related to the subject matter. We did not focus on clinical outcomes publications that provide information related to VLU treatment with BLCC. However, this study provides detailed information related to QoL and an economic evaluation of BLCC in VLU treatment. This information may help in solving the issue of the significant economic burden on the US healthcare system and payers. Payers’ coverage of BLCC and encouraging healthcare professionals to expand using BLCC for VLU treatment results in reduction of the overall medical cost for treating VLU patients.
Conclusion
Patients with VLUs suffer significantly because of pain, foul odor and other factors that reduce their QoL. Although there is SOC for VLUs, the problem at hand is that a high percentage of VLU patients fail to achieve healing in a timely fashion, which leads to increased healthcare resource utilization and healthcare costs, invoking a significant economic burden on the US healthcare system and payers. Since BLCC improves time to healing of VLUs and the addition of BLCC to SOC is more effective compared with SOC alone, improving VLU patients’ QoL as well as cost-savings and cost–effectiveness can be achieved. Therefore, a solution to the mentioned economic burden is for healthcare plans to continue BLCC coverage and encourage healthcare professionals to expand using BLCC for VLU treatment. For example, if a healthcare plan has 100 VLU patients who were treated with BLCC, the cost-savings would exceed 1 million dollars.
•
Venous leg ulcers (VLUs) present a significant economic burden on the US healthcare system and payers (US$14.9 billion).
•
The objectives of this review article were: to evaluate the quality of life (QoL) of patients with VLUs; to analyze the limitations of standard of care (SOC) for VLUs; and to explain how the use of a bilayered living cellular construct (BLCC) can aid in healing VLUs sooner, can aid in improving QoL for VLU patients and can help reduce the burden on the healthcare system and payers.
•
Patients with VLUs suffer significantly because of pain, foul odor and other factors that reduce their QoL.
•
VLUs and their treatment (e.g., prolonged dressings or compression therapy) interfere with lifestyle (e.g., clothing, mobility, socialization, etc.) and work (i.e., loss of workdays).
•
A high percentage of VLU patients who used SOC alone fail to achieve healing in a timely fashion, which leads to increased healthcare resource utilization and healthcare costs, invoking a significant economic burden on the US healthcare system and payers.
•
Since BLCC improves time to healing of VLUs and the addition of BLCC to SOC is more effective compared with SOC alone, improving VLU patients’ QoL as well as cost-savings and cost–effectiveness can be achieved.
•
Although the upfront cost is high, the greater effectiveness of BLCC offsets the added cost of the product during the time period of the studies.
•
Payers’ coverage of BLCC results in reduction of the overall medical cost for treating VLU patients.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Agale SV. Chronic leg ulcers: epidemiology, aetiopathogenesis and management. Ulcers 2013, (2013) (Epub ahead of print).
2.
Zaulyanov L, Kirsner RS. A review of a bi-layered living cell treatment (Apligraf®) in the treatment of venous leg ulcers and diabetic foot ulcers. Clin. Interv. Aging 2(1), 93–98 (2007).
3.
Aydin A, Shenbagamurthi S, Brem H. Lower extremity ulcers: venous, arterial, or diabetic? Emerg. Med. J. 41(8), 18–24 (2009).
4.
Falanga V, Sabolinski M. A bilayered living skin construct (APLIGRAF®) accelerates complete closure of hard- to- heal venous ulcers. Wound Repair Regen. 7(4), 201–217 (1999).
5.
Beebe-Dimmer JL, Pfeifer JR, Engle JS, Schottenfeld D. The epidemiology of chronic venous insufficiency and varicose veins. Ann. Epidemiol. 15(3), 175–184 (2004).
6.
Carpentier PH, Maricq HR, Biro C, Poncot-Makinen CO, Franco A. Prevalence, risk factors and clinical patterns of chronic venous disorders of lower limbs: a population-based study in France. J. Vasc. Surg. 40(4), 650–659 (2004).
7.
Tang JC, Vivas A, Rey A, Kirsner RS, Romanelli P. Atypical ulcers: wound biopsy results from a university wound pathology service. Ostomy Wound Manage 58(6), 20–22 (2012).
8.
Tendera M, Aboyans V, Bartelink ML et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: the Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 32(22), 2851–2906 (2011).
9.
Hansson C andersson E, Swanbeck G. A follow-up study of leg and foot ulcer patients. Acta Derm. Venereol. 67(6), 496–500 (1987).
10.
Kahle B, Hermanns H-J, Gallenkemper G. Evidence-based treatment of chronic leg ulcers. Dtsch Arztebl. Int. 108(14), 231–237 (2011).
11.
Lurie F. Venous haemodynamics: what we know and don't know. Phlebology 24(1), 3–7 (2009).
12.
Mustoe T. Dermal ulcer healing: advances in understanding. Tissue repair and ulcer/wound healing: molecular mechanisms, therapeutic targets and future directions. Euroconferences. Paris, France, (2005).
13.
Nelzen O, Bergqvist D, Lindhagen A. Long-term prognosis for patients with chronic leg ulcers: a prospective cohort study. Eur. J. Vasc. Endovasc. Surg. 13(5), 500–508 (1997).
14.
Valencia IC, Falabella A, Kirsner RS, Eaglstein WH. Chronic venous insufficiency and venous leg ulceration. J. Am. Acad. Dermatol. 44(3), 401–424 (2001).
15.
Rice JB, Desai U, Cummings AKG, Birnbaum HG, Skornicki M, Parsons N. Burden of venous leg ulcers in the United States. J. Med. Econ. 17(5), 347–356 (2014).
•• Provides more information about the economic burden of venous leg ulcers (VLUs) in the USA.
16.
Faria E, Blanes L, Hochman B, Mesquita Filho M, Ferreira L. Health-related quality of life, self- esteem and functional status of patients with leg ulcers. Wounds 23(1), 4–10 (2011).
17.
Robson MC, Cooper DM, Aslam R et al. Guidelines for the treatment of venous ulcers. Wound Repair Regen. 14(6), 649–662 (2006).
18.
Marston W, Tang J, Kirsner RS, Ennis W. Wound Healing Society 2015 update on guidelines for venous ulcers. Wound Repair Regen. 24(1), 136–144 (2016).
• Explains the guideline of VLU treatment.
19.
O'Donnell TF, Passman MA, Marston WA et al. Management of venous leg ulcers: clinical practice guidelines of the Society for Vascular Surgery® and the American Venous Forum. J. Vasc. Surg. 60(2), S3–S59 (2014).
• Provides more information about VLU treatment.
20.
White-Chu EF, Conner-Kerr TA. Overview of guidelines for the prevention and treatment of venous leg ulcers: a US perspective. J. Multidiscip. Healthc. 7, 111–117 (2014).
• Provides more information about VLU prevention and treatment.
21.
Rai R. Standard guidelines for management of venous leg ulcer. Indian Dermatol. Online J. 5(3), 408–411 (2014).
22.
O'Meara S, Cullum NA, Nelson EA. Compression for venous leg ulcers. Cochrane Database Syst. Rev. 1, Cd000265 (2009).
23.
Falanga V, Margolis D, Alvarez O et al. Rapid healing of venous ulcers and lack of clinical rejection with an allogeneic cultured human skin equivalent. Arch. Dermatol. 134(3), 293–300 (1998).
24.
Marston WA, Carlin RE, Passman MA, Farber MA, Keagy BA. Healing rates and cost efficacy of outpatient compression treatment for leg ulcers associated with venous insufficiency. J. Vasc. Surg. 30(3), 491–498 (1999).
25.
Cunha N, Campos S, Cabete J. Chronic leg ulcers disrupt patients' lives: a study of leg ulcer-related life changes and quality of life. Br. J. Community Nurs. 22(Suppl. 9), S30–S37 (2017).
•• Provides more information related to quality of life of patients with VLUs.
26.
Persoon A, Heinen MM, van der Vleuten CJ, de Rooij MJ, van de Kerkhof PC, van Achterberg T. Leg ulcers: a review of their impact on daily life. J. Clin. Nurs. 13(3), 341–354 (2004).
27.
Roaldsen KS, Biguet G, Elfving B. Physical activity in patients with venous leg ulcer–between engagement and avoidance. A patient perspective. Clin. Rehabil. 25(3), 275–286 (2011).
28.
Green J, Jester R. Health-related quality of life and chronic venous leg ulceration: part 1. Br. J. Community Nurs. 14(12), 6–7 (2009).
29.
Green J, Jester R. Health-related quality of life and chronic venous leg ulceration: part 2. Br. J. Community Nurs. 15(3), S4–S6 (2010).
30.
Franks PJ, Barker J, Collier M et al. Management of patients with venous leg ulcers: challenges and current best practice. J. Wound Care 25(Suppl. 6), S1–S67 (2016).
•• Explains the challenges and best practice of VLU management.
31.
Hareendran A, Doll H, Wild DJ et al. The venous leg ulcer quality of life (VLU-QoL) questionnaire: development and psychometric validation. Wound Repair Regen. 15(4), 465–473 (2007).
32.
Gonzalez-Consuegra RV, Verdu J. Quality of life in people with venous leg ulcers: an integrative review. J. Adv. Nurs. 67(5), 926–944 (2011).
33.
Upton D andrews A. Sleep disruption in patients with chronic leg ulcers. J. Wound Care 22(8), 389–394 (2013).
34.
Taverner T, Closs SJ, Briggs M. The journey to chronic pain: a grounded theory of older adults' experiences of pain associated with leg ulceration. Pain Manag. Nurs. 15(1), 186–198 (2013).
35.
Green J, Jester R, McKinley R, Pooler A. Patient perspectives of their leg ulcer journey. J. Wound Care 22(2), 60–62 (2013).
36.
Heinen MM, Persoon A, van de Kerkhof P, Otero M, van Achterberg T. Ulcer-related problems and health care needs in patients with venous leg ulceration: a descriptive, cross-sectional study. Int. J. Nurs. Stud. 44(8), 1296–1303 (2007).
37.
Chase SK, Melloni M, Savage A. A forever healing: the lived experience of venous ulcer disease. J. Vasc. Nurs. 15(2), 73–78 (1997).
38.
Walshe C. Living with a venous leg ulcer: a descriptive study of patients' experiences. J. Adv. Nurs. 22(6), 1092–1100 (1995).
39.
Jones JE, Robinson J, Barr W, Carlisle C. Impact of exudate and odour from chronic venous leg ulceration. Nurs. Stand. 22(45), 53–54 (2008).
40.
Harlin SL, Harlin RD, Sherman TI, Rozsas CM, Shafqat MS, Meyers W. Using a structured, computer-administered questionnaire for evaluating health-related QOL with chronic lower extremity wounds. Ostomy Wound Manage. 55(9), 30–39 (2009).
41.
Dowsett C, Scanlon L. Compression bandaging and the clinical governance agenda. Br. J. Community Nurs. 6(Suppl. 2), 17–21 (2001).
42.
Woo KY, Brandys TM, Marin JA. Assessing chronic wound perfusion in the lower extremity: current and emerging approaches. Chronic Wound Care Manag. Res. 2, 149–157 (2015).
43.
Espensen EH, DPM, Ahmed A. Evaluating tissue perfusion to assess wound healing in patients with PAD. Podiatry Today 26(8), 56–61 (2015).
44.
Verma M, Singh AK, Kumar V, Mishra B. Role of Ankle Brachial Index (ABI) in management of non-healing ulcers of lower limb. J. Universal Surg. 6(1), 1–5 (2018).
45.
Utsunomiya M, Nakamura M, Nagashima Y, Sugi K. Predictive value of skin perfusion pressure after endovascular therapy for wound healing in critical limb ischemia. J. Endovasc. Ther. 21(5), 662–670 (2014).
46.
Gohel MS, Heatley F, Liu X et al. A randomized trial of early endovenous ablation in venous ulceration. N. Engl. J. Med. 378(22), 2105–2114 (2018).
47.
Brem H, Kirsner RS, Falanga V. Protocol for the successful treatment of venous ulcers. Am. J. Surg. 188(Suppl. 1A), 1–8 (2004).
48.
Cullum N, Nelson EA, Fletcher AW, Sheldon TA. Compression bandages and stockings for venous leg ulcers. Cochrane Database Syst. Rev. 2, CD000265 (2000).
49.
Ma H, O'Donnell TF Jr, Rosen NA, Iafrati MD. The real cost of treating venous ulcers in a contemporary vascular practice. J. Vasc. Surg. Venous Lymphat. Disord. 2(4), 355–3561 (2014).
50.
Curran MP, Plosker GL. Bilayered bioengineered skin substitute (apligraf®). BioDrugs 16(6), 439–455 (2002).
51.
Apligraf, package insert (2020). www.apligraf.com/professional/pdf/prescribing_information.pdf
52.
Hankin CS, Knispel J, Lopes M, Bronstone A, Maus E. Clinical and cost efficacy of advanced wound care matrices for venous ulcers. J. Manag. Care Pharm. 18(5), 375–384 (2012).
53.
O'Donnell TF Jr, Lau J. A systematic review of randomized controlled trials of wound dressings for chronic venous ulcer. J. Vasc. Surg. 44(5), 1118–1125 (2006).
54.
Marston WA, Sabolinski ML, Parsons NB, Kirsner RS. Comparative effectiveness of a bilayered living cellular construct and a porcine collagen wound dressing in the treatment of venous leg ulcers. Wound Repair Regen. 22(3), 334–340 (2014).
55.
Sabolinski ML, Gibbons G. Comparative effectiveness of a bilayered living cellular construct and an acellular fetal bovine collagen dressing in the treatment of venous leg ulcers. J. Comp. Eff. Res. 7(8), 797–805 (2018).
56.
Nelson EA. Venous leg ulcers. BMJ Clin. Evid. 2011, 1902 (2011).
57.
Mathias SD, Prebil LA, Boyko WL et al. Health-related quality of life in venous leg ulcer patients successfully treated with Apligraf: a pilot study. Adv. Skin Wound Care 13(2), 76–78 (2000).
58.
Fivenson D, Scherschun L. Clinical and economic impact of Apligraf® for the treatment of nonhealing venous leg ulcers. Int. J. Dermatol. 42(12), 960–905 (2003).
59.
Schonfeld WH, Villa KF, Fastenau JM, Mazonson PD, Falanga V. An economic assessment of Apligraf®(Graftskin) for the treatment of hard- to- heal venous leg ulcers. Wound Repair Regen. 8(4), 251–257 (2000).
60.
Centers for Medicare and Medicaid Services. Hospital outpatient prospective payment system (Addendum A) (2019). www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Addendum-A-and-Addendum-B-Updates
61.
Sibbald R, Torrance G, Walker V, Attard C, MacNeil P. Cost–effectiveness of Apligraf in the treatment of venous leg ulcers. Ostomy Wound Manag. 47(8), 36–46 (2001).
62.
Olin JW, Beusterien KM, Childs MB, Seavey C, McHugh L, Griffiths RI. Medical costs of treating venous stasis ulcers: evidence from a retrospective cohort study. Vasc. Med. 4(1), 1–7 (1999).
63.
Moffatt CJ, Dorman MC. Recurrence of leg ulcers within a community ulcer service. J. Wound Care 4(2), 57–61 (1995).
64.
Marston WA, Carlin RE, Passman MA, Farber MA, Keagy BA. Healing rates and cost efficacy of outpatient compression treatment for leg ulcers associated with venous insufficiency. J. Vasc. Surg. 30(3), 491–498 (1999).
65.
Bin Sawad A, Seoane-Vazquez E, Rodriguez-Monguio R, Turkistani F. Price analysis of multiple sclerosis disease-modifying therapies marketed in the United States. Curr. Med. Res. Opin. 32(11), 1783–1788 (2016).
Information & Authors
Information
Published In
Pages: 907 - 918
PubMed: 32969709
Copyright
© 2020 Future Medicine Ltd.
History
Received: 10 May 2020
Accepted: 21 July 2020
Published online: 24 September 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Treatment of venous leg ulcers using bilayered living cellular construct. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0076
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ewa Rojczyk, Kinga Spyrka, Aleksander Sieroń, Dariusz Bazalińśki, Marek Kucharzewski, Synergistic effect of octenidine gel and hydrogel dressing in the treatment of venous leg ulcers, Frontiers in Pharmacology, 10.3389/fphar.2026.1799111, 17, (2026).
- Hubert Aleksandrowicz, Agnieszka Owczarczyk-Saczonek, Waldemar Placek, Venous Leg Ulcers: Advanced Therapies and New Technologies, Biomedicines, 10.3390/biomedicines9111569, 9, 11, (1569), (2021).