The efficacy of 3D printing-assisted surgery in treating distal radius fractures: systematic review and meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the efficacy of 3D printing-assisted surgery with routine surgery in the treatment of distal radius fractures to evaluate whether 3D printing technology has more advantages. Materials & methods: To retrieve all published studies that compared the efficacy of 3D printing-assisted surgery with routine surgery for distal radius fractures. Operation time, frequency of intraoperative fluoroscopy, blood loss and other outcomes were assessed. Results: The results suggested that 3D printing-assisted surgery was better than routine surgery in the fields of operation time, frequency of intraoperative fluoroscopy, and blood loss. Conclusion: In the treatment of distal radius fractures, 3D printing-assisted surgery may be superior to routine surgery.
Distal radius fracture is one of the most common upper limb fractures, accounting for approximately 1.5% of emergency department cases [1–3]. Distal radius fractures occur more frequently in older and younger adults [4]. Osteoporosis is the main cause of distal radius fractures in the elderly, and the prognosis is good after routine treatment [5]. High-energy collisions are a common cause of such fractures in young patients [6]. Because of this, such fractures require surgical treatment to heal young patients. High-energy collisions lead to significant displacement of fractures, and surgical treatment is more effective in anatomical reduction and fixation [7]. In rare cases, conservative treatment may result in malunion, leading to a poor prognosis [8–10].
Conventional surgical treatment of distal radius fractures sometimes causes complications such as extensor and flexor tendon irritation, carpal tunnel syndrome and complex regional pain syndrome [11]. A small number of patients may also have complications such as poor alignment, nonunion and malunion [12–14]. As 3D printing technology has become more and more mature, it has been widely used in orthopedics [15]. This technology is based on the imaging data of patients, and the original fracture model is established with a 3D digital model [16]. Surgeons can use the model to simulate the surgical procedure and identify problems that may occur during surgery, thus improving surgical plans and reducing the incidence of postoperative complications [17]. Currently, there is a lack of meta-analyses comparing the efficacy of 3D printing-assisted surgery and routine surgery in the treatment of distal radius fractures. Therefore, this research analyzed the data to obtain clearer and more realistic results to guide clinical treatment.
Materials & methods
Search strategy
A detailed search for clinical studies was conducted in the major electronic databases, including PubMed, EMBASE, Web of Science, the Cochrane Library, Wan Fang data, CBM and CNKI, up to March 2020. There were no language restrictions. In addition, we searched the references contained in the relevant articles for potential studies. The keywords we used in the database searches included ‘radius fractures’, ‘three-dimensional’ and ‘3D printing’. These were combined using Boolean operators.
Inclusion & exclusion criteria
Studies were incorporated if they met the following criteria: patients were diagnosed with distal radius fracture; the study compared the efficacy of 3D printing-assisted surgery with that of routine surgery; studies were randomized controlled trials (RCTs), prospective comparative studies or retrospective comparative studies; the included Chinese studies had to have English titles and abstracts; the study included the following results: operation time, frequency of intraoperative fluoroscopy, blood loss, postoperative visual analogue scores (VAS), Gartland–Werley scores, excellent and good rate of wrist function, range of motion (ROM) and radiological outcomes. We excluded the following types of studies: other types of fractures; related data in study is incomplete; animal experiments; systematic reviews, meta-analyses, case reports, conference papers and studies which only had an abstract.
Data extraction
Two reviewers examined the included studies and extracted the main data including: name of the first author, publication year, recruitment year, country, groups, study design, sample size (males/females), patient age, distal radius fracture classifications, follow-up time and time from injury to surgery. The reviewers extracted the data independently and discussed any differences to reach a consensus.
Quality assessment
We used the Cochrane risk assessment scale to assess the quality of the RCTs, including random sequence generation, allocation concealment, blinding, selective outcome reporting, incomplete outcome data and other bias. The Methodological Index for Non-Randomized Studies (MINORS) was used to assess non-RCTs. Two reviewers evaluated the articles independently.
Statistical analysis
We performed statistical analysis using the RevMan 5.3 software (Cochrane Collaboration, Oxford, UK). Weighted mean difference (WMD) was used to pool continuous results and risk ratio was used to pool dichotomous result. We used 95% CI to estimate interval. P ≤ 0.05 was considered statistically significant. We estimated the interval using 95% CI. I2 statistics were used to assess statistical heterogeneity. I2>50% indicated significant heterogeneity, used the random-effects model for the analysis, or else, used the fixed-effect model. In addition, sensitivity analysis was performed to identify the source of heterogeneity.
Results
Results of literature retrieval
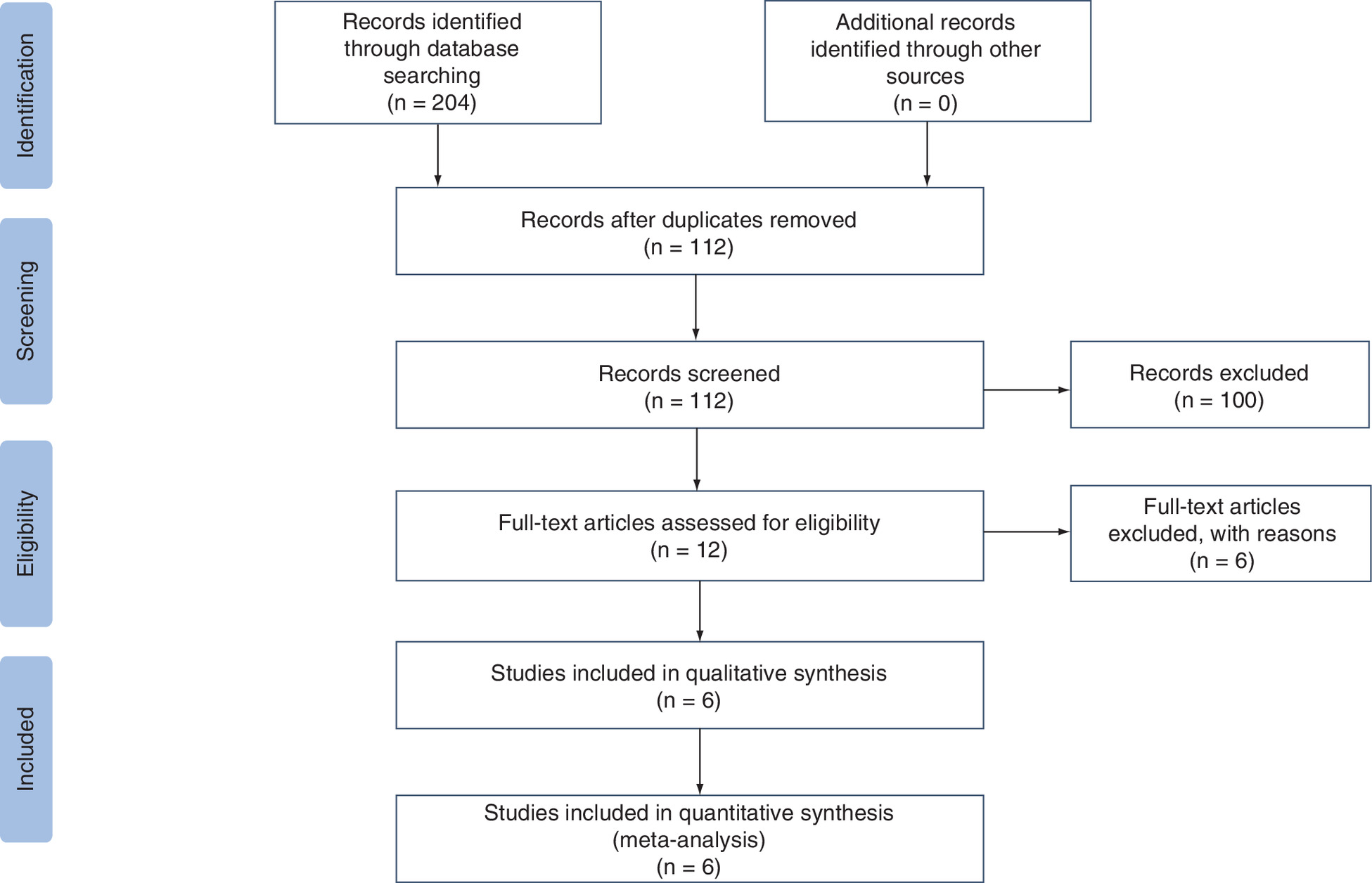
The reviewers identified 204 published articles that were potentially relevant to our study. A total of 92 duplicate articles were excluded. By conducting preliminary screening of the titles and abstracts of the articles, 100 studies were excluded. After perusing the full text, six studies were excluded because they focused on osteotomy for malunion of distal radius fractures [18–23]. Finally, six studies were included in the meta-analysis [24–29]. The characteristics of the final included studies are shown in Table 1. The literature retrieval process is shown in Figure 1.
| Study | Year | Recruitment | Country | Design | Groups | Sample size(M/F) | Age ± mean (years) | AO classification of fractures | Follow-up (month) | Time from injury to surgery (day) | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Chen et al. | 2017 | 2013–2015 | China | RCT | 3D R | 52(30/22) 55(35/20) | 27.69 ± 6.64 29.15 ± 6.86 | 52 B1 55 B1 | 13.08 ± 0.78 13.07 ± 0.79 | 3.19 ± 1.70 3.15 ± 1.55 | [24] |
| Tan et al. | 2017 | 2015–2016 | China | RCT | 3D R | 26(9/17) 29(16/13) | 38.27 45.47 | 15 C1, 6 C2, 5 C3 13 C1, 9 C2, 7 C3 | 9∼18 | NR | [28] |
| Luo et al. | 2018 | 2015–2017 | China | RCT | 3D R | 15(9/6) 15(8/7) | 41.80 ± 11.86 41.87 ± 9.52 | 10 C2, 5 C3 9 C2, 6 C3 | 6 | NR | [27] |
| Xu et al. | 2018 | 2015–2016 | China | nonRCT | 3D R | 25(11/14) 25(13/12) | 42.7 ± 1.9 43.6 ± 1.8 | 8 A, 8 B, 9 C 6 A, 13 B, 6 C | 15∼24 | 6.72 ± 0.27 4.88 ± 1.59 | [29] |
| Chen et al. | 2019 | 2014–2015 | China | RCT | 3D R | 23(14/9) 25(17/8) | 38.7 ± 13.6 40.7 ± 11.4 | 10 C1, 9 C2, 4 C3 11 C1, 11 C2, 3 C3 | 13.0 ± 0.7 13.1 ± 0.7 | 3.3 ± 1.8 3.7 ± 1.6 | [25] |
| Kong et al. | 2020 | 2017–2018 | China | RCT | 3D R | 16(10/6) 16(9/7) | 41.1 ± 6.4 42.8 ± 5.1 | 4 B, 12 C 5 B, 12 C | 6 | 7 | [26] |
3D: Print-assisted surgery; F: Female; M: Male; R: Routine surgery; RCT: Randomized controlled trial; NR: Not reported.
Study characteristics
Baseline characteristics of the selected studies were extracted, and are listed in Table 1. The six studies involved a sample size of 15–55 patients and were published between 2017 and 2020. These studies were all performed in China.
Assessing the quality of the studies
We included five RCTs, all of which showed clear inclusion and exclusion criteria. Randomization methods were clearly described in all the RCTs included [24–28]. In one RCT, the researchers used opaque sealed envelopes to perform the allocation concealment [26]. Three RCTs described details in blinding of participants and personnel [24–26]. Complete outcome indicators were reported in all RCTs. Detailed information of the study quality is shown in Figure 2. We used the MINORS scale to assess the quality of the non-RCT study, the detailed information of which is shown in Table 2.

| Quality assessment of the nonrandomized trials. | Xu et al. (2018) |
|---|---|
| A clearly stated aim | 2 |
| Inclusion of consecutive patients | 2 |
| Prospective data collection | 2 |
| End points appropriate to the aim of the study | 2 |
| Unbiased assessment of the study end point | 2 |
| A follow-up period appropriate to the aims of study | 2 |
| Less than 5% loss to follow-up | 2 |
| Prospective calculation of the sample size | 0 |
| An adequate control group | 2 |
| Contemporary groups | 2 |
| Baseline equivalence of groups | 2 |
| Adequate statistical analyses | 2 |
| Total score | 22 |
Operation time
All studies reported on operation time [24–29], and as the heterogeneity among these studies was high (I2 = 97%), we performed a meta-analysis using a random-effects model. The results showed that the operation time of the 3D printing-assisted surgery group was significantly shorter (WMD = -14.52; 95% CI: -21.79 to -7.24; p < 0.0001) (Figure 3).
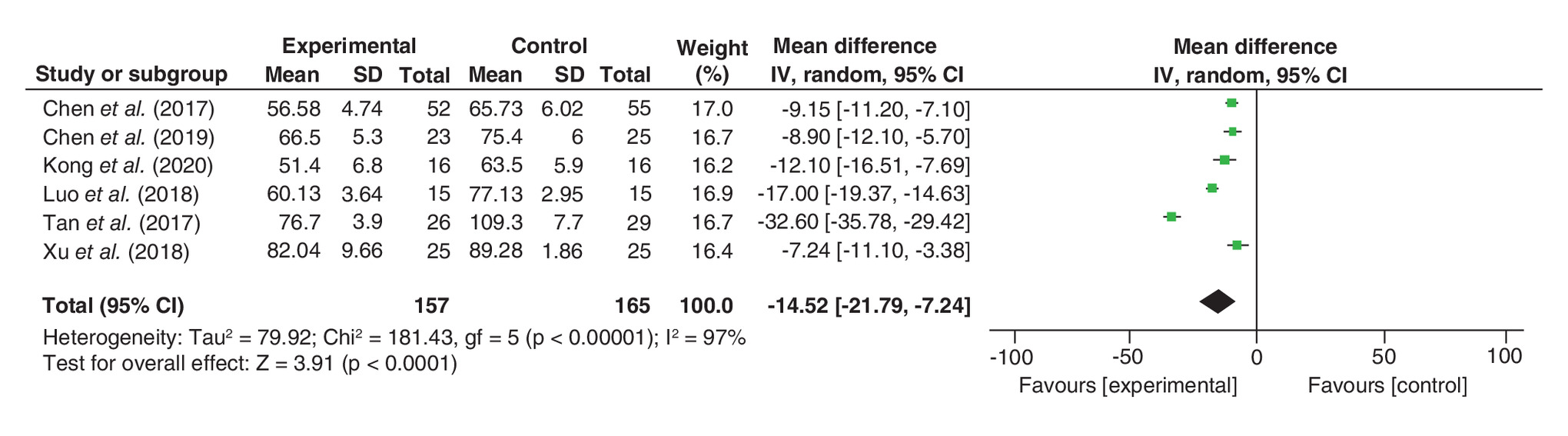
Figure 3. Comparison of operation time.
Forest plot comparing operation time between the 3D printing-assisted surgery group and the routine surgery group.
SD: Standard deviation.
Frequency of intraoperative fluoroscopy
Five studies reported on frequency of intraoperative fluoroscopy [24–28], and the results showed that the frequency of intraoperative fluoroscopy for the 3D printing-assisted surgery group was significantly less (WMD = -2.14; 95% CI: -3.43 to -0.85; p = 0.001), and the heterogeneity among these studies was high (I2 = 95%; Figure 4).
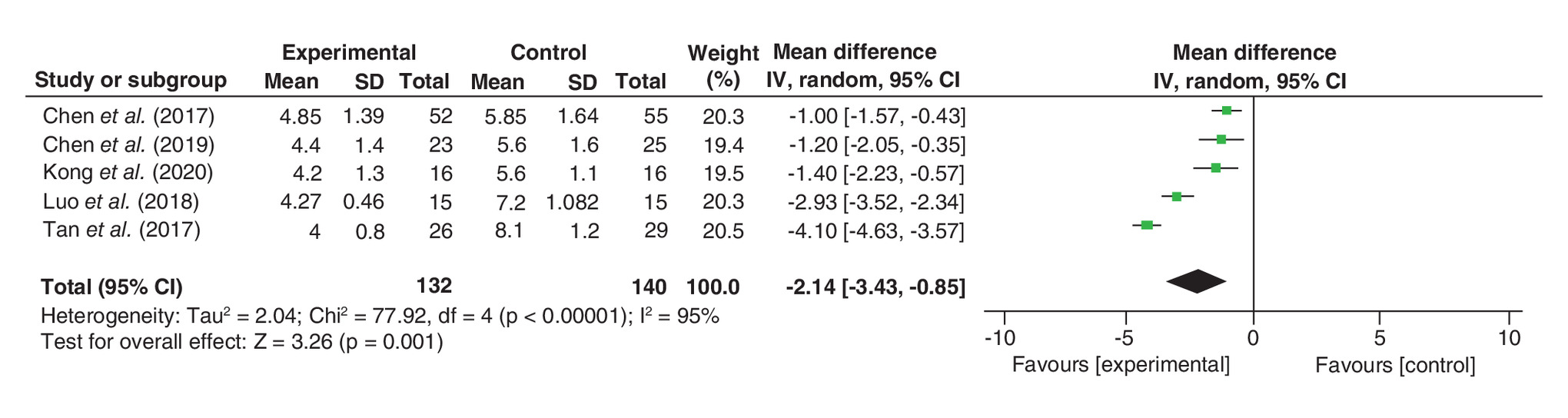
Figure 4. Comparison of frequency of intraoperative fluoroscopy.
Forest plot comparing frequency of intraoperative fluoroscopy between the 3D printing-assisted surgery group and the routine surgery group.
SD: Standard deviation.
Blood loss
Four studies reported on blood loss [24–26,29], and the results showed that blood loss during the 3D printing-assisted surgery group was significantly less (WMD = -13.59; 95% CI: -18.07 to -9.10; p < 0.00001), and the heterogeneity among these studies was high (I2 = 74%; Figure 5).
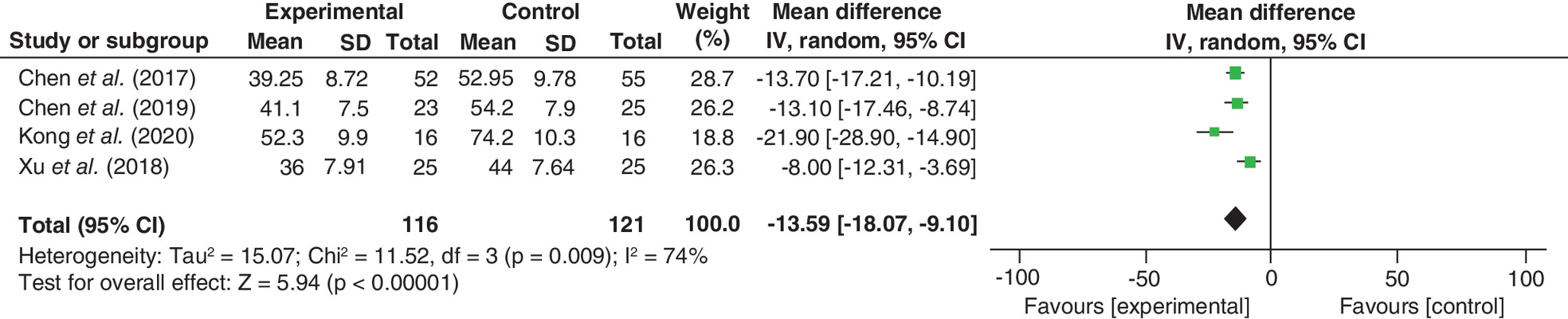
Figure 5. Comparison of blood loss.
Forest plot comparing blood loss between the 3D printing-assisted surgery group and the routine surgery group.
SD: Standard deviation.
Postoperative VAS
Postoperative VAS was reported on in two studies [26,29], and the results showed the two groups had no statistical differences (WMD = -0.55; 95% CI: -1.72 to 0.62; p = 0.36), and the heterogeneity between the studies was high (I2 = 91%; Figure 6).
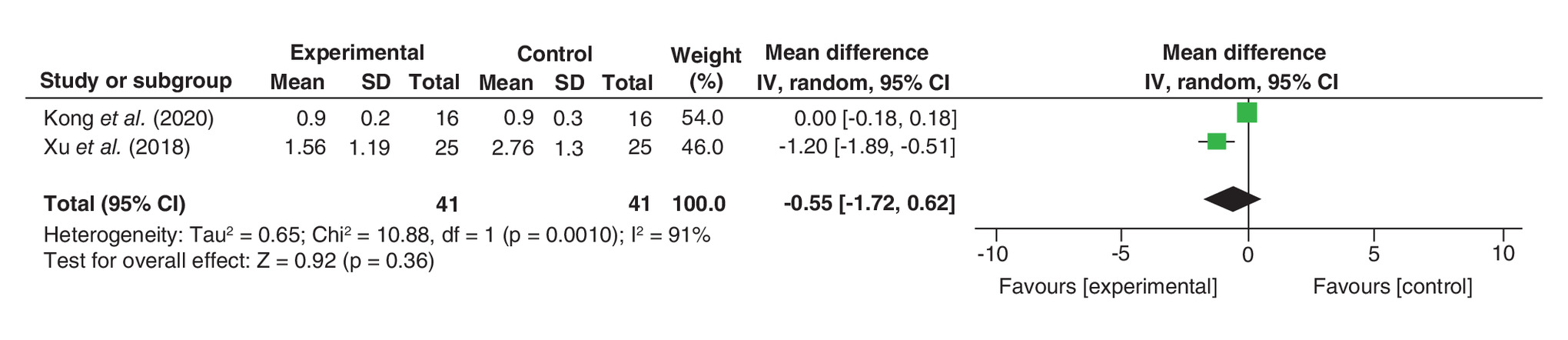
Figure 6. Comparison of postoperative visual analogue score.
Forest plot comparing postoperative visual analogue score between the 3D printing-assisted surgery group and the routine surgery group.
SD: Standard deviation.
Gartland–Werley scores
Gartland–Werley scores were reported in two studies [24,25], and the results showed the two groups had no statistical differences (WMD = 0.56; 95% CI: -4.18 to 5.30; p = 0.82), and the heterogeneity between the studies was low (I2 = 0%; Figure 7).
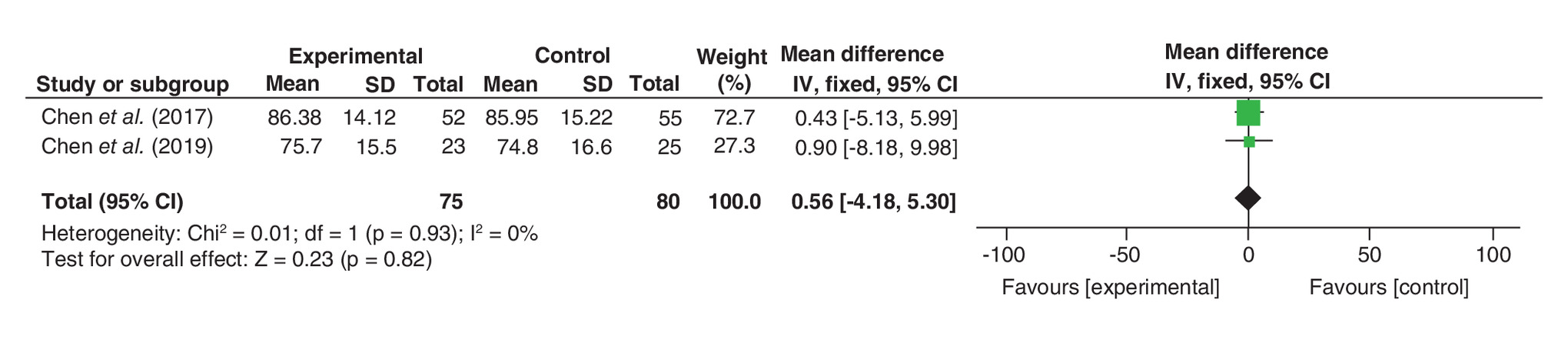
Figure 7. Comparison of Gartland–Werley scores.
Forest plot comparing Gartland–Werley scores between the 3D printing-assisted surgery group and the routine surgery group.
SD: Standard deviation.
Excellent & good rate of wrist function
Three studies reported excellent and good rate of wrist function in two groups [27–29]; the results showed the two groups had no statistical differences (risk ratio = 1.10; 95% CI: 0.96–1.27; p = 0.17) and the heterogeneity between the studies was low (I2 = 0%; Figure 8).
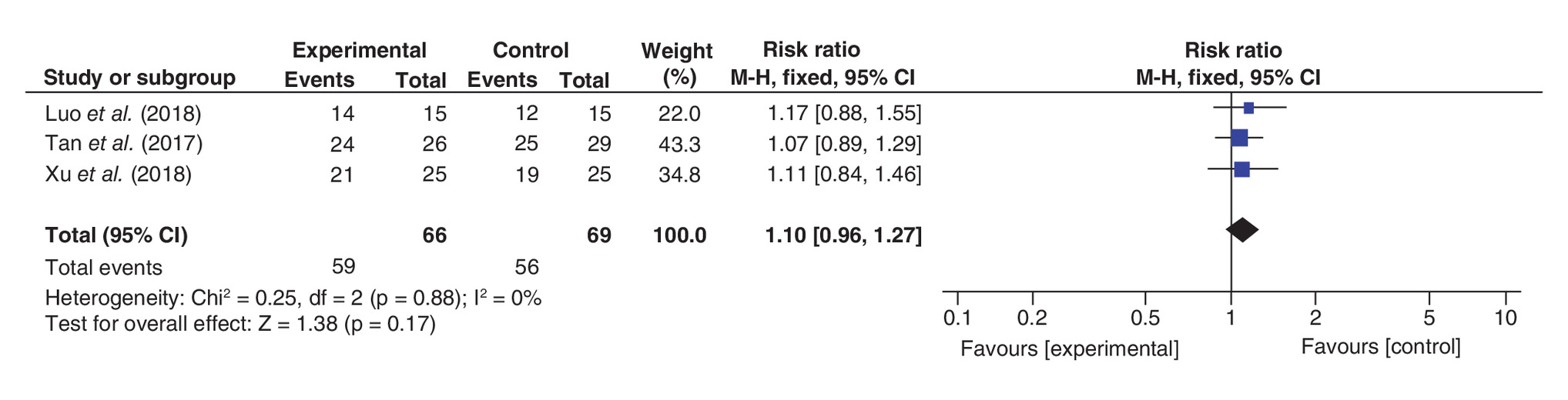
Figure 8. Comparison of excellent and good rate of wrist function.
Forest plot comparing excellent and good rate of wrist function between the 3D printing-assisted surgery group and the routine surgery group.
SD: Standard deviation.
Range of motion
Two studies reported on postoperative ROM of patients in two groups [26,28]. These studies evaluated four aspects of ROM, including extension, flexion, pronation and supination. Two studies reported postoperative ROM in two groups of patients.
Extension
In terms of extension, the results showed the two groups had no statistical differences (WMD = 1.55; 95% CI: -0.22 to 3.31; p = 0.09), and the heterogeneity between the studies was low (I2 = 0%; Figure 9A).
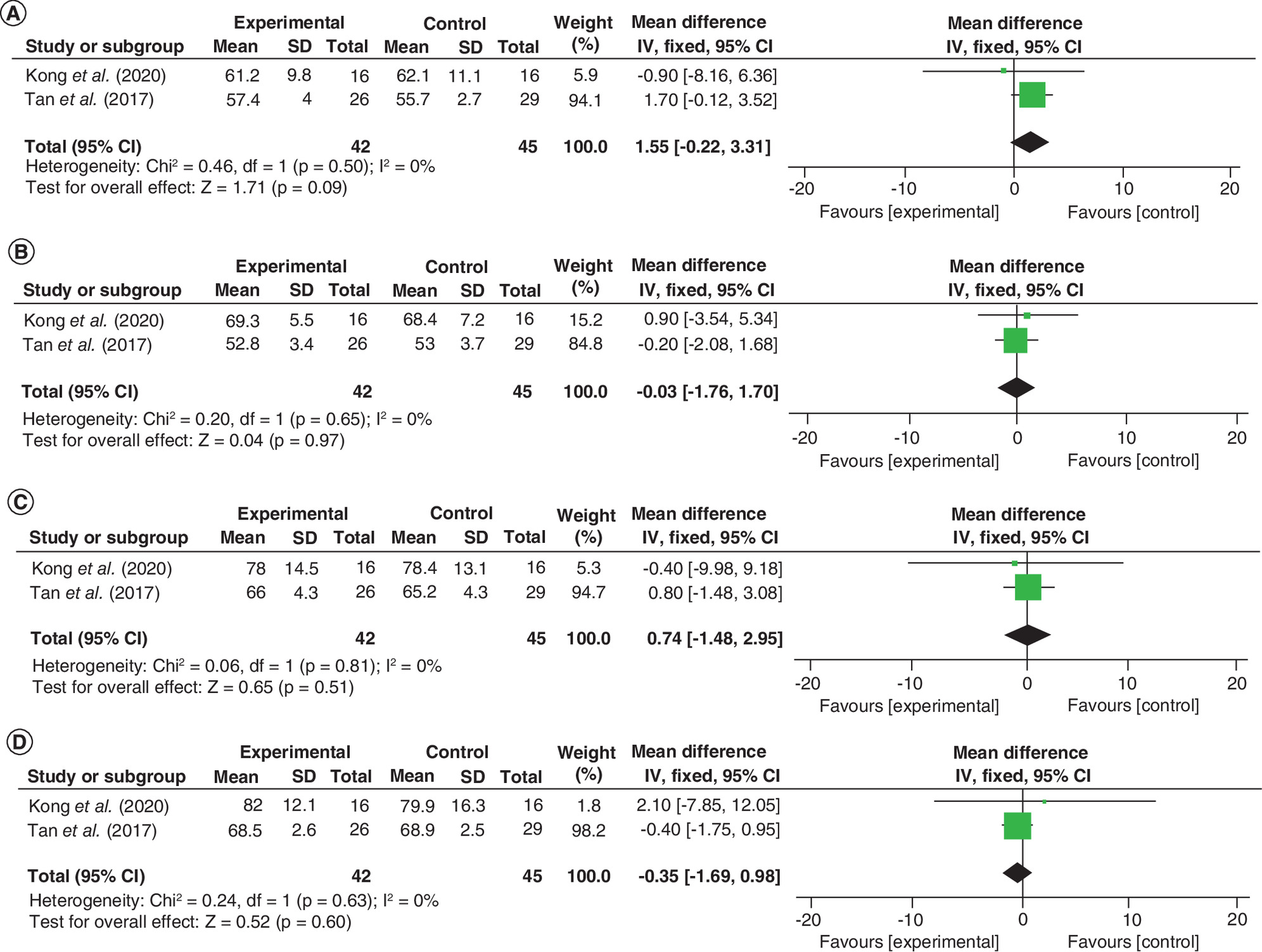
Figure 9. Comparison of range of motion.
(A) Comparison of extension between the 3D printing-assisted surgery group and the routine surgery group. (B) Comparison of flexion between the 3D printing-assisted surgery group and the routine surgery group. (C) Comparison of pronation between the 3D printing-assisted surgery group and the routine surgery group. (D) Comparison of supination between the 3D printing-assisted surgery group and the routine surgery group.
SD: Standard deviation.
Flexion
In terms of flexion, the results showed the two groups had no statistical differences (WMD = -0.03; 95% CI: -1.76 to 1.70; p = 0.97), and the heterogeneity between the studies was low (I2 = 0%; Figure 9B).
Pronation
In terms of pronation, the results showed the heterogeneity between the studies was low (I2 = 0%), and the two groups had no statistical differences (WMD = 0.74; 95% CI: -1.48 to 2.95; p = 0.51; Figure 9C).
Supination
In terms of supination, the results showed the heterogeneity between the studies was low (I2 = 0%), and the two groups had no statistical differences (WMD = -0.35; 95% CI: -1.69 to 0.98; p = 0.60; Figure 9D).
Radiological outcomes
Ulnar deviation
Five studies reported on ulnar deviation [24–26,28,29], and the results showed the two groups had no statistical differences (WMD = 0.36; 95% CI: -0.06 to 0.77; p = 0.09), and the heterogeneity among these studies was low (I2 = 0%; Figure 10A).
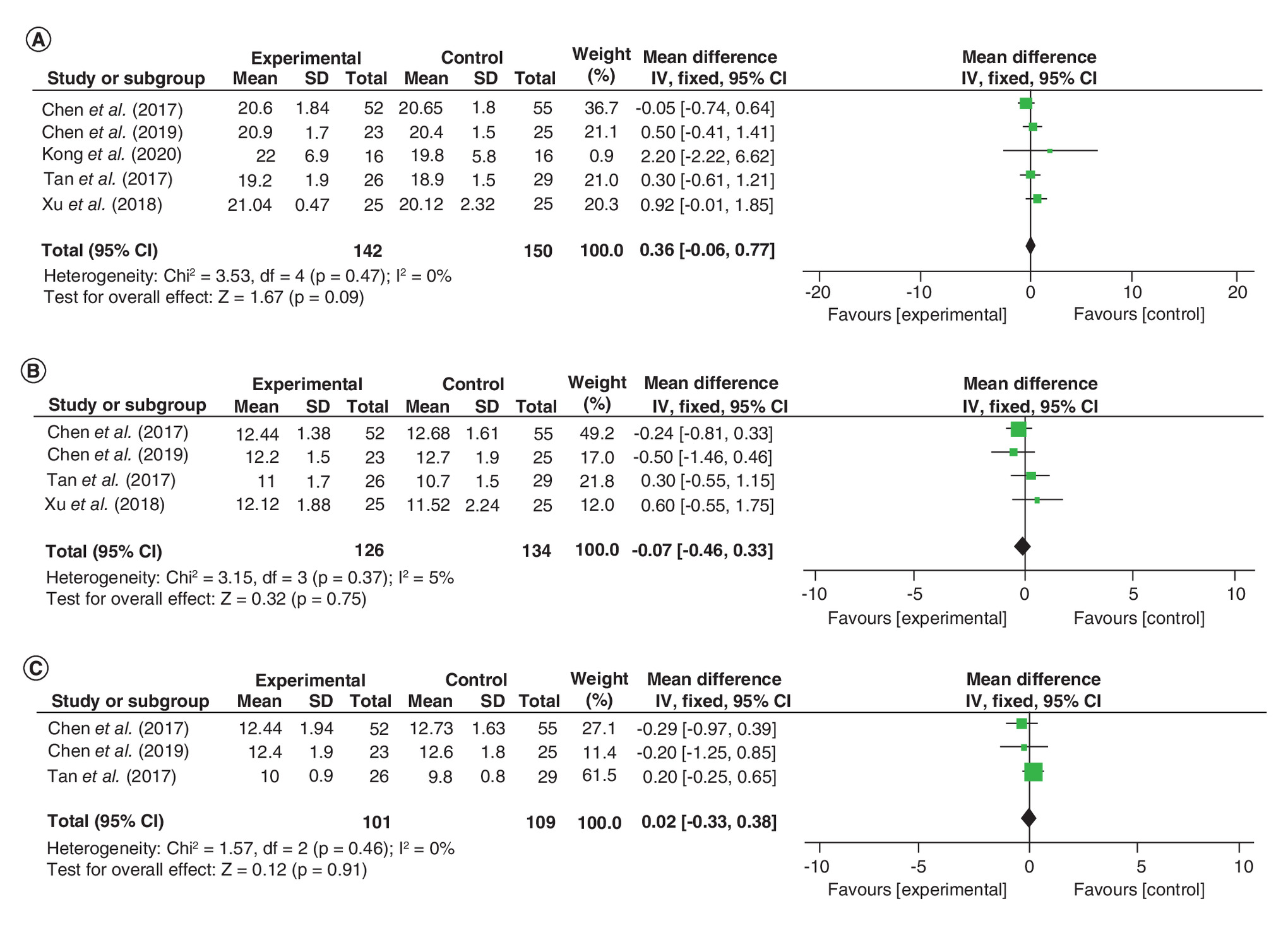
Figure 10. Comparison of radiological outcomes.
(A) Comparison of ulnar deviation between the 3D printing-assisted surgery group and the routine surgery group. (B) Comparison of palmar tilt between the 3D printing-assisted surgery group and the routine surgery group. (C) Comparison of height of the radial styloid process between the 3D printing-assisted surgery group and the routine surgery group.
SD: Standard deviation.
Palmar tilt
Height of the radial styloid process
Sensitivity analysis
Due to the low number of studies relating to some of the results, sensitivity analyses were performed only for operative time, frequency of intraoperative fluoroscopy and blood loss. After excluding a study each time, these results remained stable and the heterogeneity among the studies remained high.
Discussion
Main findings
The results of our meta-analysis found that 3D printing-assisted surgery was better than routine surgery in terms of operation time, frequency of intraoperative fluoroscopy and blood loss. The advantages of 3D printing-assisted surgery included shorter operation time, less frequent intraoperative fluoroscopy and less blood loss.
Unlike long shaft fractures, distal radius fractures are usually more complex because they are often accompanied by comminuted fractures and intra-articular fractures [30,31]. Routine treatment often leads to malunion, so most distal radius fractures require surgery. Radial malunion usually results in difficulty in daily activities and requires corrective surgery [22]. Before using 3D printing technology, surgeons have relied on x-rays and other imaging data to analyze the details of distal radius fractures. These fractures are complex, so inadequate preoperative planning can lead to surgical failure [32]. Inadequate imaging data can lead to poor preoperative planning, which will prolong operation time and increase intraoperative blood loss [33] or even cause soft tissue necrosis and fracture repair failure [34].
3D printing technology allows the creation of a 1:1 fracture model, enabling orthopedic surgeons to simulate the entire surgical processes, fully assess key points to note during surgeries and design the best surgical methods and plans [25]. The surgeons can use the model to prebend the fixed steel plate, reducing operation time and improving the operation effect [35]. In addition, orthopedic surgeons can use 3D-printed models to communicate with the patients before the surgeries, so that the patients can understand the surgical procedures more intuitively, enhance their cognition and confidence in the operations and improve the satisfaction of the patients [36].
Although there is still room for improvement in 3D printing technology, it can promote the development of orthopedic surgery [37]. The increasing costs and expenses of surgery limit the spread and application of the technique [38]. At the same time, expensive 3D printing equipment and complex technical operations have also prevented many hospitals from performing 3D printing-assisted surgical treatment [32]. Many patients in trauma departments are in an emergency and require immediate treatment; however, 3D printing technology requires a certain amount of time to prepare for surgery, so can only be used for patients undergoing elective surgery. In more severe cases of fracture, it is not only necessary to treat the patients with fracture reduction and internal fixation, but also to repair the soft tissue around the fracture as well as nerves and blood vessels [31]. 3D printing cannot currently play a role in these aspects.
Due to the small number of studies involved, the impact of 3D printing on postoperative joint function recovery and reduction of complications has not been reflected. A large number of relevant clinical studies are needed to support a more accurate meta-analysis, depending on the further uptake of 3D printing technology.
Moreover, the clinical heterogeneity of the report is enumerated as follows: nonsurgical factors including 3D printing technology settings, postoperative measures and patient fracture classification; surgical factors including the differences in fracture fixation methods in different studies and the level of orthopedic surgeons.
Limitations
This study was based on five RCTs and one nonRCT to evaluate the efficacy of 3D printing-assisted surgery for distal radius fractures. We enumerate the limitations of the report: the small sample size in these included studies had an impact on obtaining accurate conclusions; in some RCTs, the methods used to generate, allocate, hide, blind and selectively report the results were not described, which may affect the accuracy of the results; we included one nonRCT, which may also influence the accuracy of the results.
Conclusion
This meta-analysis indicated that 3D printing-assisted surgery had shorter operation time, reduced frequency of intraoperative fluoroscopy and less blood loss. In terms of intraoperative results, 3D printing-assisted surgery was found to be better than routine surgery. A large number of more rational RCTs are needed to validate and update the conclusions of this meta-analysis. Increased uptake of 3D printing-assisted surgery may be the future trend of orthopedic surgery.
Future perspective
3D printing technology will become a routine orthopedic surgery auxiliary means in the next 5–10 years. At present, 3D printing technology is developing rapidly. It is believed that with the maturity of this technology, its application in orthopedic surgery will be more extensive.
•
A meta-analysis was conducted and the literature pooled to assess the clinical efficacy of 3D printing technology in surgery for distal radius fractures. Potential academic articles were identified from PubMed, EMBASE, Web of Science, Cochrane Library and other databases. RevMan 5.3 was used to analyze the merged data.
•
The total participants in the 3D printing-assisted surgery group were 157, compared with 165 in the routine surgery group.
•
This meta-analysis found that 3D printing-assisted surgery had shorter operation times, less frequent intraoperative fluoroscopy and less blood loss.
•
However, no difference was found in postoperative visual analogue scores, Gartland–Werley scores, excellent and good rate of wrist function, range of motion and radiological outcomes.
Author contributions
LQ Yan conceived of the design of the study. DM Zhu, J Zhang and Z Zhang participated in the literature search, study selection, data extraction and quality assessment. DM Zhu, DY Chen, B Xie, YZ Shan and PR Liu performed the statistical analysis. DM Zhu finished the manuscript. All authors read and approved the final manuscript.
Acknowledgments
We thank the authors of the included studies for their help.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest
1.
Bentohami A, Bosma J, Akkersdijk GJ, Van Dijkman B, Goslings JC, Schep NW. Incidence and characteristics of distal radial fractures in an urban population in The Netherlands. Eur. J. Trauma Emerg. Surg. 40(3), 357–361 (2014).
2.
Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J. Hand Surg. 26(5), 908–915 (2001).
3.
Kopylov P, Johnell O, Redlund-Johnell I, Bengner U. Fractures of the distal end of the radius in young adults: a 30-year follow-up. J. Hand Surg. 18(1), 45–49 (1993).
4.
Singer BR, Mclauchlan GJ, Robinson CM, Christie J. Epidemiology of fractures in 15,000 adults: the influence of age and gender. J. Bone Joint Surg. Br. 80(2), 243–248 (1998).
5.
Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J. Bone Joint Surg. Am. 93(23), 2146–2153 (2011).
6.
Van Der Vliet QMJ, Sweet AaR, Bhashyam AR et al. Polytrauma and high-energy injury mechanisms are associated with worse patient-reported outcomes after distal radius fractures. Clin. Orthopaed. Relat. Res. 477(10), 2267–2275 (2019).
7.
Armstrong KA, Von Schroeder HP, Baxter NN, Zhong T, Huang A, Mccabe SJ. Stable rates of operative treatment of distal radius fractures in Ontario, Canada: a population-based retrospective cohort study (2004–2013). Can. J. Surg. 62(6), 386–392 (2019).
8.
Aparicio P, Izquierdo Ó, Castellanos J. Conservative treatment of distal radius fractures: a prospective descriptive study. Hand (N Y) 13(4), 448–454 (2018).
9.
Bartl C, Stengel D, Bruckner T, Gebhard F. The treatment of displaced intra-articular distal radius fractures in elderly patients. Dtsch. Arztebl. Int. 111(46), 779–787 (2014).
10.
Bilgin SS, Armangil M. Correction of nascent malunion of distal radius fractures. Acta Orthop. Traumatol. Turc. 46(1), 30–34 (2012).
11.
Arora R, Lutz M, Hennerbichler A, Krappinger D, Espen D, Gabl M. Complications following internal fixation of unstable distal radius fracture with a palmar locking-plate. J. Orthop. Trauma 21(5), 316–322 (2007).
12.
Henry M. Vascularized medial femoral condyle bone graft for resistant nonunion of the distal radius. J. Hand Surg. Asian Pac. Vol. 22(1), 23–28 (2017).
13.
Jones CW, Lawson RD. One size does not fit all: distal radioulnar joint dysfunction after volar locking plate fixation. J. Wrist Surg. 3(1), 42–45 (2014).
14.
Rosenauer R, Pezzei C, Quadlbauer S et al. Complications after operatively treated distal radius fractures. Arch. Orthop. Trauma Surg. 140(5), 665–673 (2020).
15.
Bagaria V, Bhansali R, Pawar P. 3D printing- creating a blueprint for the future of orthopedics: current concept review and the road ahead!. J. Clin. Orthop. Trauma 9(3), 207–212 (2018).
16.
Honigmann P, Thieringer F, Steiger R, Haefeli M, Schumacher R, Henning J. A simple 3-dimensional printed aid for a corrective palmar opening wedge osteotomy of the distal radius. J. Hand Surg. 41(3), 464–469 (2016).
17.
Bizzotto N, Tami I, Tami A et al. 3D printed models of distal radius fractures. Injury 47(4), 976–978 (2016).
18.
Bauer AS, Storelli DaR, Sibbel SE, Mccarroll HR, Lattanza LL. Preoperative computer simulation and patient-specific guides are safe and effective to correct forearm deformity in children. J. Pediatric Orthop. 37(7), 504–510 (2017).
19.
Ma B, Kunz M, Gammon B, Ellis RE, Pichora DR. A laboratory comparison of computer navigation and individualized guides for distal radius osteotomy. Int. J. Comput. Assist. Radiol. Surg. 9(4), 713–724 (2014).
20.
Michielsen M, Van Haver A, Vanhees M, Van Riet R, Verstreken F. Use of three-dimensional technology for complications of upper limb fracture treatment. EFORT Open Rev. 4(6), 302–312 (2019).
21.
Roner S, Carrillo F, Vlachopoulos L, Schweizer A, Nagy L, Fuernstahl P. Improving accuracy of opening-wedge osteotomies of distal radius using a patient-specific ramp-guide technique. BMC Musculoskelet. Disord. 19(1), 374 (2018).
22.
Shintani K, Kazuki K, Yoneda M et al. Computer-assisted three-dimensional corrective osteotomy for malunited fractures of the distal radius using prefabricated bone graft substitute. J. Hand Surg. Asian Pac. Vol. 23(4), 479–486 (2018).
23.
Storelli DA, Bauer AS, Lattanza LL, Mccarroll HR. The use of computer-aided design and 3-dimensional models in the treatment of forearm malunions in children. Tech. Hand Up. Extrem. Surg. 19(1), 23–26 (2015).
24.
Chen C, Cai L, Zhang C, Wang J, Guo X, Zhou Y. Treatment of die-punch fractures with 3D printing technology. J. Invest. Surg. 31(5), 385–392 (2018).
• A relatively high-quality clinical trial used for this meta-analysis.
25.
Chen C, Cai L, Zheng W, Wang J, Guo X, Chen H. The efficacy of using 3D printing models in the treatment of fractures: a randomised clinical trial. BMC Musculoskelet. Disord. 20(1), 65 (2019).
• A relatively high-quality clinical trial used for this meta-analysis.
26.
Kong L, Yang G, Yu J et al. Surgical treatment of intra-articular distal radius fractures with the assistance of three-dimensional printing technique. Medicine 99(8), e19259 (2020).
• A relatively high-quality clinical trial used for this meta-analysis.
27.
Luo W, Wu S, Chen JK, Deng YJ. Application value of 3D printing technique in the treatment of comminuted fracture of distal radius. CJCM 10(24), 125–127 (2018).
• A relatively high-quality clinical trial used for this meta-analysis.
28.
Tan X. Clinical application and research of 3-D printing technology in the treatment of distal radius fracture. Guangxi Medical University (2017). https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CMFD&dbname=CMFD201702&filename=1017202467.nh&v=MDY5MzMzcVRyV00xRnJDVVI3cWZiK2R1RkN2bFVMekJWRjI2R2JHNEhOWEtxSkViUElSOGVYMUx1eFlTN0RoMVQ=
• A relatively high-quality clinical trial used for this meta-analysis.
29.
Xu S, Gu H, He Y, Huang G, Zhang ZQ, Lu W. Application of 3D printing in reduction and internal fixation for treatment of distal radius fractures. Chin. Orthop. J. Clin. Basic Res. 10(3), 133–139 (2018).
• A relatively high-quality clinical trial used for this meta-analysis.
30.
Biondi M, Keller M, Merenghi L, Gabl M, Lauri G. Hook plate for volar rim fractures of the distal radius: review of the first 23 cases and focus on dorsal radiocarpal dislocation. J. Wrist Surg. 8(2), 93–99 (2019).
31.
Cook A, Baldwin P, Fowler JR. Incidence of flexor pollicis longus complications following volar locking plate fixation of distal radius fractures. Hand (NY) (2019) (Epub ahead of print).
32.
Jinsihan N, Jin G. Recent developments of 3d-printing technique assisted surgery in the management of complex fractures. Int. J. Clin. Exp. Med. 11(11), 11578–11583 (2018).
33.
Zhou J, Tang W, Li D, Wu Y. Morphological characteristics of different types of distal radius die-punch fractures based on three-column theory. J. Orthop. Surg. Res. 14(1), 390 (2019).
34.
Zhou Y, Zhu Y, Zhang X, Tian D, Zhang B. Comparison of radiographic and functional results of die-punch fracture of distal radius between volar locking plating (VLP) and external fixation (EF). J. Orthop. Surg. Res. 14(1), 373 (2019).
35.
Han Q, Qin Y, Zou Y et al. Novel exploration of 3D printed wrist arthroplasty to solve the severe and complicated bone defect of wrist. Rapid Prototyping J. 23(3), 465–473 (2017).
36.
Kim SJ, Jo YH, Choi WS et al. Biomechanical properties of 3-dimensional printed volar locking distal radius plate: comparison with conventional volar locking plate. J. Hand Surg. 42(9), 747.e741–747.e746 (2017).
37.
Inge S, Brouwers L, Van Der Heijden F, Bemelman M. 3D printing for corrective osteotomy of malunited distal radius fractures: a low-cost workflow. BMJ Case Rep. (2018) (Epub ahead of print).
38.
Wan S-X, Meng F-B, Zhang J, Chen Z, Yu L-B, Wen J-J. Experimental study and preliminary clinical application of mini-invasive percutaneous internal screw fixation for scaphoid fracture under the guidance of a 3D-printed guide plate. Curr. Med. Sci. 39(6), 990–996 (2019).
Information & Authors
Information
Published In
Pages: 919 - 931
PubMed: 32969712
Copyright
© 2020 Future Medicine Ltd.
History
Received: 6 June 2020
Accepted: 3 August 2020
Published online: 24 September 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The efficacy of 3D printing-assisted surgery in treating distal radius fractures: systematic review and meta-analysis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0099
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ramazan Kurul, Busra Inal, Murat Diramali, Hamza Ozer, Kevser Ezgi Erdogan, Evaluating the educational impact of tomography-based high-resolution 3D-printed distal radius fracture models, BMC Medical Education, 10.1186/s12909-025-08164-w, 25, 1, (2025).
- Emilia Gryska, Dimitrios Zarkadas, Charlotte Stor Swinkels, Katleen Libberecht, Anders Björkman, Patient-specific plates for distal radius osteotomy: a review of the literature and a parametric plate design concept, Expert Review of Medical Devices, 10.1080/17434440.2025.2519477, 22, 8, (881-888), (2025).
- François Lintz, Enrico Pozzessere, Wolfram Grün, Antoine Acker, Erik Jesús Huánuco Casas, Eric Ferkel, Cesar de Cesar Netto, A Hallux Valgus Surgical Planning Survey Using WBCT-based 3D Printing, Foot & Ankle Orthopaedics, 10.1177/24730114251325854, 10, 1, (2025).
- Lin Xiao, Peiyuan Tang, Shengwu Yang, Jingyue Su, Wenbo Ma, Han Tan, Ying Zhu, Wenfeng Xiao, Ting Wen, Yusheng Li, Shuguang Liu, Zhenhan Deng, Comparing the efficacy of 3D-printing-assisted surgery with traditional surgical treatment of fracture: an umbrella review, Journal of Orthopaedics and Traumatology, 10.1186/s10195-025-00819-0, 26, 1, (2025).
- 嘉文 梁, Advances in 3D Printing Technology in Orthopedics, Advances in Clinical Medicine, 10.12677/acm.2025.1572103, 15, 07, (1133-1139), (2025).
- Lisanne J. M. Roelofs, Nick Assink, Joep Kraeima, Kaj ten Duis, Job N. Doornberg, Jean-Paul P. M. de Vries, Anne M. L. Meesters, Frank F. A. IJpma, Clinical Application of 3D-Assisted Surgery Techniques in Treatment of Intra-Articular Distal Radius Fractures: A Systematic Review in 718 Patients, Journal of Clinical Medicine, 10.3390/jcm13237296, 13, 23, (7296), (2024).
- Chaoran Hu, Bing Qiu, Chaode Cen, Qin Luo, Yongfei Cao, 3D printing assisted MIPO for treatment of complex middle-proximal humeral shaft fractures, BMC Musculoskeletal Disorders, 10.1186/s12891-024-07202-w, 25, 1, (2024).
- Lily X. LI, Angela E. KEDGLEY, Maxim D. HORWITZ, A Review of the Use of 3D Printing Technology in Treatment of Scaphoid Fractures, The Journal of Hand Surgery (Asian-Pacific Volume), 10.1142/S2424835523500042, 28, 01, (22-33), (2023).
- Lea Wood, Zubair Ahmed, Does using 3D printed models for pre-operative planning improve surgical outcomes of foot and ankle fracture fixation? A systematic review and meta-analysis, European Journal of Trauma and Emergency Surgery, 10.1007/s00068-022-02176-7, 50, 1, (21-35), (2022).
- Kai Li, Zhendong Liu, Xiaolei Li, Jingcheng Wang, 3D printing-assisted surgery for proximal humerus fractures: a systematic review and meta-analysis, European Journal of Trauma and Emergency Surgery, 10.1007/s00068-021-01851-5, 48, 5, (3493-3503), (2022).