Health state utilities in patients with advanced non-small-cell lung cancer in China
Abstract
Aim: Non-small-cell lung cancer (NSCLC) is a leading global health threat that impairs patient health outcomes. Health state utilities are fundamental values in economic evaluation and significantly vary across countries. Given the scarce data on the Chinese population, the current study measured utility values in the Chinese patients with NSCLC. Methods: This study was conducted as a cross-sectional survey of patients with advanced NSCLC at the Shanghai Chest Hospital. Utility values were assessed using the EuroQol five-dimension (EQ-5D) instrument and scored based on the Chinese-specific value algorithm. Predictors of utility values were examined using a subgroup analysis and a multiple regression model. Results: The mean EQ-5D utility value of recruited patients was 0.814. The regression analysis revealed that tumor stage, treatment regimen and line of therapy were the potential predictors of utility values. Conclusion: This study provides the Chinese-specific health utility data for advanced NSCLC using the EQ-5D.
The measurement of health states is fundamental to cost-utility analyses in economic evaluation [1]. Health state utilities are used for calculating quality-adjusted life-years, which combine survival outcomes and quality of life. Health utility values are regarded as useful in health economics for their role as a suitable instrument in the quality-adjusted life-year model [2]. The EuroQol five-dimension (EQ-5D) questionnaire is a standardized and generic instrument that describes and rates health states [3]. EQ-5D scores can be calculated based on respondents’ descriptions of their current health states using a value set elicited from the general population. The scores represent social valuation of the respondents’ own health states [4,5].
Lung cancer is the leading cause of cancer-related death worldwide, with approximately 1.8 million new cases and 1.6 million deaths per year [6]. Non-small-cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer cases [7]. According to a population-based study in China, the incidence of NSCLC was 54.20 per 100,000 people, however, it was 42.6 per 100,000 people for the US population in 2011 [8]. This indicated that the disease becomes a major threat to health in China. Given the progress in health technologies over the past decade, there are now more options for the treatment of NSCLC. Newly emerged chemotherapy agents and targeted anticancer drugs can improve patient survival and health-related quality of life (HRQOL) [9–11]. Several studies have elicited health utilities in NSCLC using generic preference measures [12–16]. Although those studies assessed the symptom burden on patients, few discussed the effects of different treatment strategies. In addition, these data were derived from the western population, and there is still an absence of Chinese-specific data calculated by the Chinese population-based EQ-5D value set. Due to the potential difference in health preferences between western and eastern regions [17], local utility values of a disease are necessary when conducting local health economic evaluations.
In China, the use of preference instruments (e.g., the EQ-5D questionnaire) has been restricted for decades, which is one of the major reasons for the lack of sufficient economic research on health utilities [18]. The EQ-5D questionnaire has been used to examine HRQOL in patients with different diseases worldwide. The China Guidelines for Pharmacoeconomic Evaluations 2011 recommended the EQ-5D questionnaire for health technology assessments in this country [19]. The EQ-5D self-report questionnaire's descriptive system has been validated in the Chinese populations [20]; however, its application was previously restricted because of the lack of a Chinese value set. Recently, researchers have provided effective methods to calculate EQ-5D utility values for the Chinese population. Therefore, this paper sought to measure utility values among patients with advanced NSCLC and assess the predictors of utility values based on the Chinese EQ-5D value sets established by Liu GG et al. [21].
Methods
Patient selection & data collection
This study was designed as a cross-sectional survey of patients with advanced NSCLC. We enrolled patients who were treated in one medical ward of Lung Cancer Clinical Medical Centers, Shanghai Chest Hospital, China, from January to June 2016. Our hospital specializes in the diagnosis and treatment of lung cancer, admitting nearly 40,000 inpatients and treating more than 300,000 outpatients with this disease per year.
The patients were eligible for the study if they had clinical stage III or IV NSCLC and were ineligible for surgery and received drug treatment for lung cancer within the last month. The patients who did not meet the above criteria were excluded. Finally, of the 235 recruited patients with advanced NSCLC, 232 (98.7%) completed the EQ-5D questionnaire and were involved in the analysis (Figure 1). The patients who did not complete questionnaires (n = 3) were directly deleted. All study participants signed informed consent documents after the nature of the research was explained to them.
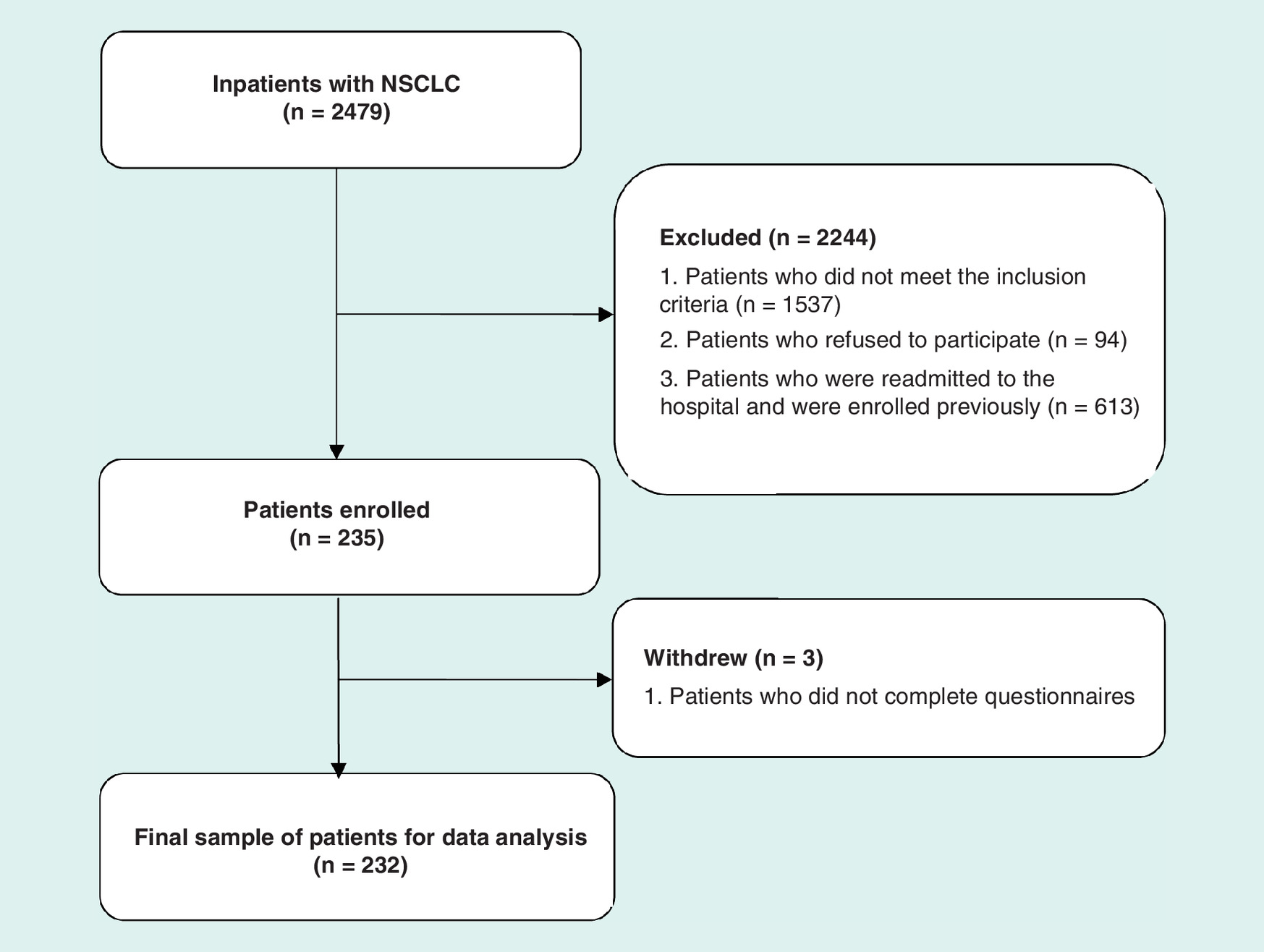
Figure 1. Flow chart of patient recruitment and withdrawal.
A total of 2479 patients were diagnosed with non-small-cell lung cancer (NSCLC). A final sample of 232 patients was eligible for analysis.
The data used for the analysis were obtained from in-person interviews with the patients and from their physician-written medical records. The enrolled patients completed the paper questionnaires regarding HRQOL on admission and only included once in the study. Questionnaires were completed in private space at appropriate time to avoid interference. Two trained investigators (Yunjie Shen and Xiaohui Wang) provided assistance to the patients when necessary (e.g., to read questions aloud for those who could not read, however, their answers must be confirmed repeatedly in order to reduce bias). The investigators completed a patient chart review to collect clinical information. We collected the following patient and disease characteristics from the medical records: age, gender, clinical stage, histology, previous treatment, line of treatment, response evaluation criteria in solid tumors and adverse effects. Microsoft Excel was used to store the answers to the questionnaires and chart review data for subsequent management.
Ethics approval & consent to participate
All the patients were fully informed of the study and provided written informed consent. The protocol was approved by the ethics committees of Shanghai Chest Hospital (reference number: KS(Y) 1718).
Questionnaire
The EQ-5D questionnaire is used to measure the health outcomes worldwide because of its brevity and convenience for self-completion; it also has proven discriminative and valuable for lung cancer and lung disease [12,22]. The EQ-5D questionnaire measures health status based on five dimensions: mobility, self-care, usual activity, pain/discomfort and anxiety/depression. The patients were asked to rate their level of severity for each dimension as one (no health problems), two (some health problems), or three (extreme health problems). As a result, the patients’ health statuses were described by combining the different levels of each dimension. The EQ-5D utility score was generated by converting the above health statuses into a societal preference weight. Many countries have developed value sets (i.e., preference weights) for their own population. In this study, we adopted a China-specific value based on the general population of China using the time trade-off method that was recently published to score the EQ-5D questionnaire [21].
Statistical analysis
We initially analyzed patient/disease characteristics using descriptive statistics. Means and standard deviations (SDs) were used to describe the continuous variables, and the number of cases and proportions were used to describe the categorical variables. We compared means and case numbers using Student's t-test or one-way analysis of variance where appropriate [23].
To compare the HRQOL (which differed among subgroups of patients) assessed by the utility scores, we grouped patients based on their characteristics (e.g., age, gender, clinical stage, histology, treatment modality [i.e., chemotherapy, targeted therapy, or a combination] and line of treatment). Third-line or later treatments were be merged into one group since there is still no clear standard of treatment options for the patients in these lines treatments. We conducted additional analyses by grouping the patients into the following three categories: the pemetrexed-included chemotherapy group, the nonpemetrexed-included chemotherapy group and the targeted therapy group, on the grounds that the treatments were considered different in the novelty and adverse drug reactions. We examined utility by treatment groups based on the assumption that adverse events have significant effects on HRQOL and differ among regimens [12]. The percentage of patients who had problems in each EQ-5D functional domain was also calculated. A χ2 test was applied to test differences among the EQ-5D dimensions, and one-way analysis of variance was used to compare the utility scores [23,24].
Finally, a stepwise multiple linear regression model was used to investigate the utility determinants [25]. The utility score was considered the dependent variable. The following variables were assigned values as possible explanatory variables: age (entered the analysis as a continuous variable), gender (men = 1, women = 0) and disease stage (stage IV = 1, stage III = 0). The dummy variables were included to analyze the treatment regimen (dummy treatment 1: nonpemetrexed-included chemotherapy = 1, otherwise 0; dummy treatment 2: pemetrexed-included chemotherapy = 1, otherwise 0; dummy treatment 3: targeted therapy = 1, otherwise 0; dummy treatment 4: combined therapy = 1, otherwise 0), and current line of treatment (dummy line 1: first-line = 1, otherwise 0; dummy line 2: second-line = 1, otherwise 0; dummy line 3: third- or later-line = 1, otherwise 0; dummy line 4: maintenance = 1, otherwise 0). Because different subtypes of NSCLC probably lead to different treatment options, histology was not included in the step-wise regression analysis to avoid inter-relationship. The interaction of pemetrexed-included chemotherapy and first-line was also included in the multifactor analysis because it was relevant in the independent variable correlation analysis (correlation coefficient >0.2). Insignificant co-variates were removed via backward elimination, and the full model and the final model are both presented.
All analyses were performed using Stata 13.0 for Windows (StataCorp., TX, USA). A p-value < 0.05 was considered statistically significant.
Results
Study population
The mean age of these patients was 59.9 years (range = 27–82 years). Approximately 65.5% of the sample was male. The majority (74.6%) of the participants were classified as stage IV, whereas 16.8% were classified as stage IIIb, and 6.9% were classified as stage IIIa. Approximately 72% of the patients were diagnosed with adenocarcinoma, and 15.5% were diagnosed with squamous cell carcinoma. Most patients (65.5%) were treated with chemotherapy, 28% were treated with targeted therapy, 3.4% were treated with combined chemotherapy and radiotherapy and 3% were treated with combined chemotherapy and targeted therapy. However, due to the small sample size of the combined chemotherapy and radiotherapy as well as the combined chemotherapy and targeted therapy, we grouped them together in subsequent analyses. Approximately 56.9% of the patients received a first-line treatment at the time of questionnaire completion. The patient characteristics for the study population are listed in Table 1.
| Characteristics | n = 232 (100%) |
|---|---|
| Age (years): | |
| – Mean (SD) | 59.9 (9.0) |
| – Range | 27–82 |
| Gender: | |
| – Male | 152 (65.5%) |
| – Female | 80 (34.5%) |
| Clinical stage: | |
| – IIIa | 16 (6.9%) |
| – IIIb | 39 (16.8%) |
| – IV | 173 (74.6%) |
| Not available/missing | 4 (1.7%) |
| Histology: | |
| – Adenocarcinoma | 167 (72.0%) |
| – Squamous cell carcinoma | 36 (15.5%) |
| – Other | 29 (12.5%) |
| Treatment: | |
| – Chemotherapy | 152 (65.5%) |
| – Pemetrexed-included chemotherapy | 89 (38.4%) |
| – Nonpemetrexed-included chemotherapy | 63 (27.1) |
| – Targeted therapy | 65 (28.0%) |
| – Combined chemotherapy and radiotherapy | 8 (3.5%) |
| – Combined chemotherapy and targeted therapy | 7 (3.0%) |
| Line of treatment: | |
| – First | 132 (56.9%) |
| – Second | 53 (22.8%) |
| – Third or later | 30 (12.9%) |
| – Maintenance | 17 (7.3%) |
SD: Standard deviation.
Utility scores
The health state results are presented in Table 2 and Figure 2. The mean EQ-5D utility score for the 232 patients was 0.814 (SD = 0.165). The subgroup analyses revealed that elderly patients had higher EQ-5D utility scores (p < 0.05). The utility scores significantly differed among the patients who received different lines of treatment (p < 0.01). The utility scores were highest for the patients receiving first-line treatments and lowest for patients receiving third- or later-line treatments. Moreover, as expected, the mean utility score of patients in stage IV was lower than that of those in stage III (p < 0.01).
| Patient characteristics | n | Mean (SD) | p-value |
|---|---|---|---|
| Age: | 0.046 | ||
| – <60 years | 108 | 0.794 (0.181) | |
| – ≥60 years | 124 | 0.831 (0.149) | |
| Gender: | 0.168 | ||
| – Male | 152 | 0.821 (0.169) | |
| – Female | 80 | 0.800 (0.157) | |
| Clinical stage: | 0.0001 | ||
| – III | 55 | 0.886 (0.090) | |
| – IV | 173 | 0.791 (0.177) | |
| Histology: | 0.077 | ||
| – Adenocarcinoma | 167 | 0.807 (0.173) | |
| – Squamous cell carcinoma | 36 | 0.868 (0.092) | |
| – Other | 29 | 0.785 (0.180) | |
| Treatment: | 0.0001 | ||
| – Chemotherapy | 152 | 0.838 (0.144) | |
| – Targeted therapy | 65 | 0.787 (0.186)† | |
| – Combined therapy | 15 | 0.678 (0.195) | |
| Line of treatment: | 0.0001 | ||
| – First | 132 | 0.856 (0.135) | |
| – Second | 53 | 0.768 (0.173) | |
| – Third or later | 30 | 0.703 (0.198) | |
| – Maintenance | 17 | 0.825 (0.178) | |
The variables were examined using Student's t-test or one-way analysis of variance (ANOVA).
†p > 0.05 when compared with the chemotherapy group.
SD: Standard deviation.
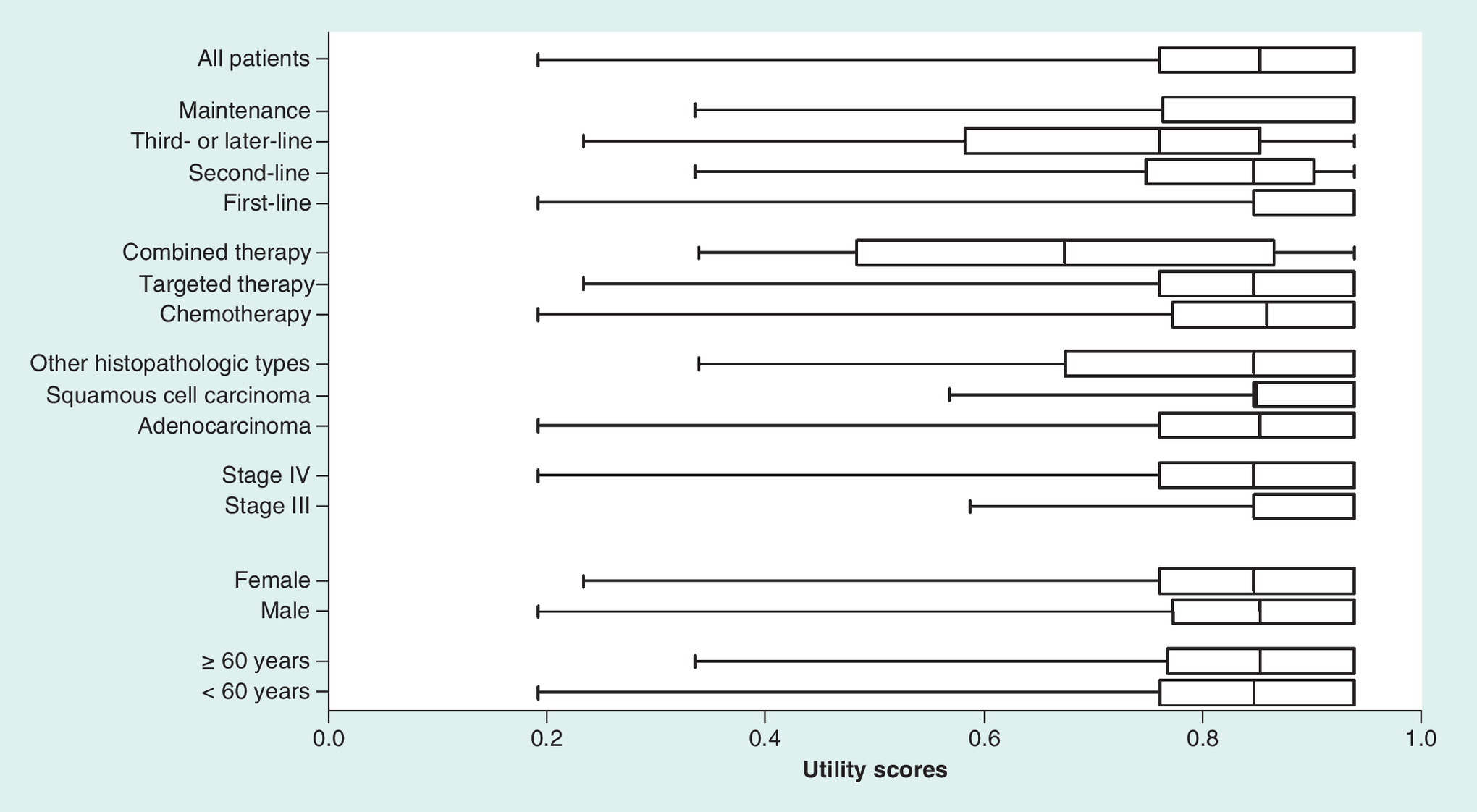
Figure 2. Boxes plot of EQ-5D utility scores for the 232 patients.
The boxes represent the range between the 25th and 75th percentiles, the inner lines in boxes represent the median, and the whiskers represent the minimum and maximum values.
Most patients were treated with chemotherapy alone and showed a higher mean utility score (0.838 ± 0.144) than those treated using other regimens (p < 0.01). However, a direct comparison between the chemotherapy and targeted therapy groups did not reveal a significant difference (p > 0.05).
Subgroup analyses by gender and tumor histology did not reveal significant differences (p > 0.05).
Analysis by treatment groups
The patients receiving different lines of treatment varied with regard to their health status. Taking this result and the sample size into account, patients receiving first line treatments were selected for a further study that will examine the influence of detailed treatment regimens.
Table 3 shows the effect of treatment regimen on the EQ-5D utility score and its five functional domains among patients receiving first-line treatments. The patients in the combined therapy group, whose utility scores were considered difficult to evaluate because of the low sample size, were excluded.
| EQ-5D utility scores and dimension | Treatment regimen | p-value | ||
|---|---|---|---|---|
| Pemetrexed-included chemotherapy | Non-pemetrexed-included chemotherapy | Targeted therapy | ||
| EQ-5D utility scores: mean (SD); n = 127† | 0.877 (0.110); n = 65 | 0.823 (0.148); n = 36 | 0.892 (0.120); n = 26 | 0.052 |
| EQ-5D dimension: the number and proportion of patients having any problems‡, n = 127 (100%) | ||||
| Mobility | 7 (10.77%) | 5 (13.89%) | 1 (3.85%) | 0.428 |
| Self-care | 3 (4.62%) | 2 (5.56%) | 1 (3.85%) | 0.951 |
| Usual activities | 7 (10.77%) | 8 (22.22%) | 1 (3.85%) | 0.081 |
| Pain/discomfort | 19 (29.23%) | 18 (50.00%) | 6 (23.08%) | 0.046 |
| Anxiety/depression | 7 (10.77%) | 11 (30.56%) | 3 (11.54%) | 0.028 |
The utility scores were examined using one-way analysis of variance (ANOVA), and the differences among the EQ-5D dimensions were compared using a χ2 test.
†The total number of patients analyzed in this table is 127. The combined therapy group is not included.
‡Patients who reported some problems (level 2) and extreme problems (level 3) for EQ-5D dimensions.
EQ-5D: EuroQol five-dimension; SD: Standard deviation.
Among the remaining three groups of patients, those patients treated with nonpemetrexed-included chemotherapy reported the lowest EQ-5D values and the highest proportion of problems across all five dimensions. The majority of the patients did not report difficulties in the dimensions of mobility, self-care and usual activities, and no significant differences were observed among the groups with regard to these dimensions (p > 0.05). However, significant differences were observed with regard to the pain/discomfort and anxiety/depression dimensions of the EQ-5D (p < 0.05). The patients who received targeted therapy had the lowest pain/discomfort impairments, whereas those who received pemetrexed-included chemotherapy reported similar values on the anxiety/depression dimension and a lower proportion of problems than those who received nonpemetrexed-included chemotherapy.
Health utility-influencing factors
As Table 4 shows, the regression model revealed that pemetrexed-included chemotherapy was associated with significant gains in utility, whereas combined therapy, second- or later-line treatments and stage IV were significant and negative predictors of EQ-5D utility scores (all p < 0.05). None of the following variables predicted the utility scores: age, gender, nonpemetrexed-included chemotherapy, targeted therapy, first-line treatment, maintenance therapy, or the examined interaction.
| Variable | Full model | Trimmed model | ||||
|---|---|---|---|---|---|---|
| Parameter estimate | SE | p-value | Parameter estimate | SE | p-value | |
| Intercept | 0.841 | 0.077 | 0.0001 | 0.873 | 0.021 | 0.0001 |
| Age | 0.0006 | 0.001 | 0.587 | NS | NS | NS |
| Gender (male) | -0.001 | 0.022 | 0.957 | NS | NS | NS |
| Clinical stage (stage IV) | -0.067 | 0.024 | 0.005 | -0.067 | 0.023 | 0.004 |
| Pemetrexed-included chemotherapy | 0.125 | 0.039 | 0.002 | 0.063 | 0.021 | 0.003 |
| Targeted therapy | 0.020 | 0.027 | 0.466 | NS | NS | NS |
| Combined therapy | -0.090 | 0.043 | 0.039 | -0.102 | 0.041 | 0.013 |
| Second-line treatment | -0.093 | 0.031 | 0.003 | -0.062 | 0.024 | 0.012 |
| Third- or later-line treatment | -0.117 | 0.034 | 0.001 | -0.099 | 0.031 | 0.002 |
| Maintenance treatment | -0.019 | 0.043 | 0.650 | NS | NS | NS |
| Interaction between pemetrexed-included chemotherapy and first-line | -0.078 | 0.045 | 0.086 | NS | NS | NS |
| Adjusted R2 | 0.182 | – | – | 0.186 | – | – |
SE: Standard error; NS: Not significant.
Discussion
This cross-sectional study measured health state utilities in the Chinese patients with advanced NSCLC using the EQ-5D instrument. Based on our data, the utility scores for these patients decreased with additional lines of treatment. This finding is in line with the result of another study [14]. Moreover, the current study showed the influence of different treatment regimens on health utility scores. To the best of our knowledge, this study is the first to measure the health state utility of patients with NSCLC using a Chinese population-based EQ-5D social value set.
The mean health state utility score of the patients who completed the questionnaire in this study was 0.814 (SD = 0.165), which indicates that these patients were in good health on average. This value was slightly higher than that reported in previous studies in other countries, such as that reported by Grutters et al. [12] in the UK population consisting of 245 patients with NSCLC (0.74). In a study by Nafees et al. [17] that also measured EQ-5D utility scores from the Chinese patients with NSCLC, the utility for tumor disease state was 0.804. This discrepancy may have arisen because of the method of elicitation as well as new treatments and drugs. The results of our study showed that patients under 60 years old had lower utility scores than those over 60 years old, and this finding is difficult to explain. Based on our understanding, NSCLC develops violently and progresses suddenly in younger patients. In addition, younger patients typically expect to have better health than do the elderly, given their higher baseline health status before their illness. These occurrences may have contributed to the lower utility scores among younger patients.
A subgroup analysis based on treatment revealed significantly different utility scores among the chemotherapy, targeted therapy and combined therapy groups, although a paired comparison did not reveal significant results between the targeted therapy and chemotherapy groups. Among the patients who received first-line therapy, patients who received targeted therapy showed the highest utility scores (p > 0.05) and reported the fewest problems in the pain/discomfort dimension, in which impairments were most often reported (p < 0.05). According to the regression analysis, treatment regimen and line of therapy were important predictors of health state utility.
The findings from this study are partially consistent with those from previous studies. Chouaid et al. [14] conducted a cross-sectional survey on 390 patients in four countries with advanced NSCLC. The results indicated that the disease had a significant effect on patients’ health states. The presence of a stage IV progressive disease and higher lines of treatment contributed to the deterioration in utility. Grutters et al. [12] included 260 patients with NSCLC in another study. These researchers examined the influence of disease stage, adverse events, initial treatment and tumor recurrence on HRQOL. Adverse events had a significant effect; thus, that study stressed the necessity of proper treatment. The present study did not discuss adverse events because the data collected were insufficient for this analysis. Many cases may have been under-recognized and under-reported because of the brief hospitalization time. Therefore, future studies should explore the role of adverse events further. Nafees et al. [17] recently studied the utility scores of the local populations in several countries, including the UK, France, Australia, South Korea, Taiwan and China. As that study showed, utilities were country-specific. This finding emphasizes the importance of using local data to reflect the preferences of a local population. However, none of these studies explored the influence of NSCLC subtypes, treatment regimen, or (in particular) new, targeted drugs. Therefore, the current study sought to assess the predictive factors of utility values, providing important and relevant insights.
The current study has several limitations. First, because of its lack of randomization, this study showed risk of selection bias. However, we addressed this weakness by applying stratification to the subgroup analyses. Second, a priori sample size calculation was lacking in this paper. This sample size calculation was absent because of the primary and exploratory nature of this study, which aimed to assess health utilities in Chinese patients and provide a reference for further research. We determined the sample size based a similar previous study [12,13]. Third, because of the lack of adverse events reports, this study did not analyze the relationship between adverse reactions and HRQOL. This analysis should be performed in future studies. Fourth, the calculated utility values based on the EQ-5D questionnaire might have been overestimated because specific symptoms of lung cancer might not distinctly affect the EQ-5D dimensions [14]. Recently, researchers have sought to develop mapping algorithms to enable disease-specific instruments, such as the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30), to be converted to the EQ-5D utility index [26–28]. Mapping approaches are often used for economic evaluations when a generic instrument is not available. In the future, we will examine this approach further.
Conclusion
The results from the current study demonstrate that tumor stage, therapy line and treatment regimen are associated with health utilities in advanced NSCLC. Future investigations regarding the potential benefits of novel therapeutic techniques among patients with lung cancer are critical. Furthermore, the values used to measure health states will be helpful for future economic research related to NSCLC in China.
Health state utilities are used for calculating the quality-adjusted life-year, which are fundamental in economic evaluation. However, Chinese utility data of non-small-cell lung cancer (NSCLC) are few.
This study measured utility values among Chinese patients with advanced NSCLC and assessed the impact factors.
Utility values were assessed using the EuroQol five-dimension (EQ-5D) instrument and scored based on the Chinese-specific value algorithm. Predictors of utility values were examined using a subgroup analysis and a multiple linear regression model.
A total of 232 patients with advanced NSCLC were recruited, and their mean EQ-5D utility value was 0.814.
Subgroup analyses showed that age, tumor stage and treatment patterns had no tumor impacts on utility values (p < 0.05).
The regression analysis demonstrated that tumor stage, therapy line and treatment regimen are the potential predictors of the health utilities in advanced NSCLC.
This study provides Chinese-specific health utility data for advanced NSCLC using the EQ-5D. These results will be valuable for future health economic studies related to NSCLC in China.
Authors’ contributions
J Zhu and B Wu conceived of the study and participated in its design and coordination. Y Shen and X Wang collected clinical data. Y Shen performed the statistical analysis and drafted the manuscript. All authors read and approved the final version of the manuscript.
Financial & competing interests disclosure
This work was supported by grants from Shanghai Jiao Tong University School of Medicine (grant number: JDYX2016QN014). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
All patients were fully informed of the study and provided written informed consent. The protocol was approved by the ethics committees of Shanghai Chest Hospital (reference number: KS(Y) 1718).
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Levy AR, Kowdley KV, Iloeje U et al. The impact of chronic hepatitis B on quality of life: a multinational study of utilities from infected and uninfected persons. Value Health 11(3), 527–538 (2008).
2.
Torrance GW. Preferences for health outcomes and cost-utility analysis. Am. J. Manag. Care 3(Suppl.), S8–S20 (1997).
3.
Rabin R, De Charro F. EQ-5D: a measure of health status from the EuroQol group. Ann. Med. 33(5), 337–343 (2001).
4.
Lidgren M, Wilking N, Jonsson B, Rehnberg C. Health related quality of life in different states of breast cancer. Qual. Life Res. 16(6), 1073–1081 (2007).
5.
Dolan P. Modeling valuations for EuroQol health states. Med. Care 35(11), 1095–1108 (1997).
6.
Torre LA, Siegel RL, Jemal A. Lung cancer statistics. Adv. Exp. Med. Biol. 893, 1–19 (2016).
7.
Zappa C, Mousa SA. Non-small-cell lung cancer: current treatment and future advances. Transl. Lung Cancer Res. 5(3), 288–300 (2016).
8.
Fan H, Shao ZY, Xiao YY et al. Incidence and survival of non-small-cell lung cancer in Shanghai: a population-based cohort study. BMJ Open 5(12), e009419 (2015).
9.
Ge L, Shi R. Progress of EGFR-TKI and ALK/ROS1 inhibitors in advanced non-small-cell lung cancer. Int. J. Clin. Exp. Med. 8(7), 10330–10339 (2015).
10.
Schuette W, Tesch H, Buttner H, Krause T, Soldatenkova V, Stoffregen C. Second-line treatment of stage III/IV non-small-cell lung cancer (NSCLC) with pemetrexed in routine clinical practice: evaluation of performance status and health-related quality of life. BMC Cancer 12, 14 (2012).
11.
Boolell V, Alamgeer M, Watkins DN, Ganju V. The evolution of therapies in non-small-cell lung cancer. Cancers (Basel) 7(3), 1815–1846 (2015).
12.
Grutters JP, Joore MA, Wiegman EM et al. Health-related quality of life in patients surviving non-small-cell lung cancer. Thorax 65(10), 903–907 (2010).
13.
Doyle S, Lloyd A, Walker M. Health state utility scores in advanced non-small-cell lung cancer. Lung Cancer 62(3), 374–380 (2008).
14.
Chouaid C, Agulnik J, Goker E et al. Health-related quality of life and utility in patients with advanced non-small-cell lung cancer: a prospective cross-sectional patient survey in a real-world setting. J. Thorac. Oncol. 8(8), 997–1003 (2013).
• Measures health state utility values in advanced non-small-cell lung cancer patients and revealed that stage IV disease, higher lines of treatment, and health state were significant predictors of utility.
15.
Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual. Life Outcomes 6, 84 (2008).
16.
Sturza J. A review and meta-analysis of utility values for lung cancer. Med. Decis. Making 30(6), 685–693 (2010).
17.
Nafees B, Lloyd AJ, Dewilde S, Rajan N, Lorenzo M. Health state utilities in non-small-cell lung cancer: an international study. Asia Pac. J. Clin. Oncol. 13(5), e195–e203 (2016).
18.
Xu Y, Zhou Z, Li Y et al. Exploring the nonlinear relationship between body mass index and health-related quality of life among adults: a cross-sectional study in Shaanxi Province, China. Health Qual. Life Outcomes 13, 153 (2015).
19.
China RGOPEO. Guide to pharmacoeconomics evaluation of China (revision 2011). China J. Pharm. Econom. (Chin.) (03), 6–48 (2011).
20.
Wang HM, Patrick DL, Edwards TC, Skalicky AM, Zeng HY, Gu WW. Validation of the EQ-5D in a general population sample in urban China. Qual. Life Res. 21(1), 155–160 (2012).
21.
Liu GG, Wu H, Li M, Gao C, Luo N. Chinese time trade-off values for EQ-5D health states. Value Health 17(5), 597–604 (2014).
•• Establishes a Chinese general population-based three-level EuroQol five-dimension social value set using the time trade-off method.
22.
Wu M, Zhao Q, Chen Y, Fu C, Xu B. Quality of life and its association with direct medical costs for COPD in urban China. Health Qual. Life Outcomes 13, 57 (2015).
23.
Chen J, Wong CK, Mcghee SM, Pang PK, Yu WC. A comparison between the EQ-5D and the SF-6D in patients with chronic obstructive pulmonary disease (COPD). PLoS ONE 9(11), e112389 (2014).
24.
Fiteni F, Vernerey D, Bonnetain F et al. Prognostic value of health-related quality of life for overall survival in elderly non-small-cell lung cancer patients. Eur. J. Cancer 52, 120–128 (2016).
25.
Katz MH. Multivariable analysis: a primer for readers of medical research. Ann. Intern. Med. 138(8), 644–650 (2003).
26.
Brazier JE, Yang Y, Tsuchiya A, Rowen DL. A review of studies mapping (or cross walking) non-preference-based measures of health to generic preference-based measures. Eur. J. Health Econ. 11(2), 215–225 (2010).
27.
Kim SH, Jo MW, Kim HJ, Ahn JH. Mapping EORTC QLQ-C30 onto EQ-5D for the assessment of cancer patients. Health Qual. Life Outcomes 10, 151 (2012).
28.
Khan I, Morris S. A non-linear beta-binomial regression model for mapping EORTC QLQ- C30 to the EQ-5D-3L in lung cancer patients: a comparison with existing approaches. Health Qual. Life Outcomes 12, 163 (2014).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 1 September 2017
Accepted: 14 December 2017
Published online: 18 May 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Health state utilities in patients with advanced non-small-cell lung cancer in China. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0069
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yihong Guo, Shixian Liu, Chuang Yang, Chengjun Wang, Rongyu Zhang, Yunfei Wang, Yanan Song, Mingfei Liu, Ruolin Zhang, Tiantian Xuan, Wen Zhao, Jisheng Li, Cost-effectiveness of first-line osimertinib plus chemotherapy versus amivantamab plus lazertinib for advanced EGFR-mutant NSCLC in the US and China, Therapeutic Advances in Medical Oncology, 10.1177/17588359261465356, 18, (2026).
- Hui Zhang, Yuhang Liu, Guihao Zeng, Shuangshuang Hu, Haonan Li, Hong Wang, Cost-effectiveness of hypofractionated radiation therapy versus conventional radiation therapy for unresectable stage III non-small cell lung cancer, Scientific Reports, 10.1038/s41598-025-28781-1, 15, 1, (2025).
- Parnnaphat Luksameesate, Nithinan Phatchararuangkit, Sutinee Soopairin, Chanida Vinayanuwattikun, Nattanichcha Kulthanachairojana, Suthira Taychakhoonavudh, Cost-utility and budget impact analyses of anaplastic lymphoma kinase inhibitors in Thailand, Scientific Reports, 10.1038/s41598-025-25113-1, 15, 1, (2025).
- Hui Zhang, Yuhang Liu, Bikun Cai, Mengyi Wang, Haonan Li, Hong Wang, Durvalumab consolidation therapy in patients with stage III small cell lung cancer after concurrent chemoradiation: a China-based cost-effectiveness analysis, Frontiers in Oncology, 10.3389/fonc.2025.1643022, 15, (2025).
- Qingqing Chai, Congling Gu, Luis Hernandez, Yan-Jun Zhang, Pharmacoeconomic Analysis of Brigatinib versus Alectinib in First‑Line Treatment of Anaplastic Lymphoma Kinase‑Positive Advanced Non‑Small‑Cell Lung Cancer in China, Oncology and Therapy, 10.1007/s40487-025-00361-3, 13, 3, (755-763), (2025).
- Longfeng Zhang, Hongcai Chen, Huide Zhu, Zhiwei Zheng, Toripalimab plus chemotherapy versus chemotherapy as first-line therapy for extensive-stage small cell lung cancer: a cost-effectiveness analysis, Frontiers in Immunology, 10.3389/fimmu.2025.1591517, 16, (2025).
- Xiaoyan You, Jiali Qin, Xiaomei Wang, Xianying Wang, Cost-effectiveness analysis of penpulimab combined with paclitaxel and carboplatin as first-line treatment for advanced squamous non-small cell lung cancer, Frontiers in Pharmacology, 10.3389/fphar.2025.1563788, 16, (2025).
- Yurou Xing, Junmeng Huang, Yi Zhang, Yongsheng Wang, Shaochong Qi, Advancing the understanding and management of angioimmunoblastic T-cell lymphoma: insights into its pathogenesis, clinical features, and emerging therapeutic strategies, Frontiers in Oncology, 10.3389/fonc.2025.1479179, 15, (2025).
- Liangxiao Wang, Na Lv, Yuan Gao, Chunyan Yan, Xuechen Huo, Ruigang Diao, Cost-effectiveness analysis of penpulimab combined with paclitaxel and carboplatin as a first-line treatment for metastatic squamous non-small cell lung cancer in China, BMJ Open, 10.1136/bmjopen-2024-091650, 15, 3, (e091650), (2025).
- Dai Lian, Yi Yang, Yuling Gan, Dunming Xiao, Yuliang Xiang, Shan Jiang, Yuanyuan Gu, Yingyao Chen, Cost-effectiveness of toripalimab plus chemotherapy versus chemotherapy as first-line treatment for advanced non-small cell lung cancer in China: a societal perspective, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2025.2451748, 25, 4, (587-596), (2025).
- See more