Front-line treatment of patients with chronic lymphocytic leukemia: a systematic review and network meta-analysis
Abstract
Aim: A systematic literature review and network meta-analysis were conducted to determine the relative efficacy and safety of interventions for treatment-naive chronic lymphocytic leukemia patients, as comparative evidence is scarce. Materials & methods: Relative treatment effects of progression-free survival, overall survival and safety outcomes were estimated via network meta-analysis based on data identified via systematic literature review. Results: Ibrutinib was superior in all pairwise comparisons for progression-free survival (probability to be better [P] range: overall population: 69–100%; fludarabine-ineligible population: 69–100%) and overall survival (P range: overall: 89–100%; fludarabine-ineligible: 91–100%) and had the highest probability of being best for all outcomes. Conclusion: Ibrutinib provides superior benefit in survival and safety compared with other front-line treatments of chronic lymphocytic leukemia.
Chronic lymphocytic leukemia (CLL) is the most common hematologic malignancy in western countries and occurs mainly in older people. Overall, 4.2 per 100,000 population per year develop the condition, a figure that rises to over 30 per 100,000 per year among those aged over 80 years [1]. The overall 5-year survival rate for people with CLL is 83%, although survival varies widely according to disease stage [2]. Treatment for CLL has evolved rapidly over the past two decades, with the addition of CD20-targeted antibodies, B-cell lymphoma-2 (BCL-2)-targeted treatment and B-cell receptor-targeted treatment resulting in improved outcomes [3–4].
As indicated by both the European Society for Medical Oncology (ESMO) and the National Comprehensive Cancer Network [1,5], there are various management options for CLL, and treatment choices must account for key patient and disease characteristics known to affect therapeutic outcomes. These include patient age [6], fitness/comorbidities [7] and molecular cytogenetics [6,8]. Generally, for fit patients with advanced, symptomatic disease, the so-called ‘full-dose fludarabine-based’ regimen of fludarabine + cyclophosphamide + rituximab (FCR) is recommended [1]. However, for elderly patients and/or those with significant comorbidities, FCR is associated with significant risk of myelosuppression and severe infection [9]. Options are further limited if these individuals also have cytogenetic characteristics associated with poor outcomes from current treatments (such as 17p or 11q deletion, or absence of IgVH mutation). For these patients, ESMO and National Comprehensive Cancer Network guidelines recommend ibrutinib monotherapy [1,5,9].
Given the range of CLL treatment options for people with differing levels of fitness, and the dearth of head-to-head clinical trials comparing front-line treatments, there remains considerable uncertainty regarding the optimal regimen for each patient group. The objectives of the presented systematic literature review (SLR) and network meta-analyses (NMAs) were therefore to determine the relative efficacy and safety of interventions for the front-line treatment of patients with CLL, and for the subgroup considered ineligible to receive full-dose fludarabine-based treatment.
Materials & methods
Systematic literature review
The SLR involved a search strategy designed to find clinical trials that had investigated front-line treatment of patients with CLL and which had reported efficacy and safety outcomes. Literature searches were conducted on 19 October 2015 in MEDLINE (via PubMed), Medline In-Process (via PubMed), Embase, Embase In-Process, the Cochrane Collection Central Register of Clinical Trials (CENTRAL) and the Database of Abstracts of Reviews of Effects, with no temporal or language limits. An update of this search was conducted in April 2017 to check whether any additional relevant studies or updated data had been published since the original search.
The inclusion criteria targeted prospective, interventional trials (either randomized controlled trials [RCTs], non-RCTs or single-arm studies) that had investigated efficacy or safety outcomes in patients receiving a treatment of interest as front-line therapy for CLL, small cell lymphoma or small lymphocytic lymphoma – conditions that are pathologically very similar to CLL.
Abstracts were screened for inclusion by two independent investigators, with any discrepancies in inclusion eligibility between them being resolved by a third investigator. Full-text versions of those articles that had passed abstract screening were then screened for inclusion by a single investigator, with a second investigator independently verifying whether each rejection by the first investigator had been appropriate, and again, a third investigator resolved any discrepancies. Articles that appeared potentially eligible on abstract screening were subsequently rejected if they were not an RCT or if their full-text version was found to be in a non-English language. The inclusion/exclusion criteria for the interventions/comparators of interest were applied only during full-text screening, with relevant comparators having been determined by considering recommendations in the 2015 ESMO treatment guidelines. Specifically, relevant treatments for elderly and/or unfit patients (who are not eligible for fludarabine-based treatment) included bendamustine, bendamustine + rituximab (BR), obinutuzumab + chlorambucil (Obi-Chl), ofatumumab + chlorambucil (Ofa-Chl), rituximab + chlorambucil (R-Chl) and reduced-dose FCR. By contrast, for young and/or fit patients, full-dose fludarabine-based regimens were also relevant treatments, including fludarabine, fludarabine + cyclophosphamide and FCR.
Information from included full-text articles was extracted by one investigator and validated by a second, and a third investigator was consulted to resolve any discrepancies. Quality-control measures and logic checks were conducted on all extracted data. Quality assessment of RCTs was evaluated using a tool based on the NICE quality assessment summary tables. Studies were categorized into one of the two groups: those conducted in patients eligible for full-dose fludarabine treatment and those conducted in patients ineligible for full-dose fludarabine treatment (typically elderly or unfit patients, per comorbidity status).
Network meta-analysis
A feasibility assessment was conducted to evaluate whether NMAs could be performed for the RCTs identified within the SLR. Two separate networks were established: one which included all studies of patients with CLL receiving front-line therapy (referred to below as the overall front-line population) and another subnetwork which included only those studies in patients ineligible for full-dose fludarabine treatment (referred to below as the fludarabine-ineligible population). NMAs based on these two networks were considered the ‘base-case’ analyses. Additionally, to account for variability among trial populations in potentially important prognostic factors and considering that one of the RCTs (RESONATE-2) enrolled only patients aged ≥65 years who did not have a del17p mutation, the following populations were identified and explored as ‘subgroup’ analyses where data permitted: patients aged ≥65 years; those with unmutated IgVH; those with del11q mutation; and those without del17p mutation. Because information on these variables was not consistently reported across studies, the potential impact of these factors was investigated as sensitivity analyses within those studies that could be stratified or had outcomes reported by similar strata.
Analyses included
The outcomes assessed in the base-case NMA for each of the two networks (i.e., overall front-line CLL patients and fludarabine-ineligible patients) included overall survival (OS), independent review committee (IRC)-assessed progression-free survival (PFS), investigator (INV)-assessed PFS and safety outcomes, including overall proportion of patients who discontinued treatment (total discontinuations [TD]) and the proportion with treatment discontinuations due to adverse events (DAE). For each outcome, a model was used to estimate the mean relative treatment effect along with a 95% credible interval, and the posterior distribution was used to determine the probability that a given regimen was the best among all treatments within the analyzed network. Specifically, the methodological approach in these analyses followed long-established techniques for integrating odds ratios (OR) and hazard ratios (HR) into NMAs, including those used and/or recommended by the NICE [10,11]. Accordingly, the analyses used both random-effect models and fixed-effect models. Random-effect analyses are widely accepted as the appropriate, more conservative approach when generalizations need to be made on a greater group of studies and populations and/or when there is heterogeneity across study methods. By contrast, fixed-effect models assume that effect size associated with a given intervention does not vary from study to study, and they may be particularly appropriate when only few studies are available for analysis. The best model fit for each network was selected on the basis of a review of the deviance information criterion and a clinical evaluation of the different model assumptions.
In the case of the overall front-line CLL patient NMA, random-effect analyses could be used, as there were sufficient studies for a between-effects variance to be estimated, with some uncertainty, from the data. These analyses used two different priors for the between-study variability (which was assumed to be identical across all comparisons) that were vaguely informative, N (0, 1.0) and N (0, 0.4), since the power to detect random variation among all studies was limited and the results were expected to be sensitive to the selection of the prior. Given the sparseness of the evidence networks for safety outcomes in the overall population and in the fludarabine-ineligible population, only fixed-effects Bayesian NMAs were conducted for these networks. Fixed-effects Bayesian NMAs were also conducted in the four subgroups of interest, to evaluate INV-assessed PFS, OS and DAEs in the fludarabine-ineligible population only (due to the limited data available).
Chlorambucil was chosen as the common comparator across both evidence networks given that it was used as a comparator in the majority of studies (10 of 15 studies in the overall front-line network and four of five studies in the fludarabine-ineligible network). As both evidence networks relied on chlorambucil as the key common comparator, this raised a potential issue given that there were known to be marked between-study differences in chlorambucil dosing (with regards to dose unit, number of cycles and cycle length), and this variation could have had an impact on the treatment effects observed from study to study and thus on the results of the NMAs. To explore this possibility, regression analyses of PFS and OS using cumulative chlorambucil dose as a covariate was carried out as a sensitivity analysis. Specifically, this analysis was used the estimated cumulative chlorambucil dose in milligram at 24 weeks, calculated using reported doses and scheduling in the study protocols and assuming a mean patient body surface area of 1.69 m2 and weight of 63.5 kg.
The research presented in this article is based on previously conducted studies and did not involve any new studies of human or animal subjects performed by any of the authors.
Results
Systematic literature review
Of the 2367 abstracts screened for the SLR, 1911 references were excluded at the abstract level through application of screening criteria listed in the ‘Materials & methods’ section. Among the remaining 456 publications, 146 reported data on a total of 58 primary studies that investigated the front-line treatments of interest. The 58 RCTs were examined for comparability with the RESONATE-2 patient population. This process identified five RCTs [12,13,14] that had investigated front-line treatment in CLL patients ineligible for full-dose fludarabine and ten RCTs [15,16] that had investigated fludarabine or fludarabine-based regimens as front-line treatment in treatment-naive patients with CLL, and which had reported outcomes of interest (see the Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram in Figure 1). Collectively, the 15 RCTs included over 5300 patients and provided adequate evidence to support an NMA to estimate the comparative efficacy and safety of treatments of interest in the front-line setting. Of note, the updated search conducted in April 2017 identified that no additional relevant RCT data that could affect the NMA had been published since the original SLR in October 2015.

Figure 1. Preferred reporting items for systematic reviews and meta-analyses diagram.
BR: Bendamustine + rituximab; CLL: Chronic lymphocytic leukemia; FC: Fludarabine + cyclophosphamide; FCR: Fludarabine + cyclophosphamide + rituximab; FCR-Lite: Reduced-dose fludarabine + cyclophosphamide + rituximab, where fludarabine was given at relatively low frequency (dose); iWCLL: International Workshop on Chronic Lymphocytic Leukemia; NMA: Network meta-analysis; Obi-Chl: Obinutuzumab + chlorambucil; Ofa-Chl: Ofatumumab + chlorambucil; PRISMA: Preferred Reporting Items for Systematic Review and Meta-Analysis; R-Chl: Rituximab + chlorambucil; RCT: Randomized controlled trial.
Patient characteristics at study baseline are shown in Table 1. Across the overall network, most studies that reported the number of evaluable patients at baseline included at least 100 participants in each treatment arm, with exceptions being the MaBLe [14], Mulligan et al. [17] and CLL5 [18] studies, in which the number of evaluable patients per treatment arm ranged from 40 to 93. Of the 13 studies that reported follow-up duration, the median value ranged from 22 to 83 months in the fludarabine-based studies and from 18.4 to 54 months in the studies of fludarabine-ineligible patients. The mean patient age at baseline ranged from 58 to 71 years across the fludarabine-based studies and 63 to 74 years in the fludarabine-ineligible studies. Of the studies that reported Eastern Cooperative Oncology Group performance status, the majority were restricted to patients with Eastern Cooperative Oncology Group 0 to 1. Across the 15 RCTs, PFS and OS outcomes were available for all but three studies and the PFS outcomes were either INV- or IRC-assessed (Table 2). IRC results were used preferentially for the NMA wherever reported (in three of the eight studies in the overall front-line CLL network, and in four of the five studies in the fludarabine-ineligible network) as they are considered less prone to bias than INV assessments. Where the reporting methodology for PFS was not specified, it was included in the analyses as INV-assessed PFS. Safety data were considerably scarcer across the 15 RCTs, with five studies reporting DAE outcomes and three studies TD outcomes.
| Trial name, study [Ref.] | Related publications, study (year) [Ref.] | Group descriptor | Median follow-up (months) | N evaluated at baseline | Primary end point | Male (%) | Age (years), median (range) | ECOG (%) 0/>0/>1 | 17p/11q/unmutated IgVH (%) | Binet (%) A/B/C | Rai (%) 0–II/I–II/III–IV |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Front-line treatments in fludarabine-ineligible population | |||||||||||
| RESONATE-2, Burger et al. (2015) [13] | – | Ibrutinib | 18.4 | 136 | PFS | 64.7 | 73 (65–89) | 44.1/55.9/8.1 | 0/21.3/43 | 25.7/30.1/44.1† | 55.9/53.7/44.1 |
| Chl | 133 | 60.9 | 72 (65–90) | 40.6/59.4/9 | 0/18.8/45 | 22.6/30.8/46.6† | 53.4/51.9/46.6 | ||||
| COMPLEMENT1, Hillmen et al. (2015) [19] | Online appendix to Hillmen et al. (2015) [19] | Ofa-Chl | 28.9 | 221 | PFS | 64.3 | 69 (35–92) | 38.9/61.1/8 | 4.5/19/57 | 34.8/33.5/31.7 | –/51.1/42.1 |
| Chl | 226 | 61.9 | 70 (36–91) | 37.2/62.8/8 | 7.5/11.1/56 | 31/38.5/30.5 | –/50.9/38.9 | ||||
| CLL11, Goede et al. (2014) [12] | Hallek et al. (2012) [20] | Obi-Chl | NR | 238 | PFS | 58.8 | 74 (39–88) | –/–/– | 6.7/13.4/61 | 23.1/41.2/35.7 | –/–/– |
| Goede et al. (2013) [21] | R-Chl | 233 | 63.9 | 73 (40–90) | –/–/– | 3.9/16.3/62 | 21/42.9/36.1 | –/–/– | |||
| Goede et al. (2013) [22] | Chl | 118 | 63.6 | 72 (43–87) | –/–/– | 8.5/11.9/59 | 20.3/42.4/37.3 | –/–/– | |||
| Knauf et al. (2012) [23] | Knauf et al. (2007) [24] | Bendamustine | 54 | 162 | OR | 63 | 63 (45–77) | 69.8/–/– | –/–/– | 0/71.6/28.4 | –/–/– |
| Knauf et al. (2009) [25] | Chl | 157 | 60.5 | 66 (35–78) | 65/–/– | –/–/– | 0/70.7/29.3 | –/–/– | |||
| MaBLe, Michallet (2015) [14] | – | BR | NR | 40 | NR | – | – | –/–/– | –/–/– | –/–/– | –/–/– |
| R-Chl | 45 | – | – | –/–/– | –/–/– | –/–/– | –/–/– | ||||
| Front-line treatments with fludarabine or fludarabine-based regimens in CLL | |||||||||||
| Mulligan et al. (2014) [17] | Karlsson et al. (2007) [26] | Fludarabine | 83 | 74 | OR | 81.1 | 63.5 | –/–/– | –/–/53.7 | 27/25.7/47.3 | 43.2/36.5/56.8 |
| Karlsson et al. (2004) [27] | Chl | 77 | 74 | 63 | –/–/– | –/–/65 | 23.4/35.1/41.6 | 54.5/49.4/45.5 | |||
| CLL4, Eichhorst et al. (2006) [28] | Eichhorst et al. (2005) [29] Eichhorst et al. (2005) [30] Eichhorst et al. (2003) [31] Eichhorst et al. (2007) [32] | Fludarabine | 22 | 182 | NR | 70.3 | 59 (43–65) | 52.7/47.3/2.2 | –/–/– | 11/53.8/35.2 | 58.8/56.6/41.2 |
| FC | 180 | 75 | 58 (42–64) | 53.9/46.1/3.3 | –/–/– | 7.8/57.2/35 | 61.1/58.3/38.9 | ||||
| E2997, Flinn et al. (2007) [33] | Grever et al. (2007) [34] | Fludarabine | 24 | 137 | Response | 70.1 | 61 (33–83) | 48.9/–/– | 6.6/11.7/47 | –/–/– | 56.2/54/42.3 |
| FC | 141 | 70.2 | 61 (39–86) | 45.4/–/– | 7.1/17/47 | –/–/– | 53.9/51.1/44.7 | ||||
| CALGB 9011, Rai et al. (2000) [16] | Morrison et al. (2001) [35] | Fludarabine | 62 | 179 | NR | 70.9 | 64 (33–88) | 63.1/–/– | –/–/– | –/–/– | –/60.9/39.1 |
| Chl | 193 | 66.8 | 62 (36–89) | 62.7/37.3/4.1 | –/–/– | –/–/– | –/59.1/40.9 | ||||
| F-Chl | 137 | 65.7 | 63 (32–83) | 51.8/46.7/5.8 | –/–/– | –/–/– | –/61.3/38.7 | ||||
| LRF CLL4, Catovsky et al. (2007) [15] | Skowronska et al. (2012) [36] Dearden et al. (2011) [37] | Fludarabine | 41 | 194 | OS | 73.2 | 64 (38–85) | –/–/– | 5.2/–/– | 23.7/46.9/29.4 | –/–/– |
| Chl | 387 | 73.9 | 65 (35–85) | –/–/– | 3.6/–/– | 24.8/44.4/30.7 | –/–/– | ||||
| FC | 196 | 74 | 65 (40–86) | –/–/– | 4.6/–/– | 25/45.4/29.6 | –/–/– | ||||
| CLL8, Cramer et al. (2013) [38] | Adena et al. (2014) [39] Hallek et al. (2010) [40] Main et al. (2010) [41] Hallek et al. (2008) [42] Stilgenbauer et al. (2014) [43] | FC | 47 | 409 | PFS | 74.3 | 61 (36–81) | 55.3/–/– | 7.1/16.9/63 | 5.4/63.3/30.8 | –/–/– |
| FCR | 408 | 74.3 | 61 (30–80) | 54.2/–/– | 5.4/20.6/63 | 4.4/64.5/30.9 | –/–/– | ||||
| CLL5, Eichhorst et al. (2009) [18] | Eichhorst et al. (2013) [44] Eichhorst et al. (2004) [45] Eichhorst et al. (2007) [46] Schmitt et al. (2002) [47] Eichhorst et al. (2003) [48] | Fludarabine | 42 | 93 | PFS and OS | 65.6 | 71 (65–78) | 46.2/53.8/2.2 | 5.4/15.1/– | 12.9/50.5/36.6 | 60.2/54.8/39.8 |
| Chl | 100 | 63 | 70 (65–78) | 42/58/9 | 5/8/– | 16/44/40 | 57/52/43 | ||||
| CLL1 EORTC, Jaksic et al. (2000) [49] | Jaksic et al. (1996) [50] Jaksic et al. (1998) [51] | Chl | 33 | NR | Response | NR | NR | NR | NR | NR | NR |
| Fludarabine | NR | NR | NR | NR | NR | NR | NR | ||||
| CLL10, Eichhorst et al. (2013) [52] | Langerbeins et al. (2014) [53] Eichhorst et al. (2014) [54] | FCR | 27.9 | 282 | NR | – | NR | NR | –/–/55 | NR | NR |
| BR | 279 | – | NR | NR | –/–/68 | NR | NR | ||||
| Rai et al. (1996) [55] | Rai et al. (1995) [56] | Fludarabine | 30 | NR | NR | – | NR | NR | NR | NR | NR |
| Chl | NR | – | NR | NR | NR | NR | NR | ||||
The sources of data stated in the table may include the primary publication and related publications listed for each study.
†Calculated with the patient-level data from the RESONATE-2 trial (data on file), equating Rai stages 0–I with Binet stage A, Rai stage II with Binet stage B and Rai stage III–IV with Binet stage C.
BR: Bendamustine + rituximab; CLL: Chronic lymphocytic leukemia; ECOG: Eastern Cooperative Oncology Group; FC: Fludarabine + cyclophosphamide; F-Chl: Fludarabine + chlorambucil; FCR: Fludarabine + cyclophosphamide + rituximab; FCR-Lite: Reduced-dose fludarabine + cyclophosphamide + rituximab, where fludarabine was given at relatively low frequency (dose); NR/–: Not reported; Obi-Chl: Obinutuzumab + chlorambucil; Ofa-Chl: Ofatumumab + chlorambucil; OR: Overall response; OS: Overall survival; PFS: Progression-free survival; R-Chl: Rituximab + chlorambucil.
| Trial Name, study (year) [Ref.] | Comparison | Median follow-up (months) | Cumulative 24-week Chl dose (mg) | PFS HR (95% CrI) | OS HR (95% CrI) | Percentage of patients with TDs | Percentage of patients with DAEs |
|---|---|---|---|---|---|---|---|
| Front-line treatments in fludarabine-ineligible population | |||||||
| RESONATE-2, Burger et al. (2015) [13] | Ibrutinib versus Chl | 18.4 | 450 | IRC 0.16 [0.09, 0.28] INV 0.09 [0.04, 0.17] | 0.16 [0.05, 0.56] | Ibrutinib: 12.6% Chl: 59.4% | Ibrutinib: 8.8% Chl: 23.3% |
| CLL11, Goede et al. (2014) [12] | Obi-Chl versus Chl R-Chl versus Chl | NR | 384 | IRC 0.19 [0.14, 0.27] INV 0.18 [0.13, 0.24] IRC 0.46 [0.35, 0.61] INV 0.44 [0.34, 0.57] | 0.41 [0.23, 0.74] 0.66 [0.39, 1.11] | Obi-Chl: 20% R-Chl: 12.8% Chl: 33.9% | Obi-Chl: 12.7% R-Chl: 7.1% Chl: 13.5% |
| COMPLEMENT1, Hillmen et al. (2015) [19] | Ofa-Chl versus Chl | 28.9 | 772.8 | IRC 0.58 [0.46, 0.73] INV 0.54 [0.41, 0.69] | 0.91 [0.57, 1.43] | Ofa-Chl: 23.5% Chl: 32.5% | Ofa-Chl: 12.9% Chl: 12.7% |
| Knauf et al. (2012) [23] | Bendamustine versus Chl | 35 | 720 | IRC 0.23 [0.16, 0.33] INV 0.35 [0.27, 0.46] | 0.77 [0.52, 1.12] | – | Bendamustine: 11.1% Chl: 3.3% |
| MaBLe trial, Michallet (2015) [14] | BR versus R-Chl | 24 | – | IRC or INV 0.52 [0.34, 0.8]‡ | 0.98 [0.51, 1.9] | – | – |
| Front-line treatments with fludarabine or fludarabine-based regimens in CLL | |||||||
| Mulligan et al. (2014) [17] | Fludarabine versus Chl | 83 | 1104 | IRC 1.14 [0.85, 1.51]† | 1.08 [0.72, 1.63] | – | – |
| CLL4, Eichhorst et al. (2006) [28] | FC versus fludarabine | 22 | – | IRC or INV 0.56 [0.39, 0.81]† | 1.15 [0.60, 2.19] | – | Fludarabine: 14% FC: 30% |
| E2997, Flinn et al. (2007) [33] | FC versus fludarabine | 24 | – | IRC or INV 0.51 [0.37, 0.71] | 1.06 [0.62, 1.79] | – | – |
| CALGB 9011, Rai et al. (2000) [16] | Fludarabine versus Chl | 62 | 441.6 | IRC or INV 0.65 [0.51, 0.82]† | 0.78 [0.59, 1.05] | – | – |
| LRF CLL4, Catovsky et al. (2007) [15] | Fludarabine versus Chl FC versus fludarabine FC versus Chl | 41 | 772.8 | IRC 0.86 [0.71, 1.04] IRC 0.46 [0.37, 0.58] IRC 0.41 [0.32, 0.52] | 1.24 [0.90, 1.70]† 0.87 [0.64, 1.12]† 1.14 [0.82, 1.57]† | – | – |
| CLL8, Cramer et al. (2013) [38] | FCR versus FC | 47 | – | IRC 0.56 [0.46, 0.69] | 0.67 [0.48, 0.92] | – | FCR: 18% FC: 18% |
| CLL5, Eichhorst et al. (2009) [18] | Fludarabine versus Chl | 42 | 450 | IRC or INV 0.98 [0.72, 1.31]† | 1.39 [0.87, 2.23] | – | Fludarabine: 26% Chl: 19% |
| CLL10, Eichhorst et al. (2013) [52] | BR versus FCR | 27.9 | – | IRC or INV 1.42 [1.02, 1.98] | 0.61 [0.31, 1.20] | – | – |
The sources of data stated in the table may include the primary publication and related publications listed for each study.
Results in bold font represent statistically significant advantages for the tested treatment over the comparator (e.g., with an HR < 1, with the upper end of 95% CI < 1 indicating a survival benefit for treatment vs comparator).
†PFS/OS imputed from survival curves.
‡Study was presented in meeting abstract, which did not specify whether PFS was assessed by investigator or IRC.
–: Not reported; BR: Bendamustine + rituximab; Chl: Chlorambucil; CLL: Chronic lymphocytic leukemia; CrI: Credible interval; DAE: Discontinuation due to adverse event; FC: Fludarabine + cyclophosphamide; FCR: Fludarabine + cyclophosphamide + rituximab; HR: Hazard ratio; INV: Investigator; IRC: Independent review committee; Obi-Chl: Obinutuzumab + chlorambucil; Ofa-Chl: Ofatumumab + chlorambucil; OS: Overall survival; PFS: Progression-free survival; R-Chl: Chlorambucil + rituximab; TD: Total treatment discontinuation.
Base-case NMA results
The results for the base-case analyses for both the overall front-line population and the fludarabine-ineligible population are described below.
Survival outcomes: overall front-line population
Thirteen studies contributed to the NMA of PFS and OS outcomes in the base-case analysis (Figure 2A). The base-case random-effects NMA for the overall front-line population suggested that ibrutinib was superior to the other treatments in improving IRC-assessed PFS, with HRs (and the associated probability of being more effective) ranging from 0.16 (P[HR<1] = 100.0%; vs chlorambucil) to 0.82 (P[HR<1] = 69.3%; vs Obi-Chl) (Figure 3A). Results based on INV-assessed PFS showed a similar trend, with HRs between 0.09 (P[HR<1] = 100.0%; vs chlorambucil) and 0.44 (P[HR<1] = 95.5%; vs bendamustine) (Figure 3B). Similarly, ibrutinib showed the greatest OS benefit, with HRs ranging from 0.14 (P[HR<1] = 99.8%; vs fludarabine + cyclophosphamide) to 0.41 (P[HR<1] = 89.2%; vs Obi-Chl) (Figure 3C). Overall, ibrutinib had the highest probability of being the best treatment in the network for improving both IRC-assessed PFS (59.9%) and OS (87.7%) (Figure 4A).
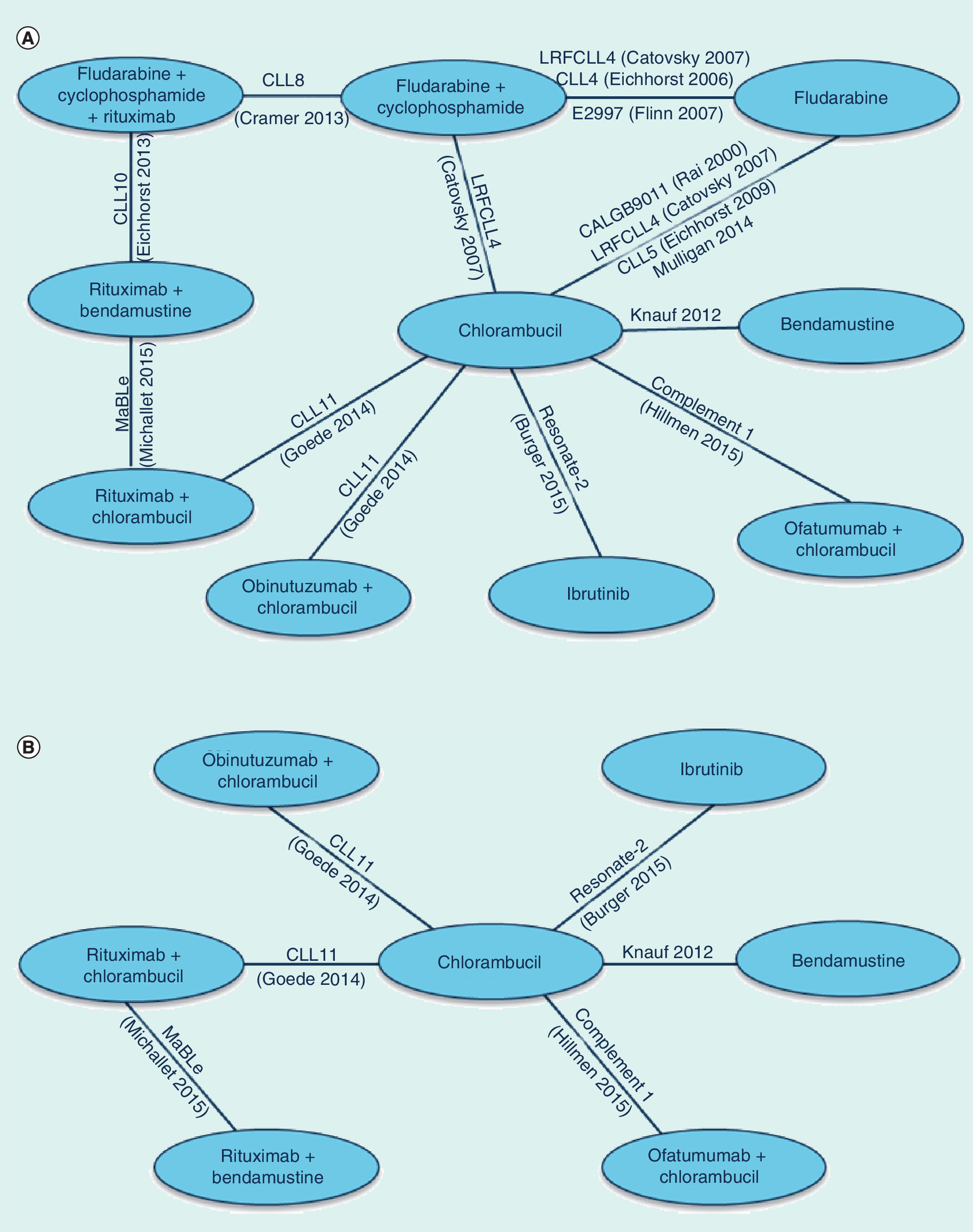
Figure 2. Network of randomized controlled trials in patients with chronic lymphocytic leukemia receiving front-line treatment.
Network of studies and treatments included in the NMAs for the (A) overall front-line CLL population and (B) fludarabine-ineligible population (2-part figure, A & B). In CLL11, the results for the comparison between Obi-Chl and R-Chl included 190 additional patients who were randomized after termination of the chlorambucil arm (i.e., stage 2), and these data were not considered to be relevant evidence for the NMA. Therefore, no link between these two treatments is presented in the network.
CLL: Chronic lymphocytic leukemia; NMA: Network meta-analysis; Obi-Chl: Obinutuzumab + chlorambucil; R-Chl: Chlorambucil + rituximab; RCT: Randomized controlled trial.

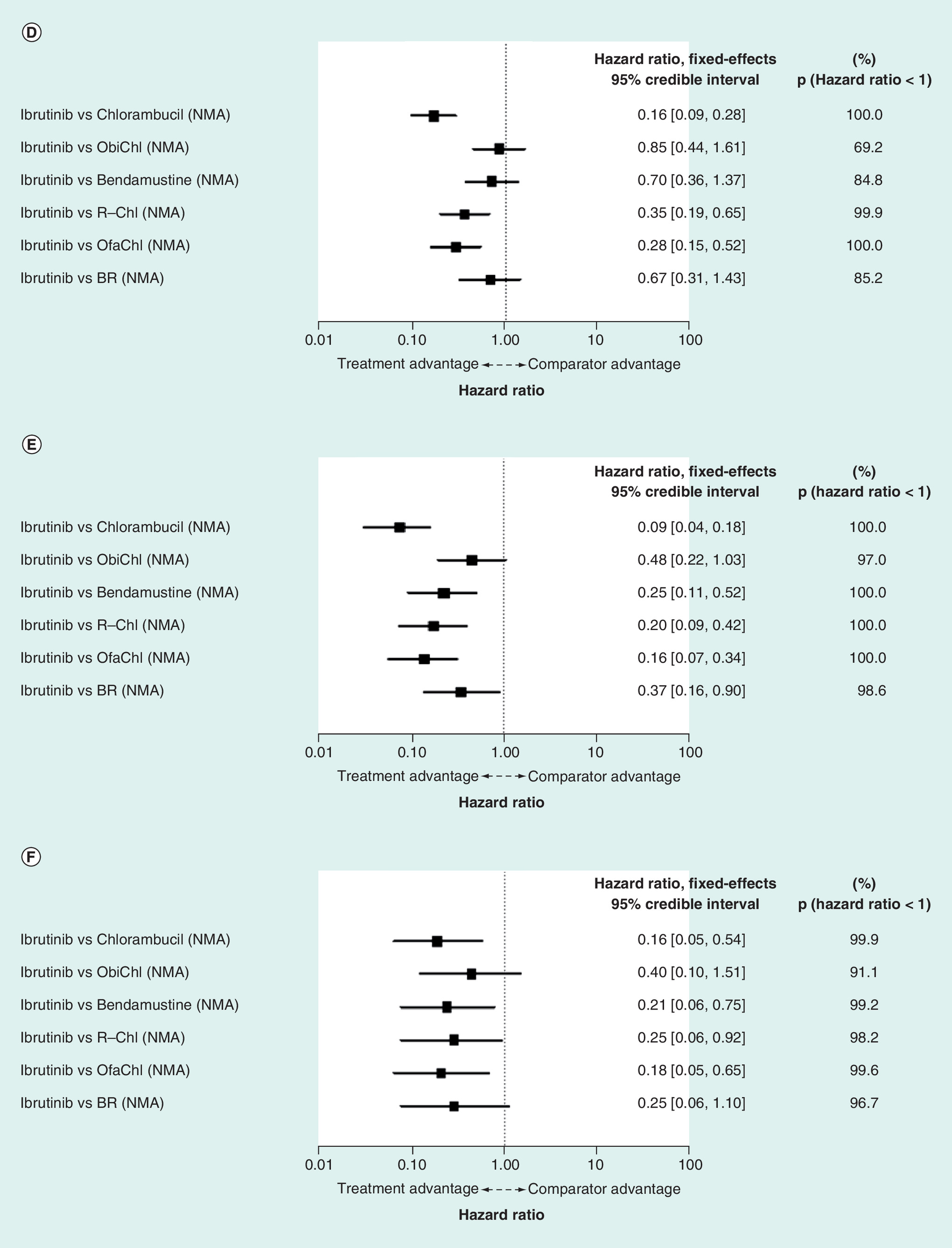
Figure 3. Progression-free survival and overall survival of front-line treatments in chronic lymphocytic leukemia.
(A) IRC-assessed progression-free survival (PFS) network meta-analysis (NMA) outcomes: overall front-line population. (B) INV-assessed PFS NMA outcomes: overall front-line population. (C) OS NMA outcomes: overall front-line population. (D) IRC-assessed PFS NMA outcomes: fludarabine-ineligible population. (E) INV-assessed PFS NMA outcomes: fludarabine-ineligible population. (F) OS NMA outcomes: fludarabine-ineligible population (6-part figure, A–F).
CLL: Chronic lymphocytic leukemia; INV: Investigator; IRC: Independent review committee; OS: Overall survival.

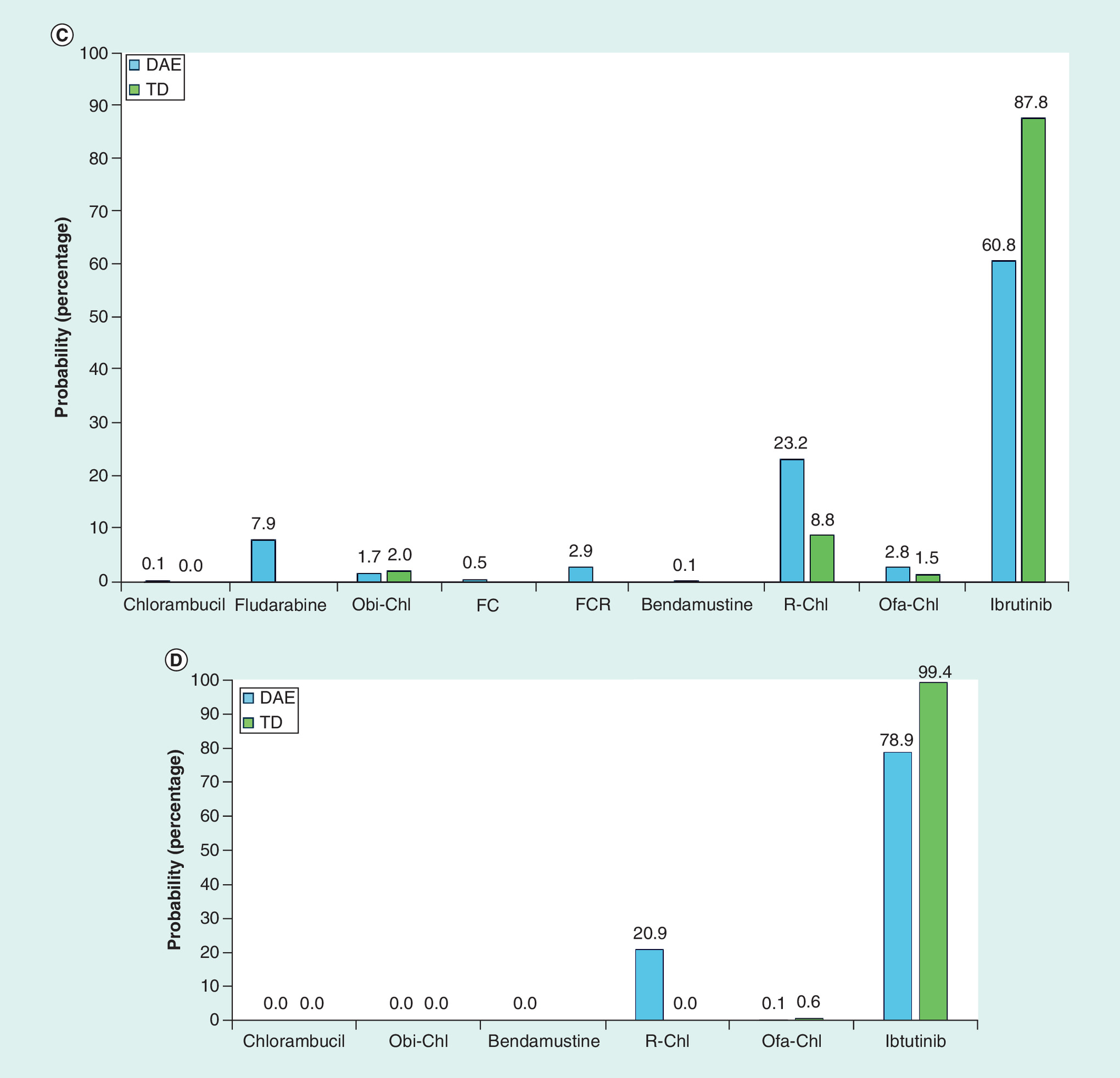
Figure 4. Probability of being best treatment in network.
(A) Probability of being best treatment in network in terms of IRC-assessed PFS and OS in the overall front-line population. (B) Probability of being best treatment in network in terms of IRC-assessed PFS and OS in the fludarabine-ineligible population. (C) Probability of being best treatment in network in terms of TDs and DAEs in the overall front-line population. (D) Probability of being best treatment in network in terms of TDs and DAEs in the fludarabine-ineligible population (4-part figure, A–D).
BR: Bendamustine + rituximab; DAE: Discontinuation due to adverse event; FC: Fludarabine + cyclophosphamide; FCR: Fludarabine + cyclophosphamide + rituximab; IRC: Independent review committee; Obi-Chl: Obinutuzumab + chlorambucil; Ofa-Chl: Ofatumumab + chlorambucil; OS: Overall survival; PFS: Progression-free survival; R-Chl: Rituximab + chlorambucil; TD: Total discontinuation.
Survival outcomes: fludarabine-ineligible population
Five RCTs contributed to the NMA of survival outcomes in the base-case analysis for the population of fludarabine-ineligible patients. The network comprised seven treatment arms (pairs depicted in Figure 2B). The base-case fixed-effects NMA for the fludarabine-ineligible CLL population found that the IRC-assessed PFS HRs (and probabilities of being better) ranged from 0.16 (P[HR<1] = 100.0%; vs chlorambucil) to 0.85 (P[HR<1] = 69.2%; vs Obi-Chl) (Figure 3D); INV-assessed PFS HRs ranged from 0.09 (P[HR<1] = 100.0%; vs chlorambucil) to 0.48 (P[HR<1] = 97.0%; vs Obi-Chl) (Figure 3E); and OS HRs ranged from 0.16 (P[HR<1] = 99.9%; vs chlorambucil) to 0.40 (P([HR<1] = 91.1%; vs Obi-Chl) (Figure 3F). In the fludarabine-ineligible network, ibrutinib had the highest probability of being the best treatment in the network for improving both PFS (62.7%) and OS (89.9%) (Figure 4B).
Safety outcomes: overall front-line population
The network of evidence for analysis of TDs included three RCTs (RESONATE-2 [13], COMPLEMENT1 [19] and CLL11 [12]). The random-effects NMA showed that patients receiving ibrutinib experienced fewer TDs than those in other treatment groups, with ORs (and probabilities of being better [i.e., associated with fewer discontinuations]) ranging from 0.10 (P[OR<1] = 99.8%; vs chlorambucil) to 0.35 (P[OR<1] = 89.9%; vs R-Chl). Five studies reported DAEs and were therefore included in the network for this outcome. Compared with eight other treatments, ORs for ibrutinib (and this drug's probabilities of being the better treatment) ranged from 0.08 (P[OR<1] = 99.0%; vs bendamustine) to 0.66 (P[OR<1] = 70.4%; vs R-Chl) (Table 3). Ibrutinib was least likely to be associated with negative safety outcomes, having an 87.8% probability of having the lowest risk of TDs and 60.8% probability of having the lowest risk of DAEs (Figure 4C).
| Ibrutinib versus chlorambucil | Ibrutinib versus Obi-Chl | Ibrutinib versus R-Chl | Ibrutinib versus Ofa-Chl | Ibrutinib versus bendamustine | Ibrutinib versus fludarabine | Ibrutinib versus FC | Ibrutinib versus FCR | |
|---|---|---|---|---|---|---|---|---|
| Safety outcomes, overall front-line population | ||||||||
| TD, random-effects OR [95% CrI] Probability ibrutinib is better | 0.1 [0.02, 0.37] 99.8% | 0.21 [0.03, 1.35] 95.8% | 0.35 [0.05, 2.28] 89.9% | 0.15 [0.02, 0.99] 79.5% | NA | NA | NA | NA |
| DAE, random-effects OR [95% CrI] Probability ibrutinib is better | 0.32 [0.08, 1.18] 96.2% | 0.31 [0.05, 2] 91.5% | 0.66 [0.1, 4.31] 70.4% | 0.31 [0.05, 1.9] 92.2% | 0.08 [0.01, 0.6] 99% | 0.46 [0.07, 2.99] 83.5% | 0.21 [0.03, 1.74] 92.2% | 0.21 [0.02, 2.35] 92.2% |
| Safety outcomes, fludarabine-ineligible population | ||||||||
| TD, fixed-effects OR [95% CrI] Probability ibrutinib is better | 0.1 [0.05, 0.17] 100% | 0.2 [0.09, 0.44] 100% | 0.34 [0.15, 0.78] 99.4% | 0.15 [0.07, 0.32] 100% | NA | NA | NA | NA |
| DAE, fixed-effects OR [95% CrI] Probability ibrutinib is better | 0.23 [0.15, 0.63] 100% | 0.31 [0.11, 0.8] 99.3% | 0.65 [0.23, 1.81] 79.2% | 0.31 [0.12, 0.77] 99.5% | 0.08 [0.02, 0.27] 100% | NA | NA | NA |
Results in bold font represent statistically significant advantages for the tested treatment over the comparator (e.g., with an OR < 1 with upper end of 95% CI < 1 indicating a statistically significant safety benefit for the tested treatment or ibrutinib over comparator/s).
CrI: Credible interval; DAE: Discontinuation due to adverse event; FC: Fludarabine + cyclophosphamide; FCR: Fludarabine + cyclophosphamide + rituximab; NA: Not applicable; NMA: Network met-analysis; Obi-Chl: Obinutuzumab + chlorambucil; Ofa-Chl: Ofatumumab + chlorambucil; OR: Odds ratio; OS: Overall survival; R-Chl: Chlorambucil + rituximab; TD: Total treatment discontinuation.
Safety outcomes: fludarabine-ineligible population
Of the five RCTs that investigated treatment in fludarabine-ineligible patients, three reported the proportions of patients with TDs, and four reported proportions of patients with DAEs. ORs and probabilities of ibrutinib being better in terms of TDs ranged from 0.10 (P[OR<1] = 100%; vs chlorambucil) to 0.34 (P[OR<1] = 99.4%; vs R-Chl) and in terms of DAEs from 0.08 (P[OR<1] = 100%; vs bendamustine) to 0.65 (P[OR<1] = 79.2%; vs R-Chl) (Table 3). Fixed-effect modeling results indicated that ibrutinib was most likely to be the best treatment, with the lowest relative chance of experiencing TDs (99.4% probability of being best) and DAEs (78.9% probability of being best) (Figure 4D).
Regression analyses for survival outcomes using chlorambucil dosing as covariate
There was significant variation in chlorambucil dosing across the RCTs that had investigated this treatment, and this was particularly marked in the fludarabine-ineligible network. For instance, in that network, the median cumulative chlorambucil dose in CLL11 was 384 mg, while in RESONATE-2, the mean dose ranged between 252 and 672 mg. COMPLEMENT1 had the highest cumulative chlorambucil dose among the five RCTs (reported to be median 728 mg and range 98–1848 mg). To explore the potential effect of such differences, regression analyses for PFS and OS, using cumulative chlorambucil dose at 24 weeks as a covariate, were conducted for both networks. This analysis showed a strong correlation between dose and PFS/OS outcomes in studies involving fludarabine-eligible patients, but no correlation in studies of fludarabine-ineligible patients.
Subgroup analyses in fludarabine-ineligible patients
RESONATE-2 enrolled only patients aged at least 65 years and who did not have del17p mutation. Across the other trials, there were between-study differences in patient age and the proportion of participants without del17p mutations, as well as in the proportion of patients with other mutations, including IgVH and del11q. As both age and mutation status are prognostic indicators and potential treatment-effect-modifiers in CLL [6], analyses were conducted, where data permitted, on the subgroups of patients aged ≥65 years, those with unmutated IgVH, those with del11q mutation and those without del17p mutation.
Some or all outcomes of interest for the four subgroups were available from four RCTs: RESONATE-2 [13], CLL11 [12], COMPLEMENT1 [19] and Knauf et al. [23]. Pairwise comparisons were conducted for ibrutinib versus Obi-Chl, R-Chl, Ofa-Chl and bendamustine, respectively, and effects were tested in the subgroups for which data were available. The data inputs used in the subgroup NMAs are presented in Table 4.
| Ibrutinib versus Chl | Obi-Chl versus Chl | R-Chl versus Chl | Ofa-Chl versus Chl | Bendamustine versus Chl | |
|---|---|---|---|---|---|
| INV-assessed PFS (subgroup ≥65 years) HR [95% CI] | 0.09 [0.04, 0.17] | 0.21 [0.15, 0.3] | NA | NA | |
| INV-assessed PFS (subgroup with 11q mutation) HR [95% CI] | 0.024† [0.003, 0.186] | 0.37 [0.17, 0.81] | 0.99 [0.49, 2.03] | NA | NA |
| INV-assessed PFS (IgVH unmutated subgroup) HR [95% CI] | 0.06‡ [0.02, 0.18] | 0.23 [0.16, 0.34] | 0.54 [0.38, 0.76] | NA | NA |
| INV-assessed PFS (subgroup without 17p) HR [95% CI] | 0.09 [0.04, 0.17] | 0.25 [0.18, 0.33] | 0.42 [0.33, 0.55] | NA | NA |
| OS (subgroup ≥65 years) HR [95% CI]† | 0.16 [0.05, 0.56] | NA | NA | NA | 0.92 [0.55, 1.55] |
| DAE (subgroup ≥65 years) OR [95% CI]† | 0.32† [0.16, 0.66] | NA | NA | 0.96§ [0.51, 1.8] | NA |
Results in bold font represent statistically significant advantages for the tested treatment over the comparator (e.g., with an HR/OR < 1 with upper end of 95% CI < 1 indicating a statistically significant safety benefit for the tested treatment or ibrutinib over comparator/s).
†Relative results were derived using the number or proportion of patients that achieved an overall response as reported in the study publications.
‡Relative results were derived using the patient-level data from RESONATE-2.
§Relative results were derived using the number or proportion of patients that experience event (discontinuation or adverse event) as reported in the study publications.
Chl: Chlorambucil; DAE: Discontinuation due to adverse event; HR: Hazard ratio; INV: Investigator; NA: Not available; NMA: Network meta-analysis; Obi-Chl: Obinutuzumab + chlorambucil; Ofa-Chl: Ofatumumab + chlorambucil; OR: Odds ratio; OS: Overall survival; PFS: Progression-free survival; R-Chl: Chlorambucil + rituximab.
Overall, results of the Bayesian NMA in the subgroups showed comparable or even higher relative efficacy of ibrutinib versus the other treatments, compared with that shown in the base-case analyses (Table 5). Analysis of the age ≥65 years subgroup resulted in very similar INV-assessed PFS, OS and DAE HRs or ORs compared with the all-patient base-case analyses, as did analysis of the population without del17p in terms of INV-assessed PFS. Results from the analyses of the del11q and IgVH unmutated populations indicated that in these high-risk subgroups ibrutinib may confer a particularly large PFS advantage over Obi-Chl (del11q: HR = 0.06, P[HR<1] = 99.9%; IgVH unmutated: HR = 0.27, P[HR<1] = 91.8%) and R-Chl (del11q: HR = 0.02; P[HR<1] = 100.0% and IgVH unmutated: HR = 0.11; P[HR<1] = 100.0%), as suggested by the much lower HRs compared with the all-patient base-case analyses. These comparative estimates were associated with a very high (i.e., nearly 100%) probability that ibrutinib was the most effective treatment within the network.
| Ibrutinib versus Obi-Chl | Ibrutinib versus R-Chl | Ibrutinib versus Ofa-Chl | Ibrutinib versus bendamustine | |
|---|---|---|---|---|
| INV-assessed PFS (≥65 years subgroup) HR [95% CrI] Probability ibrutinib is better | 0.41 [0.19, 0.89] 98.8% | 0.19 [0.09, 0.41] 100.0% | NA | NA |
| INV-assessed PFS (subgroup with 11q mutation) HR [95% CrI] Probability ibrutinib is better | 0.06 [0.01, 0.58] 99.9% | 0.02 [0, 0.21] 100.0% | NA | NA |
| INV-assessed PFS (IgVH unmutated subgroup) HR [95% CrI] Probability ibrutinib is better | 0.27 [0.04, 1.68] 91.8% | 0.11 [0.04, 0.34] 100.0% | NA | NA |
| INV-assessed PFS (subgroup without 17p) HR [95% CrI] Probability ibrutinib is better | 0.35 [0.16, 0.75] 99.7% | 0.20 [0.1, 0.43] 100.0% | NA | NA |
| OS (≥65 years subgroup) OR [95% CrI]† | NA | NA | NA | 0.18 [0.05, 0.67] |
| DAE (≥65 years subgroup) OR [95% CrI]† | NA | NA | 0.37 [0.12, 0.84] | NA |
†A total of 31% patients in the COMPLEMENT1 ITT population were younger than 65 years.
Chl: Chlorambucil; CrI: Credible interval; DAE: Discontinuation due to adverse event; HR: Hazard ratio; INV: Investigator; NA: Not available; NMA: Network meta-analysis; Obi-Chl: Obinutuzumab + chlorambucil; Ofa-Chl: Ofatumumab + chlorambucil; OR: Odds ratio; OS: Overall survival; PFS: Progression-free survival; R-Chl: Chlorambucil + rituximab.
Discussion
The NMA results for the overall front-line CLL population showed that ibrutinib treatment was associated with greater benefit than other treatments in improving IRC- and INV-assessed PFS and OS. Specifically, ibrutinib showed the highest probability of being the most effective treatment in the network in terms of improving both IRC-assessed PFS (59.9%) and OS (87.7%). Also, NMA results for all survival outcomes were very similar when the network was restricted to studies in fludarabine-ineligible patients only, with ibrutinib again having the highest probability of being the most effective treatment in the network in terms of IRC-assessed PFS (62.7%) and OS (89.9%). Ibrutinib showed the lowest risk in the network for negative safety outcomes, including likelihood of experiencing TDs and DAEs in both the overall front-line population and in the fludarabine-ineligible population. The safety outcomes indicate with high certainty that ibrutinib resulted in fewer patients with TDs and DAEs than each of the other treatments. In addition, subgroup analyses showed that ibrutinib had either comparable (age ≥65 years subgroup, subgroup without del17p) or superior (subgroup with del11q, IgVH unmutated subgroup) treatment effect estimates compared with those demonstrated in the general fludarabine-ineligible NMA. Overall, therefore, the NMA results provide strong evidence that ibrutinib offers better efficacy and safety outcomes than does a range of comparators, especially in high-risk, previously untreated patients with genetic mutations.
Of note, the data source for ibrutinib was the RESONATE-2 trial with a median follow-up of 18.4 months [13]. Survival data at a longer follow-up from this study were recently published [57]; however, these were not used because by this time 41% of the patients originally randomized to chlorambucil had crossed over to the ibrutinib arm; an NMA based on this data cut would have produced a substantially increased survival estimate for chlorambucil and significantly underestimated the survival benefit from ibrutinib. Therefore, the NMA used the data cut per the final trial analyses reported in Burger et al. [13] at which point the much lower proportion of patients who had switched to ibrutinib upon progression would have had only a minor effect on the estimated relative efficacy of the two treatments.
It is worth highlighting that there were between-study variations in age, patient fitness, presence of cytogenetic mutations and disease severity, and the cumulative dosage of the common comparator, chlorambucil. However, only characteristics known to be potential treatment-effect-modifiers are of relevance for the interpretation of the NMA results. Across the 13 RCTs, two studies excluded patients with del17p mutation, whereas IgVH mutation status or presence of del11q mutation was inconsistently reported across the studies. All of these characteristics are known to be adverse prognostic factors and potential treatment-effect-modifiers [6,7]. The impact of these differences on relative treatment effects was studied by performing subgroup analyses. These showed comparable or even larger benefit estimates for ibrutinib relative to comparators in the subgroups of patients with del11q and unmutated IgVH. The issue of whether differences in reported dosing of chlorambucil-impacted outcomes were explored by regression analyses for PFS and OS using 24-week cumulative chlorambucil dose as covariate. Regression analysis was performed for all studies identified in the SLR that had a chlorambucil treatment arm. The regression analysis (results not shown) indicated a very weak correlation between chlorambucil dose and PFS across fludarabine-ineligible studies, and a strong correlation between chlorambucil dose and PFS outcomes in the overall front-line population. This strong correlation was driven by a small number of studies conducted in young/fit patients, with relatively high chlorambucil dose. These results suggested that in the overall front-line population, the survival advantages of ibrutinib observed in the NMAs were conservative, given that they were demonstrable despite the bias toward better treatment outcomes from regimens that involved a high cumulative dose of chlorambucil. Also, the lack of correlation in the regression analysis of fludarabine-ineligible population, offers reassurance that any differences in cumulative chlorambucil dose did not introduce significant bias with regards to relative treatment effects in the survival NMAs conducted for that group.
Differences in the treatment schedules of the compared regimens complicate the interpretation of the analyzed safety outcomes, which comprised the proportion of patients with TDs and with DAEs. Importantly, ibrutinib was the only treat-to-progression treatment in contrast to all other interventions, which had fixed treatment durations. Once administration of a fixed-duration regimen is complete, the ratio of discontinuations between treatment arms does not change. However, with the ibrutinib treat-to-progression approach, patients were continually exposed to treatment and therefore continued to be at risk for TDs and DAEs. Outcomes for TD and DAE in this analysis were not adjusted for exposure time as no such data are available in any of the included studies publications, meaning that the reported safety outcomes are conservative for ibrutinib. This difference in the treatment schedule of ibrutinib compared with the other treatments is expected to have a substantial impact on the relative safety outcomes, with likely underestimation of the safety benefits of ibrutinib treatment.
Our analysis follows several previous NMAs conducted to compare PFS and OS outcomes of treatment regimens for the front-line treatment of CLL. However, we are not aware of any other that has been conducted since the publication of the pivotal front-line study of ibrutinib, RESONATE-2 and none of the previously published NMAs include ibrutinib in the studied networks. It is notable, though, that results for treatment regimens that were common across all these NMAs are consistent with the current analysis.
This broad agreement in findings is exemplified by the results of an NMA by Rancea et al. that included 33 RCTs of front-line treatment for patients with untreated CLL, evidence that was presented at the 19th Congress of the European Hematology Association (2014) [58]. The network in this study included 21 regimens for front-line CLL that were compared with chlorambucil in terms of their effect on PFS and OS [58]. Obi-Chl and FCR showed 99 and 95% probabilities of providing greater PFS benefit than chlorambucil, respectively (probability of each being the most effective treatment for PFS in the network not presented); whereas results for OS ranked Obi-Chl first (72%), followed by BR (16%), with FCR ranked fifth (1%) [58]. In the current analyses, ibrutinib had the highest probability of being the most effective of all front-line treatments in the network in terms of improving both PFS and OS (59.9 and 87.7%), followed by Obi-Chl (21.8 and 9.2%), bendamustine (9.8 and 0.2%), BR (0.8 and 2.4%) and FCR (7.8 and 0.1%). In summary, the Rancea NMA found that Obi-Chl had the highest probability of being the best treatment in improving OS [58], a result in line with findings of the present analysis, which ranked Obi-Chl second, after ibrutinib.
A more recent NMA by Stadler et al. compared the relative efficacy of front-line treatments (excluding ibrutinib) in patients with CLL who were unfit (because of comorbidities and/or ineligibility for full-dose fludarabine), in terms of PFS and OS, across eight RCTs [59]. The NMA (fixed-effects) results for PFS indicated Obi-Chl was ranked first (with a 56% probability of being the most effective), followed by reduced-dose FCR, BR, R-Chl, Ofa-Chl, fludarabine monotherapy and chlorambucil monotherapy [59]. The OS results were generally consistent with the PFS results, indicating an OS advantage with Obi-Chl over the other treatments [59]. The NMA presented in this paper shows that when included in the network of evidence, ibrutinib is the most effective treatment (i.e., ranked first, with the highest probability for OS and PFS). Obi-Chl was ranked the second most effective treatment, which is in line with previously published NMAs (that did not include ibrutinib) that ranked Obi-Chl first.
The presented analyses have various strengths. They were performed using a Bayesian analytic framework, which allowed the ranking of treatments in terms of various efficacy and safety end points. This approach provided a systematic and structured means of establishing relative outcomes for treatment arms that had not been directly compared in a head-to-head trial. Also, a wide range of front-line treatment regimens were included in the network, specifically reflecting recommendations in current treatment guidelines, and this is the first published indirect treatment comparison for front-line CLL treatment that includes ibrutinib.
There are also some limitations to our analyses, arising mainly from lack of data availability for some of the end points of interest, and inconsistency of data reporting across the included RCTs. An example is PFS, the most commonly reported outcome across the overall network. The definitions of this outcome were largely consistent across studies, with reporting of both INV- and IRC-assessed PFS. However, this approach was not used in one of the fludarabine-ineligible studies (MaBLe), and five of the fludarabine-eligible studies did not specify whether PFS was assessed by INV or IRC. In reality, these limitations would appear to have little or no bearing on the key findings of the NMA, given the broad consistency between the INV-assessed and IRC-assessed PFS results. Another limitation was that the reporting of safety outcomes was relatively sparse across the fludarabine-eligible RCTs. However, safety outcomes were more consistently reported across the fludarabine-ineligible RCTs, such that only one study (MaBLe) did not report the proportion of patients with either TDs or DAEs. Therefore, confident conclusions can be drawn about comparative treatment effects in a subgroup for whom therapeutic options are already more limited than for patients with CLL in general. The studies also varied in the range of follow-up periods (between 18 and 83 months). However, this is to be expected when the network includes both older studies, for which multiple time points may be reported, and more recent studies, for which follow-up to data might be more limited. This limitation can be overcome by updating the NMA results once data from the newer studies with longer follow-up periods become available. Finally, while the cut-off date for the SLR in our study (October 2015) could be seen as a limitation, in reality, an updated search conducted in April 2017 found no additional RCTs that would change the network for either the overall or the fludarabine-ineligible CLL population.
Conclusion
Overall, the results of the NMA demonstrate a clear therapeutic advantage for ibrutinib in the front-line treatment of CLL over other currently available treatment regimens in PFS, OS and safety outcomes. The observed treatment benefit was consistent in key high-risk subgroups and across both the overall network (patients considered eligible for full-dose fludarabine treatment) and the fludarabine-ineligible network (those considered ineligible due to patient age and fitness).
There are numerous front-line treatment options for chronic lymphocytic leukemia (CLL), but the limited number of head-to-head clinical trials results in uncertainty regarding optimal treatment regimens for patient groups with differing levels of fitness.
A systematic literature review without temporal limits was performed using MEDLINE, Medline In-Process, Embase, Embase In-Process, Cochrane Collection Central Register of Clinical Trials (CENTRAL) and Database of Abstracts of Reviews of Effects.
Relative treatment effects of progression-free survival, overall survival and safety outcomes were estimated via network meta-analysis (NMA).
Two networks, one based on an ‘overall’ patient population, leveraging data from 15 studies, and one based on a ‘fludarabine-ineligible’ patient population, leveraging data from five studies, were established and analyzed. Subgroup analyses explored relative treatment effects in patients with known treatment-effect-modifying characteristics.
The ‘overall’ NMA network (overall front-line CLL population) included >5300 patients from 15 studies; of these, five were conducted in ‘fludarabine-ineligible’ patients, making up the ‘fludarabine-ineligible’ network. The base-case NMA for each network indicated that ibrutinib was superior to the other treatments in terms of progression-free survival and overall survival, and had the highest probability of having the lowest risk of discontinuations overall.
Ibrutinib provides a clear benefit in survival and safety outcomes for front-line treatment of patients with CLL, including high-risk subgroups and patients considered ineligible for full-dose fludarabine treatment.
Financial & competing interests disclosure
Janssen-Cilag Ltd funded the study reported in this manuscript, development of the manuscript and the article processing charges. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and the accuracy of the data analysis. S Baculea, S Côté, S van Sanden and J Diels are employees of Janssen-Cilag Ltd. Y Xu, E Dorman and K Fahrbach are employees of Evidera, a research and consulting firm for the biopharma industry. As a condition of their salaried employment, they are precluded from accepting any payment or honoraria directly from Evidera clients. Evidera received funding from Janssen-Cilag Ltd. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing assistance was utilized in the production of this manuscript. R Sallum (a former employee of Evidera) contributed substantially to the design and implementation of the SLR and NMA reported in this manuscript. Editorial assistance for the preparation of this manuscript was provided by L Rutherford of Evidera. C Gulea supported the execution of the SLR and write up of technical reports for both SLR and NMAs. Support for these contributions was funded by Janssen-Cilag Ltd.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Eichhorst B, Robak T, Montserrat E et al. Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 26(Suppl. 5), V78–V84 (2015). www.esmo.org/Guidelines/Haematological-Malignancies/Chronic-Lymphocytic-Leukaemia/eUpdate-Treatment-Recommendations.
• Illustrates how quickly the treatment landscape for front-line chronic lymphocytic leukaemia (CLL) is changing. The previous version of the European Society for Medical Oncology guidance was issued only a year before this 2015 version and updates were issued electronically in both 2016 and June 2017.
2.
American Cancer Society. Cancer Facts & Figures 2017. American Cancer Society, GA, USA (2017). www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2017.html.
3.
Byrd JC, Brown JR, O'brien S et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N. Engl. J. Med. 371(3), 213–223 (2014).
4.
Roberts AW, Davids MS, Pagel JM et al. Targeting BCL2 with Venetoclax in relapsed chronic lymphocytic leukemia. N. Engl. J. Med. 374(4), 311–322 (2016).
5.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: chronic lymphocytic leukemia/small lymphocytic lymphoma. Version 1.2017 (2016). www.nccn.org/professionals/physician_gls/pdf/cll.pdf.
6.
Pflug N, Bahlo J, Shanafelt TD et al. Development of a comprehensive prognostic index for patients with chronic lymphocytic leukemia. Blood 124(1), 49–62 (2014).
7.
Zent CS, Kay NE. Management of patients with chronic lymphocytic leukemia with a high risk of adverse outcome: the Mayo Clinic approach. Leuk. Lymphoma 52(8), 1425–1434 (2011).
8.
Van Sanden S, Baculea S, Diels J, Cote S. Comparative efficacy of ibrutinib versus obinutuzumab + chlorambucil in first line treatment of chronic lymphocytic leukemia: a matching-adjusted indirect comparison. Adv. Ther. 34(7), 1650–1661 (2017).
9.
Eichhorst B, Fink AM, Bahlo J et al. First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukaemia (CLL10): an international, open-label, randomised, Phase III, non-inferiority trial. Lancet Oncol. 17(7), 928–942 (2016).
10.
Caldwell DM, Ades AE, Higgins JP. Simultaneous comparison of multiple treatments: combining direct and indirect evidence. BMJ 331(7521), 897–900 (2005).
• Details the methodological underpinning of network meta-analyses (NMAs), the methodology used in the current analysis.
11.
Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 23(20), 3105–3124 (2004).
12.
Goede V, Fischer K, Busch R et al. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N. Engl. J. Med. 370(12), 1101–1110 (2014).
• It reports the efficacy and safety findings from the CLL11 pivotal trial upon which the primary NMAs are based.
13.
Burger JA, Tedeschi A, Barr PM et al. Ibrutinib as initial therapy for patients with chronic lymphocytic leukemia. N. Engl. J. Med. 373(25), 2425–2437 (2015).
14.
Michallet AS. Rituximab in combination with bendamustine or chlorambucil for the treatment of chronic lymphocytic leukemia: primary results from the randomised Phase IIIb MABLE study. Presented at: XVI International Workshop on Chronic Lymphocytic Leukaemia. Sydney, Australia, 7–9 September, 2015.
15.
Catovsky D, Richards S, Matutes E et al. Assessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukaemia (the LRF CLL4 Trial): a randomised controlled trial. Lancet 370(9583), 230–239 (2007).
16.
Rai KR, Peterson BL, Appelbaum FR et al. Fludarabine compared with chlorambucil as primary therapy for chronic lymphocytic leukemia. N. Engl. J. Med. 343(24), 1750–1757 (2000).
17.
Mulligan SP, Karlsson K, Stromberg M et al. Cladribine prolongs progression-free survival and time to second treatment compared with fludarabine and high-dose chlorambucil in chronic lymphocytic leukemia. Leuk. Lymphoma 55(12), 2769–2777 (2014).
18.
Eichhorst BF, Busch R, Stilgenbauer S et al. First-line therapy with fludarabine compared with chlorambucil does not result in a major benefit for elderly patients with advanced chronic lymphocytic leukemia. Blood 114(16), 3382–3391 (2009).
19.
Hillmen P, Robak T, Janssens A et al. Chlorambucil plus ofatumumab versus chlorambucil alone in previously untreated patients with chronic lymphocytic leukaemia (COMPLEMENT 1): a randomised, multicentre, open-label Phase III trial. Lancet 385(9980), 1873–1883 (2015).
• Reports the efficacy and safety findings from the COMPLEMENT1 pivotal trial upon which the primary NMAs are based.
20.
Hallek M, Fischer K, Humphrey K et al. Obinutuzumab (GA101) + chlorambucil (CLB) or rituximab (R) + CLB versus CLB alone in patients with chronic lymphocytic leukaemia (CLL) and pre-existing medical conditions (comorbidities): final stage 1 results of the CLL11 (BO21004) Phase III trial. Hematol. Oncol. 31(Suppl. 1), 114 (2013).
21.
Goede V, Fischer K, Busch R et al. Head-to-head comparison of obinutuzumab (GA101) plus chlorambucil (Clb) versus rituximab plus Clb in patients with chronic lymphocytic leukemia (CLL) and co-existing medical conditions (comorbidities): final stage 2 results of the CLL11 trial. Presented at: The 55th American Society of Hematology (ASH) Annual Meeting and Exposition. LA, USA, 7–10 December. Blood 122(21), 6 (2013).
22.
Goede V, Fischer K, Humphrey K et al. Obinutuzumab (GA101) + chlorambucil (CLB) or rituximab (R) + CLB versus CLB alone in patients with chronic lymphocytic leukaemia (CLL) and pre-existing medical conditions (comorbidities): final stage 1 results of the CLL11 (BO21004) Phase III trial. Presented at: ASCO Annual Meeting 2013. IL, USA, 31 May–4 June 2013.
23.
Knauf WU, Lissitchkov T, Aldaoud A et al. Bendamustine compared with chlorambucil in previously untreated patients with chronic lymphocytic leukaemia: updated results of a randomized Phase III trial. Br. J. Haematol. 159(1), 67–77 (2012).
• Reports the efficacy and safety findings from one of the pivotal trials upon which the primary NMAs are based.
24.
Knauf WU, Lissitchkov T, Aldaoud A et al. Bendamustine versus chlorambucil in treatment-naive patients with B cell chronic lymphocytic leukemia (B-CLL): results of an international Phase III study. Blood 110, Abstract 2043 (2007).
25.
Knauf WU, Lissichkov T, Aldaoud A et al. Phase III randomized study of bendamustine compared with chlorambucil in previously untreated patients with chronic lymphocytic leukemia. J. Clin. Oncol. 27(26), 4378–4384 (2009).
26.
Karlsson K, Stromberg M, Jonsson V, Mulligan SP, Liliemark J, Juliusson G. Cladribine (CdA) gives longer response duration than fludarabine (F) and high-dose intermittent chlorambucil (Chl) as first-line treatment of symptomatic chronic lymphocytic leukemia (CLL). First results from the international randomized Phase III trial. Blood 110, Abstract 630 (2007).
27.
Karlsson K, Stromberg M, Jonsson V et al. Cladribine (CdA) or fludarabine (F) or high-dose intermittent chlorambucil (Chl) as first-line treatment of symptomatic chronic lymphocytic leukemia? First interim analysis of data from the international randomized Phase III trial. Blood 104, Abstract 3470 (2004).
28.
Eichhorst BF, Busch R, Hopfinger G et al. Fludarabine plus cyclophosphamide versus fludarabine alone in first-line therapy of younger patients with chronic lymphocytic leukemia. Blood 107(3), 885–891 (2006).
29.
Eichhorst B, Busch R, Emmerich B, Hallek M et al. Fludarabine plus cyclophosphamide (FC) induces higher remission rates and longer progression free survival (PFS) than fludarabine (F) alone in first line therapy of younger patients (Pts) with chronic lymphocytic leukemia (CLL): results of a Phase III study of the German CLL Study Group (GCLLSG). Ann. Oncol. 16(Suppl. 5), V89–V90 (2005).
30.
Eichhorst B, Busch R, Hopfinger G et al. Fludarabine plus cyclophosphamide (FC) is superior to fludarabine (F) alone in first line therapy of chronic lymphoblastic leukemia (CLL): results of a Phase III study of the German CLL Study Group (GCLLSG). Haematologica 90(S2), 144 (2005).
31.
Eichhorst B, Busch R, Hopfinger G et al. Fludarabine plus cyclophosphamide (FC) induces higher remission rates and longer progression free survival (PFS) than fludarabine alone in first line therapy of advanced chronic lymphocytic leukemia (CLL): results of a Phase III study (CLL4 protocol). Blood 102(11), 72a (2003).
32.
Eichhorst BF, Busch R, Schweighofer C et al. Due to low infection rates no routine anti-infective prophylaxis is required in younger patients with chronic lymphocytic leukaemia during fludarabine-based first line therapy. Br. J. Haematol. 136(1), 63–72 (2007).
33.
Flinn IW, Neuberg DS, Grever MR et al. Phase III trial of fludarabine plus cyclophosphamide compared with fludarabine for patients with previously untreated chronic lymphocytic leukemia: US Intergroup Trial E2997. J. Clin. Oncol. 25(7), 793–798 (2007).
34.
Grever MR, Lucas DM, Dewald GW et al. Comprehensive assessment of genetic and molecular features predicting outcome in patients with chronic lymphocytic leukemia: results from the US Intergroup Phase III Trial E2997. J. Clin. Oncol. 25(7), 799–804 (2007).
35.
Morrison VA, Rai KR, Peterson BL et al. Impact of therapy with chlorambucil, fludarabine, or fludarabine plus chlorambucil on infections in patients with chronic lymphocytic leukemia: Intergroup Study Cancer and Leukemia Group B 9011. J. Clin. Oncol. 19(16), 3611–3621 (2001).
36.
Skowronska A, Parker A, Ahmed G et al. Biallelic ATM inactivation significantly reduces survival in patients treated on the United Kingdom leukemia research fund chronic lymphocytic leukemia 4 trial. J. Clin. Oncol. 30(36), 4524–4532 (2012).
37.
Dearden CE, Richards S, Else M, Catovsky D, Hillmen P. A comparison of the efficacy and safety of oral and intravenous fludarabine in chronic lymphocytic leukemia in the LRF CLL4 trial. Cancer 117(11), 2452–2460 (2011).
38.
Cramer P, Fink AM, Busch R et al. Second-line therapies of patients initially treated with fludarabine and cyclophosphamide or fludarabine, cyclophosphamide and rituximab for chronic lymphocytic leukemia within the CLL8 protocol of the German CLL Study Group. Leuk. Lymphoma 54(8), 1821–1822 (2013).
39.
Adena M, Houltram J, Mulligan SP, Todd C, Malanos G. Modelling the cost–effectiveness of rituximab in chronic lymphocytic leukaemia in first-line therapy and following relapse. Pharmacoeconomics 32(2), 193–207 (2014).
40.
Hallek M, Fischer K, Fingerle-Rowson G et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, Phase III trial. Lancet 376(9747), 1164–1174 (2010).
41.
Main C, Pitt M, Moxham T, Stein K. The clinical and cost–effectiveness of rituximab for the 1st line treatment of chronic lymphocytic leukaemia: an evidence review of the submission from Roche. Produced by the Peninsula Technology Assessment Group (Pentag) on behalf of the National Institute of Health and Care Excellence (NICE). NICE, London (2009). www.nice.org.uk/guidance/ta174/documents/leukaemia-chronic-lymphocytic-first-line-rituximab-evidence-review-group-report2.
42.
Hallek M, Fingerle-Rowson G, Fink AM et al. Immunochemotherapy with fludarabine (F), cyclophosphamide (C), and rituximab (R) (FCR) versus fludarabine and cyclophosphamide (FC) improves response rates and progression-free survival (PFS) of previously untreated patients (pts) with advanced chronic lymphocytic leukemia (CLL). Presented at: 50th ASH Annual Meeting and Exposition. CA, USA, 6–9 December, 2008.
43.
Stilgenbauer S, Schnaiter A, Paschka P et al. Gene mutations and treatment outcome in chronic lymphocytic leukemia: results from the CLL8 trial. Blood 123(21), 3247–3254 (2014).
44.
Eichhorst B, Bahlo J, Stauch M et al. First line therapy of elderly patients with chronic lymphocytic leukaemia (CLL) – long term follow-up (FU) results of a randomized Phase III study of the German CLL Study Group (CLL5 study of the GCLLSG). Oral presentation (Abstract 107) presented at: 12th International Conference on Malignant Lymphoma. Lugano, Switzerland, 19–22 June 2013. Hematol. Oncol. 31(Suppl. 1), 132 (2013).
45.
Eichhorst B, Busch R, Stauch M et al. Fludarabine (F) induces higher response rates and longer event free survival in first line therapy of older patients (pts) with advanced chronic lymphocytic leukemia (CLL) than chlorambucil: interim analysis of a Phase Ill study of the German CLL Study Group (GCLLSG). Onkologie 27(Suppl. 3), O145 (2004).
46.
Eichhorst B, Busch R, Stauch M et al. No significant clinical benefit of first line therapy with fludarabine (F) in comparison to chlorambucil (Clb) in elderly patients (Pts) with advanced chronic lymphocytic leukemia (CLL): results of a Phase III study of the German CLL Study Group (GCLLSG). Blood 110(11), 629 (2007).
47.
Schmitt B, Kneba M, Ritgen M et al. First line therapy with fludarabine versus chlorambucil for patients with advanced chronic lymphocytic leukemia (CLL) older than 65 years: first interim analysis of a Phase Ill study (CLL5 protocol) of the German CLL Study Group (GCLLSG). Onkologie 25(4), 170 (2002).
48.
Eichhorst B, Busch R, Stauch M et al. Fludarabine (F) induces higher response rates in first line therapy of older patients (pts) with advanced chronic lymphocytic leukemia (CLL) than chlorambucil: interim analysis of a Phase III study of the German CLL Study Group (GCLLSG). Blood 102(11), 109a (2003).
49.
Jaksic B, Brugiatelli M, Suciu S et al. Fludarabine versus high-dose continuous chlorambucil in untreated patients with B-CLL: results of CLL1 EORTC randomized trial. Hematol. Cell Ther. 42(1), 97 (2000).
50.
Jaksic B, Delmer A, Brugiatelli M et al. Fludarabine vs. high dose continuous chlorambucil: interim analysis of a randomized Phase II study in untreated B-cell chronic lymphocytic leukemia (B-CLL). Blood 88(10 Suppl. 1), 588a (1996).
51.
Jaksic B, Brugiatelli M, Suciu S et al. Randomized Phase II study in untreated B-cell chronic lymphocytic leukemia (B:CLL) comparing fludarabine (FAMP) vs. high dose continuous chlorambucil (HD-CLB). Blood 92(10 Suppl. 1), 103a (1998).
52.
Eichhorst B, Fink AM, Busch R et al. Chemoimmunotherapy with fludarabine (F), cyclophosphamide (C), and rituximab (R) (FCR) versus bendamustine and rituximab (BR) in previously untreated and physically fit patients (pts) with advanced chronic lymphocytic leukemia (CLL): results of a planned interim analysis of the CLL10 trial, an international, randomized study of the German CLL study group (GCLLSG). Abstract presented at: 55th American Society of Hematology Annual Meeting and Exposition. LA, USA, 7–13 December 2013. Blood 122(21), 526 (2013).
53.
Langerbeins P, Busch R, Schweighofer C et al. Severe infections are more common in physically fit CLL patients with FCR-therapy compared to BR: results of the intermin-analysis of the CLL10 trial of the German Cll Study Group. www.newevidence.com/oncology/wp-content/uploads/2015/07/journal-201409.pdf.
54.
Eichhorst B, Fink AM, Busch R et al. Frontline chemoimmunotherapy with fludarabin (F), cyclophosphamide (C), and rituximab (R) (FCR) shows superior efficacy in comparison to bendamustine (B) and rituximab (BR) in previously untreated and physically fit patients (pts) with advanced chronic lymphocytic leukemia (CLL): final analysis of an international randomized study of the German CLL Study Group (GCLLSG) (CLL10 study). Blood 124(21), 19 (2014).
55.
Rai KR, Peterson B, Elias L et al. A randomized comparison of fludarabine and chlorambucil for patients with previously untreated chronic lymphocytic leukemia. A CALGB, SWOG, CTG/NCI-C and ECOG inter-group study. Blood 88(Suppl. 10), 141a (1996).
56.
Rai KR, Peterson B, Kolitz J et al. Fludarabine induces a high complete remission rate in previously untreated patients with active chronic lymphocytic leukemia (CLL). A randomized inter-group study. Blood 86(10 Suppl. 1), Abstract 2414 (1995).
57.
Barr PM, Robak T, Owen CJ et al. Updated efficacy and safety from the Phase III RESONATE-2 study: ibrutinib as first-line treatment option in patients 65 years and older with chronic lymphocytic leukemia/small lymphocytic leukemia. Abstract presented at: American Society of Hematology 58th Annual Meeting & Exposition, CA, USA, 3–6 December 2016. Blood 128(22), 234 (2016).
• Reports the efficacy and safety findings from the RESONATE-2 pivotal trial upon which the primary NMAs are based.
58.
Rancea M, Skoetz N, Trelle S et al. First-line treatment strategies for previously untreated patients with chronic lymphocytic leukaemia: preliminary results of a network meta-analysis. Presented at: 19th Congress of the European Hematology Association. Milan, Italy, 12–15 June 2014.
59.
Stadler N, Shang A, Bosch F et al. A systematic review and network meta-analysis to evaluate the comparative efficacy of interventions for unfit patients with chronic lymphocytic leukemia. Adv. Ther. 33(10), 1814–1830 (2016).
Information & Authors
Information
Published In
Copyright
© 2017 Janssen-Cilag Ltd.
History
Received: 12 October 2017
Accepted: 14 November 2017
Published online: 6 December 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Front-line treatment of patients with chronic lymphocytic leukemia: a systematic review and network meta-analysis. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0086
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yen-Chou Chen, Paulo Miranda, Yazan K. Barqawi, Grace E. Fox, Chinenye Chukwu, Javid Moslehi, Rupal P. O’Quinn, Cardiovascular Safety Outcomes of Chronic Lymphocytic Leukemia Treatments: A Systematic and Targeted Literature Review, Critical Reviews in Oncology/Hematology, 10.1016/j.critrevonc.2025.104877, (104877), (2025).
- Tingyu Wen, Guangyi Sun, Wenxin Jiang, Kat Steiner, Suzannah Bridge, Peng Liu, Comparing the efficacy and safety of first-line treatments for chronic lymphocytic leukemia: a network meta-analysis, JNCI: Journal of the National Cancer Institute, 10.1093/jnci/djae245, 117, 2, (322-334), (2024).
- Monia Marchetti, Paolo Rivela, Claudia Bertassello, Manuela Canicattì, Comparative Clinical Value of Pharmacologic Therapies for B-Cell Chronic Lymphocytic Leukemia: An Umbrella Analysis, Journal of Clinical Medicine, 10.3390/jcm11071868, 11, 7, (1868), (2022).
- Kai Wen Chen, David Owen Rees, David Watson, Mared Owen-Casey, Unusual cause of light chain cast nephropathy, BMJ Case Reports, 10.1136/bcr-2021-246777, 15, 3, (e246777), (2022).
- Neda Alrawashdh, Daniel O Persky, Ali McBride, Joann Sweasy, Brian Erstad, Ivo Abraham, Comparative Efficacy of First-Line Treatments of Chronic Lymphocytic Leukemia: Network Meta-Analyses of Survival Curves, Clinical Lymphoma Myeloma and Leukemia, 10.1016/j.clml.2021.06.010, 21, 11, (e820-e831), (2021).
- Matthew S. Davids, Catherine Waweru, Pauline Le Nouveau, Amie Padhiar, Gautamjeet Singh, Sarang Abhyankar, Veronique Leblond, Comparative Efficacy of Acalabrutinib in Frontline Treatment of Chronic Lymphocytic Leukemia: A Systematic Review and Network Meta-analysis, Clinical Therapeutics, 10.1016/j.clinthera.2020.08.017, 42, 10, (1955-1974.e15), (2020).
- Steven E. Coutre, John C. Byrd, Peter Hillmen, Jacqueline C. Barrientos, Paul M. Barr, Stephen Devereux, Tadeusz Robak, Thomas J. Kipps, Anna Schuh, Carol Moreno, Richard R. Furman, Jan A. Burger, Michael O’Dwyer, Paolo Ghia, Rudolph Valentino, Stephen Chang, James P. Dean, Danelle F. James, Susan M. O’Brien, Long-term safety of single-agent ibrutinib in patients with chronic lymphocytic leukemia in 3 pivotal studies, Blood Advances, 10.1182/bloodadvances.2018028761, 3, 12, (1799-1807), (2019).
- Tadeusz Robak, Jan A. Burger, Alessandra Tedeschi, Paul M. Barr, Carolyn Owen, Osnat Bairey, Peter Hillmen, David Simpson, Sebastian Grosicki, Stephen Devereux, Helen McCarthy, Steven E. Coutre, Hang Quach, Gianluca Gaidano, Zvenyslava Maslyak, Don A. Stevens, Carol Moreno, Devinder S. Gill, Ian W. Flinn, John G. Gribben, Ahmad Mokatrin, Mei Cheng, Lori Styles, Danelle F. James, Thomas J. Kipps, Paolo Ghia, Single‐agent ibrutinib versus chemoimmunotherapy regimens for treatment‐naïve patients with chronic lymphocytic leukemia: A cross‐trial comparison of phase 3 studies, American Journal of Hematology, 10.1002/ajh.25259, 93, 11, (1402-1410), (2018).