The clinical effectiveness of insulin glargine in patients with Type I diabetes in Brazil: findings and implications
Abstract
Aim: Published studies have challenged the cost–effectiveness of insulin glargine versus neutral protamine hagedorn (NPH) insulins in Brazil with limited evidence of increased effectiveness despite considerably higher acquisition costs. However, still a controversy. Consequently, there is a need to address this. Materials & methods: Retrospective cohort study of Type I diabetes patients receiving insulin glargine in Brazil following NPH insulin who met the criteria. Results: 580 patients were enrolled. HbA1c varied from 8.80 ± 1.98% in NPH insulin users to 8.54 ± 1.88% after insulin glargine for 6 months, which is not clinically significant. Frequency of glycemic control varied from 22.6% with NPH insulin to 26.2% with insulin glargine. No statistically significant difference was observed between controlled and still uncontrolled groups for all analyzed factors including type and frequency of insulin use and carbohydrate counting. Conclusion: Limited differences between NPH insulins and insulin analogs in routine clinical care do not justify an appreciable cost difference.
First draft submitted: 22 December 2016; Accepted for publication: 25 April 2017; Published online: 29 September 2017
Type I diabetes is a chronic disease resulting from the inability of the pancreas to produce insulin [1]. In view of the natural history of Type I diabetes, the use of insulin immediately after diagnosis is advocated to adequately treat these patients [2]. The most widely used insulins are called neutral protamine hagedorn (NPH) insulins and fast-acting insulin (soluble insulin). However, in order to make the profile of injected insulins closer to physiological insulins, insulin analogs were created (insulin glargine and insulin detemir) which have a prolonged action.
There are concerns though with the cost–effectiveness of long acting insulins versus NPH insulins, especially where there are appreciable cost differences as currently seen in Brazil [3,4]. Published studies, including systematic reviews and reviews by health authorities, have demonstrated no superiority of insulin glargine in terms of effectiveness and safety compared with NPH insulin [3–11]. Other studies however, have found the opposite. Raskin et al. showed a greater efficacy of insulin glargine in reducing HbA1c [12]. Herwig et al. (2007), Schreiber et al. and Salemyr et al. also showed that patients with Type I diabetes using insulin glargine achieved a better response in terms of glycemic control and decreasing HbA1c when compared with those using NPH insulin [13–15]. The differences in the findings may reflect the study sponsors as seen in our recent meta-analysis of cohort studies comparing the effectiveness of insulin glargine versus NPH insulin [4].
Consequently, in view of current controversies, we wished to undertake our own cohort study evaluating the effectiveness of insulin glargine versus NPH insulin for the treatment of patients with Type I diabetes to support decision making for greater efficiency within our healthcare system. This study aimed to evaluate the effectiveness of insulin glargine compared with NPH insulin for patients with Type I diabetes in routine clinical care within Brazil.
Materials & methods
Sample
This study was conducted in accordance with the Declaration of Helsinki. A historical cohort was conducted from January 2011 to January 2015, including users of the Specialized Pharmaceutical Care Component of the Brazilian National Healthcare system (SUS) in Minas Gerais, developed from the construction of a database of individuals with Type I diabetes treatment, registered according to the clinical protocol and therapeutic guidelines for insulin glargine use in Brazil [16]. Patients have to fulfill these criteria in order to have their insulin approved and reimbursed [17].
To analyze the clinical effectiveness, individuals were compared with themselves in an analysis of HbA1c values before and after 6 months of using insulin glargine. In this way, each patient acted as their own control thereby avoiding concerns with randomization in routine clinical care.
Individuals who met the eligibility criteria were included in the cohort. These included: (i) patients who had been diagnosed with Type I diabetes or latent autoimmune diabetes in adults; (ii) whose cases met the inclusion criteria described in the clinical protocol and therapeutic guidelines (Supplementary Table 1); (iii) were currently on NPH insulin and who had not used long-acting insulin analogs prior to the approved use of insulin glargine; (iv) whose inclusion in the program was between January 2011 and January 2015; and (v) who had at least two renewal processes for insulin glargine evaluated by reviewers of SUS Collaborating Centre – Technology Assessment and Excellence in Health (CCATES). The SUS CCATES is a part of the National Network for Technology Assessment in Health (REBRATS) in Brazil. CCATES has an institutional partnership with the Ministry of Health and the Health department of Minas Gerais. Among its many activities, CCATES undertakes the analysis of administrative and judicial requests for medicines, medical procedures, and devices, and develops rapid advice on issues relevant to health for the Ministry of Health. Individuals who were excluded at the first request to administer of insulin glargine or insulin detemir as part of SUS, or patients whose term renewal request had exceeded 9 months from the last release date, were excluded.
Study variables
Outcomes were assessed from the following variables: (i) demographic variables – ethnicity, sex and age; (ii) clinical variables – time with a diagnosis of Type I diabetes, age at diagnosis and reporting of comorbidities of individuals at baseline; (iii) treatment characteristics – type of treatment, carbohydrate counting, prescribed doses of insulin, administration frequency of NPH insulin and insulin glargine, insulin type and prescribed doses of rapid-acting insulin and/or ultrafast and (iv) laboratory results of HbA1c.
Laboratory results of HbA1c were used for clinical effectiveness analysis, by comparison of the HbA1c values of each person after 6 months of insulin glargine use, with the reference values recommended in the literature for their age. For individuals between 6 and 18 years, HbA1c ≤7.5%; between 19 and 59 years, HbA1c ≤7.0% and over 60 years, HbA1c ≤8.0% [18] were considered controlled and the individuals who were outside this reference range values were considered uncontrolled.
This study did not assess glucose fasting values, since this measure has low validation to assess the efficacy and effectiveness of medicines for diabetes because of being susceptible to divergences with actual glycemic control [19].
Statistical analysis
Categorical variables were analyzed using absolute and relative frequencies and continuous variables as a mean, median and standard deviation (SD). The difference between the mean doses of NPH insulin and insulin glargine were compared using the t-test for paired samples. To identify factors associated with glycemic control of individuals after 6 months using insulin glargine, χ2 test of Pearson was conducted for categorical variables and an analysis of variance, one-way analysis of variance, for continuous variables. In case of a statistically significant difference, Tukey’s test was used for multiple comparisons. Variables were considered significant with p < 0.05 in the multiple model. Statistical analysis was performed using the software SPSS® version 20 (SPSS Inc., IL, USA).
Results
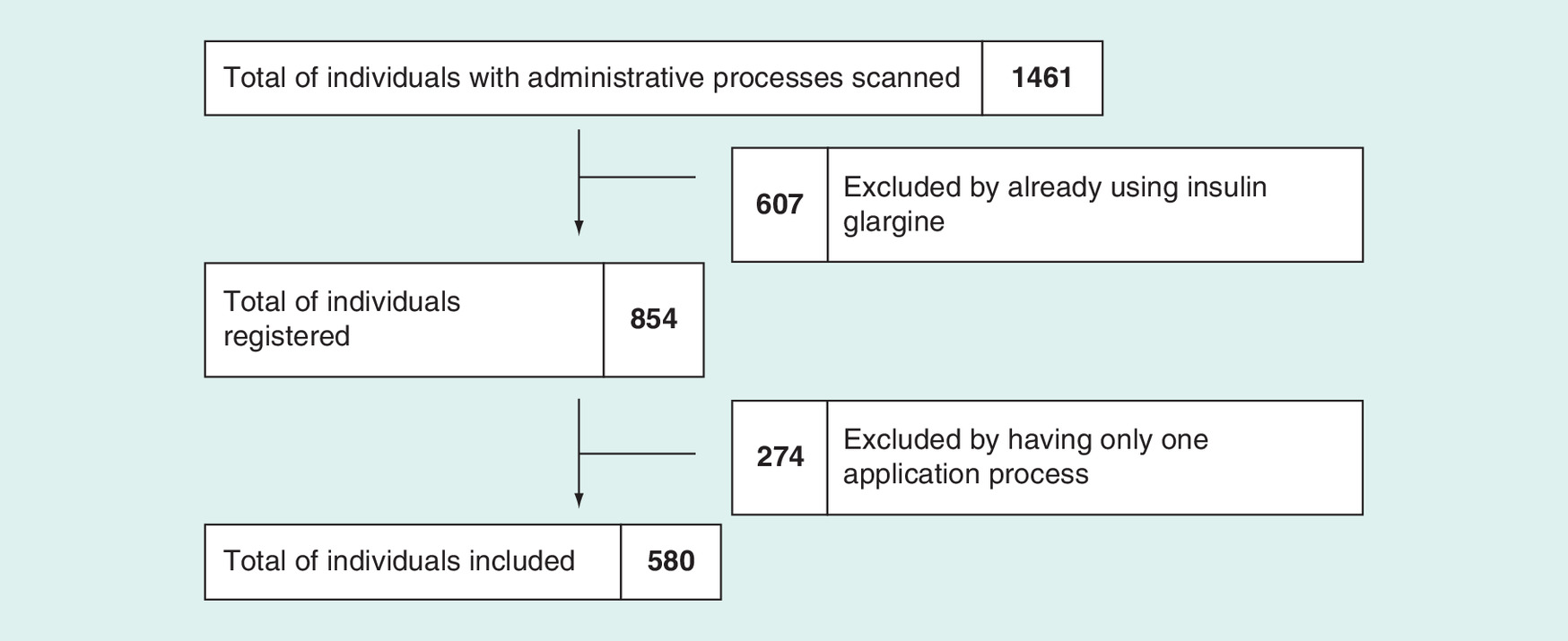
Individuals’ demographic and clinical characteristics; all administrative processes scanned by CCATES were evaluated. In all, 1461 individuals received long acting insulins from January 2011 to January 2015. A total of 854 patients were subsequently registered for the study, according to the eligibility criteria. After analyzing administrative procedures, 580 patients were finally included in the study sample (Figure 1).
The sex distribution was similar between the groups; the predominant ethnicity was white (33.8%) and most individuals were between 20 and 59 years old (63.1%). 79% of patients did not report the presence of comorbidities associated with Type I diabetes (Supplementary Table 2).
The average age of participants was 33 years (SD = 17.3), with the average age at diagnosis of Type I diabetes being 17.5 years (SD = 13.2). At the end of the study, the average time of treatment of patients was 14.8 years (Supplementary Table 3).
Treatment characteristics
When patients were administering NPH insulin, 41% were using conventional treatment – in which they receive insulin injections twice a day, nutritional assessment and quarterly clinic visits. After 6 months of using insulin glargine, this number decreased to 25.9%. Either when using NPH insulin or insulin glargine, most patients followed intensive treatment in which they received multiple administrations of insulin each day along with extensive educational and medical support.
Carbohydrate counting, reported initially among 21% of the patients, increased to 24.8% by the end of the study period. When using NPH insulin, 40% of the patients used soluble insulin and 13.8% ultra-fast analogs. After 6 months of using insulin glargine, the percentage of individuals using soluble insulin was 31% and ultrafast-acting insulin analogs 24.8% (Supplementary Table 4).
49% of patients when using of NPH insulin were injecting three-times a day. When using insulin glargine, the frequency of administration once a day was 92.6% (Supplementary Table 4).
The average daily dose of basal insulin ranged from 35.23 ± 15 IU when using NPH insulin to 34.38 ± 15 IU after 6 months of using insulin glargine (p = 0.018). The average daily dose of fast-acting and ultra-fast insulin ranged from 14.44 ± 11 IU when using NPH insulin to 14.69 ± 11 IU (p = 0.130) after 6 months of using insulin glargine (Table 1).
| Variable | Average | SD | Median | Minimum | Maximum | p-value |
|---|---|---|---|---|---|---|
| Daily dose of basal insulin (IU) | ||||||
| NPH insulin dosage | 35.23 | 15.524 | 34.00 | 5 | 122 | 0.018† |
| Insulin glargine dosage | 34.38 | 15.219 | 32.00 | 6 | 120 | – |
| Difference in the daily dose of basal insulin | -0.8460 | 8.5725 | 0.00 | -70.00 | 32.00 | – |
| Prescribed dose of rapid-acting/ultrafast insulin (IU) | ||||||
| In NPH insulin users | 14.44 | 11.079 | 12.00 | 6 | 90 | 0.130 |
| In insulin glargine users | 14.69 | 10.934 | 12.00 | 4 | 90 | – |
†Statistically significant variation by paired t-test.
NPH: Neutral protamine hagedorn; SD: Standard deviation.
The doses of insulin glargine in 6 months of use were evaluated as a function of age. There was a statistically significant difference between the mean doses among the various age groups. The post hoc analysis showed a statistically significant difference in the mean dose in individuals from 6 to 12 years compared with other age groups (Supplementary Table 5).
Glycemic control
Comparison of glycated hemoglobin levels before and after 6 months of using insulin glargine demonstrated a statistically significant reduction ranging from 8.80 ± 1.98% when using NPH insulin to 8.54 ± 1.88% (p = 0.001). The mean difference of glycated hemoglobin before and after 6 months of treatment with insulin glargine was 0.23% (Table 2).
| Variable | Average | SD | Median | Minimum | Maximum | p-value |
|---|---|---|---|---|---|---|
| HbA1c value (%) | ||||||
| In NPH insulin users | 8.80 | 1.98 | 8.52 | 4.56 | 16.00 | 0.001† |
| In insulin glargine users | 8.54 | 1.88 | 8.30 | 4.42 | 17.10 | – |
| Difference in HbA1c | -0.23 | 1.937 | 0.00 | -8 | 9 | – |
†Value with a statistically significant difference between groups. Analysis by t-test paired.
HbA1c: Glycated hemoglobin; NPH: Neutral protamine hagedorn; SD: Standard deviation.
Individuals’ glycemic control ranged from 22.6% when using NPH insulin and 26.2% when using insulin glargine – Table 3 (In Supplementary Figure 1, there is documentation of the percentage of people achieving glycemic control after 6 months of using insulin glargine for different age groups during the study).
| Insulin type | Glycemic control | |||
|---|---|---|---|---|
| Uncontrolled | Controlled | |||
| n | % | n | % | |
| In neutral protamine hagedorn insulin users | 449 | 77.4 | 131 | 22.6 |
| In insulin glargine users | 428 | 73.8 | 152 | 26.2 |
There were no statistically significant differences between the controlled and uncontrolled groups for variables including age, history of comorbidities, sex, ethnicity, type of insulin used, type of treatment, carbohydrate counting and frequency of use when using NPH insulin and after 6 months of using insulin glargine (Table 4).
| Variable | Uncontrolled | Controlled | p-value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Comorbidities: | |||||
| – Yes | 94 | 77.0 | 28 | 23.0 | 0.357 |
| – No | 334 | 72.9 | 124 | 27.1 | |
| Sex: | |||||
| – Male | 211 | 72.8 | 79 | 27.2 | 0.571 |
| – Female | 217 | 74.8 | 73 | 25.2 | |
| Ethnicity: | |||||
| – White | 151 | 77 | 45 | 23 | 0.758 |
| – Black | 11 | 73.3 | 4 | 26.7 | |
| – Brown | 48 | 72.7 | 18 | 27.3 | |
| Type of treatment: | |||||
| – Conventional | 110 | 73.3 | 40 | 26.7 | 0.425 |
| – Intensive | 200 | 69.7 | 87 | 30.3 | |
| Carbohydrate counting: | |||||
| – Yes | 99 | 68.8 | 45 | 31.3 | 0.248 |
| – No | 132 | 74.6 | 45 | 25.4 | |
| Age: | |||||
| – 6–12 | 44 | 67.7 | 21 | 32.3 | 0.177 |
| – 13–19 | 71 | 74.0 | 25 | 26.0 | |
| – 20–59 | 279 | 76.2 | 87 | 23.8 | |
| – ≥60 | 34 | 64.2 | 19 | 35.8 | |
| Type of Insulin: | |||||
| – Soluble insulin | 130 | 72.2 | 50 | 27.8 | 0.385 |
| – Short-acting analog | 107 | 74.3 | 37 | 25.7 | |
| Frequency of use: | |||||
| – Once a day | 394 | 73.4 | 143 | 26.6 | 0.414 |
| – Twice a day | 34 | 79.1 | 9 | 20.9 | |
| – Three-times a day | 0 | 0 | 0 | 0 | |
Factors associated with glycemic control were analyzed after 6 months of using insulin glargine through differences between means for continuous variables including: age, age at diagnosis, time since diagnosis, basal-acting insulin dose and fast-acting and ultrafast-acting insulin dose. No statistically significant difference was observed between controlled and uncontrolled groups for all variables (Table 5).
| Variable | Uncontrolled | Controlled | p-value† | |
|---|---|---|---|---|
| Age (years) | Average | 33.04 | 33.07 | 0.326 |
| SD | 17.14 | 18.01 | ||
| Age at diagnosis (years) | Average | 17.19 | 18.38 | 0.6154 |
| SD | 13.14 | 13.31 | ||
| Time since diagnosis (years) | Average | 15.09 | 13.97 | 0.386 |
| SD | 12.31 | 14.01 | ||
| Basal-acting insulin dose (IU) | Average | 35.64 | 31.07 | 0.888 |
| SD | 15.32 | 14.50 | ||
| Fast/ultrafast-acting insulin dose (IU) | Average | 15.35 | 12.51 | 0.256 |
| SD | 12.47 | 7.38 | ||
| Total | n | 428 | 152 |
†p-value between neutral protamine hagedorn insulin and insulin glargine controlled.
At the beginning of the cohort, when 580 patients were using NPH insulin, 449 of them did not show good control of the disease and 131 had good blood glycemic control. After 6 months of using insulin glargine, only 78 of these patients achieved glycemic control while the others (371 patients) continued without control (Figure 2). Of the individual patients who had early glycemic control (131 individuals), 74 patients kept it while the others lost it.
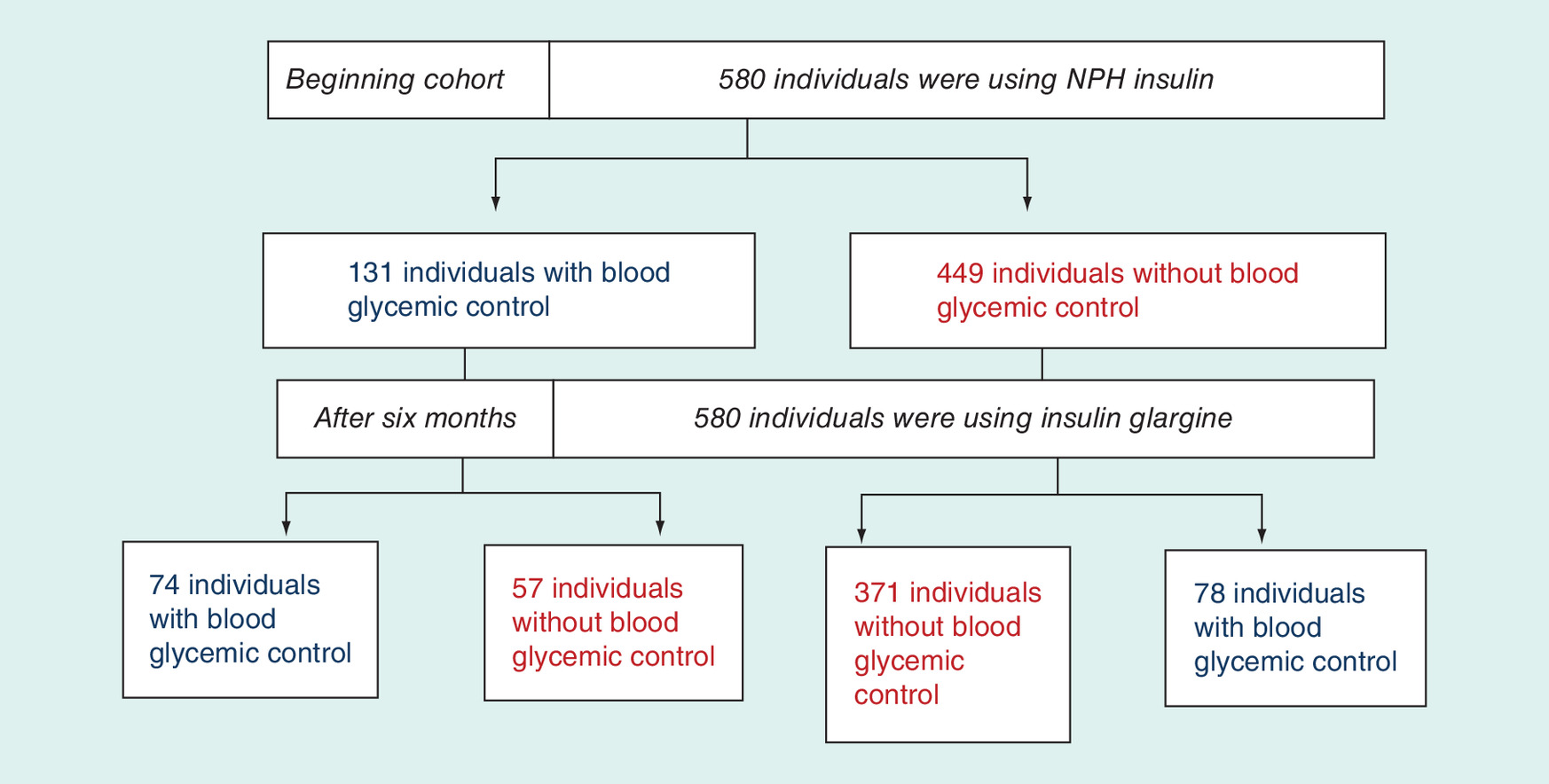
Figure 2. Flowchart of patients and glycaemic control.
NPH: Neutral protamine hagedorn.
Discussion
The analysis of the effectiveness and safety of insulin glargine use in patients with Type I diabetes is an important tool for decision makers, especially where there are considerable differences in acquisition costs and resources are limited.
In this cohort of 580 patients, insulin glargine reduced by an average of 0.23% patients’ HbA1c levels (Table 2), which is less than considered clinically significant (0.7–1%) [20]. The same was observed in the study by Singh et al. (2009) in which the differences between insulin glargine and NPH insulin in terms of HbA1c were considered only marginal among adults with Type I diabetes (weighted mean difference for insulin glargine: -0.11%; 95% CI (-0.21; -0.02%) [21].
According to the American Diabetes Association (ADA; 2015) and Mendes et al. (2010), children aged between 6 and 12 years reach glycemic control more easily when compared with the other age groups [18,22]. Even taking into account this influence of age in controlling the disease, this study did not find significant differences between the groups with and without glycemic control, in individuals who were using insulin glargine (Tables 4 & 5).
When assessing the basal insulin dose, we perceived a slight decrease (2.4%), but significant (p = 0.018) after 6 months of using insulin glargine (Table 1). This has important clinical consequences since this value differs from the insulin glargine manufacturer’s guidelines (Lantus®), which states that the average starting dose of insulin glargine is 80% of the NPH insulin dose. This though is in line with Garg et al. (2014) who showed similar results – for example, the average dose of insulin glargine showed a significant decrease (p = 0.03) when compared with the group that used NPH insulin [23]. There is a relationship between insufficient guidance for self-care and unsatisfactory adherence to treatment with 95% of hypoglycemic crisis occurrences. Individuals with Type I diabetes who follow intensive treatment also have a 3-kg weight gain versus individuals submitted to conventional therapy [16].
In a cost–effectiveness study, the results obtained suggest that treatment with insulin analogs is associated with a reduction of complications related to diabetes (in other words, more years of quality-adjusted life) compared with conventional insulins. However, benefits conferred and associated to this reduction complications are not compensatory when we add in the high acquisition costs of insulin analogs versus NPH insulin particularly in Brazil [3,24].
Two other studies of effectiveness [5,25] corroborate the data found in this study that the clinical evidence does not support the superiority of insulin glargine compared with NPH insulin. Sanches et al. (2011) also found no statistically significant reduction of HbA1c when comparing insulin glargine and NPH insulin [25].
However Tricco et al. (2014) in their study, when evaluating the safety, effectiveness and cost–effectiveness among insulin analogs and NPH insulin in individuals with Type I diabetes, concluded that long-acting insulin analogs are probably superior to NPH insulin, although it is by a small difference in HbA1c levels [26]. This suggests that patients and their physicians should adapt their insulin choice according to preference, cost and accessibility.
Although an economic evaluation has not been the subject of this study, the fact that there are higher acquisition costs and lack of therapeutic superiority of insulin glargine over NPH insulin suggests a favorable cost–effectiveness profile with NPH insulin, mirroring the findings from our two published meta-analysis [3,4]. Consequently, we believe it is up to managers and decision makers to renegotiate therapy costs with insulin glargine since NPH insulin in this and other studies appears to offer the same patient benefits as insulin glargine but with substantially lower acquisition costs within public health systems certainly in Brazil. This is similar to the suggestions of Laranjeira et al. who worked on a discount of 37.5% when calculating the potential budget impact of insulin glargine used in restricted cases [27].
We acknowledge though that there are limitations with this study design. First, we confined our analysis to patients within Minas Gerais. However, this is one of the most populated regions in Brazil with similar age and sex characteristics to other regions in Brazil, representing well Brazil as a whole. Second, only patients with completed and approved report forms for insulin glargine where included, which limited some of the analysis. The variable reporting of comorbidities was also an optional field in the report. The fact that the individuals with Type I diabetes did not report the presence of comorbidities (79% of individuals) does not mean they do not have these. It wasn't possible to also evaluate the reduction of hypoglycemic episodes from the data entered onto the SUS database. In addition, the use of a retrospective data limits access to important data. The conditions of observational studies are also not under the control of the investigator, and the researcher does not intervene in the allocation of participants. This is a characteristic of this type of design. We tried, however, to minimize possible biases by confirming the results through laboratory tests and reviews of medical reports where we could. Despite these limitations, we believe our findings are robust giving direction to Ministry of Health personnel in Minas Gerais and Brazil to potentially renegotiate prices for insulin glargine. Prices of insulin glargine may start falling anyway now that biosimilars have been approved in the USA and Europe [28,29].
It is noteworthy that the evaluation of insulin glargine for the treatment of Type I diabetes demonstrated in this study that analog insulins were not superior to insulin NPH in terms of their effectiveness. These results impact on the likely scenario of the new analogs such as insulin degludec. Having said this, recent studies have indicated insulin degludec is a more cost effective option than insulin glargine [30,31]. However studies in patients in routine clinical care are needed that directly compare the effectiveness of these analogs, as well as their effectiveness versus NPH insulins, to conclude about their cost-effectiveness within universal healthcare systems such as Brazil. We await further evidence.
Conclusion
Insulin glargine showed no clinical advantage over NPH insulin in reducing HbA1c values and glycemic control in our cohort study, confirming the findings from our previous meta-analyses. While insulin glargine has an appreciably higher cost than NPH insulin, we believe it is mandatory for health authority personnel to review the pricing strategy of insulin glargine in Brazilian states that provide insulin free of charge to their citizens, and renegotiate prices where pertinent in order to ensure the sustainability of public health systems. The availability of biosimilar insulin glargine may facilitate this in Brazil.
This is an observational, longitudinal, analytical and prospective study that evaluates the comparative clinical effectiveness of two insulins for the treatment of Type I diabetes. This type of design is useful to generate evidence about the benefits and harms of the different interventions in routine clinical care (real world).
The cost of medicines, specifically insulin glargine, has grown considerably in Brazil in recent years, which raises the need for rationalization and optimization of financial resources in order to guarantee the sustainability of the health system as well as access to an effective and safe therapy to people with diabetes.
This review of clinical data did not show any additional clinical benefit in Type I diabetes patients using insulin glargine in relation to neutral protamine hagedorn (NPH) insulin, confirming the results from other previous studies and reviews.
There appeared to be no association between glycemic control and individual’s characteristics or treatment between patients receiving NPH insulin and then switched to insulin glargine.
Insulin glargine reduced by an average of 0.23% patients’ HbA1c, which is less than considered clinically significant (0.7–1%). The limited benefits conferred are not compensated by the high acquisition cost of insulin analogs versus NPH insulin in Brazil.
There are higher costs and lack of therapeutic superiority of insulin glargine over NPH insulin suggests a favorable cost–effectiveness for NPH insulin versus insulin glargine.
This review provides a basis for health system managers to maintain or exclude insulin glargine from the reimbursed list of medicines offered for the treatment of diabetes while there are still appreciable differences in acquisition costs between the two insulins.
It is up to managers and decision makers to renegotiate therapy costs, or even discuss the possibility of disinvestment, once proven that NPH insulin offers the same benefits as insulin glargine but with substantially lower costs within public health systems.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2016-0099
Financial & competing interests disclosure
The research was supported by the Research Group in Pharmacoepidemiology, Federal University Minas Gerais. This research is an integral part of the research project ‘Comparative Clinical Effectiveness and cost–effectiveness of Glargine insulin analog for the treatment of patients suffering from Diabetes Mellitus’ with financial support from the National Scientific and Technological Development Council (CNPq). The write-up was in part supported by a Newton Advanced Fellowship awarded to Professor Augusto Afonso Guerra Junior by the Academy of Medical Sciences, through the UK Government’s Newton Fund programme. All named authors take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published. Lays P Marra, Vânia E Araújo, Gerusa CC Oliveira, Leonardo M Diniz, Augusto A Guerra Júnior, Francisco de Assis Acurcio, Brian Godman and Juliana Álvares declare they have no conflicts of interest. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (suppl_appendix.docx)
- Download
- 60.18 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
WHO: Global report on diabetes. http://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdf?ua=1
2.
Branchtein L, Matos MCG. Antidiabéticos. In: Farmacologia clínica: fundamentos da terapêutica racional (3rd Edition). Fuchs FD, Wannmacher L, Ferreira MBC (Eds.). Guanabara Koogan, Rio de Janeiro, Brazil, 832–844 (2006).
3.
Caires de Souza AL, de Assis Acurcio F, Guerra Júnior AA, Rezende Macedo do Nascimento RC, Godman B, Diniz LM. Insulin glargine in a Brazilian state: should the government disinvest? An assessment based on a systematic review. Appl. Heal. Econ. Heal. Pol. 12(1), 19–32 (2014).
•• Good meta-analysis of the effectiveness and safety of neutral protamine hagedorn (NPH) insulin versus insulin glargine based on randomized clinical trials.
4.
Marra LP, Araújo VE, Silva TBC et al. Clinical effectiveness and safety of analog glargine in Type I diabetes: a systematic review and meta-analysis. Diabetes Ther. 7(2), 241–258 (2016).
•• Good study assess the effectiveness and safety of NPH insulin versus NPH insulin in cohort patients.
5.
Olivera GC, Melo LM, Guerra Júnior AA, Alvares J. Efetividade clínica comparativa do análogo de insulina glargina para tratamento de pacientes acometidos por diabetes mellitus Tipo I. Value Health 18(7), A862–A863 (2015).
6.
German Institute for Quality and Efficency in Healthcare (IQWiG). Long-acting insulin analogues in the treatment of diabetes mellitus Type I: executive summary commission no. A05-01 (2010). www.iqwig.de/en/projects_results/projects/drug_assessment/a05_01_long_acting_insulin_analogues_in_the_treatment_of_diabetes_mellitus_type_1.1197.html
7.
WHO. Review of the evidence comparing insulin (human or animal) with analogue insulins. 18th expert committee on the selection and use of Essential medicines. 1–51 (2011). www.who.int/selection_medicines/committees/expert/18/applications/Insulin_review.pdf
8.
Vardi M, Jacobson E, Nini A, Bitterman H. Intermediate acting versus long acting insulin for Type I diabetes mellitus. Cochrane Database Syst. Rev. (3), CD0062979 (2008).
9.
Horvath K, Jeitler K, Berghold A et al. Long-acting insulin analogues versus NPH insulin (human isophane insulin) for Type II diabetes mellitus. Cochrane Database Syst. Rev. (2), CD005613 (2007).
10.
Holden SE, Poole CD, Morgan CL, Currie CJ. Evaluation of the incremental cost to the National Health Service of prescribing analogue insulin. BMJ Open 1(2), e000258 (2011).
11.
NICE. Guidance on the use of long-acting insulin analogues for the treatment of diabetes–insulin glargine (2002). www.nice.org.uk/guidance/ta53/documents/final-appraisal-determination-longacting-insulin-analogues-for-the-treatment-of-diabetes-insulin-glargine-2
12.
Raskin P, Klaff L, Bergenstal R, Hallé JP, Donley D, Mecca T. A 16-week comparison of the novel insulin analog insulin glargine (HOE 901) and NPH human insulin used with insulin lispro in patients with Type I diabetes. Diabetes Care 23(11), 1666–1671 (2000).
13.
Herwig J, Scholl-Schilling G, Bohles H. Glycaemic control and hypoglycaemia in children, adolescents and young adults with unstable Type I diabetes mellitus treated with insulin glargine or intermediate-acting insulin. J. Pediatr. Endocrinol. Metab. 20(4), 517–525 (2007).
14.
Schreiber SA, Russmann A. Long-term efficacy of insulin glargine therapy with an educational programme in Type I diabetes patients in clinical practice. Curr. Med. Res. Opin. 23(12), 3131–3136 (2006).
15.
Salemyr J, Bang P, örtqvist E. Lower HbA1c after 1 year, in children with Type I diabetes treated with insulin glargine vs NPH insulin from diagnosis: a retrospective study. Pediatr. Diabetes 12(5), 501–505 (2011).
16.
MINAS GERAIS. Secretaria de Estado de Saúde de Minas Gerais. Resolução SES-MG No 2359 de 17 de junho de 2010 – Dispõe sobre o Protocolo Clínico e Diretrizes Terapêuticas para a utilização de análogo Glargina em portadores de diabetes mellitus Tipo I (DM1). Diário da Imprensa Oficial de Minas Gerais Poder Executivo, Belo Horizonte. 10(23), 1–27 (2010). http://ws.mpmg.mp.br/biblio/informa/180613576.htm
17.
Centro Colaborador do SUS para Avaliação de Tecnologias, Excelência em Saúde C. DIRETRIZES METODOLÓGICAS Detalhamento acadêmico. 1–47 (2015). www.ccates.org.br/content/_pdf/PUB_1437678333.pdf
18.
American Diabetes Association. Standards of medical care in diabetes – 2015. Diabetes Care 38(Suppl. 1), S01–S98 (2015).
19.
Lassere MN, Johnson KR, Boers M et al. Definitions and validation criteria for biomarkers and surrogate endpoints: development and testing of a quantitative hierarchical levels of evidence schema. J. Rheumatol. 34(3), 607–615 (2007).
20.
Canadian Agency for Drugs and Technologies in Health. Optimal therapy recommendations for the prescribing and use of insulin analogues. COMPUS 2(7), 87 (2009).
21.
Singh SR, Ahmad F, Lal A, Yu C, Bai Z, Bennett H. Efficacy and safety of insulin analogues for the management of diabetes mellitus: a meta-analysis. CMAJ 180(4), 385–397 (2009).
22.
Mendes AB V, Fittipaldi JAS, Neves RCS, Chacra AR, Moreira ED. Prevalence and correlates of inadequate glycaemic control: results from a nationwide survey in 6671 adults with diabetes in Brazil. Acta Diabetol. 47(2), 137–145 (2010).
23.
Garg SK, Paul JM, Karsten JI, Menditto L, Gottlieb PA. Reduced severe hypoglycemia with insulin glargine in intensively treated adults with Type I Diabetes. Diabetes Technol. Ther. 6(5), 589–595 (2004).
24.
Cameron CG, Bennett HA. Cost-effectiveness of insulin analogues for diabetes mellitus. Can. Med. Assoc. J. 180(4), 400–407 (2009).
• Good summary evaluating insulin analogs.
25.
Sanchesa ACC, Correrb CJ, Venson R, Pontarolo R. Revisiting the efficacy of long-acting insulin analogues on adults with Type I diabetes using mixed-treatment comparisons. Diabetes Res. Clin. Pract. 94(3), 333–339 (2011).
• Good summary re-evaluating insulin analogs.
26.
Tricco AC, Ashoor HM, Antony J et al. Safety, effectiveness, and cost effectiveness of long acting versus intermediate acting insulin for patients with Type I diabetes: systematic review and network meta-analysis. BMJ 349, 1–13 (2014).
• Good summary re-evaluating insulin analogs versus NPH insulin.
27.
Laranjeira FO, Silva EN, Pereira MG. Budget impact of long-acting insulin analogues: the case in Brazil. PLoS ONE 11(12), e0167039 (2016).
• Good paper evaluating the budget impact of long acting insulin analogs.
28.
NICE. Diabetes mellitus Type I and Type II: insulin glargine biosimilar (Abasaglar). NICE Guidance (2015) ESNM64. www.nice.org.uk/advice/esnm64/chapter/key-points-from-the-evidence
29.
US FDA. FDA approves Basaglar, the first ‘follow-on’ insulin glargine product to treat diabetes (2015). www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm477734.htm
30.
Yamamoto C, Miyoshi H, Fujiwara Y et al. Degludec is superior to glargine in terms of daily glycemic variability in people with Type I diabetes mellitus. Endocrine J. 63(1), 53–60 (2016).
31.
Evans M, Chubb B, Gundgaard J. Cost–effectiveness of Insulin degludec versus insulin glargine in adults with Type I and Type II diabetes mellitus. Diabetes Ther. 8(2), 275–291 (2017).
Information & Authors
Information
Published In
Copyright
© 2017 Future Medicine Ltd.
History
Published online: 29 September 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The clinical effectiveness of insulin glargine in patients with Type I diabetes in Brazil: findings and implications. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0099
Export citation
Select the citation format you wish to export for this article or chapter.