Analysis of the cost–effectiveness of carbetocin for the prevention of hemorrhage following cesarean delivery in Ecuador
Abstract
Aim: To compare the cost of carbetocin with that of oxytocin for the prevention and management of hemorrhage following cesarean delivery in Ecuador. Materials & methods: We developed a decision tree based cost–effectiveness model to compare carbetocin with oxytocin in the prevention of hemorrhage following cesarean delivery in Ecuador. Our model was run from a third party payer perspective and was validated by local experts in the field. The efficacy of the interventions was determined based on a systematic review of the literature. Direct costs were calculated based on current National Health Service price lists and retail price. Since the period covered by the analysis was 1 year, costs and health effects were not discounted. Results: The difference in costs between the interventions was US$16.26, with a difference in effectiveness of 0.0067 disability adjusted life years averted. The incremental cost–effectiveness ratio for carbetocin compared with oxytocin for prevention of hemorrhage following cesarean delivery was US$2432.89 per disability adjusted life year averted. Conclusion: Carbetocin is as efficacious and safe as oxytocin for primary prevention of hemorrhage in cesarean delivery in Ecuador. It is highly cost effective for reducing the need for additional uterotonic drugs in both emergency and elective cesarean delivery.
First draft submitted: 11 January 2017; Accepted for publication: 25 April 2017; Published online: 8 September 2017
Postpartum hemorrhage (PPH) is the main cause of maternal death throughout the world [1]. In Ecuador, it is the second most common cause of maternal death after pregnancy-related hypertensive disorders [2]. The most frequent cause of PPH is the inability of the uterus to contract appropriately owing to uterine hypotony or atony. Uterotonic drugs play a key role in the prevention of this condition [3]. Cesarean delivery, whether elective or emergency, is a known risk factor for PPH (odds ratio: 3.4 [95% CI: 3.28–3.95] for emergency cesarean and 2.0 [95% CI: 2.18–2.80] for elective cesarean) [4,5]. The frequency of cesarean delivery has increased significantly in Ecuador during the past years; on an average 39.2% of all hospital births were by cesarean delivery between 2010 and 2015 (Table 1). Surprisingly the rates of cesarean hysterectomy seem to be extremely high (0.4–3.1 per 100 deliveries) when compared with high-income countries, but this is probably due to the coding errors in the Ecuadorian databases [6].
| Diagnosis (ICD-10) | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 |
|---|---|---|---|---|---|---|
| Elective cesarean delivery (O820) | 11,061 | 11,820 | 10,026 | 11,665 | 10,236 | 13,648 |
| Emergency cesarean delivery (O821) | 1817 | 952 | 1176 | 2472 | 3652 | 4894 |
| Cesarean hysterectomy (O822) | 10,020 | 8861 | 8142 | 1118 | 4243 | 4410 |
| Other cesarean delivery (single; O828) | 58 | 247 | 456 | 302 | 128 | 200 |
| Cesarean delivery, no other specification (O829) | 45,569 | 48,612 | 47,880 | 53,352 | 52,523 | 41,862 |
| Multiple births, all by cesarean (O842) | 326 | 293 | 436 | 415 | 500 | 554 |
| Total cesarean deliveries | 68,851 | 70,785 | 68,116 | 69,324 | 71,282 | 65,568 |
| Total deliveries in hospital facilities (080–84) | 188,400 | 191,622 | 179,743 | 170,237 | 167,810 | 161,284 |
| All registered live births (O80–O84) | 326,028 | 332,642 | 319,227 | 292,659 | 284,203 | 273,280 |
Data taken from Instituto Nacional de Estadísticas y Censos – INEC, Egresos hospitalarios 2010–2015 [7].
The options available in Ecuador for pharmacologic management and prevention of PPH include oxytocin, misoprostol, methylergonovine and carbetocin [2]. However, only the first three are on the National Essential Medication List – the definitive list of obligatory medication in the National Health Service – and are financed by the state [8].
Carbetocin is a long-acting synthetic octapeptide analog of oxytocin with agonist properties. Its clinical and pharmacologic properties are similar to those of natural oxytocin. Compared with oxytocin, carbetocin induces a uterine response that is prolonged in terms of both amplitude and frequency of contractions when administered postpartum [9].
The efficacy of carbetocin has been evaluated by several authors. The studies by Dansereau et al. [10], Boucher et al. [11], Borruto et al. [12], Attilakos et al. [13], Reyes and Gonzalez [14], Elgafor El Sharkwy [15] and Fahmy et al. [16] and the meta-analyses of Su et al. [17] and Jin et al. [18] show that the efficacy of carbetocin is comparable to that of oxytocin for the prevention of PPH.
The administration of carbetocin in women who undergo cesarean delivery significantly reduces the need for additional uterotonic agents (RR: 0.64 [95% CI: 0.51–0.81]) and uterine massage (RR: 0.54 [95% CI: 0.31–0.96]) when compared with oxytocin [17]. Carbetocin is also associated with reduced blood loss compared with syntometrine (oxytocin + ergometrine) for prevention of PPH in vaginal delivery and is associated with significantly fewer adverse effects [17]. The systematic review and meta-analysis of Su et al. [17] did not reveal a significant increase in the frequency of adverse events after comparing carbetocin with oxytocin. Similarly, after comparing carbetocin with oxytocin in patients with severe pre-eclampsia, Reyes and Gonzalez [14] did not find significant differences in the frequency of adverse events. Elgafor el Sharkwy [15] recorded significantly less frequent fever and chills in patients who received carbetocin than in patients who received misoprostol and oxytocin. The Society of Obstetricians and Gynecologists of Canada recommends intravenous administration of carbetocin over continuous infusion of oxytocin for prevention of PPH in elective cesarean delivery, since it reduces the need for uterotonic agents [3]. The society also recommends intramuscular carbetocin over continuous infusion of oxytocin during vaginal delivery in women at risk of PPH because it reduces the need for uterine massage to prevent PPH. A large Phase III multinational randomized controlled trial sponsored by the WHO is ongoing to evaluate the noninferiority of room temperature stable carbetocin compared with oxytocin in the prevention of PPH after vaginal birth [19].
Given the increasingly frequent use of carbetocin as the drug of choice for prevention of hemorrhage after cesarean delivery in Ecuador, we compared its cost–effectiveness with that of oxytocin from the perspective of a public third party payer.
Methods
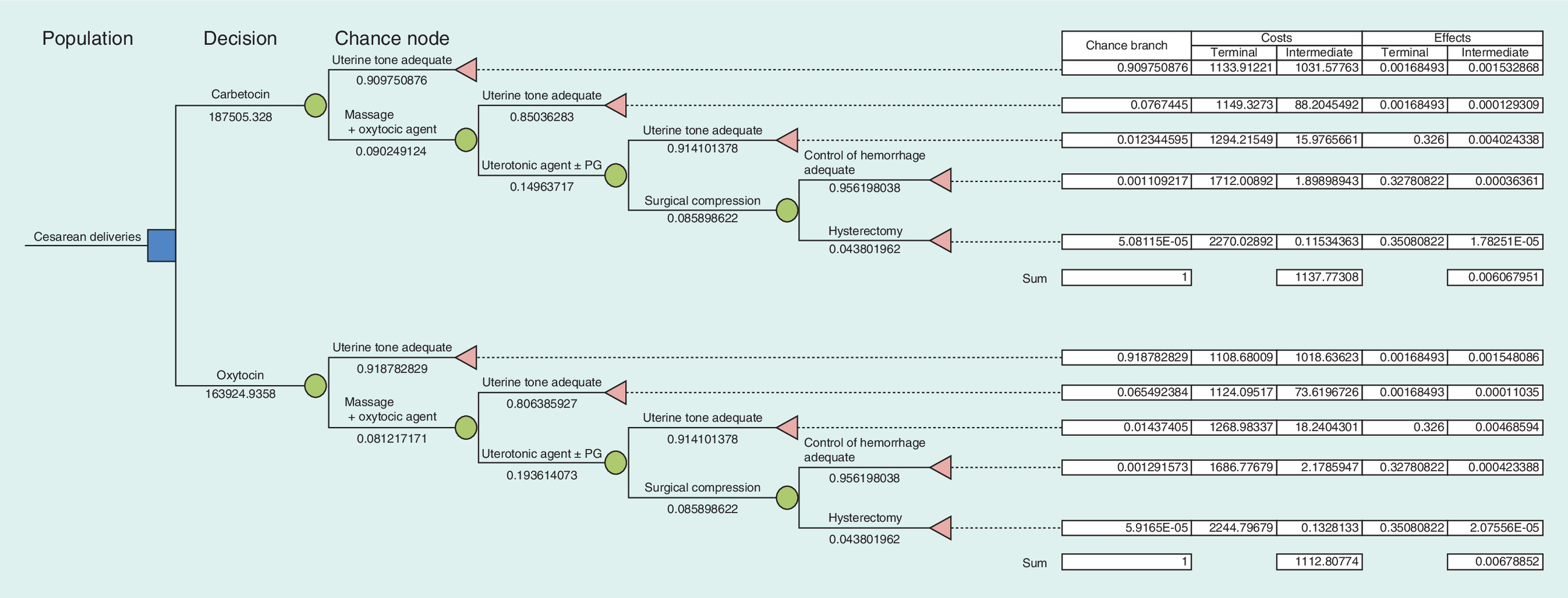
We performed a decision tree based cost–effectiveness study to compare the use of carbetocin with that of oxytocin for prevention of hemorrhage after cesarean delivery, the probability of using uterine massage and additional uterotonic agents, and the habitual sequence of interventions for control of bleeding resulting from uterine atony (Figure 1). The face validity of the model and the sequence of interventions were confirmed based on interviews with specialists in gynecology and obstetrics from the public and private sectors. The model was constructed using an MS Excel® spreadsheet, which was programmed with macros to run a probabilistic sensitivity analysis with 1000 iterations.
As it is an acute event, the time period for the analysis was 1 year; therefore, costs and health effects were not discounted. The efficacy of interventions to control uterine tone and the weight of the disability associated with cesarean delivery (elective and emergency) complicated by PPH were determined based on the review of the literature (Table 2).
| Variable | Deterministic | Probabilistic | Study | Ref. | ||
|---|---|---|---|---|---|---|
| Base | Range | Distribution | Parameters | First author (year) | ||
| Probability of uterine massage with carbetocin | 0.0786 | 0.0553–0.1106 | β | α = 29, β = 340 | Su et al. (2012) | [17] |
| Probability of uterine massage with oxytocin | 0.1459 | 0.1136–0.1856 | β | α = 54, β = 316 | Su et al. (2012) | [17] |
| Probability of additional uterotonic agents with carbetocin | 0.1365 | 0.1111–0.1667 | β | α = 80, β = 506 | Su et al. (2012) | [17] |
| Probability of additional uterotonic drugs with oxytocin | 0.2147 | 0.1833–0.2497 | β | α = 126, β = 461 | Su et al. (2012) | [17] |
| Probability of additional uterotonic drugs with ergotamine | 0.0874 | 0.0704–0.108 | β | α = 76, β = 794 | Butwick et al. (2015) | [20] |
| Probability of additional uterotonic drugs with misoprostol | 0.1064 | 0.0775–0.1444 | β | α = 35, β = 294 | Conde-Agudelo et al. (2013) | [21] |
| Probability of controlling hemorrhage with uterine compression sutures | 0.958 | 0.798–0.993 | β | α = 103, β = 6 | Matsubara et al. (2013) | [22] |
| Weight of disability arising from elective cesarean | -0.123 | -0.123 to -0.123 | – | – | Chatterjee et al. (2015) | [23] |
| Weight of disability arising from emergency cesarean | -0.326 | -0.123 to -0.123 | – | – | Chatterjee et al. (2015) | [23] |
| Weight of disability arising from hysterectomy | -0.349 | -0.349–0.349 | – | – | WHO (2004) | [24] |
| Weight of disability arising from anemia | -0.011 | -0.011 to -0.011 | – | – | WHO (2004) | [24] |
We used a public third party payer perspective, which included only direct costs (human resources, medications, consumables, medical procedures and hospital stay) of the interventions evaluated and their complications (Table 3). The direct costs were determined based on the price list of the National Health System and on retail prices in Ecuador [25]. All prices were in US dollars, which is the official currency in Ecuador. The cost–effectiveness of the interventions was measured as the cost in monetary units of averting one disability adjusted life year (DALY). Cost–effectiveness ratios were calculated, as was the incremental cost–effectiveness ratio, which was defined as the quotient of the difference in costs divided by the difference in effects [26]. The probabilistic sensitivity analysis was performed using Monte Carlo simulations with 1000 iterations [27]. Following the rules of the WHO's Commission on Macroeconomics in Health, the intervention under evaluation was considered cost effective if the cost of averting one DALY is equal or below the monetary value of 3 gross domestic products per capita (GDP per capita); and highly cost effective if the cost of averting one DALY was equal or below 1 GDP per capita [28].
| Parameter | Deterministic (US$) | Probabilistic (US$) | Source | |||
|---|---|---|---|---|---|---|
| Base | Range | Distribution | Mean | SD | ||
| Cost of one ampoule of carbetocin (100 μg/ml) | 25.60 | 21.39–30.19 | γ | 25.79 | 4.40 | MSP 2015 |
| Cost of one ampoule of oxytocin (10 IU/ml) | 0.15 | 0.13–0.19 | γ | 0.16 | 0.03 | MSP 2015 |
| Cost of one ampoule of ergotamine (0.2 mg/ml) | 0.65 | 0.55–0.78 | γ | 0.67 | 0.12 | MSP 2015 |
| Cost of one misoprostol tablet (200 μg) | 0.52 | 0.44–0.63 | γ | 0.54 | 0.10 | MSP 2015 |
| Cost per hour of use of an infusion pump | 0.03 | 0.03–0.04 | γ | 0.03 | 0.00 | Mean retail price |
| Cost of material for compressive suture (B-Lynch) | 6.37 | 6.37–6.58 | γ | 6.48 | 0.11 | Mean retail price |
| Cost of 1000 ml Ringer lactate or saline solution | 1.93 | 1.49–2.37 | γ | 1.93 | 0.44 | Mean retail price |
| Cost of 500 ml de Ringer lactate or saline solution | 1.29 | 1.10–1.47 | γ | 1.29 | 0.18 | Mean retail price |
| Cost of venoclysis set with vasocan | 4.10 | 3.42–4.78 | γ | 4.10 | 0.68 | Mean retail price |
| Cost of each 3- or 5-cc syringe | 0.20 | 0.17–0.23 | γ | 0.20 | 0.03 | Mean retail price |
| Cost of cesarean procedure | 892.64 | 892.64–892.64 | – | – | – | RPIS 2015 price list |
| Cost of hysterectomy | 1234.99 | 1234.99–1234.99 | – | – | – | RPIS 2015 price list |
| Cost per minute of physician/specialist (SP12) | 0.36 | 0.36–0.36 | – | – | – | SENRES 2010 |
| Cost per minute of nurse (SP8) | 0.23 | 0.23–0.23 | – | – | – | SENRES 2010 |
| Mean cost of daily hospital stay | 71.89 | 71.89–98.42 | – | – | – | RPIS 2015 price list |
MSP: Ministerio de Salud Pública (Ministry of Public Health); RPIS: Red Pública Integral de Salud (National Health Service); SD: Standard deviation; SP: Civil service salary scale.
Results
For the base case, the difference in costs between the interventions was US$16.26, with a difference in effectiveness of 0.0067 DALYs averted (this is the equivalent of gaining approximately 2.4 days of healthy life). The incremental cost–effectiveness ratio for carbetocin compared with oxytocin for prevention of hemorrhage following cesarean delivery was US$2432.89 per DALY averted. The probabilistic sensitivity analysis revealed the mean (standard deviation) difference in costs to be US$20.93 (0.29) and the difference in effectiveness to be 0.0066 DALYs averted, with a mean incremental cost–effectiveness ratio of US$3387.69 per DALY averted (95% CI: US$3307.18–3468.20).
The probabilistic sensitivity analysis (Figure 2) showed that carbetocin was highly cost effective in 97% of the iterations of the Monte Carlo simulations, with an incremental cost–effectiveness ratio below the threshold equal or below 1 GDP per capita (US$6302 for the year 2015), and in 100% of the simulations, the incremental cost–effectiveness ratio was below the threshold of 3 GDP per capita. Therefore, carbetocin proved to be highly cost effective in Ecuador.

Figure 2. Probabilistic sensitivity analysis.
Each dot shows the ICER estimated during Monte Carlo simulations with 1000 iterations.
DALY: Disability adjusted life year; GDP: Gross domestic product; ICER: Incremental cost–effectiveness ratio.
Discussion
The present study took into account all possible interventions for control of hemorrhage during cesarean delivery, thus increasing the amount of resources used. Nevertheless, carbetocin proved highly cost effective for primary prevention of hemorrhage during cesarean delivery. Similar studies performed in other countries [29–32] show that administration of carbetocin can reduce costs in the prevention of hemorrhage after cesarean delivery. From these, the prospective cost–effectiveness cohort study conducted by Luni et al. [30] is the largest on this topic, and shows in the context of the UK a significant reduction in PPH rates with financial savings.
As with any cost–effectiveness study, the results might not be generalizable to other settings. It is important to note that the present study is subject to limitations of available data in Ecuador. Cesarean rates reported in Ecuador are higher than in other countries, with low quality of coding and reporting of outcomes. Studies with misoprostol conducted in Ecuadorian population suggest the presence of genetic polymorphisms that increase adverse reactions like hyperpyrexia and shivering [33,34]. However, the parameters used can be considered as appropriate proxies for the model.
Finally, the large ongoing clinical trials sponsored by WHO can contribute to better estimates of the effectiveness of carbetocin on the prevention of PPH in vaginal deliveries [19]; however, women scheduled for a planned caesarean are not eligible limiting the generalizability of the findings. It is increasingly important that researchers conducting clinical trials with carbetocin include methods of economic evaluations alongside the trials.
Conclusion
Carbetocin is as efficacious and safe as oxytocin for primary prevention of hemorrhage after cesarean delivery in Ecuador. It is highly cost effective for reducing the need for additional uterotonic drugs in both emergency and elective cesarean delivery.
Postpartum hemorrhage is the main cause of maternal death throughout the world.
Cesarean delivery, whether elective or emergency, is a known risk factor for postpartum hemorrhage.
Carbetocin induces prolonged and frequent uterine contractions.
Carbetocin is associated with reduced blood loss.
Several authors have shown that carbetocin is as efficacious as oxytocin for prevention of postpartum hemorrhage.
Compared with oxytocin, administration of carbetocin in cesarean delivery significantly reduces the need for additional uterotonic agents and uterine massage.
Carbetocin is increasingly used as the drug of choice for the prevention of hemorrhage after cesarean delivery in Ecuador.
Based on official data, carbetocin proved to be highly cost effective for primary prevention of hemorrhage during cesarean delivery in Ecuador.
Acknowledgements
The authors thank W León and E Yépez for their feedback on the validity of the model and definition of the case-base scenarios.
Author contributions
A Henríquez-Trujillo conceived, developed and analyzed the economic evaluation model. R Lucio-Romero and K Bermúdez-Gallegos collected and analyzed epidemiological and cost information. A Henríquez-Trujillo, K Bermúdez-Gallegos and R Lucio-Romero drafted and revised the final version of the article.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Editorial assistance was provided by Content Ed Net (Madrid, Spain) with funding from Ferring.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
World Health Statistics 2014. World Health Organization, Geneva (2014). http://apps.who.int/iris/bitstream/10665/112738/1/9789240692671_eng.pdf.
2.
León W, Villamarín S, Velasco S, González-Andrade F, Henríquez R, Aguinaga G. Prevención, Diagnóstico Y Tratamiento De La Hemorragia Posparto. Guía de Práctica Clínica. Ministerio de Salud Pública, Quito, Ecuador (2013).
3.
Leduc D, Senikas V, Lalonde AB et al. Active management of the third stage of labour: prevention and treatment of postpartum hemorrhage. J. Obstet. Gynaecol. Can. 31(10), 980–993 (2009).
4.
Fescina R, De Mucio B, Ortiz E, Jarquin D. Guías Para La Atención De Las Principales Emergencias Obstétricas. CLAP/SMR, Montevideo, Uruguay (2012).
5.
Arulkumaran S, Mavrides E, Penney G. Royal College of Obstetricians and Gynaecologists. Postpartum haemorrhage: Prevention And Management. Green-top No. 52. Royal College of Obstetricians and Gynaecologists, London, UK (2009).
6.
de la Cruz CZ, Thompson EL, O'Rourke K, Nembhard WN. Cesarean section and the risk of emergency peripartum hysterectomy in high-income countries: a systematic review. Arch. Gynecol. Obstet. 292(6), 1201–1215 (2015).
7.
Instituto Nacional de Estadísticas y Censos – INEC. www.inec.gob.ec.
8.
Cuadro Nacional de Medicamentos Básicos y Registro Terapéutico (9th Review). Ministerio de Salud Pública, QuitoEcuador (2014). www.conasa.gob.ec/phocadownload/cnmb9na/Cuadro_Nacional_de_Medicamentos_Basicos_9na_Revision.pdf.
9.
Hunter DJ, Schulz P, Wassenaar W. Effect of carbetocin, a long-acting oxytocin analog on the postpartum uterus. Clin. Pharmacol. Ther. 52(1), 60–67 (1992).
10.
Dansereau J, Joshi AK, Helewa ME et al. Double-blind comparison of carbetocin versus oxytocin in prevention of uterine atony after cesarean section. Am. J. Obstet. Gynecol. 180(3 Pt 1), 670–676 (1999).
11.
Boucher M, Horbay GL, Griffin P et al. Double-blind, randomized comparison of the effect of carbetocin and oxytocin on intraoperative blood loss and uterine tone of patients undergoing cesarean section. J. Perinatol. 18(3), 202–207 (1998).
12.
Borruto F, Treisser A, Comparetto C. Utilization of carbetocin for prevention of postpartum hemorrhage after cesarean section: a randomized clinical trial. Arch. Gynecol. Obstet. 280(5), 707–712 (2009).
13.
Attilakos G, Psaroudakis D, Ash J et al. Carbetocin versus oxytocin for the prevention of postpartum haemorrhage following caesarean section: the results of a double-blind randomised trial. BJOG 117(8), 929–936 (2010).
14.
Reyes OA, Gonzalez GM. Carbetocin versus oxytocin for prevention of postpartum hemorrhage in patients with severe preeclampsia: a double-blind randomized controlled trial. J. Obstet. Gynaecol. Can. 33(11), 1099–1104 (2011).
15.
Elgafor El Sharkwy IA. Carbetocin versus sublingual misoprostol plus oxytocin infusion for prevention of postpartum hemorrhage at cesarean section in patients with risk factors: a randomized, open trail study. Arch. Gynecol. Obstet. 288(6), 1231–1236 (2013).
16.
Fahmy NG, Yousef HM, Zaki HV. Comparative study between effect of carbetocin and oxytocin on isoflurane-induced uterine hypotonia in twin pregnancy patients undergoing cesarean section. Egypt. J. Anaesth. 32(1), 117–121 (2016).
17.
Su LL, Chong YS, Samuel M. Carbetocin for preventing postpartum haemorrhage. Cochrane Database Syst. Rev. (2), CD005457 (2012).
•• Provides a meta-analysis of the comparative effectiveness of carbetocin in postpartum hemorrhage.
18.
Jin B, Du Y, Zhang F, Zhang K, Wang L, Cui L. Carbetocin for the prevention of postpartum hemorrhage: a systematic review and meta-analysis of randomized controlled trials. J. Matern. Fetal Neonatal Med. 29(3), 400–407 (2016).
• Provides an updated overview of carbetocin efficacy in postpartum hemorrhage.
19.
Widmer M, Piaggio G, Abdel-Aleem H et al. Room temperature stable carbetocin for the prevention of postpartum haemorrhage during the third stage of labour in women delivering vaginally: study protocol for a randomized controlled trial. Trials 17(1), 143 (2016).
•• The protocol of the biggest ongoing trial evaluating room-stable carbetocin.
20.
Butwick AJ, Carvalho B, Blumenfeld YJ, El-Sayed YY, Nelson LM, Bateman BT. Second-line uterotonics and the risk of hemorrhage-related morbidity. Am. J. Obstet. Gynecol. 212(5), 642.e1-7 (2015).
21.
Conde-AgudeloA, Nieto A, Rosas-Bermudez A, Romero R. Misoprostolto reduce intraoperative and postoperative hemorrhage during cesarean delivery:a systematic review and meta-analysis. Am. J. Obstet. Gynecol. 209(1), 40e1-40.e17 (2013).
22.
Matsubara S, Yano H, Ohkuchi A, Kuwata T, Usui R, Suzuki M. Uterine compression sutures for postpartum hemorrhage: an overview. Acta. Obstet. Gynecol. Scand. 92(4), 378–385 (2013).
23.
Chatterjee S, Gosselin RA. Estimating the effectiveness of a hospital's interventions in India: impact of the choice of disability weights. Bull. World Health Organ. 93(7), 476–482 (2015).
24.
WHO. Global burden of disease 2004 update: disability weights for diseases and conditions. www.who.int/healthinfo/global_burden_disease/GBD2004_DisabilityWeights.pdf.
25.
Tarifario De Prestaciones Para El Sistema Nacional de Salud. Ministerio de Salud Pública, Quito, Ecuador (2014).
26.
Meltzer MI. Introduction to health economics for physicians. Lancet 358(9286), 993–998 (2001).
27.
Briggs AH. Handling uncertainty in cost–effectiveness models. Pharmacoeconomics 17(5), 479–500 (2000).
28.
Bertram MY, Lauer JA, De Joncheere K et al. Cost–effectiveness thresholds: pros and cons. Bull. World Health Organ. 94(12), 925–930 (2016).
29.
Mills F, Siu E, Poinas AC, Chamy C. A cost-minimization analysis of carbetocin for the prevention of postpartum hemorrhage in Canada. Value Health 17(3), A161 (2014).
30.
Luni Y, Borakati A, Matah A, Skeats K, Eedarapalli P. A prospective cohort study evaluating the cost–effectiveness of carbetocin for prevention of postpartum haemorrhage in caesarean sections. J. Obstet. Gynaecol. 37(5), 1–7 (2017).
•• Provides real-world prospective cost–effectiveness information about the use of carbetocin in the context of a high-income country.
31.
van der Nelson HA, Draycott T, Siassakos D, Yau CW, Hatswell AJ. Carbetocin versus oxytocin for prevention of post-partum haemorrhage at caesarean section in the United Kingdom: an economic impact analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 210, 286–291 (2017).
32.
Sobkowski M, Celewicz Z, Kalinka J et al. Costs of the use of carbetocin in the prevention of uterine atony following delivery of the infant by Caesarean section – retrospective multicenter study. Ginekol. Pol. 87(9), 621–628 (2016).
33.
Durocher J, Bynum J, Leon W, Barrera G, Winikoff B. High fever following postpartum administration of sublingual misoprostol. BJOG 117(7), 845–852 (2010).
34.
Alfirevic A, Durocher J, Elati A et al. Misoprostol-induced fever and genetic polymorphisms in drug transporters SLCO1B1 and ABCC4 in women of Latin American and European ancestry. Pharmacogenomics 16(9), 919–928 (2015).
Information & Authors
Information
Published In
Copyright
© 2017 Future Medicine Ltd.
History
Published online: 8 September 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Analysis of the cost–effectiveness of carbetocin for the prevention of hemorrhage following cesarean delivery in Ecuador. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0004
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Joshua F. Ginnane, Samia Aziz, Saima Sultana, Connor Luke Allen, Annie McDougall, Katherine E. Eddy, Nick Scott, Joshua P. Vogel, The cost-effectiveness of preventing, diagnosing, and treating postpartum haemorrhage: A systematic review of economic evaluations, PLOS Medicine, 10.1371/journal.pmed.1004461, 21, 9, (e1004461), (2024).
- Kiara Bautista, Yi-Fang (Ashley) Lee, Colleen R. Higgins, Petra Procter, Sara Rushwan, Abraham Baidoo, Kofi Issah, Chris Opoku Fofie, A. Metin Gülmezoglu, Lester Chinery, Sachiko Ozawa, Modeling the economic burden of postpartum hemorrhage due to substandard uterotonics in Ghana, PLOS Global Public Health, 10.1371/journal.pgph.0003181, 4, 6, (e0003181), (2024).
- Ahmad N. Fasseeh, Nada Korra, Baher Elezbawy, Amal S. Sedrak, Mary Gamal, Randa Eldessouki, Mariam Eldebeiky, Mohsen George, Ahmed Seyam, Asmaa Abourawash, Ahmed Y. Khalifa, Mayada Shaheen, Sherif Abaza, Zoltán Kaló, Framework for developing cost-effectiveness analysis threshold: the case of Egypt, Journal of the Egyptian Public Health Association, 10.1186/s42506-024-00159-7, 99, 1, (2024).
- Suzette Matthijsse, Fredrik L. Andersson, Michael Gargano, Yum L. Yip Sonderegger, Cost-effectiveness analysis of carbetocin versus oxytocin for the prevention of postpartum hemorrhage following vaginal birth in the United Kingdom, Journal of Medical Economics, 10.1080/13696998.2022.2027669, 25, 1, (129-137), (2022).
- Jamaica Roanne Briones, Pattarawalai Talungchit, Montarat Thavorncharoensap, Usa Chaikledkaew, Economic evaluation of carbetocin as prophylaxis for postpartum hemorrhage in the Philippines, BMC Health Services Research, 10.1186/s12913-020-05834-x, 20, 1, (2020).
- Hua Liu, Xiu-Yun Xu, Ning Gu, Xiao-Dong Ye, Zhi-Qun Wang, Ya-Li Hu, Yi-Min Dai, Intravenous Administration of Carbetocin Versus Oxytocin for Preventing Postpartum Hemorrhage After Vaginal Delivery in High Risk Women: A Double-blind, Randomized Controlled Trial, Maternal-Fetal Medicine, 10.1097/FM9.0000000000000048, 2, 2, (72-79), (2020).
- Pan Sun, Hongzhi Xiao, Jianzhong Wang, Suxia Zhang, Xingyuan Cao, Pharmacokinetics and bioavailability of carbetocin after intravenous and intramuscular administration in cows and gilts, Journal of Veterinary Pharmacology and Therapeutics, 10.1111/jvp.12830, 43, 2, (237-240), (2019).