Appraisal of the cardiovascular risks of azithromycin: an observational analysis
Abstract
Aim: To assess the association of cardiovascular mortality in patients prescribed azithromycin compared with patients prescribed alternative antibiotics in an outpatient setting. Methods: This study was a retrospective observational analysis using the South Carolina Medicaid claims and pharmacy databases over the years from 2000 to 2011 housed at the Revenue and Fiscal Affairs Office. Study antibiotics included azithromycin, amoxicillin, clindamycin, clarithromycin and quinolones (levofloxacin, ciprofloxacin and moxifloxacin), and excluded patients at a high risk of death from causes other than the study antibiotics. This study used both matching and regression adjustment with propensity scores to reduce possible bias in the estimated treatment (group) effect from confounders. Results: The total number of prescriptions evaluated in the study include: 283,743 azithromycin; 143,191 amoxicillin; 52,714 clindamycin; 38,133 clarithromycin and 49,734 for the quinolones. After propensity score weighting, cardiac deaths per million within the first 5 days were: 84.6 for azithromycin, 78.3 for clarithromycin, 69.4 for amoxicillin, 61.6 for quinolones and 15.0 for clindamycin. Our multivariate models reveal that the study antibiotics’ (amoxicillin, clindamycin, clarithromycin, levofloxacin, ciprofloxacin and moxifloxacin) mortality rates are not statistically different from azithromycin in any time interval (days: 0–5, 6–10, 0–10 and 0–30). In comparison with previous studies, the results are consistent in Amoxicillin. In the first 5 and 10 days, it is associated with lower odds of cardiovascular death than azithromycin (5 days: odds ratio [OR]: 0.70 [95% CI: 0.25–1.99]; 10 days: OR: 0.92 [95% CI: 0.39–2.14]). However, we find no statistically significant difference between the two antibiotics. Conclusion: Our study shows that the odds of cardiovascular mortality between azithromycin and other antibiotics are not statistically significantly different and previous published findings may not be applicable to the general population. Additionally our results suggest that while we cannot rule out the increased risk of cardiovascular death from azithromycin in patients at low risk of death, the risk may not be as large initial studies suggest. Further research is needed to define the population at greatest risk.
First draft submitted: 4 November 2016; Accepted for publication: 21 April 2017; Published online: 29 September 2017
The azalide antibiotic azithromycin is widely used to treat respiratory track, skin and soft tissues, and sexually transmitted infections. Azithromycin has been touted as having minimal cardiovascular sequelae. This is in contrast to the macrolide antibiotics erythromycin and clarithromycin, which are associated with an increased risk of cardiac arrhythmias, torsade de pointes (TdP) and cardiovascular death [1]. While the QT interval prolongation from azithromycin is similar to that of erythromycin and clarithromycin, there is dissociation between the QT prolongation and cardiac arrhythmias [2]. Due to the dissociation of azithromycin and cardiac arrhythmias in animal models and clinical trials, azithromycin has been regarded as having minimal cardiovascular risk.
Recently, Ray et al. (2012) and Rao et al. (2014) conducted a retrospective observational analysis reporting that the risks of azithromycin may be more substantial than previously understood. The investigators reported a 2.02- and 1.48-fold higher risk of death, respectively, within 5 days of starting azithromycin compared with amoxicillin [3,4]. Subsequent published studies have yielded discordant results; three studies were not associated with an increased risk of death related to azithromycin utilization and one study was associated with an increased mortality with azithromycin [5–8]. A study from Denmark (2013) found that in comparison with penicillin V, azithromycin use was not associated with increased risks of death from cardiovascular causes in a general population of young, middle-aged adults [5]. Among older veteran patients hospitalized with pneumonia, treatment that included azithromycin compared with other antibiotics was associated with a lower risk of 90-day mortality; however, there was an increased risk of myocardial infarction (odds ratio [OR]: 1.17 [95% CI: 1.08–1.25]) [6]. Compared with amoxicillin–clavulanate treatment, the use of azithromycin in a Taiwan nationwide study was associated with significant increases in the risks of ventricular arrhythmia and cardiovascular death (adjusted ORs for ventricular arrhythmia 4.32 [95% CI: 2.95–6.33]; adjusted ORs for cardiovascular death 2.62 [95% CI: 1.69–4.06]) [7]. Finally, azithromycin use was not associated with higher risk of death from any cause in a meta-analysis (hazard ratio [HR]: 0.99 [CI: 0.82–1.19]) or cardiovascular cause (HR: 1.15 [CI: 0.66–2.00]) [8]. However, subgroup analyses have shown azithromycin (within 1–5 days of therapy) was associated with a higher risk of death among an older population (HR: 1.64 [CI: 1.23–2.19]). Prior to the Ray et al. study, the only documented association between azithromycin and cardiovascular death were case reports of QT prolongation and TdP following azithromycin administration [9–16]. Since the study by Ray et al., US FDA updated azithromycin package labeling to include risk of prolonged cardiac repolarization and QT prolongation, increasing the possibility of cardiac arrhythmias and TdP, especially in elderly patients [17].
Due to the widespread use of azithromycin and the potential consequences of the mortality risk reported by Ray et al. and Rao et al., we conducted a retrospective observational analysis to assess the association of mortality in patients prescribed azithromycin compared with patients prescribed alternative antibiotics. We hypothesized that when confounding variables were controlled, patients prescribed azithromycin would have higher adjusted odds of cardiovascular mortality.
Methods
Data overview
This study was conducted using the South Carolina Medicaid claims and pharmacy databases housed at the South Carolina Revenue and Fiscal Affairs Office. The study was conducted in compliance with the University of South Carolina Institutional Review Board requirements. The unit of analysis was antibiotic prescription course. Study antibiotics included azithromycin, amoxicillin, clindamycin, clarithromycin, levofloxacin, ciprofloxacin and moxifloxacin. Due to low sample sizes, the antibiotics levofloxacin, ciprofloxacin and moxifloxacin were aggregated to one group, designated ‘floxacin’. The study cohort consisted of antibiotic prescriptions for persons aged 17–74 years, over the time period from January 2000 to December 2011. Given that the unit of analysis was antibiotic course, one person could have multiple antibiotic courses with multiple antibiotics.
Cohort selection
Initially, all outpatient prescriptions for the study antibiotics in the South Carolina Medicaid databases were pulled using their 11-digit National Drug Code. Both the fee for service and managed care claims were included. To form the initial study cohort, four selection criteria were applied. First, if a person was prescribed more than one of the study antibiotics within 30 days of each other, those prescriptions were dropped. Second, to ensure adequate medical surveillance, persons without a prescription for any drug within 365 days prior to the study antibiotics were dropped. Third, study prescriptions that were preceded by an inpatient hospital stay within 30 days of being prescribed a study antibiotic were dropped. Fourth, those at high risk of death from causes other than study antibiotics (e.g., QTc prolongation) were excluded. These criteria were formulated to exclude persons at high risk for death from causes unrelated to a short-term effect of proarrhythmic medication. A list of exclusionary diagnoses appears in Supplementary Table 1.
Outcome variable
The primary outcome of this study is cardiovascular death. Cardiovascular death was flagged based on International Classification of Diseases (ICD) 10 codes from linked vital records data. Cardiovascular ICD10 codes are listed in Supplementary Table 4. In the computerized vital records data, there are up to 20 causes of death. If any of those codes were equal to one of the cardiovascular codes, the record was flagged as a cardiovascular death. The date of death and the prescription dispense date were subtracted to get the number of days until cardiovascular death. To create a dependent variable for the multivariate models, cardiovascular death was flagged (yes = 1, no = 0) based on four intervals including: 0–5 days, 6–10 days, 0–10 days and 0–30 days. All records that did not have an occurrence of cardiovascular death within the intervals were coded as 0.
Control variables
Standard variables including sex, age, race and year of prescription were included in the multivariate models. The age of the subject, in years, was calculated at each antibiotic dispense date. Race includes white, black and other. We account for comorbid diagnoses in the models by counting all comorbid diagnoses found at any time prior to the prescription course (Supplementary Table 5). All diagnoses were pulled from medical claims within the South Carolina Medicaid claims database. These claims included inpatient, outpatient hospital as well as nonhospital outpatient visits.
We also include a total number of confounding prescriptions each subject was prescribed in the previous year for each antibiotic prescription. All pharmacy claims for the study cohort were pulled from the South Carolina Medicaid pharmacy database. See Supplementary Table 6 for a list of all confounding medications.
Statistical analysis
Assignment to each antibiotic treatment group was not randomized. As a result, differences in cardiovascular mortality might have been due to the different characteristics of the treatment groups rather than the treatment itself. Therefore, this study used both matching and regression adjustment with propensity scores to reduce possible bias in the estimated treatment (group) effect from confounders [18–22]. To create overlap among the treatment groups, the data were matched based on treatment propensity scores (i.e., the conditional probability of being prescribed each of the study antibiotics). Treatment propensity scores were estimated using a multinomial logistic regression model. The probability of being in a treatment group was modeled as a function of confounding medications, diagnoses, hospital visits, demographic data (age, race and sex) and month of prescription. Percentile rankings were then created for each of the five propensity scores. The percentiles were used to match the data, increasing the number of available possible matches. Regression adjustment with inverse probability treatment weighting (IPTW) was additionally used to reduce bias. The weights were created in the following manner:
| Actual prescription | Treatment weight calculation |
| Floxacin, Clindamycin, Clarithromycin, Amoxicillin |  |
| Azithromycin |  |
To avoid undue influence from prescriptions with large weights, we normalized the weights by dividing by the mean of all the weights and then trimmed by setting all weights above the 99th percentile to the 99th percentile value [23]. Extreme weights are the result of treatments that are very contrary to conditional probability of their treatment assignment [24,25]. In other words, the actual treatment given had an extremely low propensity based on the model. Extreme values are a common problem in IPTW. However, our computed IPTWs did not indicate any problem in our study. The number of extreme values is small, and less than 1% of the prescriptions.
To evaluate the closeness of the groups, we calculated the standardized difference between each antibiotic and azithromycin. In essence, this is the mean difference as a percentage of the average standard deviation [26].
We took the maximum value of the standardized differences as the measure of closeness among the groups. The covariate balance was improved significantly after matching and using IPTW (Supplementary Tables 2 & 3). After matching and weighting the samples, we used a pooled logistic regression model to evaluate the odds of cardiovascular death between the antibiotic groups. We also used generalized estimating equations (GEE) to account for within subject correlation.
Results
Table 1 shows the prescription counts for the initial data pull after applying the exclusion criteria and postmatching. The majority of the study attrition took place after matching each of the groups to the azithromycin treatment group. Table 2 displays the postmatching characteristics of the antibiotic prescription for select variables. All variables, except for age, have a largest standardized difference less than 10%. Further among all 83 variables, the mean largest standardized difference is 4.21 (Supplementary Table 7) indicating that the matching resulted in relatively homogeneous characteristics among the antibiotic groups. Supplementary Tables 8 & 9 display the largest standardized difference for each variable. The total number of prescriptions evaluated in the study include: 283,743 azithromycin, 143,191 amoxicillin, 52,714 clindamycin, 38,133 clarithromycin and 49,734 for the floxacin group.
| Data | Amoxicillin | Azithromycin | Clindamycin | Clarithromycin | Floxacin |
|---|---|---|---|---|---|
| Initial counts | 292,769 | 331,519 | 76,517 | 48,451 | 90,663 |
| After exclusion criteria | 263,171 | 296,491 | 68,821 | 44,048 | 73,914 |
| After matching | 143,191 | 283,743 | 52,714 | 38,133 | 49,734 |
| Variable | Amoxicillin | Azithromycin | Clindamycin | Clarithromycin | Floxacin | Largest standardized difference (%) |
|---|---|---|---|---|---|---|
| Age | 37.29 | 34.88 | 33.16 | 35.09 | 33.66 | 15.98 |
| Female (%) | 84.85 | 83.19 | 83.35 | 81.12 | 84.3 | 3.64 |
| Race (%): | ||||||
| - White | 51.43 | 51.69 | 43.80 | 59.87 | 55.13 | 5.19 |
| - Black | 44.22 | 43.41 | 52.71 | 34.69 | 39.83 | |
| - Other | 4.35 | 4.89 | 3.49 | 5.44 | 5.04 | |
| Confounding medications (%) | ||||||
| Acei | 1.34 | 1.21 | 1.05 | 1.2 | 1.17 | 1.65 |
| β-blocker | 2.92 | 2.67 | 2.2 | 2.34 | 2.5 | 3.14 |
| Calcium blocker | 1.11 | 1.03 | 0.74 | 0.54 | 1.03 | 5.54 |
| Digoxin | 0.36 | 0.39 | 0.37 | 0.41 | 0.4 | 0.38 |
| Loop diuretic | 5.38 | 4.43 | 4.15 | 4.48 | 4.26 | 4.96 |
| Statin | 1.95 | 1.74 | 1.32 | 0.84 | 1.75 | 7.79 |
| Insulin | 1.93 | 1.71 | 1.58 | 1.67 | 1.6 | 1.81 |
| Oral hypoglycemic | 2.52 | 2.24 | 1.84 | 2 | 2.17 | 2.89 |
| β-agonist | 0.1 | 0.1 | 0.1 | 0.09 | 0.12 | 0.69 |
| Aspirin | 0.19 | 0.19 | 0.16 | 0.14 | 0.17 | 1.09 |
| Corticosteroid | 5.94 | 5.44 | 4.63 | 5.2 | 5.43 | 3.82 |
| Comorbid conditions (%) | ||||||
| Congestive heart failure | 4.17 | 3.72 | 3.23 | 3.4 | 3.62 | 2.81 |
| Chronic obstructive pulmonary disease | 6.17 | 4.84 | 3.71 | 4.63 | 4.86 | 6.89 |
| Myocardial infarction | 1.16 | 0.99 | 0.8 | 0.89 | 0.93 | 2.18 |
| Diabetes | 12.45 | 11.36 | 9.92 | 10.59 | 10.51 | 4.73 |
| Smoking | 10.9 | 9.95 | 8.39 | 8.53 | 9.64 | 5.23 |
| Obese | 5.51 | 5.62 | 5.14 | 4.87 | 5.68 | 3.42 |
To analyze the outcome cardiovascular death, we first consider descriptive statistics. Figure 1 displays the mortality rate, per 1,000,000 prescriptions, for each antibiotic in each time interval adjusted for IPTW. There are several notable features. First, azithromycin has the highest mortality rate in the first 5 days (84.62) while clindamycin has the lowest (after propensity score weighting, cardiac deaths per million within the first 5 days were: 84.6 for azithromycin, 78.3 for clarithromycin, 69.4 for amoxicillin, 61.6 for floxacin and 15.0 for clindamycin). However, for the 6–10 day interval, the mortality rate of azithromycin drops substantially before rebounding in later periods. Second, amoxicillin has the highest mortality rate over the 11–15, 16–20 and 20–25 day intervals. Third, clindamycin starts with a low mortality rate but displays an increasing trend with successive intervals. The opposite is true for clarithromycin. The mortality rate starts relatively high, but in the 26–30 day interval clarithromycin has the lowest mortality rate.
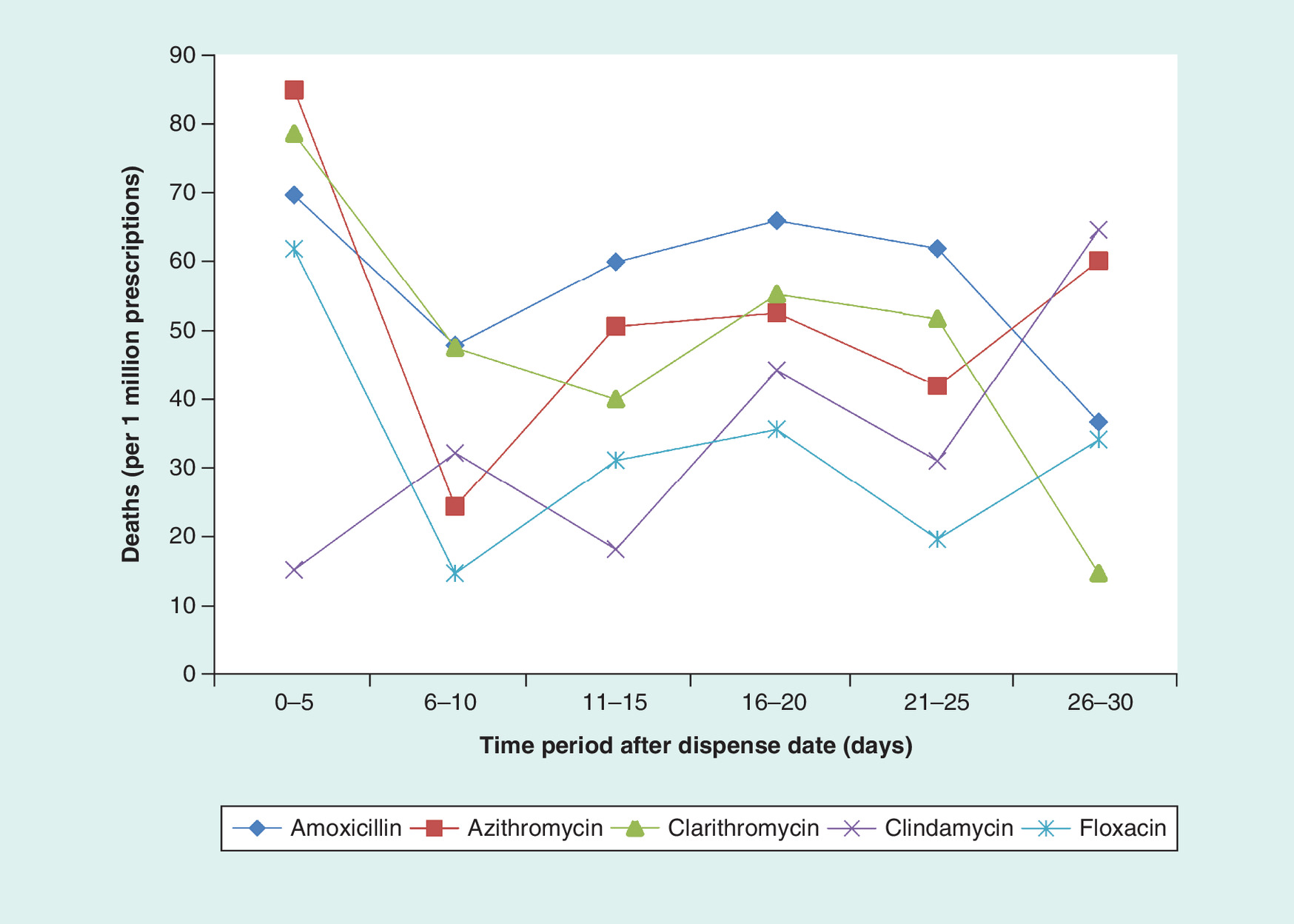
Figure 1. Inverse probability treatment weighting adjusted mortality rate at each time interval.
Floxacin = levofloxacin, ciprofloxacin, moxifloxacin.
We estimate multivariate logistic regression models to evaluate the odds of cardiovascular death.
Table 3 displays OR estimated from the pooled logistic regression models for each of the four time-intervals. Each model is estimated using the IPTW as described in the above sections. The estimates reveal a nonstatistically significant difference (p > 0.05) between study antibiotics and the reference group azithromycin in all time intervals. During the 0–5 day inteval, all study antibiotics have lower odds (not statistically significant) of cardiac death compared with azithromycin (amoxicillin OR: 0.71 [95% CI: 0.25–1.99]; clarithromycin OR: 0.96 [95% CI: 0.37–2.46]; clindamycin OR: 0.22 [95% CI: 0.04–1.07]; floxacin OR: 0.96 [95% CI: 0.35–2.65]). During 6–10 day interval, the odds of cardiac death are increased (not statically significant) for amoxicillin (OR: 1.65 [95% CI: 0.34–8]), clarithromycin (OR: 2.29 [95% CI: 0.50–10.45]) and clindamycin (OR: 1.57 [95% CI: 0.31–7.84]). Estimates for the 0–10 day and 0–30 day timeframe reveal nonstatistically significant differences between azithromycin and all study antibiotics.
| Variables | Model; OR (95% CI) | |||
|---|---|---|---|---|
| 0–5 days | 6–10 days | 0–10 days | 0–30 days | |
| Amoxicillin | 0.71 (0.25–1.99) | 1.65 (0.34–8.00) | 0.92 (0.39–2.15) | 0.94 (0.57–1.55) |
| Clarithromycin | 0.96 (0.37–2.46) | 2.29 (0.50–10.45) | 1.24 (0.56–2.74) | 0.97 (0.59–1.58) |
| Clindamycin | 0.22* (0.04–1.07) | 1.57 (0.31–7.84) | 0.52 (0.19–1.45) | 0.81 (0.48–1.38) |
| Floxacin | 0.96 (0.35–2.65) | 0.72 (0.10–5.11) | 0.90 (0.37–2.21) | 0.81 (0.47–1.40) |
| Race: | ||||
| – White | 0.97 (0.32–2.95) | 2.68 (0.31–23.18) | 1.26 (0.47–3.37) | 1.10 (0.58–2.07) |
| – Black | 0.63 (0.19–2.10) | 1.70 (0.17–16.60) | 0.81 (0.28–2.33) | 1.47 (0.78–2.78) |
| Age | 1.08*** (1.05–1.11) | 1.13*** (1.07–1.19) | 1.10*** (1.07–1.12) | 1.09*** (1.08–1.11) |
| Sex (male) | 1.45 (0.67–3.14) | 6.86*** (2.60–18.13) | 2.58*** (1.47–4.53) | 2.39*** (1.70–3.36) |
| Comorbid diagnoses | 1.20** (1.03–1.39) | 0.95 (0.73–1.24) | 1.11 (0.97–1.27) | 1.10** (1.01–1.19) |
| Confounding prescriptions | 1.01 (0.75–1.36) | 1.35* (0.97–1.88) | 1.13 (0.91–1.42) | 1.15** (1.01–1.32) |
| Year | 0.92 (0.80–1.06) | 0.93 (0.74–1.16) | 0.92 (0.82–1.04) | 0.93** (0.87–0.99) |
Significance levels: *p ≤ 0.1; **p ≤ 0.05; ***p ≤ 0.001. Azithromycin is the reference group.
OR: Odds ratio.
To take a closer look at the relationships between the antibiotics, we examined the pairwise OR for cardiovascular death for the 0–5 day interval. Table 4 displays the OR along with unadjusted confidence intervals and Tukey-adjusted intervals. Both intervals cross 1 for all comparisons indicating no statistically significant differences. To account for subject correlation within our data, we estimated population-averaged models using GEE [27]. Table 5 displays the estimation results for all four time intervals. All models use IPTW adjustment. The results are consistent with our pooled analysis. We find no statistically significant difference between any of the antibiotics and azithromycin. Finally, Supplementary Tables 10 & 11 display pooled logit and GEE model, respectively, without IPTW adjustment. There is no statistically significant difference between the antibiotics.
| Antibiotic | OR | 95% CI | Tukey adjusted 95% CI |
|---|---|---|---|
| Amoxicillin–Clarithromycin | 0.739 | 0.261–2.094 | 0.173–3.149 |
| Amoxicillin–Clindamycin | 3.281 | 0.624–17.264 | 0.325–33.086 |
| Amoxicillin–Floxacin | 0.737 | 0.248–2.190 | 0.162–3.356 |
| Azithromycin–Amoxicillin | 1.410 | 0.504–3.968 | 0.338–5.921 |
| Azithromycin–Clarithromycin | 1.045 | 0.407–2.686 | 0.281–3.887 |
| Azithromycin–Clindamycin | 4.643 | 0.931–23.144 | 0.496–43.424 |
| Azithromycin–Floxacin | 1.042 | 0.378–2.876 | 0.254–4.281 |
| Clarithromycin–Clindamycin | 4.442 | 0.891–22.148 | 0.475–41.56 |
| Clarithromycin–Floxacin | 0.997 | 0.35–2.845 | 0.232–4.29 |
| Clindamycin–Floxacin | 0.225 | 0.043–1.161 | 0.023–2.209 |
ORs were computed by setting all other predictors at their means/medians.
OR: Odds ratio.
| Variable | Model; OR (95% CI) | |||
|---|---|---|---|---|
| 0–5 days | 6–10 days | 0–10 days | 0–30 days | |
| Amoxicillin | 0.7 (0.32–1.57) | 1.65 (0.48–5.67 | 0.92 (0.47–1.8) | 0.94 (0.64–1.39) |
| Clarithromycin | 0.96 (0.38–2.41) | 2.29 (0.54–9.78) | 1.25 (0.58–2.68) | 0.97 (0.59–1.58) |
| Clindamycin | 0.21 (0.03–1.61) | 1.57 (0.16–15.54) | 0.52 (0.11–2.5) | 0.81 (0.37–1.78) |
| Floxacin | 0.96 (0.28–3.3) | 0.72 (0.16–3.19) | 0.9 (0.32–2.56) | 0.81 (0.45–1.46) |
| Race: | ||||
| – Black | 0.63 (0.12–3.21) | 1.7 (0.17–16.83) | 0.81 (0.2–3.32) | 1.46 (0.68–3.14) |
| – White | 0.97 (0.21–4.56) | 2.66 (0.5–14.1) | 1.26 (0.35–4.5) | 1.11 (0.51–2.37) |
| Sex (male) | 1.45 (0.62–3.36) | 6.89*** (1.89–25.12) | 2.59*** (1.25–5.34) | 2.39*** (1.55–3.67) |
| Age | 1.08*** (1.06–1.1) | 1.13*** (1.06–1.2) | 1.09*** (1.07–1.12) | 1.09*** (1.07–1.12) |
| Comorbid diagnoses | 1.2 (0.97–1.49) | 0.95 (0.8–1.13) | 1.11 (0.93–1.32) | 1.09 (0.99–1.21) |
| Confounding prescriptions | 1.01 (0.75–1.36) | 1.35 (0.88–2.08) | 1.14 (0.88–1.47) | 1.15* (1–1.32) |
| Year | 0.92 (0.79–1.08) | 0.92 (0.74–1.15) | 0.92 (0.82–1.04) | 0.92** (0.85–1) |
Significance levels: *p ≤ 0.1; **p ≤ 0.05; ***p ≤ 0.001. Azithromycin is the reference group.
OR: Odds ratio.
Discussion
This retrospective database analysis of South Carolina Medicaid patients evaluated the association of cardiovascular mortality in patients prescribed azithromycin compared with patients prescribed alternative antibiotics in an outpatient setting. Our data reveals that the study antibiotics’ (amoxicillin, clindamycin, clarithromycin, levofloxacin, ciprofloxacin and moxifloxacin) mortality rates are not statistically different from azithromycin during the 0–30 day time intervals in patients at a low risk of death from causes other than study antibiotics. Additionally, both pooled multivariate models and GEE demonstrate that the antibiotics are not statistically different from azithromycin in any time interval. Our study was initiated based upon evidence that azithromycin increases cardiovascular mortality, which led us to hypothesize that azithromycin would increase the risk of cardiovascular death in our population [3,4]. Table 6 displays comparable results for the risk of death in the first 5 days across studies. The Svanström and Pasternak (Denmark) study shows a low number of deaths (15) per 1,000,000 prescriptions. In comparison with Ray et al. (Tennessee) study, the deaths per million prescriptions are very similar to South Carolina, 85.2 and 84.6, respectively. Comparing the risk ratios, we find that the Rao et al. (US veterans), Ray et al. (Tennessee) and the South Carolina results are consistent; azithromycin is associated with higher odds of cardiovascular death compared with amoxicillin. The risk ratio in South Carolina is 1.41, 1.48 in the US veterans study and 2.49 in the Tennessee Medicaid study. However, in the South Carolina, we find no statistically significant difference between the two antibiotics. One reason for our null results could be the lack of statistical power. We calculated the posthoc power for our unweighted and IPTW pooled logit models. We found that the unweighted pooled model had 80% power to detect an increased risk of death by a factor of at least 2.5 at an α-level of 0.05. Our IPTW model had 80% power to detect an increased risk of death by at least a factor of 3.5. Our results suggest that, while we cannot rule out the increased risk of cardiovascular death from azithromycin, the risk may not be as large initial studies suggest. Further, our results coupled with those from Svanström and Pasternak, Abdulhak, and Mortensen, suggest that the increase in cardiovascular mortality associated with azithromycin found in initial studies may not be applicable to the general population.
| Study | Risk ratio | 95% CI | Deaths per 1,000,000 prescriptions |
|---|---|---|---|
| Tennessee† | 2.49 | 1.38–4.50 | 85.2 |
| US veterans† | 1.48 | 1.05–2.09 | 228.0 |
| Denmark‡ | 0.93 | 0.56–1.55 | 15.4 |
| South Carolina† | 1.41 | 0.33–5.92 | 84.6 |
†Azithromycin to amoxicillin comparison.
‡Azithromycin to penicillin comparison.
Data taken from [3–5].
An important concern in this observational study was confounding by factors associated with both antibiotic use and an increased risk of cardiovascular death. The Ray et al. study demonstrated a statistically significant effect on a sample of Tennessee Medicaid patients, but this was not supported by our study of South Carolina Medicaid patients. Therefore, there could be other factors (besides or in addition to antibiotic treatment) that may influence outcomes. One important difference between our study and the Ray et al. study is that the Ray et al. study evaluated an older cohort (ages 30–74 years) whereas our cohort evaluated a wider range (ages 17–74 years). It is possible that the cardiovascular risk associated with azithromycin found by Ray et al. is specific to older age groups. Abdulhak et al. demonstrated in a meta-analysis subgroup analysis that azithromycin use within 1–5 days of therapy was associated with a higher risk of death among older populations (≥40 years of age), but not the entire cohort. However, our study lacks the power to find an effect in the age restricted sample size. Additionally, the studies evaluating cardiovascular death among azithromycin have utilized different methodology. There are studies that utilized HR (Ray et al. [3] and Rao et al. [4]) and there are studies that utilized OR (Mortensen et al. [6] and Chou et al. [7]). The HR is the analysis of the time to event and the OR is the analysis of whether an event occurred within a designated time frame. HRs and ORs cannot be directly compared; however, the ratios can compare whether each approach determined an association between similar variables. Select azithromycin analyses have found associations of azithromycin with cardiac mortality using HRs and ORs. Although our point estimates indicate the increased odds of cardiac death within 5 days as not statistically significant.
This study has a number of strengths. We utilized a large sample of a similar population as Ray et al. (Medicaid patients). We included several study antibiotics and the risk of azithromycin was analyzed relative to several study antibiotics and several different time points. We used multiple strategies to minimize confounding based upon both matching and regression adjustment with propensity scores to reduce possible bias in the estimated treatment (group) effect from confounders. The results for the covariates are consistent with common causes of cardiovascular death in that the older people are more likely to die from cardiovascular causes. Additionally, we believe that restriction to patients receiving outpatient antibiotics introduces consistency to the analysis and thus validity, because patients receiving outpatient antibiotics are more likely to have similar acute conditions (vital signs, temperature) compared with those not receiving antibiotics. Although the study utilized regression models to adjust for known confounders, unexpected confounders may have affected the study outcomes. These potential limitations are possible within observational studies. We did not have information for all cardiovascular risk (e.g., smoking status, body mass and family history). Therefore, residual confounding cannot be ruled out. Specifically, patients given a prescription for azithromycin or alternative study antibiotic may be different from those who were not, in ways that could bias the results. Such differences or biases may be related to the antibiotics used (confounding by indication), severity of the disease and comorbidities. Furthermore, vital records were obtained from the Department of Health and Environmental Control and cause of death was linked to the Medicaid member from the death certificate. Mortality data were not confirmed using a secondary data source. Therefore, it is plausible that the lack of mortality difference is because of error or delay in data reporting.
Conclusion
Our study shows that the cardiovascular mortality associated with azithromycin is not statistically significant from other antibiotics and the previous [3,4] findings may not be applicable to the general population. Additionally, our results suggest that while we cannot rule out the increased risk of cardiovascular death from azithromycin in patients at low risk of death, the risk may not be as large initial studies suggest. Further research is needed to define the population at greatest risk.
The mortality and cardiovascular effects of azithromycin are not statistically significant from other antibiotics.
Previous published findings (Ray et al. and Rao et al.) may not be applicable to the general population.
Further research is needed to define the population at greatest risk.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/full/10.2217/cer-2016-0080
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (suppl_appendix.docx)
- Download
- 73.38 KB
References
1.
Shaffer D, Singer S, Korvick J, Honig P. Concomitant risk factors in reports of Torsades de Pointes associated with macrolide use: review of the US FDA Adverse Event Reporting System. Clin. Infect. Dis. 35(2), 197–200 (2002).
2.
Milberg P, Eckardt L, Bruns H-J et al. Divergent proarrhythmic potential of macrolide antibiotics despite similar QT prolongation: fast Phase III repolarization prevents early afterdepolarizations and Torsade de Pointes. J. Pharmacol. Exp. Ther. 303(1), 218–225 (2002).
3.
Ray WA, Murray KT, Hall K, Arbogast PG, Stein CM. Azithromycin and the risk of cardiovascular death. N. Engl. J. Med. 366(20), 1881–1890 (2012).
4.
Rao GA, Mann JR, Shoaibi S et al. Azithromycin and levofloxacin use and increased risk of cardiac arrhythmia and death. Ann. Fam. Med. 12, 121–127 (2014).
5.
Svanström H, Pasternak B, Hviid A. Use of azithromycin and death from cardiovascular causes. N. Engl. J. Med. 368, 1704–1712 (2013).
6.
Mortensen EM, Halm EA, Pugh MJ et al. Association of azithromycin with mortality and cardiovascular events among older patients hospitalized with pneumonia. JAMA 311(21), 2199–2208 (2014).
7.
Chou HW, Wang JL, Chang CH, Lai CL, Lai MS, Chan KA. Risks of cardiac arrhythmia and mortality among patients using new generation macrolides, fluoroquinolones and β-lactam/β-lactamase inhibitors: a Taiwanese nationwide study. Clin. Infect. Dis. 60(4), 566–577 (2015).
8.
Bin Abdulhak AA, Khan AR, Garbati MA et al. Azithromycin and risk of cardiovascular death: a meta-analytic review of observational studies. Am. J. Ther. 22(5), E122–E129 (2015).
9.
Samarendra P, Kumari S, Evans SJ, Sacchi TJ, Navarro V. QT prolongation associated with azithromycin/amiodarone combination. Pacing Clin. Electrophysiol. 24(10), 1572–1574 (2001).
10.
Arellano-Rodrigo E, Garcia A, Mont L, Roque M. Torsade de Pointes and cardiorespiratory arrest induced by azithromycin in a patient with congenital long QT syndrome. Med. Clin. (Barc.) 117(3), 118–119 (2001).
11.
Santos N, Oliveira M, Galrinho A, Oliveira JA, Ferreira L, Ferreira R. QT interval prolongation and extreme bradycardia after a single dose of azithromycin. Rev. Port. Cardiol. 29(1), 139–142 (2010).
12.
Huang BH, Wu CH, Hsia CP, Yin Chen C. Azithromycin-induced Torsade de Pointes. Pacing Clin. Electrophysiol. 30(12), 1579–1582 (2007).
13.
Kezerashvili A, Khattak H, Barsky A, Nazari R, Fisher JD. Azithromycin as a cause of QT-interval prolongation and Torsade de Pointes in the absence of other known precipitating factors. J. Interv. Card. Electrophysiol. 18(3), 243–246 (2007).
14.
Kim MH, Berkowitz C, Trohman RG. Polymorphic ventricular tachycardia with a normal QT interval following azithromycin. Pacing Clin. Electrophysiol. 28(11), 1221–1222 (2005).
15.
Matsunaga N, Oki Y, Prigollini A. A case of QT-interval prolongation precipitated by azithromycin. NZ Med. J. 116(1185), U666 (2003).
16.
Lu ZK, Yuan J, Li M et al. Cardiac risks associated with antibiotics: azithromycin and levofloxacin. Expert Opin. Drug Saf. 14(2), 295–303 (2014).
17.
Zithromax. Pfizer Inc., NY, USA (2013).
18.
Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika 70(1), 41–55 (1983).
19.
Imbens GW. The role of the propensity score in estimating dose-response functions. Biometrika 87(3), 706–710 (2000).
20.
Ima K, Van Dyk DA. Causal inference with general treatment regimes. J. Am. Stat. Assoc. 99(467), 854–866 (2004).
21.
Foster EM. Propensity score matching: an illustrative analysis of dose response. Med. Care 41(10), 1183–1192 (2003).
22.
Wang J, Donnan PT, Steinke D, MacDonald TM. The multiple propensity score for analysis of dose–response relationships in drug safety studies. Pharmacoepidemiol. Drug Saf. 10(2), 105–111 (2001).
23.
Harder VS, Stuart EA, Anthony JC. Propensity score techniques and the assessment of measure covariate balance to test causal associations in psychological research. Psychol. Methods 15(3), 234–249 (2010).
24.
Stürmer T, Rothman KJ, Avorn J, Glynn RJ. Treatment effects in the presence of unmeasured confounding: dealing with observations in the tails of the propensity score distribution– a simulation study. Am. J. Epidemiol. 172(7), 843–854 (2010).
25.
Kurth T, Walker AM, Glynn RJ et al. Results of multivariable logistic regression, propensity matching, propensity adjustment and propensity-based weighting under conditions of nonuniform effect. Am. J. Epidemiol. 163(3), 262–270 (2006).
26.
Rosenbaum PR, Rubin DB. Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am. Stat. 39(1), 33–38 (1985).
27.
Hardin JW, Hilbe JM. Generalized Estimating Equations (2nd Edition). CRC Press, FL, USA (2012).
Information & Authors
Information
Published In
Copyright
© 2017 Future Medicine Ltd.
History
Published online: 29 September 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Appraisal of the cardiovascular risks of azithromycin: an observational analysis. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0080
Export citation
Select the citation format you wish to export for this article or chapter.