Characteristics and treatment patterns among US patients with hairy cell leukemia: a retrospective claims analysis
Abstract
Aim: Describe hairy cell leukemia (HCL) treatment patterns using a large, nationally representative US database. Patients & methods: Adults newly diagnosed with HCL (1 January 2006 to 30 June 2014) with continuous health plan enrollment ≥180 days pre- and 90 days post-diagnosis were identified from the QuintilesIMS PharMetrics Plus Health Plan Claims Database. Treatment patterns by line of therapy were assessed over the variable follow-up. Results: Among 749 HCL patients (77.4% male; mean age 55.6; mean 32.3 months follow-up), only 37.7% initiated first-line therapy during the available follow-up in a mean of 4.4 months following diagnosis; the majority (75.5%) received cladribine (mean duration 7.3 days). Thirty-eight patients (5.1%) received second-line treatment. Conclusion: Over 2.7 years follow-up, more than a third of patients initiated first-line therapy which appeared to provide a long-lasting response.
First draft submitted: 21 February 2017; Accepted for publication: 20 April 2017; Published online: 9 May 2017
Hairy cell leukemia (HCL) is a rare, indolent, low-grade B-cell lymphoid leukemia, comprising approximately 2% of all leukemias and with an estimated 900 new cases in the USA each year [1]. HCL is more common in males (with a 4:1 ratio to women) and median age at diagnosis is approximately 55 years [1]. While HCL is not curable, it is responsive to available therapies and the goal is to achieve complete remission [1,2]. Over the last few decades, the treatment strategy for HCL has shifted from the use of splenectomy and interferon-alfa to use of a single-agent purine nucleoside analog (PNA), either pentostatin or cladribine [3]. The CD20-targeting monoclonal antibody, rituximab, may be considered in patients with relapse or refractory following initial PNA therapy [4].
Not all newly diagnosed patients with HCL will require treatment immediately, and for symptomatic patients, or patients with significant cytopenias, National Comprehensive Cancer Network (NCCN) guidelines recommend first-line (1L) therapy with either pentostatin or cladribine [4]. Second-line (2L) treatment options for patients with relapsed/refractory HCL depend upon the quality and duration of remission to initial therapy [4]. For patients with a complete response that relapse 1 year or later from initial response, NCCN guidelines recommend retreatment with the same PNA with or without rituximab, or treatment with the alternative PNA with or without rituximab [4]. For patients with a complete response that relapse within 1 year of initial response, or for patients with less than a complete response to initial therapy, 2L options include treatment with the alternative PNA with or without rituximab, rituximab alone, IFN-α or participation in a clinical trial [4]. Recent guidelines from the European Society for Medical Oncology and consensus guidelines from an international conference convened by the Hairy Cell Leukemia Foundation provide similar treatment recommendations for patients with HCL in 1L with some differences in treatment recommendations following 1L [5,6].
While no clinical trials have compared pentostatin and cladribine, a long-term retrospective, single institute study in the UK found no significant difference in outcome (e.g., response rates and disease-free survival) between pentostatin and cladribine either at first or subsequent lines of therapy [7,8]. The majority (76–91%) of patients treated with either therapy are expected to achieve a durable complete remission [1]. Overall survival rates have ranged from 80 to 90% with pentostatin at 10 years, and 97% with cladribine at 9 years [9]. However, relapse occurs in 30–40% of patients after 5–10 years of follow-up [3]. Response may vary by age, and long-term follow-up is needed for this rare malignancy to determine overall survival versus competing mortalities associated with aging [2].
Common toxicities with PNA therapy are neutropenia and thrombocytopenia; however, long-term retrospective studies among large samples have reported high rates of febrile neutropenia with cladribine (42%) and relatively lower rates with pentostatin (17%) [9–11]. Duration of therapy until documented complete remission also varies between the two therapies, and pentostatin may be given at 2-week intervals for up to 6 months or longer, while patients treated with cladribine usually receive a single 5–7 day course of therapy [1]. The comparative ease of administration of cladribine, delivered as a single course of therapy, has led to cladribine being the initial therapy selected by most hematologists/oncologists [2,12].
Real world data on HCL treatment pathways and treatment outcomes among large sample sizes are limited, particularly in the USA. Real-world studies have primarily focused on single-institution or multicenter studies evaluating clinical outcomes outside of the USA, and the larger studies (with patient sample sizes of at least 100) have been located in Italy, France, Spain and the UK [7,8,13–15]. In the USA, the Surveillance, Epidemiology, and End Results (SEER) database has been used to investigate survival and autoimmune conditions in HCL, while clinical characteristics and long-term outcomes have recently been reported among 88 young HCL patients treated with cladribine at the Scripps Clinic in La Jolla, California [16–19]. Costs associated with HCL, relevant to both the payer and patient perspectives, are unavailable from the literature.
Given the absence of real-world data, the primary objectives of this study were to identify newly diagnosed HCL patients using a large, US database, nationally representative of the commercially insured population, to describe patient characteristics, to evaluate treatment utilization and patterns by line of therapy (LOT) and to measure healthcare resource utilization (HCRU) and costs.
Patients & methods
Data source
This observational retrospective cohort study utilized data from the QuintilesIMS PharMetrics Plus Health Plan Claims Database from 1 January 2006 to 30 June 2014. The database is comprised of longitudinal, adjudicated administrative claims data for more than 150 million unique health plan members across the USA. Data elements include in-patient and outpatient diagnoses and procedures, retail and mail order prescription records, pharmacy and medical benefit information, in-patient stay and provider details, demographic variables, product type, payer type, and start and stop dates of health-plan enrollment. Amounts charged by providers and amounts allowed and paid by health plans are available for all services rendered. PharMetrics Plus also has detailed information on the pharmacy and medical benefit (copayment, deductible). Due to the broad reach of the data (∼1 in 3 Americans), the database is nationally representative of the commercially insured US population in terms of age and gender. All data are compliant with the Health Insurance Portability and Accountability Act (HIPAA) to protect patient’s privacy.
Sample selection
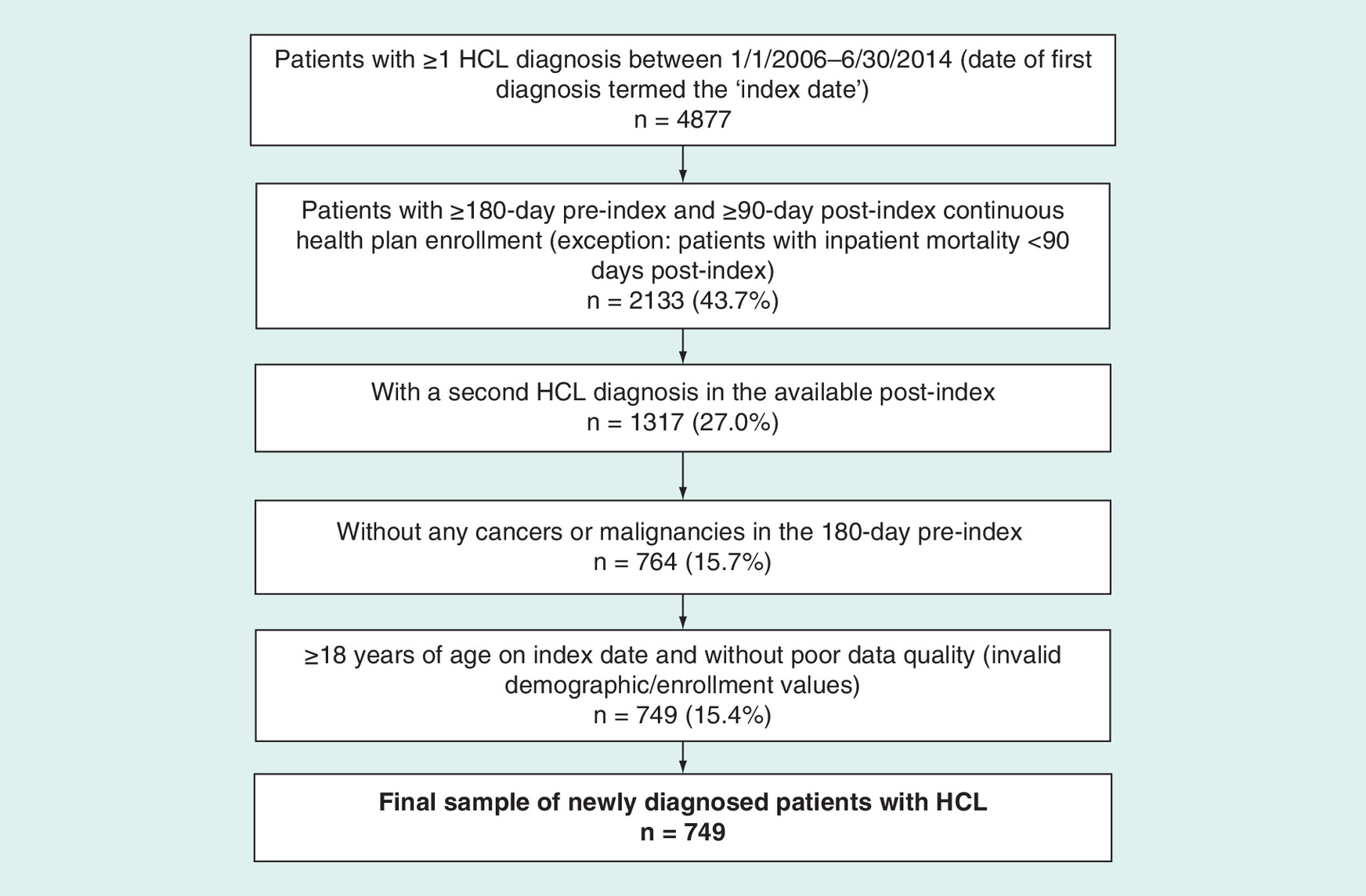
Patients were evaluated for study inclusion if they had a diagnosis of HCL (ICD-9-CM code 202.4×) on a medical claim between 1 January 2006 and 30 June 2014. The date of the first observed diagnosis was termed as the ‘index date’. Patients were required to have continuous enrollment (CE) in the health plan ≥180 days prior to the index date (the ‘preindex’ period) in order to assess baseline patient characteristics and ≥90 days CE following the index date (the variable ‘follow-up’ period) to evaluate the study outcomes; however, patients with in-patient mortality within 90 days postindex were not excluded. A confirmatory, second HCL diagnosis was required at any time in the available follow-up. Patients were excluded with any cancer or malignancies (ICD-9-CM 3-digit level codes for neoplasms [140–239]) in the preindex period to help ensure observation of newly diagnosed HCL patients without any other cancers, which could complicate the exploration of HCL-treatment patterns. Patients were required to be ≥18 years of age at index date. Patients with incomplete data (e.g., invalid demographic or enrollment data, Medicare cost or State Children's Health Insurance Program [SCHIP] plans) were excluded.
Line of therapy definitions
Chemotherapy and/or biologic therapy use was examined for each patient following the index date in order to identify the LOT regimens. LOT was defined based on the sequencing and dates of therapy use (i.e., initiation and discontinuation). A comprehensive list of drugs/biologics were evaluated as HCL related, based on those recommended by NCCN treatment guidelines, as well as those recommended for leukemia and non-Hodgkin's lymphoma in general (steroids were not included). This claims-based algorithm to define LOT was developed prior to data analysis based on a review of the published cancer literature using administrative claims data given the absence of relevant HCL studies [20–22].
Initiation of a 1L treatment regimen was identified by the first chemotherapy and/or biologic drug for HCL following the index date. A treatment regimen was identified by all chemotherapies and/or biologics given to a patient within the first 2 weeks of initiation. The date of the first HCL therapy in the 1L regimen was termed the date of 1L therapy initiation. An LOT was defined as ending based on the first occurrence of either: use of a new drug not in the treatment regimen (either addition or switch) following the first 2 weeks of therapy; a gap in all HCL therapy of >90 days (for orals, the 90-day gap was assessed after days’ supply end date [i.e., date of prescription fill plus days’ supply]); or end of follow-up. End of follow-up was defined based on the first occurrence of end of patient continuous enrollment, in-patient mortality or end of study period (30 June 2014). The date of the use of the new drug, the first day in the 90-day gap or the date of end of follow-up, respectively, defined the end of that LOT. The subsequent LOT started with the use of a new drug (new drug addition to the existing treatment regimen or switch to a new drug) following the first 2 weeks of therapy, or next drug following the >90-day gap in therapy. Subsequent 2L and third-line (3L) treatment regimens were assessed applying the same methods.
Study outcomes
Patient characteristics were reported for the overall sample of newly diagnosed HCL patients, with clinical characteristics measured over the 180 days preindex. Clinical characteristics included Charlson Comorbidity Index (CCI) score (with HCL excluded from the calculation), physician specialty associated with the index diagnosis (the physician specialty on the index date, or if missing, the physician specialty for the office visit closest to [before or after] the index date), presence of relevant comorbidities (HCL-related or common comorbidities) and total 180-day preindex healthcare costs. Characteristics were also assessed for the 1L population, 2L population and patients that did not receive any HCL therapy over the follow-up. Among patients initiating 1L and 2L therapy, clinical characteristics were also evaluated as measured over the 180 days prior to 1L and 2L initiation, respectively, in order to understand characteristics that may be associated with disease progression or treatment.
Number of LOTs received was evaluated. Time to initiation of an LOT was described at the patient level. Therapies utilized in each LOT were described as well as sequential treatment pathways. Each LOT was characterized by duration (from initiation of an LOT treatment regimen to the end of the LOT).
Given the lack of clinical data and lab values (e.g., to identify complete response etc.), relapse and refractory disease following 1L were defined based on time to initiation of 2L therapy. Patients who initiated 2L were either classified as having relapsed disease following 1L if the gap between the prior regimen and subsequent regimen was ≥365 days or as having refractory disease following 1L if the gap was <365 days.
All-cause HCRU and costs were assessed over the variable follow-up period. HCRU included the mutually exclusive categories of outpatient pharmacy prescriptions, hospitalizations, emergency room visits and outpatient care (including outpatient physician office visits, outpatient surgical visits, and lab tests and other services [including HCL-related injections]). Costs were assessed for HCRU service categories by summing the allowed amounts reported by payers, comprising the amount paid by the health plan and patient combined. HCL-related costs were also assessed based on the presence of an HCL diagnosis code and/or HCL-associated therapies. Healthcare utilization and costs over the variable follow-up period were evaluated on a per-patient basis. All costs were adjusted to 2014 US dollars using the medical care component of the US Consumer Price Index. Total HCRU was also reported at an annualized level using the calculation: annualized rate of use = (units used postindex)/(days follow-up postindex/365). Total healthcare costs were also reported at an annualized level using the calculation: annualized cost = (cost postindex)/(days follow-up postindex/365).
Analyses
Descriptive summary statistics were used to describe the data. In general, findings were reported for categorical variables using frequency and percentage distributions, while mean, standard deviation (SD) and median were used to describe continuous variables. Analyses were performed using SAS version 9.3 (SAS Institute, Inc., NC, USA).
Results
Patient sample
A total of 749 adults newly diagnosed with HCL between 2006 and 2014 were identified that met all study eligibility criteria (see Figure 1). The majority (n = 467; 62.3%) of newly diagnosed HCL patients did not initiate any HCL therapy over the available follow-up. Of the overall sample (n = 749), 37.7% (n = 282) initiated 1L therapy, 5.1% of patients (n = 38) initiated 2L therapy and 1.5% (n = 11) initiated 3L therapy. Among the 282 patients initiating therapy, 86.5% (n = 244) received 1L therapy only, 9.6% (n = 27) received both 1L and 2L therapy and 3.9% (n = 11) received three LOTs.
Demographic characteristics
Demographic characteristics of the overall sample, patients initiating 1L therapy, patients initiating 2L therapy and patients that did not initiate HCL therapy can be found in Table 1. Among the overall sample, mean (SD) age was 55.6 (10) years at diagnosis. The majority of patients were male (77.4%) and commercially insured (64.1%). Patients were most frequently located in the Midwest (37.5%). Overall, patients had a mean follow-up from diagnosis of 32.3 (22.0) months. Patients who did and did not initiate HCL-related therapy over the follow-up appeared to be similar in most demographic characteristics. However, patients that did not initiate therapy had a slightly higher mean age of 56.8 (9.9) years at diagnosis, compared with 53.8 (9.8) years for patients initiating 1L and 53.9 (12.1) years for patients initiating 2L. Additionally, available follow-up time varied. Patients who did not initiate HCL-related therapy over the available follow-up had mean follow-up from diagnosis of 31.3 (21.8) months. Compared with patients not initiating HCL-related therapy, mean follow-up from diagnosis was longer for patients who initiated 1L therapy (33.8 [22.3] months) and even longer for patients who initiated 2L therapy (39.9 [22.6] months).
Clinical characteristics
Clinical characteristics of the overall sample, the 1L sample, the 2L sample and patients that did not initiate HCL therapy can be found in Table 2. Among the overall sample, more than half (57.8%) of patients had a CCI score of 0 at diagnosis. The most frequent comorbidities in the 6 months prior to diagnosis were hypertension (24.2%), aplastic anemia (21.5%), anemia (19.4%) and splenomegaly (14.2%). A total of five (0.7%) patients died in hospital over the available follow-up. For patients that did not initiate any HCL therapy over the follow-up, presence of several baseline comorbidities was lower compared with patients that went on to initiate HCL therapy: anemia (12.2 vs 31.2%), aplastic anemia (12.8 vs 35.8%) and splenomegaly (10.1 vs 20.9%). In the 6 months preindex, mean all-cause healthcare costs were US$5858 (US$13,836) with median costs of US$2593.
Among patients receiving 1L therapy, a number of clinical characteristics as measured in the 6 months prior to 1L therapy initiation suggested worsening disease compared with as measured in the 6 months prior to HCL diagnosis Supplementary Table 1. At initiation of 1L therapy, half of the patients had a CCI score greater than 0 (53.2%), while at baseline, half (50.4%) had a CCI score of 0. Presence of a number of comorbidities appeared to increase from 6 months prior to diagnosis to 6 months prior to initiation of 1L therapy: aplastic anemia (49.6 vs 35.8%), anemia (39.7 vs 31.2%) and splenomegaly (37.2 vs 20.9%). The median duration of follow-up after initiation of 1L therapy was 23.2 months. Among patients receiving 1L therapy, mean all-cause healthcare costs were US$6635 (US$7246) in the 6 months prior to diagnosis, which increased to US$16,018 (US$17,172) in the 6 months prior to 1L initiation. Among patients receiving 2L therapy (n = 38), at initiation of 2L therapy, 65.8% of patients had a CCI score of 2 or higher, while at baseline, half (44.7%) had a CCI score of 0 (Supplementary Table 1).
Treatment patterns
Among patients receiving 1L, patients initiated 1L therapy in a mean of 4.4 (9.8) months from the date of HCL diagnosis and patients had mean follow-up of 29.5 (21.0) months following 1L therapy initiation (Supplementary Table 2). The mean duration of 1L therapy was 34.1 (104.4) days with a median of 5 days. Almost all patients (92.9%) initiated a single therapy regimen in 1L, and cladribine was most frequently utilized (75.5%). Next, most frequent therapies in 1L were pentostatin (8.5%) and rituximab (6.0%). See Figure 2 for the distribution of 1L, 2L and 3L therapies.
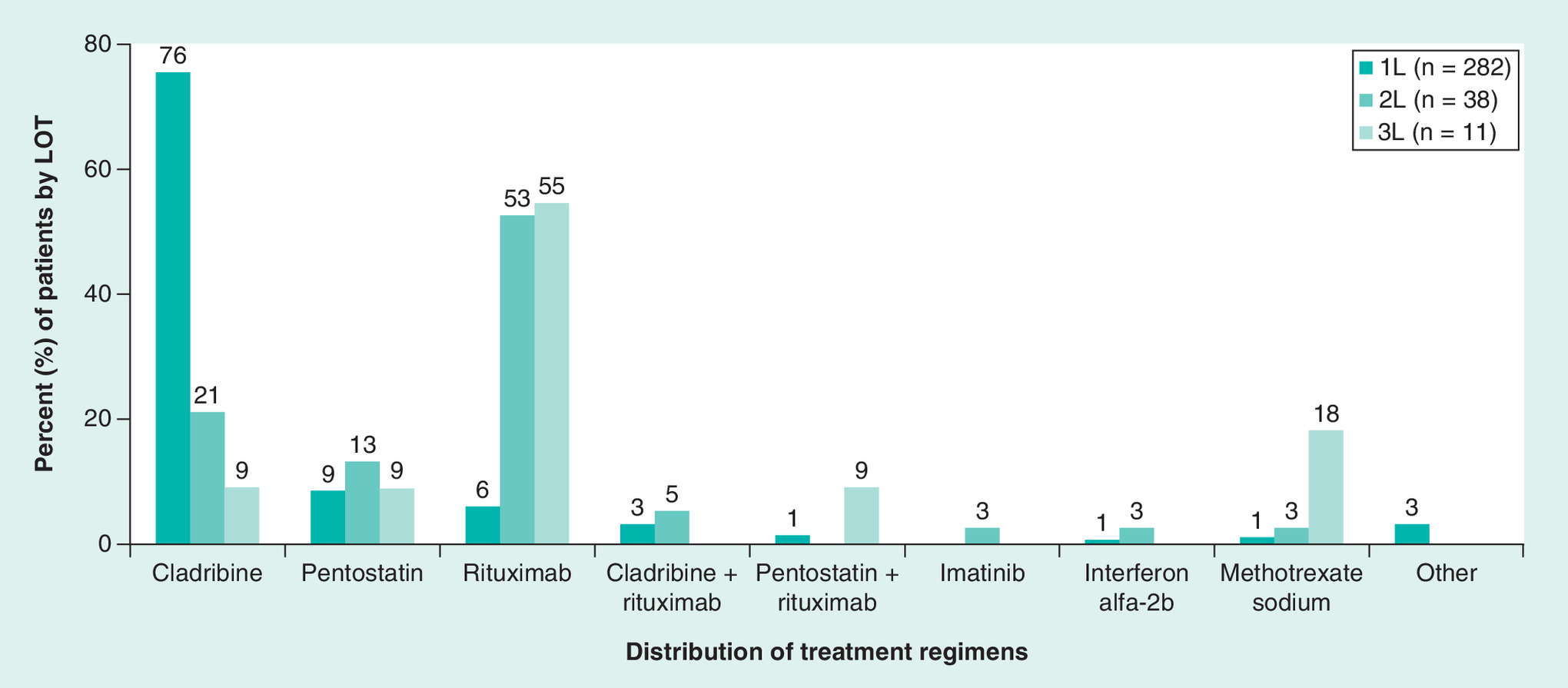
Figure 2. Treatment regimens used by line of therapy.
1L: First line; 2L: Second line; 3L: Third line; LOT: Line of therapy.
Among patients receiving 1L cladribine (n = 213), mean duration of therapy was 7.3 (16.2) days (Supplementary Table 2). Patients most often had a duration of 1 day (43.2%), followed by 5 days (38.5%) and then 36 days (4.2%; data not shown). Patients had a mean of 3.4 (3.0) days of cladribine administration over 1L duration (Supplementary Table 2). The majority (88.7%) of 1L cladribine patients did not receive any HCL therapy following end of 1L therapy, while 6.6% went on to receive rituximab in 2L, and 2.8% were retreated with cladribine. See Figure 3 for treatment pathways/sequences in 1L and 2L. Given the extended study period, 2L treatments were stratified by year of 1L treatment initiation for 1L cladribine patients (Supplementary Figure 1). Following the end of 1L cladribine therapy, the proportion that did not receive any HCL therapy, as well as 2L therapies utilized, remained fairly consistent over time.
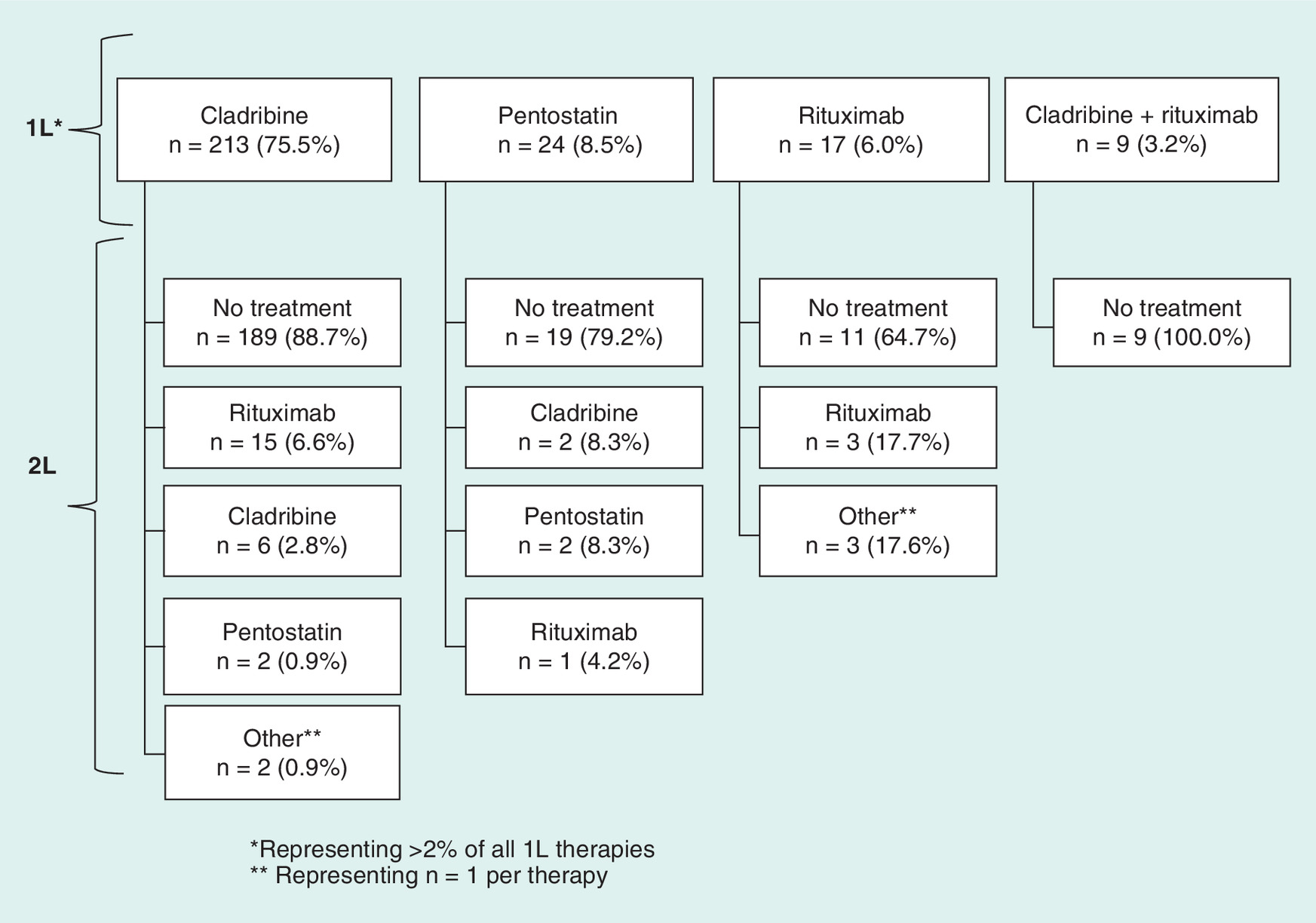
Figure 3. Treatment pathways.
1L: First line; 2L: Second Line.
Among patients receiving 2L therapy (n = 38), patients initiated 2L therapy in a mean of 16.0 (16.7) months from the date of HCL diagnosis, and in a mean of 10.1 (13.5) months from the end of 1L therapy (Supplementary Table 2). The majority (76.3% [29/38]) of patients receiving 2L therapy had refractory disease to 1L while the remaining 23.7% (9/38) had relapsed following 1L (data not shown). The mean duration of 2L therapy was 53.7 (70.9) days (Supplementary Table 2). Almost all patients (94.7%) initiated a single therapy regimen in 2L, with rituximab used by the majority (52.6%). Next, most frequent were cladribine (21.1%) and pentostatin (13.2%). Among patients receiving 2L rituximab (n = 20), patients had a mean of 4.9 (2.1) days of rituximab administration over 2L duration, which lasted a mean of 69.4 (78.0) days (Supplementary Table 2). Among the 11 patients receiving 3L therapy, rituximab (54.5%) was most commonly used, followed by methotrexate sodium (18.2%).
HCRU and costs
Over the variable follow-up, 43.3% of patients had ≥1 hospitalization with a mean of 0.8 (1.4) hospitalizations per patient. Patients had a mean of 4.5 (7.0) outpatient surgical visits, 34.0 (41.1) outpatient physician office visits and 118.2 (114.5) lab tests and other services per patient.
Patients had a mean of 3.1 (6.2) HCL-related drug injections. When HCRU over the variable follow-up was annualized, patients had a mean of 0.8 (6.9) hospitalizations, 2.3 (7.3) outpatient surgical visits, 17.7 (53.4) outpatient physician office visits and 62.4 (99.2) lab tests and other services per patient. Annualized, patients had a mean of 1.9 (5.7) HCL-related injections. See Table 3 for HCRU over the follow-up.
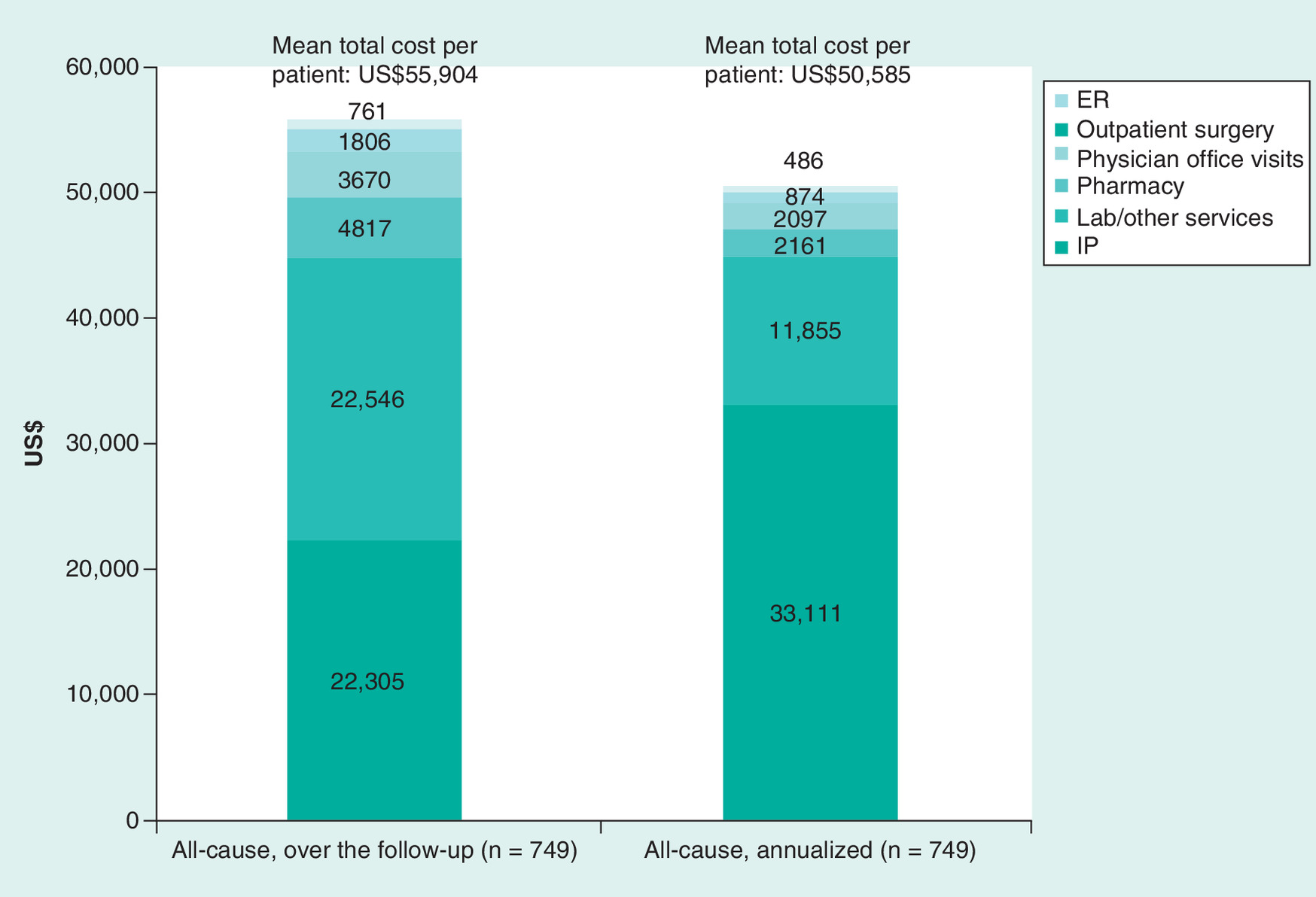
Over the variable follow-up period, mean all-cause cost per patient was US$55,904 (US$91,341) with median costs of US$29,040. Costs for outpatient care comprised 50.1% of total costs, while 39.9% were due to in-patient costs. Mean HCL-related cost per patient was US$31,234 (US$61,750) with median costs of US$10,677, and mean HCL-related costs represented 55.9% of mean all-cause costs (data not shown). Mean total cost of HCL-related drug injections was US$5530 (US$17,055) per patient, representing 9.9% of total costs (data not shown). When healthcare costs over the variable follow-up were annualized, the mean all-cause cost per patient was US$50,585 (US$430,041) with median costs of US$12,989. It is important to note that costly in-patient stays (particularly those resulting in mortality) contributed to the high average and SD. In-patient care represented the majority (65.5%) of total costs, while 29.3% were due to outpatient care. The mean annualized HCL-related cost per patient was US$38,588 (US$404,600) with median costs of US$4784, and mean HCL-related costs represented 76.3% of mean annualized all-cause costs (data not shown). Annualized, mean total cost of HCL-related drug injections was US$2624 (US$8024) per patient representing 5.2% of total costs (data not shown). See Figure 4 for healthcare costs over the follow-up.
Discussion
This observational retrospective study utilized administrative claims data to identify a large cohort of newly diagnosed HCL patients in the USA, to descriptively assess patient characteristics and HCRU and costs, and to evaluate treatment patterns by LOT from a real-world perspective.
Patient characteristics were consistent with observations from other studies. The majority of patients were male (77%) with mean/median age of diagnosis 55.6/56.0 years, respectively. A SEER-17 database analysis in the USA described 3360 patients diagnosed with HCL between 1978 and 2008 [17]. The majority (78%) was male and among patients diagnosed from 2000 to 2008 (closest to the time period of our analysis), mean/median age of diagnosis was 57/56 years, respectively. The SEER-18 database was used to describe 3033 patients diagnosed with HCL between 1978 and 2011 [16]. Median age at diagnosis was 56 years and 78% were male. However, the SEER database analyses are limited as they cannot capture specific treatment modalities.
The majority of 1L patients in our study received cladribine (76%) while 9% received pentostatin. NCCN guidelines do not recommend one PNA over the other; however, in general, cladribine should be avoided in patients with an active life-threatening infection or chronic infections [4]. It appears treating physicians may have a preference for the use of cladribine, corroborating observations of other physicians, related to the relative ease of use and administration convenience of cladribine compared with pentostatin [2,12]. This perhaps suggests the need for revisiting of clinical guidelines or larger studies comparing long-term outcomes between the two PNAs, although given the rarity of HCL a randomized trial may not be feasible. A study describing 88 young HCL patients treated with cladribine at the Scripps Clinic (CA, USA) found that single courses of cladribine induce high rates of complete and durable responses in the majority of young HCL patients [19]. The authors conclude that cladribine remains an excellent therapeutic approach for HCL patients, recommended regardless of age. While real-world treatment patterns have not been described in the USA among a large sample, a few large studies conducted in France, Spain and Italy among patients with HCL also suggest cladribine to be used by a majority [13–15]. A UK analysis at a single institute (1986–2010) found contradictory results, and pentostatin was used to treat the majority (78%) [7]. It is important to keep in mind with any comparisons the different time periods and follow-up periods, with varying recommended treatment modalities, as well as country-specific treatment guidelines and/or reimbursement policies which may impact prescribing and utilization patterns.
In our analysis, only 38% of patients were identified as initiating 1L therapy following diagnosis, in a mean of 4.4 months following diagnosis. Only 5% of the overall sample was identified as initiating 2L therapy (13% of patients who received 1L therapy), in a mean of 16 months following diagnosis, suggesting 1L therapy was effective in providing a lasting response. However, these findings are also likely related to the lack of long-term follow-up for our sample (on average 32 months of follow-up from diagnosis) as other studies have demonstrated long-lasting duration of response and remission-free periods. Cornet et al. reported on a retrospective survey of physicians with data obtained from 487 patients with HCL from 36 clinical centers in France [14]. Overall median follow-up was 60 months, and only 23 (5%) patients were identified as receiving no treatment, among whom, median follow-up was 32 months, suggesting the importance of adequate follow-up time to capture HCL therapy. In particular, physicians may use a ‘watch and wait’ approach among asymptomatic HCL patients in accordance with commonly accepted treatment guidelines [4]. Related to this, we found that among patients receiving 1L therapy, a number of clinical characteristics measured in the 6 months prior to 1L therapy suggested worsening disease and higher cost burden as compared with the 6 months prior to HCL diagnosis. Cornet et al. found that median relapse-free survival was similar between 1L cladribine and 1L pentostatin (median 164 months and 159 months, respectively) [14]. In the UK, Else et al. found an overall median relapse-free survival of 16 years following 1L [8]. In a study in Italy, 44% of 1L patients relapsed, and of these patients, median duration of response was 2.7 years following 1L therapy [13].
To the author's knowledge, this is the first study to evaluate HCRU and costs among HCL patients in the USA. Our findings indicate that HCL patients have considerable HCRU and costs. Mean annualized healthcare costs postdiagnosis were US$50,585, approximately 9-times higher than the average costs in the 6 months prior to diagnosis (US$5858). Median annualized healthcare costs were US$12,989, approximately 5-times higher than the average costs in the 6 months prior to diagnosis (US$2953). Medical care, and in-patient care in particular, was an important cost driver. Mean annualized HCL-related costs represented 76.3% of mean annualized all-cause costs.
It is important to note the limitations inherent to this study with respect to the data source. Our study relied upon administrative claims data, which are collected for payment purposes and not for clinical research, and which lack clinical detail and are subject to potential coding errors. Due to the lack of lab results or medical records, we were unable to confirm certain baseline comorbidities (e.g., aplastic anemia), or evaluate clinical outcomes or understand reasons for discontinuation or switch of HCL therapy (outcomes such as treatment response, treatment relapse or treatment refractory, or experience of adverse events). We therefore developed our LOT definitions based solely on therapy claims supported by a review of the literature and exploratory data analyses. In addition, while these claims data are representative of commercially insured beneficiaries, the results of this analysis may not be generalizable to patients who are uninsured or covered by other payers, such as the elderly population which is typically insured by Medicare. However, no other studies in the USA have been identified which have described treatment utilization patterns among a large sample of HCL patients. Additionally, while patient mortality is identified in the hospital setting, it is not captured in other settings of care. It is another limitation that the database does not capture in-patient administered drugs or clinical trial entry/use of clinical trial drugs.
A few limitations are inherent due to the study design. We required continuous health plan enrollment for 180 days preindex and ≥90 days postindex, in order to eliminate the impact of insurance coverage interruptions, to help ensure a newly diagnosed HCL population with no secondary malignancies, and to provide adequate follow-up time to investigate treatment patterns. However, patients who died <90 postindex were retained. It is possible that our sample was not restricted to only newly diagnosed HCL patients without any other malignancy, as we utilized only a fixed 180 day preindex period to require patients to be free of any HCL or other cancer diagnosis. Given the potential for a long-lasting duration of response and remission with therapy, it is possible that selected patients had diagnosed HCL and were asymptomatic and treatment free in the 180 days preindex. Related to this, it is also possible that patients were treated for HCL prior to the 180 days preindex, and any observed 1L treatment in our study was actually a later LOT. However, this 180 day preindex period was chosen to best maximize the patient sample. Finally, our small sample sizes in 2L and 3L limit interpretation.
Conclusion
HCL treatment pathways and outcomes in the real-world setting are not well understood, particularly among large sample sizes and in the USA. This study provides real-world data on HCL patient characteristics, treatment patterns and HCRU and costs in the USA using a large and nationally representative administrative claims database. With a mean follow-up of 32 months following HCL diagnosis, only 38% of patients initiated HCL therapy over the available follow-up. Among patients initiating 1L therapy, 76% were treated with cladribine, of whom only 11% went on to receive 2L therapy. First-line therapy duration lasted approximately 1 month, and appeared to provide a long-lasting response. Patients also had considerable HCRU and costs.
| Characteristic | Overall (n = 749) | 1L (n = 282) | 2L (n = 38) | No HCL therapy (n = 467) |
|---|---|---|---|---|
| Age (years): | ||||
| – Mean | 55.6 | 53.8 | 53.9 | 56.8 |
| – SD | 10 | 9.8 | 12.1 | 9.9 |
| – Median | 56 | 55 | 55 | 57 |
| Age group (%): | ||||
| – 18–34 years | 2.5 | 3.9 | 7.9 | 1.7 |
| – 35–44 years | 10.5 | 12.4 | 13.2 | 9.4 |
| – 45–54 years | 29.6 | 33.3 | 28.9 | 27.4 |
| – 55–64 years | 43.8 | 41.8 | 36.8 | 45.0 |
| – 65–74 years | 8.4 | 4.6 | 5.3 | 10.7 |
| – 75+ years | 5.1 | 3.9 | 7.9 | 5.8 |
| Gender (%): | ||||
| Male | 77.4 | 80.9 | 84.2 | 75.4 |
| Female | 22.6 | 19.1 | 15.8 | 24.6 |
| Geographic region (%): | ||||
| – Northeast | 21.9 | 21.6 | 21.1 | 22.1 |
| – Midwest | 37.5 | 39.4 | 34.2 | 36.4 |
| – South | 27.4 | 27.0 | 34.2 | 27.6 |
| – West | 13.2 | 12.1 | 10.5 | 13.9 |
| Health plan type (%): | ||||
| – PPO | 77.3 | 77.3 | 76.3 | 77.3 |
| – HMO | 10.4 | 10.6 | 18.4 | 10.3 |
| – Other | 12.3 | 12.1 | 5.3 | 12.4 |
| Payer type (%): | ||||
| – Commercial | 64.1 | 62.8 | 68.4 | 64.9 |
| – Medicaid | 0.1 | 0.4 | 0.0 | 0.0 |
| – Medicare risk | 1.5 | 1.4 | 0.0 | 1.5 |
| – Self insured | 34.0 | 35.5 | 31.6 | 33.2 |
| – Unknown | 0.3 | 0.0 | 0.0 | 0.4 |
| Duration of follow-up (months) from index date: | ||||
| – Mean | 32.3 | 33.8 | 39.9 | 31.3 |
| – SD | 22.0 | 22.3 | 22.6 | 21.8 |
| – Median | 27.4 | 28.4 | 37.3 | 26.9 |
1L: First line; 2L: Second line; HCL: Hairy cell leukemia; HMO: Health maintenance organization; PPO: Preferred provider organization; SD: Standard deviation.
| Characteristic | Overall (n = 749) | 1L (n = 282) | 2L (n = 38) | No HCL therapy (n = 467) |
|---|---|---|---|---|
| Physician specialty associated with the index diagnosis: | ||||
| – Hem/Onc | 28.6 | 30.1 | 36.8 | 27.6 |
| – Primary | 18.7 | 14.2 | 10.5 | 21.4 |
| – Hospitalist | 17.4 | 19.5 | 23.7 | 16.1 |
| – Hematology | 6.7 | 6.0 | 0.0 | 7.1 |
| – Unknown | 6.7 | 7.8 | 2.6 | 6.0 |
| – Other | 22.0 | 22.3 | 26.3 | 21.8 |
| CCI score: | ||||
| – Mean | 0.8 | 1 | 1 | 0.8 |
| – SD | 1.1 | 1.1 | 1.1 | 1.2 |
| – Median | 0 | 0 | 1 | 0 |
| CCI score distribution (%): | ||||
| – 0 | 57.8 | 50.4 | 44.7 | 62.3 |
| – 1 | 11.1 | 11.7 | 15.8 | 10.7 |
| – 2 | 23.6 | 29.4 | 34.2 | 20.1 |
| – 3+ | 7.5 | 8.5 | 5.3 | 6.9 |
| Frequent (>10%) relevant comorbidities of interest (%): | ||||
| – Abdominal pain | 11.9 | 13.5 | 10.5 | 10.9 |
| – Adenopathy | 3.5 | 5.7 | 2.6 | 2.1 |
| – Anemia | 19.4 | 31.2 | 18.4 | 12.2 |
| – Aplastic anemia | 21.5 | 35.8 | 18.4 | 12.8 |
| – Diabetes | 10.9 | 11.0 | 13.2 | 10.9 |
| – Fatigue | 11.5 | 19.5 | 15.8 | 6.6 |
| – Hypertension | 24.2 | 26.2 | 28.9 | 22.9 |
| – Mild liver disease | 2.3 | 2.8 | 0.0 | 1.9 |
| – AMI | 6.9 | 7.1 | 7.9 | 6.9 |
| – Splenomegaly | 14.2 | 20.9 | 18.4 | 10.1 |
| All-cause healthcare costs: | ||||
| – Mean (US$) | 5858 | 6635 | 4370 | 5389 |
| – SD (US$) | 13,836 | 7246 | 4429 | 16,584 |
| – Median (US$) | 2593 | 4627 | 2590 | 1671 |
1L: First line; 2L: Second line; AMI: Acute myocardial infarction; CCI: Charlson Comorbidity Index; HCL: Hairy cell leukemia; Hem/Onc: Hematology/Oncology; Primary: General practitioner/family medicine/internal medicine; SD: Standard deviation.
| Resource use per patient | Over the available follow-up (n = 749) | Annualized (n = 749) | ||
|---|---|---|---|---|
| mean | SD | mean | SD | |
| Number of outpatient prescription fills | 48.9 | 71.3 | 20.1 | 23.5 |
| In-patient visits | ||||
| Number of hospitalizations | 0.8 | 1.4 | 0.8 | 6.9 |
| Average number of hospital days | 5.8 | 13.2 | 6.1 | 50.2 |
| Length of in-patient stay (days) | 3.2 | 6.2 | ||
| Number of ER visits | 0.9 | 3.0 | 0.7 | 6.8 |
| Outpatient care | ||||
| Number of outpatient office visits | 34.0 | 41.1 | 17.7 | 53.4 |
| – Number of primary care visits | 8.4 | 11.6 | 4.4 | 20.5 |
| – Number of hematology/oncology visits | 4.8 | 8.0 | 2.6 | 6.0 |
| Number of outpatient surgical visits | 4.5 | 7.0 | 2.3 | 7.3 |
| Number of lab tests and other services | 118.2 | 114.5 | 62.4 | 99.2 |
| – Number of HCL-related drug injections | 3.1 | 6.2 | 1.9 | 5.7 |
ER: Emergency room; HCL: Hairy cell leukemia; SD: Standard deviation.
Hairy cell leukemia (HCL) is a rare leukemia; treatment pathways and outcomes in the real-world setting are not well understood, particularly among large sample sizes and in the USA.
Real-world treatment patterns and healthcare utilization and costs for 749 adults newly diagnosed with HCL in the USA were described using a large, nationally representative database.
Over the mean follow-up of 2.7 years following HCL diagnosis, the majority of patients did not receive any HCL therapy.
Only 37.7% of patients (n = 282) initiated first-line (1L) therapy during the available follow-up in a mean (standard deviation) of 4.4 (9.8) months following diagnosis; the majority (75.5%) received cladribine with mean duration of therapy of 7.3 (16.2) days.
First-line patients had mean follow-up of 29.5 (21.0) months following 1L initiation, over which, the majority did not receive subsequent therapy; 1L therapy appeared to provide a long-lasting response.
Thirty-eight patients (5.1%) received second-line treatment, with rituximab (52.6%) most commonly utilized; 21.1% received cladribine.
Only 11 patients (1.5%) initiated third line.
Over the variable follow-up, mean annualized all-cause costs were US$50,585 (median US$12,989), and in-patient care was an important cost driver.
Mean annualized HCL-related costs were US$38,588 (median US$4784), representing 76.3% of mean annualized all-cause costs.
Larger studies comparing long-term outcomes between HCL therapies are warranted.
Acknowledgements
The authors would like to thank Chun-Lan Chang, formerly Director at QuintilesIMS, for her assistance with the initial study design.
Financial & competing interests disclosure
This study was sponsored by AstraZeneca. A Gaughan and S Karve are employees and shareholders of AstraZeneca which sponsored this study. G Gao is an employee of MedImmune LLC and shareholder of AstraZeneca. At the time of the study, MC Lanasa was an employee of MedImmune LLC and shareholder of AstraZeneca. M DeKoven and V Divino are employed by QuintilesIMS, which received funding from AstraZeneca for this study. KB Knopf received consulting fees from QuintilesIMS for this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical conduct of research
Ethics approval was not required as this was a retrospective analysis of anonymized patient claims records. All data utilized were de-identified, pre-existing and retrospective, with no risk of identifying patients.
Supplementary Material
File (suppl_material.docx)
- Download
- 310.67 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Grever MR, Blachly JS, Andritsos LA. Hairy cell leukemia: update on molecular profiling and therapeutic advances. Blood Rev. 28, 197–203 (2014).
2.
Grever MR. How I treat hairy cell leukemia. Blood 115, 21–28 (2010).
3.
Maevis V, Mey U, Schmidt-Wolf G, Schmidt-Wolf IG. Hairy cell leukemia: short review, today's recommendations and outlook. Blood Cancer J. 4, e184 (2014).
4.
NCCN Clinical Practice Guidelines in Oncology: Hairy Cell Leukemia. National Comprenhensive Cancer Network (2017). www.nccn.org/professionals/physician_gls/f_guidelines.asp
•• Recommended National Comprehensive Cancer Network treatment guidelines for hairy cell leukemia (HCL) in the USA.
5.
Robak T, Matutes E, Catovsky D, Zinzani PL, Buske C. ESMO Guidelines Committee. Hairy cell leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 26(Suppl. 5), v100–v107 (2015).
6.
Grever MR, Abdel-Wahab O, Andritsos LA et al. Consensus guidelines for the diagnosis and management of patients with classic hairy cell leukemia. Blood 129, 553–560 (2017).
7.
Dearden CE, Else M, Catovsky D. Long-term results for pentostatin and cladribine treatment of hairy cell leukemia. Leuk. Lymphoma 52, 21–24 (2011).
•• A long-term retrospective, single institute study in the UK with a median follow-up of 16 years found no significant difference in outcome between pentostatin and cladribine either at first or subsequent lines of therapy. Overall, the complete response rate was 81% and the median disease-free survival was 16 years.
8.
Else M, Dearden CE, Matutes E et al. Long-term follow-up of 233 patients with hairy cell leukaemia, treated initially with pentostatin or cladribine, at a median of 16 years from diagnosis. Br. J. Haematol. 145, 733–740 (2009).
9.
Jain P, Pemmaraju N, Ravandi F. Update on the biology and treatment options for hairy cell leukemia. Curr. Treat. Options Oncol. 15, 187–209 (2014).
10.
Maloisel F, Benboubker L, Gardembas M et al. Long-term outcome with pentostatin treatment in hairy cell leukemia patients. A French retrospective study of 238 patients. Leukemia 17, 45–51 (2003).
11.
Saven A, Burian C, Koziol JA, Piro LD. Long-term follow-up of patients with hairy cell leukemia after cladribine treatment. Blood 92, 1918–1926 (1998).
12.
Naik RR, Saven A. My treatment approach to hairy cell leukemia. Mayo Clin. Proc. 87, 67–76 (2012).
13.
Zinzani PL, Pellegrini C, Stefoni V et al. Hairy cell leukemia: evaluation of the long-term outcome in 121 patients. Cancer 116, 4788–4792 (2010).
14.
Cornet E, Tomowiak C, Tanguy-Schmidt A et al. Long-term follow-up and second malignancies in 487 patients with hairy cell leukaemia. Br. J. Haematol. 166, 390–400 (2014).
•• Retrospective survey of physicians in France that found over a median follow-up of 60 months, only 5% of patients had received no treatment. While the majority of patients received cladribine in first-line (1L), median relapse-free survival was similar between 1L cladribine and 1L pentostatin.
15.
López Rubio M, Da Silva C, Loscertales J et al. Hairy cell leukemia treated initially with purine analogs: a retrospective study of 107 patients from the Spanish Cooperative Group on Chronic Lymphocytic Leukemia (GELLC). Leuk. Lymphoma 55, 1007–1012 (2014).
16.
Giri S, Shrestha R, Pathak R, Bhatt VR. Racial differences in the overall survival of hairy cell leukemia in the United States: a population-based analysis of the Surveillance, Epidemiology, and End Results database. Clin. Lymphoma Myeloma Leuk. 15, 484–488 (2015).
• A US analysis using the Surveillance, Epidemiology, and End Results 17 database found significantly worse overall survival for African-Americans versus other races.
17.
Chandran R, Gardiner SK, Smith SD, Spurgeon SE. Improved survival in hairy cell leukaemia over three decades: a SEER database analysis of prognostic factors. Br. J. Haematol. 163, 407–409 (2013).
• A US analysis using the Surveillance, Epidemiology, and End Results 18 database found that the survival of HCL patients has improved over the last three decades with a significant benefit being seen after 1984. Increasing age and African-American race are associated with lower survival.
18.
Anderson LA, Engels EA. Autoimmune conditions and hairy cell leukemia: an exploratory case-control study. J. Hematol. Oncol. 3, 35 (2010).
19.
Rosenberg JD, Burian C, Waalen J, Saven A. Clinical characteristics and long-term outcome of young hairy cell leukemia patients treated with cladribine: a single-institution series. Blood 123, 177–183 (2014).
•• A retrospective single-institution study in the USA that found single courses of cladribine-induced high rates of complete and durable responses in young HCL patients.
20.
Chastek B, Kulakodlu M, Valluri S, Seal B. Impact of metastatic colorectal cancer stage and number of treatment courses on patient health care costs and utilization. Postgrad. Med. 125, 73–82 (2013).
21.
Song X, Zhao Z, Barber B, Gregory C, Wang PF, Long SR. Treatment patterns and metastasectomy among mCRC patients receiving chemotherapy and biologics. Curr. Med. Res. Opin. 27, 123–130 (2011).
22.
Hess GP, Wang PF, Quach D, Barber B, Zhao Z. Systemic therapy for metastatic colorectal cancer: patterns of chemotherapy and biologic therapy use in US medical oncology practice. J. Oncol. Pract. 6, 301–307 (2010).
Information & Authors
Information
Published In
Copyright
© AstraZeneca.
History
Published online: 9 May 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Characteristics and treatment patterns among US patients with hairy cell leukemia: a retrospective claims analysis. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0014
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Xavier Troussard, Elsa Maître, Jérôme Paillassa, Hairy cell leukemia 2024: Update on diagnosis, risk‐stratification, and treatment—Annual updates in hematological malignancies, American Journal of Hematology, 10.1002/ajh.27240, 99, 4, (679-696), (2024).
- Tuba ERSAL, Fahir ÖZKALEMKAŞ, Vildan OZKOCAMAN, İbrahim Ethem PINAR, Cumali YALÇIN, Bedrettin ORHAN, Ömer CANDAR, Sinem ÇUBUKÇU, Tuba GÜLLÜ KOCA, Rıdvan ALİ, Subcutaneous and Intravenous Cladribine Treatment of Hairy Cell Leukemia Patients: Do We Still Need Intravenous Cladribine?, Turkish Journal of Internal Medicine, 10.46310/tjim.1239905, 5, 2, (109-116), (2023).
- Xavier Troussard, Elsa Maître, Edouard Cornet, Hairy cell leukemia 2022: Update on diagnosis, risk‐stratification, and treatment, American Journal of Hematology, 10.1002/ajh.26390, 97, 2, (226-236), (2021).
- Gustavo Alves, Introduction, Chemotherapy and Pharmacology for Leukemia in Pregnancy, 10.1007/978-3-030-54058-6_1, (1-21), (2020).
- Narendranath Epperla, Melissa Pavilack, Temitope Olufade, Richa Bashyal, Jieni Li, Shaum M. Kabadi, Huseyin Yuce, Leslie Andritsos, Adverse event rates and economic burden associated with purine nucleoside analogs in patients with hairy cell leukemia: a US population-retrospective claims analysis, Orphanet Journal of Rare Diseases, 10.1186/s13023-020-1325-9, 15, 1, (2020).
- Elsa Maitre, Edouard Cornet, Xavier Troussard, Hairy cell leukemia: 2020 update on diagnosis, risk stratification, and treatment, American Journal of Hematology, 10.1002/ajh.25653, 94, 12, (1413-1422), (2019).
- Carl Samuelsen, Jonathan Lim, Amanda Golembesky, Sulena Shrestha, Li Wang, Ingolf Griebsch, Healthcare resource utilization and costs associated with patients prescribed afatinib or erlotinib as first-line therapy for EGFR mutation-positive NSCLC in the United States, Journal of Medical Economics, 10.1080/13696998.2019.1645681, 23, 1, (48-53), (2019).
- Wellington F. da Silva, Abel Costa Neto, Lidiane Inês da Rosa, Isabela Assis de Siqueira, Guilherme Duffles Amarante, Elvira D.R.P. Velloso, Eduardo Magalhães Rego, Vanderson Rocha, Valeria Buccheri, Outcomes and second neoplasms in hairy cell leukemia: A retrospective cohort, Leukemia Research, 10.1016/j.leukres.2019.06.001, 83, (106165), (2019).
- Jonathan Lim, Carl Samuelsen, Amanda Golembesky, Sulena Shrestha, Li Wang, Ingolf Griebsch, Duration of treatment among patients prescribed afatinib or erlotinib as first-line therapy for EGFR mutation-positive non-small-cell lung cancer in the USA, Future Oncology, 10.2217/fon-2019-0052, 15, 13, (1493-1504), (2019).
- Robert J. Kreitman, Claire Dearden, Pier Luigi Zinzani, Julio Delgado, Lionel Karlin, Tadeusz Robak, Douglas E. Gladstone, Philipp le Coutre, Sascha Dietrich, Mirjana Gotic, Loree Larratt, Fritz Offner, Gary Schiller, Ronan Swords, Larry Bacon, Monica Bocchia, Krimo Bouabdallah, Dimitri A. Breems, Agostino Cortelezzi, Shira Dinner, Michael Doubek, Bjorn Tore Gjertsen, Marco Gobbi, Andrzej Hellmann, Stephane Lepretre, Frederic Maloisel, Farhad Ravandi, Philippe Rousselot, Mathias Rummel, Tanya Siddiqi, Tamar Tadmor, Xavier Troussard, Cecilia Arana Yi, Giuseppe Saglio, Gail J. Roboz, Kemal Balic, Nathan Standifer, Peng He, Shannon Marshall, Wyndham Wilson, Ira Pastan, Nai-Shun Yao, Francis Giles, Moxetumomab pasudotox in relapsed/refractory hairy cell leukemia, Leukemia, 10.1038/s41375-018-0210-1, 32, 8, (1768-1777), (2018).