Healthcare resource utilization and costs in patients with multiple myeloma administered ciltacabtagene autoleucel in outpatient versus inpatient settings after one to three prior lines of therapy
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: Ciltacabtagene autoleucel (cilta-cel) was approved for patients with relapsed or refractory multiple myeloma who received 1–3 prior lines of therapy in April 2024. Although traditionally administered inpatient (IP), there is an increasing trend in outpatient (OP) cilta-cel administration. However, few studies have quantified the healthcare resource utilization (HCRU) and cost implications of OP versus IP administration in clinical practice. Aim: To compare HCRU and costs following OP versus IP administration of cilta-cel among patients with relapsed or refractory multiple myeloma after 1–3 prior lines of therapy. Materials & methods: This retrospective observational study used the Loopback Analytics electronic medical records database (28 February 2017 to 30 June 2025). We classified patients into OP or IP cohorts. All-cause and multiple myeloma-related HCRU and per-patient-per-month imputed costs were compared over 30 and 90 days post-infusion. Results: There were 99 patients included (OP: 37; IP: 62). In the first 30 days post-infusion, 40.5% of the OP cohort did not require IP admission. Compared with the IP cohort, the OP cohort had significantly lower all-cause IP days (adjusted incidence rate ratio: 0.31; p < 0.001) and significantly lower all-cause IP-related imputed costs (adjusted mean difference: -$39,786; p < 0.001). Results were consistent over the first 90 days post-infusion and for multiple myeloma related HCRU and costs. Overall, OP administration was associated with an estimated cost savings of approximately $40,000 and $53,000 per patient in the first 30 and 90 days post-infusion, respectively. Conclusion: OP administration of cilta-cel was associated with significantly lower IP resource utilization and imputed costs over the first 3 months post-infusion relative to IP administration, supporting the potential economic value and adoption of OP cilta-cel delivery.
Plain language summary
What is this article about?
Ciltacabtagene autoleucel (cilta-cel) is a therapy for patients with multiple myeloma (MM) after previous treatment stops working. It can be given in a single-day outpatient (OP) setting or an inpatient (IP) setting, requiring hospitalization. We explored if administering cilta-cel in the OP versus IP setting reduces healthcare resource use and costs.
What methodology was used in this study?
This was an observational study using electronic medical records (EMR) data from US hospitals. Adults with MM who received cilta-cel after 1–3 prior lines of therapy were identified and classified into OP or IP administration groups. Healthcare resource use and associated costs were compared during the first 3 months following treatment between groups. Since the EMR data do not capture cost information, costs associated with healthcare resource use were imputed using published cost inputs on patients with MM.
What were the results?
We identified 99 patients treated with cilta-cel, with 37 in the OP setting and 62 in the IP setting. OP-treated patients experienced fewer hospitalized days per month compared with IP-treated patients. OP administration was associated with lower monthly total imputed costs driven primarily by reduced hospital days. Overall, OP cilta-cel administration led to an estimated cost savings over IP administration of approximately $40,000 and $53,000 per patient in the first 30 and 90 days following treatment.
Why are these results important?
These findings support the potential economic value of OP administration and highlight that its adoption may improve feasibility of and expand access to treatment.
Ciltacabtagene autoleucel (cilta-cel) is a B-cell maturation antigen-directed chimeric antigen receptor T-cell (CAR-T) therapy that has demonstrated deep and durable responses among patients with relapsed or refractory multiple myeloma (RRMM) [1–3]. The pivotal CARTITUDE-1 and CARTITUDE-4 trials established the clinical efficacy and safety of cilta-cel in patients who had received ≥4 prior lines of therapy (LOT) and those who had received 1–3 prior LOT, respectively. Findings from these trials led to the US FDA approvals of cilta-cel for patients with RRMM after ≥4 prior LOT in February 2022 and after ≥1 prior LOT in April 2024 [4]. Specifically, in CARTITUDE-4, which enrolled patients with 1–3 prior LOT, cilta-cel demonstrated superior outcomes compared with standard of care, with 30-month progression-free survival (PFS) and overall survival (OS) rates of 59% and 76%, respectively, versus 26% and 64% [3].
In clinical trials, cilta-cel was primarily administered in the inpatient (IP) setting to allow for close monitoring of acute toxicities such as cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) [1,2]. However, growing clinical experience has indicated that these events are typically predictable and manageable, with most CRS and ICANS events occurring within the first week post-infusion and presenting as low-grade in severity [5,6]. Indeed, in the pivotal trials, the pooled median time to onset was 7 days (range: 1–23) for CRS and 8 days (range: 1–28) for ICANS [7]. The pooled incidences of any-grade events were 84% for CRS and 13% for ICANS, and of grade ≥3 events were 4% and 2%, respectively [7]. Coupled with improvements in institutional infrastructure for CAR-T monitoring, this has spurred an increasing trend toward outpatient (OP) administration of cilta-cel [8,9]. Consequently, several institutions have implemented OP CAR-T delivery models supported by standardized protocols and close monitoring capabilities [10,11].
Early real-world evidence has reported that OP cilta-cel administration in clinical practice may achieve comparable safety and effectiveness outcomes compared with IP administration, while reducing hospitalization duration and overall healthcare resource utilization (HCRU) [11,12]. Moreover, pooled analyses of costs from clinical trials of CAR-T therapies across hematologic malignancies suggest that OP delivery is associated with significantly lower costs in the first 6 months post-infusion compared with IP ($36,702 vs $89,535), primarily driven by shorter length of hospitalization, without compromising clinical outcomes [13]. Given that selection of OP versus IP CAR-T administration is multifactorial, reflecting institutional readiness, patient suitability, geographic proximity, caregiver support, logistical considerations, and clinician preference, observed differences may in part reflect underlying selection factors [14]. Important gaps remain, as real-world evidence quantifying the HCRU and cost implications of OP versus IP cilta-cel administration is limited, particularly in patients receiving cilta-cel after 1–3 prior LOT.
Given the increasing feasibility and adoption of OP CAR-T administration, understanding the value of OP delivery is critical to inform value-based care and clinical decision-making. Therefore, this study aimed to compare HCRU and costs following OP versus IP administration of cilta-cel among patients with RRMM who received 1–3 prior LOT.
Materials & methods
Data source
This retrospective study used structured electronic medical records (EMR) from the Loopback Analytics database, covering the period from 28 February 2017 to 30 June 2025. Loopback Analytics is a multisource EMR database comprising data from both community and academic institutions, including over 800 care sites and over 90 academic and community health system partners across more than 40 US states, including National Comprehensive Cancer Network members and National Cancer Institute designated sites. The database included detailed information on patient demographics, clinical encounters, medication prescribing and administration, laboratory test results, procedures, and provider details. These data captured care delivered within the network of participating institutions and did not reflect services received outside of the network. Finally, direct cost data were not available in the database. The study was considered exempt research under 45 CFR § 46.104(d)(4) as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act, specifically, 45 CFR § 164.514. This research study was conducted in accordance with the principles stated in the Declaration of Helsinki.
Study design & population
This was a retrospective observational cohort study of patients with RRMM treated with cilta-cel after 1–3 prior LOT. We defined the index date as the date of cilta-cel infusion, and the baseline period spanned 12 months prior to infusion. We assessed outcomes from the index date until the earliest of 90 days post-infusion, end of clinical activity, death, or end of data availability (30 June 2025; Figure 1).
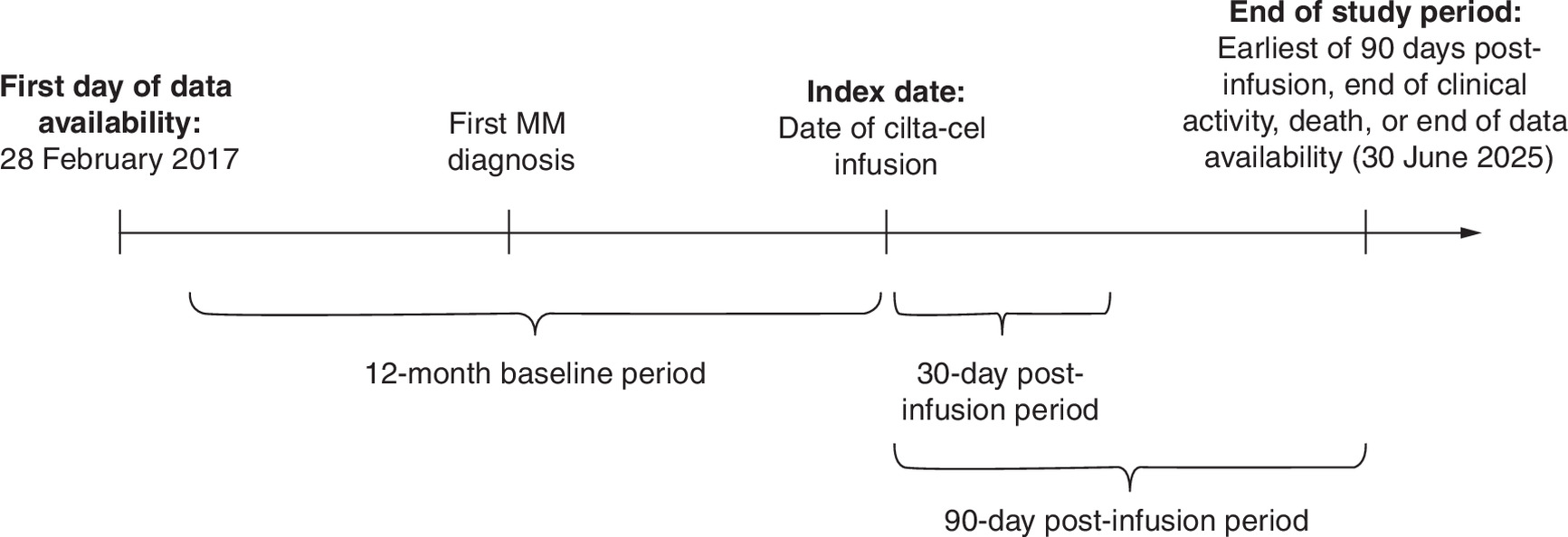
Figure 1. Study design.
cilta-cel: Ciltacabtagene autoleucel; MM: Multiple myeloma.
The study included patients aged ≥18 years who were treated with cilta-cel after 1–3 prior LOT following FDA approval (5 April 2024), with LOT classification done using a previously reported algorithm in RRMM (applicable to EMR data) [12,15], and had at least 12 months of data availability prior to the index date. Patients without lymphodepleting chemotherapy, with clinical trial participation during the cilta-cel LOT, with a diagnosis of amyloidosis prior to the index date, or with CAR-T administration prior to the index date were excluded. Furthermore, only patients with a known setting of cilta-cel administration (i.e., OP or IP) were included and were classified into the OP or IP cohort accordingly (Figure 2).
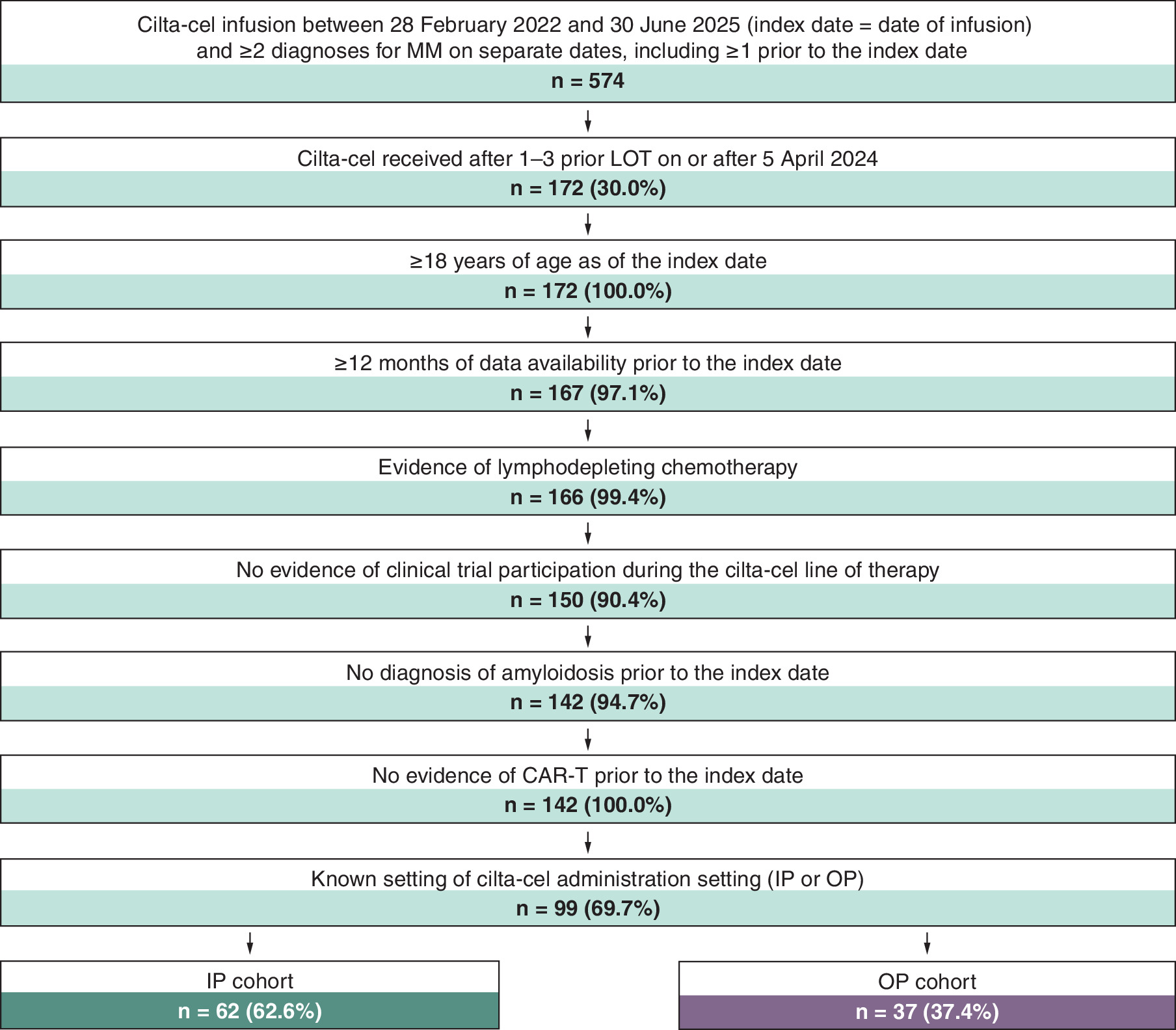
Figure 2. Sample selection.
CAR-T: Chimeric antigen receptor T-cell; cilta-cel: Ciltacabtagene autoleucel; IP: Inpatient; LOT: Line of therapy; MM: Multiple myeloma; OP: Outpatient.
Outcomes
We evaluated all-cause HCRU (i.e., HCRU associated with any diagnosis code) and multiple myeloma (MM)-related HCRU (i.e., HCRU associated with a diagnosis code for MM) as well as associated imputed costs over the 30-day post-infusion period and the 90-day post-infusion period (inclusive of the index date) among the OP and IP cohorts. We considered both all-cause and MM-related HCRU to account for potential inconsistencies in disease-specific coding in EMR data, particularly for treatment-related complications such as CRS or ICANS that may not be explicitly coded with an MM diagnosis code [16]. Hence, assessment of all-cause alongside MM-related HCRU enabled a more comprehensive evaluation of HCRU attributable to both MM and the management of treatment-related complications. The 30-day post-infusion period aligned with standard clinical practice for intensive monitoring, making it the period with the highest expected clinical complexity and resource use [17,18]. In addition, the 90-day post-infusion period reflected the acute post-CAR-T phase during which the majority of clinically significant toxicities (e.g., CRS, ICANS, neurologic toxicities, prolonged cytopenias and severe infections) typically occur, are actively managed, and resolve [19].
In both cohorts, we reported the number of patients with ≥1 IP stay or ≥1 OP visit over the period of evaluation, in addition to the number of IP days and OP days. As cost data were not available in the database, we estimated costs associated with IP and OP days following cilta-cel infusion (i.e., not including cilta-cel drug costs) using published cost inputs. The focus of the analysis was on HCRU and associated costs attributable to the site of infusion rather than the infusion itself. Therefore, cilta-cel acquisition costs were not included, as they were assumed to be equivalent between IP and OP cohorts. The cost analysis therefore focused on encounter-related costs to evaluate differences in HCRU associated with the treatment setting. Drawing on methodologies described in prior research on cost imputation [20–23], we imputed costs based on multiplying the number of observed IP or OP days by literature-derived per-day cost estimates for IP and OP services among patients with MM. Costs were inflated to 2025 US dollars using the medical care component of the Consumer Price Index. Based on this methodology, we attributed a cost of $3943.10 per day to IP days and a cost of $122.51 per day to OP days in 2025 US dollars (Supplementary Table 1). To account for variable follow-up time observed across patients, outcomes were reported per-patient-per-month (PPPM).
Statistical analysis
We used descriptive statistics to summarize patient characteristics evaluated during the baseline period, as well as HCRU and costs evaluated during the 30-day post-infusion period and the 90-day post-infusion period. We assessed balance in patient characteristics between OP and IP cohorts using standardized differences (std. diff.; ≥10% suggesting a potential imbalance) [24]. We fitted multivariate negative binomial regression models to estimate incidence rate ratios (IRRs) for the comparison of the number of IP and OP days between cohorts. Linear regression models were used to estimate mean monthly cost differences associated with IP and OP days between cohorts, as the primary outcome of interest was the adjusted mean difference in costs. To account for the skewed distribution of cost data, nonparametric bootstrap procedures were used to estimate 95% CI and p-values. We adjusted for the following patient characteristics in multivariate analyses based on variables in current literature that may impact HCRU and costs, key differences observed between cohorts, and clinical relevance: age, sex, race, payer type, calendar year of index date, Quan-Charlson Comorbidity Index (CCI) score, frailty index score in the 3 months prior to infusion (evaluated based on 31 conditions used in a published algorithm for patients with MM by Patel et al.) [25], and presence of ≥1 CRAB symptom in the month prior to infusion (i.e., hypercalcemia, renal impairment, anemia, or bone lesions). The 95% CIs and p-values were obtained from non-parametric bootstrap procedures with 500 replications. All statistical analyses were conducted using SAS Enterprise Guide Software version 8.3 (SAS Institute, Cary NC).
Results
Patient characteristics
After applying eligibility criteria, a total of 99 patients with RRMM treated with cilta-cel after 1–3 prior LOT were included in our study. Of them, 37 (37.4%) patients received cilta-cel in an OP setting and 62 (62.6%) in an IP setting. Compared with the IP cohort, patients in the OP cohort were older (OP: 70 years, IP: 67 years, std. diff.: 41.9%). Furthermore, a higher proportion of patients in the OP cohort were female (OP: 54.1%, IP: 45.2%, std. diff.: 17.9%), Black (OP: 8.1%, IP: 4.8%, std. diff.: 13.3%), Medicare beneficiaries (OP: 73.0%, IP: 50.0%, std. diff.: 48.6%), and received cilta-cel in 2025 (OP: 54.1%, IP: 35.5%, std. diff.: 38.0%) relative to the IP cohort (Table 1). With respect to clinical characteristics, patients in the OP cohort had a lower mean CCI (OP: 2.7, IP: 3.2, std. diff.: 32.2%), similar proportion of mild-to-severe frailty in the 3 months prior to infusion (OP: 10.8%, IP: 12.9%, std. diff.: 6.5%), and were more likely to have CRAB symptoms in the month prior to infusion (OP: 45.9%, IP: 29.0%, std. diff.: 35.5%), compared with the IP cohort.
| OP cohort (N = 37) | IP cohort (N = 62) | Std. diff. (%) | |
|---|---|---|---|
| Age at infusion, mean ± SD [median] | 67.9 ± 9.1 [70.0] | 64.2 ± 8.8 [67.0] | 41.9† |
| <50 years, n (%) | 2 (5.4) | 3 (4.8) | 2.6 |
| 50–59 years, n (%) | 4 (10.8) | 16 (25.8) | 39.5† |
| 60–69 years, n (%) | 12 (32.4) | 25 (40.3) | 16.5† |
| ≥70 years, n (%) | 19 (51.4) | 18 (29.0) | 46.8† |
| Sex, n (%) | |||
| Female | 20 (54.1) | 28 (45.2) | 17.9† |
| Male | 17 (45.9) | 34 (54.8) | 17.9† |
| Race, n (%) | |||
| White | 20 (54.1) | 37 (59.7) | 11.4† |
| Black | 3 (8.1) | 3 (4.8) | 13.3† |
| Asian | 1 (2.7) | 2 (3.2) | 3.1 |
| Other | 13 (35.1) | 20 (32.3) | 6.1 |
| Region, n (%) | |||
| West | 14 (37.8) | 46 (74.2) | 78.7† |
| Midwest | 11 (29.7) | 5 (8.1) | 57.6† |
| Northeast | 6 (16.2) | 9 (14.5) | 4.7 |
| South | 6 (16.2) | 2 (3.2) | 44.9† |
| Payer type, n (%) | |||
| Medicare | 27 (73.0) | 31 (50.0) | 48.6† |
| Commercial | 8 (21.6) | 21 (33.9) | 27.6† |
| Medicaid/managed care | 2 (5.4) | 6 (9.7) | 16.2† |
| Other/Unknown | 0 (0.0) | 4 (6.5) | 37.1† |
| Calendar year and quarter of infusion, n (%) | |||
| 2024 | 17 (45.9) | 40 (64.5) | 38.0† |
| Q2 | 5 (13.5) | 12 (19.4) | 15.8† |
| Q3 | 3 (8.1) | 11 (17.7) | 29.0† |
| Q4 | 9 (24.3) | 17 (27.4) | 7.1 |
| 2025 | 20 (54.1) | 22 (35.5) | 38.0† |
| Q1 | 9 (24.3) | 14 (22.6) | 4.1 |
| Q2 | 11 (29.7) | 8 (12.9) | 42.0† |
| Quan-CCI, mean ± SD [median] | 2.7 ± 1.2 [2.0] | 3.2 ± 1.9 [2.0] | 32.2† |
| Frailty index score in the 3 months prior to infusion,§ mean ± SD [median] | 0.10 ± 0.08 [0.10] | 0.07 ± 0.09 [0.03] | 38.4† |
| Nonfrail (0–0.1) | 22 (59.5) | 47 (75.8) | 35.5† |
| Prefrail (0.11–0.20) | 11 (29.7) | 7 (11.3) | 46.9† |
| Mildly to severely frail (>0.20) | 4 (10.8) | 8 (12.9) | 6.5 |
| Mild frailty (0.21–0.30) | 3 (8.1) | 7 (11.3) | 10.8† |
| Moderate frailty (0.31–0.40) | 1 (2.7) | 1 (1.6) | 7.5 |
| Severe frailty (>0.40) | 0 (0.0) | 0 (0.0) | 0.0 |
| CRAB symptoms in the 1 month prior to infusion, n (%) | 17 (45.9) | 18 (29.0) | 35.5† |
| Anemia | 16 (43.2) | 17 (27.4) | 33.6† |
| Bone lesions | 1 (2.7) | 2 (3.2) | 3.1 |
| Hypercalcemia | 1 (2.7) | 1 (1.6) | 7.5 |
| Renal impairment | 0 (0.0) | 1 (1.6) | 18.1† |
†
Std. diff ≥10%.
‡
Demographic characteristics were evaluated at the index date other than insurance type which was evaluated during the 12-month baseline period.
§
Calculated as the sum of frailty index score components divided by 31 as defined by Patel et al.
CCI: Charlson Comorbidity Index; CRAB: Hypercalcemia, renal impairment, anemia, and bone lesions; ICD-10 CM: International Classification of Diseases, 10th Revision, Clinical Modification; IP: Inpatient; MM: Multiple myeloma; OP: Outpatient; SD: Standard deviation; Std. diff: Standardized difference.
Healthcare resource utilization
Over the 30-day post-infusion period, among patients in the OP cohort, 59.5% had ≥1 IP stay, hence 40.5% of patients did not require an IP admission during the first 30 days post-infusion. The mean number of all-cause IP days was 4.7 PPPM, while the mean number of all-cause OP days was 13.8 PPPM. Among patients in the IP cohort, the mean number of all-cause IP days was 14.7 PPPM, and the mean number of all-cause OP days was 5.9 PPPM; 96.8% of patients had ≥1 OP visit. Compared with the IP cohort, the OP cohort had a significantly lower mean number of all-cause IP days PPPM (IRR [95% CI]: 0.31 [0.21; 0.42], p < 0.001) and a significantly higher mean number of all-cause OP days PPPM (IRR [95% CI]: 1.88 [1.40; 2.56], p < 0.001; Table 2 & Figure 3).
| 30-day post-infusion period | 90-day post-infusion period | |||
|---|---|---|---|---|
| OP cohort (N = 37) | IP cohort (N = 62) | OP cohort (N = 37) | IP cohort (N = 62) | |
| Follow-up duration (months), mean ± SD [median] | 1.0 ± 0.2 [1.0] | 1.0 ± 0.1 [1.0] | 2.6 ± 0.8 [3.0] | 2.8 ± 0.5 [3.0] |
| All-cause HCRU | ||||
| IP stays | ||||
| ≥1 IP stay, n (%) | 22 (59.5) | 62 (100.0) | 24 (64.9) | 62 (100.0) |
| Days PPPM, n, mean ± SD [median] | 4.7 ± 5.2 [3.9] | 14.7 ± 5.0 [13.7] | 2.7 ± 3.7 [1.7] | 7.6 ± 5.2 [5.0] |
| OP visits | ||||
| ≥1 OP visit, n (%) | 37 (100.0) | 60 (96.8) | 37 (100.0) | 61 (98.4) |
| Number of days PPPM, mean ± SD [median] | 13.8 ± 8.9 [15.7] | 5.9 ± 3.6 [4.9] | 11.0 ± 8.3 [10.0] | 5.7 ± 4.0 [5.1] |
| MM-related HCRU‡ | ||||
| IP stays | ||||
| ≥1 IP stay, n (%) | 20 (54.1) | 62 (100.0) | 22 (59.5) | 62 (100.0) |
| Days PPPM, n, mean ± SD [median] | 4.0 ± 4.8 [2.0] | 14.2 ± 5.0 [12.8] | 2.5 ± 3.7 [1.7] | 7.4 ± 5.2 [5.0] |
| OP visits | ||||
| ≥1 OP visit, n (%) | 36 (97.3) | 57 (91.9) | 37 (100.0) | 59 (95.2) |
| Days PPPM, n, mean ± SD [median] | 9.8 ± 7.6 [6.9] | 4.4 ± 2.6 [3.9] | 6.8 ± 6.1 [6.4] | 3.8 ± 2.6 [3.2] |
†
HCRU was evaluated over the observation period, which was defined as the time from the index date to the earliest of 90 days post-infusion, end of clinical activity, death, or end of data availability (30 June 2025).
‡
MM-related medical claims are defined as those associated with an ICD-10-CM diagnosis of MM (C90.0).
HCRU: Healthcare resource utilization; ICD-10 CM: International Classification of Diseases, 10th Revision, Clinical Modification; IP: Inpatient; MM: Multiple myeloma; OP: Outpatient; PPPM: Per patient per month; SD: Standard deviation.
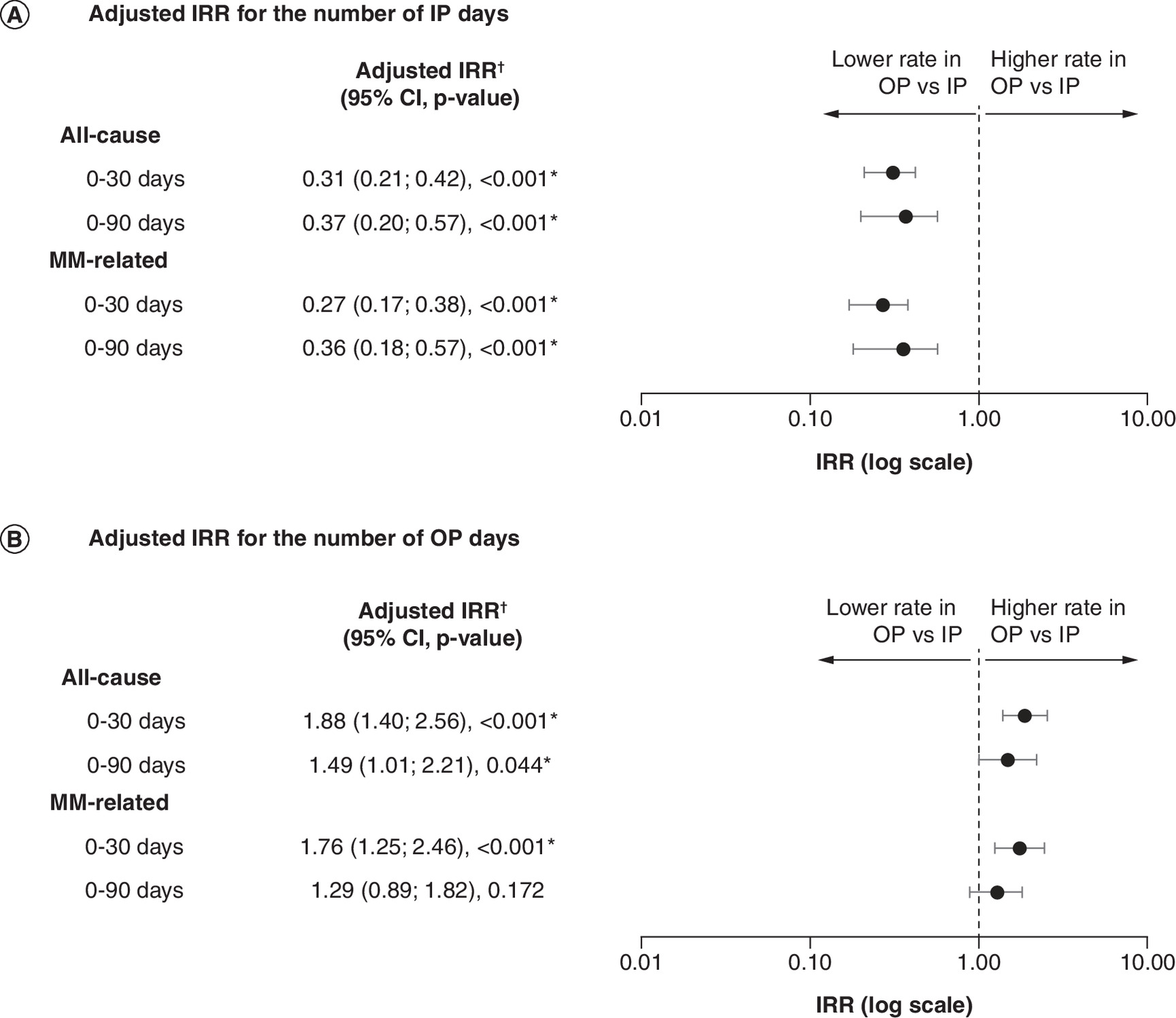
Figure 3. Comparisonof healthcare resource utilization between the outpatient and inpatient cohorts.
(A) Number of IP days. (B) Number of OP days.
HCRU was evaluated over the observation period defined as the time from the index date to the earliest of 90 days post-infusion, end of clinical activity, death, or end of data availability (30 June 2025).
*Statistical significance.
†The model adjustedfor age (reference group: ≥70 years), sex, race (reference group: White), payer type (reference group: Medicare), year of index (reference group: 2024), Quan-CCI score, frailty index score in 3 months prior to infusion (reference group: nonfrail), and having ≥1 CRAB symptom in the month prior to infusion.
CCI: Charlson Comorbidity Index; CRAB: Hypercalcemia, renal impairment, anemia, and bone lesions; HCRU: Healthcare resource utilization; IP: Inpatient; IRR: Incidence rate ratio; MM: Multiple myeloma; OP: Outpatient.
Over the 90-day post-infusion period, among patients in the OP cohort, 64.9% had ≥1 all-cause IP stay, and the mean number of IP days was 2.7 PPPM, while the mean number of all-cause OP days was 11.0 PPPM. Among patients in the IP cohort, the mean number of all-cause IP days was 7.6 PPPM, and the mean number of all-cause OP days was 5.7 PPPM; 98.4% of patients had ≥1 OP visit. Compared with the IP cohort, the OP cohort had a significantly lower mean number of all-cause IP days PPPM (IRR [95% CI]: 0.37 [0.20; 0.57], p < 0.001) and a significantly higher mean number of all-cause OP days PPPM (IRR [95% CI]: 1.49 [1.01; 2.21], p = 0.044; Table 2 & Figure 3). Findings were consistent for MM-related HCRU during both the 30- and 90-day post-infusion periods (Table 2 & Figure 3).
Healthcare costs
With respect to imputed (estimated) all-cause healthcare costs, over the 30-day post-infusion period, among patients in the OP cohort, imputed mean all-cause IP-related costs were $18,613 PPPM and all-cause OP-related costs were $1693 PPPM. Among patients in the IP cohort, imputed mean all-cause IP-related costs were $57,830 PPPM and all-cause OP-related costs were $725 PPPM. Compared with the IP cohort, the OP cohort had significantly lower imputed mean all-cause IP-related costs (mean difference [95% CI]: -$39,786 [-$48,120; -$30,765], p < 0.001) and significantly higher imputed mean all-cause OP-related costs (mean difference [95% CI]: $788 [$486; $1188], p < 0.001; Figure 4).
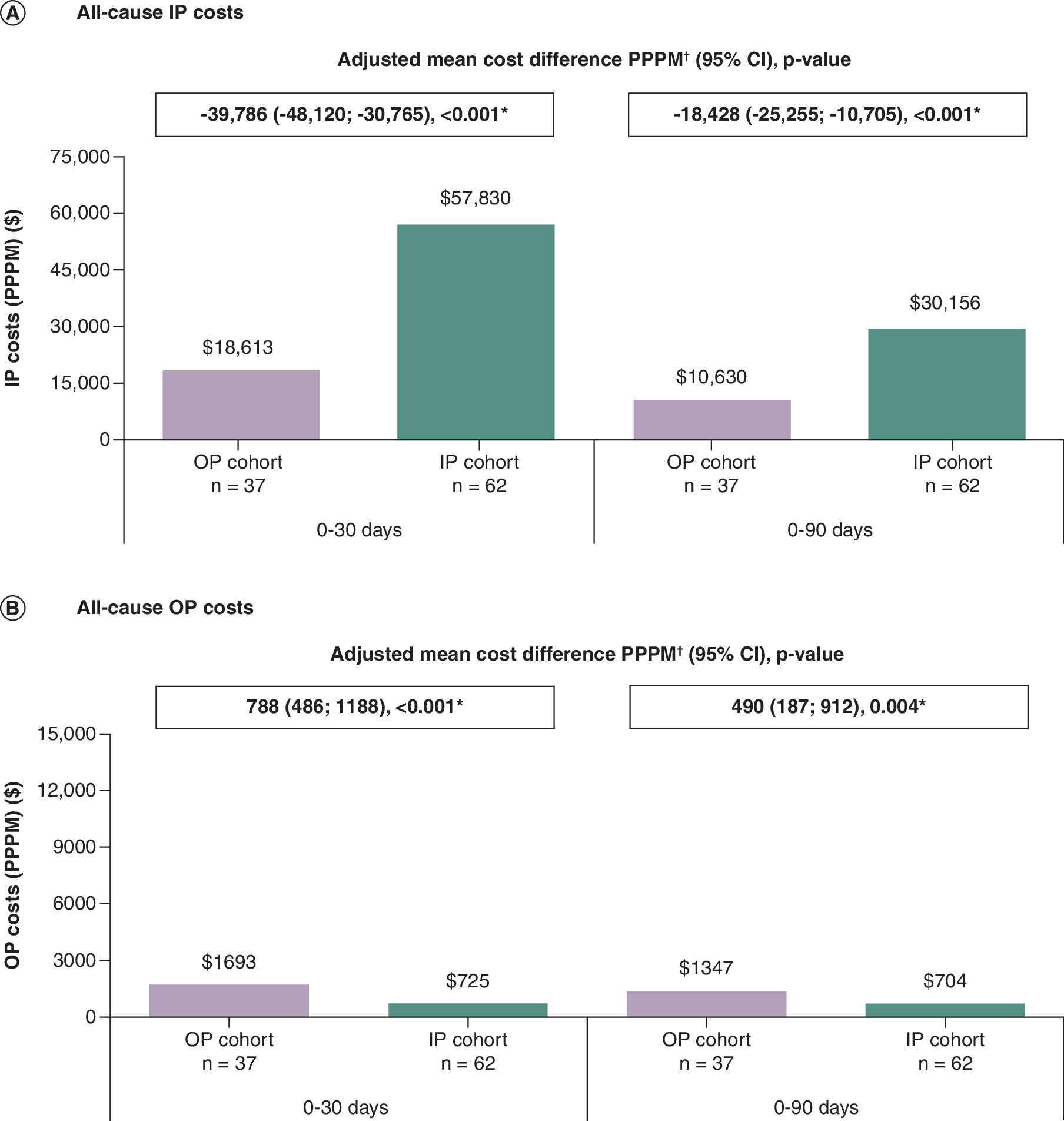
Figure 4. Comparisonof all-cause costs between the outpatient and inpatient cohorts.
(A) All-cause IP costs. (B) All-cause OP costs.
Costs were evaluated following cilta-cel administration from the index date to the earliest of 90 days post-infusion, end of clinical activity, death, or end of data availability (30 June 2025). Costs were standardized to 2025 USD and calculated by multiplying the number of IP days by $3943.10/day and the number of OP days by $122.51/day.
*Statistical significance.
†The model adjusted for age (reference group: ≥70 years), sex, race (reference group: White), payer type (reference group: Medicare), year of index (reference group: 2024), Quan-CCI score, frailty index score within 3 months of infusion (reference group: nonfrail), and having ≥1 CRAB symptom in the month prior to infusion.
CCI: Charlson Comorbidity Index; CRAB: Hypercalcemia, renal impairment, anemia, and bone lesions; IP: Inpatient; OP: Outpatient; PPPM: Per patient per month; USD: US dollar.
Over the 90-day post-infusion period, among patients in the OP cohort, imputed mean all-cause IP-related costs were $10,630 PPPM and all-cause OP-related costs were $1347 PPPM. Among patients in the IP cohort, imputed mean all-cause IP-related costs were $30,156 PPPM and all-cause OP-related costs were $704 PPPM. Compared with the IP cohort, the OP cohort had significantly lower imputed mean all-cause IP-related costs (mean difference [95% CI]: -$18,428 [-$25,255; -$10,705], p < 0.001) and significantly higher imputed mean all-cause OP-related costs (mean difference [95% CI]: $490 [$187; $912], p = 0.004; Figure 4). These findings were consistent for MM-related imputed costs during both the 30- and 90-day post-infusion periods (Figure 5). A summary of coefficients for covariates included in the multivariate models for HCRU and imputed costs is presented in Supplementary Tables 4 & 5.
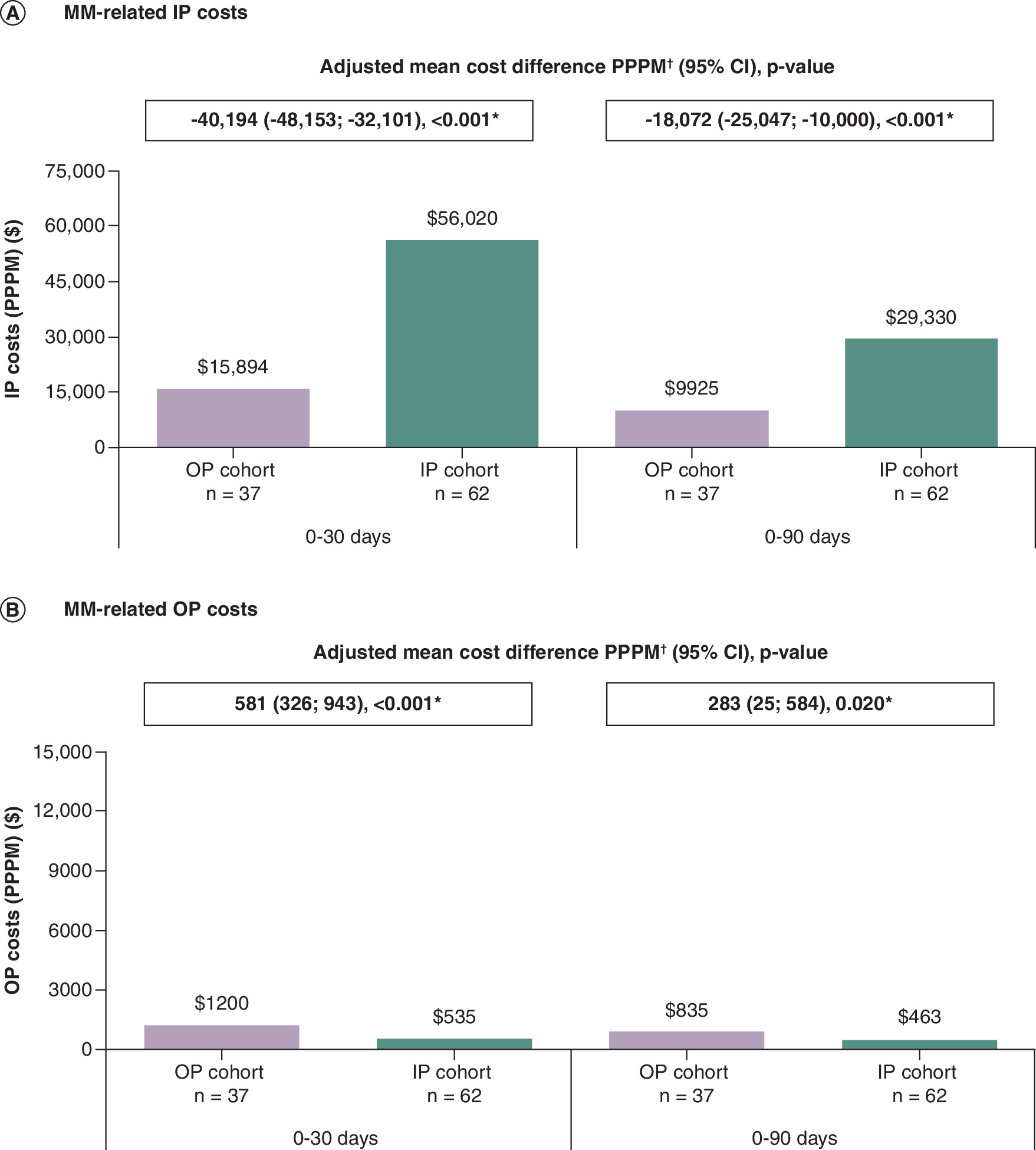
Figure 5. Comparisonof MM-related costs between the outpatient and inpatient cohorts.
(A) MM-related IP costs. (B) MM-related OP costs.
Costs were evaluated following cilta-cel administration from the index date to the earliest of 90 days post-infusion, end of clinical activity, death, or end of data availability (30 June 2025). Costs were standardized to 2025 USD and calculated by multiplying the number of IP days by $3943.10/day and the number of OP days by $122.51/day.
*Statistical significance.
†The model adjusted for age (reference group: ≥70 years), sex, race (reference group: White), payer type (reference group: Medicare), year of index (reference group: 2024), Quan-CCI score, frailty index score within 3 months of infusion (reference group: nonfrail), and having ≥1 CRAB symptom in the month prior to infusion.
CCI: Charlson Comorbidity Index; CRAB: Hypercalcemia, renal impairment, anemia, and bone lesions; IP: Inpatient; MM: Multiple myeloma; OP: Outpatient; PPPM: Per patient per month; USD: US dollar.
Discussion
In this observational analysis of patients with RRMM treated with cilta-cel after 1–3 prior LOT in real-world clinical practice, OP administration of cilta-cel was associated with significantly lower IP days and lower imputed cost estimates compared with IP administration of cilta-cel. In the first 30 days post-infusion, OP administration of cilta-cel was associated with a mean cost savings of approximately $40,000 due to a lower number of IP days, offsetting the slight increase of $800 due to a higher number of OP days. In the first 90 days post-infusion, we found a mean monthly cost savings of approximately $18,000 in the OP cohort due to a lower number of IP days, and an increase of $500 due to a higher number of OP days. Based on these monthly cost savings, we estimated an overall cost savings of approximately $53,000 per patient with OP administration of cilta-cel over the first 3 months post-infusion relative to IP administration, with the vast majority of HCRU and associated cost savings being MM-related. These findings reinforce the potential HCRU and economic value of OP cilta-cel delivery, align with emerging evidence on OP administration of CAR-T therapy [8,9], and provide early insights into a growing trend toward OP CAR-T administration.
The observed reduction of approximately 10 IP days within 30 days post-infusion among patients with OP versus IP administration of cilta-cel may support a meaningful shift in post-cilta-cel care. The magnitude of reduction was consistent with prior single-center preliminary evaluations of OP cilta-cel administration, where the median number of IP days during the first 30 days post-infusion was 15 days shorter for OP versus IP administration (OP: 4 days; IP: 19 days) [11]. Similarly, in a retrospective claims-based analysis of patients receiving cilta-cel after ≥4 prior LOT, OP administration of cilta-cel was associated with approximately 9 fewer IP days in the first 30 days post-infusion, and a substantial proportion of patients in the OP cohort did not require IP admission during the early post-infusion period, consistent with our findings despite differences in LOT [12]. Studies of CAR-T therapies across hematologic malignancies have also shown that OP administration reduced overall early IP-related HCRU post-infusion despite the occurrence of some unplanned IP stays among patients with OP CAR-T administration, which were primarily driven by anticipated symptoms of CRS [13]. Indeed, previous studies reported a mean length of IP stays among patients with OP CAR-T administration two-to-three-times shorter than those among patients with IP CAR-T administration [13]. This difference likely reflected the structured monitoring protocols integral to OP CAR-T delivery, which emphasize proactive symptom management and selective escalation to IP care when needed, therefore resulting in a reduction in overall IP-related resource use [13].
Consistent with structured monitoring protocols, patients in the OP cohort in our study had more OP days during the first month post-infusion than those in the IP cohort. This pattern aligns with the expected timing of CAR-T-related adverse events such as CRS and ICANS, which typically occur within the first 2 weeks following infusion [5,6,16]. Our findings indicate that, in this cohort, 40.5% of patients with OP administration of cilta-cel did not require an IP admission within the first 30 days post-infusion. These results were consistent with a prior study in patients with ≥4 prior LOT, where 32% of patients treated with OP cilta-cel did not require IP admission during the first 30 days post-infusion [12].
Although costs in this analysis were extrapolated using literature-based estimates, the observed cost savings were consistent with previously reported real-world evaluations of OP and IP CAR-T administration. In our study, OP administration of cilta-cel was associated with an estimated cost savings of $40,000 per patient within the first 30 days post-infusion and $53,000 over the first 90 days. Prior cost analyses have reported total savings of $30,000–50,000 per patient in the first 6 months post-infusion with OP versus IP CAR-T administration, largely attributable to fewer IP days [13], while a recent conference proceeding reported more modest cost savings of approximately $20,000 in the first 30 days among patients receiving OP cilta-cel compared with a matched IP cohort [26]. However, the latter analysis matched patients on severity and timing of subsequent CRS and ICANS – key cost drivers – which likely attenuated post-infusion cost differences between cohorts. Accordingly, OP cilta-cel administration may help offset the upfront costs of CAR-T infusion by lowering post-infusion resource utilization and overall costs of care.
The present study builds upon previous findings in patients with ≥4 prior LOT [12] by evaluating HCRU and costs among patients who received cilta-cel after 1–3 prior LOT, a population in which cilta-cel adoption has increased following its expanded FDA approval in 2024. By focusing on earlier LOT, this study provides new insights into the potential cost efficiencies that may be achieved through implementation of OP CAR-T programs for patients with RRMM. This is particularly relevant as cilta-cel use extends to less heavily pretreated populations. Collectively, this study adds to the growing body of evidence that supports the continued expansion of OP cilta-cel programs to optimize value-based care delivery in RRMM. Shifting post-infusion monitoring care from an IP to OP setting may improve health-system efficiency, alleviate capacity constraints, and expand access to CAR-T therapy [8,9]. Institutions adopting OP administration models may also benefit from improved patient experience and faster throughput for advanced therapies [8,9].
Findings from this study should be interpreted considering some limitations. First, we relied on EMR data, which provides a more comprehensive view of patient encounters within the EMR network relative to claims data which includes claims billed for insurance purposes. However, EMR does not capture care delivered out of network and may have varying degrees of data completeness across EMR sources. To mitigate this, patients were required to have a known setting of cilta-cel administration, which may have ensured a minimum level of data completeness across patients. However, misclassification of LOT status due to incomplete capture or coding of healthcare encounters was still possible, and MM-related HCRU may have been underestimated, particularly if treatment-related complications were miscoded [16]. To mitigate the potential for bias, we additionally evaluated all-cause HCRU to capture IP and OP utilization that may not have been explicitly coded as MM-related, and findings were consistent across all-cause and MM-related HCRU. Additionally, IP utilization included admissions associated with the initial CAR-T infusion for the IP cohort; therefore, differences in total IP days partly reflect the structure of the treatment pathway itself that accounts for post-infusion monitoring of patients while hospitalized. The dataset did not capture the intent of admissions, and some OP pathways may include protocol-driven or scheduled IP monitoring; therefore, results did not distinguish between planned and unplanned care. Furthermore, cost estimates were imputed, using methodologies described in prior research on cost imputation [20], based on current literature-derived costs [21,23] and may not reflect variation in payer-paid amounts or intensity of IP and OP services, and may not have accounted for differences in costs associated with virtual or remote care. For example, IP days involving higher-intensity care may incur greater costs than routine monitoring days; per-day cost estimates may not fully capture heterogeneity within care settings and may result in over- or underestimation of absolute costs. Furthermore, follow-up time was limited, precluding assessment of long-term HCRU and costs. As this was a real-world retrospective study, patients were classified into cohorts based on observed site of administration rather than randomized assignment; thus, differences in patient characteristics and system-level factors may have influenced cohort classification. Adjusted regression analyses were conducted to account for observed differences between cohorts, but residual confounding due to unmeasured factors not captured in the EMR (e.g., institutional characteristics, practice patterns) may remain. The relatively small cohort sizes limited the extent of covariate adjustment to avoid overfitting and precluded the use of more complex methodologies (e.g., propensity score-based approaches or clustering to account for variation across centers). In addition, only limited facility-level information was available; therefore, variation in center and regional factors may not be fully captured. Future studies with larger sample sizes are warranted to more comprehensively characterize and adjust for factors influencing OP versus IP administration. Nonetheless, the consistency of our findings with prior studies across multiple data sources supports the robustness of the observed patterns.
In conclusion, in this observational study, OP administration of cilta-cel was associated with lower IP resource utilization and reduced imputed costs during the first 3 months post-infusion compared with IP administration. In this cohort, 40.5% of patients receiving OP cilta-cel did not require an IP admission in the first 30 days post-infusion. These findings reflect early experience with an evolving shift toward OP CAR-T administration and underscore the potential economic value of OP cilta-cel delivery, while highlighting an opportunity for further evaluation of OP CAR-T models in supporting high-value, patient-centered care for the eligible population with RRMM.
Summary points
•
Outpatient (OP) administration of ciltacabtagene autoleucel (cilta-cel), a chimeric antigen receptor T-cell therapy, may improve feasibility and accessibility compared with inpatient (IP) administration.
•
This real-world study compared healthcare resource utilization and imputed cost estimates following OP or IP administration of cilta-cel among patients with relapsed or refractory multiple myeloma (RRMM) treated after 1–3 prior lines of therapy.
•
Electronic medical records from Loopback Analytics (2017–2025) were used.
•
Over the first 30 days post-infusion, patients with OP administration had significantly fewer IP days per month compared with those with IP administration.
•
OP administration resulted in significantly lower IP-related costs compared with IP administration over the first 30 days post-infusion.
•
Overall, OP administration was associated with an estimated cost savings of approximately $40,000 per patient in the first month following infusion.
•
The results suggest OP delivery of cilta-cel may reduce healthcare resource utilization, while providing substantial associated economic benefits, reinforcing the potential feasibility of OP chimeric antigen receptor T-cell administration models.
Author contributions
All authors have made substantial contributions to the conception or design of the study, or the acquisition, analysis, or interpretation of data, drafting the manuscript and revising it critically for important intellectual content, and have provided final approval of this version to be published and agree to be accountable for all aspects of the work.
Financial disclosure
This study was funded by Johnson & Johnson (NJ, USA), and Legend Biotech USA Inc. (NJ, USA).
Competing interests disclosure
M Janakiram reports research for Johnson & Johnson, BMS, Legend, FATE Therapeutics, and advisory board with Johnson & Johnson and BMS. S Ghosh, V Alegria, T Bixby, SP Nagar and ZP Qureshi are employees and stockholders of Johnson & Johnson. M Perciavalle is an employee and stockholder of Legend Biotech. B Emond and J Maitland are employees of Analysis Group ULC, a consulting company that has provided paid consulting services to Johnson & Johnson, which along with Legend Biotech USA Inc., funded the development and conduct of this study. DR Bakaloudi has no conflicts of interest to disclose. D Dima reports consulting for Karyopharm, Caribou, KITE and Pfizer. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Editorial and analytical support was provided by Alvi Rahman, Ph.D., Jingyi Liu, M.BI. and Alessio Palladino, B.Eng., employees of Analysis Group ULC, a consulting company that has provided paid consulting services to Johnson & Johnson, which, along with Legend Biotech USA Inc., funded the development and conduct of this study.
Ethical conduct of research
This study was considered exempt from review by an institutional review board as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA). This research study was conducted in accordance with the principles stated in the Declaration of Helsinki.
Data transparency statement
The authors certify that this manuscript reports the original results of a real-world evidence study. No prespecified study protocol or preregistration was reported for this study. The data that support the findings of this study are available from Loopback Analytics. Restrictions apply to the availability of these data, which were used under license for this study. The data are available through requests made directly to Loopback Analytics, subject to their respective requirements for access.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplemtary data.docx)
- Download
- 76.11 KB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Berdeja JG, Madduri D, Usmani SZ et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b/2 open-label study. Lancet 398(10297), 314–324 (2021).
2.
San-Miguel J, Dhakal B, Yong K et al. Cilta-cel or standard care in lenalidomide-refractory multiple myeloma. N. Engl. J. Med. 389(4), 335–347 (2023).
3.
Einsele H, San-Miguel J, Dhakal B et al. Cilta-cel in lenalidomide-refractory multiple myeloma (CARTITUDE-4): an updated analysis including overall survival from an open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 27(2), 254–268 (2026).
4.
Johnson & Johnson. CARVYKTI® is the first and only BCMA-targeted treatment approved by the U.S. FDA for patients with relapsed or refractory multiple myeloma who have received at least one prior line of therapy. April 2024. (Accessed: 23 June 2025). https://www.jnj.com/media-center/press-releases/carvykti-is-the-first-and-only-bcma-targeted-treatment-approved-by-the-u-s-fda-for-patients-with-relapsed-or-refractory-multiple-myeloma-who-have-received-at-least-one-prior-line-of-therapy
5.
Wesson W, Dima D, Suleman N et al. Timing of toxicities and non-relapse mortality following CAR T therapy in myeloma. Transplant. Cell. Ther. 30(9), 876–884 (2024).
6.
Merz M, Albici AM, von Tresckow B et al. Idecabtagene vicleucel or ciltacabtagene autoleucel for relapsed or refractory multiple myeloma: an international multicenter study. Hemasphere 9(1), e70070 (2025).
7.
U.S. Food and Drug Administration. CARVYKTI® (ciltacabtagene autoleucel) highlights of prescribing information. October 2025. (Accessed: 25 February 2026). https://www.fda.gov/media/156560/download?attachment
8.
Hansen DK, Dhakal B, Hamadani M et al. Clinician and administrator perspectives on outpatient administration of ciltacabtagene autoleucel in relapsed or refractory multiple myeloma. Front. Immunol. 15, 1405452 (2024).
9.
Alsina M, Dhakal B, Pantin J, Huff CA, Janakiram M. Establishing a successful outpatient CAR T-Cell program with cilta-cel: real-world experience from an expert roundtable. Future Oncol. 21(10), 1137–1144 (2025).
•• This expert roundtable based on real-world experience provides insights on feasibility, safety and effectiveness of outpatient (OP) chimeric antigen receptor T-cell (CAR-T) administration, and identifies key success factors to prepare institutions, patients, and caregivers.
10.
Ly A, Huff CA, Gocke C et al. Safety and feasibility of outpatient administration of ciltacabtagene autoleucel (cilta-cel). Transplant. Cell. Ther. 30(Suppl. 2), S186–S187 (2024).
11.
Waqar S, Hansen D, Freeman C et al. Evaluation of outpatient administration of ciltacabtagene autoleucel in relapsed/refractory multiple myeloma: single center experience. Transplant. Cell. Ther. 2S, S388 (2024).
12.
Janakiram M, Fan L, Ghosh S et al. Real-world healthcare resource utilization and clinical outcomes among patients with relapsed/refractory multiple myeloma receiving ciltacabtagene autoleucel after four or more prior lines of therapy in inpatient versus outpatient settings. J. Med. Econ. 29(1), 871–884 (2026).
13.
Hansen DK, Liu YH, Ranjan S et al. The impact of outpatient versus inpatient administration of CAR-T therapies on clinical, economic, and humanistic outcomes in patients with hematological cancer: a systematic literature review. Cancers (Basel) 15(24), 5746 (2023).
14.
Myers GD, Verneris MR, Goy A, Maziarz RT. Perspectives on outpatient administration of CAR-T cell therapy in aggressive B-cell lymphoma and acute lymphoblastic leukemia. J. Immunother. Cancer 9(4), e002056 (2021).
•• This real-world claims study shows OP administration of cilta-cel yielded similar effectiveness and safety outcomes relative to inpatient (IP) administration, while significantly reducing IP resource use among patients treated after 4 or more prior lines of therapy (LOT) using the same LOT algorithm employed in the current study.
15.
Sidana S, Nagar SP, Ghosh S et al. Real-world description of non-ICANS neurologic events among patients with relapsed or refractory multiple myeloma treated with ciltacabtagene autoleucel using two large US databases. Oncol. Ther. doi: (2026) (Epub ahead of print).
16.
Ferver K, Burton B, Jesilow P. The use of claims data in healthcare research. Open Public Health J. 2, 11–24 (2009).
17.
Brammer JE, Braunstein Z, Katapadi A et al. Early toxicity and clinical outcomes after chimeric antigen receptor T-cell (CAR-T) therapy for lymphoma. J. Immunother. Cancer 9(8), e002303 (2021).
18.
Rejeski K, Subklewe M, Locke FL. Recognizing, defining, and managing CAR-T hematologic toxicities. Hematology Am. Soc. Hematol. Educ. Program 2023(1), 198–208 (2023).
19.
Bishop MR. Late complications and long-term care of adult CAR T-cell patients. Hematology Am. Soc. Hematol. Educ. Program 2024(1), 109–115 (2024).
20.
Rogers KA, Muluneh B, Qureshi ZP et al. A comparison of healthcare resource utilization and costs between patients with chronic lymphocytic leukemia treated with first-line ibrutinib or acalabrutinib using two large US real-world databases. J. Comp. Eff. Res. 14(6), e240210 (2025).
21.
Jagannath S, Joseph N, Crivera C et al. Component costs of CAR-T therapy in addition to treatment acquisition costs in patients with multiple myeloma. Oncol. Ther. 11(2), 263–275 (2023).
••Identifies cost components and unit costs associated with administration of cilta-cel and provided the key input for estimation of the cost of an OP day following cilta-cel infusion that was used within the cost imputation in the current study.
22.
Roemer M. Statistical Brief #270. Cancer-related hospitalizations for adults, 2017. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality, MD, USA, Accessed: 24 November 2025. https://www.ncbi.nlm.nih.gov/books/NBK568320/
23.
Kuhr FK, Mishiev MN, Spinner WA, Warren N, Faulkner EC. Increasing costs of hospitalizations for multiple myeloma in the United States: a database analysis on aggregate costs and patient subpopulations. Value Health 28(6), S66 (2025).
•• Analyzes the cost of IP care within multiple myeloma over time, and provided the key input for estimation of the cost of an IP day within this population that was used within the cost imputation in the current study.
24.
Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun. Stat-Simul. Comput. 38(6), 1228–1234 (2009).
25.
Patel BG, Luo S, Wildes TM, Sanfilippo KM. Frailty in older adults with multiple myeloma: a study of US veterans. JCO Clin. Cancer Inform. 4, 117–127 (2020).
26.
Ferreri C, Gaballa M, Santiago M et al. Cost-conscious CAR T delivery: outpatient (OP) cilta-cel administration reduces health care resource utilization (HCRU) and the associated post-infusion cost. Blood 146(Suppl. 1), 2634 (2025).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 7 March 2026
Accepted: 22 May 2026
Published online: 29 June 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Healthcare resource utilization and costs in patients with multiple myeloma administered ciltacabtagene autoleucel in outpatient versus inpatient settings after one to three prior lines of therapy. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0052
Export citation
Select the citation format you wish to export for this article or chapter.