Use of intracardiac echocardiography and three-dimensional mapping during catheter ablation for atrial fibrillation is associated with reduced complications: a retrospective analysis of United States Medicare Fee-For-Service Database
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This retrospective cohort study assessed differences in procedure-related complications and death among old patients with atrial fibrillation (AF) undergoing catheter ablation (CA) procedure with versus without use of intracardiac echocardiography (ICE) and advanced three-dimensional (3D) electroanatomical mapping. Materials & methods: Using the Medicare Database, a retrospective cohort of AF patients ≥65 years of age who underwent CA procedure were identified, and categorized into two cohorts: CA without ICE/3D mapping versus CA with ICE/3D mapping. Outcomes including a composite of complications (any), cardiac perforation, esophageal fistula and death, respectively, in the 30-day period post-CA were assessed. Inverse probability of treatment weighting method was used for covariate balancing. Cox regression models were performed to evaluate outcomes. Results: There were 35,490 patients in CA without ICE/3D mapping cohort and 170,762 in the CA with ICE/3D mapping cohort. Cox regression model revealed that patients who underwent CA without ICE/3D mapping use were ∼3.5-times more likely to have 30-day any complication versus those who had CA with ICE/3D mapping (7.3% vs 2.2%, log-rank test p < 0.001; hazard ratio: 3.507; 95% CI: 3.307–3.720, p < 0.001). The incidence of cardiac perforation (2.5% vs 0.1%, log-rank test p < 0.001), atrio-esophageal fistula (0.03% vs 0.01%, log-rank test p = 0.03) and death (1.6% vs 0.2%, log-rank test p < 0.001) were significantly higher among patients without ICE/3D mapping versus those who had CA with ICE/3D mapping. Conclusion: The absence of ICE and 3D mapping during CA procedures was associated with significantly increased risk of complications and death among Medicare eligible patients with AF.
Plain language summary
What is this article about?
Atrial fibrillation (AF) is the most common heart rhythm disorder that increasingly be treated with a procedure called catheter ablation (CA). During the procedure, intracardiac echocardiography (ICE) and electroanatomical mapping (EAM) systems help make the treatment better by creating a real-time, detailed picture of the heart. This study compared 30-day complications and death after CA performed between older patients without versus with ICE/3D mapping during the procedure.
What were the results?
Analyzing the data of 206,252 Medicare patients with AF treated with CA, older patients treated without ICE/3D mapping use were ∼3.5-times more likely to have 30-day any complication versus those who had CA with ICE/3D mapping. Older patients who underwent CA without ICE/3D mapping were also more likely to die during or within 30 days of CA. Similar results were observed in patients who had ablation procedure in hospitals without on-site cardiac surgery support.
What do the results mean?
These findings suggest that use of ICE and ED mapping during CA may offer an advantage in preventing complications and death during or post procedure. As CA increasingly expands to smaller hospitals, this study highlighted the importance of having ICE and 3D mapping as a part of a comprehensive CA workflow.
In the US, approximately 6 million people suffer from atrial fibrillation (AF) [1]. AF is strongly associated with advanced age and its prevalence is expected to increase as the population ages [2–5]. In recent years, catheter ablation (CA) has emerged as a mainstay treatment option for AF [6–12]. Studies have demonstrated CA to be associated with a reduction in the burden of AF, an improvement in quality of life, as well as a decrease in health resource utilization and mortality [13–16]. The rate of complications during CA has been reported to be 2.5–8% across various studies [17]. However, some complications, such as pericardial tamponade, stroke, thromboembolic event or esophageal perforation, can be severe or potentially fatal [17].
Intracardiac echocardiography (ICE) is an established imaging modality that enables real-time visualization of internal heart structures, allowing for more precise catheter positioning, transseptal puncture and monitoring for potential complications [18,19]. ICE use during AF ablation has been shown to be associated with significant reductions in fluoroscopy time, fluoroscopy dose and procedure time versus ablation without ICE [20]. More importantly, the use of ICE during CA has been shown to be associated with a significant reduction in complications [21–23], in-hospital mortality [21], length of hospital stay [21], hospital readmission [24] and 12-month repeat ablation [23]. In addition to ICE, advanced three-dimensional (3D) electroanatomical mapping systems (EAM) greatly facilitate ablation procedures. The EAM system works by recording electrical information using mapping catheters and producing a 3D geometrical reconstruction with a color-coded display of the electrical activation sequence, providing a highly targeted treatment region as well as reliable tagging of areas treated with ablation [25]. The use of advanced 3D mapping systems in CA procedures has been shown to optimize patient outcomes and reduce procedural time and radiation exposure [26–30].
Given these factors, CA procedures have increasingly adopted the use of ICE and 3D mapping. To date, however, no large observational study has examined the difference in complication rates between patients who had concurrent ICE and 3D mapping use during CA procedure and those who did not. As ablation becomes the mainstay treatment modality for AF and is increasingly performed in hospitals with or without cardiothoracic backup (including potential future transition to Ambulatory Surgery Centers [ASCs]), it is critical to understand the role of intraoperative procedural tools in influencing outcomes. As such, the purpose of this study was to compare the incidence of complications in patients who underwent CA procedure without ICE and 3D mapping use versus those who had the procedure with ICE and 3D mapping use.
Materials & methods
Data source
The 2016–2023 Medicare Limited DataSet Standard Analytic Files (SAFs) Database was used for study purposes. The Medicare SAF database is a deidentified administrative claims database of Medicare fee-for-service beneficiaries, and includes medical claims spanning multiple settings of care (i.e. inpatient, outpatient, skilled nursing facility, home health agency and hospice). The Medicare SAFs database allows for longitudinal analysis of patient-level claims. This analysis of the Medicare SAFs database was conducted under exemption from Institutional Review Board oversight for US-based studies using de-identified healthcare records, as dictated by Title 45 Code of Federal Regulations (45 CFR 46.101(b)(4)).
Study population
Older patients (≥65 years of age) who had CA procedure with a primary diagnosis of AF (based on International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM] diagnosis codes: I48.0, I48.1x, I48.2x, I48.91) between January 2017 and May 2023 (with the first CA procedure as ‘index’) were identified. Patients were included if they had Medicare as primary payor; had continuous enrollment in Medicare parts A & B and no Health Maintenance Organization (HMO) enrollment for 6 months in pre-index period; did not receive care outside the US during index; did not have AF-related CA procedure any time prior to index ablation. Patients were further excluded if they had AF-related surgical ablation within 6-month pre-index period; had cardiac surgery within 6-month pre-index period; had left atrial appendage occlusion (LAAO) procedure within 6-month pre-index period; were diagnosed with end stage renal disease (ESRD); had unclear death date in the database. Patients who met the study criteria were then classified into two groups: without ICE and 3D mapping (without ICE/3D mapping) group (i.e., where ICE and 3D mapping were not used during index CA procedure); with ICE and 3D mapping (with ICE/3D mapping) group (i.e., where ICE and 3D mapping was used during index CA procedure). The use of ICE and 3D mapping was determined based on ICD-10 Procedural Coding System (PCS) (ICE: B244YZZ, B244ZZZ, B245YZZ, B245ZZZ, B246YZZ, B246ZZZ, B244ZZ3, B245ZZ3, B246ZZ3), Current Procedural Terminology (CPT) codes (ICE: 93662; 3D mapping: 93613) and Healthcare Common Procedure Coding System (HCPCS) (ICE: C1759; 3D mapping: C1732). Figure 1 depicts study attrition.
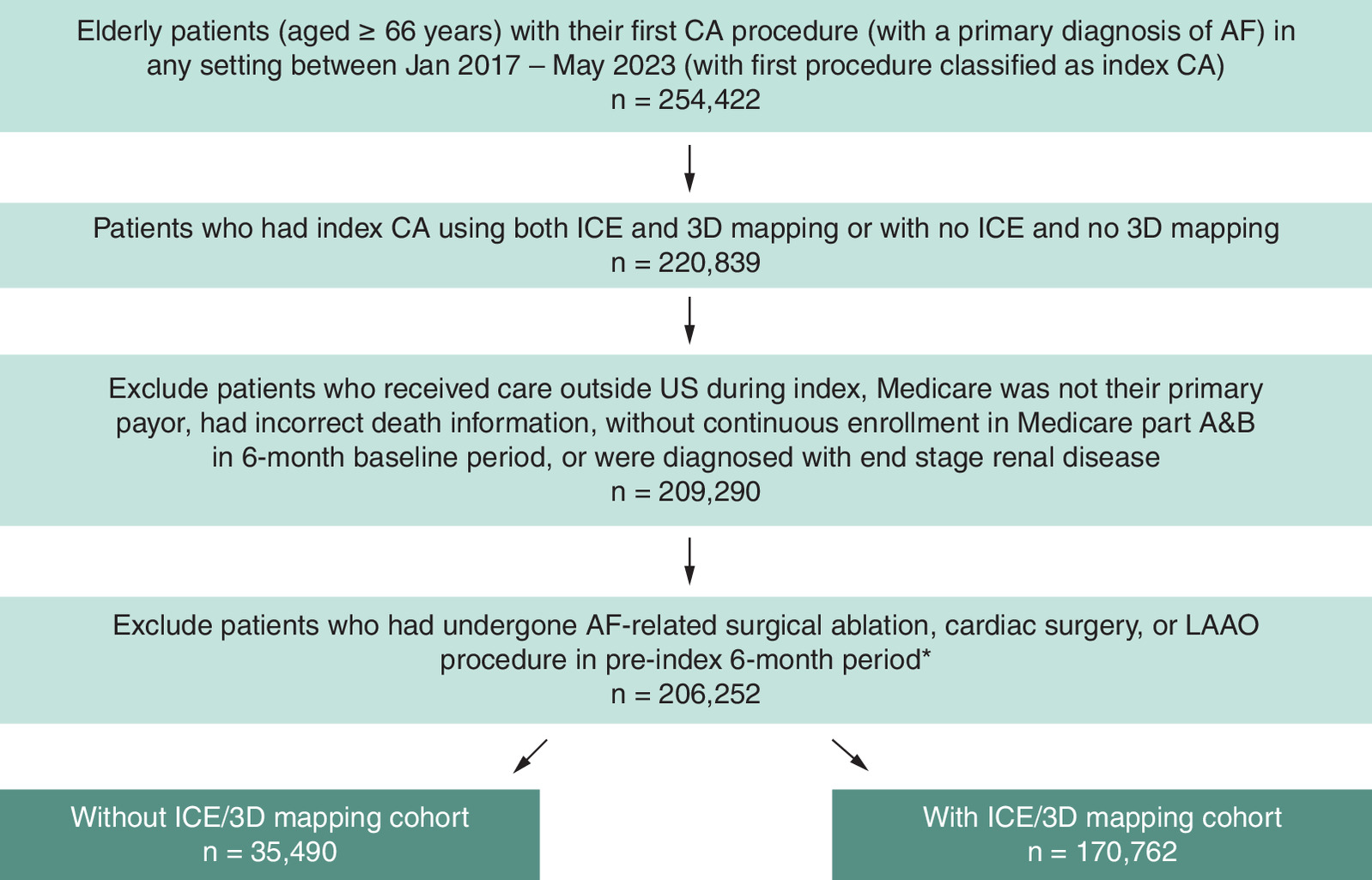
Figure 1. Patient attrition chart.
*100 patients were further excluded due to the missing region information.
AF: Atrial fibrillation; CA: Catheter ablation; ICE: Intracardiac echocardiography; LAAO: Left atrial appendage occlusion.
Study outcome
The primary outcome of this study was procedure-related complications within 30 days post-index CA procedure. The complications assessed included acute coronary syndrome, ischemic stroke, hemorrhagic stroke, thromboembolism, transient ischemic attack, phrenic nerve palsy, pericarditis, bleeding, blood transfusion, atrio-esophageal fistula, severe pulmonary vein stenosis requiring intervention, vagus nerve injury, vascular access complication requiring repair and cardiac tamponade or perforation. Complications were defined by a primary or secondary diagnosis code during index ablation procedure, or hospitalization/emergency room (ER) visit with a primary diagnosis in 30 days post-index ablation procedure. If a patient had the same event in 6-month period prior to the index date, the identified event was not classified as a complication. Patients' data were censored at the point when they lost enrollment, had a repeat CA, died or reached the end of a 30-day follow-up period, if no complications was identified prior to this. Secondary outcomes included procedure-related cardiac perforation (i.e. hemopericardium, pericardiocentesis and cardiac tamponade), atrio-esophageal fistula and death in 30 days post index CA procedure.
CA procedures are increasingly being performed in smaller hospitals, which may not have on-site cardiothoracic surgery (CTS) backup. Sub-group analysis was performed among patients who had their index CA procedure in hospitals without onsite CTS. A hospital was considered as having no CTS if a coronary artery bypass grafting procedure was not performed at any time during the pre-index period [31].
Study covariates
Patients' demographics including age, sex, race, and region were reported. The Elixhauser comorbidity score [32] and the CHA2DS2-VASc score [33] were calculated based on the patients' medical claims during the 6-month period prior to the index. Patients' AF subtypes were determined based on the diagnosis during index CA procedure. Other pre-index clinical characteristics, such as sleep apnea and cardiomyopathy, were also assessed in the 6-month pre-index period. The history (in 6-month prior to the index) of healthcare resource utilization related to AF, including electrical cardioversion and AF-related hospitalization, were also included as covariates.
Statistical analysis
The inverse probability of treatment weighting (IPTW) of propensity score approach was adopted to minimize the effect of potential confounders [34,35]. Due to the potential imbalance of baseline characteristics between patients treated with ICE/3D mapping and without ICE/3D mapping, the IPTW method allows for creating a pseudo-population with a comparable group of patients treated with and without ICE/3D mapping [34]. Each patient was assigned a weight by using the IPTW technique along with an estimation of the average treatment effect [35]. Standardized mean difference (SMD) was used to assess if the distribution of these covariates were balanced after weighting (with SMD >0.1 or <-0.1 considered as imbalanced distribution). Weighted Cox proportional hazards regression model with robust standard errors was used to estimate hazard ratio (HR) and 95% CI of without ICE/3D mapping (versus with ICE/3D mapping) for study outcomes. The Benjamini–Hochberg (BH) correction method was used to control false discovery rate caused by multiple comparisons of outcomes assessment in the regression analysis [36]. Values of p < 0.05 were considered statistically significant (for BH correction, the highest p-value that was smaller than the BH critical value was identified with false discovery rate of 0.10. All p-values greater than the highest p-value were then considered significant). Statistical analyses were conducted with R software (version 4.1.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 206,252 patients were included in the study, with 35,490 patients undergoing CA procedure without ICE/3D mapping and 170,762 with ICE/3D mapping (Figure 1). Before IPTW, patients who underwent ablation without ICE/ 3D mapping were older (75 years and above, 53.8% vs 34.1%, absolute SMD [aSMD]: 0.406), had more female patients (53.8% vs 42.6%, aSMD: 0.226) as compared with those who underwent ablation with ICE/3D mapping (Table 1). Patients without ICE/3D mapping use were more likely to have persistent and chronic AF diagnosis (persistent AF, without ICE/3D mapping: 43.0%, with ICE/3D mapping: 38.8%; chronic AF, without ICE/3D mapping: 9.0%, with ICE/3D mapping: 1.0%, aSMD: 0.435) during index, were more likely to have a high Elixhauser score (4 and above, without ICE/3D mapping: 81.3%, with ICE/3D mapping: 60.1%, aSMD: 0.478) and CHA2DS2-VASc score (4 and above, without ICE/3D mapping: 69.9%, with ICE/3D mapping: 44.8%, aSMD: 0.525). However, the two cohorts were well balanced on all study covariates after weighting (aSMD <0.1) (Table 1).
| Pre-weighted | Post-weighted | |||||
|---|---|---|---|---|---|---|
| Without IC/3D mapping, N (%) | With ICE/3D mapping, N (%) | aSMD | Without ICE/3D mapping, % | With ICE/3D mapping, % | aSMD | |
| 35,490 | 170,762 | |||||
| Age | 0.406 | 0.046 | ||||
| Mean (SD) | 76.13 (6.89) | 72.80 (4.83) | 73.85 (6.71) | 73.07 (4.90) | ||
| 66–74 | 16,398 (46.2%) | 112,603 (65.9%) | 65.1% | 62.9% | ||
| 75+ | 19,092 (53.8%) | 58,159 (34.1%) | 34.9% | 37.1% | ||
| Sex | 0.226 | 0.035 | ||||
| Male | 16,384 (46.2%) | 97,989 (57.4%) | 57.4% | 55.7% | ||
| Female | 19,106 (53.8%) | 72,773 (42.6%) | 42.6% | 44.3% | ||
| Race | 0.006 | 0.001 | ||||
| White | 32,937 (92.8%) | 158,746 (93.0%) | 92.9% | 92.9% | ||
| Non-white | 2553 (7.2%) | 12,016 (7.0%) | 7.1% | 7.1% | ||
| Region | 0.230 | 0.022 | ||||
| Midwest | 6916 (19.6%) | 34,715 (20.3%) | 19.5% | 20.1% | ||
| Northeast | 6401 (18.0%) | 25,130 (14.7%) | 15.5% | 15.3% | ||
| South | 17,346 (48.9%) | 73,881 (43.3%) | 45.1% | 44.3% | ||
| West | 4782 (13.5%) | 37,036 (21.7%) | 19.9% | 20.3% | ||
| AF type during index | 0.435 | 0.014 | ||||
| Paroxysmal | 13,946 (39.3%) | 90,584 (53.0%) | 51.0% | 50.9% | ||
| Persistent | 15,267 (43.0%) | 66,294 (38.8%) | 39.7% | 39.7% | ||
| Chronic | 3201 (9.0%) | 1554 (1.0%) | 2.1% | 2.0% | ||
| Unspecified | 3076 (8.7 %) | 12,330 (7.2%) | 7.2% | 7.4% | ||
| Electrical cardioversion | 7138 (20.1%) | 43,938 (25.7%) | 0.134 | 27.1% | 24.9% | 0.050 |
| AF-related hospitalization | 7206 (20.3%) | 23,523 (13.8%) | 0.174 | 14.9% | 14.9% | 0.001 |
| CTS status (with on-site CTS) | 34,764 (98.0%) | 168,212 (98.5%) | 0.042 | 98.7% | 98.5% | 0.018 |
| Elixhauser score | 0.478 | 0.037 | ||||
| 0–3 | 6,640 (18.7%) | 68,089 (39.9%) | 38.2% | 36.4% | ||
| 4 and above | 28,850 (81.3%) | 102,673 (60.1%) | 61.8% | 63.6% | ||
| CHA2DS2-VASc score | 0.525 | 0.035 | ||||
| 0–3 | 10,672 (30.1%) | 94,248 (55.2%) | 52.9% | 51.2% | ||
| 4 and above | 24,818 (69.9%) | 76,514 (44.8%) | 47.1% | 48.8% | ||
| Cardiomyopathy | 7976 (22.5%) | 17,816 (10.4%) | 0.329 | 11.8% | 12.3% | 0.015 |
| Sleep apnea | 8127 (22.9%) | 35,744 (20.9%) | 0.048 | 21.8% | 21.3% | 0.011 |
3D: Three dimensional; AF: Atrial fibrillation; aSMD: Absolute standardized mean difference; CTS: Cardiothoracic surgery; ICE: Intracardiac echocardiography; SD: Standard deviation.
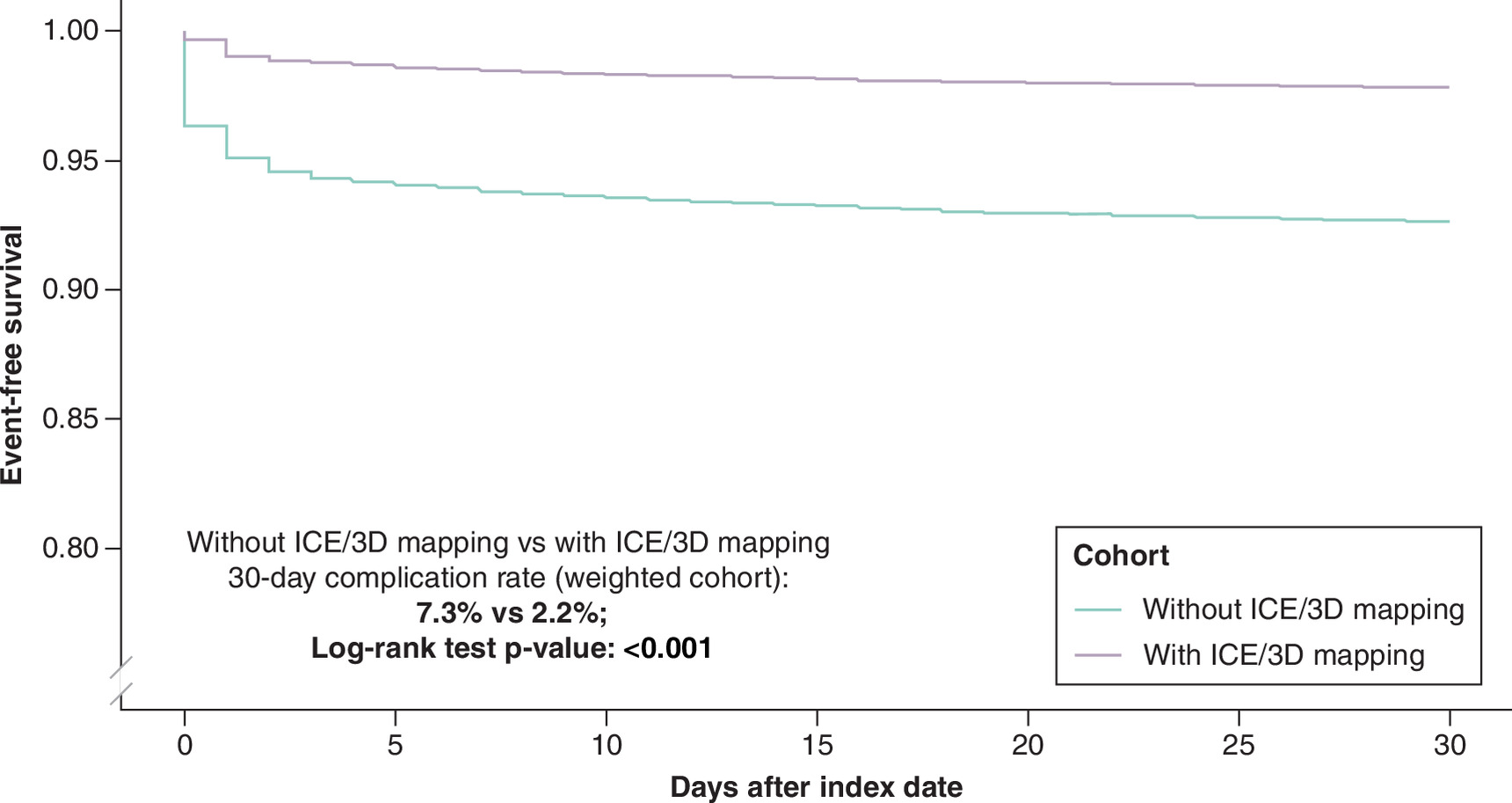
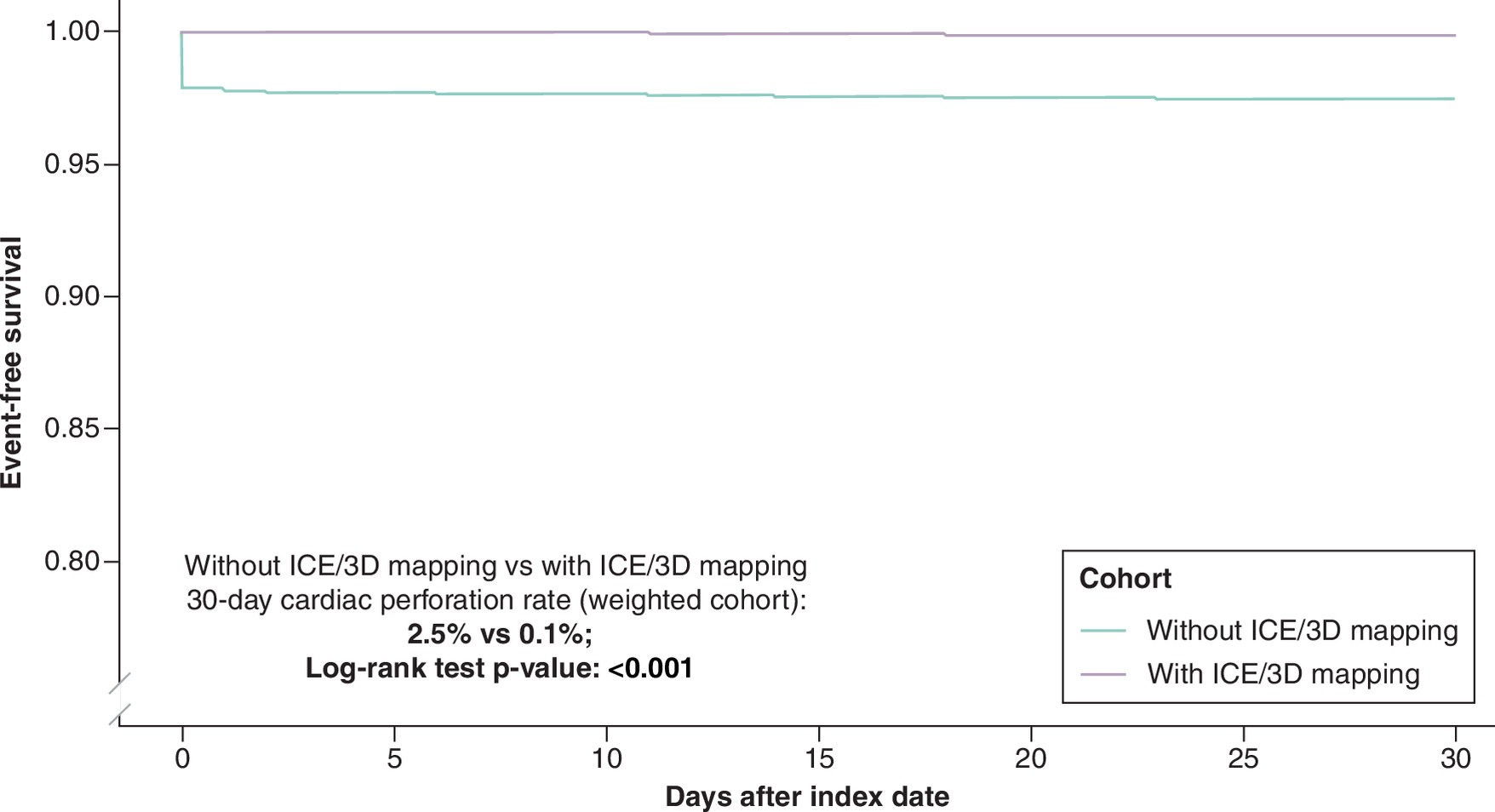
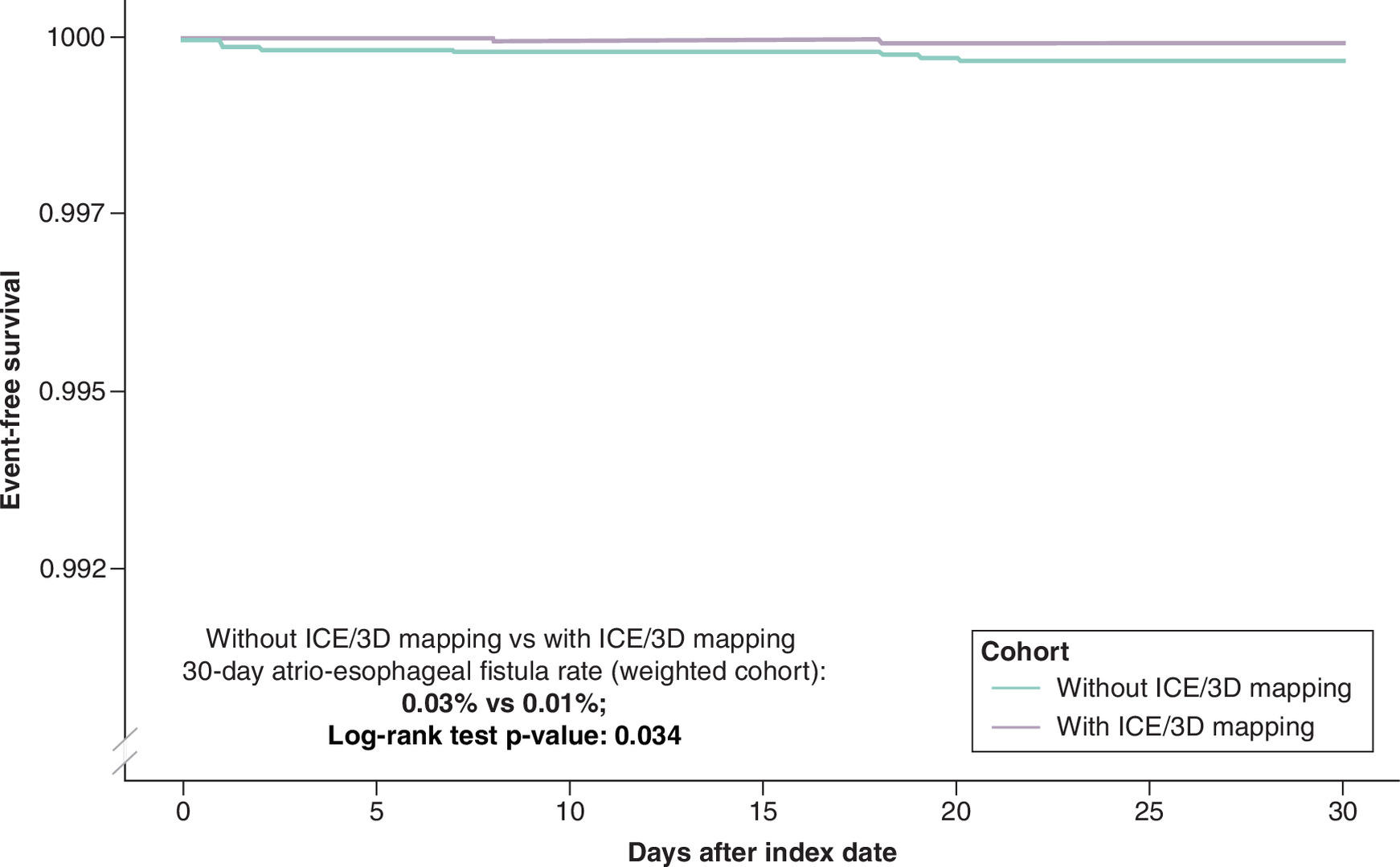
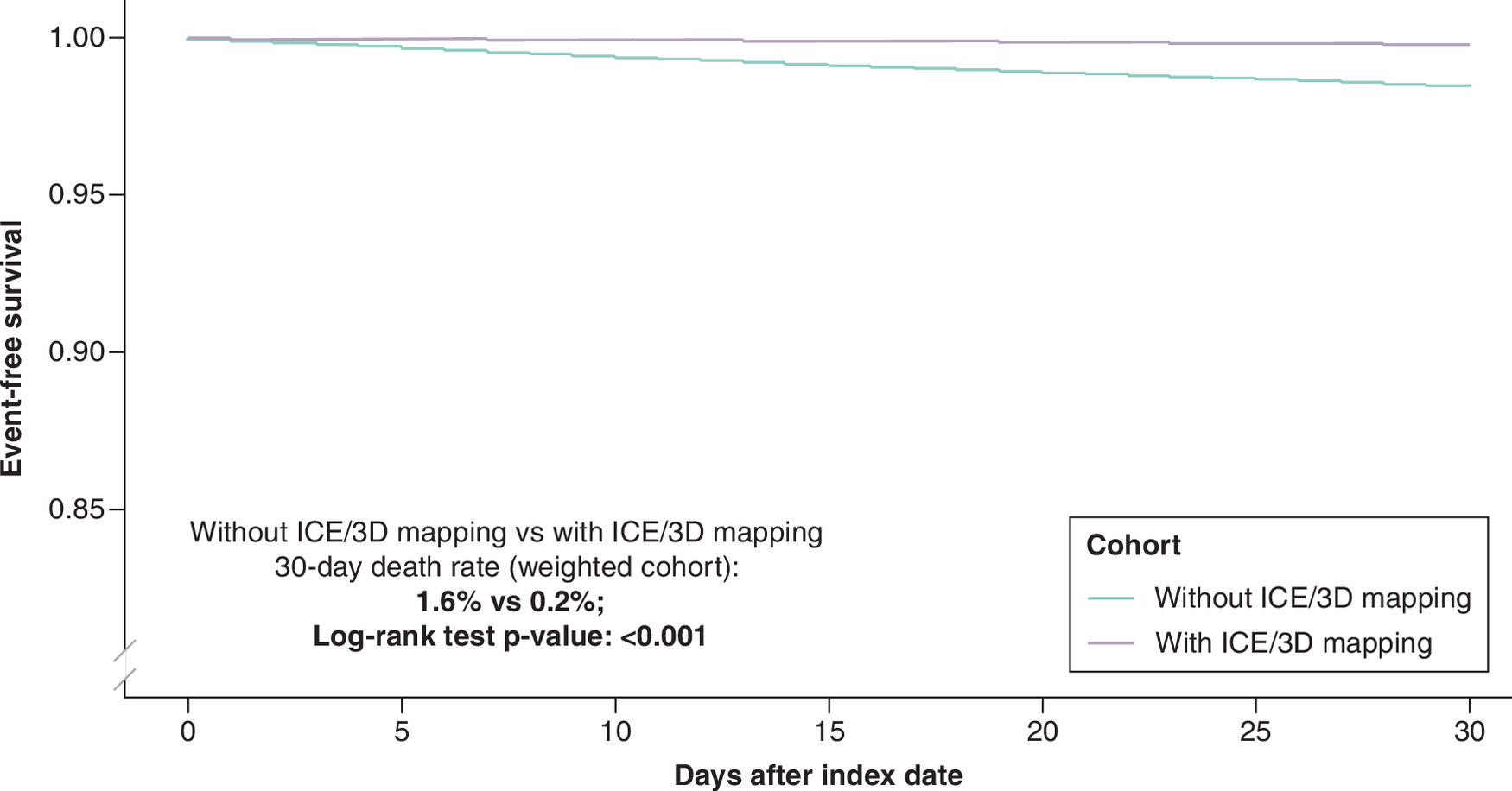
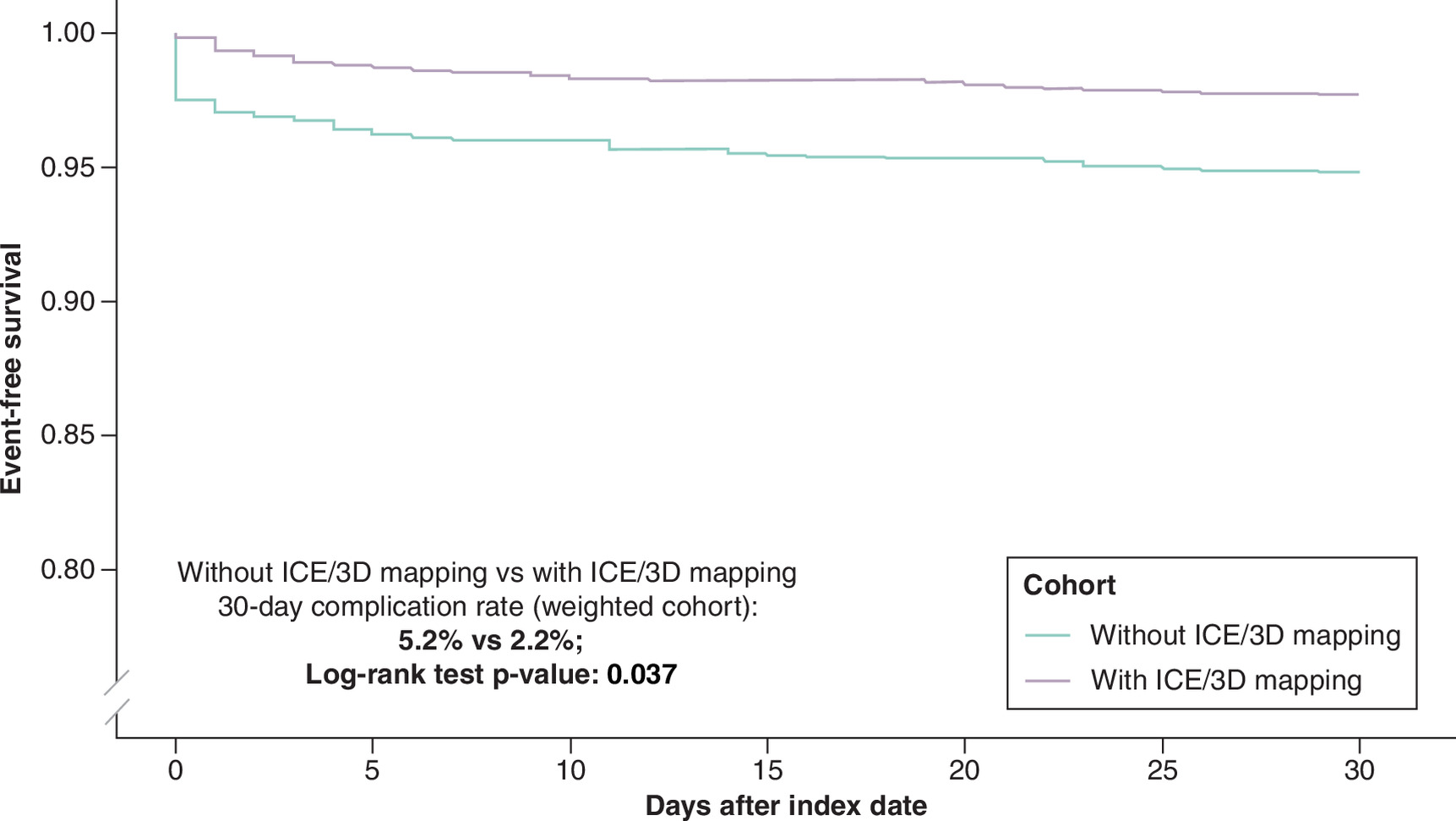
As shown in Figure 2, the 30-day incidence of overall complications was significantly higher for patients who had CA without ICE/3D mapping versus those who had CA with ICE/3D mapping (7.3% vs 2.2%, log-rank test p < 0.001). Weighted Cox regression model revealed that patients who had CA without ICE/3D mapping were ∼3.5-times more likely to have 30-day complications versus those who underwent ablation with ICE/3D mapping (HR: 3.507; 95% CI: 3.307–3.720, p < 0.001). As per secondary outcome assessment, patients undergoing CA without ICE/3D mapping had significantly higher risk of cardiac perforation as compared with those in the ICE/3D mapping group (2.5% vs 0.1%, log-rank test p < 0.001 [Figure 3]; HR: 19.840, 95% CI: 16.910–23.280, p < 0.001). Patients who underwent CA without ICE/3D mapping were approximately 3.5-times more likely to experience atrio-esophageal fistula versus those in the ICE/3D mapping group (0.03% vs 0.01%, log-rank test p = 0.03 [Figure 4]; HR: 3.454; 95% CI: 1.553–7.683, p = 0.002). The 30-day risk of death was significantly higher for those undergoing CA without ICE/3D mapping use versus those in the ICE/3D mapping group, with patients in the former group having ∼seven-times higher risk of death than those in the latter group (1.6% vs 0.2%, log-rank test p < 0.001 [Figure 5]; HR: 7.274, 95% CI: 6.359–8.321, p < 0.001). The results after BH correction remained significant for all study outcomes.
When restricting the cohort to patients who underwent CA in the hospital without on-site CTS back-up (as part of sub-analysis), 3276 patients were identified (726 in the without ICE/3D mapping cohort and 2550 in the ICE/3D mapping cohort). Study results in this cohort of patients undergoing CA in hospitals without on-site CTS backup were consistent with those of the full cohort (Figure 6 & Supplementary Figures 1 & 2). Cox models demonstrated that in this sub-analysis cohort, those who had ablation without ICE/3D mapping were at a significantly higher risk of 30-day complications (HR: 2.347, 95% CI: 1.288–4.278, p = 0.005), cardiac perforation (HR: 41.400, 95% CI: 7.778–220.400, p < 0.001) and death (HR: 9.636, 95% CI: 4.063–22.860, p < 0.001) versus those in the ICE/3D mapping group. No atrio-esophageal fistula case was observed in both groups.
Discussion
In this retrospective cohort study, AF patients who underwent CA without using ICE and 3D mapping had a significantly higher risk of overall complications, cardiac perforation, atrio-esophageal fistula, and all-cause death compared with patients who had ablation with ICE and 3D mapping use. Results were consistent when restricting our sample to a cohort of patients who had ablation procedure in hospitals without onsite CTS backup. To the best of our knowledge, this is the first study to examine the safety impact of concurrent ICE and 3D mapping use among patients with AF undergoing an ablation procedure.
A few studies have reported ICE use to be associated with better procedural related outcomes, particularly reduction in complication occurrences. In their retrospective analysis of a US national inpatient database, Isath et al. found the use of ICE during CA to be associated with a significant reduction in complications (9.35% vs 10.41%, HR: 0.48 [95% CI: 0.44–0.51], p < 0.0001) and in-hospital mortality (0.11% vs 0.54%, HR: 0.72 [95% CI: 0.71–0.73], p < 0.0001) [21]. Another study by Deshpande et al. found ICE use to be associated with a 12% lower risk of readmission in 90 days post CA period (HR: 0.88 [95% CI: 0.83–0.94], p < 0.0001) [24]. In their study of Medicare beneficiaries, Friedman et al. found that patients without ICE use during CA procedure had ∼five-times increased risk of experiencing cardiac perforation (odds ratio [OR]: 4.85; 95% CI: 4.11–5.71; p < 0.0001) for CA procedure than those who had ICE use during ablation procedure [22]. A recent analysis of US privately insured nonelderly patients found ICE use to be associated with 50% lower risk of 30-day complications (2.9% vs 5.8%; HR: 0.50 [95% CI: 0.34–0.72]) versus no ICE use [23]. With real-time visualization of the left atrium, ICE use enables accurate identification of key anatomical locations during the ablation, guidance of transseptal puncture, determination of exact transseptal sheath location, assessment of catheter contact with cardiac tissue, and rapid detection of early manifestations of complications such as pericardial effusions, tamponades, thrombosis and pulmonary vein stenosis [18,19]. In light of this, the recent 2024 European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society (LAHRS) expert consensus statement on catheter and surgical ablation of atrial fibrillation lists ICE use as important for early diagnosis and prevention of cardiac tamponade [17].
Advanced 3D mapping systems allow continuous visualization of the ablation catheter and may contribute to the safety of the procedure. There has also been emerging evidence demonstrating the benefit of using 3D mapping technique with or without ICE use during CA procedure, including reduced procedure time, fluoroscopy time and fluoroscopy dose [26–30]. Creating a 3D cardiac map allows for identification of patient specific anatomy, the substrate for arrhythmia and provides the ability to accurately track ablation sites. This provides valuable information for the physician in order to avoid complications such as PV stenosis, perforation, phrenic nerve or esophageal injury. In the 2019 APHRS Expert Consensus Statement on three-dimensional mapping systems for tachycardia developed in collaboration with HRS, EHRA and LAHRS, 3D mapping has been recommended for use during AF ablation procedures for “careful identification of the pulmonary vein (PV) ostia and left atrial geometry to avoid ablation within the PVs, and obtain durable PV ablation”, and “ to assess for line completeness if linear ablation lesions are applied” [25]. The integration of real-time ICE imaging guidance and EAM system has been reported to be effective and safe [37–39]. The combined use of the two imaging modalities enables visualization of a comprehensive 3D left atrial anatomy and reconstruction of all relevant anatomical structures for AF ablation [37–39]. Given these demonstrated benefits, it was not surprising to see significantly higher risk of complications associated nonuse of ICE and 3D mapping system in our study. Recently, use of EAM has been reduced in some ablation workflows employing contemporary pulsed field ablation (PFA) technologies. This trend may be attributed to the nature of first-generation PFA devices, the initial lack of readily available integration across mapping systems, as well as the higher cost of first-generation PFA technologies. Until larger studies involving PFA with or without use of EAM and ICE are available, our results suggest that use of EAM likely remains important as a part of a comprehensive workflow strategy to minimize adverse events.
Notably, CA procedures for AF are increasingly being performed in smaller hospitals [40], which may lack CTS backup. In the event of rare but potentially severe complications (such as cardiac perforation) following a CA procedure, immediate intervention might be required, including cardiac surgery, pericardiocentesis, or vascular repair [17,41]. AF ablation is currently recommended to “only be performed in hospitals equipped or prepared to manage these types of emergencies with access to emergency surgical support when required” [17]. In our sub-analysis of patients undergoing ablation in hospitals without CTS backup, non use of ICE and 3D mapping was associated with significantly worse patient outcomes, highlighting the importance of these technologies in a non-CTS backup setting. The ASCs are increasingly being considered as a setting of care for ablation procedures for Medicare beneficiaries, with some ASCs already expanding these procedures to commercially insured patients. As physicians evaluate appropriate clinical strategies and ablation workflows to mitigate adverse events in ASCs, our results emphasize the importance of electroanatomic mapping and ICE, even in lower-acuity environments.
Limitations
This study has some limitations. First, due to the retrospective nature of our analysis, we can only arrive at an association and not causation, as additional confounding factors may not be accounted for despite our best attempts. Certain confounders (e.g. therapeutic catheter used during ablation, ablation energy/technique, surgeon experience, hospital characteristics, medication use, etc.) could not be controlled in our study because the information was not available in the Medicare SAF database. Second, this study solely investigated the effectiveness of using both ICE and 3D mapping together, without considering the impact of each technique when applied independently. It is possible that the beneficial effect observed in this study were primarily attributable to one technique versus the other. However, to quantify the separate impact of ICE and 3D mapping is beyond the scope of the current study. Third, complication events may be underestimated as physician office encounter information was not available in Medicare SAF database. However, given the low likelihood of procedure-related complications being treated in an office setting, this impact is likely to be negligible. Complication events may also be misclassified because the identification of those events or exposures relied on diagnosis procedure codes. Fourth, the source population in the Medicare SAFs database is primarily representative of US Medicare fee-for-service patients. As such, our results may not be generalizable to older AF patients enrolled in Medicare Advantage program or individuals without insurance as well as to the younger adult AF patients undergoing ablation procedures. In addition, as the reason of death information is not available in the Medicare SAF database, our analyses of all-cause death may have overestimated the direct impact of the ICE and 3D mapping used during CA procedure on noncardiac mortality.
Conclusion
The absence of ICE and 3D mapping during cardiac CA procedures for AF was associated with higher rates of complications (including cardiac perforation and atrio-esophageal fistula) and death. As CA increasingly becomes the mainstay treatment for AF and expands to smaller hospitals, ICE and 3D mapping are likely to remain key drivers of improved patient outcomes in lower acuity settings.
Summary points
•
Using the Medicare Database, this retrospective cohort study assessed data of older AF patients (≥65 years of age) who underwent catheter ablation (CA) procedure and compared the complication outcomes between patients without ICE/3D mapping during CA versus those patients with ICE/3D mapping.
•
Study results demonstrated that patients who underwent CA without ICE/3D mapping use were ∼3.5-times more likely to have 30-day any complication versus those who had CA with ICE/3D mapping.
•
The incidence of cardiac perforation, atrio-esophageal fistula, and death were significantly higher among patients who underwent CA without ICE/3D mapping versus those who had CA with ICE/3D mapping.
•
Results were consistent when restricting our sample to a cohort of patients who had ablation procedure in hospitals without on-site cardiothoracic surgery backup.
Author contributions
All authors were responsible for study conception and design; R Khanna and Y Rong were responsible for acquisition of data; R Khanna and Y Rong were responsible for data analysis. All authors contributed to draft review and revision of the manuscript.
Financial disclosure
This study was funded by Johnson & Johnson (NJ, USA).
Competing interests disclosure
R Khanna, T Wei, K Corriveau and Y Rong are employees of Johnson & Johnson. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This analysis of the Medicare SAFs database was conducted under exemption from Institutional Review Board oversight for US-based studies using de-identified healthcare records, as dictated by Title 45 Code of Federal Regulations (45 CFR 46.101(b)(4)).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary figures.docx)
- Download
- 193.42 KB
Reference
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Khavjou O, Phelps D, Leib A. Projections of Cardiovascular Disease Prevalence and Costs: 2015–2035. American Heart Association, TX, USA (2016).
2.
Kornej J, Borschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ. Res. 127, 4–20 (2020).
3.
Morseth B, Geelhoed B, Linneberg A et al. Age-specific atrial fibrillation incidence, attributable risk factors and risk of stroke and mortality: results from the MORGAM Consortium. Open Heart 8(2), e001624 (2021).
4.
Wasmer K, Eckardt L, Breithardt G. Predisposing factors for atrial fibrillation in the elderly. J. Geriatr. Cardiol. 14(3), 179–184 (2017).
5.
Parks AL, Frankel DS, Kim DH et al. Management of atrial fibrillation in older adults. BMJ 386, e076246 (2024).
6.
Pappone C, Augello G, Sala S et al. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation: the APAF study. J. Am. Coll. Cardiol. 48, 2340–2347 (2006).
7.
Jaïs P, Cauchemez B, Macle L et al. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. Circulation 118, 2498–2505 (2008).
8.
Wilber DJ, Pappone C, Neuzil P et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA 303, 333–340 (2010).
9.
Stabile G, Bertaglia E, Senatore G et al. Catheter ablation treatment in patients with drug-refractory atrial fibrillation: a prospective, multi-centre, randomized, controlled study (catheter ablation for the cure of atrial fibrillation study). Eur. Heart J. 27, 216–221 (2006).
10.
Mont L, Bisbal F, Hernández-Madrid A et al. Catheter ablation vs. antiarrhythmic drug treatment of persistent atrial fibrillation: a multicentre, randomized, controlled trial (SARA study). Eur. Heart J. 35, 501–507 (2014).
11.
Saglietto A, Gaita F, De Ponti R, De Ferrari GM, Anselmino M. Catheter ablation vs. anti-arrhythmic drugs as first-line treatment in symptomatic paroxysmal atrial fibrillation: a systematic review and meta-analysis of randomized clinical trials. Front. Cardiovasc. Med. 8, 664647 (2021).
12.
Joglar JA, Chung MK, Armbruster AL et al; Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 149(1), e1–e156 (2024).
13.
Asad ZUA, Yousif A, Khan MS, Al-Khatib SM, Stavrakis S. Catheter ablation versus medical therapy for atrial fibrillation: a systematic review and meta-analysis of randomized controlled trials. Circ. Arrhythm Electrophysiol. 12(9), e007414 (2019).
14.
Mark DB, Anstrom KJ, Sheng S et al; CABANA Investigators. Effect of catheter ablation vs medical therapy on quality of life among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA 321(13), 1275–1285 (2019).
15.
Marrouche NF, Brachmann J, Andresen D et al; CASTLE-AF Investigators. Catheter ablation for atrial fibrillation with heart failure. N. Engl. J. Med. 378(5), 417–427 (2018).
16.
Packer DL, Piccini JP, Monahan KH et al; CABANA Investigators. Ablation versus drug therapy for atrial fibrillation in heart failure: results from the CABANA trial. Circulation 143(14), 1377–1390 (2021).
17.
Tzeis S, Gerstenfeld EP, Kalman J et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 26(4), euae043 (2024).
18.
Marrouche NF, Martin DO, Wazni O et al. Phased-array intracardiac echocardiography monitoring during pulmonary vein isolation in patients with atrial fibrillation: impact on outcome and complications. Circulation 107(21), 2710–2716 (2003).
19.
Dello Russo A, Russo E, Fassini G et al. Role of intracardiac echocardiography in atrial fibrillation ablation. J. Atr. Fibrillation 5(6), 786 (2013).
20.
Goya M, Frame D, Gache L et al. The use of intracardiac echocardiography catheters in endocardial ablation of cardiac arrhythmia: meta-analysis of efficiency, effectiveness, and safety outcomes. J. Cardiovasc. Electrophysiol. 31(3), 664–673 (2020).
•• This meta-analysis found that use of intracardiac echocardiography (ICE) in the cardiac arrhythmias ablation was associated with significantly lower fluoroscopy time, fluoroscopy dose and shorter procedure time versus ablation without ICE use; and these efficiency gains did not compromise the clinical effectiveness or safety of the ablation procedure.
21.
Isath A, Padmanabhan D, Haider SW et al. Does the use of intracardiac echocardiography during atrial fibrillation catheter ablation improve outcomes and cost? A nationwide 14-year analysis from 2001 to 2014. J. Interv. Card. Electrophysiol. 61(3), 461–468 (2021).
• Using a US national in-patient sample database, results of this study demonstrated that use of ICE during atrial fibrillation (AF) ablation was associated with lower in-hospital mortality and procedural complications, shorter length of stay (LOS) but an increased cost of hospitalization.
22.
Friedman DJ, Pokorney SD, Ghanem A et al. Predictors of cardiac perforation with catheter ablation of atrial fibrillation. JACC Clin. Electrophysiol. 6(6), 636–645 (2020).
23.
Pimentel RC, Rahai N, Maccioni S, Khanna R. Differences in outcomes among patients with atrial fibrillation undergoing catheter ablation with versus without intracardiac echocardiography. J. Cardiovasc. Electrophysiol. 33(9), 2015–2047 (2022).
• Using a US commercial claims database, results of this study demonstrates that use of ICE during AF ablation was associated with lower incidence of peri-procedural complications and repeat ablation in 12 months post ablation.
24.
Deshpande S, Sawatari H, Ahmed R et al. Impact of intracardiac echocardiography on readmission morbidity and mortality following atrial fibrillation ablation. J. Cardiovasc. Electrophysiol. 33(12), 2496–2503 (2022).
25.
Kim YH, Chen SA, Ernst S et al. 2019 APHRS expert consensus statement on three-dimensional mapping systems for tachycardia developed in collaboration with HRS, EHRA, and LAHRS. J. Arrhythm. 36(2), 215–270 (2020).
26.
Shurrab M, Laish-Farkash A, Lashevsky I et al. Three-dimensional localization versus fluoroscopically only guided ablations: a meta-analysis. Scand. Cardiovasc. J. 47(4), 200–209 (2013).
27.
Obeng-Gyimah E, Nazarian S. Advancements in imaging for atrial fibrillation ablation: is there a potential to improve procedural outcomes? J. Innov. Card. Rhythm Manag. 11(7), 4172–4178 (2020).
28.
Hofer D, Steffel J, Duru F et al. Feasibility, efficiency, and safety of zero-fluoroscopy catheter interventions for right-sided cardiac arrhythmias using only electroanatomic mapping. Cardiology 147(5–6), 547–556 (2022).
• In this single center retrospective cohort study, the results demonstrates that it is a feasible, efficient and safe approach to use only electroanatomic mapping without additional invasive procedures to diagnose and treat right-sided cardiac arrhythmias.
29.
Debreceni D, Janosi K, Bocz B et al. Zero fluoroscopy catheter ablation for atrial fibrillation: a systematic review and meta-analysis. Front. Cardiovasc. Med. 10, 1178783 (2023).
30.
Huang HD, Abid QU, Ravi V et al. Meta-analysis of pulmonary vein isolation ablation for atrial fibrillation conventional vs low- and zero-fluoroscopy approaches. J. Cardiovasc. Electrophysiol. 31(6), 1403–1412 (2020).
31.
Friedman DJ, Pokorney SD, Khanna R et al. Catheter ablation of atrial fibrillation with and without on-site cardiothoracic surgery. J. Am. Coll. Cardiol. 73(19), 2487–2489 (2019).
32.
Elixhauser A, Steiner C, Harris DR et al. Comorbidity measures for use with administrative data. Med. Care 36(1), 8–27 (1998).
33.
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest 137(2), 263–272 (2010).
34.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
35.
Desai RJ, Franklin JM. Alternative approaches for confounding adjustment in observational studies using weighting based on the propensity score: a primer for practitioners. BMJ 367, l5657 (2019).
36.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. Series B Stat. Methodol. 57, 289–300 (1995).
37.
Liu GA, Shao B, Wu W et al. Safety and efficacy of intracardiac echocardiography-guided zero-fluoroscopy ablation in atrial fibrillation patients: a comparative study of high-power short-duration and low-power long-duration strategies. Front. Cardiovasc. Med. 11, 1510889 (2024).
38.
Antolič B, Kajdič N, Vrbajnščak M, Jan M, Žižek D. Integrated 3D intracardiac ultrasound imaging with detailed pulmonary vein delineation guided fluoroless ablation of atrial fibrillation. Pacing Clin. Electrophysiol. 44(9), 1487–1496 (2021).
39.
Jan M, Žižek D, Kuhelj D et al. Combined use of electro-anatomic mapping system and intracardiac echocardiography to achieve zero-fluoroscopy catheter ablation for treatment of paroxysmal atrial fibrillation: a single centre experience. Int. J. Cardiovasc. Imaging 36(3), 415–422 (2020).
40.
Cheung JW, Yeo I, Cheng EP et al. Inpatient hospital procedural volume and outcomes following catheter ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 31(8), 1908–1919 (2020).
41.
Wu SJ, Fan YF, Chien CY. Surgical strategies for cardiac perforation after catheter ablation or electrophysiology study. Int. Heart J. 62(6), 1257–1264 (2021).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 7 February 2026
Accepted: 5 June 2026
Published online: 22 June 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Use of intracardiac echocardiography and three-dimensional mapping during catheter ablation for atrial fibrillation is associated with reduced complications: a retrospective analysis of United States Medicare Fee-For-Service Database. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0037
Export citation
Select the citation format you wish to export for this article or chapter.