Matching-adjusted indirect comparison of acoltremon ophthalmic solution 0.003% and cyclosporine 0.05% ophthalmic emulsion for increased tear production in patients with dry eye disease
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Dry eye disease (DED) is a chronic, multifactorial condition arising through loss of tear film and ocular surface homeostasis. Treatment aims to restore natural tear production and normalize ocular surface homeostasis. Several prescription medications are available in the US that increase tear production in patients with DED. In the absence of head-to-head trials, this study employed a matching-adjusted indirect comparison (MAIC) approach to estimate the comparative tear production efficacy of acoltremon 0.003% and cyclosporine 0.05% for the treatment of DED. Materials & methods: MAICs were conducted for the key outcome of categorized Schirmer test score (STS), where higher values indicate greater tear production. Patient data were available for acoltremon 0.003% (from COMET-2 and COMET-3 trials) and summary level data for cyclosporine 0.05%. Populations were matched on clinically relevant variables including age, race, sex and anesthetized categorized STS. The primary analysis compared mean change from baseline (CFB) categorized STS at day 90. An exploratory analysis investigated earlier onset of tear production (day 14) attributed to acoltremon 0.003% compared with the earliest available data (day 90) for cyclosporine 0.05%. Results: After all adjustments, a greater mean CFB categorized STS was observed for acoltremon 0.003% compared with cyclosporine 0.05% (mean difference [MD]: 1.62 categories, 95% CI: 1.42–1.83, p < 0.001) at day 90. The exploratory analysis also demonstrated a greater mean CFB categorized STS for day 14 acoltremon 0.003% compared with day 90 cyclosporine 0.05% (MD: 1.62 categories, 95% CI: 1.42–1.82, p < 0.001). Conclusion: Our findings suggest that acoltremon 0.003% may provide a greater increase in tear production relative to cyclosporine 0,05% at day 90, with exploratory findings suggesting similar results at day 14. As this was an unanchored MAIC, results may be influenced by residual confounding from unmeasured differences between trials.
Plain language summary
A statistical comparison of two prescription eye drops (acoltremon 0.003% and cyclosporine 0.05%) for increasing tear production in patients with eye disease.
What is the article about?
Dry eye disease (DED) is generally associated with a deficiency in the quantity and/or quality of tears. We compared how well acoltremon 0.003% and cyclosporine 0.05% increase tear production in adults with DED.
What was the methodology used?
As there are no direct comparison trials between acoltremon 0.003% and cyclosporine 0.05%, we used a matching-adjusted indirect comparison approach using patient-level data for acoltremon 0.003% and published population data for cyclosporine 0.05%. This method reweights individual patient data from the acoltremon 0.003% trials to match published summary cyclosporine 0.05% data. This ensures the two groups are as similar as possible for a fair comparison. A categorized Schirmer test score was used as a measure of tear production, and we considered the average difference in the change from baseline in categorized Schirmer’s test result at day 90 for each treatment as the main end point in this analysis.
What were the results?
Our results suggest that after 90 days on the therapies, patients using acoltremon 0.003% had significantly greater tear production than patients using cyclosporine 0.05%, with a mean difference of 1.62 categories for the Schirmer test score.
Why is this important?
These results support acoltremon 0.003% as a valuable treatment option for the signs and symptoms of DED.
Dry eye disease (DED) is a chronic, multifactorial disease, affecting millions globally, including an estimated 38 million patients in the US [1]. Recently, the Dry Eye Workshop III of the Tear Film Ocular Society refined the definition of DED, broadening the concept of a loss of homeostasis to include the tear film in addition to the ocular surface: “Dry eye is a multifactorial, symptomatic disease characterized by a loss of homeostasis of the tear film and/or ocular surface, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities are etiological factors” [2]. This recognition of the negative consequences that an unstable and/or deficient tear film plays in the pathology of DED underscores the critical role of this dynamic biologic fluid in ocular surface health.
Dry eye disease, if not adequately treated, is associated with significant symptoms as well as ocular surface changes that can continue to worsen over time leading to impairment of daily living activities, particularly those requiring sustained visual focus, as well as a reduction in work productivity [3–7]. In addition, dry eye disease is associated with a substantial direct cost burden. In 2008, the estimated cost of managing DED in the US was $3.84 billion, while the societal burden was estimated at $55 billion US annually [8]. Between 2015 and 2016, per capita expenditures on Restasis prescription therapy in the US reached $1872.80, a significant increase compared with the 2007–2008 period (p < 0.001; 2016 USD) [9].
As the pathophysiology of DED is multifactorial, an opportunity exists to employ therapies of differing mechanisms of action. Inflammation has long been the primary therapeutic target for DED, with immunomodulatory medications such as various formulations of cyclosporine (i.e., Restasis [Abbvie], Cequa [Sun Ophthalmics], Vevye [Harrow], Ikervis [Santen]) [10–12] as well as lifitegrast (Xiidra [Bausch and Lomb]) [11,13] representing the largest therapeutic class of US FDA approved products. Although cyclosporine 0.05% (Restasis) is commonly used as a first-line prescription treatment, surveys of physician and patient satisfaction and real-world treatment patterns indicate suboptimal disease management due to factors such as inadequate symptom control and adverse effects [14–17]. In addition, real-world data indicate high rates of discontinuations associated with topical immunomodulators for DED [14,18].
To address these treatment gaps in combination with the growing appreciation that while not all dry eye is driven by inflammation, tear deficiency is generally a common denominator between all forms of DED [2], attention has recently turned to addressing other mechanisms aimed more directly at the tear film. Specifically, addressing tear deficiency based on either slowing evaporation (perfluorohexyloctane ophthalmic solution [Miebo; Bausch and Lomb]) [19] or stimulating basal tear production (varenicline nasal spray solution [Tyrvaya, Oyster Point Pharma]) [20]; have emerged as viable treatment alternatives [11].
In May of 2025, the US FDA approved acoltremon ophthalmic solution 0.003% (acoltremon 0.003%; Tryrptyr, Alcon Inc.) for the treatment of the signs and symptoms of DED [21]. Acoltremon is a selective agonist of transient receptor potential melastatin 8 (TRPM8) ion channels which are expressed on cold thermosensory nerve endings that innervate the cornea and upper eye lids [22,23]. TRPM8 receptors are considered key regulators of basal tear production and are stimulated by small reductions in ocular surface temperature such as what occurs during the interblink interval due to evaporative cooling [24]. Once stimulated, activation of the trigeminal nerve triggers basal tear production [25]. In the COMET-2 and COMET-3 Phase III pivotal trials, up to 59% of acoltremon 0.003% treated patients achieved an increase of 10 mm or more in unanesthetized Schirmer test scores (STS) on day 1 and similar magnitudes of tear production were consistently observed through day 90, yielding robust treatment differences from vehicle ranging from 26.7% to 43.8% (p < 0.0001) [26].
While there are existing international guidelines [11] and national consensus reports [27–30] for the treatment of DED, there is a lack of a universally agreed, comparative, treatment-selection algorithm that incorporates newly approved agents, such as acoltremon 0.003%. Compounding this lack of consensus that integrates the everchanging treatment landscape is the lack of head-to-head data comparing the relative efficacies of available treatment options, leaving the ability to objectively choose the best treatment option for a given patient difficult at best. In the absence of direct comparative trials, matching-adjusted indirect comparisons (MAICs) offer a robust method for estimating the relative efficacy of treatments using data from separate trials. MAIC leverages individual patient data from one trial and summary level data from another, reweighting the individual patient data so that the baseline characteristics of the populations are closely matched. MAICs are a useful tool for comparative research and provide valuable clinical insight when considering various treatment options [31]. The purpose of this study was to conduct an unanchored MAIC to estimate the comparative tear production efficacy of acoltremon 0.003% and cyclosporine 0.05%.
Materials & methods
Data sources
Phase III randomized, double-masked, vehicle-controlled trials supporting FDA approval of acoltremon 0.003% (COMET-2 [NCT05285644] and COMET-3 [NCT05360966] [26]) and cyclosporine 0.05% (pooled results from Trials -002 and -003 as reported in Sall et al. [32]) were included (Table 1). Individual patient data from COMET-2 and COMET-3 and summary-level data from the cyclosporine 0.05% trials were available.
| Trial NCT | Methods | Sample size | Key inclusion criteria | Key exclusion criteria |
|---|---|---|---|---|
| COMET-2 NCT05285644 | Phase III multicenter double-masked US | 230 patients randomized to acoltremon 0.003% BID 235 randomized to receive Vehicle | • ≥30 years old • DED diagnosis within 6 months • Used/desired use of artificial tears in previous 2 months • Both signs of DED in same eye: tCFS ≥ 2 to ≤ 15 based on mNEI with no one region >3 based on mNEI; anesthetized STT ≥ 2 and <10 mm/5 min • ≥50 on ODS-VAS • ≥50 on SANDE • Increase in signs/symptoms of DED based on CAE exposure: ≥1 point increase in ICSS based on Ora Calibra after 90-minute CAE exposure; Ora Calibra ODS ≥3 at ≥2 consecutive timepoints | • History/presence of ocular condition other than DED that would interfere with study results, safety of patients or require topical medication • History of ocular surgery within 1 year • Corneal transplant in either/both eyes • Use of contact lens within previous 7 days or planned use • Use of artificial tears within 2 h or planned use • Use of topical ocular anti-inflammatory or other medication within 30 days • Use of varenicline within 30 days |
| COMET-3 NCT05360966 | Phase III multicenter double-masked US | 232 patients randomized to acoltremon 0.003% BID 234 randomized to receive vehicle | ||
| Sall 2000 (Pooled analysis) | Phase III Multicenter Double-masked US | 293 randomized to receive Cyclosporine 0.05% BID† 292 randomized to receive vehicle | Moderate to severe DED diagnosis based on criteria: • Unanesthetized STT ≤ 5 mm/5 min (if result of 0 mm/5 min, then STT with nasal stimulation of >3 mm/5 min in same eye) • Sum of corneal and interpalpebral conjunctival staining ≥15 in same eye where corneal staining was ≥2 • Baseline OSDI of 0.1 with max of 3 ‘NA’ responses • ≥3 on SFES • Signs and symptoms present despite conventional management • Normal lid position and closure • Best-corrected ETDRS of +0.7 logMAR or better | • Presence/history of systemic or ocular condition interferes with study results • Current/recent use of topical ophthalmic or systemic medications that could affect DED • Required contact lens wear during study • Recent/anticipated use of punctal plugs • Occlusion of lacrimal puncta within 3 months • End-stage lacrimal gland disease (Schirmer reading with nasal stimulation of <3 mm/5 min) • DED due to destruction of conjunctival goblet cells or scarring • Did not meet moderate to severe DED criteria after 2 week run-in phase |
†
Only dosages that received regulatory approval were included in the MAIC. Sall 2000 [32] also reported on patients receiving cyclosporine 0.1% BID.
BID: Twice daily; CAE: Controlled adverse environment; DED: Dry eye disease; ETDRS: Early Treatment Diabetic Retinopathy Study; ICSS: Inferior corneal staining score; logMAR: Logarithm of the minimum angle of resolution; mNEI: Modified National Eye Institute; NA: Not applicable; NCT: National Clinical Trial; ODS: Ocular discomfort score; OSDI: Ocular Surface Disease Index; SANDE: Symptom assessment in dry eye; SFES: Subjective facial expression scale; STT: Schirmer test score; tCFS: Total corneal fluorescein staining; VAS: Visual analogue scale.
Feasibility assessment
A feasibility assessment was conducted to compare the COMET-2 and COMET-3 acoltremon 0.003% trials [26] and two pooled Phase III trials investigating cyclosporine 0.05% [32]. The trials were assessed for cross-trial heterogeneity in various domains, including trial design, eligibility criteria, patient baseline characteristics and outcome definitions. The NICE Single Technology Appraisal Checklist [33] was used to assess quality of the trials (Supplementary Table 1: Supplementary Materials).
A key consideration for an MAIC was to determine whether an anchored comparison using vehicle as a common comparator was feasible. DED trials are especially susceptible to variations in vehicle response based on the varied chemical composition and delivery form of the vehicle, both of which can contribute to a ‘treatment effect’ as was observed to differing degrees in both the acoltremon 0.003% and cyclosporine 0.05% Phase III trials [34]. As substantial differences were perceived to exist in both the inactive ingredients included in either vehicle formulation as well their delivery forms (ophthalmic solution vs ophthalmic emulsion for acoltremon 0.003% [21] and cyclosporine 0.05% [35], respectively), it was deemed unfeasible to consider a common vehicle comparator and therefore an unanchored MAIC was pursued.
Acoltremon 0.003% and cyclosporine 0.05% trials differed in the method used for measuring tear production; specifically, acoltremon 0.003% used an unanesthetized Schirmer’s test whereas cyclosporine 0.05% conducted the Schirmer’s test with anesthesia. To mitigate this methodological difference, the relative mean difference based on change from baseline (CFB) data were statistically compared. Additionally, reporting of STS differed between the two treatments as acoltremon 0.003% reported continuous data (0–35), whereas cyclosporine 0.05% utilized a categorical scale. Thus, STS from the acoltremon 0.003% trials’ individual patient data were converted to categories to align with those used in the cyclosporine 0.05% trials. Specifically, both anesthetized as well as pre-drop and post-drop unanesthetized STS for each COMET-2 and COMET-3 subject were assigned a category value of 1–5 based on the following category definitions: 1: <3 mm/5 min, 2: 3–6 mm/5 min, 3: 7–10 mm/5 min, 4: 11–14 mm/5 min and 5: >14 mm/5 min.
The primary outcome of this study was the mean CFB categorized STS at day 90. An exploratory analysis comparing the mean CFB categorized STS at day 14 for acoltremon 0.003% and mean CFB categorized STS at day 90 for cyclosporine 0.05% was also conducted, noting that there was no data with cyclosporin 0.05% reported earlier than day 90.
Comparison of other sign or symptom outcome measures was deemed not possible due to either lack of available data or substantial methodological differences between trials. This was particularly noteworthy for the assessment of total corneal staining where the modified NEI grading scheme was employed in the COMET trials [26], whereas the Oxford grading scheme was employed in the evaluation of cyclosporine 0.05% [32]. Assessment of patient reported symptoms were also conducted using vastly different questionnaires (i.e., symptom assessment in dry eye (SANDE) versus Ocular Surface Disease Index, in acoltremon 0.003% and cyclosporine 0.05%, respectively) [26,32].
Selection of treatment effect modifiers & prognostic factors
If left unadjusted, MAIC estimates can be biased due to the confounding effect of treatment effect modifiers and prognostic factors [36]. To reduce the potential for bias, baseline characteristics that were considered treatment effect modifiers or prognostic factors were identified based on evidence from the literature and/or assumed clinical relevance. This list was constrained by the factors commonly reported in the trials and included age, race, sex, baseline STS and eye dryness score. These factors were ranked in order of importance by independent clinical experts (Supplementary Table 2: Supplementary Materials). Covariates selected for adjustment included baseline age, race, sex and anesthetized categorized STS. As discussed above, other baseline characteristics, such as ocular surface staining and symptoms were not used as modifiers due to substantial methodological differences in clinical assessments performed and lack of reporting in the cyclosporine 0.05% trials.
Matching-adjusted indirect comparison
Individual patient data from COMET-2 and COMET-3 and summary-level data from the cyclosporine 0.05% trials were used. An unanchored MAIC was conducted to estimate the relative mean difference (MD) attributed to acoltremon 0.003% versus cyclosporine 0.05% with respect to mean CFB categorized STS. As such, only the absolute treatment effect, mean CFB categorized STS, from the treatment arms of each trial, were compared in the analysis.
Typically, the first step in an MAIC involves removing patients from the individual patient data who would not have been eligible for the comparator trials. In this case, comparator trial eligibility criteria were broader than COMET-2 and COMET-3, meaning all patients in COMET-2 and COMET-3 met eligibility criteria for the cyclosporine 0.05% trials. Therefore, no patients needed to be removed from the individual patient data based on eligibility criteria.
The acoltremon 0.003% patients in COMET-2 and COMET-3 individual patient data were reweighted using a method-of-moments propensity score model [37,38] such that the distribution of the identified baseline characteristics (age, race, sex and categorized STS) matched those reported in the cyclosporine 0.05% pooled analysis. Each adjustment factor was applied iteratively until all four factors were utilized in the primary analysis scenario. An unadjusted comparison was also conducted, in which individual patient data were not re-weighted to match comparator trials. The effective sample size was calculated to reflect the sample size of the weighted acoltremon 0.003% patients [37]. Standardized mean differences were calculated to assess the population differences between acoltremon 0.003% patients and cyclosporine 0.05% patients before and after weighting, with values between 0 and 0.1 indicating small differences, 0.1–0.2 indicating moderate differences and values > 0.2 indicating substantial differences [39].
The comparative effect estimate was the arithmetic mean difference in mean CFB categorized STS between acoltremon 0.003% and cyclosporine 0.05%. Mean differences were estimated by calculating the weighted mean CFB categorized STS for acoltremon 0.003% and subtracting the reported mean CFB categorized STS from the comparator study. The variances were estimated using a robust sandwich estimator and corresponding 95% CIs were reported. Statistical significance was defined using a two-tailed p-value of <0.05.
In addition, an exploratory analysis was conducted to evaluate the efficacy of acoltremon 0.003% at day 14, compared with cyclosporine 0.05% at the earliest timepoint reported which was day 90. These timepoints were selected to evaluate whether the efficacy observed with acoltremon 0.003% at day 14 was significantly greater than that achieved with cyclosporine 0.05% at day 90, thereby enabling comparative insight with respect to the speed of onset between the two treatments. While day 1 and 7 timepoints were available for acoltremon 0.003%, day 14 was chosen on the basis that day 14 was the timepoint selected for the primary end point characterizing tear production in the COMET Phase III pivotal trials.
All analyses were conducted with R version 4.3.1, following the methodological guidelines described by Signorovitch et al. 2012 and the NICE Decision Support Unit Technical Support Document 18 [36].
Results
Baseline characteristics before and after adjustment are shown in Table 2. Out of 462 total COMET-2 and COMET-3 patients in the treatment arms, 422 had available outcome data at day 90. Only patients with available outcome data were included in the MAIC. After adjustment for age, race, sex and categorized STS, acoltremon 0.003% trial populations closely matched the cyclosporine 0.05% trial populations (standardized mean difference = 0.00 for all baseline characteristics in the fully-adjusted population) with an effective sample size of 323 (77% of patients with data at day 90).
| Characteristic | Cyclosporine 0.05% treatment arm† | Acoltremon 0.003% treatment Arm (COMET-2 & COMET-3) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||||||||
| 1 Characteristic | 2 Characteristics | 3 Characteristics | 4 Characteristics (primary scenario) | ||||||||
| N = 293 | N = 422‡ | ESS = 388 | ESS = 348 | ESS = 335 | ESS = 323 | ||||||
| Stat | Stat | SMD | Stat | SMD | Stat | SMD | Stat | SMD | Stat | SMD | |
| Age, mean (SD) | 58.7 (13.9) | 61.5 (12.5) | 0.21 | 58.7 (13.9) | 0.00 | 58.7 (13.9) | 0.00 | 58.7 (13.9) | 0.00 | 58.7 (13.9) | 0.00 |
| Race, % | |||||||||||
| White | 86.3% | 75.6% | 0.27 | 72.1% | 0.36 | 86.3% | 0.00 | 86.3% | 0.00 | 86.3% | 0.00 |
| Non-white | 13.7% | 24.4% | 27.9% | 13.7% | 13.7% | 13.7% | |||||
| Sex, % | |||||||||||
| Female | 83.3% | 74.2% | 0.22 | 73.9% | 0.23 | 75.0% | 0.20 | 83.3% | 0.00 | 83.3% | 0.00 |
| Male | 16.7% | 25.8% | 26.1% | 25.0% | 16.7% | 16.7% | |||||
| Baseline categorized anesthetized Schirmer test score, mean (SD)§ | 2.1 (0.6) | 2.2 (0.7) | 0.19 | 2.2 (0.7) | 0.20 | 2.2 (0.6) | 0.21 | 2.2 (0.4) | 0.20 | 2.1 (0.6) | 0.00 |
†
Data sources: Sall 2000 [32].
‡
The pooled N for COMET-2 and COMET-3 treatment arm is 462. Mean CFB was based on available data as reported in the Clinical Study Reports, and only the treatment arms of the COMET trials were considered for the unanchored analysis. 422 COMET patients had results for unanesthetized STS at day 90.
§
Anesthetized STS in COMET-2 and COMET-3 were categorized to align with Sall 2000 on a 5-point scale as follows: 1 (<3 mm/5 min), 2 (3–6 mm/5 min), 3 (7–10 mm/5 min), 4 (11–14 mm/5 min) and 5 (>14 mm/5 min).
CFB: Change from baseline; ESS: Effective sample size; SD: Standard deviation; SMD: Standardized mean difference; Stat: Statistic; STS: Schirmer test score.
In the primary analysis, significantly greater tear production at day 90 was observed with acoltremon 0.003% compared with cyclosporine 0.05% based on a statistically significantly greater mean difference in mean CFB categorized STS in favor of acoltremon 0.003% compared with cyclosporine 0.05% (MD: 1.62 categories, 95% CI: 1.42–1.83, p < 0.001). This result was consistent across all adjustment scenarios as shown in Figure 1.
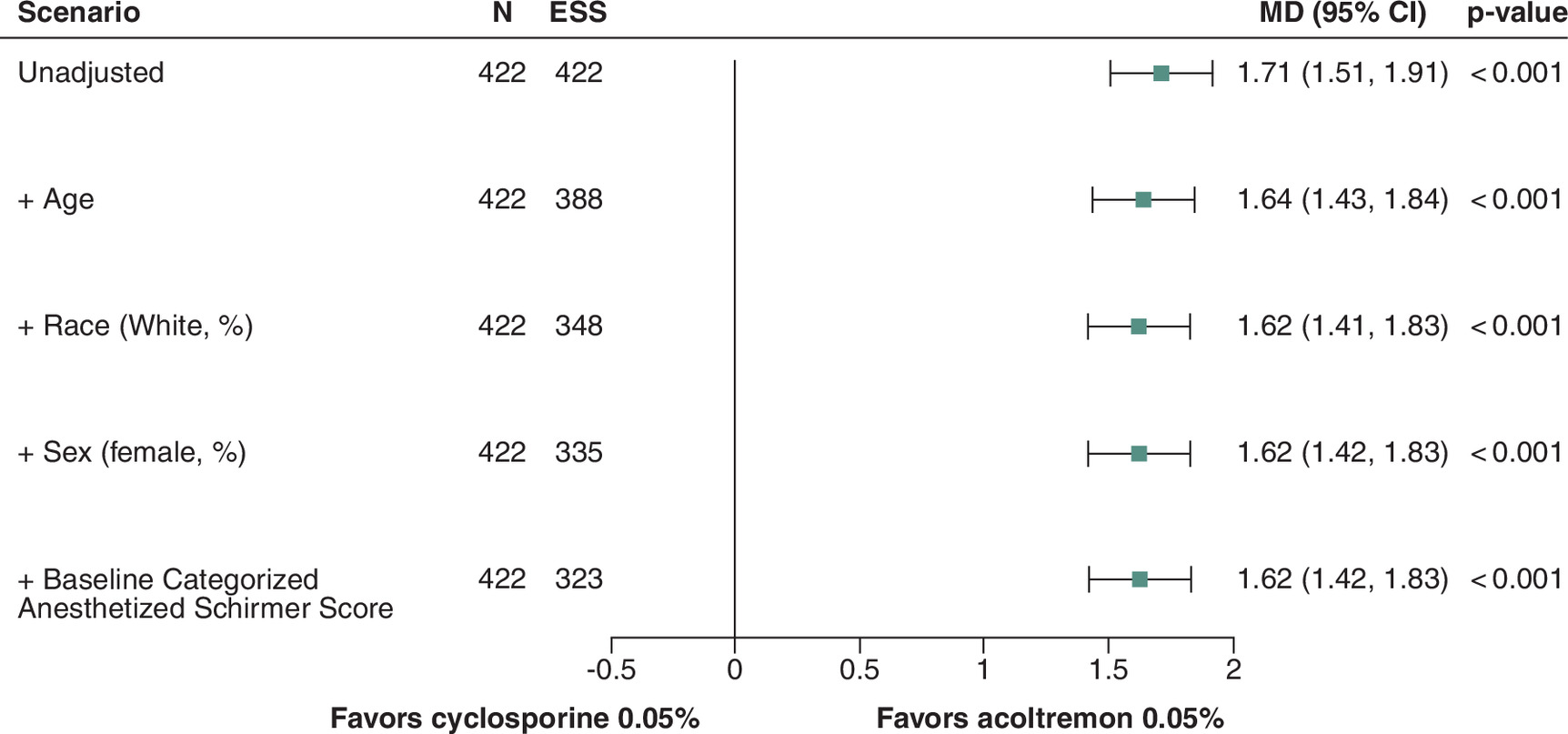
Figure 1. Matching-adjusted indirect comparison results: mean change from baseline in categorized Schirmer test score at day 90.
Mean difference > 0 implies that the comparison favors acoltremon 0.003%. Unanesthetized pre-drop to post-drop mean CFB from COMET-2 and COMET-3 was compared with anesthetized mean CFB from Sall 2000.
CFB: Change from baseline; ESS: Effective sample size; MAIC: Matching-adjusted indirect comparison; MD: Mean difference; STS: Schirmer test score.
Similarly, in the exploratory analysis after adjusting for the same four factors as the primary analysis, significantly greater tear production was observed in favor of acoltremon 0.003% at day 14 compared with cyclosporine 0.05% at day 90 (MD: 1.62 categories, 95% CI: 1.42–1.82, p < 0.001). This result was consistent across all adjustment scenarios as shown in Figure 2.
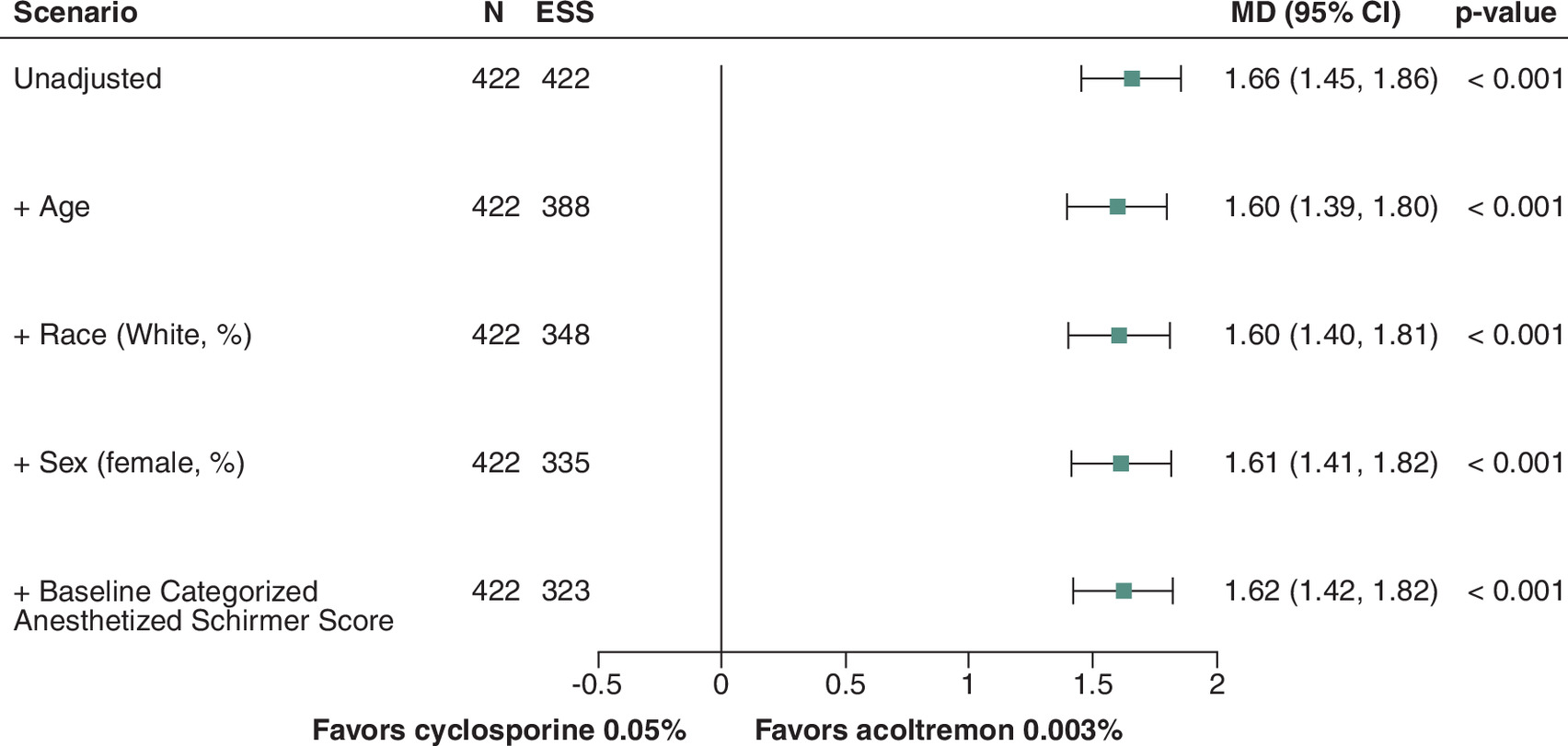
Figure 2. Matching-adjusted indirect comparison results: mean change from baseline in categorized Schirmer test score at day 14.
Mean difference > 0 implies that the comparison favors acoltremon. Unanesthetized pre-drop to post-drop mean CFB from COMET-2 and COMET-3 was compared with anesthetized mean CFB from Sall 2000.
CFB: Change from baseline; ESS: Effective sample size; MAIC: Matching-adjusted indirect comparison; MD: Mean difference; STS: Schirmer test score.
Discussion
This study provides comparative estimates of tear production efficacy for acoltremon 0.003% versus cyclosporine 0.05% in adults with DED, offering insights to inform treatment selection in the absence of direct comparative trials.
In this work, evidence of both a greater magnitude of tear production as well as faster onset of action in favor of acoltremon 0.003% compared with cyclosporine 0.05% was observed. Specifically, in both the primary analysis comparing the mean difference in mean CFB categorized STS at day 90 as well as an exploratory analysis comparing the mean difference between day 14 mean CFB categorized STS for acoltremon 0.003% and day 90 mean CFB categorized STS for cyclosporine 0.05%, significantly greater tear production in favor of acoltremon 0.003% was observed. As categorized scores were utilized, it is difficult to interpret the absolute magnitude of the Schirmer score increase observed in favor of acoltremon 0.003%, however for context, the day 90 unweighted mean CFB categorized STS observed for acoltremon 0.003% [26] was 1.79 and the mean CFB categorized STS reported in the trials for cyclosporine 0.05% was approximately 0.1 [32].
The goal of DED therapy is restoration of ocular surface homeostasis. The tear film, owing to its complex and rich biochemistry, plays a vital role in this process by providing lubrication, nourishment, protection and optical clarity [40–42]. Mechanistically, acoltremon stimulates tear production through a novel topical ocular neuromodulatory mechanism initiated by potent TRPM8 agonism. Consistent with this proposed mechanism, the primary end point in both Phase III pivotal clinical trials was met, with 43–53% of patients achieving an increase of 10 mm or more in unanesthetized Schirmer score compared with only 8–14% of vehicle-treated patients on day 14 [26]. Similar magnitudes of tear production and treatment differences were observed as early as day 1 and consistently through day 90 [26]. While cyclosporine 0.05% also leads to increased tear production via indirectly targeting the inflammatory component of DED and inhibition of calcineurin, published data reports only 15% of cyclosporine 0.05% treated patients achieved an increase of 10 mm or more in anesthetized STS after 6 months [35].
The findings from these MAIC analyses are noteworthy as cyclosporine 0.05% has long been utilized as a first-line pharmaceutical option for the treatment of DED, yet real-world data has indicated significant patient attrition, with poor efficacy documented by patients and physicians as a major reason for discontinuation [15,16]. For example, a real-world study of claims data from the US reported a 70.8% discontinuation rate of cyclosporine within a median of 89 days [14]. Of note, generalizability of the MAIC findings may be limited by the predominantly white US populations enrolled in both the COMET trials and Sall trials (75% [26] and 86% [32], respectively).
Strengths
A notable strength of this analysis was the thorough comparison of trial designs, eligibility criteria, baseline characteristics and outcome definitions. Additionally, pre-specified covariate identification and ranking of treatment effect modifiers ensured rigorous adjustment methods, enhancing the validity of the MAIC and ensuring clinically meaningful alignment between trial populations. Access and use of individual patient data from the COMET trials enabled precise reweighting and adjustment of baseline characteristics, enhancing the validity and reliability of the MAIC.
Limitations
Limitations of the study include the unanchored design, which assumes all relevant prognostic factors and effect modifiers are accounted for and differences in STS measurement methods and timepoints across trials. These factors may introduce residual bias despite adjustment. Several methods were employed to minimize these limitations. A thorough feasibility assessment was conducted to compare trials included in the MAIC, confirming similar populations and trial designs. Since including unnecessary covariates might increase variance of the estimated treatment effects, but omitting an important covariate might be costly in terms of bias, clinically relevant covariates were selected among the available covariates reported in the trials. In general, the trials were deemed sufficiently comparable for incorporation in an MAIC. Generalizability may be limited by the predominantly white US populations enrolled in the trials informing these analyses.
A source of cross-trial heterogeneity was the difference in minimum age for trial inclusion. In the COMET-2 and -3 trials, minimum age for inclusion was 30, whereas cyclosporine 0.05% trials included participants aged 18 years and older. Given that the range of patient ages was narrower in the acoltremon 0.003% trials compared with cyclosporine 0.05% trials, matching was not feasible. This difference between the populations could have contributed to bias in estimating treatment effects. However, the average patient age from the acoltremon 0.003% trials was adjusted through reweighting to match the average age from the cyclosporine 0.05% trials, across all conducted analyses.
Comparison of additional DED sign and symptom outcomes may have provided additional context to inform on overall efficacy. However, additional analyses were not possible due to substantive differences in clinical procedures and/or data availability.
Differences in measurement and reporting of STS between trials present several limitations. First, the cyclosporine 0.05% trials only reported STS as categories, so using categorized STS for the MAICs was required. It is possible that the use of categorized STS resulted in some loss of precision, leading to possible residual bias. Additionally, only anesthetized data were available for cyclosporine 0.05%, while only unanesthetized data were available for acoltremon 0.003%. Unanesthetized STS examines both basal tear production and reflex tear secretion elicited by the Schirmer test strip, while anesthetized STS only examines basal tear production by blunting the reflex tearing. Variation in the use of anesthesia across trials was presumably due to differing mechanisms of the two drugs [43]. Acoltremon 0.003% increases tear production by activating nociceptor ion channels, an effect which could be dampened by anesthesia. While the mechanism of action of cyclosporine 0.05% has not been fully established, it is hypothesized that it increases tear production with an immunomodulatory effect on the lacrimal functional unit, which would likely be unaffected by anesthesia use [44,45]. While some residual bias could remain, the authors hypothesize that the use of anesthetized STS data for cyclosporine 0.05% is unlikely to meaningfully affect the results of this MAIC, due to examining STS as a relative measure from baseline to the follow-up timepoint in this study.
Overall, these results provide context on effect trajectory but not proof of comparative onset of action as would be achieved in a head-to-head trial. These data are hypothesis-generating and should be interpreted as such. Future head-to-head or real-world comparative trials with harmonized outcomes are needed to provide additional context to these findings.
Conclusion
The overarching goal of this study was to compare the relative tear production achieved with acoltremon 0.003% compared with cyclosporine 0.05% in patients with DED. After adjustment for key treatment effect modifiers and prognostic factors, significantly greater tear production was observed with acoltremon 0.003% compared with cyclosporine 0.05% at day 90. In addition, exploratory analysis showed greater tear production with acoltremon 0.003% at day 14 compared with tear production measured at day 90 with cyclosporine 0.05%. Given the critical role played by the tear film in restoration of ocular surface homeostasis, acoltremon 0.003% may represent a more effective and faster alternative for the treatment of the signs and symptoms of DED. However, due to limitations inherent to the unanchored MAIC design, these findings should be interpreted as preliminary and would benefit from confirmation in direct comparative studies.
Summary points
•
Dry eye disease (DED) is a common, multifactorial condition with significant impact on quality of life and work productivity.
•
Cyclosporine 0.05% (Restasis) is generally used as a first-line prescription treatment. However, physician and patient satisfaction surveys and real-world treatment patterns indicate frequent discontinuation likely due to dissatisfaction.
•
Acoltremon ophthalmic solution 0.003% (Tryptyr®), approved by the US FDA for the treatment of signs and symptoms of DED, is a TRPM8 agonist that stimulates basal tear production via topical ocular neurosensory pathways.
•
As direct comparative evidence is lacking, this study performed an unanchored matching-adjusted indirect comparison to evaluate relative efficacy of tear production for acoltremon 0.003% versus cyclosporine 0.05%, using the mean change from baseline (CFB) of the categorized Schirmer test score (STS) at day 90.
•
Individual patient data from Phase III trials of acoltremon 0.003% were reweighted for key treatment effect modifiers (age, race, sex and baseline tear production) to match the population level baseline characteristics that have been reported in published literature for the Phase III cyclosporine 0.05% trials.
•
Results indicate that acoltremon 0.003% leads to significantly greater tear production at day 90 compared with cyclosporine 0.05%, with a mean difference in CFB of 1.62 categories on the STS (p < 0.001).
•
In addition, an exploratory analysis indicated significantly greater tear production associated with acoltremon 0.003% at day 14 as compared with cyclosporine 0.05% at day 90, suggesting robustness of results (mean difference in CFB of 1.62 categories on the STS, p < 0.001).
•
The superior tear production results observed in this study further support acoltremon 0.003% as a valuable alternative strategy for the treatment of the signs and symptoms of DED.
•
Limitations of this analysis include the unanchored design, the lack of day 14 data for cyclosporine 0.05% and the absence of other common DED clinical outcomes due to significant methodological differences between trials.
Author contributions
Authors S Pflugfelder, M Senchyna, T Okoro, EM Salvo-Halloran and A Haltner were responsible for study conception and design, interpretation of results, drafting and revision of the manuscript. A Haltner also performed data analysis. EK Prentiss and N Srikanth were involved in data analysis, drafting and revision of the manuscript. EK Akpek and M Ainslie-Garcia were involved in interpretation of results, drafting and revision of the manuscript.
Acknowledgments
The authors thank Nikita Sir and Sabrina Santos for their assistance in the conduct of the research.
Financial disclosure
This work was sponsored by Alcon (TX, USA).
Competing interest disclosure
EM Salvo-Halloran, M Ainslie-Garcia, A Haltner, N Srikanth and EK Prentiss are current or former employees of EVERSANA. M Senchyna and T Okoro are current or former employees of Alcon. S Pflugfelder and EK Akpek are consultants for Alcon. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical conduct of research
As this study used anonymized clinical trial data, ethics approval or informed consent for the purposes of data generated for this work was not required.
Writing assistance disclosure
Writing support was provided by EVERSANA and was funded by Alcon.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of these shared data is in accordance with the terms agreed upon their receipt. Data were provided by Alcon.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 31.88 KB
References
Papers of special note have been highlighted as: • of interest
1.
MarketScope. 2024 dry eye products market report: a global analysis for 2023 to 2029. (2024). https://www.market-scope.com/pages/reports/481/2024-dry-eye-products-market-report-global-analysis-for-2023-to-2029-december-2024
2.
Wolffsohn JS, Benítez-Del-Castillo JM, Loya-Garcia D et al. TFOS DEWS III: diagnostic methodology. Am. J. Ophthalmol. 279, 387–450 (2025).
3.
Nichols KK, Bacharach J, Holland E et al. Impact of dry eye disease on work productivity, and patients' satisfaction with over-the-counter dry eye treatments. Invest. Ophthalmol. Vis. Sci. 57(7), 2975–2982 (2016).
4.
Dana R, Bradley JL, Guerin A et al. Estimated prevalence and incidence of dry eye disease based on coding analysis of a large, all-age united states health care system. Am. J. Ophthalmol. 202, 47–54 (2019).
5.
Guo OL, Akpek E. The negative effects of dry eye disease on quality of life and visual function. Turk. J. Med. Sci. 50(Si–2), 1611–1615 (2020).
6.
Akpek EK, Karakus S, Ramulu PY, Mathews PM. Sustained gazing causes measurable decline in visual function of patients with dry eye. Am. J. Ophthalmol. 210, 107–115 (2020).
7.
Chan C, Ziai S, Myageri V, Burns JG, Prokopich CL. Economic burden and loss of quality of life from dry eye disease in Canada. BMJ Open Ophthalmol. 6(1), e000709 (2021).
8.
Yu J, Asche CV, Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea 30(4), 379–387 (2011).
9.
Chen E, Kombo N, Teng CC, Mruthyunjaya P, Nwanyanwu K, Parikh R. Ophthalmic medication expenditures and out-of-pocket spending: an analysis of United States prescriptions from 2007 through 2016. Ophthalmology 127(10), 1292–1302 (2020).
10.
Wirta DL, Galor A, Aune CA et al. Long-term safety and efficacy of a water-free cyclosporine 0.1% ophthalmic solution for treatment of dry eye disease: ESSENCE-2 OLE. Cornea 44(6), 692–670 (2025).
11.
Jones L, Craig JP, Markoulli M et al. TFOS DEWS III: management and therapy. Am. J. Ophthalmol. 279, 289–386 (2025).
• Highlights current approaches to management of dry eye disease, including providing a detailed description of prescription therapy options.
12.
Leonardi A, Van Setten G, Amrane M et al. Efficacy and safety of 0.1% cyclosporine a cationic emulsion in the treatment of severe dry eye disease: a multicenter randomized trial. Eur. J. Ophthalmol. 26(4), 287–296 (2016).
13.
Haber SL, Benson V, Buckway CJ, Gonzales JM, Romanet D, Scholes B. Lifitegrast: a novel drug for patients with dry eye disease. Ther. Adv. Ophthalmol. 11, 2515841419870366 (2019).
14.
White DE, Zhao Y, Ogundele A et al. Real-world treatment patterns of cyclosporine ophthalmic emulsion and lifitegrast ophthalmic solution among patients with dry eye. Clin. Ophthalmol. 13, 2285–2292 (2019).
• This claims database analysis highlights rates of discontinuation among users of cyclosporine 0.05% and another common dry eye prescription therapy (lifitegrast).
15.
White DE, Zhao Y, Jayapalan H, Machiraju P, Periyasamy R, Ogundele A. Treatment satisfaction among patients using anti-inflammatory topical medications for dry eye disease. Clin. Ophthalmol. 14, 875–883 (2020).
• Assesses patient satisfaction among current or former users of anti-inflammatory topical prescriptions therapies for dry eye disease (cyclosporine 0.05% and lifitegrast 5.0%), including reasons for switching therapies, in 207 patients with dry eye disease.
16.
White DE, Zhao Y, Jayapalan H, Machiraju P, Periyasamy R, Ogundele A. Physician satisfaction with anti-inflammatory topical medications for the treatment of dry eye disease. Clin. Ophthalmol. 14, 931–938 (2020).
• Assesses physician satisfaction with anti-inflammatory topical prescriptions therapies for dry eye disease (cyclosporine 0.05% and lifitegrast 5.0%).
17.
Cook N, Mullins A, Gautam R et al. Evaluating patient experiences in dry eye disease through social media listening research. Ophthalmol. Ther. 8(3), 407–420 (2019).
18.
Mbagwu M, LaPrise A, Harris J et al. Characterization of discontinuation and switching patterns of dry eye disease medications using linked EHR registry and claims data. Presented at: American Society of Cataract and Refractive Surgery Annual Meeting, Boston, MA, USA (2024). 8 April 2024, Abstract 99117. https://ascrs.confex.com/ascrs/24am/meetingapp.cgi/Paper/99117
19.
Ahmed B, Shahzad Y, Urooj W, Siddiqui A, Nisa Mughal ZU, Abbasher Hussien Mohamed Ahmed K. Navigating dry eye relief: meibo's approach to controlling tear evaporation. Ann. Med. Surg. (Lond.) 86(10), 5680–5684 (2024).
20.
Frampton JE. Varenicline solution nasal spray: a review in dry eye disease. Drugs 82(14), 1481–1488 (2022).
21.
Alcon. Tryptyr (acoltremon ophthalmic solution) 0.003%. (2025). https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217370s000lbl.pdf
22.
Viana F. Chemosensory properties of the trigeminal system. ACS Chem. Neurosci. 2(1), 38–50 (2011).
23.
Wirta DL, Senchyna M, Lewis AE et al. A randomized, vehicle-controlled, Phase IIb study of two concentrations of the TRPM8 receptor agonist AR-15512 in the treatment of dry eye disease (COMET-1). Ocul. Surf. 26, 166–173 (2022).
24.
Belmonte C, Nichols JJ, Cox SM et al. TFOS DEWS II pain and sensation report. Ocul. Surf. 15(3), 404–437 (2017).
25.
Gallar J, Pflugfelder S, Galor A, Gupta PK, Hamrah P. Corneal sensory nerve regulation of tear production through stimulation of transient receptor potential melastatin 8 (TRPM8) channel: a potential new approach for treating dry eye disease. Ocul. Surf. 38, 142–154 (2025).
26.
Pattar GR, Wirta D, Jerkins G et al. Acoltremon ophthalmic solution 0.003% for signs and symptoms of dry eye disease: results of Phase III pivotal studies COMET-2 and COMET-3. Ophthalmology 133(5), 563–574 (2026).
• Summarizes two randomized, multicenter, double-masked, vehicle-controlled Phase III studies that evaluates the safety and efficacy of the transient receptor potential melastatin 8 agonist acoltremon on signs and symptoms of dry eye disease.
27.
Sun CC, Hsu SL, Liang CM, Tsai YY, Lin PY. Bridging the gap in managing dry eye disease: a consensus report by the Taiwan Society of Cataract and Refractive Surgeons. BMC Ophthalmol. 24(1), 314 (2024).
28.
Aragona P, Giannaccare G, Mencucci R et al. The management of dry eye disease: proceedings of Italian Dry Eye Consensus Group using the Delphi method. J. Clin. Med. 11(21), 6437 (2022).
29.
Amescua G, Ahmad S, Cheung AY et al. American Academy of Ophthalmology Preferred Practice Pattern Cornea/External Disease Panel. Dry Eye Syndrome Preferred Practice Pattern®. Ophthalmology 131(4), P1–P49 (2024).
30.
Milner MS, Beckman KA, Luchs JI et al. Dysfunctional tear syndrome: dry eye disease and associated tear film disorders – new strategies for diagnosis and treatment. Curr. Opin. Ophthalmol. 27(Suppl. 1), 3–47 (2017).
31.
Signorovitch JE, Sikirica V, Erder MH et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health 15(6), 940–947 (2012).
32.
Sall K, Stevenson OD, Mundorf TK, Reis BL. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. CSA Phase III Study Group. Ophthalmology 107(4), 631–639 (2000).
• Summarizes the Phase III studies assessing the safety and effectiveness of cyclosporine 0.05% for the treatment of dry eye disease.
33.
NICE. NICE single technology appraisal and highly specialised technologies evaluation: user guide for company evidence submission template. (2024). https://www.nice.org.uk/process/pmg24/resources/single-technology-appraisal-and-highly-specialised-technologies-evaluation-user-guide-for-company-evidence-submission-template-pdf-72286715419333
34.
Montecchi-Palmer M, Wu M, Rolando M, Lau C, Perez Quinones VL, Dana R. Possible strategies to mitigate placebo or vehicle response in dry eye disease trials: a narrative review. Ophthalmol. Ther. 12(4), 1827–1849 (2023).
35.
AbbVie. Restasis (cyclosporine 0.05%). (2025). https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/050790s031lbl.pdf
36.
Phillippo D, Ades T, Dias S, Palmer S, Abrams KR, Welton N. NICE DSU Technical Support Document 18: methods for population-adjusted indirect comparisons in submissions to NICE. NICE Decision SupportUnit. (2016). Accessed 5 May 2026. http://www.nicedsu.org.uk/Populationadjusted-ICs-TSD(3026862).html
37.
Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for population-adjusted indirect comparisons in health technology appraisal. Med. Decis. Mak. 38(2), 200–211 (2018).
38.
Signorovitch JE, Wu EQ, Yu AP et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics 28(10), 935–945 (2010).
39.
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 28(25), 3083–3107 (2009).
40.
Craig JP, Nichols KK, Akpek EK et al. TFOS DEWS II definition and classification report. Ocul. Surf. 15(3), 276–283 (2017).
41.
Stern ME, Beuerman RW, Fox RI, Gao J, Mircheff AK, Pflugfelder SC. The pathology of dry eye: the interaction between the ocular surface and lacrimal glands. Cornea 17(6), 584–589 (1998).
42.
Pflugfelder SC, Stern ME. Biological functions of tear film. Exp. Eye Res. 197, 108115 (2020).
43.
Brott NR, Zeppieri M, Ronquillo Y. Schirmer Test. 2024 Feb 24. In: StatPearls. StatPearls Publishing, FL, USA (2024).
44.
Periman LM, Mah FS, Karpecki PM. A review of the mechanism of action of cyclosporine A: the role of cyclosporine a in dry eye disease and recent formulation developments. Clin. Ophthalmol. 14, 4187–4200 (2020).
45.
Bian X, Ma J, Liu Y et al. Cyclosporine A in the treatment of dry eye disease: a narrative review. Front. Ophthalmol. 5, 1700163 (2025).
Information & Authors
Information
Published In
Copyright
© 2026 Alcon. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 28 January 2026
Accepted: 23 April 2026
Published online: 14 May 2026
Keywords:
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Matching-adjusted indirect comparison of acoltremon ophthalmic solution 0.003% and cyclosporine 0.05% ophthalmic emulsion for increased tear production in patients with dry eye disease. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0032
Export citation
Select the citation format you wish to export for this article or chapter.