Economic evaluation of stapokibart for chronic rhinosinusitis with nasal polyps in China: a cost–effectiveness analysis
Abstract
Aim: To evaluate the cost–effectiveness of stapokibart compared with dupilumab in treating chronic rhinosinusitis with nasal polyps (CRSwNP) from the healthcare system perspective in China. The focus is on assessing the economic viability of biologic treatments in managing CRSwNP, particularly when conventional treatments and/or surgery fail to provide sufficient relief. Materials & methods: A decision tree Markov model was developed to assess the cost–effectiveness of stapokibart and dupilumab. Clinical data from multiple trials were used, and a matching-adjusted indirect comparison was conducted to account for differences in patient populations across studies. Sensitivity analysis was performed to evaluate the robustness of the model results under varying assumptions. Results: The study results indicate that stapokibart offers a clear economic advantage over dupilumab. It both lowers treatment costs and enhances patients' quality of life. Sensitivity analysis shows that stapokibart remains cost-effective at the threshold of one to three-times China’s per capita GDP, demonstrating strong economic viability in the Chinese healthcare context. Conclusion: The study demonstrates that stapokibart is a cost-effective treatment option for CRSwNP compared with dupilumab. It offers significant improvements in patient outcomes and is economically viable under the prevailing healthcare budget in China, providing valuable insights for policy-makers and healthcare providers.
Plain language summary: Comparing the economic value of stapokibart & dupilumab for chronic rhinosinusitis with nasal polyps in China
What is this article about?
In China, stapokibart and dupilumab are biologic treatments for chronic rhinosinusitis with nasal polyps, a long-term condition that can seriously affect how people feel and live. For some patients, standard medicines or surgery do not provide enough relief, and biologic treatments may then be considered. However, these treatments are expensive, so it is important to understand which option provides better value.
To assess the economic value of stapokibart compared with dupilumab, this study evaluated the costs and health outcomes of the two treatments from the healthcare system perspective in China. Because there was no direct clinical trial comparing stapokibart with dupilumab, data from separate clinical studies were used and adjusted to make the comparison as fair as possible.
What were the results?
The results showed that stapokibart was associated with lower overall treatment costs and better health outcomes than dupilumab in the main analysis. Additional analyses also showed that the findings remained stable under different assumptions. When the price difference between the two drugs was removed, stapokibart was no longer cost-saving, but it still remained cost-effective.
What do the results mean?
These findings suggest that stapokibart may offer an economic advantage over dupilumab for patients with chronic rhinosinusitis with nasal polyps in China. The results may help support treatment selection and medical insurance decision-making in clinical practice.
Chronic rhinosinusitis with nasal polyps (CRSwNP) is mainly characterized by T2 inflammation, with eosinophilic infiltration and elevated levels of cytokines such as IL-4, IL-5 and IL-13. This condition is further complicated by tissue remodeling and epithelial barrier dysfunction, with the presence of nasal polyps. CRSwNP often co-occurs with bronchial asthma and aspirin-exacerbated respiratory disease [1]. A cross-sectional study conducted in seven cities across China shows that the overall prevalence of chronic rhinosinusitis (CRS) is 8.0%, slightly lower than in Europe (10.9%) and the USA (12–14%). Among the general population in China, CRS is estimated to affect approximately 8.0% of individuals [2]. The estimated nationwide prevalence of CRSwNP is approximately 20–33%, which translates to 10 million to 38 million cases. CRSwNP is predominantly a disease of middle age, with a peak incidence between the fourth and fifth decades of life. CRSwNP places a significant health burden on patients and significantly impacts their quality of life. Symptoms like nasal congestion, reduced sense of smell, and headaches often seen in CRSwNP can severely affect daily activities and sleep quality [3].
Conventional treatments for CRSwNP include intranasal corticosteroids, macrolides, mucolytics, antihistamines, leukotriene receptor antagonists and biologics, with functional endoscopic sinus surgery as the primary surgical option. The emergence of biologics has offered new treatment options for CRSwNP patients, mainly for those with inadequate control by conventional treatments or surgery. Dupilumab is the first biologic approved for CRSwNP worldwide, receiving approval from the US FDA in June 2019. Omalizumab and mepolizumab were approved by the FDA in December 2020 and July 2021, respectively. In China, stapokibart, a biologic the same as dupilumab in targeting the IL-4Rα receptor, was approved by the National Medical Products Administration in December 2024. It is the first biologic approved in China for the treatment of CRSwNP. However, the high cost of surgery and biologic treatments has already placed a significant economic burden on CRSwNP patients. Studies have shown that their medical costs are 30–50% higher than those of the general population, primarily due to frequent surgeries and long-term medication. In the USA, CRSwNP accounts for approximately $5.7 billion in annual direct healthcare expenditures [4], while indirect costs of CRS exceed $20 billion per year [5]. In a recent study in Europe, direct costs for patients with CRSwNP were $1651 per patient/year, with indirect costs of $6225 per patient/year, largely due to outpatient/hospital visits and productivity losses, respectively. In China, the average annual direct medical cost for these patients is $1158, with indirect costs (productivity loss due to sick leave) averaging $797 per year. The total economic burden of the disease represents 12.3% of the patient’s family’s annual income [6]. From an economic perspective, the high recurrence and long-term symptoms of CRSwNP result in productivity loss and excessive use of social resources.
Currently, research on the treatment of CRSwNP remains limited, with most economic evaluations focusing on biologic therapies and surgical procedures. Yong M et al. used dupilumab, omalizumab and mepolizumab as the starting points in the decision tree model in Canada. The results indicated that omalizumab was the most cost-effective treatment when compared with dupilumab and mepolizumab [7]. Yong M et al. compared the cost–effectiveness of dupilumab and Aspirin Desensitization for CRSwNP patients in the US. While dupilumab shows some cost–effectiveness, its high cost presents an economic challenge [8]. According to Eugenio De Corso et al., dupilumab’s ICUR was below the commonly accepted cost–effectiveness threshold compared with best supportive care in Italy, and sensitivity analysis confirmed the robustness and economic sustainability of the results [9]. George A et al. found that endoscopic sinus surgery is more economically viable than dupilumab in treating CRSwNP, as it is less costly and offers long-term treatment outcomes [10]. Although the cost–effectiveness of dupilumab, omalizumab and mepolizumab have been assessed in the context of US, Canada and Italy, a similar assessment tailored to the Chinese context remains to be conducted. To address this gap, the present study employs the decision tree Markov model, incorporating data from the CROWNS-2 (NCT06801353) [11] and SINUS-52 (NCT02898454) [12] clinical trials. This model is used to evaluate the cost–effectiveness of stapokibart, which was the first biologic approved for treating CRSwNP in China.
Materials & methods
Study design
Target population & research perspective
Stapokibart is recommended for patients with CRSwNP who have poor control with glucocorticoids and/or surgery. Based on the clinical trial population selection, this study focuses on adults with CRSwNP who have poor control with conventional treatment and/or surgery.
The study adopts the healthcare system perspective, focusing on the viewpoint of healthcare decision-makers and considering the resource consumption and patient benefits of both the intervention and control measures. Given the difficulty in calculating indirect costs and other related expenses caused by the disease, and the relatively good efficacy of this treatment, this study does not account for indirect costs.
Intervention & comparator
In this study, stapokibart is employed as the primary intervention. Given that the dosage recommendation in the package insert differs from the clinical trial protocol, and considering the study predominantly relies on the clinical trial framework, the intervention adheres to the clinical trial regimen. Specifically, stapokibart is administered at a dosage of 300 mg every 2 weeks, while mometasone furoate nasal spray (MFNS) is used at a dosage of 200 μg once daily.
Dupilumab is employed as the reference intervention. Given that it targets the same receptor as stapokibart, shares the primary indication of atopic dermatitis, and that its published Phase III clinical trials closely align with the stapokibart trial design, the control regimen follows the dosage used in those Phase III trials. Specifically, dupilumab is administered at a dosage of 300 mg every 2 weeks, while MFNS is used at a dosage of 200 μg once daily.
Model description & structure
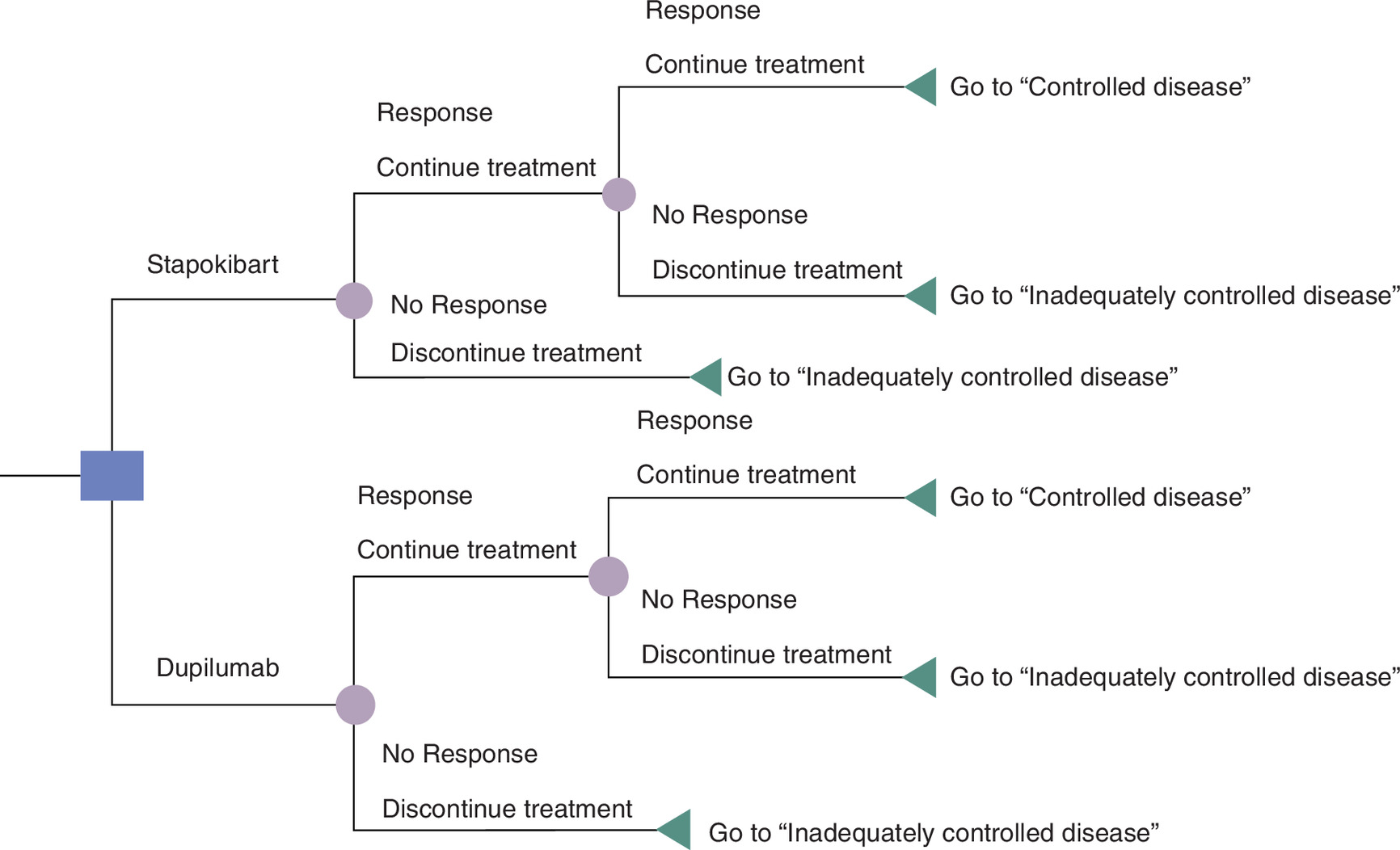
In the decision tree model, the continuation of biologic therapy for patients treated with biologics is evaluated both at 24 and 52 weeks. Based on The Chinese expert consensus on the use of biologics in patients with chronic rhinosinusitis [13] and the study by Eugenio De Corso et al. [9], we established the criteria for determining whether patients achieved a response. Specifically, patients are considered to have achieved a response if the nasal polyp score (NPS) decreases by at least 1 point and the Sino-Nasal Outcome Test-22 (SNOT-22) score improves by at least 8.9 points from baseline. Otherwise, biologic treatment is discontinued (Figure 1). In accordance with the clinical trial design, product labeling, and relevant guidelines, patients in the continuous biologic treatment arm receive stapokibart 300 mg every 2 weeks in the experimental group or dupilumab 300 mg every 2 weeks in the control group. In the discontinuation arm, patients receive prednisone acetate 30 mg daily for 14 days, followed by MFNS 200 μg once daily, hereinafter referred to as standard drug therapy. After completion of the decision tree phase, patients transition to the Markov model for long-term simulation of health state transitions and associated costs and outcomes.
After the 52-week decision tree phase, patients transition into the Markov model. In the initial state, those who discontinue biologic therapy enter the ‘Inadequately controlled’ state, whereas those who continue biologic therapy remain in the ‘Controlled disease’ state. Patients remain in the ‘Controlled disease’ state if the NPS decreases by at least 1 point and the Sino-Nasal Outcome Test-22 (SNOT-22) score improves by at least 8.9 points from baseline; otherwise, they move to the ‘Inadequately controlled’ state. It is assumed that once the disease transitions from ‘Controlled disease’ to ‘Inadequately controlled’, it does not revert to the ‘Controlled disease’ state (Figure 2).
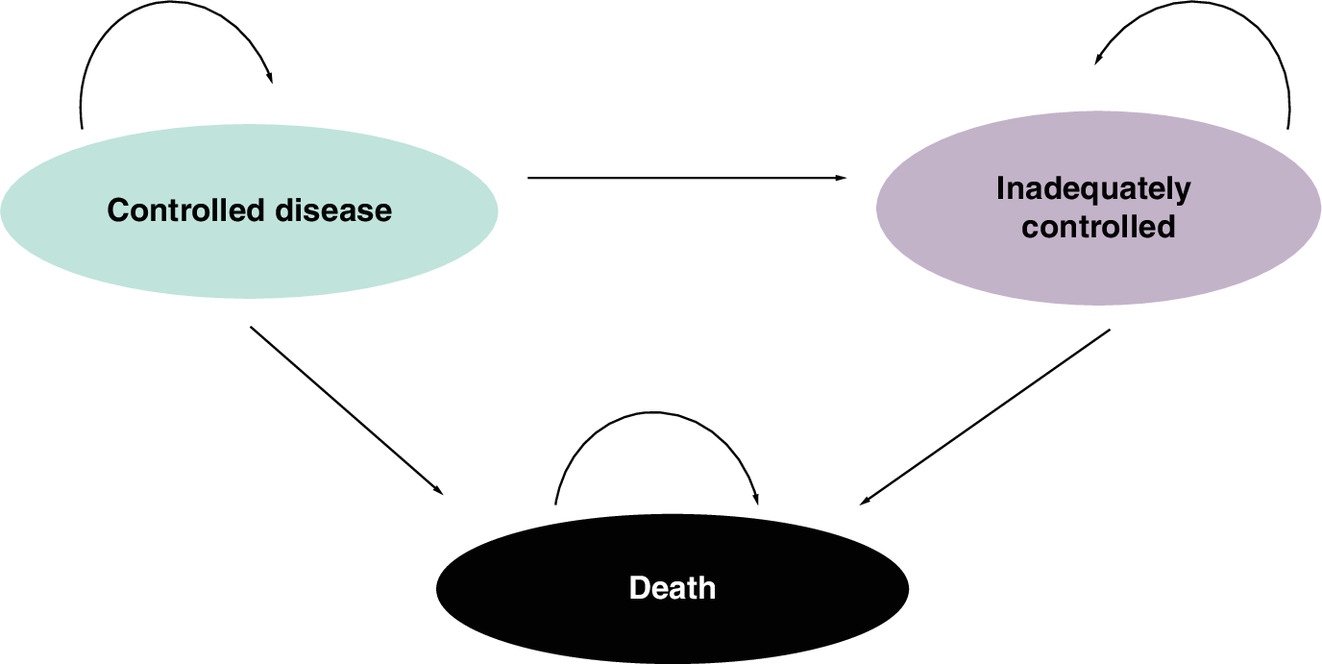
According to The 2023 Health and Wellness Development Statistical Bulletin of China, the country’s average life expectancy is 78.9 years [14]. The average age of onset for CRSwNP is 46 years [15]. Therefore, the Markov model adopts a 33-year time horizon with a 1-year cycle length. In the ‘Controlled disease’ state, patients in the experimental arm receive stapokibart 300 mg every 2 weeks plus MFNS 200 μg once daily. According to the Chinese Expert Consensus on the Use of Biologics in Patients with Chronic Rhinosinusitis [13], when a single biologic fails to control the disease, switching to another biologic or considering surgery with standard drug therapy is recommended. Given that mepolizumab was approved by the National Medical Products Administration in 2025 for the treatment of CRSwNP, this study specifies mepolizumab as the replacement biologic. In the ‘Inadequately controlled’ state, some patients undergo surgery followed by standard drug therapy, while others switch to mepolizumab 300 mg every 4 weeks in combination with standard drug therapy.
Comparison of efficacy & safety
Due to the lack of direct clinical trial evidence comparing stapokibart with dupilumab, this study uses indirect comparison instead of direct comparison [16]. Since the control group in the CROWNS-2 trial used stapokibart instead of a placebo from 24 to 52 weeks, this study applied the anchored MAIC method for the 0–24 week period and the unanchored MAIC method for the 24–52 week period. These methods were used to align individual patient data (IPD) of the CROWNS-2 with aggregated data (AgD) from SINUS-24 and SINUS-52. Using multivariable regression, the clinical treatment guidelines and expert consensus for CRSwNP, along with the effective sample size after matching and adjustment, selected age, gender, baseline NPS and baseline SNOT-22 total score as baseline characteristics for both anchored and unanchored MAIC. In R, logistic regression was used to adjust the weights of the experimental group’s IPD data at 24 and 52 weeks of stapokibart, generating a weight histogram and the corresponding weights for each patient.
In the unanchored MAIC, the efficacy ORAB for stapokibart versus dupilumab is calculated using the following formula, where ORAC represents the efficacy of stapokibart versus placebo, and ORBC represents the efficacy of dupilumab versus placebo:
(Equation 1)
Data were processed using R® version 4.3.0, with count data expressed as percentages and analyzed using the χ2 test. Continuous data are presented as χ ± s and analyzed using the t-test, with p ≤ 0.05 indicating statistical significance. In the MAIC analysis, binary variable results are expressed as odds ratios (OR).
Model input
Efficacy input
The clinical parameters used in the economic evaluation mainly consist of efficacy data. These include parameters such as achievement rate, transition probability, the probability of using alternative treatments under inadequately controlled conditions, and the incidence of adverse reactions. The achievement rate of stapokibart was derived from the IPD of CROWNS-2 after matching adjustment through a MAIC comparison with dupilumab. In the Markov model, the probability of maintaining disease control is based on the 52-week achievement rate from the decision tree model. The mortality rate is based on the natural mortality rate reported by the WHO [18]. The probability of switching biologics or undergoing surgery is derived from expert consultation. The detailed parameter values are provided in Table 1.
| Variable name | Parameter description | Base value | Standard error | Distribution | Upper limit | Lower limit | Source | Ref. |
|---|---|---|---|---|---|---|---|---|
| Decision tree achievement rates | 24-week stapokibart achievement rate | 0.563 | 0.029 | Beta | 0.620 | 0.507 | Derived through MAIC | |
| 24-week dupilumab achievement rate | 0.520 | 0.027 | Beta | 0.572 | 0.468 | De Corso E et al. | [10] | |
| 52-week stapokibart achievement rate | 0.908 | 0.046 | Beta | 0.998 | 0.817 | Derived through MAIC | ||
| 52-week dupilumab achievement rate | 0.560 | 0.029 | Beta | 0.616 | 0.504 | De Corso E et al. | [10] | |
| Markov transition probabilities | Stapokibart disease control maintenance probability | 0.908 | 0.046 | Beta | 0.998 | 0.817 | Derived through MAIC | |
| Stapokibart disease control to inadequate probability | 0.091 | 0.005 | Beta | 0.100 | 0.082 | Derived through MAIC | ||
| Dupilumab disease control maintenance probability | 0.560 | 0.029 | Beta | 0.616 | 0.504 | De Corso E et al. | [10] | |
| Dupilumab disease control to inadequate probability | 0.439 | 0.022 | Beta | 0.483 | 0.395 | De Corso E et al. | [10] | |
| Natural mortality rate | 0.001 | 0.000 | Beta | 0.001 | 0.001 | WHO China Natural Mortality Rate | ||
| Probability of using other treatments in inadequate control state | Probability of surgery use in the standard treatment group | 0.106 | 0.005 | Beta | 0.117 | 0.095 | Expert consultation | |
| Probability of medication use in the standard treatment group | 0.894 | 0.046 | Beta | 0.983 | 0.805 | Expert consultation |
Based on previous literature research, clinical trial realities and data availability, this study includes only adverse events with an incidence rate of 0.05% or higher. The adverse events for stapokibart that meet the criteria include upper respiratory tract infection, pharyngitis, urinary tract infection, cough, toothache, joint pain and COVID-19. For dupilumab, the adverse events include injection site erythema, bronchitis, pharyngitis, upper respiratory tract infection, joint pain, back pain, headache, asthma, cough and nosebleeds, among others. The common adverse events for both biologics, such as upper respiratory tract infection, cough and joint pain, were included for MAIC, and the corresponding adverse event costs were calculated. Specific adverse events are listed in the Table 2.
| Parameter description | Base value | Standard error | Distribution | Upper limit | Lower limit | Source | |
|---|---|---|---|---|---|---|---|
| Stapokibart | Upper respiratory tract infection | 0.034 | 0.003 | Beta | 0.041 | 0.027 | Derived through MAIC |
| Cough | 0.265 | 0.027 | Beta | 0.318 | 0.212 | ||
| Joint pain | 0.046 | 0.005 | Beta | 0.056 | 0.037 | ||
| Dupilumab | Upper respiratory tract infection | 0.060 | 0.007 | Beta | 0.072 | 0.048 | Derived through MAIC |
| Cough | 0.067 | 0.007 | Beta | 0.080 | 0.054 | ||
| Joint pain | 0.064 | 0.020 | Beta | 0.077 | 0.051 | ||
Cost input
Based on the research perspective, this study focuses only on the direct medical costs related to treatment, including drug costs, adverse event management costs and drug administration costs. As some patients require surgery, surgery and inpatient care costs are also included. For details on the cost parameters, refer to Table 3. All the costs were presented in US dollar based on 2024 prices (USD: RMB = 1: 7.1217).
| Parameter description | Base value | Standard error | Distribution | Upper limit | Lower limit | Source |
|---|---|---|---|---|---|---|
| Stapokibart (300 mg/$) | 169.622 | 17.308 | Gamma | 203.547 | 135.698 | The current PAP-adjusted sales price |
| Dupilumab (300 mg/$) | 211.747 | 21.607 | Gamma | 254.097 | 169.398 | Local price |
| Mepolizumab (100 mg/$) | 404.398 | 41.265 | Gamma | 485.277 | 323.518 | |
| Mometasone furoate nasal spray (per use/$) | 0.513 | 0.052 | Gamma | 0.616 | 0.410 | PharmCube Database |
| Prednisone acetate (per use/$) | 0.051 | 0.005 | Gamma | 0.061 | 0.040 | |
| Drug preparation cost | 4.774 | 0.487 | Gamma | 5.729 | 3.819 | Healthcare price list |
| Nasal polyp removal surgery cost | 312.451 | 31.883 | Gamma | 374.942 | 249.961 | |
| Follow-up cost | 221.174 | 22.569 | Gamma | 265.409 | 176.939 |
The price of stapokibart is provided by enterprises. The prices of dupilumab and mepolizumab are based on local drug pricing in China. MFNS and prednisone acetate have been marketed for many years, with many manufacturers. The median price were obtained from the Public database. Drug preparation cost, nasal polyp removal surgery cost and follow-up cost prices are based on the healthcare price list. Follow-up costs include sinus CT, nasal endoscopy, blood routine tests, blood biochemistry (dry chemical method), urine routine tests, 12-lead ECG, PK blood sample collection, olfactory function testing and the collection of nasal secretions and exfoliated nasal cells. The frequency of use is based on CROWNS-2. Surgical costs include the cost of nasal polyp removal surgery and standard treatment. The adverse event management costs used in this study are based on literature research. The detailed values are presented in Table 4 [19,20].
Utility inputs
In the CROWNS-2, EQ-5D was used to measure the utility values of CRSwNP patients at baseline, 24 weeks, and 52 weeks. Thus, the utility value is based on the IPD of CROWNS-2, and the detailed values are presented in Table 5.
| Parameter description | Base value | Standard error | Distribution | Upper limit | Lower limit | Source |
|---|---|---|---|---|---|---|
| Adequately controlled utility | 0.9770 | 0.056 | Beta | 1.000 | 0.782 | CROWNS-2 |
| Inadequately controlled utility | 0.9242 | 0.066 | Beta | 1.000 | 0.739 | CROWNS-2 |
Analysis
Basic analysis
The base case analysis was run with Microsoft Office Excel, and the direct medical costs and CRSwNP health outcomes were discounted at a rate of 5.0% according to the recommendations of Guidelines for Pharmaceutical Economic Evaluation of China (2020 edition) [21]. The end points included incremental cost–effectiveness ratio (ICER), net monetary benefit (NMB). To avoid overestimating the incremental value, half-cycle corrections to utility were performed. The economic viability is assessed by the guideline as follows: when ICER <1 times the per capita GDP, the additional cost is entirely worthwhile; when 1 times the per capita GDP < ICER <three-times the per capita GDP, the additional cost is acceptable; and when ICER >three-times the per capita GDP, the additional cost is not justified [21]. Since there was no fixed willingness-to-pay (WTP) to evaluate cost–effectiveness in China, this study recommended the WTP threshold of $13,445 and $40,335, which was associated with the one-time and three-times GDP per capita of China in 2024 [22], to assess whether stapokibart is highly cost-effective (ICER ≤ $13,445) or acceptable (ICER ≤ $40,335) compared with dupilumab. In addition, if NMB >0, the intervention is cost-effective; if NMB <0, it is not cost-effective, given the specified WTP threshold.
Sensitivity analysis
To assess the robustness of the base-case results, deterministic sensitivity analysis (DSA) and probabilistic sensitivity analysis (PSA) were conducted to address the uncertainty in the model. NMB was used for DSA because it provides a continuous, single-valued measure directly linked to the WTP threshold, avoiding the instability and interpretational difficulties of ICER when incremental effects are near zero or change sign.
As for DSA, the discount rate ranged from 0 to 8%, while other parameter estimates varied within their 95% CI based on the mean estimate and standard deviation. The cost parameters fluctuate by 20%, and the transition probabilities fluctuate by 10%. DSA results were visualized using tornado diagrams, highlighting the parameters with the greatest influence on model outcomes.
AS for PSA, the PSA was performed by means of a Second-order Monte Carlo simulation. A total of 10,000 iterations were conducted following the assignment of different distribution functions to the key parameters. The gamma distribution was applied for cost parameters, while the Beta distribution was applied for utility value, transition probability parameters and discount rate. Scatter plots were developed to represent uncertainty, and cost–effectiveness acceptability curves were created based on the patient’s WTP $13,445 and $40,335 QALY [23].
Result
Basic analysis
The analysis shows that over the entire study period, the total treatment cost for the stapokibart group is $80,923.24, with a total utility value of 15.32 QALYs; the total treatment cost for the dupilumab group is $82,027.20, with a total utility value of 15.22 QALYs (Table 6).
| Cost | QALY | Incremental cost | Incremental QALYs | ICER | INMB | |
|---|---|---|---|---|---|---|
| Stapokibart | $80,923.24 | 15.32 | -$1103.95 | 0.10 | Absolute economic advantage | 2467.35 |
| Dupilumab | $82,027.20 | 15.22 | \ | \ | \ |
QALY: Quality-adjusted life year; ICER:Incremental cost-effectiveness ratio; INMB: Incremental net monetary benefit.
In conclusion, the stapokibart group achieved 0.10 more QALYs than the dupilumab group, with a cost reduction of $1103.95. Stapokibart not only increased utility but also reduced treatment costs, indicating an absolute cost–effectiveness advantage.
| Cost | QALY | Incremental cost | Incremental QALYs | ICER | INMB | |
|---|---|---|---|---|---|---|
| Stapokibart | $80,923.24 | 15.32 | $207.22 | 0.101 | 2043.48 | 1156.21 |
| Dupilumab | $80,716.02 | 15.22 | \ | \ | \ | \ |
QALY: Quality-adjusted life year; ICER:Incremental cost-effectiveness ratio; INMB: Incremental net monetary benefit.
Sensitivity analysis
Deterministic sensitivity analysis
A deterministic sensitivity analysis was performed on the model parameters to assess the impact of parameter variations on result robustness, producing the tornado diagram (Figure 3). The main parameters that influenced the results of the analysis included stapokibart disease control maintenance probability and dupilumab disease control maintenance probability, the price of dupilumab, inadequately controlled utility, adequately controlled utility, the price of stapokibart, the price of mepolizumab, the price of dupilumab, with other parameters having minimal impact on the results. Transition probability and utility are key model parameters that exert the greatest influence on the number of patients in each health state. As biologics are relatively expensive, their unit price significantly impacts the results. Therefore, these factors have a larger impact on the study results. The tornado diagram shows that the model results are relatively robust.
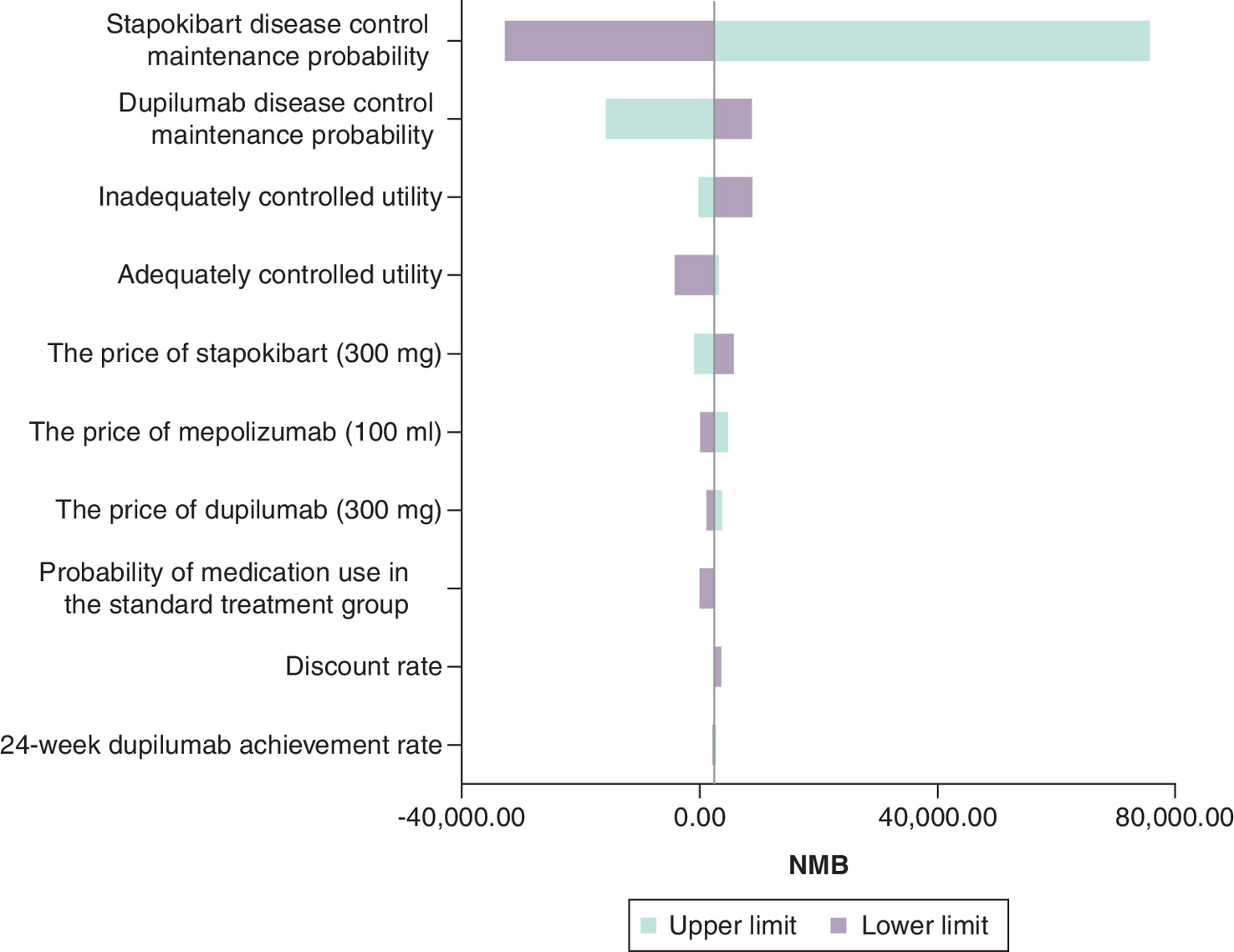
Figure 3. Results of the deterministic sensitivity analysis.
NMB: Net monetary benefit.
Probabilistic sensitivity analysis
In the PSA, a scatter plot (Figure 4) was generated based on 10,000 Monte Carlo simulations. Applying a conventional WTP threshold of $13,445 per unit of gained benefit, stapokibart is cost-effective in 83.09%. Applying a conventional WTP threshold of $40,335 per unit of gained benefit, stapokibart is cost-effective in 68.97% of the cases.
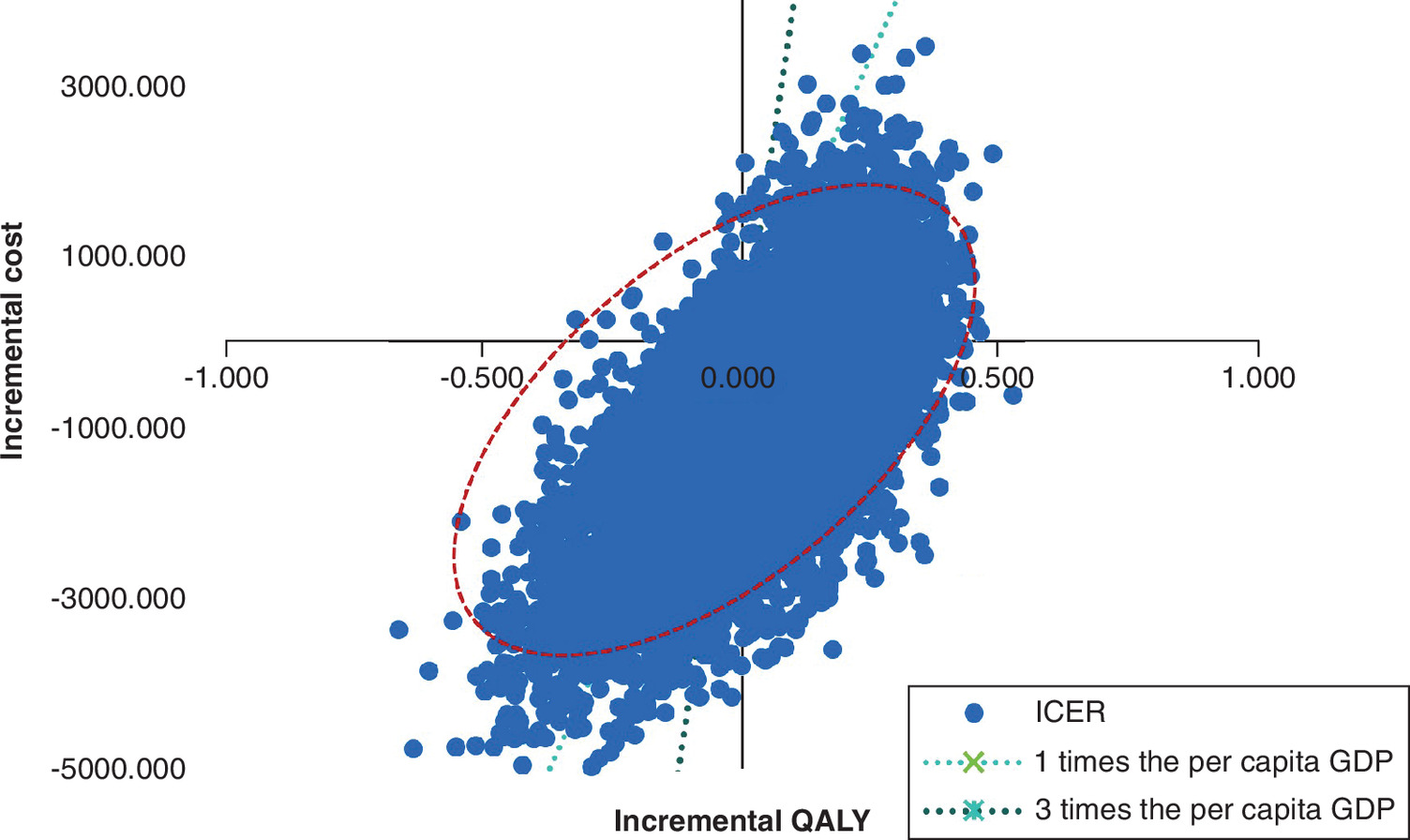
Figure 4. Monte Carlo scatter plot.
GDP: Gross domestic product; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
The WTP value for each QALY ranges from 0 to $47,000, and a CEAC is generated (Figure 5). The CEAC suggests that the cost–effectiveness conclusions are robust. The CEAC indicates that the cost–effectiveness conclusions are robust. At a WTP threshold of one and three-times the per capita GDP, the curve shows that the stapokibart group has a higher probability of being cost-effective than the dupilumab group.
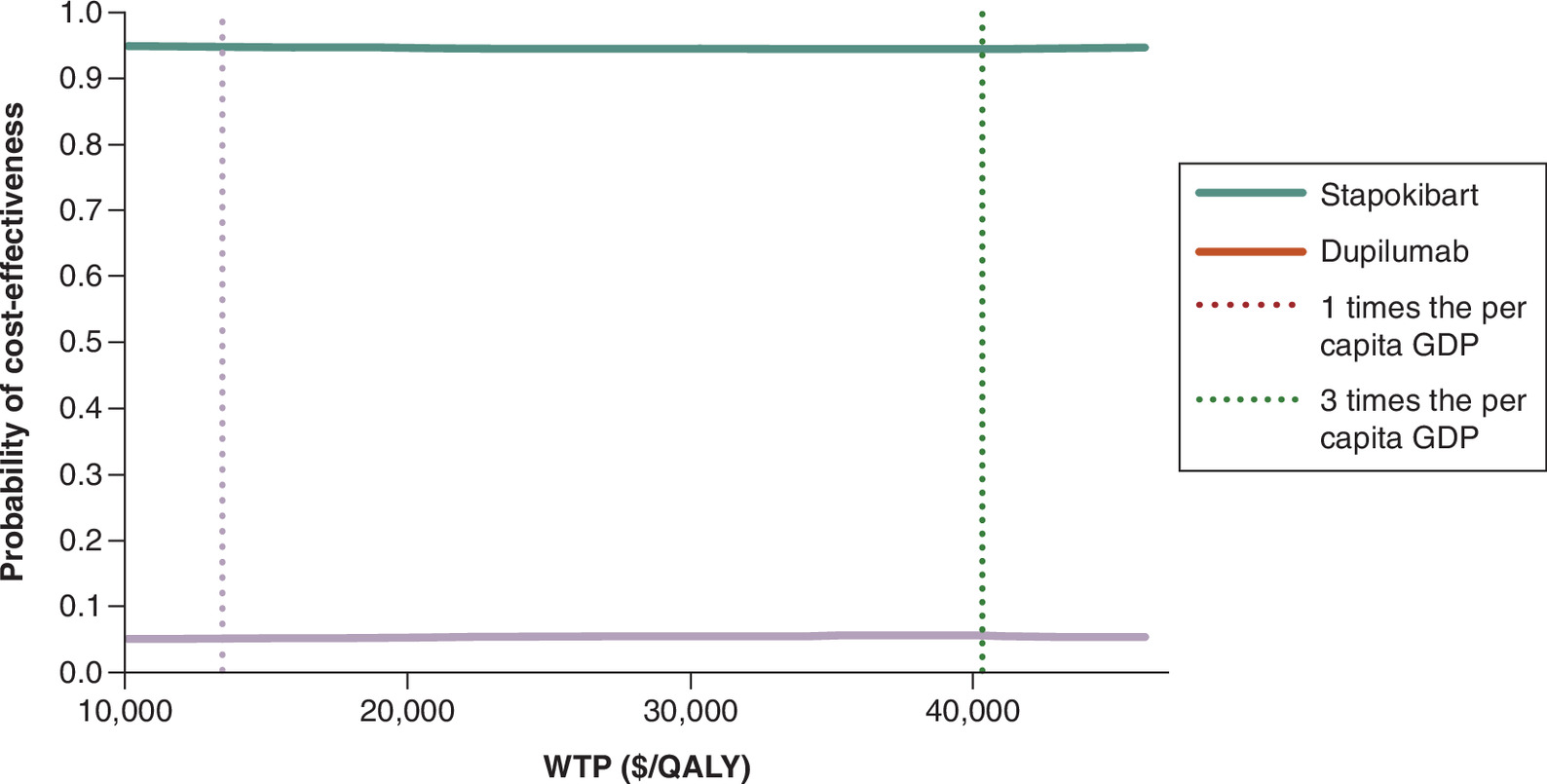
Figure 5. Cost–effectiveness acceptability curve.
GDP: Gross domestic product; QALY: Quality-adjusted life year; WTP: Willingness to pay.
Scenario analysis
In the price-equalized scenario analysis, stapokibart was associated with an incremental cost of 207.22 and an incremental gain of approximately 0.101 QALYs versus dupilumab, resulting in an ICER of 2043.48 per QALY gained, which remained well below the WTP threshold of 13,445. Therefore, stapokibart was no longer dominant but remained cost-effective (Table 7).
Discussion
The study aims to compare the cost–effectiveness of stapokibart and dupilumab in treating CRSwNP patients unresponsive to standard treatment, from the healthcare system perspective. By constructing the decision tree Markov model, the study compares the economic viability of stapokibart and dupilumab treatment options for CRSwNP in China. The basic analysis results indicate that the stapokibart group offers a clear economic advantage over the dupilumab group. The sensitivity analysis shows that the model results are robust. At one to siya kolthree-times China’s per capita GDP, stapokibart is cost-effective compared with dupilumab. The price-equalized scenario analysis showed that, although stapokibart was no longer dominant, it remained cost-effective, indicating that its economic advantage was not solely attributable to price differences.
Stapokibart is a humanized IgG4 monoclonal antibody targeted against the interleukin (IL)-4 receptor alpha subunit (IL-4Rα). By binding IL-4Rα, stapokibart blocks the binding by (and subsequent signaling of) IL-4 and IL-13, two type 2 cytokines. stapokibart shows broad and significant efficacy in treating CRSwNP. It alleviates symptoms, improves imaging results, enhances quality of life and reduces reliance on traditional treatments. Research indicates that frequent nasal symptoms and comorbidities cause significant social dysfunction and mental health issues, particularly increasing the risk of depression and anxiety in patients with CRSwNP. Their quality of life scores are much lower than those of the general population [24]. Treatment with stapokibart significantly improves patients’ quality of life. The survey also indicates that 56.7% of patients report limitations in social activities due to symptoms, and 34.2% experience a work efficiency reduction of over 30%. Worryingly, the postoperative recurrence rate is as high as 18.3%, and the number of work absenteeism days for recurrence patients is 3.2-times that of nonrecurrence patients [25]. Treatment with stapokibart can partially replace surgery, thereby indirectly reducing social resource loss and productivity decline.
Besides CRSwNP, stapokibart is also indicated for severe atopic dermatitis (approved in China on 12 September 2024) and allergic rhinitis (approved on 17 February 2025). Using a drug across multiple indications broadens the treated population, enabling fixed costs to be spread over a larger volume and lowering the marginal cost per patient. Biologics have provided an important treatment option for patients with refractory CRSwNP who do not respond to conventional therapy or surgery. However, their high cost poses challenges in terms of long-term affordability and accessibility.
A limitation of this study is that adjustment for multiple baseline characteristics may substantially reduce the effective sample size, which in turn can compromise the statistical power to detect differences between treatment groups. Moreover, despite adjustment for available baseline characteristics, including age, sex, NPS and SNOT-22, unobserved or unreported confounding factors between the CROWNS-2 and SINUS-52 trials may still exist and could influence the estimated magnitude of stapokibart’s superiority.
Conclusion
Based on data from China, the efficacy comparison shows that stapokibart has better clinical outcomes than dupilumab. This study also shows that the stapokibart group has a clear economic advantage over the dupilumab group, by improving patients’ symptoms, enhancing quality of life and indirectly boosting social productivity.
Summary points
•
Stapokibart and dupilumab are biologic treatments for chronic rhinosinusitis with nasal polyps (CRSwNP).
•
This study assessed the cost–effectiveness of stapokibart compared with dupilumab from the healthcare system perspective in China.
•
Decision tree Markov model was used to estimate long-term costs and health outcomes.
•
Because no direct comparison trial was available, a matching-adjusted indirect comparison was conducted using data from separate clinical studies.
•
In the base-case analysis, stapokibart was associated with lower treatment costs and higher QALYs than dupilumab.
•
Sensitivity analyses showed that the base-case results were robust.
•
In the price-equalized scenario analysis, stapokibart was no longer dominant but remained cost-effective.
•
Stapokibart may represent an economically favorable treatment option for CRSwNP in China.
Author contributions
J Yang: methodology, validation, data curation, writing – original draft, writing – review and editing; L Ren: funding acquisition, validation, writing – review & editing; F Xie: methodology, data curation; R Shao: supervision, project administration; R Jiang: validation, supervision, project administration, writing – review and editing.
Financial disclosure
The author(s) received no financial and/or material support for this research or the creation of this work.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Data sharing statement
The author confirms that all data generated or analyzed during this study are included in this published article.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Editorial Board of Chinese Journal of Otorhinolaryngology Head and Neck Surgery, Rhinology Group of Otorhinolaryngology Head and Neck Surgery Branch of Chinese Medical Association, Jiang Y et al. China guidelines for the diagnosis and treatment of chronic rhinosinusitis (2024). Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 60(3), 221–249 (2025).
2.
Li D. Clinical Study on the Improvement of Olfactory Dysfunction in Patients with Chronic Rhinosinusitis without Nasal Polyps Using Nasal Three-Injection Therapy [Dissertation]. Guangzhou University of Chinese Medicine, Guangzhou, China (2023).
3.
Bachert C, Bhattacharyya N, Desrosiers M, Khan AH. Burden of disease in chronic rhinosinusitis with nasal polyps. J. Asthma Allergy. 14, 127–134 (2021).
4.
Bhattacharyya N, Villeneuve S, Joish VN et al. Cost burden and resource utilization in patients with chronic rhinosinusitis and nasal polyps. Laryngoscope 129(9), 1969–1975 (2019).
5.
Chen S, Zhou A, Emmanuel B, Garcia D, Rosta E. Systematic literature review of humanistic and economic burdens of chronic rhinosinusitis with nasal polyposis. Curr. Med. Res. Opin. 36(11), 1913–1926 (2020).
6.
Liu YB, Liu YC, Sun AX et al. Current status of symptom distress in patients with chronic rhinosinusitis with nasal polyps and its relationship with negative emotions and quality of life. Dang Dai Hu Shi 31(8), 117–121 (2024).
7.
Yong M, Kirubalingam K, Desrosiers MY, Kilty SJ, Thamboo A. Cost-effectiveness analysis of biologics for the treatment of chronic rhinosinusitis with nasal polyps in Canada. Allergy Asthma Clin. Immunol. 19(1), 90 (2023).
8.
Yong M, Wu YQ, Howlett J, Ballreich J, Walgama E, Thamboo A. Cost-effectiveness analysis comparing dupilumab and aspirin desensitization therapy for chronic rhinosinusitis with nasal polyposis in aspirin-exacerbated respiratory disease. Int. Forum Allergy Rhinol. 11(12), 1626–1636 (2021).
9.
De Corso E, Furneri G, Salsi D et al. Cost-utility analysis of dupilumab for the treatment of chronic rhinosinusitis with nasal polyps (CRSwNP) in Italy. J Pers Med. 12(6), 951 (2022).
• Methodological reference for cost–utility analysis of biologic therapies in chronic rhinosinusitis with nasal polyps (CRSwNP).
10.
Scangas GA, Wu AW, Ting JY et al. Cost utility analysis of dupilumab versus endoscopic sinus surgery for chronic rhinosinusitis with nasal polyps. Laryngoscope 131(1), E26–E33 (2021).
11.
Shen S, Yan B, Wang M et al. Stapokibart for severe uncontrolled chronic rhinosinusitis with nasal polyps: the CROWNS-2 Randomized Clinical Trial. JAMA 334(11), 962–972 (2025).
•• Key clinical data source for the efficacy and safety of stapokibart in severe uncontrolled CRSwNP.
12.
Bachert C, Han JK, Desrosiers M et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group Phase III trials. Lancet 394(10209), 1638–1650 (2019).
•• Key clinical data source for the efficacy and safety of stapokibart in severe uncontrolled CRSwNP.
13.
Hong HY, Zhang Y, Wang TC et al. Chinese expert consensus on the use of biologics in patients with chronic rhinosinusitis. ORL J. Otorhinolaryngol. Relat. Spec. 85(3), 128–140 (2023).
• Chinese expert consensus on the use of biologics in patients with chronic rhinosinusitis.
14.
National Health Commission of the People's Republic of China. Statistical bulletin on the development of China's health undertaking in 2023. National Health Commission website. (2024). (Accessed: 10 July 2025). https://file.m12333.cn/upfile/download/bf66337f-795a-c925-d6fc-efa4f99495c8.pdf
15.
Zhao Q, Yu L, Jin P et al. A comprehensive investigation of the demographics, treatments, comorbidities, and disease burden of chronic rhinosinusitis with nasal polyposis patients: a descriptive analysis. Ann. Transl. Med. 10(3), 150 (2022).
16.
Liu YX, Wang RT, Li GW. Application of matching-adjusted indirect comparison in medical research. Chin. J. Evid. Based Med. 22(10), 1201–1205 (2022).
17.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. (6), –691 (1997).
18.
World Health Organization. Life tables by country: China. Global Health Observatory data repository. (2025). (Accessed: 10 July 2025). https://apps.who.int/gho/data/view.main.60340?lang=en
19.
Gong Y, Lin C, Jin Y et al. The efficacy and cost-effectiveness of umeclidinium/vilanterol versus tiotropium in symptomatic patients with chronic obstructive pulmonary disease. Can. Respir. J. 2022, 2878648 (2022).
20.
Lin YT, Wang C, He XY et al. Comparative cost-effectiveness of first-line pembrolizumab plus chemotherapy vs. chemotherapy alone in persistent, recurrent, or metastatic cervical cancer. Front. Immunol. 14, 1345942 (2024).
21.
China guidelines for pharmacoeconomic evaluations (2020 edition). China Medical Science Press, Beijing, China (2020).
•• Core methodological guidance for pharmacoeconomic evaluation in China.
22.
National Bureau of Statistics of China. National data. National Bureau of Statistics of China website. (2025). (Accessed: 10 July 2025). http://data.stats.gov.cn/
23.
Cai D, Shi S, Jiang S et al. Estimation of the cost-effective threshold of a quality-adjusted life year in China based on the value of statistical life. Eur. J. Health Econ. 23(4), 607–615 (2022).
24.
Bachert C, Bhattacharyya N, Desrosiers M et al. Burden of disease in chronic rhinosinusitis with nasal polyps. J. Asthma Allergy 14, 127–134 (2021).
25.
Peters AT, Bengtson LGS, Chung Y et al. Clinical and economic burden of chronic rhinosinusitis with nasal polyposis: a US administrative claims analysis. Allergy Asthma Proc. 43(5), 435–445 (2022).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 18 November 2025
Accepted: 24 April 2026
Published online: 20 May 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Economic evaluation of stapokibart for chronic rhinosinusitis with nasal polyps in China: a cost–effectiveness analysis. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0189
Export citation
Select the citation format you wish to export for this article or chapter.