Association of physical activity levels and estimated glomerular filtration rate with all-cause mortality: a 10-year cohort study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Many studies have demonstrated that physical inactivity and reduced renal function are associated with an increased risk of all-cause mortality. However, most of this evidence is derived from non-Chinese populations. This study aimed to investigate the association of physical activity (PA) with the risk of all-cause mortality among Chinese adults with and without impaired kidney function. Materials & methods: We conducted a prospective cohort study among a population in Jiangsu Province, China. Cox proportional hazards regression models were used to explore the associations of estimated glomerular filtration rate (eGFR) and PA with all-cause mortality, as well as to test for potential interactions between eGFR and PA. Results: A total of 6266 participants with complete data were included in the analysis, with a median age of 52 years and 44% being male. Of these participants, 1034 (16.5%) had an eGFR <60 ml/min/1.73 m2. During a median follow-up 9.1 years (interquartile range [IQR]: 7.7–9.9), 196(3.1%) participants died. Participants with eGFR <60 ml/min/1.73 m2 had a significantly higher risk of death (hazard ratio [HR] = 1.93; 95% confidence interval [CI]: 1.39–2.68) compared with eGFR ≥60 ml/min/1.73 m2. A significant interaction was observed between PA and eGFR in relation to all-cause mortality risk (p for interaction = 0.004). Notably, participant with eGFR <60 ml/min/1.73 m2 and low PA had a highest risk of all-cause mortality, compared with those with eGFR ≥60 ml/min/1.73 m2 and high PA (HR: 4.06; 95% CI: 2.34–7.03). Conclusion: PA, a key lifestyle factor, is a potentially modifiable risk factor for both individuals with normal renal function and those with impaired kidney function. Consistent with existing literature, participants with decreased renal function exhibited a significantly higher risk of all-cause mortality. Notably, our analysis further revealed that the risk of all-cause mortality was the highest among participants with impaired renal function and low PA.
Plain language summary: The relationship between physical activity & all-cause mortality risk in Chinese adults with normal or impaired kidney function
What is this article about?
This article focuses on exploring how physical activity (PA) affects the risk of death from any cause in Chinese adults, including those with or without impaired kidney function. Previous studies have shown that insufficient PA and having impaired kidney function can increase the risk of all-cause mortality. However, most relevant studies were conducted in non-Chinese populations. This study aims to fill this gap by investigating a Chinese adult cohort.
What were the results?
The researchers conducted a long-term prospective cohort study with 6266 adults from Jiangsu Province, China. The Cox proportional hazards regression models was used to analyze the relationships between estimated glomerular filtration rate (eGFR) and PA with all-cause mortality, and also tested whether eGFR and PA interact to affect mortality risk. The results showed that the median age of the participants was 52 years, and 44% were male; 16.5% (1034 participants) had impaired kidney function (eGFR <60 ml/min/1.73 m2). During a median follow-up of 9.1 years, 3.1% (196 participants) died. Participants with impaired kidney function had a significantly higher risk of death (hazard ratio [HR] = 1.93; 95% confidence interval [CI]: 1.39 to 2.68) compared with those with normal kidney function. There was a significant interaction between PA and eGFR (p for interaction = 0.004), and the highest risk of all-cause mortality was found in participants with impaired kidney function and low PA (HR: 4.06; 95% CI: 2.34–7.03) when compared with those with normal kidney function and high PA.
What do the results mean?
The results mean that PA is an important lifestyle factor that can be adjusted, and it is beneficial for both adults with or without impaired kidney function. Consistent with previous studies, people with impaired kidney function have a higher risk of all-cause mortality. Importantly, this study further found that the combination of impaired kidney function and low PA leads to the highest risk of death in Chinese adults. This is important because it provides targeted evidence for Chinese adults, especially those with impaired kidney function, to improve their health by increasing PA, which can help reduce the risk of death.
Chronic kidney disease (CKD) is defined as an estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2 and/or the presence of kidney damage markers (such as albuminuria) for at least 3 months [1]. CKD is recognized as a major global public health challenge, and it increases the risk of all-cause mortality, cardiovascular disease (CVD), and progression to kidney failure [2–4].
It was widely recognized that regular physical activity (PA) is essential for maintaining optimal human health. A study demonstrated that, regardless of renal function level, all recommended health-related lifestyle behaviors, including regular PA, were significantly associated with a reduced risk of mortality [5,6]. Furthermore, higher levels of PA were found to be linked to a decreased risk of premature mortality in the general population [7,8].
However, evidence exploring the relationship between PA and eGFR with all-cause mortality remains limited, particularly in the Chinese population, only individual studies have examined the separate relationships of PA or eGFR with mortality risk in Chinese population among older adults [9–11]. Results from a Canadian cohort study indicated that higher levels of PA were associated with a reduced risk of all-cause mortality among individuals with eGFR <30 ml/min/1.73 m2 [12]. In two separate multivariable Cox models, compared with the PA group, hazard ratios (95% CI) of mortality for insufficiently active and active groups were 0.60 (0.45–0.81) and 0.59 (0.45–0.77) in the non-CKD subpopulation and 0.58 (0.42–0.79) and 0.44 (0.33–0.58) in the CKD subpopulation [13,14]. The other study indicated that the active PA group also showed lower all-cause (HR: 0.76; 95% CI: 0.70–0.82) and protection against ≥50% eGFR decline (HR: 0.81; 95% CI: 0.68–0.97) compared with the inactive group in the fully adjusted Cox proportional hazards regression model [15].
To enrich the racial/ethnic diversity of study populations in this field and enhance the generalizability of research findings, we conducted the present study to investigate the association between PA and all-cause mortality risk among Chinese adults with or without impaired kidney function based on a 10-year cohort study.
Materials & methods
Study design & participants
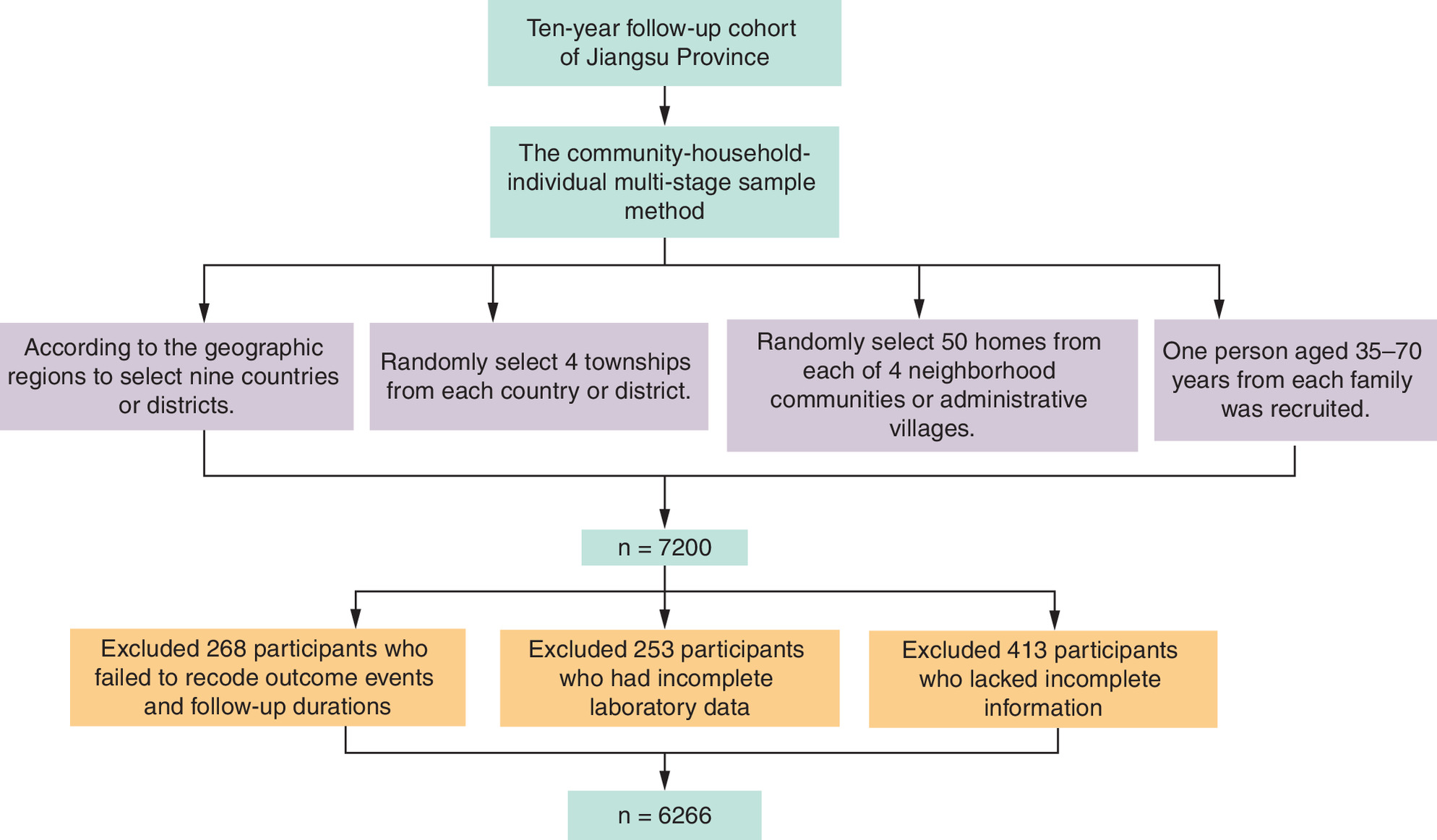
The community-household-individual multistage sample method was used to select participants representative of the general population in Jiangsu Province. In the first stage, nine counties or districts were selected according to the geographic regions (Northern, Central and Southern Jiangsu Province). In the second stage, four townships were randomly selected from each county or district using random number tables. In the third stage, 50 households were randomly selected from each of the four residential communities or administrative villages, with sampling probabilities proportional to community size. Finally, one eligible individual (exclusion criteria for study participants at baseline, in accordance with the survey design protocol, were as the following: acute phase of myocardial infarction or stroke within 3 months; severe cognitive, hearing or physical impairment resulting in poor cooperation; presence of severe comorbidities with a life expectancy of less than 1 year; voluntary refusal to participate in the study) aged 35–70 years from each household was recruited for the study according to the Kish selection table. Finally, a total of 7200 participants were enrolled at baseline. Socio-demographic characteristics, medication history, medical history, lifestyle behaviors and baseline laboratory data were collected between January 2008 and December 2008. The participants were followed up annually from January 2009 to December 2019. A total of 268 participants were excluded due to missing outcome events or follow-up time; 253 were excluded for incomplete laboratory data; and 413 were excluded due to missing data on PA, age, education level, smoking status, alcohol consumption, height, weight, history of disease and blood pressure. Eventually, a total of 6266 participants were included in the final analysis. Participants were classified into six groups based on renal function (eGFR ≥60 or eGFR <60 ml/min/1.73 m2) and PA levels (low/moderate/high) [6,16]. The study flow chart is presented in Figure 1. Death cases were verified through the death surveillance system of the Chinese Center for Disease Control and Prevention.
Informed consent
All participants provided written informed consent prior to enrollment. The study protocol was approved by the Ethics Review Committee of Jiangsu Provincial Center for Disease Control and Prevention (approval number: SL2015-B004-01). No individual-level identifiable data, including personal details, images or videos, are presented in this manuscript.
Baseline variables
Baseline information was collected via standardized questionnaires, including sociodemographic characteristics, lifestyle factors, medical history, and family history. Physical examination measurements comprised height, weight and blood pressure, while serum biochemical parameters were obtained through laboratory testing.
Height (without shoes) was measured to the nearest 0.1 cm using a stadiometer. Body weight was measured to the nearest 0.1 kg using an electronic scale with participants in light clothing and barefoot. BMI was calculated as weight in kilograms divided by height in meters squared. Participants were stratified into four groups based on Chinese national obesity guidelines [17]: underweight (BMI <18.5 kg/m2), normal weight (18.50 ≤ BMI <24.00 kg/m2), overweight (24.00 ≤ BMI <28.00 kg/m2) and obesity (BMI ≥28.00 kg/m2).
Blood pressure (mmHg) was measured in the left upper arm using an automated sphygmomanometer (Omron HEM-757; Omron, Kyoto, Japan). Each participant’s blood pressure was measured three-times at a 1 min interval, with the midpoint of the appropriate cuff at the same level as the heart. The final blood pressure was determined by averaging the three measurements. Hypertension was defined as a prior diagnosis of hypertension, current use of antihypertensive treatment, or an average measured systolic blood pressure of ≥140 mmHg and/or diastolic blood pressure of ≥90 mmHg.
Individuals were divided into three smoking groups: never smokers, former smokers (defined as those who had ceased smoking for more than 1 year), and current smokers (those who smoked tobacco products at any time in the past year, including those who had quit within the previous year) [18]. Regarding alcohol consumption, participants were considered drinkers if they had a history of drinking and consumed alcohol at least once a month in the past year [19].
At the baseline investigation, a 12 h fasting venous blood sample was obtained to measure creatinine, low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), total cholesterol (TC), triglyceride (TG) and fasting blood glucose (FBG). The blood samples were centrifuged, aliquoted, and stored in a -80°C freezer or -180°C liquid nitrogen for subsequent testing within 1 month.
A certified laboratory used glucose oxidase or hexokinase methods to measure FBG within 12 h after sample collection. Diabetes was defined as a self-reported diagnosis diabetes, current use of hypoglycemic drugs, or FBG ≥7.0 mmol/l [20].
Creatinine, TG, TC, HDL-C and LDL-C were measured using an autoanalyzer (Abbott Laboratories, USA) in Jiangsu Province Center for Disease Control and Prevention, which is certificated by The China National Laboratory Accreditation (CNLA). Dyslipidemia was defined as current use of antidyslipidemia treatment, or TC ≥6.22 mmol/l, and/or TG ≥2.26 mmol/l and/or LDL-C ≥4.14 mmol/l and/or HDL-C ≤ 1.04 mmol/l [21].
Renal function assessment
The body surface area (BSA) effect was not considered while calculating the creatinine clearance rate (CrCl) using the Cockcroft-Gault (CG) equation [22]. A modified CG equation was used to estimate eGFR in this study [23]. Thus, the eGFR was calculated as follows: eGFR = (1.73/BSA) × [(140 age) × weight(kg)]/(72 × creatinine(mg/dl) × 0.85(for female). BSA was calculated using the formula: BSA = 0.007184 × weight0.425 × height0.725 [24]. Reduced renal function (abnormal renal function) or CKD was defined as eGFR <60 ml/min/1.73 m2 [25]. Accordingly, participants were divided into two groups based on eGFR levels: eGFR ≥60 ml/min/1.73 m2 and eGFR <60 ml/min/1.73 m2 [25].
PA assessment
The International PA Questionnaire (IPAQ) was used to assess PA [26]. This scale covers four domains: household, transportation, recreational and occupational activity. Participants recalled all activities performed over the past week, including the number of active days, daily duration and activity intensity. Total PA, expressed as metabolic equivalent (MET)-min/week, was summed across the four domains. Weekly PA energy expenditure was calculated as: MET value of each activity × weekly frequency (d/w) × daily duration (min/d) [26]. Participants were further categorized into three PA level based on total MET-min/week: low (≤600 MET-min/week), moderate (600–3000 MET-min/week) and high (≥3000 MET-min/week) [6].
Follow-up & outcome events
Trained professional interviewer collected annual follow-up data on all-cause mortality for each participant via telephone or face-to-face interviews. Information regarding deaths was ascertained through household inquiry, medical records and official death certificates.
Statistical analysis
For categorical variables, baseline characteristics of participants were presented as percentages and frequencies. The Chi-square test was used to compare differences between groups. Renal function and all-cause mortality risk were analyzed using the Cox proportional hazard model. The proportional hazards assumption for the Cox regression model was evaluated using Schoenfeld residual plots and global tests. The assumption was satisfied for all variables included in the model (global test p > 0.05). Meanwhile, the multiplicative interaction between renal function and PA were assessed in the Cox model to investigate whether PA levels modify the associations between renal function and all-cause mortality. When examining the association of the combination of PA level and renal function with all-cause mortality, the group with high PA and eGFR ≥60 ml/min/1.73 m2 was used as the reference. Hazard ratio (HRs) and 95% CIs were reported. For all analyses, two nested models were constructed. Model 1 was adjusted for age, sex, region; Model 2 was further adjusted for BMI, alcohol consumption, smoking status, educational level, hypertension, dyslipidemia, diabetes, chronic respiratory disease, CVD, cancer and other covariates, while retaining adjustment for age, sex and region. The proportional hazards assumption was tested and satisfied for all variables in the Cox models. All statistical analyses were performed using SPSS 25.0. A 2-sided p-value < 0.05 was considered statistically significant.
Results
Baseline characteristics of the population based on renal function & PA level
Of the 7200 participants recruited from Jiangsu Province, 6266 eligible participants were included in our analysis, of whom 1034(16.5%) had an eGFR <60 ml/min/1.73 m2. A total of 2756 (44.0%) participants were male, and 3095 (49.4%) participants were from urban areas. Over a median follow-up of 9.1 years (IQR: 7.7–9.9), 196 (3.1%) deaths occurred. Table 1 presents the baseline characteristics of participants across groups. Age, sex, region, alcohol consumption, smoking status, education level, hypertension, cancer, chronic respiratory diseases, dyslipidemia, CVDs and BMI were all significantly different across the groups. Regardless of renal function level, the low PA group had the highest proportion of obese participants, whereas the high PA group had the lowest proportion of individuals with diabetes. In both the eGFR <60 ml/min/1.73 m2 and the eGFR ≥60 ml/min/1.73 m2 subgroups, the prevalence of dyslipidemia, hypertension and CVD was lowest in high PA group, followed by the moderate and low PA groups.
| Characteristics | eGFR ≥60 ml/min/1.73 m2 | eGFR <60 ml/min/1.73 m2 | p-value | ||||
|---|---|---|---|---|---|---|---|
| Low PA (n = 1009) | Moderate PA (n = 2349) | High PA (n = 1874) | Low PA (n = 219) | Moderate PA (n = 499) | High PA (n = 316) | ||
| Age (years) | <0.001 | ||||||
| 35–44 | 388 (38.5) | 718 (30.6) | 666 (35.5) | 1 (0.5) | 7 (1.4) | 12 (3.8) | |
| 45–54 | 319 (31.6) | 858 (36.5) | 688 (36.7) | 29 (13.2) | 75 (15.0) | 52 (16.5) | |
| 55–70 | 302 (29.9) | 773 (32.9) | 520 (27.7) | 189 (86.3) | 417 (83.6) | 252 (79.7) | |
| Male | 545 (54.0) | 903 (38.4) | 877 (46.8) | 98 (44.7) | 188 (37.7) | 145 (45.9) | <0.001 |
| Urban | 510 (50.5) | 1272 (54.2) | 928 (49.5) | 81 (37.0) | 193 (38.7) | 111 (35.1) | <0.001 |
| Smoking status | <0.001 | ||||||
| Former | 37 (3.7) | 73 (3.1) | 57 (3.0) | 9 (4.1) | 22 (4.4) | 14 (4.4) | |
| Current | 362 (35.9) | 542 (23.1) | 530 (28.3) | 59 (26.9) | 113 (22.6) | 84 (26.6) | |
| Never | 610 (60.5) | 1734 (73.8) | 1287 (68.7) | 151 (68.9) | 364 (72.9) | 218 (69.0) | |
| Education level | <0.001 | ||||||
| None, primary or unknown | 255 (25.3) | 760 (32.4) | 588 (31.4) | 126 (57.5) | 276 (55.3) | 182 (57.6) | |
| Secondary/High/Higher secondary | 728 (72.2) | 1513 (64.4) | 1218 (65.0) | 80 (36.5) | 209 (41.9) | 122 (38.6) | |
| Trade or College/University | 26 (2.6) | 76 (3.2) | 68 (3.6) | 13 (5.9) | 14 (2.8) | 12 (3.8) | |
| Alcohol consumption | 315 (31.2) | 460 (19.6) | 476 (25.4) | 42 (19.2) | 96 (19.2) | 72 (22.8) | <0.001 |
| Hypertension | 395 (39.1) | 884 (37.6) | 670 (35.8) | 127 (58.0) | 253 (50.7) | 155 (49.1) | <0.001 |
| BMI | <0.001 | ||||||
| Underweight, <18.5 kg/m2 | 23 (2.3) | 34 (1.4) | 44 (2.3) | 16 (7.3) | 38 (7.6) | 23 (7.3) | |
| Normal, 18.5–23.9 kg/m2 | 403 (39.9) | 1021 (43.5) | 880 (47.9) | 122 (55.7) | 308 (61.7) | 190 (60.1) | |
| Overweight, 24–27.9 kg/m2 | 396 (39.2) | 899 (38.3) | 688 (36.7) | 63 (28.8) | 135 (27.1) | 91 (28.8) | |
| Obesity, ≥28 kg/m2 | 187 (18.5) | 395 (16.8) | 262 (14.0) | 18 (8.2) | 18 (3.6) | 12 (3.8) | |
| Chronic respiratory disease | 15 (1.5) | 40 (1.7) | 44 (2.3) | 3 (1.4) | 9 (1.8) | 14 (4.4) | 0.018 |
| Diabetes | 97 (9.6) | 207 (8.8) | 155 (8.2) | 19 (8.7) | 45 (9.0) | 25 (7.9) | 0.874 |
| Cancer | 15 (1.5) | 14 (0.6) | 22 (1.2) | 5 (2.3) | 2 (0.4) | 4 (1.3) | 0.027 |
| CVD | 59 (5.8) | 84 (3.6) | 54 (2.9) | 24 (11.0) | 35 (7.0) | 17 (5.4) | <0.001 |
| Dyslipidemia | 327 (32.4) | 738 (31.4) | 521 (22.2) | 67 (30.6) | 130 (26.1) | 73 (23.1) | 0.001 |
Data are n (%); some values shown in the table may not add up to 100% owing to rounding; chronic respiratory disease: self-reported chronic obstructive pulmonary disease, tuberculosis and asthma; CVD: self-reported stroke, heart failure, coronary heart disease and any other heart disease; cancer: self-reported cancer, including all cancer types except for nonmelanoma skin cancers.
eGFR: Estimated glomerular filtration rate; PA: Physical activity.
Association of renal function or PA with all-cause mortality
Table 2 shows that the HR for all-cause mortality (HR: 1.97; 95% CI: 1.44–2.70) was substantially higher in participants with eGFR <60 ml/min/1.73 m2 than in those with eGFR ≥ 60 ml/min/1.73 m2 in the models adjusted for age, sex and region. This association remained significant even after further adjustment for additional confounding variables. Individuals with moderate PA levels had a significantly higher risk of all-cause death (HR: 1.50; 95% CI: 1.07–2.10) compared with those with high PA levels.
| Variable | Renal function (ml/min/1.73 m2) | PA | |||
|---|---|---|---|---|---|
| eGFR ≥60 | eGFR <60 | High | Low | Moderate | |
| Model 1 | 1.00 | 1.97 (1.44, 2.70) | 1.00 | 1.28 (0.85, 1.92) | 1.43 (1.03, 1.99) |
| Model 2 | 1.00 | 1.93 (1.39, 2.68) | 1.00 | 1.34 (0.89, 2.02) | 1.50 (1.07, 2.10) |
Model 1 was adjusted for age, sex, location; Model 2 was adjusted for BMI, alcohol use, tobacco use, education, hypertension, dyslipidemia, diabetes, chronic respiratory disease, CVD, cancer, while adjusted age, sex and location.
eGFR: Estimated glomerular filtration rate; PA: Physical activity.
Cox proportional hazards regression analysis of PA level & all-cause mortality across renal function strata
Significant association was observed between renal function and PA in relation to all-cause mortality (p = 0.004) (Table 3). In the fully adjusted model, among participants with eGFR ≥60 ml/min/1.73 m2, individuals with moderate PA presented a higher hazard of all-cause mortality (HR: 1.84; 95% CI: 1.20–2.81) compared with those in the high PA group. For participants with reduced renal function (eGFR <60 ml/min/1.73 m2), low PA was independently associated with an increased risk of all-cause mortality (HR: 1.88; 95% CI: 1.03–3.44), relative to the high PA reference group.
| Total/deaths | High | Low | Moderate | Pinteraction | |
|---|---|---|---|---|---|
| Model 1 | |||||
| eGFR ≥60 ml/min/1.73 m2 | 5232/116 | 1.00 | 0.83 (0.45, 1.53) | 1.76 (1.16, 2.68) | 0.003 |
| eGFR <60 ml/min/1.73 m2 | 1034/80 | 1.00 | 1.89 (1.06, 3.35) | 1.02 (0.59, 1.76) | |
| Model 2 | |||||
| eGFR ≥60 ml/min/1.73 m2 | 5232/116 | 1.00 | 0.87 (0.47, 1.61) | 1.84 (1.20, 2.81) | 0.004 |
| eGFR <60 ml/min/1.73 m2 | 1034/80 | 1.00 | 1.88 (1.03, 3.44) | 1.10 (0.63, 1.93) |
Model 1 was adjusted for age, sex, location; Model 2 was adjusted for model 1 plus BMI, alcohol use, tobacco use, education, hypertension, dyslipidemia, diabetes, chronic respiratory disease, CVD, cancer.
EGFR: Estimated glomerular filtration rate.
HRs of all-cause mortality based on renal function & PA
Figure 2 illustrated the all-cause mortality risks according to the combined categories of PA and renal function. In model 2, compared with participants with eGFR ≥60 ml/min/1.73 m2 and high PA, those with eGFR <60 ml/min/1.73 m2 and low PA exhibited the highest risk of all-cause mortality (HR: 4.06; 95% CI: 2.34–7.03). This was followed by individuals with eGFR <60 ml/min/1.73 m2 and moderate PA (HR: 2.29; 95% CI: 1.36–3.86) and those with eGFR <60 ml/min/1.73 m2 and high PA (HR: 2.06; 95% CI: 1.18–3.62). Conversely, among participants with eGFR ≥60 ml/min/1.73 m2, low PA was not associated with a statistically significant all-cause mortality risk relative to high PA (HR: 0.86, 95% CI: 0.47–1.59).
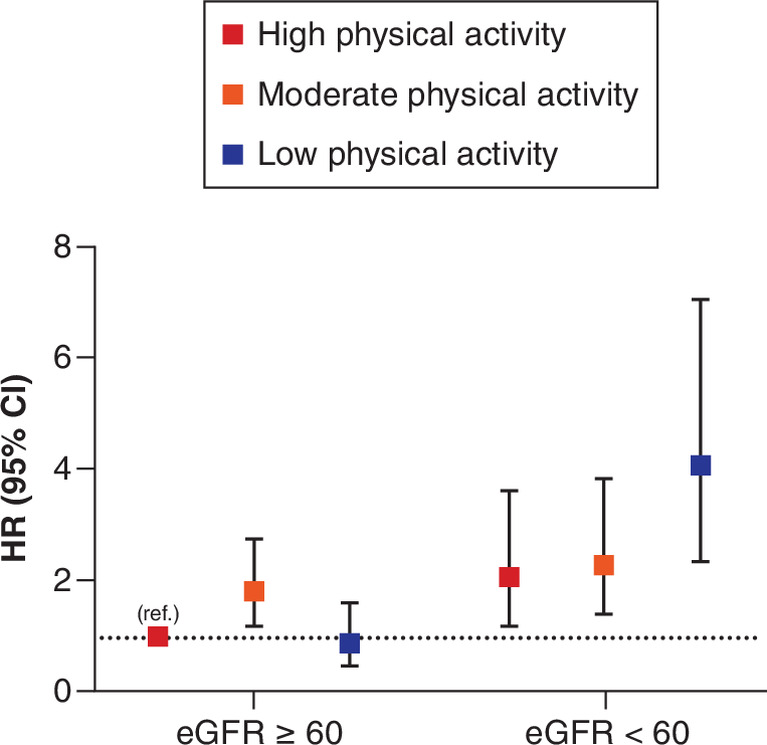
Figure 2. Plot of hazard ratios for all cause mortality by physical activity level and kidney function.
HRs of all-cause mortality according to PA and renal function status; individuals with eGFR ≥60 ml/min/1.73 m2 and high PA were used as the reference group(ref.); the model was adjusted for age, sex, location, BMI, alcohol use, tobacco use, education, hypertension, dyslipidemia,diabetes, chronic respiratory disease, CVD, cancer.
eGFR: Estimated glomerular filtration rate; HR: Hazard ratio; PA: Physical activity.
Discussion
This study demonstrated that reduced renal function is associated with an increased risk of all-cause mortality in the Jiangsu Province population. These findings are consistent with those of previous studies, which have identified an eGFR <60 ml/min/1.73 m2 as an independent risk factor for all-cause mortality [4]. Several studies have indicated that a decline in eGFR can accelerate the progression of hypertension, anemia, myocardial dystrophy, proteinuria [27,28], thereby, increasing the risk of mortality in the elderly population. Compared with the general population, patients with CKD tend to be more physically inactive and exhibit lower levels of PA [29]. This association is multifactorial and may be attributed to a combination of malnutrition, anemia, vascular dysfunction, sarcopenia and neuropathy [30–32].
In order to explore how PA levels influence the risk of all-cause mortality among individuals with reduced renal function, we adopted the Cox proportional hazards models to analyze the association of PA and eGFR with all-cause mortality. Our results of this study showed that lower PA significantly increased the risk of all-cause mortality in participants with impaired renal function. The finding is consistent with previous studies, which have demonstrated that physical inactivity is associated with increased mortality in both CKD and non-CKD populations [29]. Multiple potential mechanisms may explain why low level of PA increases the risk of mortality in patients with renal diseases. First, CVD is the leading cause of mortality among CKD patients [33]. PA confers multiple health benefits, including a reduced risk of CVD by lowering blood pressure, cholesterol, systemic inflammation, blood glucose and oxidative stress [34–37]. Second, regular exercise can not only slow the progression of CKD to end-stage renal disease, but also improve the quality of life and long-term survival of end-stage renal disease patients [38]. Furthermore, PA is especially meaningful for individuals with kidney disease. It reduces C-reactive protein levels in a dose-response pattern [39], and may alleviate frailty by improving cardiovascular fitness and muscle strength [40].
Renal function and PA were only measured at baseline in this study, while all-cause deaths occurred during follow-up period, which ensures a reasonable temporal sequence of association. The present results indicated that participants with both reduced eGFR (eGFR <60 ml/min/1.73 m2) and low PA had a 4.06-fold higher risk of all-cause mortality compared with the reference group (high PA and eGFR ≥60 ml/min/1.73 m2). Compared with the reference group, individuals with reduced eGFR (eGFR <60 ml/min/1.73 m2) but high PA still presented an elevated mortality risk, with an HR of 2.06. These findings highlight that targeted interventions for individuals with low PA levels may yield greater benefits in populations with impaired renal function, which provides important implications for public health strategies. Our results are consistent with those of a multicenter prospective cohort studies, which demonstrated that higher PA was associated with an approximately 50% reduction in all-cause mortality among patients with advanced CKD [7]. Furthermore, we were extend the findings of Artero et al. to individuals with preserved renal function. These findings have critical implications for secondary prevention in patients with impaired renal function, especially those with insufficient PA, who may derive the greatest survival benefits from PA promotion interventions. This study further confirms that low is PA a major independent modifiable risk factor for adverse health outcome. Routine screening and targeted lifestyle intervention should be recommended for all adults, regardless of renal function status.
Our findings should be interpreted in the context of several limitations. First, PA is prone to measurement bias, given the inherent limitations and discrepancies of self-reported activity data. Second, eGFR and key variables (including BMI, blood pressure, blood lipids) may fluctuate during the 10-year follow-up period. Single baseline eGFR, PA, blood lipid, BMI, and other factors, such as exposure misclassification, residual confounding, reverse causality, differences between occupational versus leisure PA, or other sources of bias may therefore weaken the predictive performance for long-term clinical outcome. Third, In Cox regression analysis we adjusted for BMI, hypertension, diabetes, dyslipidemia, CVD, cancer and other covariates. Several of these variables may lie on the causal pathway linking PA to mortality. Over-adjustment for such intermediate factors may attenuate the total effect of PA and bias the interpretation of interaction analyses. In addition, given that commonly used eGFR equations incorporate weight (and BSA is derived from weight and height), additional adjustment for BMI may introduce collinearity and collider bias, thereby complicating the interpretation of eGFR-related associations. Fourth, as an observational prospective cohort study, our analysis cannot establish a definitive causal relationship between PA in all-cause mortality. In addition, only serum creatinine data were available in our study, and information on proteinuria was lacking. Despite these limitations, our study possesses notable strengths, including a relatively large sample size and a 10-year prospective follow-up from Jiangsu Province. Furthermore, all data were collected through systematic and standardized procedures with high quality. A wide range of potential confounding factors were adequately adjusted for, enabling a robust assessment of the independent associations between renal function, PA and all-cause mortality.
Conclusion
In summary, participants with decreased renal function present a higher risk of all-cause mortality. Lower PA is independently associated with an elevated mortality risk, regardless of renal function status. Notably, the highest all-cause mortality risk was observed in patients with impaired renal function and low PA. Our findings highlight that PA is a critical modifiable lifestyle factor for both individuals with and without kidney disease.
Summary points
•
Previous studies have linked physical activity (PA) and reduced renal function to increased all-cause mortality, but most evidence comes from non-Chinese populations.
•
This study aimed to explore the association between PA and all-cause mortality risk in Chinese adults with normal or impaired kidney function.
•
A prospective cohort study was conducted among a population in Jiangsu Province, China, using Cox proportional hazards regression models for analysis.
•
A total of 6266 participants with complete data were included, with a median age of 52 years and 44% being male.
•
Among the participants, 1034 (16.5%) had impaired kidney function (eGFR <60 ml/min/1.73 m2).
•
The median follow-up period was 9.1 years, during which 196 (3.1%) participants died.
•
Participants with impaired kidney function had a significantly higher all-cause mortality risk (HR: 1.93; 95% CI: 1.39–2.68) than those with normal kidney function.
•
There was a significant interaction between PA and eGFR in relation to all-cause mortality risk (p for interaction = 0.004).
•
Participants with impaired kidney function and low PA had the highest all-cause mortality risk (HR: 4.06; 95% CI: 2.34–7.03) compared with those with normal kidney function and high PA.
•
PA is a modifiable lifestyle factor for Chinese adults regardless of renal status, and PA level interacts with kidney function to influence all-cause mortality risk.
Author contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication. Study concept and design: Q Xiang, H Jin, J Liu, Y Zhang. Acquisition of data: H Jin, L Cui, J Liu, D Wang, X Chen, Y Qin. Analysis and interpretation of data: H Jin, L Cui, J Liu, Y Qin. Drafting of the manuscript: H Jin, L Cui, J Liu, Q Xiang. Critical revision of the manuscript for important intellectual content: Q Xiang, Y Zhang, Y Qin. Statistical analysis: H Jin, J Liu, L Cui. Obtained funding: Q Xiang. Technical, or material support: Q Xiang, Y Zhang, Y Qin. Study supervision: Q Xiang.
Acknowledgments
The authors thank Z Wang and X Wang (Division of Prevention and Community Health, National Center for Cardiovascular Disease, Fuwai Hospital) for their constructive suggestions and technical support. The authors also thank all the colleagues from the study site involved in this survey.
Financial disclosure
This work was supported by the Natural Science Foundations of China (81973005), and the Projects in the Chinese National Science and Technology Pillar Program during the 12th five-year Plan Period (2011BAI11B01) PR, China.
Competing interests disclosure
The authors have no financial and/or nonfinancial competing interests or relevant affiliations with any organization/entity to declare that are relevant to the subject matter or materials discussed in this manuscript. This includes employment, grants or research funding, consultancies, membership on scientific or other advisory boards, honoraria, stock ownership or options, paid expert testimony, patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
All study participants provided written informed consent prior to enrollment. The study protocol was approved by the Ethics Review Committee of Jiangsu Provincial Center for Disease Control and Prevention (approval no.: SL2015-B004-01). No individual-level identifiable data, including personal details, images or videos, are presented in this manuscript.
Data sharing statement
The datasets used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Levey AS, Coresh J, Balk E et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann. Intern. Med. 139, 137–147 (2003).
2.
Levey AS, Atkins R, Coresh J et al. Chronic kidney disease as a global public health problem: approaches and initiatives - a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 72(3), 247–259 (2007).
3.
National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am. J. Kidney Dis. 39(Suppl. 21), S1–S266 (2002).
4.
Chronic Kidney Disease Prognosis Consortium, Matsushita K, van der Velde M et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 375, 2073–2081 (2010).
5.
Schrauben SJ, Hsu JY, Amaral S et al. Effect of kidney function on relationships between lifestyle behaviors and mortality or cardiovascular outcomes: a pooled cohort analysis. J. Am. Soc. Nephrol. 32(3), 663–675 (2021).
6.
Lear SA, Hu W, Rangarajan S et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. Lancet 390(10113), 2643–2654 (2017).
7.
Battaglia Y, Baciga F, Bulighin F et al. Physical activity and exercise in chronic kidney disease: consensus statements from the Physical Exercise Working Group of the Italian Society of Nephrology. J. Nephrol. 37(7), 1735–1765 (2024).
8.
Nocon M, Hiemann T, Müller-Riemenschneider F et al. Association of physical activity with all-cause and cardiovascular mortality: a systematic review and meta analysis. Eur. J. Cardiovasc. Prev. Rehabil. 15, 239–246 (2008).
9.
Yuan D, Chen H. The effect of glomerular filtration rate on mortality risk among elderly individuals. Chin. J. Gerontol. 33(3), 544–545 (2013).
10.
Wei J, Liu Z, Sun J et al. Association between physical activity and all-cause mortality risk and related mediators in middle-aged and elderly Chinese population: an analysis of CHARLS data. Chin. J. Public Health 40(6), 730–736 (2024).
11.
Chen X, Zhang J, Li L et al. Association between physical activity and risk of all-cause mortality in middle-aged and elderly people in China: a Prospective Cohort Study. Chin. Gen. Pract. 26(31), 3890–3895 (2023).
12.
Rampersad C, Brar R, Connelly K et al. Association of physical activity and poor health outcomes in patients with advanced CKD. Am. J. Kidney Dis. 78, 391–398 (2021).
13.
Kim H, Ko MJ, Lim CY et al. Association between physical activity and risk of renal function decline and mortality in community-dwelling older adults: a nationwide population-based cohort study. BMC Geriatr. 22(1), 973 (2022).
14.
Beddhu S, Baird BC, Zitterkoph J et al. Physical activity and mortality in chronic kidney disease (NHANES III). Clin. J. Am. Soc. Nephrol. 4(12), 1901–1906 (2009).
15.
Kim H, Ko MJ, Lim CY et al. Association between physical activity and risk of renal function decline and mortality in community-dwelling older adults: a nationwide population-based cohort study. BMC Geriatr. 22(1), 973 (2022).
16.
Expert Group on Kidney Clinical Quality Control Center in Shanghai. Guidelines for early screening, diagnosis, prevention and treatment of chronic kidney disease(2022 Edition). Chin. J. Nephrol. 38(5), 453–464 (2022).
17.
Zhou BF. Cooperative Meta-Analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults–study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed. Environ. Sci. 15, 83–96 (2002).
18.
O'Donnell MJ, Xavier D, Liu L et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 376, 112–123 (2010).
19.
World Health Organization. International guide for monitoring alcohol consumption and related harm. World Health Organization (2000). Available from: https://apps.who.int/iris/handle/10665/66529
20.
American Diabetes Association. 13. Management of diabetes in pregnancy: standards of Medical Care in Diabetes-2018. Diabetes Care 41, S137–S143 (2018).
21.
Joint committee for guideline revision. 2016 Chinese guidelines for the management of dyslipidemia in adults. J. Geriatr. Cardiol. 15, 1–29 (2018).
22.
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron 16, 31–41 (1976).
23.
Rostoker G, Andrivet P, Pham I et al. A modified Cockcroft-Gault formula taking into account the body surface area gives a more accurate estimation of the glomerular filtration rate. J. Nephrol. 20, 576–585 (2007).
24.
Du Bois D, Du Bois EF. A formula to estimate the approximate surface area if height and weight are known. Arch. Intern. Med. 17, 863–871 (1916).
25.
Yang JG, Li J, Lu C et al. Chronic kidney disease, all-cause mortality and cardiovascular mortality among Chinese patients with established cardiovascular disease. J. Atheroscler. Thromb. 17, 395–401 (2010).
26.
Craig CL, Marshall AL, Sjöström M et al. International PA questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 35(8), 1381–1395 (2003).
27.
Go AS, Chertow GM, Fan D et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization [published correction appears in N. Engl. J. Med. 18(4), 4 (2008)]. N. Engl. J. Med. 351, 1296–1305 (2004).
28.
Mok Y, Matsushita K, Ballew SH et al. Kidney function, proteinuria, and cancer incidence: The Korean Heart Study. Am. J. Kidney Dis. 70, 512–521 (2017).
29.
Beddhu S, Baird BC, Zitterkoph J et al. PA and mortality in chronic kidney disease (NHANES III). Clin. J. Am. Soc. Nephrol. 4, 1901–1906 (2009).
30.
Levey AS, Eckardt KU, Tsukamoto Y et al. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 67, 2089–2100 (2005).
31.
Thomas R, Kanso A, Sedor JR. Chronic kidney disease and its complications. Prim. Care 35, 329–344 (2008).
32.
Van Craenenbroeck AH, Van Craenenbroeck EM, Van Ackeren K et al. Impaired vascular function contributes to exercise intolerance in chronic kidney disease. Nephrol. Dial. Transplant. 31, 2064–2072 (2016).
33.
Sarnak MJ, Levey AS, Schoolwerth AC et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Circulation 108, 2154–2169 (2003).
34.
Angermayr L, Melchart D, Linde K. Multifactorial lifestyle interventions in the primary and secondary prevention of cardiovascular disease and Type 2 diabetes mellitus–a systematic review of randomized controlled trials. Ann. Behav. Med. 40, 49–64 (2010).
35.
Balducci S, Zanuso S, Nicolucci A et al. Effect of an intensive exercise intervention strategy on modifiable cardiovascular risk factors in subjects with Type 2 diabetes mellitus: a randomized controlled trial: the Italian Diabetes and Exercise Study (IDES). Arch. Intern. Med. 170, 1794–1803 (2010).
36.
Heiwe S, Jacobson SH. Exercise training for adults with chronic kidney disease. Cochrane Database Syst. Rev. 2011(10), CD003236 (2011).
37.
Johansen KL, Painter P. Exercise in individuals with CKD. Am. J. Kidney Dis. 59, 126–134 (2012).
38.
Johansen KL. Exercise in the end-stage renal disease population. J. Am. Soc. Nephrol. 18, 1845–1854 (2007).
39.
Plaisance EP, Grandjean PW. PA and high-sensitivity C-reactive protein. Sports Med. 36, 443–458 (2006).
40.
Barbieri E, Agostini D, Polidori E et al. The pleiotropic effect of physical exercise on mitochondrial dynamics in aging skeletal muscle. Oxid. Med. Cell. Longev. 2015, 917085 (2015).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 25 December 2025
Accepted: 14 May 2026
Published online: 16 June 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Association of physical activity levels and estimated glomerular filtration rate with all-cause mortality: a 10-year cohort study. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0209
Export citation
Select the citation format you wish to export for this article or chapter.