Acthar Gel treatment in patients with rheumatoid arthritis, systemic lupus erythematosus, or dermatomyositis/polymyositis: analysis of physician-reported charts
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To examine the characteristics, treatment patterns, and physicians' assessments of outcomes for patients with rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), or dermatomyositis/polymyositis (DM/PM) who received Acthar Gel. Materials & methods: This survey-based medical chart review study asked rheumatologists who met specific inclusion criteria to abstract data from patient records covering the period from April 2022 to November 2024. Eligible patients were adults ≥18 years diagnosed with RA, SLE, or DM/PM, treated with Acthar Gel for ≤24 months. An online questionnaire screened and identified contributing physicians and collected anonymized patient data (baseline demographic, medical history, concomitant medications, Acthar Gel treatment history, and physicians' assessment of health status, symptom severity, treatment outcomes with Acthar Gel). Results: The study population comprised 73 patients with RA (average age 50 years; 49 [67%] female; 44 [60%] White/non-Hispanic), 56 with SLE (average age 42 years; 47 [84%] female; 28 [50%] African–American), and 104 with DM/PM (average age 52 years; 69 [66%] female; 62 [60%] White/non-Hispanic). Patients had received Acthar Gel for an average of 9 (RA) or 8 months (SLE, DM/PM), with most receiving treatment at the time of the study. Per physicians' assessment, health status improved in 68 (93%) patients with RA, 50 (89%) patients with SLE, and 100 (96%) patients with DM/PM after starting treatment with Acthar Gel. The most common treatment goals achieved in patients with improved overall health status were improved overall symptoms, pain, physical function, and corticosteroid use in the RA cohort; overall symptoms, pain, corticosteroid use, and fatigue in the SLE cohort; and overall symptoms, strength, physical function, and corticosteroid use in the DM/PM cohort. Conclusion: These findings support the use of Acthar Gel as a potential treatment option for appropriate patients with RA, SLE, or DM/PM.
Plain language summary: How rheumatologists use Acthar Gel to treat adults with rheumatoid arthritis, systemic lupus erythematosus or dermatomyositis/polymyositis
What is this article about?
Even when using medications such as steroids, people living with rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), or dermatomyositis/polymyositis (DM/PM) experience symptoms. Acthar Gel is a prescription medicine that can be used as another treatment option. We wanted to find out how doctors use Acthar Gel in their regular practice to treat adults with RA, SLE or DM/PM. We asked rheumatologists to provide basic information about patients treated with Acthar Gel in the last 2 years, such as age, sex, symptoms, and how long they were treated with Acthar Gel. We also asked these doctors to evaluate how their patients' overall health, symptoms. and use of steroids changed from before to after the treatment.
What were the results?
We studied data from 73 adults with RA, 56 with SLE, and 104 with DM/PM. These patients had been given Acthar Gel for about 8–9 months. Rheumatologists said that many patients had better overall health after being treated with Acthar Gel. They also said that many patients experienced fewer symptoms, less pain, less tiredness, and used fewer corticosteroids.
What do the results mean?
These results suggest that Acthar Gel may be a treatment option for some patients with RA, SLE or DM/PM.
Rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and dermatomyositis/polymyositis (DM/PM) are systemic autoimmune rheumatic diseases that severely impact patients' health, quality of life, and function. RA impacts over 1.6 million people in high-income North America, with a prevalence rate of 300.5 per 100,000 [1]. Pharmacologic treatment options for people with RA include nonsteroidal anti-inflammatory drugs (NSAIDs) and glucocorticoids for symptomatic treatment as well as disease-modifying antirheumatic drugs (DMARDs), which include conventional synthetic DMARDs (e.g., methotrexate, leflunomide, hydroxychloroquine, sulfasalazine), targeted synthetic DMARDs (e.g., baricitinib, tofacitinib, upadacitinib), and biologic DMARDs (e.g., adalimumab, etanercept, infliximab, rituximab) [2–4].
SLE has an overall prevalence of 72.8 per 100,000 person-years, impacting over 200,000 people in the USA [5]. Medications commonly used to treat people with SLE include glucocorticoids, hydroxychloroquine, and NSAIDs, along with immunosuppressive agents (e.g., azathioprine, methotrexate, mycophenolate mofetil) and biologic therapies (e.g., anifrolumab, belimumab, rituximab), depending on disease severity, organ involvement, and response to prior therapy. Additional therapies such as cyclophosphamide and voclosporin are used particularly in patients with organ-threatening manifestations, including lupus nephritis [6,7]. Many of these therapies are associated with important safety considerations, including risks of serious infections, malignancy and organ toxicity; several agents (e.g., rituximab, cyclophosphamide, mycophenolate mofetil, and voclosporin) carry boxed warnings, which may limit their use in certain populations.
DM/PM is rarer than RA and SLE, with prevalence estimates ranging from 1 to 13 per 100,000 in the USA [8,9]. Medications for patients with DM/PM include glucocorticoids, immunosuppressants (e.g., methotrexate, azathioprine, mycophenolate mofetil), oral cyclosporine, intravenous immunoglobulin G, rituximab, and cyclophosphamide, particularly in patients with refractory or severe disease [8]. Because of the complex biology, clinical heterogeneity and variation across disease subtypes, treatment responses may differ among patients. Despite the availability of numerous treatments, patients with RA, SLE or DM/PM can experience breakthrough symptoms during acute episodes and exacerbations. Therapeutic advances are needed to develop therapies with improved effectiveness and fewer side effects.
Acthar® Gel (repository corticotropin injection; Keenova Therapeutics, formerly Mallinckrodt Pharmaceuticals) – a naturally sourced complex mixture of adrenocorticotropic hormone (ACTH) analogs and other pituitary peptides – has anti-inflammatory and immunomodulatory properties [10–13]. Acthar Gel is approved in the USA for 19 indications, including as adjunctive therapy for short-term administration in patients with RA during an acute episode or exacerbation, and for selected patients with SLE or DM/PM during an exacerbation or as maintenance therapy [10]. Thus, Acthar Gel is often used in patients with RA, SLE, or DM/PM after other therapies have failed. Small clinical trials and retrospective case series have found that Acthar Gel may reduce disease activity and improve signs/symptoms and functional status in patients with RA [14–18], SLE [19–25], and DM/PM [26–31]. Claims database studies have reported reduced medical resource utilization with Acthar Gel treatment in patients with RA, SLE, or DM/PM [32–34]. Another claims database study found reduced use of corticosteroids and biologics in the 6 months before versus after therapy with Acthar Gel in patients with various rheumatologic conditions [35]. In a study of deidentified medical records, physicians reported improved outcomes after Acthar Gel treatment initiation in patients with RA, SLE, or DM/PM [36].
Building on earlier research by Ho-Mahler and colleagues [36], which provided initial insights into the real-world use of Acthar Gel in rheumatologic conditions, we conducted a follow-up study with a larger, more contemporary patient sample. This study reflects current clinical practice patterns and treatment contexts, including recent advances in disease management and evolving use of immunomodulatory therapies. Additional and current real-world data from larger patient samples can provide valuable insights to inform clinical decision-making for physicians managing patients with RA, SLE, or DM/PM. In this physician-reported survey-based medical chart review study, we characterized patients with rheumatologic conditions recently treated with Acthar Gel and evaluated medication utilization patterns and physicians' assessments of its effects on health status. Here we report findings from this expanded dataset across RA, SLE, or DM/PM cohorts.
Materials & methods
Study design
This physician-reported survey-based medical chart review study had a predefined protocol and statistical analysis plan. The study sponsor and participating physicians were blinded to each other’s identities. Data abstraction was performed by physicians or their designated staff with authorized access to medical records as part of routine clinical care, and all data were deidentified prior to transfer; no identifiable patient or physician information was collected or shared, in accordance with applicable US privacy regulations, including the Health Insurance Portability and Accountability Act (HIPAA).The survey was developed via a collaboration between Indegene and Keenova Therapeutics, formerly Mallinckrodt Pharmaceuticals, and conducted in November 2024. Physicians were asked to abstract data from patient records covering the period from 1 April 2022 to 30 November 2024. For the RA study cohort, 52 rheumatologists reported data from 73 patient charts. For the SLE study cohort, 41 rheumatologists reported data from 56 patient charts. For the DM/PM study cohort, 64 rheumatologists reported data from 104 patient charts.
This study used preexisting fully deidentified data, with no direct involvement of human subjects or access to identifiable private information. Based on the authors' determination and in accordance with the US Department of Health and Human Services (45 CFR 46.102) and US FDA (21 CFR 56.102) regulations, this work does not meet the definition of human subject research. Therefore, approval from an institutional review board or ethics committee was not required. Physicians contributed data in an anonymized manner, and no identifiable information about patients or participating physicians was collected.
Study population
Study-eligible patients were adults ≥18 years diagnosed with RA, SLE, or DM/PM who had been treated with Acthar Gel in the previous 24 months and who had completely accessible medical records. Patients were excluded if they had any of the following contraindications: adrenocortical hyperfunction, congestive heart failure, ocular herpes simplex, osteoporosis, peptic ulcers, primary adrenocortical insufficiency, scleroderma, systemic fungal infections, and uncontrolled hypertension.
Data collection
A web-based questionnaire was used to screen physicians, identify potential physician contributors for this analysis, and collect anonymized patient data from the contributors who elected to participate in this study. The screening portion of the questionnaire collected data on physician demographics and practice patterns related to Acthar Gel prescribing, including patient volume and number of prescriptions across different rheumatological conditions (RA, SLE, DM/PM).
To participate in the study, physicians had to meet the following criteria: rheumatology as primary specialty; board eligible or board-certified in rheumatology; post residency or fellowship professional practice in the USA for 2 to 45 years; ≥50% of professional time spent in direct patient care seeing, treating, and/or managing patients; treated patients with rheumatological conditions with Acthar Gel in the previous 2 years; and willing to contribute data from the medical charts of 2–7 patients treated with Acthar Gel during this period.
Eligible physicians or their designated staff extracted information from the medical records of eligible patients and recorded it onto a secure online survey system via a standardized, protocol-driven, four-domain (demographics, clinical measures, pre- vs post-Acthar Gel health status and treatment outcomes) patient summary template. To ensure consistency and comparability, the template had predefined formats and definitions. The survey was pretested to ensure clarity, completeness, and consistency of data capture, consistent with established approaches used in real-world physician-reported chart review studies [36–39]. Physicians received detailed instructions for chart abstraction, eligibility criteria, and systematic patient selection to minimize bias. Participating physicians and their designated staff were blinded to study end points. Data received from participating physicians were validated for accuracy and completeness
Study variables
Collected patient baseline demographic data included age, BMI, gender, and race. Patient baseline clinical data included comorbidities and pre-Acthar Gel initiation symptomatology and health status. Patient treatment-related information included concomitant medications before initiation of Acthar Gel; time since diagnosis to initiation of Acthar Gel; Acthar Gel treatment status (currently being treated; treated in past 12 months, now stopped; treated in past 24 months, now stopped); and Acthar Gel treatment dosage, duration, and dose changes.
Via the survey template, participating physicians were asked to assess each patient's health status (i.e., excellent, very good, good, fair, poor), symptoms (e.g., fatigue, joint pain, muscle aches, stiffness) and individual treatment outcomes before and after initiation of Acthar Gel treatment. A patient’s overall health status was measured using the following questions with response categories being ‘improved’ or ‘not improved’: For patients who had completed their treatment: “How was your patient’s overall health status at the end of Acthar Gel treatment?” For patients currently undergoing treatment: “How has your patient’s overall health status changed after initiation of Acthar Gel treatment?” A reduction in overall symptoms and achievement of treatment goals were measured using the following question: “Please select the treatment goals, if any, that have improved as a result of Acthar Gel therapy.”
Data analysis
We summarized patient demographic and outcomes data using descriptive statistics, mean and standard deviation for continuous variables, and count and percentage for categorical variables. Analyses were performed using IBM® SPSS Statistics version 23.0 (IBM Corporation, Armonk, NY, USA).
Results
Patient characteristics
We analyzed physician-reported data from the medical records of 73 patients with RA, 56 patients with SLE, and 104 patients with DM/PM who had been treated with Acthar Gel from April 2022 to November 2024. The 73 patients in the RA cohort had an average age of 50 years (range: 29–76), 49 (67%) were female, and 44 (60%) were White/non-Hispanic (Table 1). Stiffness (n = 68; 93%), pain (n = 65; 89%), and fatigue (n = 51;70%) were the most frequent symptoms in these patients before initiating Acthar Gel. Arthritis/osteoarthritis (n = 27; 37%), chronic joint disease (n = 23; 32%), and hypertension (n = 19; 26%) were the most common comorbidities in this cohort. The average time since diagnosis was 4.6 years. Before starting Acthar Gel, patients with RA had an average overall health status rating of 3.4 out of 5 where 1 is excellent health status and 5 is poor health status prior to Acthar Gel initiation, with nearly half having fair (n = 27; 37%) or poor (n = 7; 10%) health status.
| RA cohort (N = 73) | SLE cohort (N = 56) | DM/PM cohort (N = 104) | |
|---|---|---|---|
| Average age, years (range) | 50 (29–76) | 42 (24–67) | 52 (18–82) |
| Gender, n (%) | |||
| Female | 49 (67) | 47 (84) | 69 (66) |
| Male | 24 (33) | 9 (16) | 35 (34) |
| Race/ethnicity, n (%) | |||
| African–American | 6 (8) | 28 (50) | 18 (17) |
| American Indian/Alaska native | 0 | 0 | 2 (2) |
| Asian | 8 (11) | 1 (2) | 7 (7) |
| Hispanic/Latino | 13 (18) | 14 (25) | 12 (11) |
| Native Hawaiian or other Pacific Islander | 0 | 0 | 1 (1) |
| White/non-Hispanic | 44 (60) | 11 (20) | 62 (60) |
| Not known | 2 (3) | 2 (5) | 2 (2) |
| Average BMI, kg/m2 | 28.1 | 27.5 | 27.3 |
| Comorbidities, n (%) | |||
| Arthritis/osteoarthritis | 27 (37) | 17 (30) | 37 (36) |
| Chronic joint disease | 23 (32) | 19 (34) | 17 (16) |
| Hypertension | 19 (26) | 19 (34) | 41 (39) |
| Hyperlipidemia | 13 (18) | 19 (34) | 29 (28) |
| Inflammatory eye disorders | 1 (1) | 0 | 1 (1) |
| Diabetes | 9 (12) | 7 (13) | 10 (10) |
| Asthma | 9 (12) | 9 (16) | 14 (13) |
| Heart conditions | 3 (4) | 0 | 9 (9) |
| Mood disorder | 6 (8) | 10 (18) | 17 (16) |
| COPD | 1 (1) | 1 (2) | 6 (6) |
| Cancer | 0 | 1 (2) | 2 (2) |
| Gastrointestinal conditions | 8 (11) | 5 (9) | 8 (8) |
| Thyroid disease | 6 (8) | 8 (14) | 7 (7) |
| Other lung disease | 4 (5) | 0 | 9 (9) |
| Chronic kidney disease | 7 (10) | 7 (13) | 10 (10) |
| Other renal disease | 1 (1) | 3 (5) | 2 (2) |
| None of the above | 19 (26) | 6 (11) | 14 (13) |
| Average time since diagnosis, years | 4.6 | 4.8 | 3.2 |
| Overall health status before initiation of Acthar Gel | |||
| Average rating (1 = excellent to 5 = poor rating scale) | 3.4 | 3.6 | 3.3 |
| Rating, n (%) | |||
| Excellent | 4 (5) | 2 (3) | 4 (4) |
| Very good | 6 (8) | 6 (11) | 21 (20) |
| Good | 29 (40) | 13 (23) | 30 (29) |
| Fair | 27 (37) | 24 (43) | 41 (39) |
| Poor | 7 (10) | 11 (20) | 8 (8) |
BMI: Body mass index; DM/PM: Dermatomyositis/polymyositis; RA: Rheumatoid arthritis; SLE: Systemic lupus erythematosus.
The 56 patients in the SLE cohort had an average age of 42 years (range: 24–67), 47 (84%) were female and 28 (50%) were African–American (Table 1). Joint pain (n = 47; 84%), rashes (n = 38; 68%), and fatigue (n = 38; 68%) were the most frequent symptoms in patients with SLE before starting Acthar Gel. Chronic joint disease (n = 19; 34%), hypertension (n = 19; 34%), and hyperlipidemia (n = 19; 34%) were the most common comorbidities in this cohort. The average time since diagnosis was 4.8 years. Before starting Acthar Gel, patients with SLE had an average overall health status of 3.6, with more than half having fair (n = 24; 43%) or poor (n = 11; 20%) health status.
The 104 patients in the DM/PM cohort had an average age of 52 years (range 18–82), 69 (66%) were female and 62 (60%) were White/non-Hispanic (Table 1). Muscle weakness (n = 88; 85%), muscle inflammation (n = 86; 83%), and skin rash (n = 78; 75%) were the most frequent symptoms in patients with DM/PM before starting Acthar Gel. Hypertension (n = 41; 39%), arthritis/osteoarthritis (n = 37; 36%), and hyperlipidemia (n = 29; 28%) were the most common comorbidities in this cohort. The average time since diagnosis was 3.2 years. Before starting Acthar Gel, patients with DM/PM had an average overall health status of 3.3, with nearly half having fair (n = 41; 39%) or poor (n = 8; 8%) health status.
Treatment patterns
Most of the 73 patients with RA were previously treated with biologic DMARDs (n = 49; 67%), corticosteroids (n = 49; 67%), and/or immunosuppressive drugs (n = 37; 51%) (Figure 1). Most of the 56 patients with SLE were previously treated with corticosteroids (n = 36; 64%), antimalarial drugs (n = 36; 64%), immunosuppressive drugs (n = 32; 57%), and biologic DMARDs (n = 31; 55%). Most of the 104 patients with DM/PM were previously treated with corticosteroids (n = 80; 77%), immunosuppressive drugs (n = 75; 72%), and/or biologic DMARDs (n = 43; 41%).
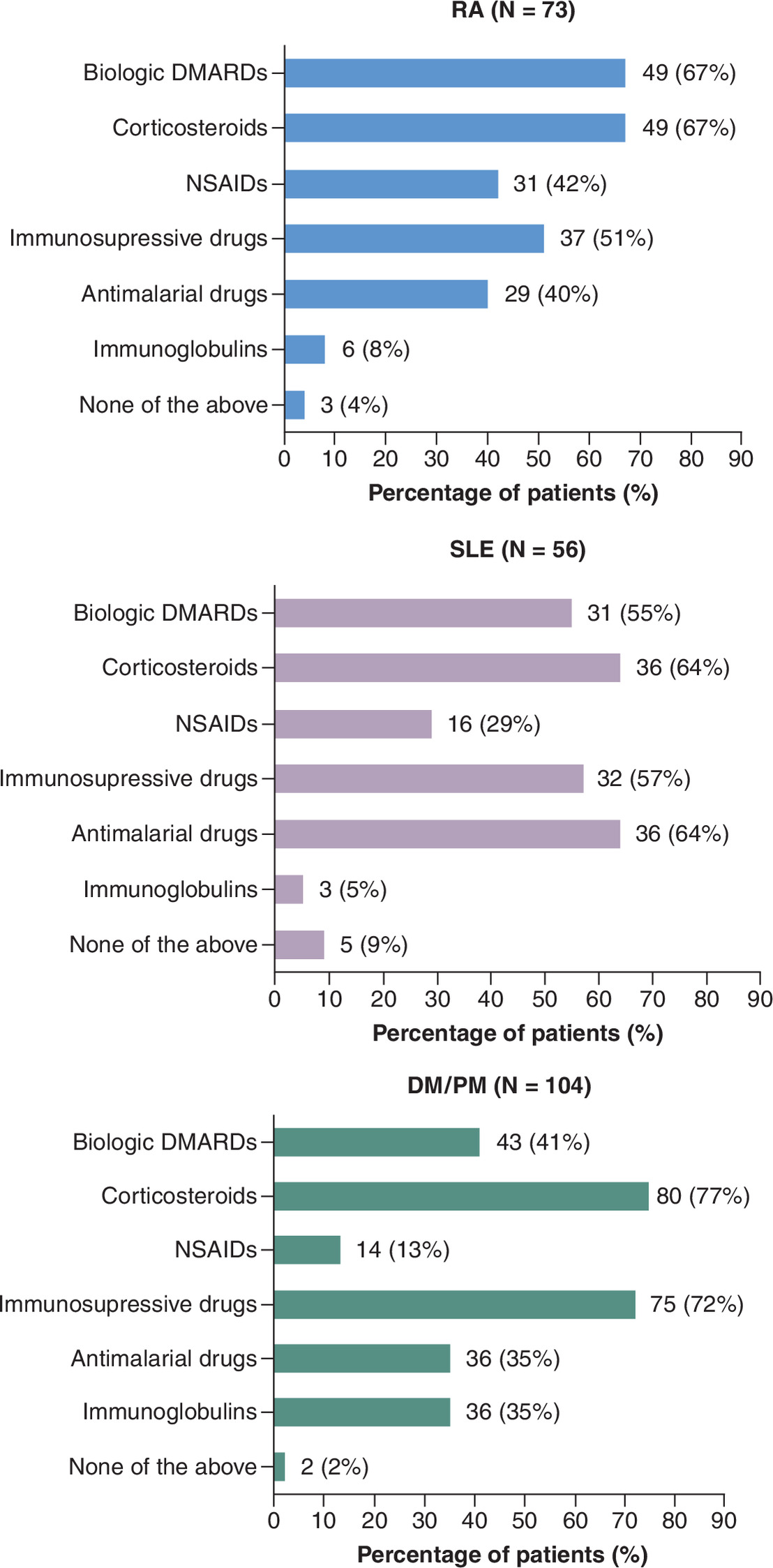
Figure 1. Medications received before initiating Acthar Gel in patients with rheumatoid arthritis, systemic lupus erythematosus, or dermatomyositis/polymyositis.
DMARD: Disease-modifying antirheumatic drug; DM/PM: Dermatomyositis/polymyositis; NSAID: Nonsteroidal anti-inflammatory drug; RA: Rheumatoid arthritis; SLE: Systemic lupus erythematosus.
‘None of the above’ category refers to other medications not listed above.
Patients with RA received Acthar Gel treatment for an average of 9 months and patients with SLE or DM/PM for an average of 8 months. Most patients with RA (n = 49; 67%), SLE (n = 30; 54%), or DM/PM (n = 52; 50%) were actively undergoing treatment with Acthar Gel at the time of the study (Figure 2). Acthar Gel was administered at a dosage of 40 or 80 units twice weekly to all 73 (100%) patients with RA, 51 (91%) of 56 patients with SLE, and 99 (95%) of 104 patients with DM/PM.
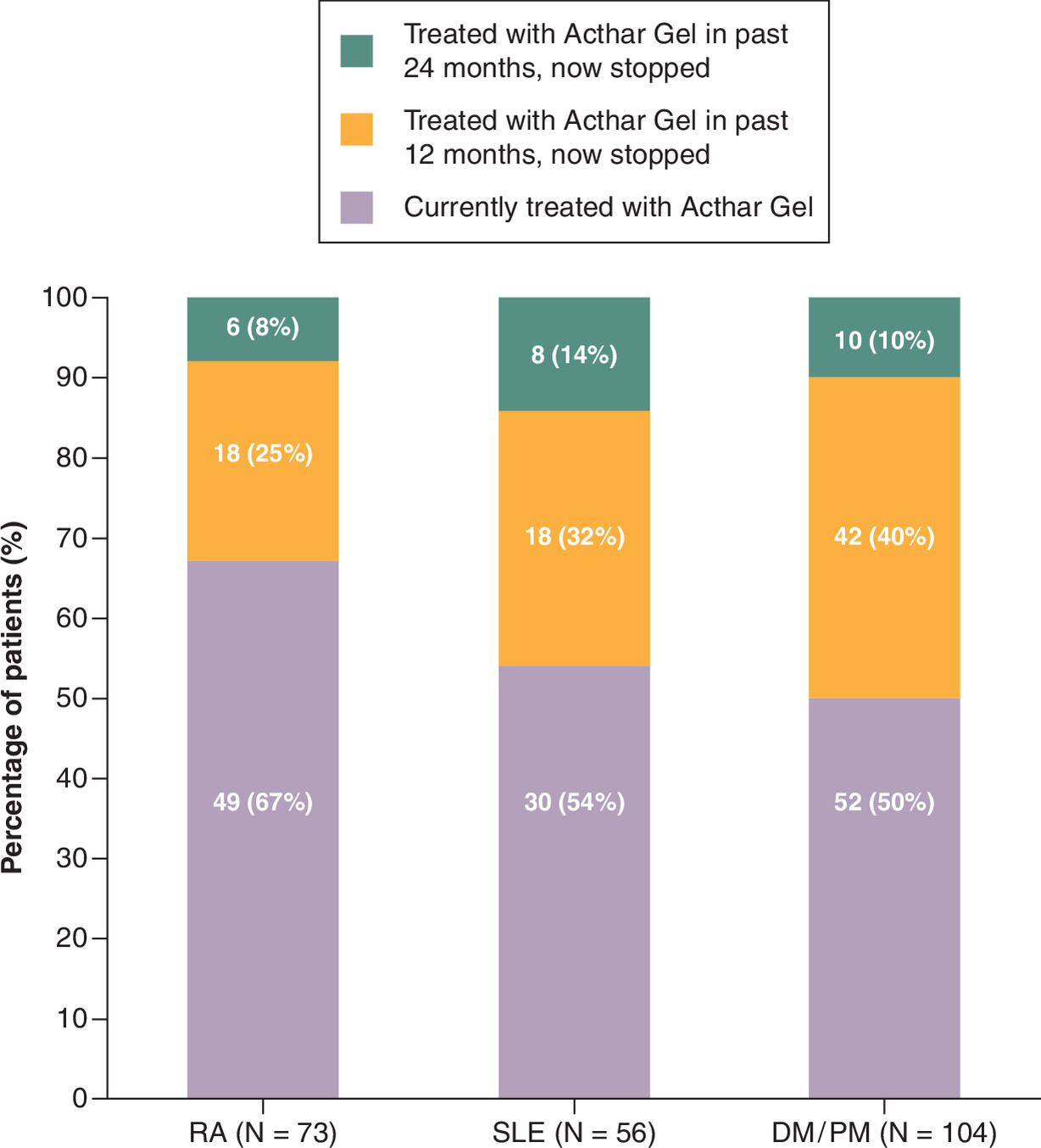
Figure 2. Acthar Gel treatment pattern in patients with rheumatoid arthritis, systemic lupus erythematosus, or dermatomyositis/polymyositis.
DM/PM: Dermatomyositis/polymyositis; RA: Rheumatoid arthritis; SLE: Systemic lupus erythematosus.
Physicians’ assessments of improvement
Physicians reported that the health status improved in 68 (93%) of 73 patients with RA, 50 (89%) of 56 patients with SLE, and 100 (96%) of 104 patients with DM/PM after starting treatment with Acthar Gel (Figure 3A). Treatment goals achieved among these 68 patients with RA included reduced overall symptoms (n = 48; 71%), decreased pain (n = 38; 56%), improved physical function (n = 32; 47%), reduced corticosteroid use (n = 24; 35%), and improved fatigue (n = 23; 34%) (Figure 3B). Improvements among the 50 patients with SLE included reduced overall symptoms (n = 41; 82%), decreased pain (n = 27; 54%), reduced corticosteroid use (n = 22; 44%), improved fatigue (n = 22; 44%), and improved physical function (n = 19; 38%). Improvements among the 100 patients with DM/PM included reduced overall symptoms (n = 65; 65%), improved strength (n = 60; 60%), improved physical function (n = 51; 51%), reduced corticosteroid use (n = 51; 51%), decreased pain (n = 31; 31%), and reduced biomarkers of disease (n = 31; 31%).
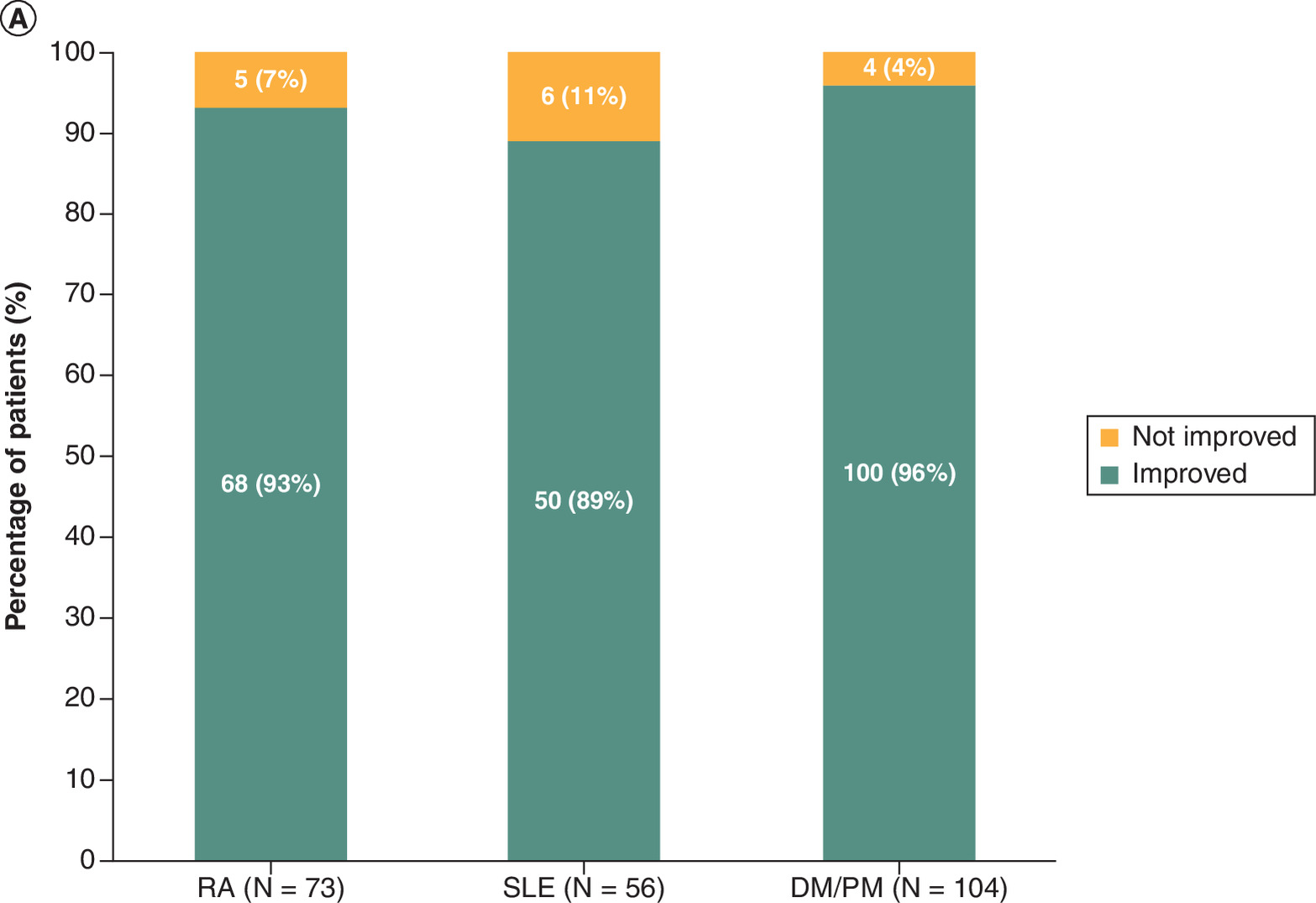
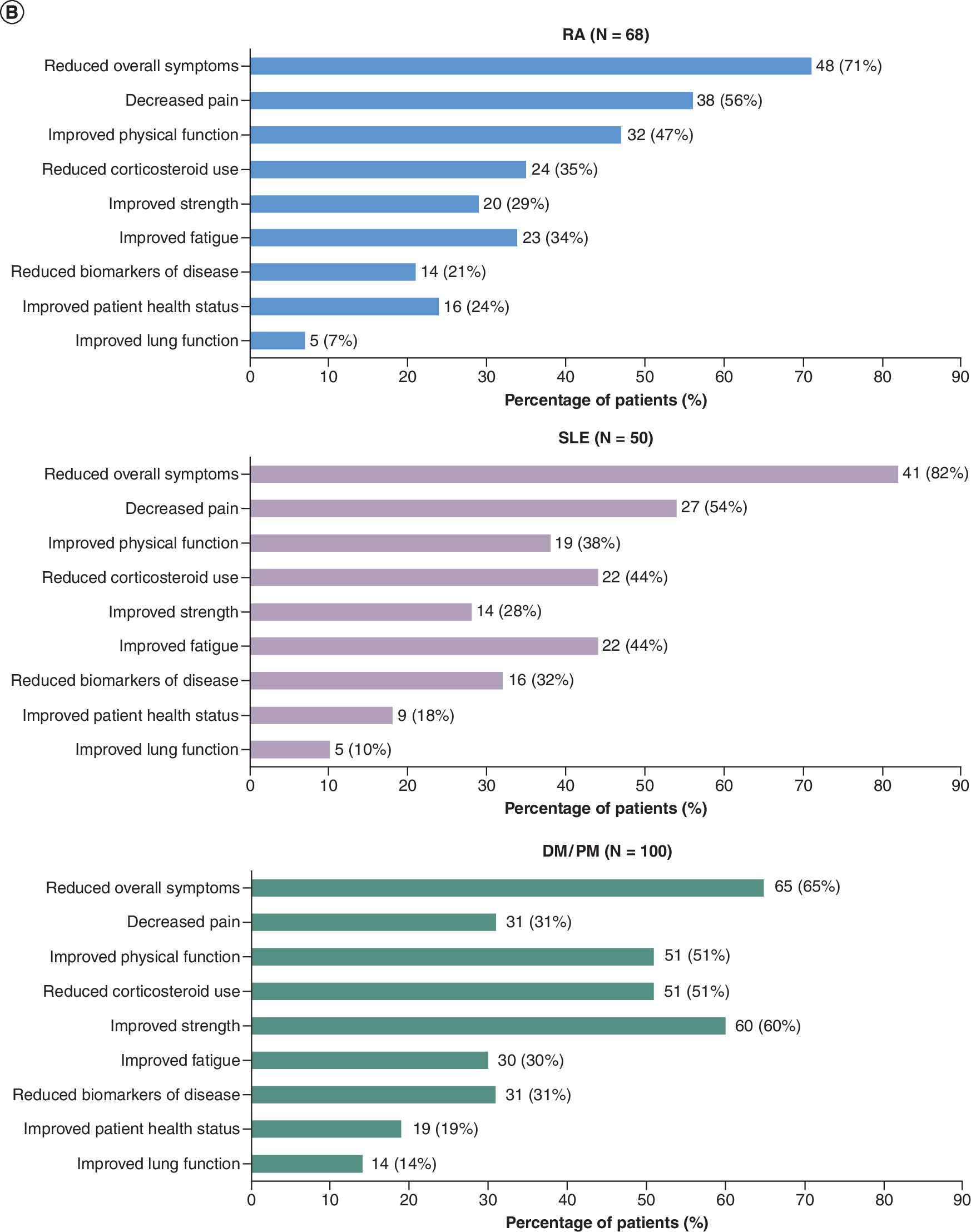
Figure 3. Changes in physicians' assessment of overall health status and achievement of treatment goals after initiation of Acthar Gel therapy.
(A) Physicians' assessment of patients' overall health status following Acthar Gel therapy. Physician’s assessment of the patient's health status was evaluated using the following questions: “How was your patient's overall health status at the end of Acthar Gel treatment?” for patients who had completed their treatment with Acthar Gel; “How has your patient's overall health status changed after initiation of Acthar Gel treatment (report either health status at the end of Acthar Gel therapy or the status at 6 months point for patients’ ongoing Acthar Gel treatment)?” for patients currently treated with Acthar Gel. (B) Achievement of treatment goals following initiation of Acthar Gel therapy. For patients with improved health status, improvements in overall symptoms and individual treatment outcomes were assessed using the following question: “Please select the treatment goals, if any, that have improved as a result of Acthar Gel therapy”.
DM/PM: Dermatomyositis/polymyositis; RA: Rheumatoid arthritis; SLE: Systemic lupus erythematosus.
Discussion
This real-world physician-reported medical record survey study examined the characteristics, treatment patterns, and physicians' assessments of outcomes for patients with RA, SLE, or DM/PM treated with Acthar Gel. These patients had received Acthar Gel for an average of 8 or 9 months, and 67% of patients with RA, 54% with SLE, and 50% with DM/PM were continuing this treatment during the reporting period. Per physicians' assessment, 93% of patients with RA, 89% with SLE, and 96% with DM/PM had improved overall health status after Acthar Gel treatment. The most commonly achieved treatment goals among patients with improved overall health status after Acthar Gel treatment were reduced overall symptoms (71%), decreased pain (56%), improved physical function (47%), and reduced corticosteroid use (35%) in the RA cohort; reduced overall symptoms (82%), decreased pain (54%), reduced corticosteroid use (44%), and improved fatigue (44%) in the SLE cohort; and reduced overall symptoms (65%), improved strength (60%), improved physical function (51%), and reduced corticosteroid use (51%) in the DM/PM cohort. These results show that many patients with RM, SLE, or DM/PM had improvements in overall health status and reductions in some symptoms after starting Acthar Gel treatment.
Using medical record data from 2022 to 2024, the present study confirms and updates the results reported in a similarly designed study by Ho-Mahler et al. that reported on a smaller population of patients with RA, SLE, or DM/PM who started Acthar Gel treatment between 2011 and 2016 [36]. In that study, physicians’ impression of change was reported as ‘improved’ for 78% of assessed patients with RA, 95% with SLE, and 67% with DM/PM.
A limitation of the current study is that it relied on survey data derived from patient medical records that may contain inaccuracies or omissions. As a real-world chart review, no standardized disease activity instruments were applied, and disease status was abstracted as documented in routine clinical practice. Although validated measures such as DAS28, SLEDAI, and other disease-specific indices are commonly used in clinical trials, their availability in real-world medical records is often limited. Prior electronic medical record studies have reported that such measures are captured in only a minority of patient records (~20%) [40,41]. As a result, physician-reported assessments were used to reflect routine clinical evaluation. The variability in physician documentation and subjective assessments of patient improvements may have introduced bias, especially given the lack of standardized objective measures of disease activity for patients with these conditions.
Future prospective studies incorporating standardized, validated disease-activity measures are warranted to more rigorously assess treatment outcomes. Because the study did not collect information on long-term Acthar Gel treatment outcomes, concomitant medications, and safety, it cannot provide information on the impact of long-term Acthar Gel treatment or its safety. Given the absence of control groups, the study also cannot provide information on comparative effectiveness. The study population, restricted to patients treated with Acthar Gel and with sufficient available data in the reviewed patient records, may prevent the generalizability of our findings to broader populations of patients with RE, SLE, or DM/PM such as patients in other healthcare settings or with varying disease severity. Practice setting-level differences (e.g., academic vs community) were not evaluated and may influence treatment patterns.
In conclusion, our findings suggest that Acthar Gel may be a potential treatment option for appropriate patients with RE, SLE, or DM/PM. After treatment with Acthar Gel, physicians reported that patients had reduced overall symptoms, decreased pain, improved fatigue, and reduced corticosteroid use. Given limited long-term safety and outcome data, further prospective studies are warranted. These findings may help inform clinical decision-making and guide future research.
Summary points
•
Despite treatment, patients with rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), or dermatomyositis/polymyositis (DM/PM) can experience breakthrough symptoms during acute episodes and exacerbations.
•
Acthar Gel (repository corticotropin injection) is approved in the USA for short-term adjunctive therapy in patients with RA during an acute episode or exacerbation and for selected patients with SLE or DM/PM during an exacerbation or as maintenance therapy.
•
This physician-reported survey-based medical chart review study characterized adults (age ≥18 years) with RA, SLE, or DM/PM recently treated with Acthar Gel in the previous 24 months and analyzed their medication utilization patterns and physicians' assessments of the effects of Acthar Gel on their health status.
•
The study population comprised 73 patients with RA, 56 with SLE, and 104 with DM/PM treated with Acthar Gel for an average of 9 (RA) or 8 months (SLE, DM/PM); most patients were receiving treatment at the time of the study.
•
Acthar Gel was administered at a dosage of 40 or 80 units twice weekly to 73 (100%) patients with RA, 51 (91%) patients with SLE, and 99 (95%) patients with DM/PM.
•
Per physicians’ assessment, health status improved in 68 (93%) patients with RA, 50 (89%) patients with SLE, and 100 (96%) patients with DM/PM after starting treatment with Acthar Gel.
•
The most common treatment goals achieved in patients who had improved overall health status were improved overall symptoms (n = 48; 71%), pain (n = 38; 56%), physical function (n = 32; 47%), corticosteroid use (n = 24; 35%) and fatigue (n = 23; 34%) in 68 patients with RA; overall symptoms (n = 41; 82%), pain (n = 27; 54%), corticosteroid use (n = 22; 44%), fatigue (n = 22; 44%), and physical function (n = 19; 38%) in 50 patients with SLE (n = 50); and overall symptoms (n = 65; 65%), strength (n = 60; 60%), physical function (n = 51; 51%), corticosteroid use (n = 51; 51%), pain (n = 31; 31%), and biomarkers of disease (n = 31; 31%) in 100 patients with DM/PM.
•
These findings support the use of Acthar Gel as a potential treatment option for appropriate patients with RE, SLE, or DM/PM.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Financial disclosure
This study was sponsored by Keenova Therapeutics, formerly Mallinckrodt Pharmaceuticals (NJ, USA).
Competing interests disclosure
K Hayes, J Purcell and GJ Wan are employees of Keenova Therapeutics, formerly Mallinckrodt Pharmaceuticals. MP Panaccio is a paid independent consultant for Keenova Therapeutics, formerly Mallinckrodt Pharmaceuticals. A Patel, PP Shanbhag and DR Evans are employees of Indegene Inc., Princeton, NJ, USA, and are paid consultants for Keenova Therapeutics, formerly Mallinckrodt Pharmaceuticals. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Monica Nicosia, PhD, and Esther Tazartes, MS, of the Global Outcomes Group provided medical writing and editorial assistance, which was funded by Keenova Therapeutics, formerly Mallinckrodt Pharmaceuticals.
Ethical conduct of research
This study used preexisting, fully deidentified data, with no direct involvement of human subjects or access to identifiable private information. Based on the authors' determination and in accordance with the US Department of Health and Human Services (45 CFR 46.102) and FDA (21 CFR 56.102) regulations, this work does not meet the definition of human subjects research. Therefore, approval from an institutional review board or ethics committee was not required. This study complies with the Declaration of Helsinki.
Data sharing statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Data transparency statement
The authors certify that this manuscript reports the original results of a real-world evidence study. A prespecified study protocol and statistical analysis plan were prespecified prior to data abstraction/analysis. The protocol is not publicly posted; it is available from the corresponding author/sponsor upon reasonable request (with any confidential/proprietary information redacted as needed). This was a retrospective, non-interventional chart review and was not preregistered. The dataset contains patient-level information and is not publicly available due to privacy/ethical and data-use/contractual restrictions. Aggregate results supporting the findings are reported in the manuscript. Additional aggregated outputs may be available from the sponsor/corresponding author upon reasonable request and subject to approval and a data-sharing agreement. Analyses were conducted using the statistical software described in the Methods. Study-specific programming code is not publicly available. Code may be shared upon reasonable request where feasible, subject to internal review and any contractual/confidentiality restrictions.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
GBD_Rheumatoid_Collaborators. Global, regional, and national burden of rheumatoid arthritis, 1990–2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 5(10), 3594–3610 (2023).
• This systematic analysis provides global, regional, and national estimates and future projections of the prevalence of rheumatoid arthritis and its associated health burdens, showing that while mortality has decreased over the past three decades, age-standardized prevalence has increased.
2.
Radu AF, Bungau SG. Management of rheumatoid arthritis: an overview. Cells 10(11), 2857 (2021).
3.
Smolen JS, Landewé RBM, Bergstra SA et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann. Rheum. Dis. 82(1), 3–18 (2023).
4.
Smolen JS, Landewé RBM, Bijlsma JWJ et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 79(6), 85–99 (2020).
5.
Izmirly PM, Parton H, Wang L et al. Prevalence of systemic lupus erythematosus in the United States: estimates from a meta-analysis of the Centers for Disease Control and Prevention National Lupus Registries. Arthritis Rheumatol. 73(6), 991–996 (2021).
• This meta-analysis of US systemic lupus erythematosus (SLE) registries provides estimates of the prevalence of SLE in the USA.
6.
Lam NV, Brown JA, Sharma R. Systemic lupus erythematosus: diagnosis and treatment. Am. Fam. Physician 107(4), 383–395 (2023).
7.
Lazar S, Kahlenberg JM. Systemic lupus erythematosus: new diagnostic and therapeutic approaches. Annu. Rev. Med. 74, 339–352 (2023).
8.
Schmidt J. Current classification and management of inflammatory myopathies. J. Neuromuscul. Dis. 5(2), 109–129 (2018).
9.
Kronzer VL, Kimbrough BA, Crowson CS, Davis JM 3rd, Holmqvist M, Ernste FC. Incidence, prevalence, and mortality of dermatomyositis: a population-based cohort study. Arthritis Care Res. 75(2), 348–355 (2023).
• This retrospective cohort study used electronic health records data from Olmsted County (MN, USA) to estimate the incidence and prevalence of dermatomyositis.
10.
Acthar Gel (repository cortiotropin injection). Prescribing information. Mallinckrodt, NJ, USA (2024).
11.
Ross AP, Ben-Zacharia A, Harris C, Smrtka J. Multiple sclerosis, relapses, and the mechanism of action of adrenocorticotropic hormone. Front. Neurol. 4, 21 (2013).
12.
Montero-Melendez T. ACTH: the forgotten therapy. Semin. Immunol. 27(3), 216–226 (2015).
13.
Mirsaeidi M, Baughman RP. Repository corticotropin injection for the treatment of pulmonary sarcoidosis: a narrative review. Pulm. Ther. 8(1), 43–55 (2022).
14.
Fleischmann R, Furst DE, Connolly-Strong E, Liu J, Zhu J, Brasington R. Repository corticotropin injection for active rheumatoid arthritis despite aggressive treatment: a randomized controlled withdrawal trial. Rheumatol. Ther. 7(2), 327–344 (2020).
15.
Fleischmann R, Hayes K, Ahn SW et al. Post hoc analysis of predictors of clinical response to repository corticotropin injection in persistently active rheumatoid arthritis. Rheumatol. Ther. 9(2), 649–661 (2022).
16.
Fleischmann R, Hayes K, Ahn SW et al. Post hoc analysis of the correlation between patient-reported outcomes and clinical response to repository corticotropin injection for persistently active rheumatoid arthritis. Rheumatol. Ther. 9(2), 435–446 (2022).
17.
Gillis T, Crane M, Hinkle C, Wei N. Repository corticotropin injection as adjunctive therapy in patients with rheumatoid arthritis who have failed previous therapies with at least three different modes of action. Open Access Rheumatol. 9, 131–138 (2017).
18.
Gaylis N, Needell S, Sagliani J. The effect of corticotropin (ACTH 80 units weekly or biweekly) in combination with MTX in newly diagnosed RA patients from a clinical and structural perspective as measured by a CDAI score and osteitis, synovitis, and erosions on MRI. Ann. Rheum. Dis. 74, 1066 (2015).
19.
Fiechtner JJ, Montroy T. Treatment of moderately to severely active systemic lupus erythematosus with adrenocorticotropic hormone: a single-site, open-label trial. Lupus 23(9), 905–912 (2014).
20.
Askanase AD, Wan GJ, Panaccio MP et al. Patient-reported outcomes from a Phase 4, multicenter, randomized, double-blind, placebo-controlled trial of repository corticotropin injection (Acthar(®) Gel) for persistently active systemic lupus erythematosus. Rheumatol. Ther. 8(1), 573–584 (2021).
21.
Askanase AD, Zhao E, Zhu J, Bilyk R, Furie RA. Repository corticotropin injection for persistently active systemic lupus erythematosus: results from a Phase 4, multicenter, randomized, double-blind, placebo-controlled trial. Rheumatol. Ther. 7(4), 893–908 (2020).
22.
Askanase AD, Zhao E, Zhu J, Bilyk R, Furie RA. Correction to: repository corticotropin injection for persistently active systemic lupus erythematosus: results from a Phase 4, multicenter, randomized, double-blind, placebo-controlled trial. Rheumatol. Ther. 8(4), 1915 (2021).
23.
Furie R, Mitrane M, Zhao E, Das M, Li D, Becker PM. Efficacy and tolerability of repository corticotropin injection in patients with persistently active SLE: results of a Phase 4, randomised, controlled pilot study. Lupus Sci. Med. 3(1), e000180 (2016).
24.
Furie RA, Mitrane M, Zhao E, Becker PM. Repository corticotropin injection in patients with persistently active SLE requiring corticosteroids: post hoc analysis of results from a two-part, 52-week pilot study. Lupus Sci. Med. 4(1), e000240 (2017).
25.
Li X, Golubovsky J, Hui-Yuen J et al. Adrenocorticotropic hormone gel in the treatment of systemic lupus erythematosus: a retrospective study of patients. F1000Res 4, 1103 (2015).
26.
Levine T. Treating refractory dermatomyositis or polymyositis with adrenocorticotropic hormone gel: a retrospective case series. Drug Des. Devel. Ther. 6, 133–139 (2012).
27.
Levine T, Malone J, Efthimiou P et al. H.P. Acthar® Gel in Dermatomyositis and Polymyositis Treatment Registry: An Interim Analysis. J. Neurol. Disord. 4(5), 292 (2016).
28.
Pender TM, Patel AM, Rosenkranz ME. Efficacy of repository-corticotropin injection (Acthar) in refractory juvenile dermatomyositis: a case series. J. Clin. Rheumatol. 27(Suppl. 8), S405 (2021).
29.
Fernandez AP, Gallop J, Polly S, Khanna U. Efficacy and safety of repository corticotropin injection for refractory cutaneous dermatomyositis: a prospective, open-label study. Rheumatology (Oxford, England) 63(12), 3370–3379 (2024).
30.
Aggarwal R, Marder G, Koontz DC, Nandkumar P, Qi Z, Oddis CV. Efficacy and safety of adrenocorticotropic hormone gel in refractory dermatomyositis and polymyositis. Ann. Rheum. Dis. 77(5), 720–727 (2018).
31.
Saygin D, Oddis CV, Marder G et al. Follow-up results of myositis patients treated with H. P. Acthar gel. Rheumatology (Oxford, England) 59(10), 2976–2981 (2020).
32.
Knight T, Bond TC, Popelar B et al. Medical resource utilization in dermatomyositis/polymyositis patients treated with repository corticotropin injection, intravenous immunoglobulin, and/or rituximab. Clinicoecon. Outcomes Res. 9, 271–279 (2017).
• This US administrative claims analysis compared medical resource utilization and associated costs of patients with dermatomyositis/polymyositis treated with Acthar Gel versus intravenous immunoglobulin (IVIg) and/or rituximab.
33.
Wu B, Deshpande G, Gu T, Popelar B, Philbin M, Wan GJ. Demographics, treatment patterns, and healthcare utilization and cost of repository corticotropin injection in patients with systemic lupus erythematosus or rheumatoid arthritis. J. Med. Econ. 20(11), 1170–1177 (2017).
• This US administrative claims analysis provides real-world clinical healthcare resource utilization and cost data for patients with rheumatoid arthritis or systemic lupus erythematosus before and after they initiated treatment with Acthar Gel.
34.
Nelson WW, Philbin MJ, Gallagher JR, Heap K, Carroll S, Wan GJ. A retrospective medical record review of utilization patterns and medical resource use associated with repository corticotropin injection among patients with rheumatologic diseases in the United States. Rheumatol. Ther. 4(2), 465–474 (2017).
•• This real-world US physician survey-based medical chart review examines patient characteristics, Acthar Gel treatment patterns and barriers to its use and compares medical resource use before and after Acthar Gel therapy in patients with rheumatoid arthritis, psoriatic arthritis, dermatomyositis/polymyositis or systemic lupus erythematosus.
35.
Myung G, Nelson WW, McMahon MA. Effects of repository corticotropin injection on medication use in patients with rheumatologic conditions: a claims data study. J. Pharm. Technol. 33(4), 151–155 (2017).
•• This US administrative claims analysis reports real-world data on Acthar Gel prescription patterns and use of other medications (biologics, NSAIDs, DMARDs, corticosteroids), before, during and after Acthar Gel treatment in patients with rheumatoid arthritis, systemic lupus erythematosus or dermatomyositis/polymyositis.
36.
Ho-Mahler N, Turner B, Eaddy M, Hanke ML, Nelson WW. Treatment with repository corticotropin injection in patients with rheumatoid arthritis, systemic lupus erythematosus, and dermatomyositis/polymyositis. Open Access Rheumatol. 12, 21–28 (2020).
•• This US physician survey-based medical chart review reports real-world data on patient characteristics, reasons for Acthar Gel initiation, prescription patterns, physician’s impression of efficacy and safety in patients with rheumatoid arthritis, systemic lupus erythematosus or dermatomyositis/polymyositis.
37.
Shiozawa A, Cloutier M, Heroux J, Guerin A, Wu EQ, Jackson R. Real-world treatment patterns of gout patients treated with colchicine or other common treatments for gout in acute care settings: a retrospective chart review study. Curr. Med. Res. Opin. 31, 1611–1620 (2025).
38.
Patel A, Shanbhag PP, Evans DR, Hayes K, Panaccio MP, Wan GJ. Treatment patterns and outcomes of Acthar Gel in ankylosing spondylitis and psoriatic arthritis: a physician-reported chart review. Open Access Rheumatol. 17, 193–202 (2025).
39.
Patel A, Shanbhag P, Evans DR et al. Symptomatic sarcoidosis treated with Acthar® Gel: insights from a physician-reported chart review. Pulm. Ther. 12, 385–395 (2026).
40.
Busch H, Wan GJ, Niewoehner J et al. Real-world treatment patterns for repository corticotropin injection in patients with rheumatoid arthritis. Drug Context 11, 2021-10-4 (2022).
41.
Hayes K, Panaccio MP, Houston P et al. Real-world treatment patterns and outcomes from an electronic medical records database for patients with rheumatoid arthritis treated with repository corticotropin injection. Open Access Rheumatol. 15, 315–323 (2021).
Information & Authors
Information
Published In
Copyright
© 2026 Keenova Therapeutics, formerly Mallinckrodt Pharmaceuticals. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 8 December 2025
Accepted: 22 May 2026
Published online: 25 June 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Acthar Gel treatment in patients with rheumatoid arthritis, systemic lupus erythematosus, or dermatomyositis/polymyositis: analysis of physician-reported charts. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0200
Export citation
Select the citation format you wish to export for this article or chapter.