Effectiveness and safety of therapies for patients with opioid use disorder: a systematic review and network meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Opioid use disorder (OUD) leads to significant morbidity and mortality. While opioid agonist therapies like transmucosal buprenorphine and methadone are effective, they face challenges such as poor adherence, diversion risk and suboptimal abstinence rates, prompting the development of long-acting injectable (LAI) buprenorphine. However, comparative evidence among LAIs and versus standard treatments remains limited. The aim of this study is to provide comparative evidence among buprenorphine LAIs and versus oral opioid agonist treatments. Materials & methods: We conducted a systematic literature review and network meta-analysis (NMA) evaluating the effectiveness and safety of LAI buprenorphine treatments (extended-release buprenorphine [BUP-XR; monthly injection] and other BUP-LAI [weekly and monthly injection]) versus transmucosal buprenorphine, methadone and buprenorphine implants in adults with OUD. The review included randomized controlled trials (RCTs) and non-RCTs for LAIs (January 2012 and March 2025). Primary outcomes were treatment discontinuation and illicit opioid use. Secondary outcomes were safety and health-related quality of life. Data were synthesized using univariate NMAs, bivariate NMA with surrogate end point modelling. Studies with limited data and single-arm designs were incorporated by using study-level matching techniques. Results: Ninety-eight studies met the inclusion criteria. BUP-XR demonstrated the highest probability of achieving treatment retention and opioid abstinence across analyses. In combined evidence (RCTs and non-RCTs), BUP-XR showed significantly lower risk of illicit opioid use versus transmucosal buprenorphine (rate ratio [RR] 1.99; 95% credible interval [CrI]: 1.29–3.11) and methadone (RR: 2.66; 95% CrI: 1.40–3.56). BUP-XR showed borderline significantly lower risk of illicit opioid use versus other BUP-LAI (RR: 1.81; 95% CrI: 0.97–3.55) and buprenorphine implant (RR: 2.28; 95% CrI: 0.98–5.38). Treatment discontinuation rates were similar between OUD treatments. Safety outcomes were generally comparable across treatments. Health-related quality of life indicated better recovery among patients treated with BUP-XR. Conclusion: BUP-XR may enhance treatment retention and abstinence over other OUD therapies, supporting its integration into clinical pathways. The results may help guide future updates to OUD treatment guidelines and policies aimed at optimizing the use of long-acting formulations. Additional research is needed to better define the comparative effectiveness of LAIs.
Plain language summary
What is this article about?
This article reviews and compares how well different treatments work for people with opioid use disorder. It focuses on buprenorphine long-acting injectables, a newer type of treatment designed to improve adherence and reduce misuse compared with daily opioid agonist therapies such as methadone and oral buprenorphine. The study combines evidence from both clinical trials and real-world studies using a systematic literature review and network meta-analysis.
What were the results?
The analysis included 98 studies. Monthly injectable buprenorphine (BUP-XR) showed the highest likelihood of helping people stay on treatment and avoid illicit opioid use compared with methadone, oral buprenorphine and other long-acting formulations. Safety was generally similar across all treatments, and people treated with monthly injections reported better quality of life during recovery.
Why is this important?
Opioid use disorder remains a major global health issue, and many people struggle to remain on daily treatments. These findings suggest that monthly injectable buprenorphine could offer a more effective and convenient option, improving long-term treatment outcomes and supporting recovery in real-world settings.
Opioid use disorder (OUD) is a chronic relapsing disorder characterized as a problematic pattern of opioid use leading to clinically significant psychological or functional impairment [1–4]. Severity is categorized as mild (2–3 symptoms), moderate (4–5 symptoms) and severe (≥6 symptoms) [1]. OUD is associated with serious risks, including overdose, infectious diseases, suicide and death in severe cases [5–8]. In 2022, an estimated 60 million people globally engaged in nonmedical opioid use, including the use of heroin, morphine, codeine, fentanyl, methadone and tramadol. OUD affects approximately 5.7 million people in the US in 2023 [9]. Of 600,000 drug-related deaths reported by the world health organization, approximately 450,000 opioid related underscoring the significant burden of OUD [10]. Approximately 55,529 opioid-related overdose deaths were reported in the US in 2023 [11].
Treatment aims to support retention and/or sustained abstinence [3,4]. Opioid maintenance therapy, using opioid agonist treatment (OAT) – e.g., buprenorphine or methadone – has emerged as the most effective approach [12]. Clinical guidelines such as the American Society of Addiction Medicine National Practice Guideline and the Canadian Research Initiative on Substance Misuse National Guideline for the Clinical Management of OUD recommend transmucosal buprenorphine/naloxone or oral methadone as the standard of care for treating OUD [3,4].
Current OUD treatment options may be limited by poor treatment outcomes, persistent cravings, withdrawal symptoms, illicit opioid use, overdose risk, poor retention rates, administration burden of daily dosing, and potential misuse, abuse and diversion of transmucosal, buccal and oral formulations [13–19]. Long-acting injectables (LAIs), such as monthly extended-release buprenorphine (BUP-XR; Sublocade®, Indivior), and weekly/monthly other buprenorphine LAI (other BUP-LAI; ‘Brixadi®, Braeburn’; ‘Buvidal; Camurus’) offer a promising solution. LAIs improve treatment adherence and retention, leading to higher abstinence rates and better health outcomes compared with standard treatment [20,21]. However, no comparative evidence on efficacy and safety between LAIs and oral OAT exists. We conducted a systematic literature review (SLR) and network meta-analysis (NMA) to assess the comparative efficacy and safety profile of LAI (BUP-XR and other BUP-LAI) and oral OAT (transmucosal [TM] buprenorphine, TM buprenorphine/naloxone, methadone) therapies.
Given that buprenorphine LAIs are relatively recent developments and randomized controlled trial (RCT) data remain limited, our study included both RCT and non-RCT evidence to ensure comprehensive coverage of the available evidence base. The value of non-RCTs with real-world evidence (RWE) in complementing RCTs has been increasingly recognized by regulatory bodies and health technology assessment (HTA) agencies [22–25]. By integrating RCT and non-RCT evidence, we aimed to generate a more robust and policy-relevant assessment of the clinical effectiveness and safety of buprenorphine LAIs.
Materials & methods
We conducted an SLR following the standards described in the Cochrane Handbook of Systematic Reviews of Interventions [26] and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines extension to NMA [27] and PRISMA harms checklist [28].
Search strategy & selection criteria
Two separate searches were conducted: one for buprenorphine LAIs and another for oral OATs. For the SLR on buprenorphine LAIs, we searched comprehensively for RCTs and non-RCTs including RWE. The searches were conducted in Embase and MEDLINE (including MEDLINE Epub ahead of print, in-process and nonindexed citations), and the Cochrane Central Register of Controlled Trials (CENTRAL) from 1 January 2012, to 31 March 2025, and included conference abstracts from 2021 onwards. Full search strategies are detailed in Supplementary Appendix 1.1–1.3.
For oral OATs, we reviewed and included relevant studies from two recent SLRs by Lim et al. [29], and Degenhardt et al. [30]. Lim et al. focused on collecting evidence for buprenorphine, methadone, naltrexone and morphine from database inception until February 2022, and included only RCTs [29]. Degenhardt et al. concentrated on gathering RCTs and non-RCTs comparing buprenorphine with methadone from database inception until August 2022 [30]. We updated these SLRs from February 2022 to March 2025 for Lim et al., and from August 2022 to March 2025 for Degenhardt et al. During the updates, a similar methodology was followed, and searches were conducted in Embase, MEDLINE and CENTRAL (see Supplementary Appendix 1.4–1.9).
Searches were restricted to English-language human studies, supplemented by manual reference checks from Cochrane and systematic reviews to ensure comprehensive coverage. Inclusion criteria, detailed in Supplementary Appendix 2, required studies to involve adults (≥18 years) with OUD or opioid dependence, excluding special populations like pregnant women. For buprenorphine LAIs, both RCTs and non-RCTs including comparative or single-arm RWE studies were included (Supplementary Appendix 2.1). For oral OATs, only RCTs comparing OATs with each other, placebo, or other controls (e.g., standard of care, or no treatment) were included (Supplementary Appendix 2.2).
Two investigators independently screened titles and abstracts, followed by full-text reviews to determine eligibility based on predefined criteria. Disagreements were resolved through consensus with a third investigator.
The study did not involve the enrolment of patients and did not collect individual patient-level data; thus, the protocol of the study was not registered on public registries considering it was not a mandatory requirement.
Data analysis
Data were extracted in Microsoft Excel, including publication details, study characteristics, participants’ baseline characteristics, efficacy and safety outcomes data.
Primary outcomes were treatment discontinuation (proportion of patients discontinuing the treatment by end of the study follow-up time) and illicit opioid use (mean percentage of positive urine drug screen per patient or overall proportion of positive urine drug screen throughout the study follow-up time with and without self-reporting). Missing samples for illicit opioid use were imputed as positive. We estimated rate ratios (RRs) with 95% credible intervals (CrIs), to account for varying follow-up. Secondary outcomes included safety (adverse events [AEs], treatment-emergent AEs [TEAEs]), and health-related quality of life (HRQoL) outcomes. We estimated odds ratios (ORs) for binary outcomes and mean differences (MDs) for continuous outcomes, with 95% CrIs. For all outcomes, we ranked the preference of treatment options by calculating the probability of each treatment being the best for each of the outcome of interest [31]. For all outcomes, both RCTs and non-RCTs were included if data were available. Estimates based on RCTs only were also calculated as a scenario analysis to assess the robustness of the results. All analyses followed NICE Technical Support Document guidance [32].
TM buprenorphine and TM buprenorphine/naloxone were grouped as a single node (TM buprenorphine) as they share the same active ingredient, route of administration, and comparable efficacy and safety. NMAs were performed using a random effects model to account for between-studies heterogeneity, and a fixed effect model was included as a sensitivity analysis within a Bayesian framework. Equal heterogeneity was assumed across comparisons, and correlations in multi-arm studies were accounted for [31]. Network consistency was assessed by comparing posterior mean residual deviance from the unrelated mean effects model and the NMA model, and the node-splitting approach [33]. The absolute model fit was determined by comparing the estimated total residual deviance with the number of data points used. Analyses were conducted using WinBUGS via the R package [34], R2WinBUGS, (R version 4.4.1, package version 2.1.22.1).
To expand the evidence base, we conducted exploratory analyses by including studies only reporting treatment discontinuation but not the illicit opioid use in the NMAs. This was achieved by first predicting the illicit opioid use for these studies using surrogate end point meta-analysis [35] based on studies reporting both treatment discontinuation and illicit opioid use. Single-arm BUP-XR studies were matched with similar treatment arms from other BUP-LAI studies, based on the reported study level covariates [36]. Methodological details are provided in Supplementary Appendix 6. The results of the surrogate end points meta-analysis are provided in Supplementary Appendix 7.
Study variability was quantified by estimating between-study standard deviation and assessed through sensitivity analysis, excluding studies from correctional settings and those with comorbid populations for primary outcomes. Meta-regression analyses were also planned to explain heterogeneity if feasible.
The version 2 of the Cochrane Risk of Bias (RoB 2) tool [37] was used for RCTs, which examines potential biases in five domains. Overall bias risk was determined by the highest risk in any domain, categorized as ‘low risk’, ‘some concerns’, or ‘high risk’. For non-RCTs, the Newcastle–Ottawa Scale [38] was used to assess quality, using a star system to evaluate selection, comparability and outcome reporting. A sensitivity analysis excluding the studies with high risk of bias was conducted to assess the impact of including such studies on the results. Funnel plot was planned to assess the risk of bias due to missing results (arising from reporting biases).
Results
The database searches yielded 4162 records for LAIs SLR and 5959 records for oral OATs SLR updates. Of these, 419 and 31 records, respectively, were identified as potentially eligible based on title and abstract screening and were obtained for full-text assessment. A total of 98 unique studies were finally included (LAIs, 50; oral OATs, 48), the list of which is provided in Supplementary Appendix 3.1. A PRISMA flow diagram showing the study selection process is presented in Figure 1. A PRISMA checklist can be found in Supplementary Appendix 12.
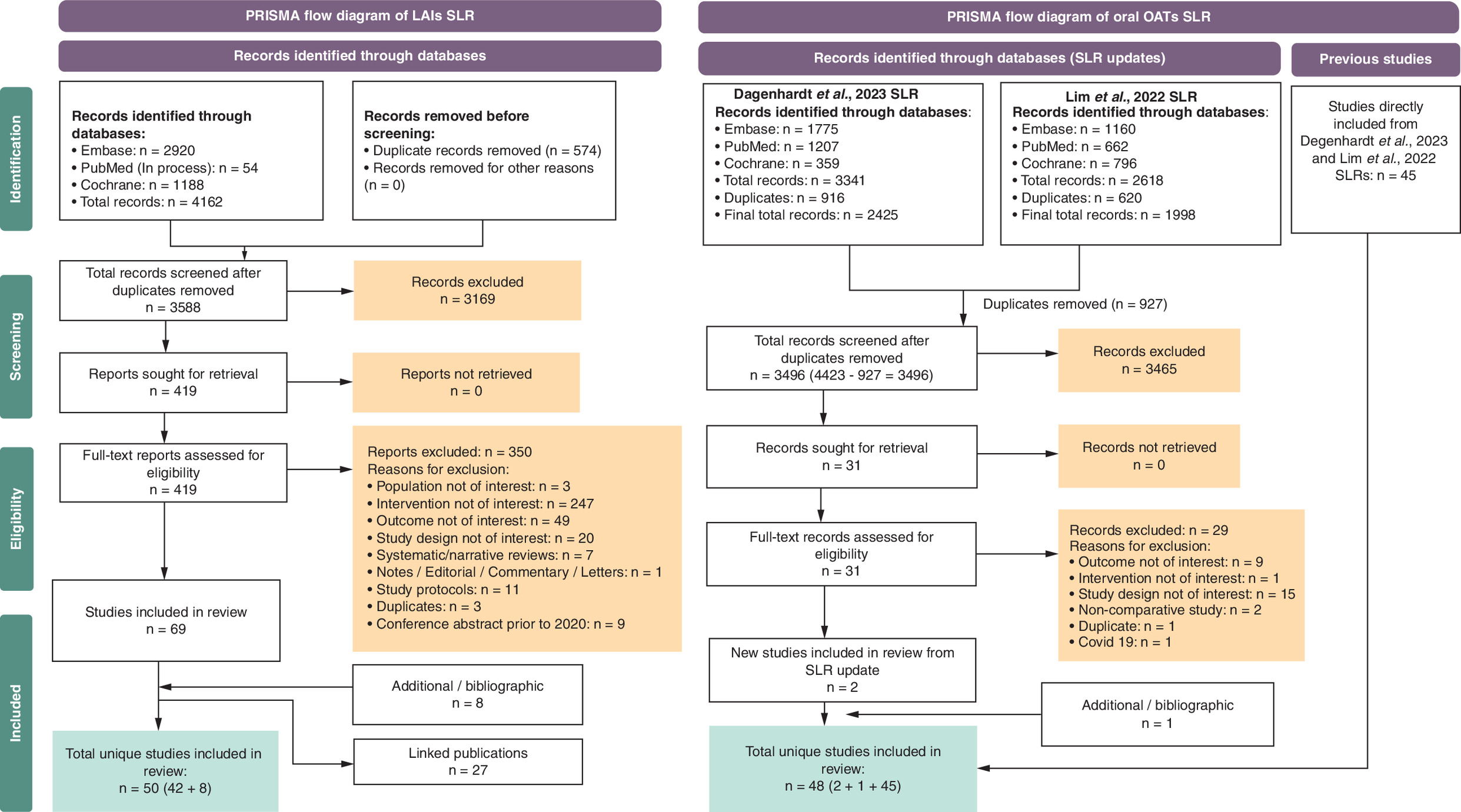
Figure 1. PRISMA flow diagram.
SLR: Systematic literature review.
Supplementary Appendix 4 shows baseline characteristics of included studies. Most studies were from the US and Canada (59%), followed by Europe (22%), Australia (11%) and Asia (9%). Sixty-four studies were comparative (RCTs and non-RCTs) and 34 single-arm. Most of the study designs included double-blind (n = 30) or open-label RCTs (n = 27). Of the 34 single-arm studies, 24 were of BUP-XR, nine of other BUP-LAI, and one of unclear LAI. Two studies were of buprenorphine implants (BUP-Implant). The most predominantly reported outcomes were retention (77 studies) and abstinence (49 studies), while others were reported invariably (Craving Visual Analogue Scale [n = 9], Clinical Opiate Withdrawal Scale [n = 9], Subjective Opiate Withdrawal Scale [n = 7]). Most of the patients in the included studies were male, with proportions ranging from 52 to 100%. The mean/median age of patients at enrolment varied between 25 and 50 years old. The baseline injection drug users differed 8–80% across studies.
In the analysis using RCTs and non-RCTs, the rate of treatment discontinuation did not differ significantly between OUD treatments, except for TM buprenorphine, which was associated with a borderline significantly higher rate of treatment discontinuation versus BUP-XR (RR: 1.44 [95% CrI: 0.99–2.11]) (Figure 2). In the analysis using RCTs only, there was no evidence of a difference between the OUD treatments. In both analyses, the treatment ranking suggests that both BUP-XR and methadone had the highest probability being the most effective treatment for treatment retention.
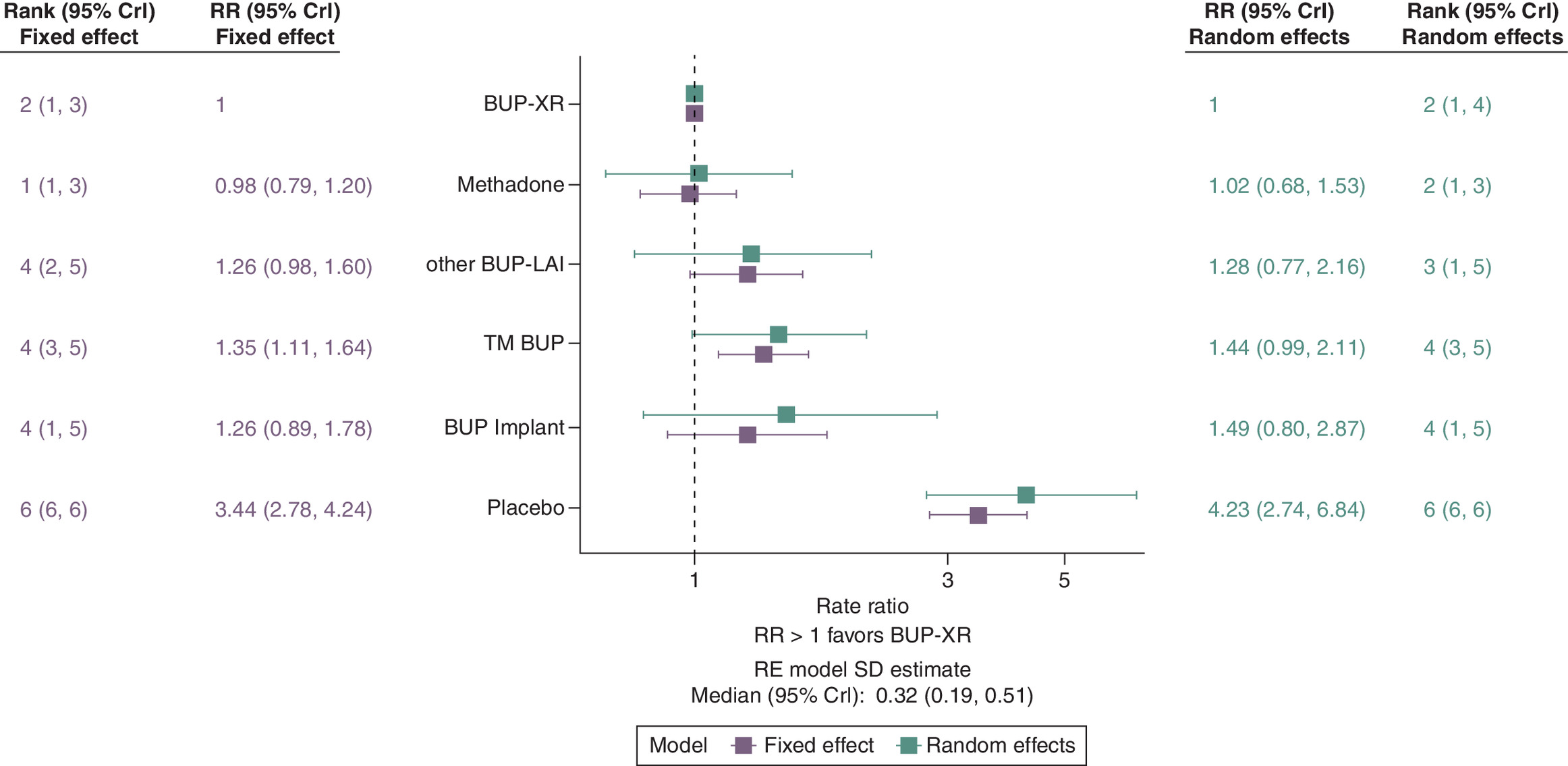
Figure 2. Forest plot showing the effectiveness of each treatment relative to extended-release buprenorphine in terms of treatment discontinuation based on a network meta-analysis of data from randomized controlled trials and nonrandomized controlled trials.
A risk ratio greater than 1 indicates individuals are more likely to discontinue treatment compared with BUP-XR.
BUP: Buprenorphine; BUP-XR: Extended-release buprenorphine; CrI: Credible interval; RR: Rate ratio; TM: Transmucosal.
BUP-XR had the highest probability of treatment retention at 3, 6, 12 and 18 months compared with other BUP-LAI, TM buprenorphine and buprenorphine implant, and similar probability versus methadone across both analyses including RCTs and non-RCTs, and RCTs only studies (Figure 3). The exploratory analysis including matched single-arm studies of LAIs showed similar results (Supplementary Appendix 8.2). The pairwise comparison results are presented in Supplementary Appendix 9.
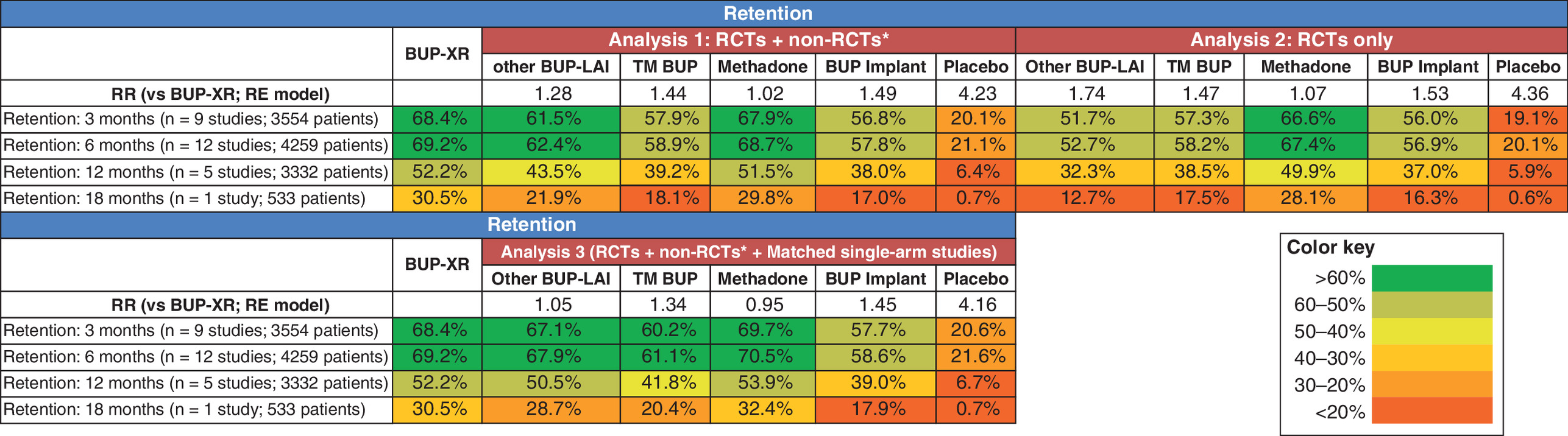
Figure 3. Percentage of study participants retained on each treatment included in the network meta-analysis at 3, 6, 12 and 18 months.
*The results for BUP-XR were obtained by averaging the reported percentages from each BUP-XR study at a fixed time point where data were available. The number in parenthesis indicates the number of studies and number of eligible patients included in calculating the percentage for BUP-XR.
BUP-XR: Sublocade®/SubutexPRO®; other BUP-LAI: Brixadi®/Buvidal®; BUP: Buprenorphine; RCT: Randomized controlled trial; TM BUP: Transmucosal buprenorphine.
Regarding abstinence, the analysis depicted in Figure 4, using RCTs and non-RCTs, showed that TM buprenorphine and methadone were associated with a significantly higher rate of illicit opioid use versus BUP-XR (RR: 1.99 [95% CrI: 1.29–3.11] and 2·26 [95% CrI: 1.40–3.56], respectively). Other BUP-LAI and buprenorphine implant were associated with a borderline significantly higher rate of opioid use against BUP-XR (RR: 1.81 [95% CrI: 0.97–3.55] and 2.28 [95% CrI: 0.98–5.38], respectively). This treatment ranking demonstrates that BUP-XR had the highest probability of being the most effective treatment for opioid abstinence. In the analysis using RCTs only, TM buprenorphine and buprenorphine implant were associated with a significantly higher rate of illicit opioid use versus BUP-XR (RR: 1.88 [95% CrI: 1.00–3.46] and 2·25 [95% CrI: 1.15–4.37], respectively); whereas, methadone was associated with a borderline significantly higher rate of opioid use against BUP-XR (RR: 1.89 [95% CrI: 0.97–3.61]) (see Supplementary Appendix 8.3). This treatment ranking demonstrates that BUP-XR had the highest probability being the most effective treatment for opioid abstinence.
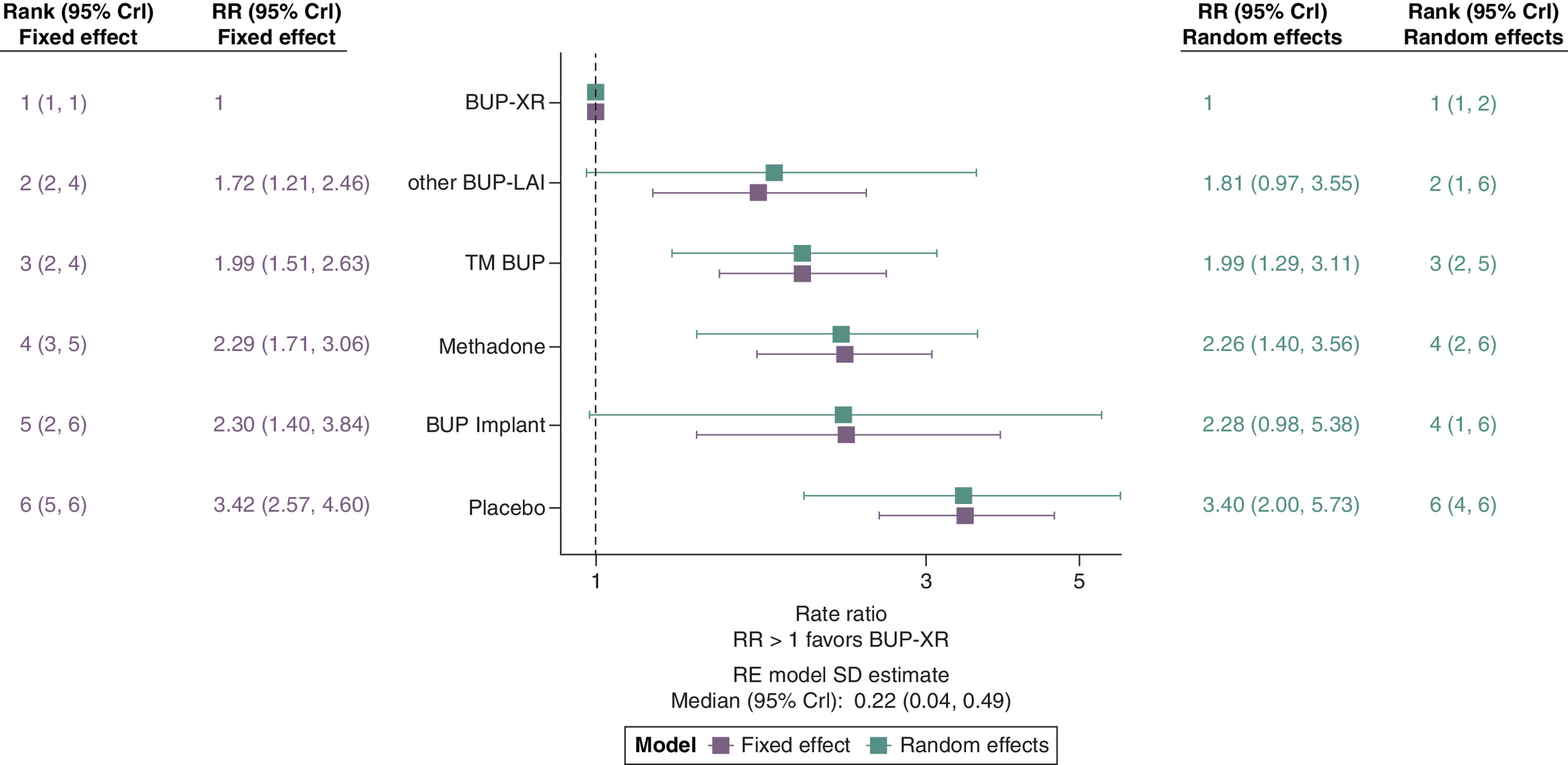
Figure 4. Forest plot showing the effectiveness of each treatment relative to extended-release buprenorphine in terms of illicit opioid use based on a network meta-analysis of data from randomized controlled trials and nonrandomized controlled trials.
A risk ratio greater than 1 indicates individuals are more likely to partake in illicit opioid use on the corresponding treatment compared with on BUP-XR.
BUP: Buprenorphine; BUP-XR: Extended-release buprenorphine; CrI: Credible interval; RR: Rate ratio; TM: Transmucosal.
BUP-XR had the highest probability of opioid abstinence at 3, 6, 12 and 18 months compared with all other OUD treatments across both analyses, including RCTs and real-world observational studies and RCTs only studies (Figure 5). The exploratory analysis including matched single-arm studies and studies with predicted opioid use given the reported treatment discontinuation showed that all other OATs were associated with significantly higher rate of illicit opioid use versus BUP-XR (Supplementary Appendix 8.4). The pairwise comparison results are presented in Supplementary Appendix 9.
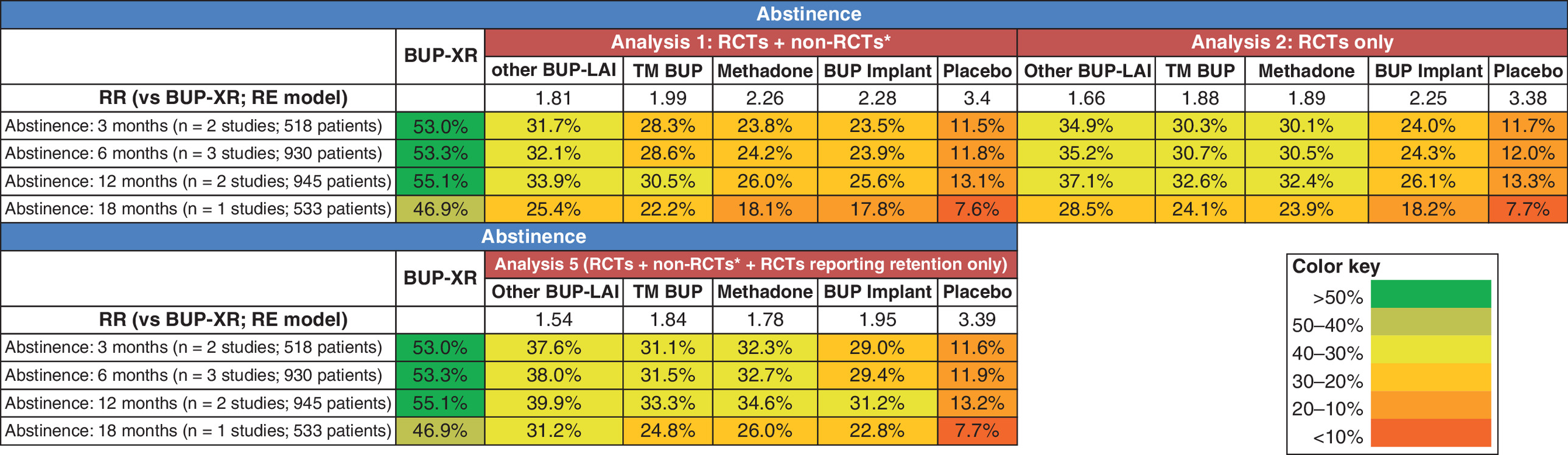
Figure 5. Percentage of study participants abstaining from opioid use on each treatment included in the network meta-analysis at 3, 6, 12 and 18 months.
*The results for BUP-XR were obtained by averaging the reported percentages from each BUP-XR study at a fixed time point where data were available. The number in parenthesis indicates the number of studies and number of eligible patients included in calculating the percentage for BUP-XR.
BUP-XR: Sublocade®/SubutexPRO®; other BUP-LAI: Brixadi®/Buvidal®; BUP: Buprenorphine; RCT: Randomized controlled trial; TM BUP: Transmucosal buprenorphine.
Overall, evidence on safety and HRQoL outcomes was sparse. There was no evidence to suggest significant differences in serious TEAE, severe TEAE, vomiting, headache and insomnia (Table 1 for the summary results and Supplementary Appendix 11 for details). NMA was feasible for only one HRQoL outcome, the Substance Use Recovery Evaluator (SURE) based on two RCTs. Patients treated with BUP-XR exhibited a higher mean SURE score than other BUP-LAI (MD: -6.64 [95% CrI: -12.02–1.23]) and TM buprenorphine (MD: -4.72 [95% CrI: -8.86–0.63]), indicating a better recovery among patients treated with BUP-XR (Supplementary Appendix 11.7).
| Safety outcome (analysis) | Model | Odds ratio (95% CrI) comparing BUP-XR vs other OUD treatments | ||||
|---|---|---|---|---|---|---|
| Other BUP-LAI | Methadone | BUP implant | TM BUP | Placebo | ||
| Serious TEAE (RCT + non-RCT) | Random effects | 0.81 (0.13, 3.79) | 2.35 (0.24, 14.11) | 0.87 (0.14, 3.74) | 1.27 (0.29, 3.61) | 1.70 (0.36, 6.11) |
| Fixed effect | 0.90 (0.34, 2.32) | 2.88 (0.86, 10.47) | 1.00 (0.35, 2.78) | 1.44 (0.75, 2.84) | 1.86 (0.77, 4.23) | |
| Serious TEAE (RCTs only) | Random effects | 0.69 (0.09, 3.47) | 3.54 (0.28, 31.10) | 0.87 (0.13, 3.78) | 1.26 (0.27, 3.73) | 1.71 (0.35, 6.30) |
| Fixed effect | 0.80 (0.29, 2.10) | 4.03 (1.06, 18.32) | 1.00 (0.34, 2.78) | 1.44 (0.74, 2.85) | 1.86 (0.76, 4.27) | |
| Severe TEAE (RCTs only; no non-RCT reported the data) | Random effects | 0.47 (0.00, 54.32) | 5.60 (0.03, >1000) | 0.82 (0.02, 41.79) | 1.28 (0.03, 64.41) | 0.51 (0.03, 7.13) |
| Fixed effect | 0.48 (0.06, 3.65) | 5.42 (0.29, 238.81) | 0.81 (0.13, 5.16) | 1.29 (0.22, 7.96) | 0.52 (0.15, 1.41) | |
| Vomiting (RCTs only; no non-RCT reported the data) | Random effects | 2.33 (0.08, 79.60) | 0.71 (0.04, 9.83) | 1.61 (0.11, 26.11) | 0.92 (0.08, 9.96) | 0.48 (0.07, 3.04) |
| Fixed effect | 2.25 (0.23, 27.39) | 0.74 (0.14, 3.59) | 1.49 (0.25, 8.19) | 0.89 (0.19, 3.71) | 0.48 (0.13, 1.28) | |
| Headache (RCTs only; no non-RCT reported the data) | Random effects | 0.98 (0.18, 4.63) | 0.83 (0.19, 3.15) | 1.03 (0.26, 3.72) | 1.04 (0.27, 3.50) | 0.63 (0.19, 1.81) |
| Fixed effect | 0.97 (0.27, 3.27) | 0.83 (0.25, 2.41) | 1.00 (0.32, 2.77) | 1.04 (0.35, 2.73) | 0.62 (0.23, 1.45) | |
| Any TEAE (RCTs only; for RCT + non-RCTs inconsistency was observed between direct and indirect evidence) | Random effects | 0.30 (0.03, 3.21) | 0.83 (0.09, 7.35) | 0.11 (0.01, 0.87) | 0.31 (0.06, 1.57) | 0.29 (0.05, 1.87) |
| Fixed effect | 0.34 (0.20, 0.58) | 0.90 (0.45, 1.86) | 0.11 (0.07, 0.18) | 0.31 (0.21, 0.45) | 0.32 (0.22, 0.47) | |
An odds ratio greater than 1 indicates individuals are more likely to experience the adverse event on the corresponding treatment compared with on BUP-XR.
BUP: Buprenorphine; BUP-XR: Extended-release buprenorphine; BUP-XR: Sublocade®/SubutexPRO®; CrI: Credible interval; LAI: Long-acting injectable; BUP-LAI: Brixadi®/Buvidal®; RCT: Randomized controlled trial; TM: Transmucosal; TM BUP: Transmucosal buprenorphine; TEAE: Treatment emergent adverse event.
We used a random effects model to quantify statistical heterogeneity among the included studies. For primary outcomes, the results suggested moderate heterogeneity according to Ren et al. [39], with the between-study heterogeneity estimated being 0.32 (95% CrI: 0.19–0.51) for treatment discontinuation (Figure 2) and 0.22 (95% CrI: 0.04–0.49) for illicit opioid use (Figure 4) for the analysis based on RCTs and non-RCTs. The estimated magnitude of heterogeneity among the studies was similar when using RCTs only studies for treatment discontinuation (0.35 [95% CrI: 0.2–0.57]) (Supplementary Appendix 8.1), but lower for illicit opioid use (0.11 [95% CrI: 0–0.38]) (Supplementary Appendix 8.3). The estimated between-study heterogeneity was moderate to high for safety and HRQoL outcomes, ranging from 0.19 to 1.00.
We also conducted a series of subgroup analyses by excluding studies conducted in correctional settings, with comorbid populations, and removing both the studies conducted in correctional settings and with comorbid populations for the primary outcomes to explore the potential reason for heterogeneity. The results of the subgroup analyses were consistent with base case results presented above, with no significant differences observed (Supplementary Appendix 10).
The risk of bias assessment of studies included in the SLR is summarized in Supplementary Appendix 5. The RoB 2 assessment of RCTs found that 48 (73%) had an overall low risk of bias. Bias arising from the randomization process led to 15 (23%) RCTs being rated as having some concerns, while three (5%) RCTs were judged to be at high risk of bias (Supplementary Appendix 5.1–5.3). The NOS scale used to assess non-RCTs showed that quality scores for included studies ranged between 2 and 9 stars, with most studies (75%) receiving a rating of 5 or more stars, indicating good quality. Conference abstracts were generally rated lower. All comparative studies received 5 or more stars, and six studies were given 7 to 9 stars (Supplementary Appendix 5.4). There were not enough studies to robustly assess the risk of bias arising from reporting biases. Piralishvili et al. was deemed to be associated with high risk of bias (Supplementary Appendix 5.1) and was included in the NMA for both treatment discontinuation (12 weeks data were used) and illicit opioid use analysis (included by predicting abstinence using the surrogate meta-analysis (Supplementary Appendix 3.1). A sensitivity analysis excluding this study provided consistent results with base case results presented above (Figures 6 & 7).
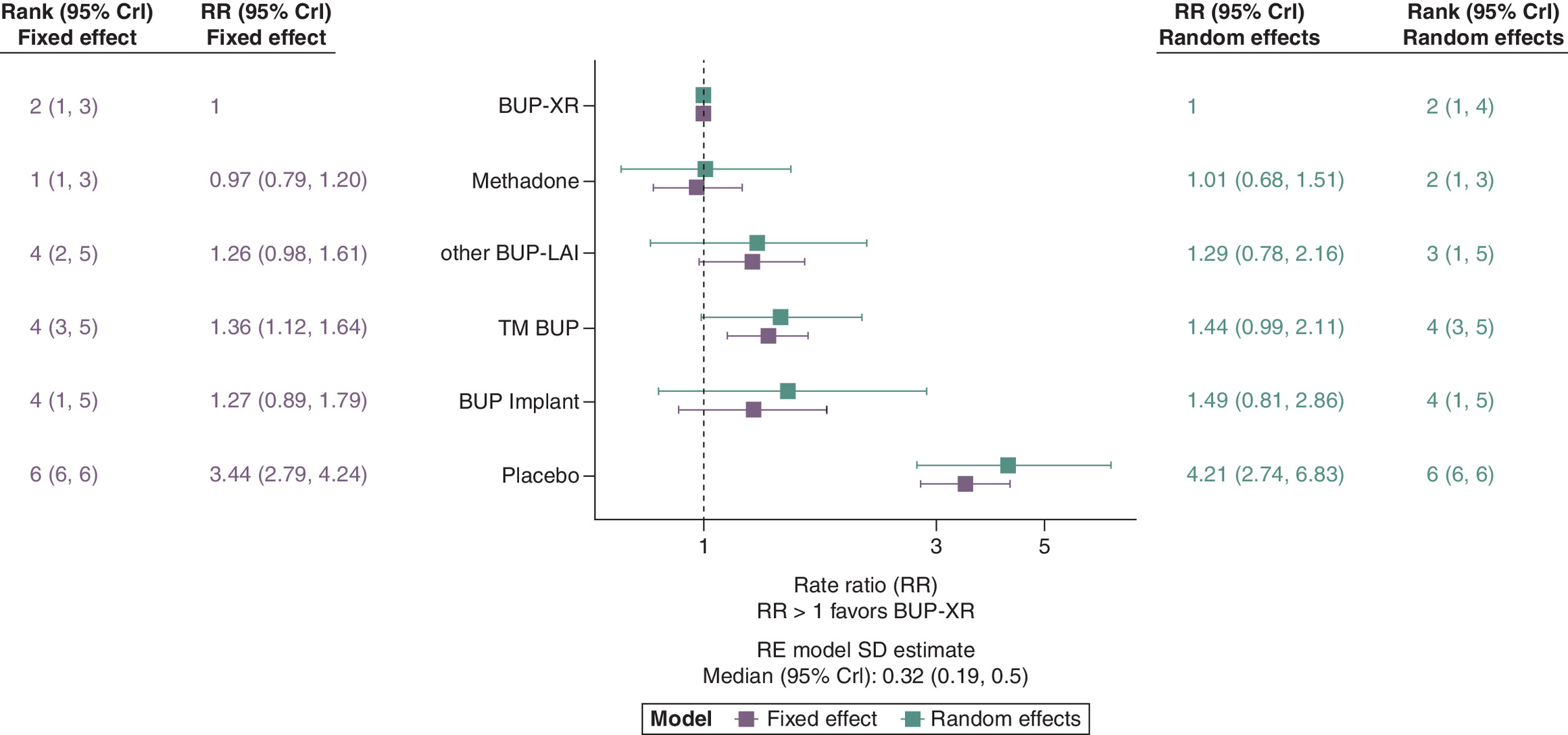
Figure 6. Sensitivity analysis: Forest plot showing the effectiveness of each treatment relative to BUP-XR in terms of treatment discontinuation based on a network meta-analysis of data from randomized controlled trials and nonrandomized controlled trials but removing the studies with high risk of bias.
A risk ratio greater than 1 indicates individuals are more likely to discontinue treatment compared with BUP-XR.
BUP: Buprenorphine; BUP-XR: Extended-release buprenorphine; CrI: Credible interval; RR: Rate ratio; TM: Transmucosal.
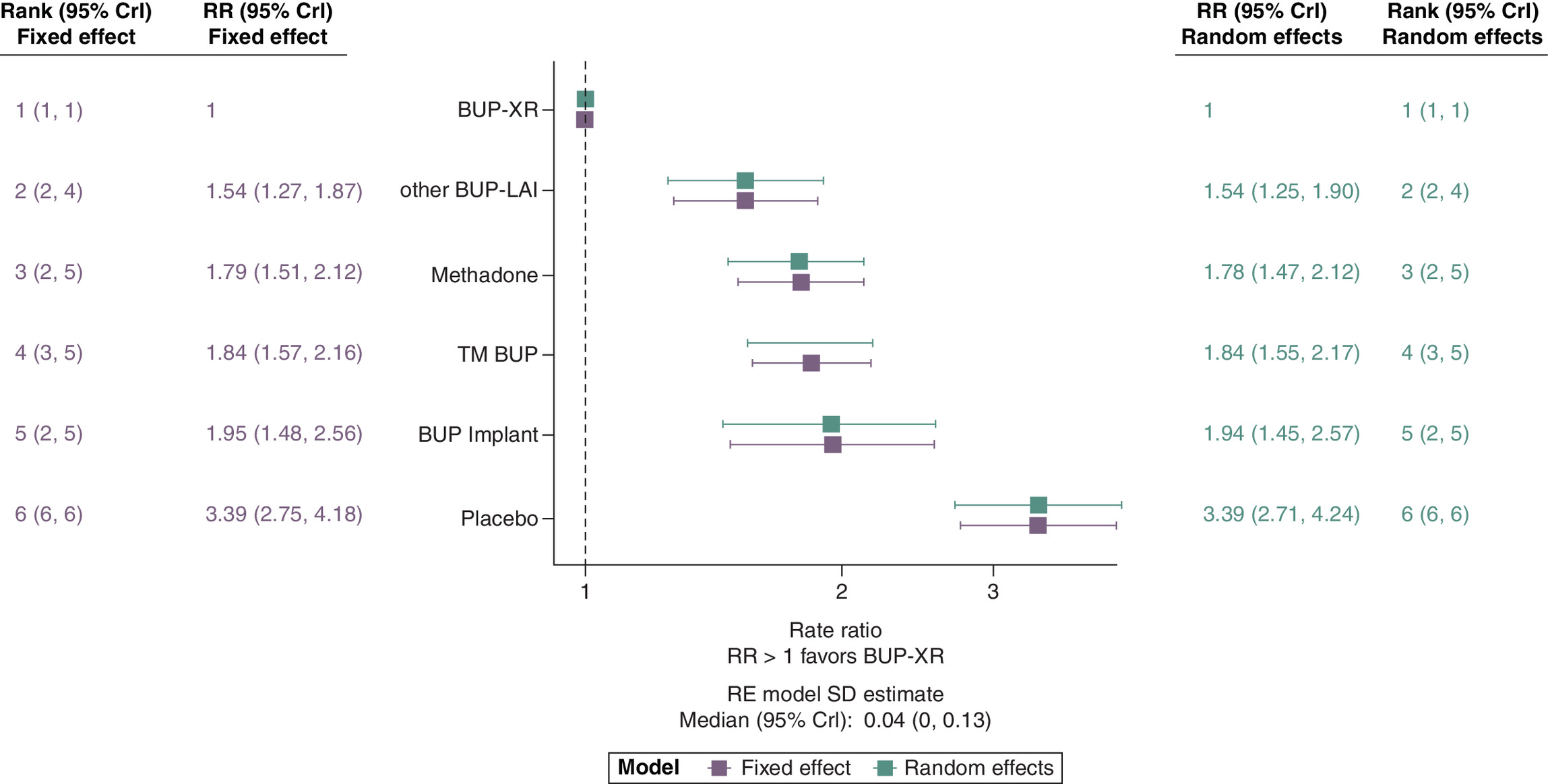
Figure 7. Sensitivity analysis: Forest plot showing the effectiveness of each treatment relative to extended-release buprenorphine in terms of illicit opioid use based on an network meta-analysis of data from randomized controlled trials, nonrandomized controlled trials, matched single-arm studies and studies where opioid use was predicted using surrogate meta-analysis, but removing the studies with high risk of bias.
A risk ratio greater than 1 indicates individuals are more likely to partake in illicit opioid use on the corresponding treatment compared with on BUP-XR.
BUP: Buprenorphine; BUP-XR: Extended-release buprenorphine; CrI: Credible interval; RR: Rate ratio; TM: Transmucosal.
Sensitivity analyses results based on using a fixed effect model had similar point estimates as the results from the random effects model but with slightly narrower CrIs. This was expected as a fixed effect model assumes no heterogeneity among the included studies.
Discussion
To our knowledge, this is the first comprehensive NMA to incorporate both RCTs and non-RCTs to compare LAIs with oral OATs and with each other. The probability of retention was consistently higher with BUP-XR compared with other BUP-LAI, TM buprenorphine, and buprenorphine implant. This observation is consistent with a Canadian study by Lee et al. which found that three-fourths of patients starting on BUP-XR were retained on treatment, with longer retention being associated with greater success in reducing illicit opioid use [40]. Furthermore, in retrospective cohort studies by Partanen et al. [41,42], most patients required a second weekly BUP-LAI injection after ∼5 days rather than the recommended 7. While many stabilized on a 7-day interval within 3–4 weeks, a substantial proportion continued to need shorter intervals. For monthly BUP-LAIs, most patients stabilized on ≥28 day dosing by the seventh dose, though about a third required more frequent injections. Finally, a 96-week long-term study (CoLAB) from Australia showed that 76 of 77 participants who consented to stay for additional follow-up were retained on monthly BUP-XR, with a median retention time of 90 weeks [43,44]. The probability for retention with BUP-XR was found to be comparable to that with methadone across analyses. However, it should be noted that in the case of methadone, treatment retention may not necessarily lead to abstinence [30].
Based on treatment rankings, BUP-XR appeared to be the most effective treatment for opioid abstinence compared with ‘other BUP-LAI’ and oral OATs, with most effects being statistically significant in favor of BUP-XR. Indeed, based on our experience, LAIs differ in real-world effectiveness. In countries such as Finland, some require 3-week dosing or top-ups in the final week when treating with other BUP-LAI, unlike RCT findings. By contrast, we have observed in practice that BUP-XR maintained patient stability across the full 4-week cycle.
Our study shows that the risk of adverse events was comparable between BUP-XR and other comparators, which aligns well with another systematic review of LAIs demonstrating that LAIs appeared to be well tolerated and there were no significant safety concerns [21].
The NMA also indicates better recovery among patients treated with BUP-XR. However, this is based on limited evidence included in the NMA. It is also important to note that HRQoL outcomes can vary significantly based on geographical location, patient demographics, and who administered the treatment (e.g., nurse and physician), potentially introducing bias.
Our study synthesized evidence from RCTs and non-RCTs, including RWE, through a comprehensive literature search on LAIs and expanded on recent meta-analyses and NMAs of other OUD treatments. We incorporated RWE using matched single-arm technique and additional studies not reporting abstinence results using surrogate meta-analysis to predict such outcome to enrich the limited evidence base for LAIs. The use of RWE and surrogate meta-analysis in this NMA highlight the growing importance of incorporating data from routine clinical practice into healthcare decision-making [45,46].
Several limitations warrant consideration. This review was not prospectively registered in a public registry, which limits external verification of the protocol; however, established methodological standards were applied consistently throughout the review process. RWE was included only for LAIs due to the scarcity of RCTs for LAIs compared with treatments such as methadone. Including RWE studies enabled us to capture a broader evidence base but introduced potential residual bias. However, our pragmatic approach of including RWE exclusively for LAIs, rather than for oral OATs could influence comparative findings if real-world studies for oral OATs differ systematically from RCTs. Heterogeneity in study design and outcome definitions was present; although subgroup analyses were conducted, meta-regression was not feasible due to the small number of studies. Where feasible, we recalculated rates of illicit opioid use by imputing missing data as events. No sensitivity analyses were conducted to assess the impact of this imputation method as this provides the most pessimistic results and is a standard approach in OUD analysis. Studies lacking consistent outcome definitions were excluded, which reduced the number of studies included in our analysis. Publication bias is also a potential concern, particularly for comparisons represented by a sparse evidence base. The limited number of studies contributing to some nodes in the network precluded formal assessment of publication bias using funnel plots, and therefore the presence of selective reporting cannot be ruled out. Finally, data on safety and HRQoL were limited and the available data were limited with small sample sizes and incomplete reporting. Hence, our findings in these areas should be interpreted with caution.
The study showed that BUP-XR may offer advantages in treatment retention and abstinence over other OUD therapies. Additionally, BUP-XR showed comparable safety to other treatments and better HRQoL in terms of recovery compared with other BUP-LAI and TM buprenorphine. These findings support the integration of LAIs into treatment pathways and suggest that policymakers and clinicians should consider the broader evidence base, including RWE, in OUD treatment decisions. Given that healthcare delivery systems differ in resource allocation, regulatory frameworks, and service integration, these contextual factors should also be considered when applying our findings in practice.
Summary points
•
The aim of the study was to provide comparative evidence among buprenorphine long-acting injectables (LAIs) and versus oral opioid agonist treatments.
•
This is the first comprehensive network meta-analysis incorporating both randomised controlled trials (RCTs) and non-RCTs to compare LAIs with oral opioid agonist therapies (transmucosal buprenorphine and methadone) and with each other.
•
Buprenorphine LAIs monthly injection (BUP-XR) demonstrated the highest probability of achieving treatment retention and opioid abstinence across analyses.
•
Safety outcomes were generally comparable across treatments.
•
Health-related quality of life indicated better recovery among patients treated with BUP-XR.
•
The inclusion of real-world data and exploratory methods to handle sparse networks enhances the relevance of these findings for broader clinical settings.
Author contributions
M Kabra, T Srivastava, S Ren conceived the study with medical expertise from A De Jong-Laird and support from R Gautam. R Gautam and T Srivastava developed the review protocol with review and subject expertise from M Kabra and A De Jong-Laird. R Gautam and T Srivastava screened titles and abstracts, performed full-text review and extracted data. A Gupta and J Singh conducted the statistical analysis and performed the network meta-analysis with oversight from S Ren and inputs from M Kabra and A De Jong-Laird. A Gupta and J Singh verified the underlying data. J Oksanen, T MacDonald, K Lee, B Boyett and B Santoro provided clinical expertise throughout the conduct of the study and writing of the manuscript. M Kabra, R Gautam and S Ren wrote the first draft of the manuscript with input from all authors. All authors critically revised the manuscript for important intellectual content. M Kabra and A De Jong-Laird obtained funding and supervised the project. All authors had full access to the data, take responsibility for its integrity and accept responsibility for the decision to submit for publication.
Acknowledgments
The authors thank Yue Zhao from Indivior for providing input on the study design.
Financial disclosure
Funding was received from Indivior PLC.
Competing interests disclosure
M Kabra is an employee of Indivior Ltd. T MacDonald has previously received honoraria, fees or professional development funding/resources from Aurora Health, Royal Australian and New Zealand College of Psychiatrists and Griffith University. K Lee has previously received honoraria and consulting fees from Indivior Ltd. A De Jong-Laird was an employee of Indivior Ltd and held stock options for Indivior Ltd when the study was conducted. T Srivastava, R Gautam, J Singh, A Gupta and S Ren have received consulting fees from Indivior Ltd. J Oksanen, B Boyett and B Santoro have no interests to disclose. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Eleni Tente of ConnectHEOR, London, UK, with funding from Indivior PLC.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 1.07 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th Edition. American Psychiatric Publishing, VA, USA (2013).
2.
American Psychiatric Association. Opioid use disorder (2018). (Accessed: 20 March 2025). Available from: https://www.psychiatry.org/patients-families/addiction/opioid-use-disorder/opioid-use-disorder
3.
Canadian Institute of Health Research, Canadian Research Initiative on Substance Misuse (CRISM) National Guideline Review Committee. CRISM National Guideline for the clinical management of opioid use disorder (2018). (Accessed: 20 March 2025). Available from: https://crism.ca/wp-content/uploads/2018/03/CRISM_NationalGuideline_OUD-ENG.pdf
4.
American Society of Addiction Medicine (ASAM). The ASAM National Practice Guideline for the treatment of opioid use disorder 2020 focused update (2020). (Accessed: 20 March 2025). Available from: https://www.asam.org/quality-care/clinical-guidelines/national-practice-guideline
5.
Iversen J, Page K, Madden A, Maher L. HIV, HCV and health-related harms among women who inject drugs: implications for prevention and treatment. J. Acquir. Immune Defic. Syndr. 69(01), S176–S181 (2015).
6.
Keeshin SW, Feinberg J. Endocarditis as a marker for new epidemics of injection drug use. Am. J. Med. Sci. 352(6), 609–614 (2016).
7.
Slawek DE, Lu TY, Hayes B, Fox AD. Caring for patients with opioid use disorder: what clinicians should know about comorbid medical conditions. Psychiatr Res Clin Pract. 1(1), 16–26 (2019).
• Of interest.
8.
Wilcox HC, Conner KR, Caine ED. Association of alcohol and drug use disorders and completed suicide: an empirical review of cohort studies. Drug Alcohol Depend. 76(Suppl.), S11–S19 (2004).
9.
Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: results from the 2023 National Survey on Drug Use and Health (PEP24-07-021, NSDUH Series H-59). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, MD, USA (2024). Available from: https://www.samhsa.gov/data/report/2023-nsduh-annual-national-report
10.
World Health Organization. WHO updates guidelines on opioid dependence treatment and overdose prevention. (2025). Available from: https://www.who.int/news/item/09-02-2025-who-updates-guidelines-on-opioid-dependence-treatment-and-overdose-prevention
• Of interest.
11.
Centers for Disease Control and Prevention. State Unintentional Drug Overdose Reporting System (SUDORS) dashboard: fatal drug overdose data. Department of Health and Human Services, Centers for Disease Control and Prevention, GA, USA (2025). https://www.cdc.gov/overdose-prevention/data-research/facts-stats/sudors-dashboard-fatal-overdose-data.html
12.
Centre for Addiction and Mental Health (Canada). Opioid Agonist Therapy (2016). (Accessed: 20 March 2025). Available from: https://www.camh.ca/-/media/files/oat-info-for-clients.pdf
13.
Kleber HD. Pharmacologic treatments for opioid dependence: detoxification and maintenance options. Dialogues Clin. Neurosci. 9(4), 455–470 (2007).
14.
Alho H, D'Agnone O, Krajci P et al. The extent of misuse and diversion of medication for agonist opioid treatment: a review and expert opinions. Heroin Addict. Relat. Clin. Prob. 17(2–3), 25–34 (2015).
15.
Lofwall MR, Walsh SL. A review of buprenorphine diversion and misuse: the current evidence base and experiences from around the world. J. Addict. Med. 8(5), 315–326 (2014).
• Of interest.
16.
Bond AJ, Witton J. Perspectives on the pharmacological treatment of heroin addiction. Clin. Med. Insights Psych. 8, 117955731773732 (2017).
17.
Schwartz RP, Highfield DA, Jaffe JH et al. A randomized controlled trial of interim methadone maintenance. Arch. Gen. Psychiatry 63(1), 102–109 (2006).
18.
Kamien JB, Branstetter SA, Amass L. Buprenorphine-naloxone versus methadone maintenance therapy: a randomised double-blind trial with opioid-dependent patients. Heroin Addict. Relat. Clin. Probl. 10(4), 5–18 (2008).
19.
Hulse GK, Morris N, Arnold-Reed D, Tait RJ. Improving clinical outcomes in treating heroin dependence: randomized, controlled trial of oral or implant naltrexone. Arch. Gen. Psychiatry 66(10), 1108–1115 (2009).
20.
Marsden J, Kelleher M, Gilvarry E et al. Superiority and cost-effectiveness of monthly extended-release buprenorphine versus daily standard of care medication: a pragmatic, parallel-group, open-label, multicentre, randomised, controlled, phase 3 trial. EClinicalMedicine 66, 102311 (2023).
21.
McMaster J, Abeysundera H. Effectiveness of long-acting buprenorphine - a systematic review. Australas. Psychiatry 33(2), 235–248 (2025).
22.
US Food & Drug Administration (FDA). Framework for FDA's real-world evidence program. (2018). (Accessed: 15 May 2025). Available from: https://www.fda.gov/media/120060/download
23.
European Medicines Agency (EMA). Guideline on registry-based studies (2021). (Accessed: 15 May 2025). Available from: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-registry-based-studies_en.pdf
24.
Makady A, Ham RT, de Boer A, Hillege H, Klungel O, Goettsch W. GetReal Workpackage 1. Policies for use of real-world data in health technology assessment (HTA): a comparative study of six HTA agencies. Value Health 20(4), 520–532 (2017).
25.
CG HTA. Guidance on the validity of clinical studies for joint clinical assessments (2024). (Accessed: 10 February 2025). Available from: https://health.ec.europa.eu/document/download/9f9dbfe4-078b-4959-9a07-df9167258772_en?filename=hta_clinical-studies-validity_guidance_en.pdf
26.
Higgins JPT, Thomas J, Chandler J et al. Cochrane Handbook for Systematic Reviews of Interventions. 2nd Edition. 736, John Wiley & Sons, NJ, USA (2022).
27.
Hutton B, Salanti G, Caldwell DM et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162(11), 777–784 (2015).
28.
Zorzela L, Loke YK, Ioannidis JP et al. PRISMA harms checklist: improving harms reporting in systematic reviews. Brit. Med. J. 352, i157 (2016).
29.
Lim J, Farhat I, Douros A, Panagiotoglou D. Relative effectiveness of medications for opioid-related disorders: a systematic review and network meta-analysis of randomized controlled trials. PLoS ONE 17(3), e0266142 (2022).
•• Of considerable interest.
30.
Degenhardt L, Clark B, Macpherson G et al. Buprenorphine versus methadone for the treatment of opioid dependence: a systematic review and meta-analysis of randomised and observational studies. Lancet Psych. 10(6), 386–402 (2023).
•• Of considerable interest.
31.
Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU Technical Support Document 2: A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials. National Institute for Health and Care Excellence, UK (NICE) (2014).
32.
NICE Decision Support Unit. Evidence Synthesis TSD series (2012). (Accessed: 1 March 2024). Available from: https://www.sheffield.ac.uk/nice-dsu/tsds/evidence-synthesis
33.
Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. NICE DSU Technical Support Document 4: Inconsistency in Networks of Evidence Based on Randomised Controlled Trials. National Institute for Health and Care Excellence (NICE), UK (2011).
34.
Sturtz S, Ligges U, Gelman A. R2WinBUGS: a package for running WinBUGS from R. J. Stat. Software 12, 1–16 (2005).
35.
Daniels MJ, Hughes MD. Meta-analysis for the evaluation of potential surrogate markers. Stat. Med. 16(17), 1965–1982 (1997).
• Of interest.
36.
Schmitz S, Maguire Á, Morris J et al. The use of single armed observational data to closing the gap in otherwise disconnected evidence networks: a network meta-analysis in multiple myeloma. BMC Med. Res. Methodol. 18(1), 66 (2018).
37.
Sterne JAC et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. Brit Med. J. 366, l4898 (2019).
38.
Wells GA, Shea B, O'Connell D et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. (Accessed: 1 March 2024). Available from: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
39.
Ren S, Oakley JE, Stevens JW. Incorporating genuine prior information about between-study heterogeneity in random effects pairwise and network meta-analyses. Med. Decis. Making 38(4), 531–542 (2018).
40.
Lee K. Treatment retention with monthly buprenorphine extended release injection: results from a Canadian Rapid Access Addiction Medicine Clinic: 21 Month Data (2025). (Accessed: 10 March 2025). Available from: https://www.cpmdependance.ca/documents/80779/0/Ken+Lee+Poster+48+x+36+Version+2+Sept+8+2021+%281%29.pdf/a0544658-f552-4d93-88d7-cddafe94c27c
41.
Partanen M, Saarenpää T, Prami T, Iso-Mustajärvi I, Ryder B, Simojoki K. Early experience of buprenorphine long-acting injection in Finland: a retrospective cohort study. Poster presented at: European Congress on Heroin Addiction & Related Clinical Problems, Pisa, Italy, 20–22 May 2022.
42.
Partanen M, Saarenpää T, Prami T et al. Early experiences of buprenorphine long-acting injection in Finland: a retrospective cohort study. Poster presented at: International Society of Addiction Medicine (ISAM) Annual Conference, Hamburg, Germany, 26–28 May 2025.
43.
Farrell M, Shahbazi J, Byrne M et al. Outcomes of a single-arm implementation trial of extended-release subcutaneous buprenorphine depot injections in people with opioid dependence. Int. J. Drug Policy 100, 103492 (2022).
44.
Farrell M, Shahbazi J, Chambers M et al. 96-week retention in treatment with extended-release subcutaneous buprenorphine depot injections among people with opioid dependence: extended follow-up after a single-arm trial. Int. J. Drug Policy 127, 104390 (2024).
45.
Burns L, Le Roux N, Kalesnik-Orszulak R et al. Real-world evidence for regulatory decision-making: updated guidance from around the world. Front. Med. 10, 1236462 (2023).
46.
Akehurst R, Murphy LA, Solà-Morales O, Cunningham D, Mestre-Ferrandiz J, de Pouvourville G. Using real-world data in the health technology assessment of pharmaceuticals: strengths, difficulties, and a pragmatic way forward. Value Health 26(4), 11–19 (2023).
Information & Authors
Information
Published In
Copyright
© 2026 Indivior Ltd. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 14 October 2025
Accepted: 18 December 2025
Published online: 12 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effectiveness and safety of therapies for patients with opioid use disorder: a systematic review and network meta-analysis. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0171
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Justin Seltzer, Riku Moriguchi, Kara Yeung, Yuri Shindo, Jeremy Hardin, Henrik Galust, Alicia Minns, Richard Clark, Encephalopathy following subcutaneous administration of Brixadi® extended-release buprenorphine, Toxicology Reports, 10.1016/j.toxrep.2026.102320, 17, (102320), (2026).
- John J. McCarthy, Martin H. Leamon, A Narrative Review of the Metabolic Assessment of Patients on Methadone: An Alternative to Pharmacokinetically Blind Prescribing, Journal of Addiction Medicine, 10.1097/ADM.0000000000001719, (2026).