Population-adjusted network meta-analyses provide new insights into the efficacy of treatment alternatives for metastatic castration-sensitive prostate cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Recent network meta-analyses (NMAs) in metastatic castration-sensitive prostate cancer have not adequately addressed potential treatment effect modifiers and population imbalances, which introduces bias. Although, individual-patient data (IPD) are seldom available across all trials, recent methodological advances allow adjustments using a combination of IPD and aggregate data. Materials & methods: IPD from the ARASENS trial (darolutamide + docetaxel + androgen-deprivation-therapy [ADT]) and aggregate data from a systematic review were analyzed. Two methods were used to adjust for population imbalances: multilevel network meta-regression (ML-NMR) using baseline characteristics, and network meta-interpolation (NMI) using subgroup data. Relative effects were estimated for an ARASENS-like population, with sensitivity analysis in an average trial population. Results: Twelve studies, including ARASENS, were included. All studies reported baseline characteristics for ML-NMR. Sufficient subgroup data for NMI were available in 8/12 studies for overall survival (OS) and 5/12 studies for progression-free survival (PFS). Darolutamide + docetaxel + ADT showed significant benefit over docetaxel + ADT, ADT and standard-nonsteroidal-antiandrogen + ADT in all analyses. ML-NMR showed improved OS for darolutamide + docetaxel + ADT compared with abiraterone + docetaxel + ADT, apalutamide + ADT, enzalutamide + ADT and abiraterone + ADT. ML-NMR also showed improved PFS for darolutamide + docetaxel + ADT compared with apalutamide + ADT and enzalutamide + ADT. Using NMI, darolutamide + docetaxel + ADT demonstrated OS benefit over abiraterone + ADT and PFS benefit relative to abiraterone + ADT and apalutamide + ADT. Findings were consistent in an average population, although ML-NMR did not show significant OS benefit of darolutamide + docetaxel + ADT over apalutamide + ADT. Conclusion: Improved outcomes were observed with darolutamide + docetaxel + ADT compared with other therapies. By incorporating effect modifiers and addressing population imbalances, we provide clinicians with a more accurate understanding of treatment efficacy for better-informed decision-making.
Plain language summary: comparing treatment options for people with metastatic prostate cancer using population adjustment methods
What is this article about?
This study examines different statistical methods for comparing treatments for metastatic castration-sensitive prostate cancer across multiple trials, taking into account differences among patients, such as age and health status. We evaluated different statistical approaches to adjust for these varying patient characteristics and assessed their strengths and limitations in producing reliable treatment comparisons. The study presents results for key clinical outcomes, including overall survival and progression-free survival.
What were the results?
Our findings provide evidence that the combination of darolutamide, docetaxel and androgen-deprivation-therapy (ADT) improves survival rates for patients with metastatic castration-sensitive prostate cancer compared with other treatment options.
What do the results mean?
The findings suggest that patients receiving the darolutamide, docetaxel and ADT combination therapy may live longer and have better outcomes, aiding doctors in making informed treatment choices.
Androgen deprivation therapy (ADT) is the cornerstone in the management of patients with metastatic prostate cancer [1]. Prostate cancer that has not previously been treated with ADT is considered to be hormone-sensitive or castration-sensitive prostate cancer (mCSPC). The treatment landscape for mCSPC has evolved rapidly over the last decade with the addition of docetaxel and the novel androgen receptor pathway inhibitor (ARPIs), such as abiraterone, enzalutamide, apalutamide and darolutamide. The European Society for Medical Oncology (ESMO) guidelines previously recommended the addition of docetaxel to ADT based on the results of the CHAARTED [2] and STAMPEDE [3] trials. These guidelines also recommend abiraterone, enzalutamide and apalutamide added to ADT as these treatments have shown to improve survival in the LATITUDE [4], ENZAMET [5], ARCHES [6] and TITAN [7] trials, as well as in later arms of STAMPEDE [8]. Recent guidelines recommend ADT with docetaxel and either darolutamide or abiraterone (triplet therapy) for patients with high-volume disease who are fit for chemotherapy based on the results of the ARASENS [9] and PEACE-1 [10] studies.
In a recent review, Shore et al. identified 15 network meta-analyses (NMA) of patients with mCSPC who received docetaxel, novel hormonal therapies plus ADT, standard of care or developmental agents [11]. NMA is the gold standard for comparing multiple treatments, endorsed by the Cochrane organization, National Institute for Health and Care Excellence (NICE), International Society for Pharmacoeconomics and Outcomes Research (ISPOR) and the World Health Organization (WHO) [12–16]. However, it relies on the assumption that distributions of effect-modifying variables do not differ between studies. If this assumption does not hold, results of NMAs might be biased [17]. There is evidence of treatment effect modifiers in mCSPC, which underscores the importance of considering these factors in analyses [11]. The gold-standard to address covariate imbalances is individual patient data (IPD) NMA [18,19]. However, IPD from all relevant studies is rarely available. This is due to legitimate competing interests preventing release of such data.
Only one previous NMA has used IPD to explore effect modification in mCSPC [18]. This found that the benefit of adding docetaxel to ADT was modified by clinical T-stage, timing of metastatic disease, volume of disease and WHO performance status. Due to competing commercial interests, the analysis excluded published randomized controlled trials (RCTs) in mCSPC that evaluated ARPI therapies. Furthermore, subgroup data were not used.
Other methods are available to address covariate imbalance. These are summarized in Figure 1. Meta-regression aims to explain between-trial heterogeneity by incorporating effect modifiers, but uses either aggregate data (AgD) or IPD rather than a combination of both [20]. Population adjustment methods combining IPD and AgD (matching adjusted indirect comparisons and simulated treatment comparisons) have also been developed. However, these methods have been limited to only one comparator and to the target population of the selected comparator [19]. These were key limitations of a recent matching adjusted indirect comparison using IPD from ARCHES to adjust for effect modifiers in a comparison of enzalutamide + ADT with darolutamide + ADT [21]. Recently, multilevel network meta-regression (ML-NMR) and network meta-interpolation (NMI) have emerged as novel population adjusted indirect comparison methods. These methods can consider multiple comparators and can be applied in arbitrary target populations [19,22]. NICE have recommended that the Methods Guide be revised to favor ML-NMR for anchored comparisons [23]. EUHTA guidelines also recommended ML-NMR [24].
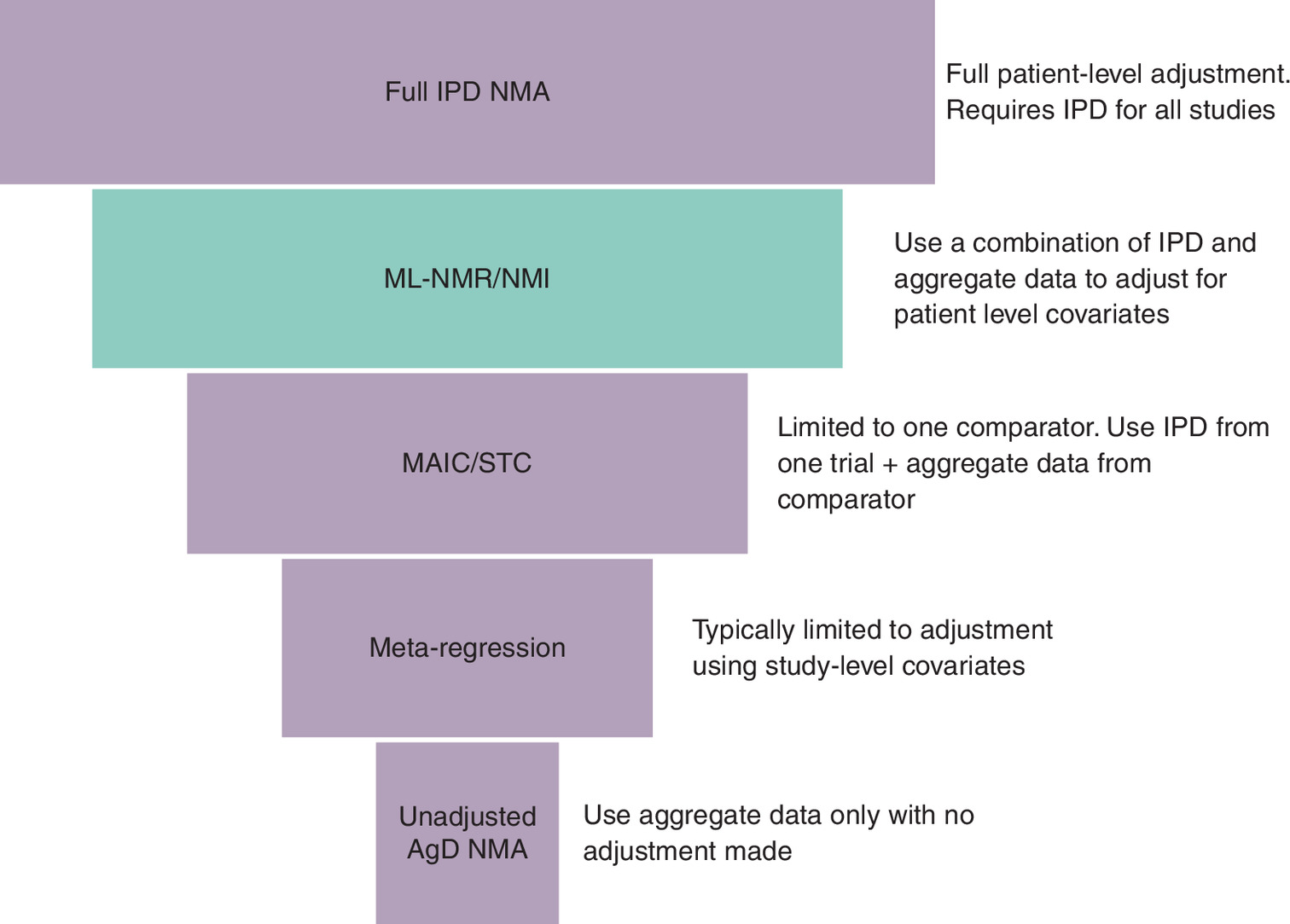
Figure 1. Hierarchy of methods for addressing covariate imbalance in network meta analysis.
AgD: Aggregate data; IPD: Individual patient data; MAIC: Matching adjusted indirect comparison; ML-NMR: Multilevel network meta-regression; NMA: Network meta-analysis; NMI: Network meta interpolation; STC: Simulated treatment comparison.
In this paper, we have applied the novel methods of ML-NMR and NMI to estimate the relative efficacy of systemic treatments for mCSPC, exploring heterogeneity without requiring full IPD access. This paper addresses a gap in the literature by being the first NMA in mCSPC to adjust for population imbalance in effect modifiers using these novel methods.
Materials & methods
Literature reviews
We conducted a targeted overview of reviews on effect modifiers in mCSPC following methodological recommendations, including the Preferred Reporting Items for Overviews of Reviews (PRIOR) statement guidelines [25]. We searched MEDLINE, EMBASE, the Cochrane Database of Systematic Reviews (CDSR) and the Epistemonikos database. Details can be found in Supplementary Materials Section 1.2.
We also conducted a systematic literature review of RCTs evaluating available treatments in mCSPC, following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement 2020 (PROSPERO registration no. CRD42023429478) [26]. We searched in Medline, EMBASE and The Cochrane Library, as well as conference proceedings and trial registers. Proceedings of the June 2022 ASCO conference were also screened. Details can be found in the Supplementary Materials Section 1.1.
We assessed the feasibility of ML-NMR and NMI by comparing trials using the PICOS (population, interventions, comparators, outcomes, study design) framework, reporting of baseline characteristics, reporting of OS and PFS subgroup results and studying network connectivity.
Multilevel network meta-regression
ML-NMR is an extension of NMA to incorporate both IPD and AgD. It allows population adjusted indirect comparisons to be estimated in arbitrary populations and for evidence networks comprising any number of comparators. ML-NMR is often required to make a shared effect modifier assumption in order to estimate treatment-covariate interactions from the available data [27]. This analysis used IPD from the ARASENS trial and intention to treat (ITT) AgD from comparator studies. Treatments except the reference (darolutamide + docetaxel + ADT) were grouped into a single class and the impact of effect modifiers was shared (identical) among them; treatment effects were estimated independently. This assumption implies that only treatment effects relative to the reference are modified by the population characteristics. Missing characteristics were set to the mean across other studies in the analysis. ML-NMR assumes proportional hazards. This assumption was tested by applying a non-proportional hazards model that fits a separate baseline hazard in each treatment arm and comparing the fit to models assuming proportional hazards (details in Supplementary Materials Section 1.3.1).
Network meta-interpolation
NMI adjusts for effect modification in NMA using subgroup analyses [22]. In the first step, available data and the correlation between effect modifiers, estimated using available IPD, are used to impute missing covariates and subgroup results. Simultaneous equations for the HR and standard error (SE) in an arbitrary population are then used to predict the treatment effect for each trial at the desired values of covariates. Finally, the resultant outputs are modeled using standard NMA, where the distribution of the effect modifiers can now be considered balanced. NMI does not rely on modelling effect modification across treatment comparisons directly – instead imputing missing covariate values based on observed data distributions. It therefore does not need to make the shared effect modifier assumption. As with ML-NMR, proportional hazards are assumed.
This analysis used IPD from the ARASENS trial and reported subgroup data from comparator studies. When data were missing, and if the head-to-head comparison reported in the study with missing effect modifiers was not reported in any other study in the network, it was assumed that the effect modifiers under consideration do not modify the relative treatment effect (otherwise a subgroup analysis would have been reported). In this case the study-level treatment effect and SEs were used. If the same head-to-head comparison was reported in another study with subgroup data available, information on effect modification was borrowed from the other study, using the methods described in Harari et al. [22].
Statistical methods
ML-NMR and NMI can be conducted on any target population of interest. In our base case we used the ARASENS population and explored a sensitivity analysis using a hypothetical ‘average’ population, which represents the average characteristics of comparator trials. The methods are illustrated in Figure 2. We conducted the analyses assuming that darolutamide + docetaxel + ADT (darolutamide triplet) is the reference treatment.
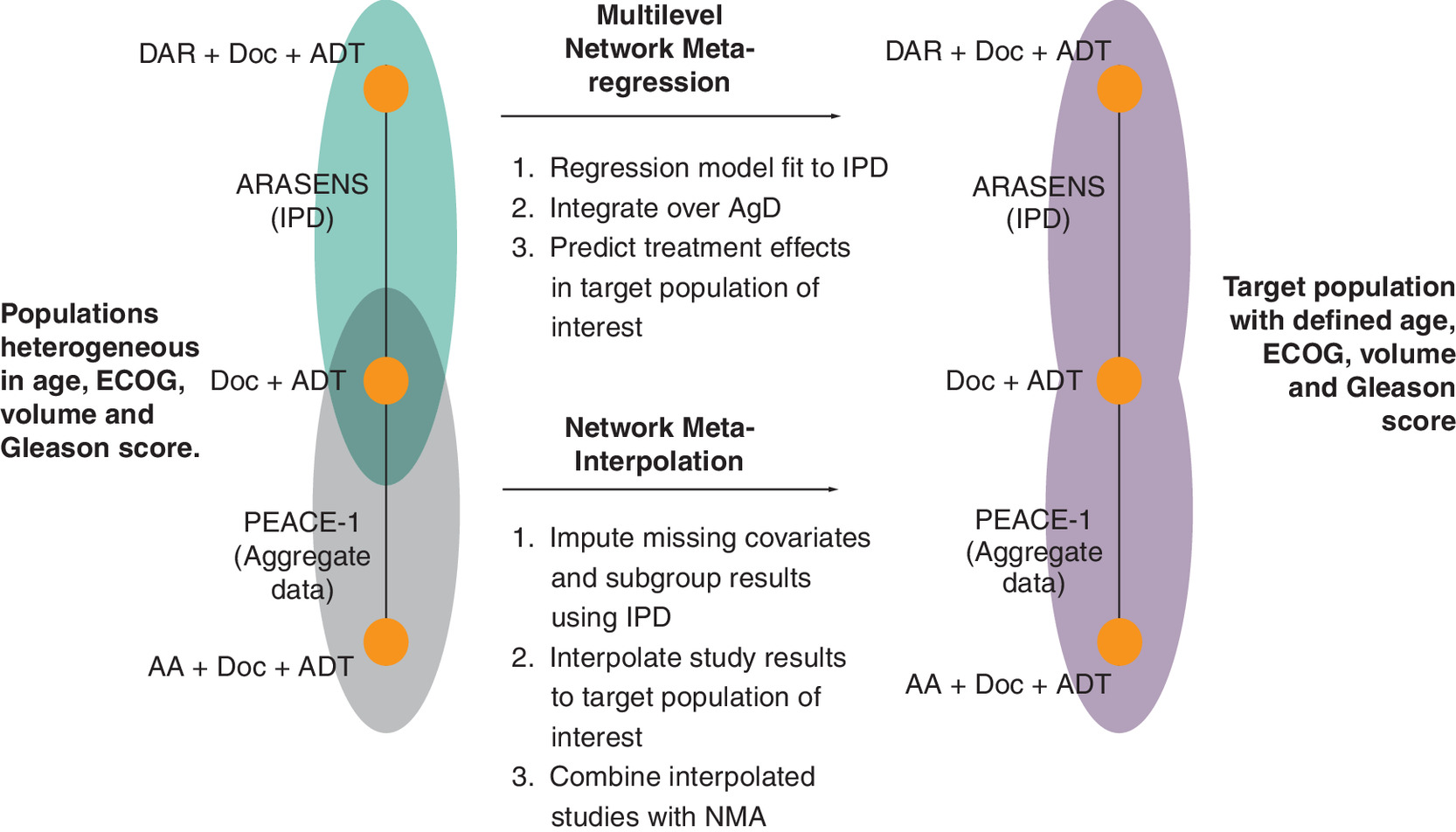
Figure 2. Illustration of multilevel network meta-regression and network meta-interpolation methods.
Subset of network used for illustration.
AA: Abiraterone acetate; ADT: Androgen deprivation therapy; AgD: Aggregate data; DAR: Darolutamide; Doc: Docetaxel; ECOG: Eastern Cooperative Oncology Group; IPD: Individual patient data.
Crossover unadjusted hazard ratios (HRs) from ARCHES [6], TITAN [7] and LATITUDE [4] were used, meaning that no adjustment was made for the multi-arm multi-stage adaptive trial STAMPEDE. This was in line with previous NMAs [28,29]. We also defined PFS from ARASENS as castration resistance or death (CROD) to better align with other included RCTs (Supplementary Materials Section 1.3.4). Results are provided as median HR compared with darolutamide + docetaxel + ADT with 95% credible intervals (CrI).
For NMI, fixed and random effects models were conducted, with the preferred model selected on the basis of statistical measures of fit (details in Supplementary Materials Section 1.3.3). Due to differences in PFS definition across RCTs and the objectivity of OS, we preferred random and fixed effects for these outcomes, respectively.
Software
All analyses were conducted using the Bayesian software OpenBUGS version 3.2.3 with data management in the R statistical software version 4.2.2 [30,31]. The ML-NMR analyses were implemented in the R package ‘multinma’ [32]. The NMI analyses used code adapted from Harari et al. [22]. The code for all analyses is available on GitHub at https://github.com/ednakeeney/MLNMR_NMI. Data are not provided as this relies on confidential IPD from the ARASENS study.
Results
Literature reviews
The targeted literature review of effect modifiers found evidence of effect modification on PFS by Gleason >8, age, metastatic status, and volume of disease (Supplementary Materials Section 2.2). Four biomarkers which are potential effect modifiers (vascular endothelial growth factor, C-reactive protein, long noncoding RNAs and programmed cell death ligand 1) were also identified. All reviews found an association between worse outcomes and higher levels of these factors. However, none of these biomarkers were measured in the studies included in our analyses. They therefore could not be modeled in either ML-NMR or NMI.
After removal of duplicates, the systematic literature review yielded 8506 results. We reviewed 1753 full texts after screening titles and abstracts, of which 27 studies met the inclusion criteria. An updated search conducted in May 2022 retrieved three new studies. The ASCO 2022 conference in June yielded OS data for the high-volume subgroup of CHAARTED from the Tripathi 2022 abstract [33]. A PRISMA flowchart detailing the original and updated searches can be found in the Supplementary Materials Section 2.1.1.
The analyses included twelve studies (ARASENS [9], PEACE-1 [10], Vaishampayan 2021 [34], ARCHES [6], ENZAMET [5], CHAARTED [33], GETUG-AFU 15 [35], LATITUDE [4], STAMPEDE arms C vs A [36], STAMPEDE arms G vs A [8], STAMPEDE arms G vs C [3], and TITAN [7]) (Figure 3 & Table 1). Full baseline characteristics of the included RCTs and a risk of bias assessment using the Cochrane RoB 2.0 are summarized in Supplementary Materials Sections 2.1.2 & 2.1.3.
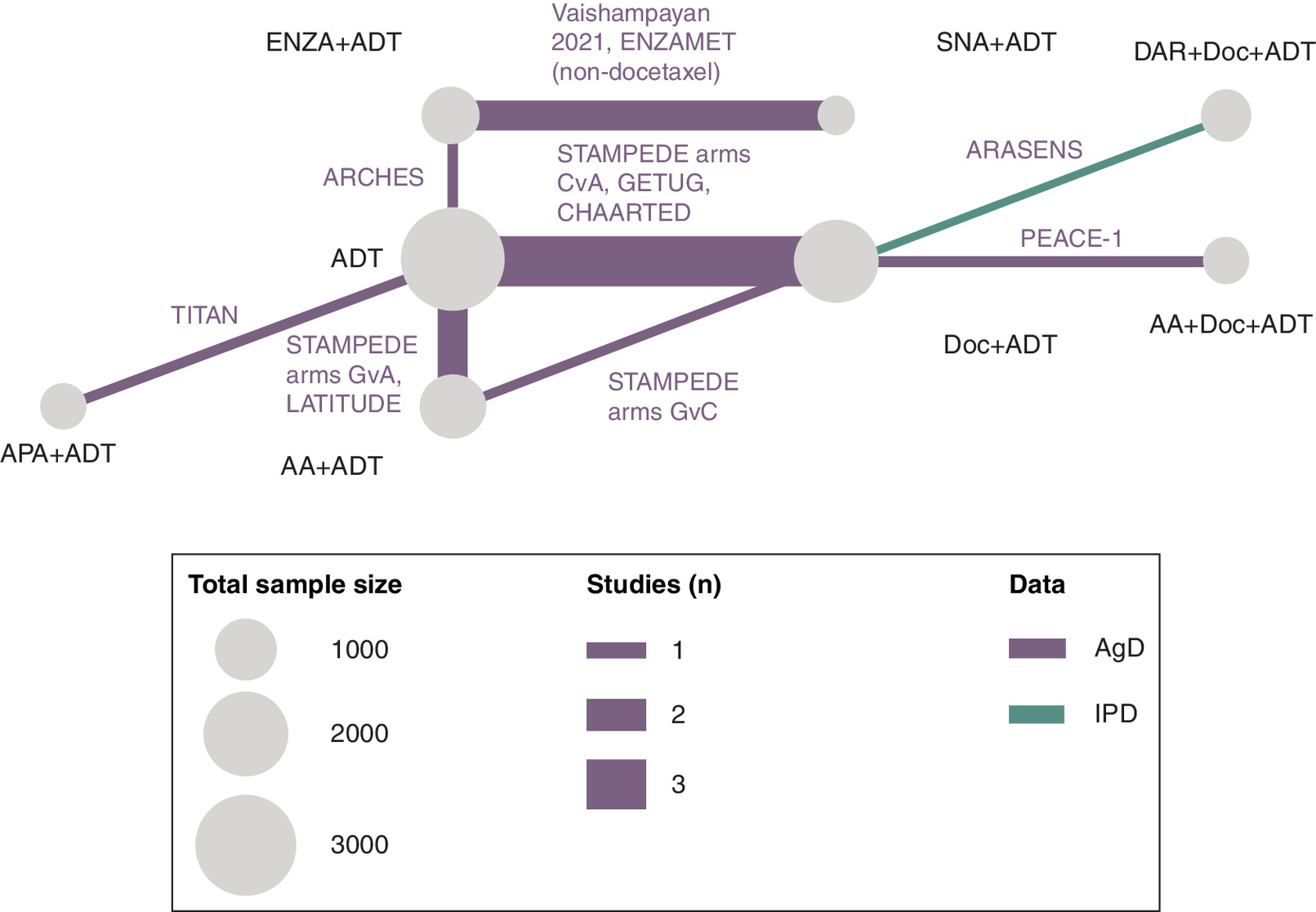
Figure 3. Network diagram.
AA: Abiraterone acetate; ADT: Androgen deprivation therapy; AgD: Aggregate; APA: Apalutamide; DAR: Darolutamide; Doc: Docetaxel; ENZA: Enzalutamide; IPD: Individual patient data; SNA: Standard nonsteroidal antiandrogen.
| Study characteristics | Treatment indicator | ARCHES [6] | Vaishampayan 2021 [34] | ENZAMET [5] | TITAN [7] | STAMPEDE G vs A [8] | LATITUDE [4] | STAMPEDE C vs A [8] | GETUG-AFU 15 [35] | CHAARTED [2] | STAMPEDE G vs C [8] | ARASENS [9] | PEACE-1 [10] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age, years, median | Treatment | 70 (range: 46–92) | 66 (range: 54–86) | NR | 69 (range: 45–94) | 67 (IQR: 63–72) | 68.0 (range: 38–89) | 65 (IQR: 60–70) | 63.0 (IQR: 57.0–68.2) | 64 (range: 36–88) | 66 (IQR: 61–70) | 67 (range: 89) | 66 (IQR: 60–70) |
| Control | 70 (range: 42–92) | 63 (range: 51–84) | NR | 68 (range: 43–90) | 67 (IQR: 62–72) | 67.0 (range: 33–92) | 65 (IQR: 60–71) | 64.0 (IQR: 58.0–70.0) | 63 (range: 39–91) | 66 (IQR: 62–71) | 67 (range: 42–86) | 66 (IQR: 59–70) | |
| ECOG status 0, n (%) | Treatment | 448 (78.0) | 16 (44.0) | 405 (71.9) | 328 (62.5) | 376 (75.0) | NR | 270 (75.0) | 181 (99.0) | 277 (69.8) | 300 (80) | 466 (71.6) | 250 (70.0) |
| Control | 443 (76.9) | 16 (45.0) | 405 (72.1) | 348 (66.0) | 371 (74.0) | NR | 521 (72.0) | 176 (96.0) | 272 (69.2) | 149 (79) | 462 (70.6) | 246 (69.0) | |
| ≥8 Gleason score (%) | Treatment | 386 (67.2) | 28 (77.0) | NR | 351 (66.9) | 366 (73.0) | 584 (98.0) | 253 (70.0) | 103 (55.0) | 241 (60.7) | 276 (75) | 505 (77.6) | 270 (77.0) |
| Control | 373 (64.8) | 28 (80.0) | NR | 358 (67.9) | 377 (75.0) | 586 (97.0) | 480 (66.0) | 113 (59.0) | 243 (61.8) | 153 (81) | 516 (78.9) | 276 (80.0) | |
| High volume disease, n (%) | Treatment | 354 (61.7) | 0 (0.0) | 151 (48.8) | 325 (61.9) | 271 (54.0) | 487 (81.6) | 148 (41.0) | 92 (48.0) | 263 (66.2) | NR | 500 (76.3) | 224 (63.0) |
| Control | 373 (64.8) | 0 (0.0) | 192 (61.5) | 335 (63.6) | 253 (51.0) | 464 (77.7) | 320 (44.0) | 91 (47.0) | 250 (63.6) | NR | 504 (77.7) | 232 (65.0) |
ECOG: Eastern Cooperative Oncology Group; NR: Not reported.
Multilevel network meta-regression
The ML-NMR was fit to the most commonly reported effect modifiers: age, Eastern Cooperative Oncology Group (ECOG), Gleason score and disease volume. Metastatic status at initial diagnosis (M0/M1) was also considered but could not be included due to limited variation within the studies. For example, three of the AgD studies contained fully M1 populations (LATITUDE [4], STAMPEDE arms C vs A [36], PEACE-1 [10]). One of twelve studies were missing data for ECOG, Gleason score and disease volume respectively (Table 1).
ML-NMR provided evidence of a significant benefit for the darolutamide triplet with respect to OS compared with enzalutamide + ADT, apalutamide + ADT, abiraterone + ADT and the abiraterone triplet in the ARASENS-like population. Similar results were found in the average population, although a significant benefit compared with apalutamide + ADT was not observed (Figure 4). There was evidence of greater PFS for the darolutamide triplet over apalutamide + ADT, enzalutamide + ADT, docetaxel + ADT, ADT and SNA + ADT in both populations (Figure 5).
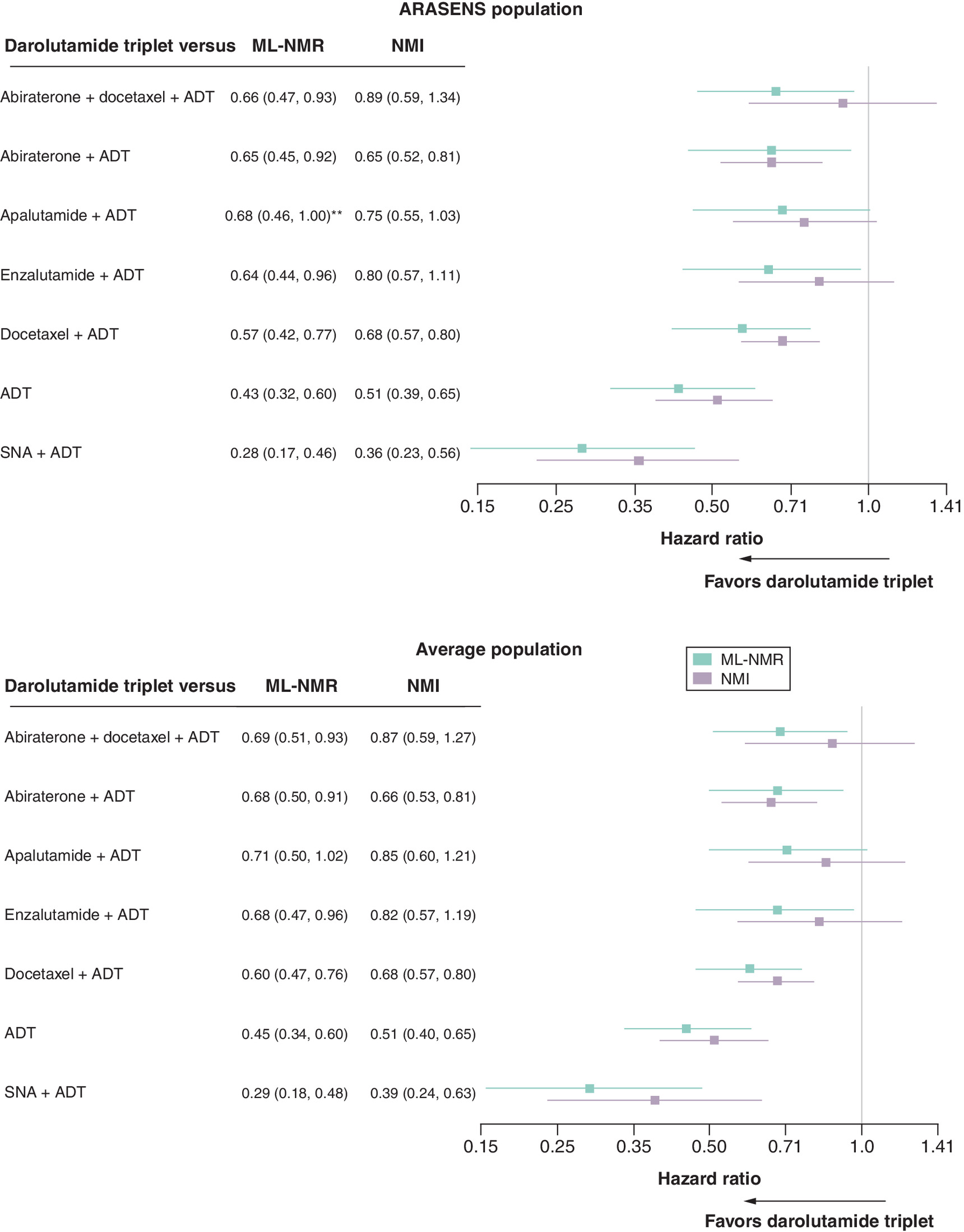
Figure 4. Hazard ratios (95% CrI) relative to darolutamide triplet on overall survival estimated by multilevel network meta-regression and network meta-interpolation.
HR <1.00 favors darolutamide triplet and 95% CrI excluding 1.00 indicates evidence of a difference. Results based on fixed effects analysis.
**Upper CrI did not cross the line of no effect.
ADT: Androgen deprivation therapy; CrI: Credible interval; SNA: Standard nonsteroidal antiandrogen.
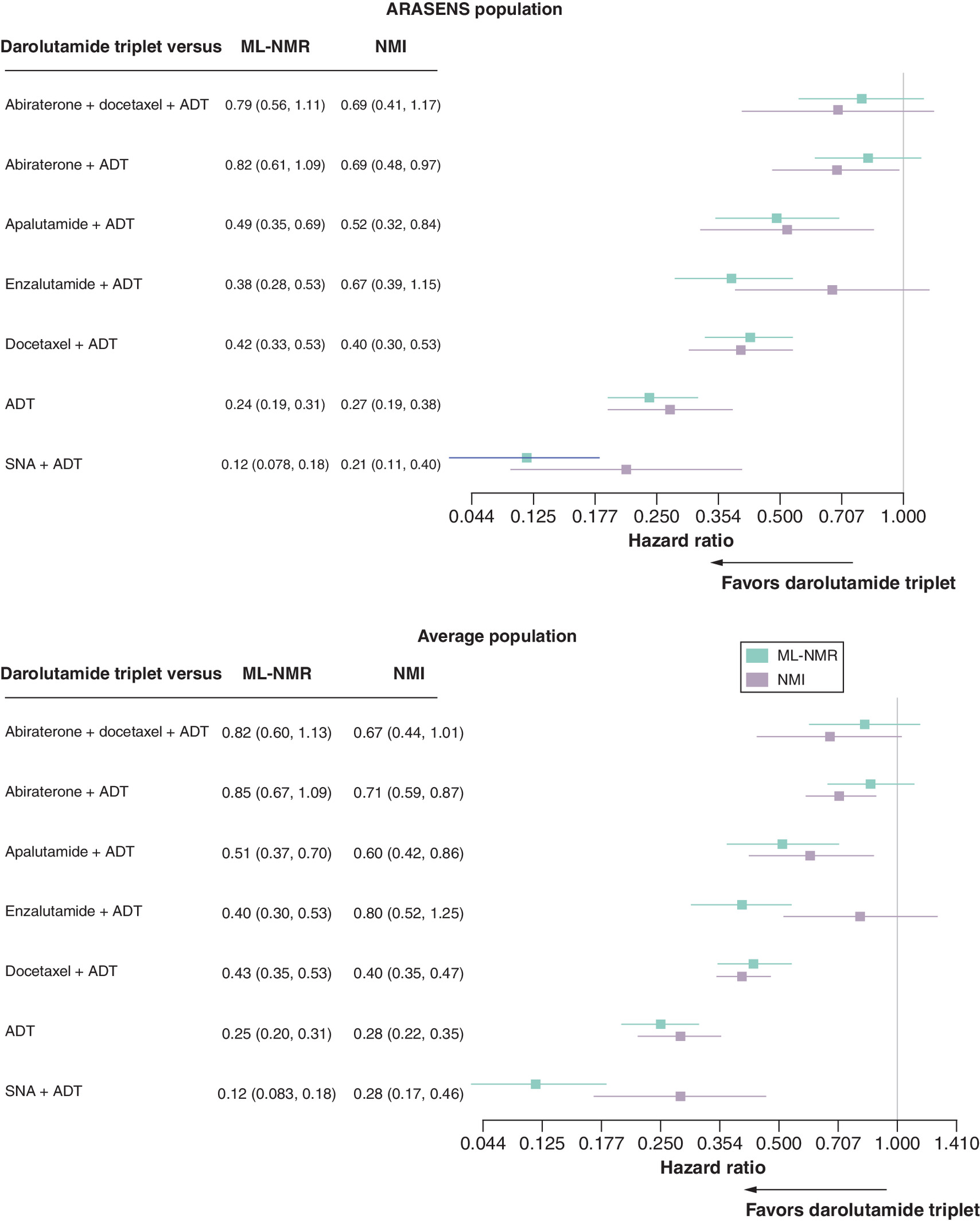
Figure 5. Hazard ratios (95% CrI) relative to darolutamide triplet on progression-free survival estimated by multilevel network meta-regression and network meta-interpolation.
HR <1.00 favors darolutamide triplet and 95% CrI excluding 1.00 indicates evidence of a difference. Results based on random effects analysis.
ADT: Androgen deprivation therapy; CrI: Credible interval; SNA: Standard nonsteroidal antiandrogen.
Network meta-interpolation
The NMI analyzed the most commonly reported effect modifier subgroups: ECOG 0/1, age <65 years old, Gleason score <7 and disease volume high/low. Full data for effect modifiers were available in only 8 of 12 studies for OS and 5 of 12 studies for PFS (Supplementary Materials Section 2.3). Borrowing of information on effect modification was possible for one study (Vaishampayan [34]) but for the other studies it was assumed that missing subgroup treatment effects were equal to the ITT treatment effect. See Supplementary Materials Section 2.5 for assumptions that were required relating to groupings within the subgroup data.
In the NMI analysis assessing OS, the darolutamide triplet was significantly favored over abiraterone + ADT, docetaxel + ADT, ADT and SNA + ADT in both populations (Figure 4). In the NMI analysis assessing PFS, the darolutamide triplet was significantly favored over abiraterone + ADT, apalutamide + ADT, docetaxel + ADT, ADT and SNA + ADT in both populations (Figure 5).
Discussion
Evaluating the efficacy of therapeutic options requires robust methodologies, particularly given the limitations of existing NMAs published in mCSPC to date. Our analysis employs ML-NMR and NMI to assess the efficacy of darolutamide triplet therapy compared with other treatment options. The results indicate that, when considering darolutamide triplet as the reference treatment, both ML-MNR and NMI showed evidence of a difference in OS and PFS against many of the other treatments. Our primary analysis assumed a target population similar to that of the ARASENS trial, where all patients were eligible for docetaxel. Notably, these results remained robust when the target population was adjusted to reflect an average population (with a mix of docetaxel eligible and ineligible patients) (Figures 4 & 5). We conclude that the darolutamide triplet demonstrates relevance for patients who are eligible for docetaxel, even as some comparator populations did not include treatment with docetaxel as a criteria for inclusion.
Despite the volume of prior NMAs, with Shore et al. identifying 15 NMAs of our included treatments in patients with mCSPC, this prior research has largely overlooked effect modification, limiting findings [11]. While several NMAs included subgroup analysis, these were often limited by underreporting and may not be powered to detect statistically significant results. Our targeted review has found effect modification to be prevalent in the mCSPC setting. Ignoring the presence of this effect modification may lead to biased results. Various methods are available to address covariate imbalance [19], and this analysis has utilized two of the best methods available in the absence of IPD on all trials. Our findings diverge from previous NMAs by identifying differences in effects between darolutamide triplet and other treatments in terms of OS and PFS [11]. Prior analyses indicated that triplet combinations were associated with greater survival benefits, but they also presented significant uncertainty, as evidenced by wide confidence intervals. Consistent with previous NMAs, our analysis has not demonstrated any significant differences between abiraterone, enzalutamide or apalutamide-based regimens.
The advantage of ML-NMR is its ability to integrate all IPD and aggregate studies in a unified analysis, producing results for any target population of interest. In contrast, NMI is a two-step process that first imputes subgroups to a single target population and then conducts standard NMA. ML-NMR also requires only baseline characteristics to be reported, does not require continuous covariates to be discretized, and makes full use of IPD, while NMI relies on the reporting of subgroup data. In addition, ML-NMR can be implemented in the R package ‘multinma’ [32], saving the user from developing custom code, while no package currently exists to implement NMI. The disadvantage of ML-NMR over NMI is that the shared effect modifier assumption is often needed. This assumption can be relaxed by making different assumptions regarding the effect modifier interactions for each treatment within a class. However, this can be difficult in practice, due to the requirement for IPD on multiple studies or larger numbers of aggregate studies. In this analysis, for example, IPD was only available from ARASENS [19,37]. Another advantage of ML-NMR it that it allows non-proportional hazards to be modeled, whereas NMI necessitates hazard ratios.
In this application, the NMI method faced challenges due to incomplete subgroup data, with full data for effect modifiers available in only 8 of 12 studies for OS and 5 of 12 studies for PFS. Borrowing of information on effect modification was possible for only one study. In addition to underreporting subgroups, most studies were underpowered to detect differences in subgroups. The ML-NMR method did not have this disadvantage as it used baseline characteristics. In addition, the use of subgroup data in NMI limits analyses beyond primary or key secondary end points such as OS and PFS for which subgroup data are commonly reported. ML-NMR can also incorporate later datacuts as only studies on the full population are needed. An advantage of the NMI method in this application was the reduced computational time compared with ML-NMR.
These methodological differences explain the differences in results between the ML-NMR and NMI. ML-NMR provided evidence of a significant benefit for darolutamide triplet with respect to OS compared with enzalutamide + ADT, apalutamide + ADT, and the abiraterone triplet, whereas NMI did not. For PFS, NMI provided evidence of a significant benefit for the darolutamide triplet compared with abiraterone + ADT and no evidence of an effect compared with enzalutamide + ADT, where ML-NMR showed the opposite. These differences are also due to incomplete subgroup data for the NMI, and its reliance on earlier datacuts as publications with later datacuts did not report subgroup results [6,8,33,35]. While ML-NMR utilised later datacuts and digitized KM data rather than reported hazard ratios, the NMI was not limited by the shared effect modifier assumption of the ML-NMR. However, as IPD was only available from ARASENS it was necessary to make a shared effect modifier assumption that all treatments other than darolutamide + docetaxel + ADT varied to the same extent with effect modifiers. This assumption strengthens the need to consider both NMI and ML-NMR when drawing conclusions in this case.
An overall limitation of our analysis is the exclusion of the ARANOTE [38] trial, which was omitted due to having a significantly shorter median follow-up compared with other studies. A further limitation of both analyses is that we could only adjust for variables that were most commonly reported and not all potential effect modifiers. In addition, the analyses were limited by reliance on a single IPD anchor.
Another limitation associated with the NMA is differences in PFS definitions across trials. Adjustments were made for this as discussed in Supplementary Materials Section 1.3.4. Additionally, crossover unadjusted HRs from ARCHES [6], TITAN [7] and LATITUDE [4] were used. The NMI could not adjust for crossover due to insufficient reporting within subgroups. Although crossover-adjusted KM curves were reported, these cannot currently be robustly included in ML-NMR as it is unclear what the impact would be on baseline characteristics and whether the distribution of effect modifiers is changed by crossover adjustment. The unadjusted and adjusted HRs in the overall patient populations are shown in Supplementary Material Section 1.3.5. As the adjusted HRs are only marginally different it is unlikely that results would be impacted. Furthermore, the Shore et al. review of NMAs in mCRPC found that all NMAs used unadjusted HRs, and this has been the approach in recent NICE appraisals in mCRPC, including that based on TITAN for apalutamide [11,39,40]. For a complete list of assumptions/limitations and justifications see Supplementary Materials Section 2.4.
Published evidence suggests that NMAs in mCSPC have often been unjustifiably duplicate and methodologically inadequate [41]. Previous analysis has assessed subgroups separately without leveraging the advantages of NMI. To address these issues, our analysis has been conducted using rigorous methodological approaches that have been recently developed and endorsed by organisations such as NICE and EUHTA. This approach provides valuable insights into available treatments and effect modification, while adjusting for population imbalances. This allows for a more accurate comparison of treatments for mCSPC.
In conclusion, our updated NMA employs rigorous methodologies to provide a comprehensive evaluation of treatment options for mCSPC. By incorporating effect modifiers and addressing population imbalances, we offer valuable insights into the efficacy of treatments within mCSPC. This analysis not only enhances the understanding of oncological treatment outcomes for mCSPC but also serves as a crucial resource for clinicians in making informed decisions that can positively impact patient care in this disease state.
Summary points
•
Recent network meta-analyses (NMAs) in metastatic castration-sensitive prostate cancer (mCSPC) have not adequately addressed potential treatment effect modifiers and population imbalances, which introduces bias.
•
Although Individual patient data are seldom available across all trials, recent methodological advances allow adjustments using a combination of Individual patient data and aggregate data.
•
This study addresses the limitations of previous NMAs in mCSPC by incorporating effect modifiers and population imbalances to provide a more accurate understanding of treatment efficacy for better-informed decision-making.
•
Twelve studies, including ARASENS, were included in the systematic review. All studies reported baseline characteristics for multilevel network meta-regression.
•
Sufficient subgroup data for network meta-interpolation were available in 8/12 studies for OS and 5/12 studies for progression-free survival (PFS).
•
Multilevel network meta-regression provided evidence of improved OS for darolutamide + docetaxel + ADT compared with abiraterone + docetaxel + ADT, apalutamide + ADT, enzalutamide + ADT and abiraterone + ADT and improved PFS compared with apalutamide + ADT and enzalutamide + ADT.
•
Using network meta-interpolation, darolutamide + docetaxel + ADT provided evidence of OS benefit over abiraterone + ADT and PFS benefit relative to abiraterone + ADT and apalutamide + ADT.
•
The findings provide evidence that darolutamide triplet therapy improves overall survival and progression-free survival outcomes compared with other therapies, offering valuable insights for treatment selection in clinical practice.
•
By discussing the strengths and limitations of NMA methodologies, this study equips clinicians with the knowledge to critically evaluate evidence from NMAs and to more accurately assess the relative benefits of therapies available for mCSPC.
Author contributions
Conception and design: N Shore, AK Morgans, N Paracha, H Thom, CJD Wallis, E Gallagher, M Boegemann. Acquisition of data: N Shore, AK Morgans, N Paracha, H Thom, CJD Wallis, E Gallagher, M Boegemann. Analysis and interpretation of data: N Shore, AK Morgans, N Paracha, H Thom, E Keeney, P Orishaba, D Phillippo, D Aceituno, CJD Wallis, E Gallagher, M Boegemann. Drafting of the manuscript: N Shore, AK Morgans, N Paracha, H Thom, E Keeney, P Orishaba, D Aceituno, CJD Wallis, E Gallagher, M Boegemann. Critical revision of the manuscript for important intellectual content: N Shore, AK Morgans, N Paracha, H Thom, E Keeney, P Orishaba, D Phillippo, D Aceituno, CJD Wallis, E Gallagher, M Boegemann. Statistical analysis: H Thom, E Keeney, P Orishaba, D Aceituno. Obtaining funding: N Shore, H Thom, A K Morgans, N Paracha, CJD Wallis, E Gallagher, M Boegemann. Administrative, technical, or material support: N Shore, AK Morgans, N Paracha, H Thom, E Keeney, P Orishaba, D Phillippo, D Aceituno, CJD Wallis, E Gallagher, M Boegemann. Supervision: N Shore, AK Morgans, N Paracha, H Thom, CJD Wallis, E Gallagher, M Boegemann. All authors provided final approval of the version of the article to be published.
Financial disclosure
This study was supported by Bayer HealthCare Pharmaceuticals Inc.
Competing interests disclosure
N Shore has received honoraria from Bayer, Janssen, Dendreon, Tolmar, Ferring, Astellas, Amgen, Pfizer, AstraZeneca, Merck, Sumitomo, Lantheus, Clarity, Telix and Daiichi-Sankyo. AK Morgans has received honoraria from Astellas, AstraZeneca, AAA, Bayer, Exelixis, Lantheus, Novartis, Pfizer, Myovant, Myriad, Merck, Sanofi and Telix. N Paracha and E Gallaher are employees at Bayer HealthCare Pharmaceuticals Inc. H Thom is shareholder and E Keeney, D Aceituno and P Orishaba are employees of Clifton Insight which has received consulting fees from Bayer HealthCare Pharmaceuticals Inc., Novartis, MSD, Merck, Janssen, Pfizer, Daiichi-Sankyo, Eisai, Argenx, Amicus, Baxter, and Roche. D Phillippo has received consulting fees from Bayer HealthCare Pharmaceuticals Inc. and BeiGene, Ltd. CJD Wallis is supported by the Hold'em for Life Early Career Professor in Cancer Research, a University limited-term named professorship at the University of Toronto. He has also received consulting fees from Janssen Oncology, Nanostics Inc, Precision Point Specialty LLC, SESEN Bio; Honoraria/Travel: AbbVie, Astellas, Astra Zeneca, Bayer, EMD Serono, Haymarket Media, Healing and Cancer Foundation, Knight Therapeutics, Merck, Science & Medicine Canada, TerSera Canada, Tolmar Pharmaceuticals Canada. He has received research funding from Knight Therapeutics, Tolmar Pharmaceuticals, Bayer, Sunnybrook HSC AFP. M Boegemann has received honoraria from Astellas, AstraZeneca, AAA, Amgen, Bayer, Exelixis, Novartis, Pfizer, Lilly, MSD, BMS, Merck, Janssen, Gilead, EUSApham, Eisai. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of this shared data are in accordance with the terms (if any) agreed upon their receipt. This analysis used IPD from the ARASENS trial and ITT AgD from comparator studies.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 461.90 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Sartor O, de Bono JS. Metastatic prostate cancer. N. Engl. J. Med. 378(7), 645–657 (2018).
2.
Sweeney CJ, Chen YH, Carducci M et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N. Engl. J. Med. 373(8), 737–746 (2015).
3.
Sydes MR, Spears MR, Mason MD et al. Adding abiraterone or docetaxel to long-term hormone therapy for prostate cancer: directly randomised data from the STAMPEDE multi-arm, multi-stage platform protocol. Ann. Oncol. 29(5), 1235–1248 (2018).
4.
Fizazi K, Tran N, Fein L et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 377(4), 352–360 (2017).
5.
Davis ID, Martin AJ, Stockler MR et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N. Engl. J. Med. 381(2), 121–131 (2019).
6.
Armstrong AJ, Azad AA, Iguchi T et al. Improved survival with enzalutamide in patients with metastatic hormone-sensitive prostate cancer. J. Clin. Oncol. 40(15), 1616–1622 (2022).
7.
Chi KN, Agarwal N, Bjartell A et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 381(1), 13–24 (2019).
8.
James ND, Clarke NW, Cook A et al. Abiraterone acetate plus prednisolone for metastatic patients starting hormone therapy: 5-year follow-up results from the STAMPEDE randomised trial (NCT00268476). Int. J. Cancer 151(3), 422–434 (2022).
9.
Smith MR, Hussain M, Saad F et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N. Engl. J. Med. 386(12), 1132–1142 (2022).
10.
Fizazi K, Foulon S, Carles J et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, Phase III study with a 2 × 2 factorial design. Lancet 399(10336), 1695–1707 (2022).
11.
Shore N, Morgans AK, Paracha N et al. Darolutamide for metastatic hormone-sensitive prostate cancer: an overview of meta-analyses and indirect treatment comparisons. Rev. Urol. 24(1), (2024). Available from: https://reviewsinurology.com/issues/vol/24/no/1/darolutamide-for-metastatic-hormone-sensitive-prostate-cancer-an-overview-of-meta-analyses-and-indirect-treatment-comparisons
12.
Dias S, Welton N, Sutton A, Ades A. NICE DSU Technical Support Document 2: A generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. NICE, UK (2014).Available from: https://www.ncbi.nlm.nih.gov/books/NBK310366/
13.
Hoaglin DC, Hawkins N, Jansen JP et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR Task Force on indirect treatment comparisons good research practices: part 2. Value Health 14(4), 429–437 (2011).
14.
Jansen JP, Fleurence R, Devine B et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on indirect treatment comparisons good research practices: part 1. Value Health 14(4), 417–428 (2011).
15.
Kanters S, Ford N, Druyts E et al. Use of network meta-analysis in clinical guidelines. Bull. World Health Organ. 94(10), 782–784 (2016).
16.
Chaimani A, Caldwell DM, Li T, Higgins JP, Salanti G. Chapter 11: undertaking network meta-analyses [last updated October 2019]. In: Higgins JP, Thomas J, Chandler Jet al. et al. (Eds). Cochrane Handbook for Systematic Reviews of Interventions, Version 6.5. Cochrane (2024). Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook/current/chapter-11
17.
Ades AE, Welton NJ, Dias S, Phillippo DM, Caldwell DM. Twenty years of network meta-analysis: continuing controversies and recent developments. Res. Synth. Methods 15(5), 702–727 (2024).
18.
Vale CL, Fisher DJ, Godolphin PJ et al. Which patients with metastatic hormone-sensitive prostate cancer benefit from docetaxel: aa systematic review and meta-analysis of individual participant data from randomised trials. Lancet Oncol. 24(7), 783–797 (2023).
• Previous network meta-analysis in the metastatic castration-sensitive prostate cancer (mCSPC) population addressing covariate imbalances using individual patient data (IPD) hence suggesting valuable methodological perspectives.
19.
Phillippo DM, Dias S, Ades AE et al. Multilevel network meta-regression for population-adjusted treatment comparisons. J. R. Stat. Soc. Ser. A Stat. Soc. 183(3), 1189–1210 (2020).
•• This publication proposed the multilevel network meta-regression method, one of the methods which we implement in the current publication.
20.
Dias S, Sutton AJ, Welton NJ, Ades AE. Evidence synthesis for decision making 3: heterogeneity – subgroups, meta-regression, bias, and bias-adjustment. Med. Decis. Making 33(5), 618–640 (2013).
21.
Armstrong AJ, Pandya BJ, Bhadauria HS et al. Matching-adjusted indirect comparison of enzalutamide versus darolutamide doublet in MHSPC. Future Oncol. 21(19), 2459–2469 (2025).
22.
Harari O, Soltanifar M, Cappelleri JC et al. Network meta-interpolation: effect modification adjustment in network meta-analysis using subgroup analyses. Res. Synth. Methods 14(2), 211–233 (2023).
•• This publication proposed the network meta-interpolation (NMI) method which uses subgroup analyses to adjust for effect modification that does not assume shared effect modification.
23.
Welton NJ, Phillippo DM, Owen R et al. CHTE2020 sources and synthesis of evidence; update to evidence synthesis methods. (2020). Available from: https://sheffield.ac.uk/nice-dsu/methods-development/chte2020-sources-and-synthesis-evidence
24.
Directorate-General for Health and Food Safety. Methodological guideline for quantitative evidence synthesis: direct and indirect comparisons (2024). Available from: https://health.ec.europa.eu/latest-updates/methodological-guideline-quantitative-evidence-synthesis-direct-and-indirect-comparisons-2024-03-25_en
25.
Gates M, Gates A, Pieper D et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the prior statement. BMJ 378, e070849 (2022).
26.
Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int. J. Surg. 88, 105906 (2021).
27.
Phillippo D, Ades A, Dias S et al. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submission to NICE. NICE, UK (2016).
28.
Menges D, Yebyo HG, Sivec-Muniz S et al. Treatments for metastatic hormone-sensitive prostate cancer: systematic review, network meta-analysis, and benefit–harm assessment. Eur. Urol. Oncol. 5(6), 605–616 (2022).
• Previous network meta-analysis in the mCSPC population assessing the efficacy and safety of treatment options and highlighting important methodological considerations.
29.
Yanagisawa T, Rajwa P, Thibault C et al. Androgen receptor signaling inhibitors in addition to docetaxel with androgen deprivation therapy for metastatic hormone-sensitive prostate cancer: a systematic review and meta-analysis. Eur. Urol. 82(6), 584–598 (2022).
• Previous network meta-analysis in the mCSPC population assessing the efficacy and safety of treatment options and highlighting important methodological considerations.
30.
Lunn D, Jackson C, Best N, Thomas A, Spiegelhalter DJ. The Bugs Book: a practical introduction to Bayesian analysis. Texts in statistical science. CRC Press (2013).
31.
The R Project for statistical computing. Available from: https://www.r-project.org/
32.
Phillippo DM. multinma: Bayesian network meta-analysis of individual and aggregate data (2025). Available from: https://research-information.bris.ac.uk/en/publications/multinma-bayesian-network-meta-analysis-of-individual-and-aggrega/
33.
Tripathi A, Chen Y-H, Jarrard DF et al. Eight-year survival rates by baseline prognostic groups in patients with metastatic hormone-sensitive prostate cancer (mHSPC): an analysis from the ECOG-ACRIN 3805 (CHAARTED) trial. J. Clin. Oncol. 40(Suppl. 16), 5081–5081 (2022).
34.
Vaishampayan UN, Heilbrun LK, Monk P 3rd et al. Clinical efficacy of enzalutamide vs bicalutamide combined with androgen deprivation therapy in men with metastatic hormone-sensitive prostate cancer: a randomized clinical trial. JAMA Netw. Open 4(1), e2034633 (2021).
35.
Gravis G, Boher JM, Joly F et al. Androgen deprivation therapy (ADT) plus docetaxel versus ADT alone in metastatic non castrate prostate cancer: impact of metastatic burden and long-term survival analysis of the randomized Phase III GETUG-AFU15 trial. Eur. Urol. 70(2), 256–262 (2016).
36.
James ND, Sydes MR, Clarke NW et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 387(10024), 1163–1177 (2016).
37.
Phillippo DM, Dias S, Ades AE et al. Validating the assumptions of population adjustment: application of multilevel network meta-regression to a network of treatments for plaque psoriasis. Med. Decis. Making 43(1), 53–67 (2023).
38.
Saad F, Vjaters E, Shore N et al. Darolutamide in combination with androgen-deprivation therapy in patients with metastatic hormone-sensitive prostate cancer from the Phase III ARANOTE trial. J. Clin. Oncol. 42(36), 4271–4281 (2024).
39.
NICE. Darolutamide with androgen deprivation therapy and docetaxel for treating hormone-sensitive metastatic prostate cancer. TA903 (2023). Available from: https://www.nice.org.uk/guidance/ta903
40.
NICE. Apalutamide with androgen deprivation therapy for treating hormone-sensitive metastatic prostate cancer. TA741 (2021). Available from: https://www.nice.org.uk/guidance/ta741
41.
Fisher DJ, Burdett S, Vale C, White IR, Tierney JF. Duplicated network meta-analysis in advanced prostate cancer: a case study and recommendations for change. Syst. Rev. 11(1), 274 (2022).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 17 June 2025
Accepted: 5 December 2025
Published online: 6 January 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Population-adjusted network meta-analyses provide new insights into the efficacy of treatment alternatives for metastatic castration-sensitive prostate cancer. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0100
Export citation
Select the citation format you wish to export for this article or chapter.